targeted literature review - health protection scotland … literature review: what are the key...
TRANSCRIPT

Targeted literature review:
What are the key infection prevention and control recommendations to inform a peripheral vascular catheter
(PVC) maintenance care quality improvement tool?
Part of HAI Delivery Plan 2011-2012:
Task 6.1: Review of existing infection prevention and control quality improvement tools to
ensure ongoing need and fitness for purpose
Version 1.0: April 2012

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
HPS ICT Document Information Grid
Purpose:
To present a review of the evidence to inform the content of HAI related
quality improvement tools for NHSScotland. This supports the functions of
HPS in developing effective guidance, good practice and a competent
workforce and translating knowledge to improve health outcomes.
Target audience:
All NHSScotland staff involved in patient care activities where interventions
can lead to HAI, particularly those interventions that can cause bloodstream
infections such as line insertion. Infection prevention and control teams in
NHS boards and other settings. Partner organisations particularly Healthcare
Improvement Scotland and National Education for Scotland to ensure
consistent information across similar improvement documentation.
Description:
Literature critique summary and presentation of key recommendations to
inform HAI quality improvement tools, based around a framework that
evaluates these against the health impact contribution and expert
opinion/practical application.
Update/review schedule: Every three years; however if significant new evidence or other implications
for practice are published updates will be undertaken.
Cross reference:
Standard Infection Control Precautions Policies in the National Infection
Prevention and Control Manual. Data on HAI incidence and prevalence and
process compliance data. Implementation support from Healthcare
Improvement Scotland and/or others, education and training support from
National Education Scotland.
Update level:
Practice – some change to practice, described throughout the document
particularly the key recommendations.
Procurement – any implications will be presented on a separate summary
sheet.
Research – broad recommendations are given where gaps were identified.
Health Protection Scotland v1.0. April 2012 Page 2 of 29
Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
Contents
1. Executive summary................................................................................................................................... 4 2. Aim of the review ...................................................................................................................................... 5 3. Background............................................................................................................................................... 5
3.1 The problem ................................................................................................................................... 5 3.2 Why PVCs are needed................................................................................................................... 5 3.3 How infections associated with the maintenance of PVCs can be prevented ............................... 5 3.4 Out of scope for this review............................................................................................................ 6 3.5 Assumptions – to ensure successful application of recommendations into practice..................... 6
4. Results ...................................................................................................................................................... 7 4.1 Review of evidence base ............................................................................................................... 7
4.1.1 Final recommendation - Ensure that the clinical need for the PVC is reviewed and recorded every day (on a daily basis) (Category 1A)........................................................... 7
4.1.2 Final recommendation - Ensure that timely removal of PVCs is considered i.e. if in longer than 72 hours (Category 1B) ................................................................................................ 7
4.1.3 Final recommendation - Ensure that hand hygiene is performed immediately before accessing the line/site (WHO Moment 2) (Category 1A) ..................................................... 8
4.1.4 Final recommendation - Ensure that medical staff review the need for intravenous (IV) therapy including antibiotics on a daily basis- switch to oral if possible (Category 1B) ....... 9
4.1.5 Final recommendation - Ensure that the PVC site is assessed; removing the PVC where there is phlebitis or other inflammation at the site (Category 1B) ...................................... 10
4.1.6 Final recommendation - Ensure that PVC dressings are intact (Category 1A).................. 11 4.1.7 Final recommendation - Ensure that an antiseptic containing 70% isopropyl alcohol is used
to clean the access hub before accessing – rub the access hub for at least 15 seconds (‘scrub the hub’) (Category 1B) .......................................................................................... 11 4.2 Review of additional evidence based on initial search findings ................................................... 12
4.2.1 Administration set replacement (Category 1A) .................................................................. 12 5. Implications for research......................................................................................................................... 13 6. References.............................................................................................................................................. 14 Appendix 1: Previous criteria under review ..................................................................................................... 18 Appendix 2: Framework – tool to evaluate evidence based recommendations alongside the health impact contribution and expert opinion (based on the target group covered by this review)...................................... 19 Appendix 3: Literature review methodology .................................................................................................... 26 Appendix 4: Search Strategy........................................................................................................................... 28 Appendix 5: Summary of key recommendations for PVC insertion and maintenance.................................... 29
Health Protection Scotland v1.0. April 2012 Page 3 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
1. Executive summary
Peripheral Vascular Catheters (PVCs) are the most commonly used invasive medical devices within all acute
care settings. The use of PVCs is necessary to provide vascular access for the administration of fluids and
drugs that cannot be given by any other route e.g. oral.
Despite the many advantages of their use, PVCs can result in complications. Reports indicate that often
PVCs are inserted unnecessarily, are not removed in a timely manner when inserted, and are the cause of a
number of patient complications including insertion site phlebitis and most importantly cause catheter related
blood stream infections (CRBSIs).1-5
There has been a focus on ensuring optimal care of PVCs by the use of quality improvement tools and as a
result, the PVC care bundle and associated tools were published on the Health Protection Scotland (HPS)
website in March 2008. A review of the content alongside the currently available guidelines and evidence
has now been undertaken to ensure that these key infection prevention recommendations are still the most
important for optimal maintenance of PVCs and subsequent safety of patients with PVCs.
The recommendations result from the review of scientific evidence and the process of assessing these within
a health impact and expert opinion framework. The key recommendations and their scientific grade of
evidence, for a PVC maintenance quality improvement tool now are:
• Ensure that the clinical need for the PVC is reviewed and recorded every day (on a daily basis)
(Category 1A) *
• Ensure that medical staff review the need for intravenous (IV) therapy including antibiotics on a daily
basis- switch to oral if possible (Category 1B)
• Ensure that hand hygiene is performed immediately before accessing the line/site (WHO Moment 2)
(Category 1A)
• Ensure that timely removal of PVCs is considered i.e. if in longer than 72 hours Category 1B)
• Ensure that the PVC site is assessed; removing the PVC where there is phlebitis or other inflammation
at the site (Category 1B)
• Ensure that PVC dressings are intact (Category 1A)
• Ensure that an antiseptic containing 70% isopropyl alcohol is used to clean the access hub before
accessing – rub the access hub for at least 15 seconds (‘scrub the hub’) (Category 1B)
* to find out more information on the categories of these recommendations see Appendix 3
Note: this review identifies the resulting key evidence based recommendations and does not aim to identify
all the elements of a checklist or standard operating procedure covering PVC management. A review and
recommendations on PVC insertion is available on HPS web pages. Other locally available procedures and
tools should address all steps related to PVC care.
Health Protection Scotland v1.0. April 2012 Page 4 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
In conclusion: It is now advised that the key recommendations listed as a result of this review here and
summarised in Appendix 5 are considered for application into practice as supported by quality improvement
tools including care bundles. These activities can also be supported by national patient safety /quality
improvement work (as directed by Healthcare Improvement Scotland).
2. Aim of the review To review the previous HPS PVC maintenance quality improvement tool content, alongside the currently
available guidelines and evidence to ensure that the key recommendations are still the most critical for
optimal maintenance of PVCs in patients who require these. The PVC care bundle and associated tools
were first published on the HPS website in May 2008.
3. Background
3.1 The problem
PVCs are the most commonly used invasive medical devices within all acute care settings. NHSScotland
National HAI Prevalence Survey Final Report, 2007 reported that 30% of inpatients have PVCs. Reports
indicate that often PVCs are inserted unnecessarily, are not removed in a timely manner when inserted, and
are the cause of a number of patient complications including insertion site phlebitis and most importantly
cause CRBSIs.3;5 PVCs can cause CRBSIs by enabling microorganisms to gain direct access to the blood
stream. Infections can arise from microorganisms at the insertion site through contamination of PVCs caused
by the hands of healthcare workers, the patient's own skin around the insertion site, as well as contaminated
drugs/infusions and entry ports where drugs are administered. Once microorganisms enter and settle on the
PVC surface, biofilm can form on the catheter lumen and if the catheter remains in situ long enough, parts of
the biofilm can float into the blood stream giving rise to a CRBSI, which is considered a significant morbidity
and mortality issue in NHSScotland.5
3.2 Why PVCs are needed
In reality, PVCs are designed to provide vascular access for the administration of fluids and drugs that
cannot be given by any other route, e.g. orally. Crucially, they also provide this access during actual or
potential life-threatening situations when the administration of fluids and or drugs must be immediate. In
achieving this they contribute to saving countless lives each day; they also reduce the need for more
advanced and invasive vascular access devices such as central vascular catheters.
