tch app conference april 2019multitonal) 34 congenitalheartdefects atrial&septal&defect&...
TRANSCRIPT

Murmurs and the Cardiac Physical Exam
Carolyn A. Altman Texas Children’s Hospital Advanced Practice Provider Conference Houston, TX April 6 , 2018
2
The Cardiac Physical Exam
Before applying a stethoscope…..
Some pearls on • General appearance • Physical exam beyond the heart

3
Jugular Venous Distention Pallor
Cyanosis

4
Work of Breathing
Normal infant breathing
Quiet Tachypnea
Increased Rate, Work of Breathing

5
Beyond the Chest
Clubbing
Observed in children older than 6 mos with chronic cyanosis
Loss of the normal angle of the nail plate with the axis of the finger
Abnormal sponginess of the base of the nail bed
Increasing convexity of the nail
Etiology: ? sludging

6
Chest
❖ Chest wall development and symmetry
❖ Long standing cardiomegaly can lead to hemihypertrophy and flared rib edge: Harrison’s groove or sulcus

7
Ready to Examine the Heart
Palpation
Auscultation
General overview
Defects
Innocent versus pathologic

8
Cardiac Palpation
❖ Consistent approach: palm of your hand, hypothenar eminence, or finger tips
❖ Precordium, suprasternal notch
❖ PMI?
❖ RV impulse?
❖ Thrills?
❖ Heart Sounds?

9
Cardiac Auscultation
Where to listen:
★ 4 main positions
★ Inching
★ Ancillary sites: don’t forget the head in infants

10
Cardiac Auscultation
Focus separately on
v Heart sounds:
• S2 normal splitting and intensity?
• Abnormal sounds? Clicks, gallops
v Murmurs
v Rubs

11
Cardiac Auscultation
Etiology of heart sounds: Aortic and pulmonic valves actually close silently
Heart sounds reflect vibrations of the cardiac structures after valve closure
Sudden deceleration of retrograde flow of the column of blood in the aorta and pulmonary artery when the elastic limits of the tensed valve leaflets are met

12
Cardiac Auscultation
S2
❖ Physiologic splitting of S2: Increased systemic venous return and increased pulmonary capacitance during inspiration causes delayed closure of the pulmonary valve
❖ S2 cannot be considered “normal” unless physiologic splitting is heard

13
S2: normal splitting Single S2: Pulmonar Hypertension
Wide, fixed splitting: ASD Paradoxical Splitting of S2: LBBB, severe LVOTO

14
S2 HInts
❖ If splitting persists while patient supine, try sitting position-‐ less volume in heart may normalize splitting
❖ Listen for splitting at mid to ULSB in kids
❖ Infants: Mid to LLSB ❖ Splitting of S2 if the HR is over 160
hard to hear: gently blowing a breath in the baby’s face will slow HR

15
Cardiac Auscultation: S1
❖ Physiologic splitting of S1:
❖ Can be heard in children with slower heart rates.
❖ Varies with respiration as does S2
❖ Soft S1: low cardiac output, tachycardia
❖ Loud S1: hyperdynamic (fever, exercise), mitral stenosis

16
Cardiac Auscultation
Gallops: S3 or S4
❖ Short, low pitched diastolic sounds
❖ Abnormal ventricular function

17
Auscultation: S3 Gallop
❖ Mid way thru diastole
❖ Muscle tensing at end of rapid, early filling which occurs with ventricular relaxation
❖ Later than split S2
❖ Earlier than S4

18
Auscultation: S4 Gallop
❖ If impaired ventricular relaxation, less filling of the ventricles during during early diastole and more during atrial contraction
❖ Hypertrophic cardimyopathy, eg
❖ S4 is thus a sound generated late in diastole
❖ Very close to S1, can mistake for split S1 or S1-‐ ejection click
S1-Ej click S4
19
S3 and S4 Gallops
❖ Heard best with bell since low pitched
❖ Can extinguish the sound by pressing too hard (turning bell into diaphragm)
❖ Usually heard over mitral area, if LV dysfunction
❖ Listen in left lateral decubitus position too
❖ If RV dysfunction-‐may hear best at LLSB
S4
S3
S1-Ej click

