new insights into vulnerable plaque
TRANSCRIPT





Hypothesis:
Monocyte-macrophages on or just beneath the plaque surface are detectable by the heat that they produce.





Multiple
non-stenotic coronary plaques
In vivo live animal study
Marked temperature heterogeneity observed with continuous blood flow

Intravascular Thermosensor Basket Catheter
Volcano Therapeutics Inc
(prototype)

Stefanadis et al, 1999First in vivo human intra-coronary thermometry study

Stefanadis et al, 2000

Coronary Infrared Thermography Catheter(prototype)



Apo-E aorta heated at 37C (staining for TUNEL and DAPI)

Apo-E aorta heated at 42 C (TUNEL and DAPI staining)
TUNEL
DAPI

DNA isolation from atherosclerotic aorta of apo-E mice by agarose gel electrophoresis
37C
37C
37C42C42C
42C




We hypothesized that plaque inflammation and macrophage infiltration can be detected by:
1- Decreased plaque pH and increased pH heterogeneity and excessive lactate content
2- pH and temperature of plaque are inversely correlated

pH Distribution in 48 Human Carotid Plaques
pH
9.008.88
8.758.63
8.508.38
8.258.13
8.007.88
7.757.63
7.507.38
7.257.13
7.006.88
6.756.63
No
of p
oint
s w
ith th
e sa
me
ph
140
120
100
80
60
40
20
0
There is a bimodal distribution of pH with a marked pH variation ranging from 6.5 to 8.9 (in 858 points)

Correlation of pH and Temperature in Human Carotid Plaques

Iron staining of mouse circulating monocyte after 30 minutes

MR Image of Abdominal Aorta After SPIO Injection in Mouse
Apo E deficient mouse
C57B1 (control) mouse
Before injection After injection (5 Days )
Dark (negatively enhanced) aortic wall, full of iron particles
Bright aortic lumen and wall without negative enhancement and no significant number of iron particles

The Online Cardiovascular Research Community
www.VulnerablePlaque.org

Conclusions
1. Temperature at the lumen of living carotid plaques correlates with density of inflammatory cells, and inversely with cap thickness.
2. Differences of more than 0.3 C were seen in all specimens but only a minority had differences of 2o C or more.
3. Large differences in temperatures were more often found in patients who were younger, symptomatic, female, and not taking aspirin.

Conclusionscontinued
4. These temperature differences can be detected by infrared cameras.
5. Compared to normal arteries, inflamed and lipid-rich plaques are acidic, while calcified and thrombosed plaques are alkaline.
6. Plaque pH correlates moderately and inversely) with plaque temperature.

Conclusionscontinued
7. Stefanadis and colleagues have reported that hot plaques confer higher risk; it will be important to determine whether plaque prognosis is best determined by T, T, pH, pH or a combination.
8. Heating to 41oC decreases expression of pro-inflammatory genes.
9. Heating to 42-43oC causes apoptosis, mainly of macrophages.

Conclusionscontinued
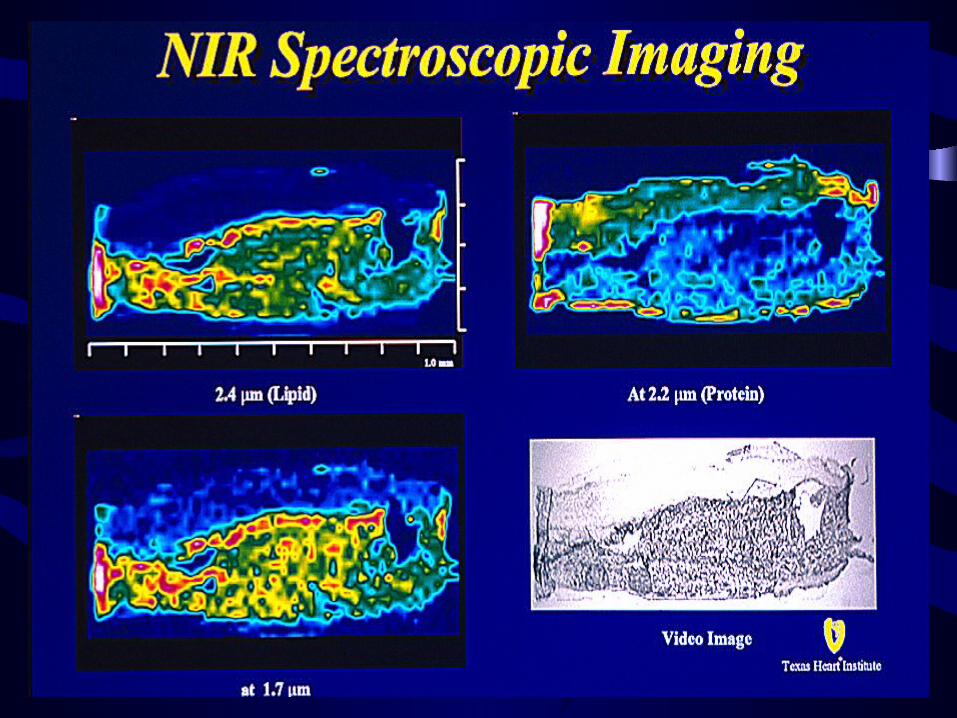
10.10. Near-IR Spectroscopy can estimate plaque Near-IR Spectroscopy can estimate plaque protein/lipid ratios and may also provide protein/lipid ratios and may also provide inferences as to concentrations of plaque inferences as to concentrations of plaque HH++, NO, glucose, O, NO, glucose, O2 2 and oxidants.and oxidants.
11.11. IR and near IR may predict plaque IR and near IR may predict plaque behaviour alone or in combination with behaviour alone or in combination with ultrasound, angioscopy, magnetic ultrasound, angioscopy, magnetic resonance or immunoscintigraphyresonance or immunoscintigraphy

www.HotPlaque.com