3.3 How infections associated with the maintenance of PVCs can be prevented
Critically, for this PVC maintenance review, the main aim is to present the evidence for removing PVCs in a
timely manner to prevent infection. Other aspects considered critical for preventing infections are care of the
insertion site and any ports being accessed to administer drugs or take blood and the need for hand hygiene
at the most critical moments when accessing a PVC.
Health Protection Scotland v1.0. April 2012 Page 5 of 29
Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
This review of current scientific literature, as well as the process of scoring the resulting recommendations
using the health impact and expert opinion framework, aims to ascertain whether there is any new guidance
or evidence to inform key recommendations from HPS, including if those existing are still relevant or should
be modified to ensure optimal PVC care.
3.4 Out of scope for this review
This literature review does not address any issues specific to:
• Paediatric patients
Activities relating to other lines including:
• Central vascular catheters (CVCs)
• Peripherally inserted central catheters (PICCs)
3.5 Assumptions – to ensure successful application of recommendations into practice
There are a number of aspects related to healthcare delivery that were not within the remit of this review as it
is clear that they are the responsibility of other professionals. These include that:
• Staff are appropriately trained and competent in all aspects of the management of PVCs preferably using
an approved educational package
• The overall approach to the delivery of healthcare is supported by patient safety and improvement
approaches and organisational readiness.
Health Protection Scotland v1.0. April 2012 Page 6 of 29
Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
4. Results
The recommendations presented are based on a review of the current evidence. The previous
recommended criteria within the HPS bundles and checklists were used as a basis for the question set in
Appendix 1. To further aid the process of deciding what final key recommendations to be included, all the
recommendations resulting from the review of the evidence were assessed using the ‘health impact and
expert opinion framework’ seen in Appendix 2. The final key recommendations were identified as a result of
this evaluation as well as being informed by the process of wider consultation.
The methodology for this is described within Appendix 3; the specific search strategy in Appendix 4 and
finally a summary page of the resulting recommendations can be found in Appendix 5.
4.1 Review of evidence base
4.1.1 Final recommendation - Ensure that the clinical need for the PVC is reviewed and recorded every day (on a daily basis) (Category 1A)
This recommendation is based on reports that often PVCs are inserted unnecessarily and evidence that the
longer the catheter is in place the greater the risk of complications such as phlebitis and infection.1-4;6;7 It is
therefore vital that there is clinical indication that PVCs are still required otherwise they should be removed.
The Center for Disease Control (CDC) guidelines do not specifically mention this however there is a
recommendation that staff should be educated on the indications for intravascular catheter use.8 The
Department of Health (DH) high impact intervention however recommends that the continuing clinical
indication for intravascular catheters is assessed twice daily and catheters are removed where no longer
indicated. Although the DH high impact intervention gives clear instruction about how often PVCs should be
assessed, there is no direct supporting evidence reported for the necessity of twice daily checking of clinical
requirement for ongoing PVC use.9 In addition it may also be practically difficult to ensure and record
compliance of twice daily checking. The effect of including this action, in line with the DH high impact
intervention, would therefore need to be considered with respect to whether it would improve
compliance/safety and reduce the risk of infection for the patient. The recommendation given results from all
evidence considerations and after applying the framework described in Appendix 2.
4.1.2 Final recommendation - Ensure that timely removal of PVCs is considered i.e. if in longer than 72 hours (Category 1B)
The HPS PVC maintenance quality improvement tool currently recommends that consideration should be
given to removal of PVCs in situ longer than 72 hours. This was based on evidence which showed that the
longer a PVC is in situ the greater the risk of complication.4;11-13 A recent study examined the effect of
increasing the routine replacement from 48-72 hours to 72-96 hours, and although it concluded that this
extension was not a risk factor for complication, e.g. phlebitis or infection, it was noted that the absence of a
dedicated intravenous (IV) team was a risk.14 Further uncertainties have arisen resulting from a recent
debate regarding the routine removal of PVCs after 72 or 96 hours versus removal only when clinically
indicated.15;16 A Cochrane review has been published which concluded that there was insufficient evidence
Health Protection Scotland v1.0. April 2012 Page 7 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
of benefit from routinely removing catheters every 72 to 96 hours and suggested that catheters including
PVCs, should be changed on clinical indication.17 Conversely, the recently updated CDC guidelines, states
that replacement of PVCs in adults as clinically indicated is as an unresolved issue and cites insufficient
current evidence specifically on CRBSIs to recommend this.8
Due to the ambiguous nature of these recommendations, the evidence which underpins the Cochrane review
was further reviewed and critically appraised to determine if it could impact on this key recommendation.
Further examination of the evidence underpinning the recommendations that PVCs should be changed when
clinically indicated1;7;15;18;19 reveals that it stems largely from studies carried out in Australia and the majority
used a dedicated intravenous (IV) team in their studies, which are rare within NHSScotland.16;18;19
The main outcome evaluated within all the studies included was phlebitis, and although CRBSI was
measured in five studies, there were only 11 cases in total described in both the intervention and non
intervention groups. Despite the reasonably high number of PVCs (~2000) included within the studies in the
Cochrane review, it may not currently provide sufficient evidence that moving from away from routine to
clinical indication replacement of PVCs would not result in increased CRBSIs. As PVCs are the most
commonly used invasive medical devices within all acute care settings this therefore needs to be taken into
account when interpreting these data/studies.5
The nature of the inclusion and exclusion criteria for Cochrane reviews means that only evidence considered
high quality, e.g. randomised control trials (RCTs) are included in the assessment of evidence. While the
results of RCTs when available in this field are valuable, there are some limitations and challenges that
result from taking this approach to the review of literature and assessment of evidence, particularly within the
field of infection prevention and control as it can cause some difficulties in assessing the effect of
interventions when examined within the wider clinical context. Although interventions have been well
described, they are often within a structured, formal study. In this situation, much of the evidence included
results from studies where a dedicated intravenous (IV) team trained in recognition of clinical complications
of PVC use, were present. NHSScotland quality improvement tools however are designed to be used in
clinical settings, which are unlikely to have such specialist staff. In addition, much of the existing evidence for
infections associated with PVC use results from outbreak reports and observational studies. This evidence is
considered as low quality customarily within the field of evidence based methodology, however in order to
form a sound recommendation for practice, the ‘body of evidence’ resulting from these studies needs to be
considered alongside the RCTs to ensure there is a full clinical context of the effect of the suggested
interventions. Any key recommendations need to be cognisant of this overall clinical context. It is possible
therefore that a change in the recommendation may result in less active monitoring/care of the PVC, which
would not be desirable. The recommendation given results from all evidence considerations and after
applying the framework described in Appendix 2.
4.1.3 Final recommendation - Ensure that hand hygiene is performed immediately before accessing the line/site (WHO Moment 2) (Category 1A)
This recommendation, and the importance of hand hygiene performance, is consistent with all current
evidence and guidelines. The WHO Guidelines on Hand Hygiene in Health Care (2009)10 clearly describe
Health Protection Scotland v1.0. April 2012 Page 8 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
the indications for hand hygiene and present these within the WHO ‘My 5 Moments for Hand Hygiene’
approach, including emphasising the importance of performing hand hygiene before clean/aseptic
procedures to prevent HAI. These 5 Moments have been widely promoted within NHSScotland for a number
of years and hand hygiene performance is measured against these Moments. This recommendation now
provides two opportunities; to emphasise the hand hygiene moment when risk is highest in relation to PVC
maintenance care/acquisition of infection, rather than attempting to use a resulting quality improvement tool
as a means of general hand hygiene promotion, and to allow for monitoring of hand hygiene practices to be
consistent across all hand hygiene auditing and quality improvement tool monitoring as is currently taking
place in NHSScotland.
