tard-15821: klinik araştırma magnezyum sülfatın...
TRANSCRIPT

Page 1 / 50
JournalAgent powered by LookUs
TARD-15821: Klinik Araştırma
Magnezyum sülfatın obstetrik hastalarda anestezi derinliği
üzerine etkisi
Amaç: Çalışmadaki öncelikli hipotezimiz, magnezyumun genel anesteziye bir yardımcı gibi davranarak anestezi derinliğini arttırabildiğidir. İkincil hipotezimiz, magnezyum infüzyonunun sezeryan seksiyo 5 operasyonu sonrası ağrıyı azaltabildiğidir. Yöntemler: Genel anestezi altında sezeryan seksiyo yapılması planlanan hastalar randomize olarak dört
gruba ayrıldı. İndüksiyon sonrası idame amacıyla Grup S’de sevofluran, Grup D’de desfluran kullanıldı (kontrol grupları). Grup S-M ve Grup D-M’de, sırasıyla sevofluran ve desfluran anestezisiyle beraber
magnezyum infüzyonu başlandı (çalışma grupları). İdame boyunca inhaler gazların minimum alveolar 10 konsantrasyonları sabit tutuldu. Bispectral index skorları (BIS), hemodinamik parametreler, train of four (TOF) değerleri ve postoperatif vizüel analog skalası değerleri kaydedildi. Tüm hastalar farkındalık
açısından değerlendirildi ve postoperatif 5 yıl boyunca takip edildi. Bulgular: Çalışmaya toplamda 100 hasta dahil edildi. BIS skorları kontrol gruplarında operasyon boyunca
belirgin biçimde yüksekti (p<0.001). Hemodinamk parametrelerde belirgin bir fark elde edilmedi. Tüm 15 zaman noktalarında kontrol gruplarının TOF değerleri daha yüksekti (p<0.05). VAS değerleri çalışma gruplarında belirgin biçimde düşüktü (p<0.05). Hastaların hiçbiri genel anestezi altında farkındalık
yaşamadı. Sonuç: Magnezyum infüzyonu belirgin biçimde daha düşük BIS değerleri ve postoperatif VAS skorları
sağlamıştır. Magnezyumun sezeryan seksiyo hastalarında genel anesteziye yardımcı olarak faydalı 20 olabileceğine inanmaktayız.
Anahtar Kelimeler: Anestezi derinliği, bi-spectral indeks, farkındalık, genel anestezi, magnezyum, postoperatif ağrı
Effect of magnesium sulphate on anesthetic depth of obstetric 25
patients
Objective: In this study, our primary hypothesis is magnesium can increase the depth of anesthesia by acting as an adjuvant to general anesthesia. Our secondary hypothesis is magnesium infusion can reduce
postoperative pain after caesarean section. Methods: The patients scheduled for caesarean section under general anesthesia were divided into four 30 groups randomly. After induction, sevoflurane was used for maintenance in Group S and desflurane in Group D (control groups). At Group S-M and Group D-M (study groups), magnesium infusion was started
with sevoflurane and desflurane anesthesia respectively. Minimum alveolar concentration of inhaler
anesthetic agents were kept constant throughout the maintenance. Bispectral index scores (BIS), hemodynamic parameters, train of four values (TOF) and postoperative visual analogue scale (VAS) 35 values were recorded. All of the patients were evaluated for awareness and followed up for five years postoperatively.
Results: A total of 100 patients were included in the study. BIS values were significantly higher in control
groups throughout the operation (p < 0.001). No significant difference was obtained at hemodynamic parameters. At all time points, TOF values of control groups were higher ( p < 0.05). VAS values were 40 significantly lower in study groups ( p < 0.05). None of the patients had awareness under general anesthesia.
Conclusion: Magnesium infusion provided significantly lower intraoperative BIS values and lower
postoperative VAS scores. We believe that magnesium can be useful as an adjuvant to general anesthesia in cesarean section patients. 45
Key words: Anesthetic depth, bi-spectral index, awareness, general anesthesia, magnesium,
postoperative pain
Ref.No: TARD-15821 (2)
Makale Grubu: Genel Anestezi 50 Makale Türü: Klinik Araştırma
Kayıt Tarihi: 08.09.2016 22:30:47