20
Other Extra Heart Sounds
❖ Ejection Click: opening of the aortic or pulmonary valve
❖ Mid-‐systolic click: MVP
❖ Opening snap of MS
❖ Listen for difference in timing, cadence

21
How to Characterize Murmurs
❖ Timing
❖ Site of maximum intensity
❖ Intensity
❖ Radiation
❖ Pitch:
❖ Associated findings: clicks, rumbles, precordial activity
❖ Different from previous in your patient
❖ Innocent or pathologic

22
Timing of Murmurs
Systolic ? Diastolic? or Continuous ?
❖ Systolic occurs as the heart contracts
❖ Diastolic as the heart relaxes
❖ Continuous murmurs continue from systole into diastole
❖ Find S2 and listen to whether the murmur comes before it, after it, or through it
❖ Inching the stethoscope can help with timing

23
Murmurs: Timing
Systolic murmurs:
❖ Regurgitant murmurs: Begin with S1
❖ Ejection murmurs: Begins shortly after S1
❖ Mid-‐systolic: MVP

24
Regurgitant Systolic Murmurs
❖MR, TR, VSD
❖Begin with S1: “coincident with S1”
❖Often holosystolic

25
Systolic Ejection Murmurs
❖AS/PS, Still’s, pulmonary flow
❖Begin after valve opens, so hear S1 then murmur
❖ Should be able to hear S2 distinctly
❖ Early systolic ejection click if semilunar valve stenosis

26
Mid Systolic Murmurs
❖Mitral valve prolapse
❖Click ushers in murmur
27
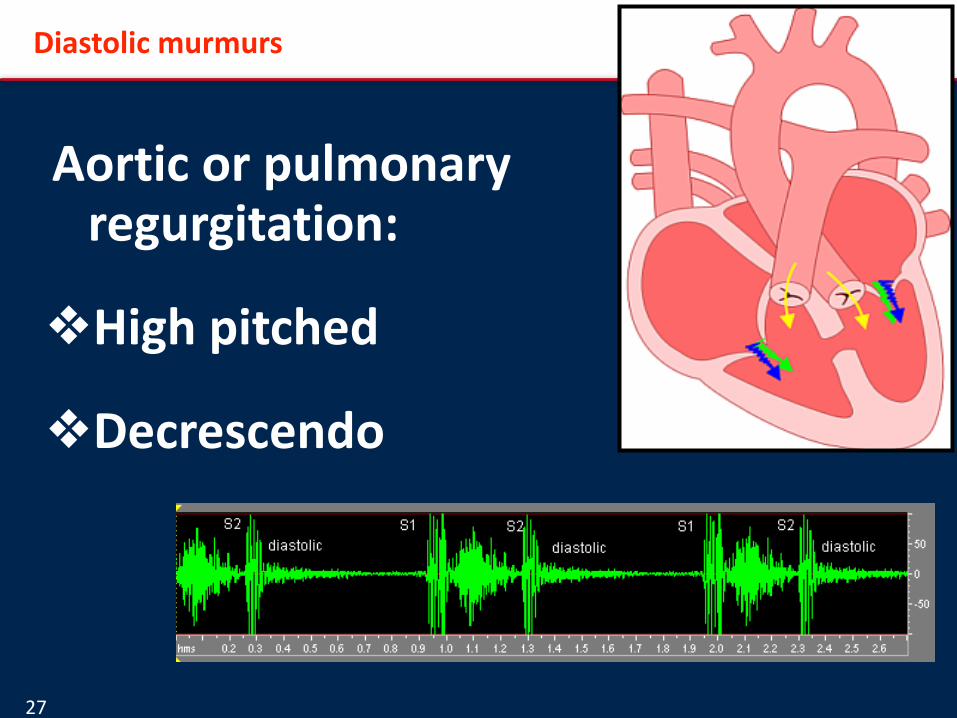
Diastolic murmurs
Aortic or pulmonary regurgitation:
❖High pitched
❖Decrescendo