Accessing the site has been emphasised as a key factor in acquiring infection and therefore this moment is
crucial to protect the patient at a vulnerable time.8;9
In summary, in relation to the risk associated with PVC maintenance, the clearest indication for hand hygiene
is Moment 2 ‘before clean/aseptic procedures’ and therefore is considered an essential step in preventing
PVC related infections in NHSScotland. The recommendation given results from all evidence considerations
and after applying the framework described in Appendix 2.
4.1.4 Final recommendation - Ensure that medical staff review the need for intravenous (IV) therapy including antibiotics on a daily basis- switch to oral if possible (Category 1B)
PVCs are commonly inserted for antibiotic therapy in acute admissions.20 The median duration of
intravenous (IV) therapy has been shown to be four days in one study.21 The results of the 2009 European
Surveillance of Antimicrobial Consumption (ESAC) survey of hospitals showed that out of a total of 8,732
patients surveyed 2,425 (27.8%, hospital range 5.6%-47.1%) were prescribed 3,511 antimicrobials. Of the
total number of antimicrobials prescribed 50.5% (hospital range 0% - 85.7%) were given by the parenteral
route.22 The majority are given through PVCs, and some occasionally through Central Vascular Catheters
(CVCs).
Antibiotic review is a key component of hospital antimicrobial stewardship programmes. The clinical and cost
effectiveness of stewardship programmes as part of overall HAI reduction strategies is well documented.23-26
A clear example of this is the impact of improved compliance with the choice of empiric treatment in Scotland
on Clostridium difficile infection (CDI) rates.27
‘Continuing care’ prescribing is now being addressed following progress on ‘front end’ hospital prescribing.
There has been an association between the long duration of PVCs and the development of CRBSIs
including Staphylococcus aureus bacteraemia (SABs), which remains a source of concern. In addition, there
is evidence to indicate that the quality of prescribing in continuing care is also an area of concern with a
practice of inadequate review of the antibiotic indication/need, route, duration and supporting microbiology.28
This could undoubtedly contribute to CDI, antibiotic resistance, line related infections and their complications.
Health Protection Scotland v1.0. April 2012 Page 9 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
There is therefore a clear need for a more robust method to support antibiotic review in the workplace. This
review is ideally timed between 48-92 hours post admission to hospital, when the patient’s clinical
progress/stability and prognosis is more certain, and there is more laboratory and imaging information
available to allow an informed adjustment to the treatment.
This would also fit into the time frame for considering the removal of PVCs in situ longer than 72 hours (a
recommendation of the PVC quality improvement tool).
The evidence base to support this antibiotic review intervention has been appraised.28-33 Existing evidence is
not based on randomised control trials (RCTs) but is primarily experiential and often in the form of quality
improvement tests, is biologically plausible, and has some consistency of association and some evidence to
support that the proposed changes influences outcomes. All of these are core components of Bradford Hill’s
criteria for examining cause and effect when reviewing evidence for the effectiveness of interventions.34
At a meeting of the Scottish Antimicrobial Management Team [AMT] Network 1st March 2011 Edinburgh,
with infection prevention nurses and hosted by the Scottish Antimicrobial Prescribing Group (SAPG), one of
the key learning points from a workshop was where the PVC quality improvement tool could incorporate
components of intravenous antibiotic review. This would also provide opportunity for team-working between
antimicrobial prescribing teams, infection control teams and attending clinical teams. The benefits would
include not only addressing the need for a PVC but a potential reduction in nursing time in administering
intravenous therapy, facilitating a clinically sound decision to move to oral therapy or discontinuing.
Therefore the combination of the requirement to review the need for a PVC and intravenous therapy
represents the Scottish infection community with a golden opportunity for implementing combined infection
prevention actions and optimising management of care in the patient’s journey. The recommendation given
results from all evidence considerations and after applying the framework described in Appendix 2.
For note: The antibiotic review should include the following components: review of the indication for the
antibiotic, review of the patient’s clinical progress and original indication for the antibiotic, review of the
microbiology so that the antibiotic choice can be further streamlined and the review of the need for further IV
therapy and duration of treatment/antibiotic stop date.35
4.1.5 Final recommendation - Ensure that the PVC site is assessed; removing the PVC where there is phlebitis or other inflammation at the site (Category 1B)
There is substantial evidence to support the removal of PVCs if clinically indicated e.g. signs of
complications such as phlebitis, infection or if the catheter is blocked, with the aim of preventing further
complications/infection.8;13;36 The DH high impact intervention9 however does not specifically include this as a
key action, but does recommend site inspection, which is a documented review of the catheter site for signs
of infection at least daily e.g. using visual infusion phlebitis (VIP) score tool. The CDC guidelines state
‘Remove peripheral vascular catheters if the patient develops signs of phlebitis (warmth, tenderness,
erythema or palpable vascular cord), infection or a malfunctioning catheter.’8 This evidence based
recommendation is therefore very clearly described in relation to potential for harm and consistent with
current quality improvement tools recommendations. The recommendation given results from all evidence
considerations and after applying the framework described in Appendix 2.
Health Protection Scotland v1.0. April 2012 Page 10 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
4.1.6 Final recommendation - Ensure that PVC dressings are intact (Category 1A)
The DH high impact intervention includes a care action, which is ‘a sterile, semi permeable, transparent
dressing is used therefore allowing observation of insertion site.’9 Although the use of a transparent dressing
is recommended and there is no supporting evidence provided or reported, it is clear however it is a practical
consideration to enable easy visualisation of the PVC site. The CDC guidelines report that the rates of
colonisation and occurrence of phlebitis from catheters dressed with either gauze or semi-permeable
transparent dressings are comparable.8 It has been concluded that the choice of dressing is based on
preference or factors like the presence of blood oozing from the catheter site, as well as visualisation.37 It is
therefore recommended that either sterile gauze or transparent, semi-permeable dressings are used to cover
the catheter site, while assessment of the PVC site occurs daily by palpation through the dressing or
inspection if the dressing is transparent. If the dressings are not intact or have become loosened this
increases the risk of microorganisms gaining entry via the PVC. Therefore dressings should always be
replaced if damp, loosened or visibly soiled.8 The recommendation given results from all evidence
considerations and after applying the framework described in Appendix 2.
4.1.7 Final recommendation - Ensure that an antiseptic containing 70% isopropyl alcohol is used to clean the access hub before accessing – rub the access hub for at least 15 seconds (‘scrub the hub’) (Category 1B)
It has been previously reported that hubs and connection points are generally contaminated and must be
disinfected before being accessed by healthcare workers (HCWs).13;36;37
On a separate issue, needleless ports were originally introduced to reduce the risk to staff from needlestick
injuries.38 Subsequent developments in this technology have resulted in numerous different connectors
which include split-septum devices, mechanical valve devices and mechanical valve devices with positive
fluid displacement. Since their introduction unfortunately there have been a number of reports of increased
CRBSIs.39-41
There has subsequently been a focus on the importance of adequate and thorough decontamination of
access hubs and connection points and specifically these needleless ports. The DH high impact intervention9
currently includes a care action which states that 2% chlorhexidine in 70% isopropyl alcohol should be used
to decontaminate the port and surrounding area and allowed to dry prior to access. The CDC guidance
however recommends that access ports should be ‘scrubbed’ with the appropriate antiseptic (chlorhexidine,
or 70% isopropyl alcohol).8 The evidence for the use of 2% chlorhexidine gluconate in 70% isopropyl alcohol
is extrapolated mainly from studies on CVCs where catheters are left in situ long term.36 There is little
specific evidence on effective decontamination and disinfection of hubs in PVC use. There is however some
debate on whether it is the design of the hubs/ ports or the method of cleaning itself which is important in the
effective decontamination.42 Two recent microbiological studies which examined decontamination of different
designs of access hubs showed that 15 seconds of a scrubbing action with 70% isopropyl alcohol was as
effective as 2% chlorhexidine in 70% isopropyl alcohol. Although these studies are relatively small scale,
they have provided further evidence that it is the method of action of cleaning the hubs which is important
rather than the use of a specific disinfectant, e.g. chlorhexidine, in this regard. This is of particular
Health Protection Scotland v1.0. April 2012 Page 11 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
importance when considering the different designs of the needleless port components.43;44 It is therefore
concluded, based on a review of the evidence, that this is a key recommendation consistent with the CDC
guidelines to ‘scrub the hub’ with 70% isopropyl alcohol.8 It could also be argued that the use of such a
recommendation will perhaps encourage staff to remember, aiding compliance with port access care and
therefore is consistent with the overall ethos of quality improvement tools and ensuring reliable good
practice. In summary, this is a microbiologically driven recommendation, given the evidence with regards to
known contamination and effectiveness of cleansing, as well as the obvious potential for PVC connectors to
become easily contaminated and pose a risk of infection on a day to day basis. The recommendation given
results from all evidence considerations and after applying the framework described in Appendix 2.