Page 3 / 50
JournalAgent powered by LookUs
Revised Files (1) Tam Metin 55 maintext Kayıt Tarihi: 03.10.2017 03:45:32
INTRODUCTION 60
Magnesium has widely been used in anesthetic management in the recent years. It was shown
to attenuate stress response to endotracheal intubation, preserving favorable hemodynamics,
block acetylcholine discharge from neuromuscular junction and potentiate the effect of non-
depolarizing neuromuscular blockers. Recently magnesium sulphate was reported to reduce
anaesthetic requirements, shorten anaesthetic induction with propofol and diminishe total 65
postoperative analgesic consumption with no adverse maternal or neonatal effects [1-3]. It has
potential analgesic and sedative properties, therefore it may be used as an adjuvant during general
anesthesia [4].
In the current literature, there are studies examining the effects of magnesium on the anesthetic
agent doses needed to keep bi-spectral index (BIS) values within a fixed range, however untill now 70
only one single pediatric study evaluated the influence of intraoperative magnesium on BIS values
while keeping other intraoperative variables (such as operation type and end-tidal anesthetic
consantration) almost constant. But in this recent study, depth of anesthesia was evaluated only by
intraoperative BIS values [5].
The term “awareness” under anesthesia is used in literature as the wakening of brain by a stimulant 75
under general anesthesia and storing this information in order to recall it in the future [6]. Although
most of the patients experienced awareness may seem to have no complaint in the long time period
postoperatively [7], symptoms like nightmares, daytime anxiety and flashbacks can be seen and in
some cases, even patients may develop posttraumatic stress disorder [7, 8].
Although over the last 20 years, there has been a large increase in the proportion of caesarean 80
section performed under regional anaesthesia, in emergency situations or when there is a
contraindication for regional anesthesia or in the situation of patient’s refusal, general anesthesia is
Page 4 / 50
JournalAgent powered by LookUs
applied [9]. Therefore general anesthesia is still frequently performed for caesarean sections in
some clinics. As low doses of general anaesthetic agents have traditionally been used in caesarean
sections, obstetric patients are reported to have a higher incidence of intraoperative awareness than 85
other surgical patients, especially during the period before delivery [10].
In this study our primary hypothesis is magnesium can increase the depth of anesthesia by acting as
an adjuvant to general anesthesia in obstetric patients. We aimed to assess this effect by monitoring
bispectral index scores and incidence of awareness. Our secondary hypothesis is magnesium
infusion can reduce postoperative pain after caesarean section. 90
95
100
105
MATERIAL AND METHOD
After receiving hospital Clinical Trials Local Ethic Committee approval (reference Number: LUT-
10/60) and patients’ informed consents, 100 patients (American society of anesthesiologists status I-
II and between 17-41 years old) undergoing cesarean section with general anesthesia were included 110
in this prospective randomized controlled study. The study was conducted in accordance with the
Helsinki declaration in Ankara Hacettepe University Hospital between 2010-2011 and patient
follow-up has been continued untill 2016 via phone calls. Patients with known history of
magnesium sulphate hypersensivity, hypermagnesemia, any degree of heart block, hypertension,
diabetus mellitus, preterm or multiple pregnancy, preoperative fetal distress or other medical 115

Page 5 / 50
JournalAgent powered by LookUs
conditions were excluded from the study. In the operating room, electrocardiogram, non invasive
blood pressure, peripheral oxygen saturation, train of four (TOF) (Datex-Ohmeda N-NMT Sensors)
and BIS (Datex-Ohmeda S/5TM) measurements were monitored. Patients were randomized into
four groups by using a computer-generated randomization schedule and each group included 25
patients. The study drug solutions were prepared into 20-mL identical syringes for bolus doses and 120
500-mL serum physiologic solutions for intraoperative infusions and labeled by an anesthetist who
did not participate in the study. The investigators and patients were blinded to group allocation. The
first and the second groups were planed to receive sevoflurane and desflurane as inhalation
anesthetic agent respectively. They were planed to receive serum physiologic in 20-mL syringes and
serum physiologic as infusion solution (Group S and D). These two groups were “control groups” 125
of the study. In the third and fourth groups, patients were planed to receive sevoflurane and
desflurane as inhalation anesthetic agent respectively. They were planed to receive 30 mg kg ֿ ֿ ¹
magnesium sulfate in 20-mL syringes and magnesium sulfate plus serum physiologic as infusion
solution (Group S-M and D-M). These two groups were our “study groups”. So there would be
totally 50 patients in control groups and 50 patients in the study groups. 130
Induction was performed with 2-3 mg kg ֿ ¹ i.v propofol and 0.6 mg kg ֿ ֿ i.v rocronium bromide in
all groups. After induction, in groups S-M and D-M, 30 mg kg ֿ ¹ i.v magnesium sulfate was
applied as bolus in 15-20 seconds and then 10 mg kg ֿ ֿ hour ֿ ¹ magnesium sulfate infusion in 500-
mL serum physiologic solution was started.
At the maintenance of anesthesia 2% end-tidal sevoflurane and 4 lt min ֿ ֿ ֿ ¹ 40% O2-60% N2O 135
were used in group S and group S-M, and 6% end-tidal desflurane and 4 lt min ֿ ¹ 40% O2-60%
N2O were used in group D and group D-M. When heart rate or blood pressure increased more than
20% of baseline values, fentanyl 1 mcg kg ֿ ֿ ¹ was applied intravenously while minimum alveolar
concentration (MAC) remained constant. In all groups BIS values, mean arterial pressure (MAP)
and heart rate of the patients were recorded before induction, right after induction and at five minute 140
intervals throughout the operation. TOF measurement started after induction and continues with five