28
Diastolic murmurs
Diastolic rumbles:
❖ Increased volume across MV or TV
❖ Low pitched filling noise
❖ Absence of silence

29
Continuous Murmurs
❖ Start during systole, continue past S2
❖ Louder in systole: PDA, AVM, shunts
❖ Louder in diastole: venous hums, coronary fistula
PDA Coronary fistula AVM
Venous Hum

30
Murmurs by location of greatest intensity:
Helpful in figuring out what is generating the murmur
❖ URSB: Aortic stenosis ❖ ULSB: Pulmonary
stenosis, pulmonary flow, ASD
❖ LLSB: VSD, Still’s, TR ❖ Apical: Mitral

31
Characterize Murmurs:
Grading system allows accurate communication between caretakers
❖ Grade I: is there something there? ❖ Grade II: Ok, I can hear it ❖ Grade III: Boy, that’s loud ❖ Grade IV: Associated with a thrill, knock your socks
off loud ❖ Grade V: Audible with scope off chest ❖ Grade VI: Audible without stethoscope

32
Characterize Murmurs:
Important to follow trends: ❖ Is an aorto-‐pulmonary shunt murmur getting softer?
A shunt may be getting obstructed, outgrown, or PVR elevated
❖ Is the outflow tract obstruction getting worse in a patient with new chest pain?
❖ Is the patient with TOF spelling or just colicky: the outflow murmur will get softer during a spell as less flow traverses the RVOT

33
Characterize Murmurs by Pitch:
❖ High
❖ Low
❖ Harsh (multitonal)

34
Congenital Heart Defects
❖ Atrial Septal Defect ❖ Patent Ductus Arteriosus ❖ Ventricular Septal Defect ❖ Pulmonary Stenosis ❖ Aortic Stenosis

35
CHD: Atrial Septal Defect
❖ Anatomy: described by location in the septum Secundum Primum Coronary Sinus Sinus Venosus
❖ Physiology and physical signs the same, regardless of location of ASD

36
CHD: Atrial Septal Defect
Physiology: Amount of shunting depends on
v Size of defect v Differences in compliance between RV
and LV-‐ flow is usually left to right

37
CHD: Atrial Septal Defect
Palpation: right ventricular impulse from increased RV volume

38
CHD: Atrial Septal Defect
❖ Widely split S2: v Persistent separation
of A2P2 components of S2 throughout respiratory cycle
v Increased pulmonary capacitance or
v Reciprocal changes in flow into the right atrium from the defect or systemic veins

39
CHD: Atrial Septal Defect
❖ Pulmonary flow murmur: v Large volume of blood crossing the
pulmonary valve v ULSB to back v Ejection v Medium pitched

40
CHD: Atrial Septal Defect
Diastolic Rumble: Consistent with at least 2:1 Qp:Qs Low pitched Listen with bell at LLSB

41
CHD: Patent Ductus Arteriosus
Physiology: v In the setting of low
pulmonary vascular resistance, flow is continuous, left to right
v If large PDA, PA pressures may be high: flow can be
•Left to right •Bidirectional •All right to left
42
CHD: Patent Ductus Arteriosus
Palpation ❖ RV impulse if pulmonary hypertension ❖ Hyperactive LV impulse if large volume
of flow PDA

43
CHD: PDA Murmur
v Continuous if low pulmonary vascular resistance
v Machinery like v Accentuated at end systole v Left infra-‐clavicular area, back, and left
supraclavicular areas

44
CHD: Ventricular Septal Defect
Anatomy described by location Perimembranous Inlet Muscular Doubly committed-‐
juxtarterial

45
CHD: VSD
Physiology: amount of shunting depends on
❖ Size of defect
❖ Pulmonary resistance: more shunting with decreasing resistance