4.2 Review of additional evidence based on initial search findings
4.2.1 Administration set replacement (Category 1A)
The Department of Health (DH) high impact intervention recommends replacement immediately after
administration of blood, blood products and all other fluid sets after 72 hours.9 The Center for Disease
Control (CDC) guidelines recommend that administration sets which are continuously used, including
secondary sets and add on devices, are changed no more frequently than at 96 hour intervals but at least
every 7 days8 (and immediately after blood, blood products or lipid). This is consistent with a Cochrane
Review.45 Despite the availability of evidence on the timing of administration set replacement, it is clear that
there is not one single recommendation that can be incorporated in a quality improvement tool, but rather a
list of instructions would need to be incorporated within procedures to ensure clear guidance for practice.
The inclusion of this recommendation was considered within the context of the overall aims of NHSScotland
quality improvement tools and it was concluded that this would not fit as it is a description of a procedure
rather than one single recommendation. Changing administration sets should therefore be considered
separately to avoid confusion in practice with regards to the critical elements for preventing PVC infections
and CRBSI. It is concluded that specific information regarding the timing of administration set replacement
will be included within other supporting tools or advice e.g. cause and effect chart.
In conclusion: It is now advised that the key recommendations listed as a result of this review here and
summarised in Appendix 5 are considered for application into practice as supported by quality improvement
tools including care bundles. These activities can also be supported by national patient safety /quality
improvement work (as directed by Healthcare Improvement Scotland).
Health Protection Scotland v1.0. April 2012 Page 12 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
5. Implications for research
There is still ambiguity around some of the key recommendations regarding whether removing PVCs on
clinical indication should be advocated after a period of 72 hours. Despite the existence of a relatively
substantial quantity of data on complications there is not sufficient data on the effect on bloodstream
infections. Therefore research which focuses on the outcome of CRBSIs rather than other complications
would provide necessary evidence to strengthen key recommendations as a result.
The recommendation to ‘scrub the hub’ is based on a combination of small scale epidemiological and
microbiological studies alongside some practical considerations regarding the design of the connectors.
Further studies which examine the evidence in some more detail regarding duration of the contact with the
antiseptic and the action of the scrubbing would be beneficial. There is a potential for a research study to be
established which would examine the effect of the introduction of this intervention and data be evaluated as
evidence.
• Focus on CRBSIs data with respect to removal of PVCs after 72 hours versus on clinical indication.
• Further research on decontamination of PVC hubs/connectors with respect to outcome on CRBSIs data.
Health Protection Scotland v1.0. April 2012 Page 13 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
6. References
(1) Lee WL, Chen HL, Tsai TY, Lai IC, Chang WC, Huang CH, et al. Risk factors for peripheral intravenous catheter infection in hospitalized patients: a prospective study of 3165 patients. American Journal of Infection Control 2009 Oct;37(8):683-6.
(2) Lee WL, Liao SF, Lee WC, Huang CH, Fang CT. Soft tissue infections related to peripheral intravenous catheters in hospitalised patients: a case-control study. J Hosp Infect 2010 Oct;76(2):124-9.
(3) Reilly J, Stewart S, Allardice GA, Noone A, Robertson C, Walker A, et al. Results from the Scottish National HAI Prevalence Survey. J Hosp Infect 2008 May;69(1):62-8.
(4) Thomas A, Hayes P, Lockie T, Harrington D. Venflons: why can't we resist putting them in? J Hosp Infect 2006 May;63(1):108-9.
(5) Zingg W, Pittet D. Peripheral venous catheters: an under-evaluated problem. Int J Antimicrob Agents 2009;34 Suppl 4:S38-S42.
(6) Webster J, Osborne S. Phlebitis associated with peripheral intravenous catheters. American Journal of Infection Control 2007 May;35(4):287-8.
(7) Webster J, Osborne S. Phlebitis rate unacceptable. Singapore Medical Journal 2009 Jan;50(1):109.
(8) O'Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, et al. Guidelines for the prevention of intravascular catheter-related infections. Am J Infect Control 2011 May;39(4 Suppl 1):S1-34.
(9) High Impact Intervention: Peripheral Intravenous cannula care bundle. Department of Health 2011 [cited 2012 Mar 30];Available from: URL: http://hcai.dh.gov.uk/whatdoido/high-impact-interventions/
(10) World Health Organization. WHO guidelines on hand hygiene in health care: first global patient safety challenge clean care is safer care. Geneva: WHO; 2009.
(11) Curran ET, Coia JE, Gilmour H, McNamee S, Hood J. Multi-centre research surveillance project to reduce infections/phlebitis associated with peripheral vascular catheters. J Hosp Infect 2000 Nov;46(3):194-202.
(12) Goddard L, Clayton S, Peto TE, Bowler IC. The 'just-in-case venflon': effect of surveillance and feedback on prevalence of peripherally inserted intravascular devices. Journal of Hospital Infection 2006 Dec;64(4):401-2.
(13) Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med 2000 Mar 7;132(5):391-402.
(14) Lai KK. Safety of prolonging peripheral cannula and i.v. tubing use from 72 hours to 96 hours. Am J Infect Control 1998 Feb;26(1):66-70.
(15) Van DP, Rickard CM, McGrail MR, Doolan G. Routine replacement versus clinical monitoring of peripheral intravenous catheters in a regional hospital in the home program: A randomized controlled trial. Infection Control & Hospital Epidemiology 2009 Sep;30(9):915-7.
(16) Webster J, Clarke S, Paterson D, Hutton A, van DS, Gale C, et al. Routine care of peripheral intravenous catheters versus clinically indicated replacement: randomised controlled trial. BMJ 2008;337:a339.
(17) Webster J, Osborne S, Rickard C, Hall J. Clinically-indicated replacement versus routine replacement of peripheral venous catheters. Cochrane Database Syst Rev 2010;(3):CD007798.
Health Protection Scotland v1.0. April 2012 Page 14 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
(18) Rickard CM, McCann D, Munnings J, McGrail MR. Routine resite of peripheral intravenous devices every 3 days did not reduce complications compared with clinically indicated resite: a randomised controlled trial. BMC Medicine 2010;8:53.
(19) Webster J, Lloyd S, Hopkins T, Osborne S, Yaxley M. Developing a Research base for Intravenous Peripheral cannula re-sites (DRIP trial). A randomised controlled trial of hospital in-patients. Int J Nurs Stud 2007 Jul;44(5):664-71.
(20) Barlow G, Palniappan S, Mukherjee R, Jones M, Nathwani D. Unnecessary peripheral intravenous catheterisation on an acute medical admissions unit: a preliminary study. Eur J Intern Med 2002 Sep;13(6):380.
(21) Seaton RA, Nathwani D, Burton P, McLaughlin C, MacKenzie AR, Dundas S, et al. Point prevalence survey of antibiotic use in Scottish hospitals utilising the Glasgow Antimicrobial Audit Tool (GAAT). Int J Antimicrob Agents 2007 Jun;29(6):693-9.