Page 6 / 50
JournalAgent powered by LookUs
minute intervals throughout the operation. Intraoperative opioid requirement was recorded
following induction and throughout the operation. For postoperative analgesia, 1000 mg
paracetamol was applied intravenously 15 minutes before the end of the surgery and 75 mg
diclofenac sodium was applied at every 8 hours in the ward. When Visual Analogue Scale (VAS) 145
scores were 4 or more, tramadol 1 mg kg ֿ ¹ i.v was applied as rescue analgesic. Patients were
evaluated at the postoperative 1st , 2nd and 24th hours by VAS.
In order to evaluate anesthesia depth in a more objective manner, patients were also assessed for
awareness under general anesthesia. For this purpose, following anesthesia induction, a text chosen
with the consultancy of Hacettepe University Medical Faculty Psychiatry Department was listened 150
to all patients via earphones. This text was a story included in the “Wechsler Memory Scale” used
for neurophysiological examination of the patients and there were 24 key words in this single line
text [11]. Similar to previous studies [12, 13], all patients were questioned at postoperative 1st, 6th,
24th hours, at the end of the 1st month by the same anesthesiogist. As an addition to previous studies,
we interviewed with the patients at the end of the first, second, third, fourth and fifth year in order 155
to evaluate long term effects of general anesthesia. First all patients were given some clues about
the story and then they were asked whether if they recalled anything about the text or not. Besides
Wechsler Memory Scale, questions from “Modified Brice interviews” which is still accepted as the
gold-standart for postoperative awareness screening were also asked [14]. The interview is
consisted of five simple questions which were first defined by Brice et al. [15] and then modified by 160
Moerman et al. [16]. These questions are listed as – “1) What is the last thing you remember before
sleeping? 2) What is the first thing you remember at awaking after the surgery? 3) Do you
remember anything in between? 4) Did you see any dreams? 5) What was the most disturbing thing
you remember about the operation and anesthesia?.
165