46
CHD: VSD
Palpation: ❖ Quiet precordium? ❖ RV impulse may be present with volume or pressure loading
❖ +/-‐ thrill: cannot determine size by presence of thrill

47
CHD: VSD
S2 in VSDs can be ❖ Normally split (typical) ❖ Widely split if very generous amount of flow crossing to fill RV ❖ Single: if pulmonary hypertension with elevated resistance

48
CHD: VSD Auscultation
Murmur ❖ Usually along LSB ❖ Very small defects do not radiate ❖ Subpulmonary VSDs follow the RV
outflow to the pulmonary arteries ❖ “Blowing” quality ❖ Start with S1

49
CHD: VSD murmurs
Holosystolic murmur: ❖ Starts with S1
(obscured) ❖ Ends with P2, S2 split
normally ❖ Plateau shape ❖ The smaller the defect,
the more high pitched

50
CHD: VSD murmur
Short systolic murmur consistent with very small defect v Starts with S1 v Ends before S2, as defect closed by ventricular
contraction v Usually very localized, may only hear in certain
positions

51
CHD: VSD
Mitral Rumble
vIndicates at
least 2:1 Qp:Qs
vLow pitched
vUse bell at apex

52
CHD: VSD
Diastolic rumble
Can be quite subtle
Listen for absence of diastolic silence
Compare right and lef chest

53
CHD: VSD
Very Large VSDs
vAllow high pressure and high flow
v If lef unrepaired: elevated PVR develops,
eventually Eisenmenger syndrome
Palpahon
v RV impulse
v Palpable S2

54
CHD: VSD
Large VSDs:
Systolic Murmur
vCan be holosystolic, if any pressure restrichon
v If no pressure restrichon, may be no murmur, or a pulmonary ouilow murmur

55
CHD: VSD
Eisenmenger’s
v S2 loud and single
v Pulmonary valve click: dilated pulmonary root
v Graham-‐Steele murmur: pulmonary insufficiency

56
CHD: Tetralogy of Fallot
Physiology:
v Balance between VSD flow and pulmonary valve and sub valve stenosis
v “Pink” tets have little pulmonary stenosis
v Other extreme: pulmonary atresia with VSD
v PS typically progresses over time

57
CHD: TOF
Palpahon:
v RV impulse
v Possible thrill

58
CHD: TOF
Systolic Murmur: reflects PS, not VSD
v MLSB to ULSB to back
v Starts with S1, given subvalvar component
v As subps worsens, murmur decreases in intensity: pop-‐off through VSD to systemic circulahon
v Listen for murmur to decrease in hypercyanohc spell

59
CHD: TOF
❖ Systolic Murmur: reflects PS, not VSD
60
CHD: TOF post repair
To and fro murmur ❖ PS/PI ❖ The murmur does
not carry through S2-‐not continuous, not the diastolic component
❖ The diastolic murmur is of a different pitch

61
CHD: Pulmonary Valve Stenosis
❖ Anatomy: thickened, possibly dysplashc valve with limited systolic excursion
❖ Physiology: usually slowly progressive obstruchon

62
CHD: Pulmonary Valve Stenosis
Palpahon:
v RV impulse: more than mild obstruchon
v Thrill indicates more severe obstruchon

63
CHD: Pulmonary Valve Stenosis
Systolic Ejechon Click:
v Either at ULSB, or upstream from valve at LLSB
v Increases in intensity with expirahon
v Moves closer to S1 with increasing PS
64
CHD: Pulmonary Valve Stenosis
Systolic Murmur:
v Louder, longer, and later peaking with increasing stenosis
v ULSB radiahng to back, axilla

65
CHD: Aortic Valve Stenosis
Anatomy:
Thickened valve with decreased excursion
Ofen bicommissural
Physiology:
Obstruchon can be rapidly progressive, parhcularly in infants
Exercise increases the relahve stenosis
66
CHD: Aortic Valve Stenosis
Palpahon:
v Increased LV impulse with significant obstruchon
v Thrills frequently presents
vDo NOT reflect severity
vCan be along LVOT, ULSB, carohds, suprasternal notch