(22) European Surveillance of Antimicrobial Consumption Point Prevalence Survey 2009 Scottish Hospitals Report. Scottish Antimicrobial Prescribing Group 2010 [cited 2012 Mar 13];Available from: URL: http://www.scottishmedicines.org.uk/files/ESAC_report_final_060510.pdf
(23) Nathwani D. Antimicrobial prescribing policy and practice in Scotland: recommendations for good antimicrobial practice in acute hospitals. J Antimicrob Chemother 2006 Jun;57(6):1189-96.
(24) Valiquette L, Cossette B, Garant MP, Diab H, Pepin J. Impact of a reduction in the use of high-risk antibiotics on the course of an epidemic of Clostridium difficile-associated disease caused by the hypervirulent NAP1/027 strain. Clin Infect Dis 2007 Sep 1;45 Suppl 2:S112-S121.
(25) Conlon G, Aldeyab MA, McElnay JC, Scott MG, Magee FA, Davies E, et al. Improving and maintaining adherence with hospital antibiotic policies: a strategy for success. J Hosp Infect 2011 Jan;77(1):88-9.
(26) Aldeyab MA, McElnay JC, Scott MG, Davies E, Edwards C, Darwish Elhajji FW, et al. An evaluation of the impact of a single-dose intravenous immunoglobulin regimen in the treatment of Clostridium difficile infections. Infect Control Hosp Epidemiol 2011 Jun;32(6):631-3.
(27) Scottish Antimicrobial Prescribing Group Progress Report for 2008-2011. NHS Quality Improvement Scotland 2011 [cited 2012 Mar 13];Available from: URL: http://www.scottishmedicines.org.uk/files/sapg/SAPG_Progress_Report_2008-11.pdf
(28) Cooke FJ, Matar R, Lawson W, Aliyu SH, Holmes A. Comment on: Antibiotic stewardship--more education and regulation not more availability? J Antimicrob Chemother 2010 Mar;65(3):598.
(29) Cooke FJ, Holmes AH. The missing care bundle: antibiotic prescribing in hospitals. Int J Antimicrob Agents 2007 Jul;30(1):25-9.
(30) Marwick C, Davey P. Care bundles: the holy grail of infectious risk management in hospital? Curr Opin Infect Dis 2009 Aug;22(4):364-9.
(31) Nathwani D et al. Antibiotic Review Bundle. NHS Tayside Report to the Health Foundation Research and Innovation Group, 2010. 2010.
(32) Pulcini C, Defres S, Aggarwal I, Nathwani D, Davey P. Design of a 'day 3 bundle' to improve the reassessment of inpatient empirical antibiotic prescriptions. J Antimicrob Chemother 2008 Jun;61(6):1384-8.
(33) Toth NR, Chambers RM, Davis SL. Implementation of a care bundle for antimicrobial stewardship. Am J Health Syst Pharm 2010 May 1;67(9):746-9.
Health Protection Scotland v1.0. April 2012 Page 15 of 29
Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
(34) Ward AC. The role of causal criteria in causal inferences: Bradford Hill's "aspects of association". Epidemiol Perspect Innov 2009;6:2.
(35) Davey P, Brown E, Fenelon L, Finch R, Gould I, Hartman G, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev 2005;(4):CD003543.
(36) Pratt RJ, Pellowe CM, Wilson JA, Loveday HP, Harper PJ, Jones SR, et al. epic2: National evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect 2007 Feb;65 Suppl 1:S1-64.
(37) O'Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, et al. Guidelines for the Prevention of Intravascular Catheter-related Infections. Clin Infect Dis 2011 Apr 1.
(38) Chittick P, Sherertz RJ. Recognition and prevention of nosocomial vascular device and related bloodstream infections in the intensive care unit. [Review] [132 refs]. Critical Care Medicine 2010 Aug;38(8:Suppl):Suppl-72.
(39) Field K, McFarlane C, Cheng AC, Hughes AJ, Jacobs E, Styles K, et al. Incidence of catheter-related bloodstream infection among patients with a needleless, mechanical valve-based intravenous connector in an Australian hematology-oncology unit. Infect Control Hosp Epidemiol 2007 May;28(5):610-3.
(40) Rupp ME, Sholtz LA, Jourdan DR, Marion ND, Tyner LK, Fey PD, et al. Outbreak of bloodstream infection temporally associated with the use of an intravascular needleless valve. Clinical Infectious Diseases 2007 Jun 1;44(11):1408-14.
(41) Salgado CD, Chinnes L, Paczesny TH, Cantey JR. Increased rate of catheter-related bloodstream infection associated with use of a needleless mechanical valve device at a long-term acute care hospital. Infect Control Hosp Epidemiol 2007 Jun;28(6):684-8.
(42) Kaler W. CR. Successful disinfection of needleless access ports: A matter of time and friction. Journal of the Association for Vascular Access 2007;12(3):140-2.
(43) Kaler W. CR. Successful disinfection of needleless access ports: A matter of time and friction. Journal of the Association for Vascular Access 2007;12(3):140-2.
(44) Simmons S, Bryson C, Porter S. "Scrub the hub": cleaning duration and reduction in bacterial load on central venous catheters. Critical Care Nursing Quarterly 2011 Jan;34(1):31-5.
(45) Gillies D, O'Riordan L, Wallen M, Morrison A, Rankin K, Nagy S. Optimal timing for intravenous administration set replacement. Cochrane Database Syst Rev 2005;(4):CD003588.
(46) The AGREE Collaboration. Appraisal of Guidelines For Research & Evaluation (AGREE) Instrument. 2001.
(47) Umscheid CA, Agarwal RK, Brennan PJ. Updating the guideline development methodology of the Healthcare Infection Control Practices Advisory Committee (HICPAC). Am J Infect Control 2010 May;38(4):264-73.
(48) Berenholtz S, Pronovost PJ. Barriers to translating evidence into practice. Curr Opin Crit Care 2003 Aug;9(4):321-5.
(49) Gurses AP, Murphy DJ, Martinez EA, Berenholtz SM, Pronovost PJ. A practical tool to identify and eliminate barriers to compliance with evidence-based guidelines. Jt Comm J Qual Patient Saf 2009 Oct;35(10):526-32, 485.
(50) O'Connor PJ. Adding value to evidence-based clinical guidelines. JAMA 2005 Aug 10;294(6):741-3.
Health Protection Scotland v1.0. April 2012 Page 16 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
(51) Sawyer M, Weeks K, Goeschel CA, Thompson DA, Berenholtz SM, Marsteller JA, et al. Using evidence, rigorous measurement, and collaboration to eliminate central catheter-associated bloodstream infections. Crit Care Med 2010 Aug;38(8 Suppl):S292-S298.
(52) Sax H, Allegranzi B, Uckay I, Larson E, Boyce J, Pittet D. 'My five moments for hand hygiene': a user-centred design approach to understand, train, monitor and report hand hygiene. J Hosp Infect 2007 Sep;67(1):9-21.
(53) IHI, Institute of Healthcare Improvement. Institute of Healthcare Improvement 2011 [cited 2012 Mar 30];Available from: URL: www.ihi.org
(54) Weiser TG, Haynes AB, Lashoher A, Dziekan G, Boorman DJ, Berry WR, et al. Perspectives in quality: designing the WHO Surgical Safety Checklist. Int J Qual Health Care 2010 Oct;22(5):365-70.
Note: A number of references listed above are cited within the literature review methodology which has been
placed in Appendix 3 for ease of reading of this document.
Health Protection Scotland v1.0. April 2012 Page 17 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
Appendix 1: Previous criteria under review
The PVC care bundle and associated tools were first published on the HPS website in May 2008.