Page 7 / 50
JournalAgent powered by LookUs
170
175
STATISTICAL ANALYSIS
Calculation of sample size was based on previous investigations conducted about the effects of Mg
sulphate on BIS values and propofol consumption. Assuming α error = 0.05 (two-tailed) and β
error = 0.1. sample size of totally 45 patients, allocated into one group, will have a power of 90 % 180
to determine an assumed clinically significant difference of 5 % (effect size d = 0.6) between the
paired measurements of BIS value in groups with and without magnesium infusion. The sample size
was calculated using Power Analysis and Sample Size 12 software (NCSS, Kaysville, UT, USA).
The statistical anaylsis was made by using the Statistical Package for Social Science, version 17.0
(SPSS Inc., Chicago, IL). All demographic datas and perioperative periods were evaluated with One 185
Way Variance Analysis. Turkey-HSD test was used for the multiple comparison between groups.
For evaluation of VAS values non-parametric Kruskal-Wallis test was performed. Exact chi-square
test was used to compare additional analgesic need, dreaming, remembering and recalling the story.
“P < 0,05” was accepted as statistically significant and all datas was defined as “mean±SD”.
190
195
200
RESULTS
A hundred and twenty patients were included into the study. Two of the patients were excluded due
to intraoperative allergic symptoms. Six patients declined to participitate in the study during their
Page 8 / 50
JournalAgent powered by LookUs
follow-up in the postoperative period and twelve patients were excluded due to intraoperative 205
techniqual faults. The demographic variables and surgical characteristics of the remaining 100
patients were similar (Table 1).
For analysis of BIS values, five different time-points were chosen; before induction (BIS 0), 5
minutes after the induction (BIS 5), total operation median time (BIS Median) and end of the
operation (BIS End) (Table 2). 210
BIS values before the induction were similar in all groups (p > 0.05) whereas values at BIS 5 were
significantly higher in the sevoflurane group (p < 0.001).
At the BIS Median point; BIS values in control groups were statistically significantly higher than
the study groups ( p < 0.001), while Group S and Group D were similar to each other ( p = 0.519).
Likewise BIS End values of control groups were significantly higher than study groups ( p < 0.001), 215
while Group S and Group D were similar to each other (p = 0.781). There was no statistically
significant difference amoung study groups ( p = 0.737). BIS values measured in each group
throughout the operation is shown in Figure 1.
There was no significant difference at MAP and heart rate between the groups throughout the
operation ( p > 0.05) (Table 3). 220
At all time points, TOF values of group S and D were found to be higher than study groups. There
was no significant difference between the groups S-M and D-M or between control groups at any
time-point (Table 4).
225
Postoperative pain was questioned at 1st, 2nd and 24th hour. VAS scores in all time points were
significantly lower in study groups (p < 0.05). VAS scores of Group S and Groups D were similar,
and groups S-M and D-M were similar to each other (Table 5).
During the interviews performed at the end of 1st, 6th and 24th hour, one patient in group S, two in
group D and one in group D-M reported to have dream intraoperatively. They stated that their 230
dreams were not related to their surgeries. At the end of the first month, same four patients reported
that they dreamed intraoperatively but couldn’t remember anything about the content of their

Page 9 / 50
JournalAgent powered by LookUs
dreams. This difference amoung groups was not statistically significant (p = 0.9) (Table 6).
At the end of the first and second years we managed to interview with all patients and non of them
could remember anything new. At the end of the third, fouth and fifth years we couldn’t contact 235
with two patients in group S and three patients in each group S-M and group D-M. None of the
patients reported to hear any sound during the operation nor remember anything. None of the
patients could give a significant answer to the questions of Modified Brice interviews by means of
intraoperative awareness. Likewise, none of the patients could remember the story played through
earphones, or find any of the key words. None of the patients had any signs of posttraumatic stress 240
disorder meanwhile.
245
250 DISCUSSION
In the current study, BIS scores were significantly lower in groups with magnesium infusion, while
none of the patients had awareness under general anesthesia. Postoperative VAS scores were
significantly lower in groups with magnesium infusion. There was no significant difference at
hemodynamic parameters. But TOF values were significantly lower in groups with magnesium 255
infuion.
In general practice, BIS is accepted as a voluable monitor for depth of anesthesia both in adult and
pediatric patients. When the underlying mechanism of general anesthesia is considered, hypnosis as
a single component of anesthesia can not be used to define overall “anesthetic depth” [17], however
the hypnotic depth is known to be the primary endpoint of anesthesia and it has become the focus of 260
contemporary depth of anesthesia monitoring [18]. Therefore we evaluated the central effect of
magnesium by using BIS monitoring. In the literature, there are several studies which have