67
CHD: Aortic Valve Stenosis
Ejechon click: vOpening of non-‐compliant valve
v Moves earlier in systole with increasing severity of obstruchon, may become inaudible
v Heard at apex (upstream) or URSB (downstream)

68
CHD: Aortic Valve Stenosis
Murmur:
v With increasing stenosis and normal cardiac output, murmur becomes louder, longer, later peaking
vMay not have significant murmur if poor funchon (neonatal AS)
v Heard at apex (upstream) or URSB (downstream)

69
Innocent Murmurs:
❖ Learn to recognize the three most common innocent murmurs of childhood: ❖ Venous hums, ❖ Still’s murmurs ❖ Physiologic pulmonary branch stenosis
in infancy
❖ Anything else is not likely to be normal!
70
Innocent Murmurs: Still’s
Shll’s: most common innocent murmur
❖ I-‐III/VI SEM
❖ Sofer with standing or sinng
❖ Vibratory, twanging
❖ Low pitched, best heard with bell

71
Still’s murmur versus subaortic stenosis
Subaortic stenosis can mimic Still’s: both can be musical

72
Still’s murmur versus Subaortic Stenosis
❖ Use positional changes to help distinguish subAS from Still’s
❖ Dynamic obstruction in HCM accentuated with decrease in filling: murmur gets louder with stand
❖ Discrete sub AS will not usually get louder, but will also not diminish with stand
73
Innocent Murmur: Venous Hum
Venous Hum: innocent continuous murmur
❖ Turbulent flow merging from internal jugular and subclavian veins into SVC
❖ Louder in diastole
❖ Disappear when patient lies supine or turns head
❖ Audible along infraclavicular area, and low anterior neck (not the head)
❖ I-‐III/VI

74
Innocent Murmur: Venous Hum
Continuous murmur: whining, roaring, whirring, waterfall

75
Venous Hum versus Pathologic Continuous Murmurs
❖ PDA
❖ Coronary fistula
❖ Cranial AVM
❖ AO-‐PA shunt

76
Innocent Murmur: Peripheral Pulmonary Stenosis
❖ PPS in infant under 6 mos: same pitch as respirations
❖ As loud or loudest in back or axilla
❖ Systolic, high pitched, blowing
❖ Relatively small branch Pas arising at acute angle from large MPA

77
PPS versus Pathologic Murmurs
PPS-‐distinguish from
❖ Tiny VSD: better heard at mid to LLSB, not back/axilla
❖ PS: has a click
❖ ASD: Has abnl S2
78
Position Changes
❖ Distinguish innocent Still’s murmurs from LVOTO ❖ Detect gallops: apex, left lateral decubitus ❖ Distinguish venous hums from non-‐innocent
continuous murmurs ❖ Mitral valve prolapse

79
Mitral Valve Prolapse

80
Auscultation
Artificial valves: should be audible without a stethoscope
★ Artificial aortic valves should have a mechanical S2
★ Artificial mitral valves should have a mechanical S1
★ Worry if it goes away-‐valve thrombosis
81
Tips for better exams
❖ Quiet room ❖ Recognize that naptime, stranger anxiety, hunger
can adversely affect the situation ❖ Make the child as comfortable as possible: ❖ Silent distracters to entertain the child-‐flashlight, ID
badge, toys, siblings

82
Tips for Better Exams
★ Tiny bodies: Use the right size stethoscope to minimize ambient noise and to accurately determine the presence and location of a murmur
★ Change the order of the exam to fit the child ★ Warm hands and scopes

83
★ Remember-‐
★ Always not normal: RV impulse, thrills, apical murmurs, murmurs that increase with sitting or standing, murmurs with extra heart sounds, diastolic murmurs
★ Need to have a normally split S2 to be normal
★ If it does not sound innocent-‐ needs further evaluation
★ Thank you.