The criteria below were used as the question set to frame this review of the evidence base
• Checking that the PVCs in situ are still required
• Removing the PVCs where there is extravasation or inflammation
• Checking that the PVC dressings are intact
• Considering removal of PVCs in situ longer than 72 hours
• Performing hand hygiene before and after all PVC procedures
Health Protection Scotland v1.0. April 2012 Page 18 of 29
Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
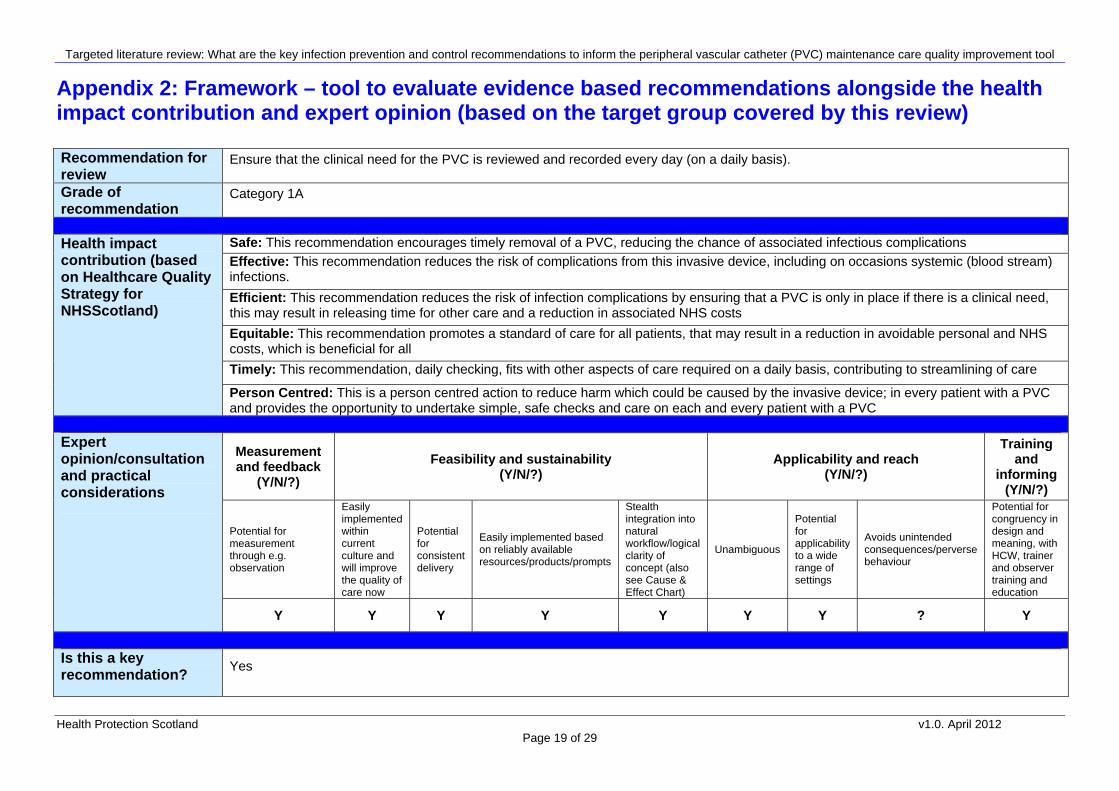
Appendix 2: Framework – tool to evaluate evidence based recommendations alongside the health impact contribution and expert opinion (based on the target group covered by this review)
Recommendation for review
Ensure that the clinical need for the PVC is reviewed and recorded every day (on a daily basis).
Grade of recommendation
Category 1A
Safe: This recommendation encourages timely removal of a PVC, reducing the chance of associated infectious complications Effective: This recommendation reduces the risk of complications from this invasive device, including on occasions systemic (blood stream) infections.
Efficient: This recommendation reduces the risk of infection complications by ensuring that a PVC is only in place if there is a clinical need, this may result in releasing time for other care and a reduction in associated NHS costs
Equitable: This recommendation promotes a standard of care for all patients, that may result in a reduction in avoidable personal and NHS costs, which is beneficial for all
Timely: This recommendation, daily checking, fits with other aspects of care required on a daily basis, contributing to streamlining of care
Health impact contribution (based on Healthcare Quality Strategy for NHSScotland)
Person Centred: This is a person centred action to reduce harm which could be caused by the invasive device; in every patient with a PVC and provides the opportunity to undertake simple, safe checks and care on each and every patient with a PVC
Measurement and feedback
(Y/N/?) Feasibility and sustainability
(Y/N/?) Applicability and reach
(Y/N/?)
Training and
informing (Y/N/?)
Potential for measurement through e.g. observation
Easily implemented within current culture and will improve the quality of care now
Potential for consistent delivery
Easily implemented based on reliably available resources/products/prompts
Stealth integration into natural workflow/logical clarity of concept (also see Cause & Effect Chart)
Unambiguous
Potential for applicability to a wide range of settings
Avoids unintended consequences/perverse behaviour
Potential for congruency in design and meaning, with HCW, trainer and observer training and education
Expert opinion/consultation and practical considerations
Y Y Y Y Y Y Y ? Y
Is this a key recommendation? Yes
Health Protection Scotland v1.0. April 2012 Page 19 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
Recommendation for review Ensure that medical staff review the need for intravenous (IV) therapy including antibiotics on a daily basis; switch to oral if possible
Grade of recommendation (based on review of evidence)
Category 1B
Safe: This recommendation encourages timely removal of a PVC, reducing the chance of associated infectious complications
Effective: This recommendation reduces the risk of complications from this invasive device, including on occasions systemic (blood stream) infections. Efficient: This recommendation reduces the risk of infectious complications by ensuring that a PVC is only in place if there is a clinical need, this will result in releasing time for other care and a reduction in associated NHS costs. Antibiotic review is a key component of hospital antimicrobial stewardship programmes as part of overall HAI reduction strategies and this recommendation helps streamlining of care Equitable: This recommendation promotes a standard of care for all patients, that may result in a reduction in avoidable personal and NHS costs, which is beneficial for all Timely: This recommendation, daily checking, fits with other aspects of care required on a daily basis, contributing to streamlining of care. This recommendation combines both infection prevention and control strategies with patient and clinical management and will fit well into the patient care routine and should aid efficient use of time
Health impact contribution (based on Healthcare Quality Strategy for NHSScotland)
Person Centred: This is a person centred action to reduce harm which could be caused by the invasive device; in every patient with a PVC and provides the opportunity to undertake simple, safe checks and care on each and every patient with a PVC
Measurement and feedback
(Y/N/?) Feasibility and sustainability
(Y/N/?) Applicability and reach
(Y/N/?)
Training and
informing (Y/N/?)
Potential for measurement through e.g. observation
Easily implemented within current culture and will improve the quality of care now
Potential for consistent delivery
Easily implemented based on reliably available resources/products/prompts
Stealth integration into natural workflow/logical clarity of concept (also see Cause & Effect Chart)
Unambiguous
Potential for applicability to a wide range of settings
Avoids unintended consequences/perverse behaviour
Potential for congruency in design and meaning, with HCW, trainer and observer training and education
Expert opinion/consultation and practical considerations
Y Y Y Y Y ? Y ? Y
Is this a key recommendation? Yes
Health Protection Scotland v1.0. April 2012 Page 20 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
Recommendation for review Ensure that hand hygiene is performed immediately before accessing the line/site (WHO Moment 2).
Grade of recommendation (based on review of evidence)
Category 1A
Safe: Not implementing this recommendation would put the patient at risk of harm
Effective: This recommendation has been shown to be effective in reducing the risk of complications resulting from contaminated hands of healthcare workers. This includes contamination of the insertion/access site which enables access to the patient’s blood stream which can result in systemic blood stream infections. Efficient: This recommendation reduces the risk of infectious complications and may result in releasing time for other care in a reduction in associated NHS costs
Equitable: This recommendation promotes a standard of care for all patients that may result in a reduction in avoidable personal and NHS costs, which is also beneficial to all Timely: This recommendation should be an integral part of healthcare worker activity and patient/ individual care
Health impact contribution (based on Healthcare Quality Strategy for NHSScotland)
Person Centred: This is a patient centred action to reduce harm caused by the invasive device in every patient with a PVC. It also provides the opportunity to undertake simple, safe checks and care on each and every patient with a PVC and allows for patients/individuals to be aware of the importance of hand hygiene and their role in this
Measurement and feedback
(Y/N/?) Feasibility and sustainability
(Y/N/?) Applicability and reach
(Y/N/?)
Training and
informing (Y/N/?)
Potential for measurement through e.g. observation
Easily implemented within current culture and will improve the quality of care now
Potential for consistent delivery
Easily implemented based on reliably available resources/products/prompts
Stealth integration into natural workflow/logical clarity of concept (also see Cause & Effect Chart)
Unambiguous
Potential for applicability to a wide range of settings
Avoids unintended consequences/perverse behaviour
Potential for congruency in design and meaning, with HCW, trainer and observer training and education
Expert opinion/consultation and practical considerations
Y Y Y Y Y ? Y Y Y
Is this a key recommendation? Yes
Health Protection Scotland v1.0. April 2012 Page 21 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
Recommendation for review Ensure that timely removal of PVCs is considered i.e. if in longer than 72 hours
Grade of recommendation (based on review of evidence)
Category 1B
Safe: This recommendation encourages timely removal of a PVC, reducing the chance of associated infectious complications Effective: This recommendation reduces the risk of complications from this invasive device, including on occasions systemic (blood stream) infections. Efficient: This recommendation reduces the risk of infectious complications by ensuring that a PVC is only in place if there is a clinical need, this may result in releasing time for other care and a reduction in associated NHS costs Equitable: This recommendation promotes a standard of care for all patients, that may result in a reduction in avoidable personal and NHS costs, which is beneficial for all Timely: This recommendation, daily checking, fits with other aspects of care required on a daily basis, contributing to streamlining of care This recommendation also combines both infection prevention and control strategies with patient and clinical management
Health impact contribution (based on Healthcare Quality Strategy for NHSScotland)
Person Centred: This is a person centred action to reduce harm which could be caused by the invasive device; in every patient with a PVC and provides the opportunity to undertake simple, safe checks and care on each and every patient with a PVC
Measurement and feedback
(Y/N/?) Feasibility and sustainability
(Y/N/?) Applicability and reach
(Y/N/?)
Training and
informing (Y/N/?)
Potential for measurement through e.g. observation
Easily implemented within current culture and will improve the quality of care now
Potential for consistent delivery
Easily implemented based on reliably available resources/products/prompts
Stealth integration into natural workflow/logical clarity of concept (also see Cause & Effect Chart)
Unambiguous
Potential for applicability to a wide range of settings
Avoids unintended consequences/perverse behaviour
Potential for congruency in design and meaning, with HCW, trainer and observer training and education
Expert opinion/consultation and practical considerations
Y ? Y Y Y ? Y ? Y
Is this a key recommendation? Yes
Health Protection Scotland v1.0. April 2012 Page 22 of 29
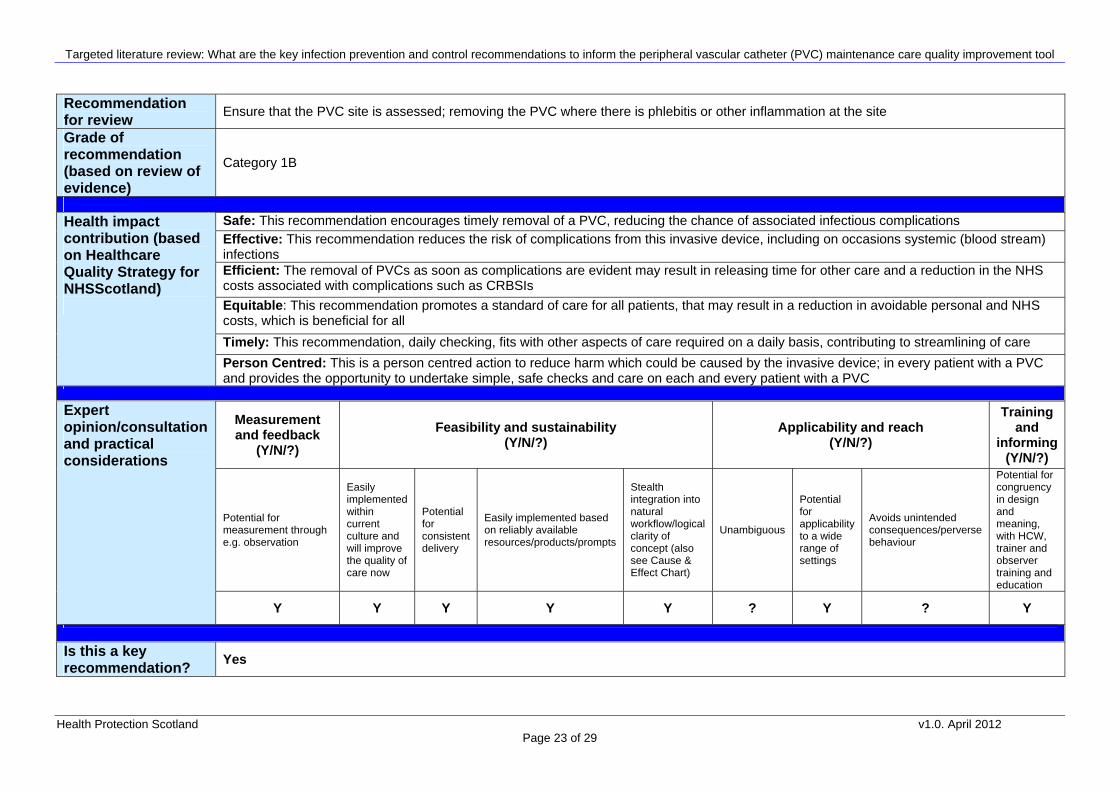
Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
Recommendation for review Ensure that the PVC site is assessed; removing the PVC where there is phlebitis or other inflammation at the site
Grade of recommendation (based on review of evidence)
Category 1B
Safe: This recommendation encourages timely removal of a PVC, reducing the chance of associated infectious complications Effective: This recommendation reduces the risk of complications from this invasive device, including on occasions systemic (blood stream) infections Efficient: The removal of PVCs as soon as complications are evident may result in releasing time for other care and a reduction in the NHS costs associated with complications such as CRBSIs Equitable: This recommendation promotes a standard of care for all patients, that may result in a reduction in avoidable personal and NHS costs, which is beneficial for all Timely: This recommendation, daily checking, fits with other aspects of care required on a daily basis, contributing to streamlining of care
Health impact contribution (based on Healthcare Quality Strategy for NHSScotland)
Person Centred: This is a person centred action to reduce harm which could be caused by the invasive device; in every patient with a PVC and provides the opportunity to undertake simple, safe checks and care on each and every patient with a PVC
Measurement and feedback
(Y/N/?) Feasibility and sustainability
(Y/N/?) Applicability and reach
(Y/N/?)
Training and
informing (Y/N/?)
Potential for measurement through e.g. observation
Easily implemented within current culture and will improve the quality of care now
Potential for consistent delivery
Easily implemented based on reliably available resources/products/prompts
Stealth integration into natural workflow/logical clarity of concept (also see Cause & Effect Chart)
Unambiguous
Potential for applicability to a wide range of settings
Avoids unintended consequences/perverse behaviour
Potential for congruency in design and meaning, with HCW, trainer and observer training and education
Expert opinion/consultation and practical considerations
Y Y Y Y Y ? Y ? Y
Is this a key recommendation? Yes
Health Protection Scotland v1.0. April 2012
Page 23 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
Recommendation for review Ensure that PVC dressings are intact
Grade of recommendation (based on review of evidence)
Category 1A
Safe: This recommendation reduces the risk of complications from this invasive device
Effective: This recommendation reduces the risk of complications from this invasive device, including on occasions systemic (blood stream) infections.
Efficient: This recommendation reduces the risk of infectious complications and may result in releasing time for other care and in a reduction in associated NHS costs Equitable: This recommendation promotes a standard of care for all patients, that may result in a reduction in avoidable personal and NHS costs, which is beneficial for all Timely: This recommendation, daily checking, fits with other aspects of care required on a daily basis, contributing to streamlining of care
Health impact contribution (based on Healthcare Quality Strategy for NHSScotland)
Person Centred: This is a person centred action to reduce harm which could be caused by the invasive device; in every patient with a PVC and provides the opportunity to undertake simple, safe checks and care on each and every patient with a PVC
Measurement and feedback
(Y/N/?) Feasibility and sustainability
(Y/N/?) Applicability and reach
(Y/N/?)
Training and
informing (Y/N/?)
Potential for measurement through e.g. observation
Easily implemented within current culture and will improve the quality of care now
Potential for consistent delivery
Easily implemented based on reliably available resources/products/prompts
Stealth integration into natural workflow/logical clarity of concept (also see Cause & Effect Chart)
Unambiguous
Potential for applicability to a wide range of settings
Avoids unintended consequences/perverse behaviour
Potential for congruency in design and meaning, with HCW, trainer and observer training and education
Expert opinion/consultation and practical considerations
Y Y Y Y Y ? Y ? Y
Is this a key recommendation? Yes
Health Protection Scotland v1.0. April 2012 Page 24 of 29

Targeted literature review: What are the key infection prevention and control recommendations to inform the peripheral vascular catheter (PVC) maintenance care quality improvement tool
Health Protection Scotland v1.0. April 2012 Page 25 of 29
Recommendation for review Ensure that an antiseptic containing 70% isopropyl alcohol is used to clean the access hub before accessing – rub the access hub for at least
15 seconds (‘scrub the hub’)
Grade of recommendation (based on review of evidence)
Category 1B
Safe: This recommendation reduces the risk of complications from this invasive device
Effective: This recommendation reduces the risk of complications from this invasive device, including on occasions systemic (blood stream) infections Efficient: This recommendation reduces the risk of infectious complications and may result in releasing time for other care and in a reduction in associated NHS costs Equitable: This recommendation promotes a standard of care for all patients, that may result in a reduction in avoidable personal and NHS costs, which is beneficial for all Timely: This recommendation, fits with other aspects of care required on a daily basis, contributing to stream lining of care
Health impact contribution (based on Healthcare Quality Strategy for NHSScotland)
Person Centred: This is a person centred action to reduce harm which could be caused by the invasive device; in every patient with a PVC
Measurement and feedback
(Y/N/?) Feasibility and sustainability
(Y/N/?) Applicability and reach
(Y/N/?)
Training and
informing (Y/N/?)
Potential for measurement through e.g. observation
Easily implemented within current culture and will improve the quality of care now
Potential for consistent delivery
Easily implemented based on reliably available resources/products/prompts
Stealth integration into natural workflow/logical clarity of concept (also see Cause & Effect Chart)
Unambiguous
Potential for applicability to a wide range of settings
Avoids unintended consequences/perverse behaviour
Potential for congruency in design and meaning, with HCW, trainer and observer training and education
Expert opinion/consultation and practical considerations
Y ? Y Y Y Y Y Y Y
Is this a key recommendation? Yes

Targeted literature review: What are the key infection prevention and control recommendations to inform the Peripheral Vascular Catheter (PVC) maintenance care quality improvement tool
Health Protection Scotland v1.0. April 2012 Page 26 of 29
Appendix 3: Literature review methodology
The evidence underpinning the criteria for a quality improvement tool was reviewed using a targeted
systematic approach to enable input and resource to be concentrated where needed. This methodology is
fully described within a separate paper ‘Rapid method for development of evidence based/expert opinion key
recommendations, based on health protection network guidelines’.
Initial rapid search and review
The initial rapid literature search was carried out to identify mandatory guidance, or recent national or
international evidence based guidance which either agrees or refutes that the current key recommendations
are the most important to ensure optimal PVC care:
• The main public health websites were searched to source any existing quality improvement tools
• Relevant guidance and quality improvement tools e.g. Department of Health (DH), Centers for Disease
Control and Prevention (CDC) etc were reviewed
• Additional literature identified and sourced e.g. from the relevant Cochrane reviews.
The quality of evidence based guidance was assessed using the AGREE instrument46 and only guidance
which achieved either a strongly recommend or recommend rating was included.
Targeted systematic review
As a result of initial rapid search and review, recommendations requiring a more in depth review were
identified. This involved searching of relevant databases including OVID Medline, CINAHL, EMBASE. All
literature pertaining to recommendations where evidence was either conflicting or where new evidence was
available were critically appraised using SIGN checklists and a ‘considered judgement’ process used to
formulate recommendations based on the current evidence for presentation and discussion with the National
HAI Quality Improvement Tools Group in Scotland.
Grading of recommendations
Grading of the evidence is using the Healthcare Infection Control Practices Advisory Committee (HICPAC)
method.47 In addition to the overall assessment of the evidence underpinning the recommendation, other
factors are considered which affect the overall strength of the recommendation such as the health impact
and expert opinion on the potential critical outcomes.
The HICPAC categories are as follows:
Category 1A – strong recommendation based on high to moderate quality evidence
Category 1B – strong recommendation based on low quality of evidence which suggest net clinical benefits
or harms or an accepted practice (e.g. aseptic technique)
Category 1C – a mandatory recommendation

Targeted literature review: What are the key infection prevention and control recommendations to inform the Peripheral Vascular Catheter (PVC) maintenance care quality improvement tool
Health Protection Scotland v1.0. April 2012 Page 27 of 29
Category II – a weak recommendation which shows evidence of clinical benefit over harm
No recommendation – not sufficient evidence to recommend one way or another
Framework for identifying final key recommendations
One way of improving implementation of evidence based guidance is by the identification of key
recommendations which if applied will improve practice and outcome.30;32;48-52 This is the foundation of ‘care
bundles’ and other quality improvement tools which rely on the identification of key evidence based
recommendations to ensure application in practice.53
A method has been developed which aims to reflect graded recommendations in line with ensuring
healthcare quality, attention to cost and practical application. It combines approaches used by the Institute of
Healthcare Improvement (IHI) and World Health Organisation, among others, in identifying the critical factors
from the evidence to ensure patient safety in a range of fields.52;54 The method considers the current
NHSScotland Quality Strategy dimensions and finally expert opinion applied within a formal framework. This
framework includes a range of practical considerations under the headings measurement and feedback,
feasibility and sustainability, applicability and reach, training and informing.
Ultimately, HPS key recommendations are presented taking all of these factors into account, with the aim of
improving practice and outcome.
The search strategy used is described in Appendix 4.

Targeted literature review: What are the key infection prevention and control recommendations to inform the Peripheral Vascular Catheter (PVC) maintenance care quality improvement tool
Health Protection Scotland v1.0. April 2012 Page 28 of 29
Appendix 4: Search Strategy
Database: Ovid MEDLINE(R) <1948 to April Week 3 2011>
Search Strategy:
--------------------------------------------------------------------------------
1 Catheterization/ or exp Catheterization, Peripheral/ (37696)
2 peripheral vascular catheter.mp. (79)
3 venflon.mp. (40)
4 1 or 2 or 3 (37751)
5 phlebitis.mp. (4605)
6 extravasation.mp. (11103)
7 exp Bacteremia/ or bacteraemia.mp. (18980)
8 blood stream infection$.mp. (346)
9 thrombophlebitis.mp. (22148)
10 5 or 6 or 7 or 8 or 9 (56084)
11 4 and 10 (1378)
12 limit 11 to (english language and humans and yr="2006 -Current") (215)
13 from 12 keep 1-212 (212)
***************************
Key literature from e.g. the relevant Cochrane reviews was also sourced and critically appraised using SIGN
methodology

Targeted literature review: What are the key infection prevention and control recommendations to inform the Peripheral Vascular Catheter (PVC) maintenance care quality improvement tool
Appendix 5: Summary of key recommendations for PVC insertion and maintenance
Health Protection Scotland v1.0. April 2012 Page 29 of 29