Page 10 / 50
JournalAgent powered by LookUs
evaluated the effect of intraoperative magnesium on intravenous or inhaled anesthetic doses, opioid
demands or muscle relaxant needs to keep BIS values between 40-60. However, Amer et al.
recently claimed that BIS values between 40-60 may be considered a relatively wide range to 265
objectively evaluate the effect of magnesium on anesthetic requirements. In their study, BIS was
used as the single monitoring and similar to the current study, BIS values were significantly lower
in magnesium group [5]. On the other hand, we have followed up the patients for five years and
performed interviews to evaluate “awareness” experience under general anesthesia. In other words,
we examined the central effect of magnesium in a long-term period beside it’s short term, 270
intraoperative effects.
Awareness under general anesthesia is often experienced due to inadequate levels of anesthesia
[19]. It’s been reported in the literature that serious psycological problems which leads to
posttraumatic stress disorder may occur during long-term follow up of these patients [6]. Today
intraoperative awareness is mostly observed when opioids and benzodiazepines or weak anesthetics 275
like nitrous oxide are used seperately or together. Contrary to this, inhalation anesthethics like
sevoflurane, desflurane, isoflurane and potent intravenous anesthetics used in proper concentrations
are believed to prevent intraoperative perception succesfully [20]. However, there are plenty of
intraopertive awareness cases experienced with inhalation anesthetics in the literature [21, 22]. In
the light of these informations, we suggested that adding an adjuvant agent to general anesthesia 280
might have helped to increase depth of anesthesia and prevent intraoperative awareness. We
prefered to add magnesium infusion to general anesthesia provided by sevoflurane or desflurane
anesthetics and none of our patients experienced awareness. Dreaming which is believed to be
related with awareness was detected at four patients, but when we compared the groups, there was
no statistically significant difference. Awareness under general anesthesia is a rare complication 285
seen between 0.1%-0.2% of all patients [6]. However, some publications reported that these
numbers can rise upto 7-28% in obstetric surgeries [6, 23]. Although the current study was held
with obstetric patients, no one reported to experience awareness. The most likely reason is our

Page 11 / 50
JournalAgent powered by LookUs
sample size may lack to detect an awareness case. Secondly, constant and reasonable MAC values
maintaned throughout the operation probably prevented awareness under general anesthesia. Beside 290
these, fentanyl was applied to the patients when hemodynamic parameters incresed more than %20
of baseline values.
In the study of Lee et al, different dosages of magnesium were compared with control group and it
was shown that BIS values were significantly lower in the groups with magnesium infusion [24]. In
the current study, BIS values were also significantly lower in the groups with magnesium infusion 295
throughout the operation. This result supports our suggestion about magnesium being a good
advujant to general anesthesia. Beside this, BIS values of the groups with magnesium infusion
didn’t differ significantly. This brings the idea that magnesium may deepen the level of anesthesia
with regardless of type of inhalated anesthetic agent. On the other hand, when we look at the non-
magnesium groups; BIS values in the 5th minute after induction was higher in sevolfurane group 300
than desflurane group. According to previous studies performed with similar inhalation anesthetics,
this difference between sevoflurane and desflurane is not suprising. It is known that different
inhalation anesthetics given at the end-tidal concentration levels providing same potency can result
in different BIS values of patients [25]. Jellish et al. compared sevoflurane and desflurane and
reported that BIS values were significantly lower in the desflurane group [26]. 305
The analgesic effect mechanism of magnesium sulfate has not been shown clearly yet, but
inhibition of calcium channels and N-methyl-D-aspartate receptors are believed to have an
important role [27]. In previous studies, bolus dosage of magnesium was shown to significantly
reduce additional analgesic requirement [28]. However in the current study, intraoperative fentanyl
consumption didn’t significantly differ between groups. The most possible reason is the difference 310
between methodologies of the studies. In the study of Gupta et al., fentanyl was applied in order to
keep BIS values between 40-60. On the other hand, we applied fentanyl according to hemodynamic
changes. As there was no significant difference in MAP and heart rate of the patients, no significant
difference was found in fentanyl consumption.

Page 12 / 50
JournalAgent powered by LookUs
In the literature, several studies have reported magnesium sulphate infusion to reduce postoperative 315
pain. Recently Mireskandari et al. have evaluated the effect of preoperatively induced magnesium
sulphate on postoperative pain in obstetric patients. They reported that intravenous bolus
magnesium sulphate prior to induction of general anesthesia could reduce postoperative VAS and
had sparing effects on morphine consumption during first 24 hours [29]. Similarly, VAS scores of
magnesium groups were significantly lower at all time points in our study. On the other hand, 320
Frassanito et al. have studied the effect of intravenous magnesium infusion on postoperative pain of
patients after total knee arthroplasty performed under spinal anesthesia. They couldn’t find any
significant difference at postoperative pain and analgesic consumption after intravenous magnesium
sulphate infusion [30]. Nowadays magnesium is in the focus of studies analyzing post operative
inflammation. It was recently reported to significantly reduce postoperative sore throat related to 325
endotracheal intubation [31]. Although the exact mechanism is not known, the attenuation effect of
magnesium on inflammatory response to surgery may also play a role to lower postoperative pain.
The major limitation of our study is the relatively small sample size. The power analyzis was
calculated in order to obtaine a significant difference between the paired measurements of BIS
value, so the calculated patient number was probably insufficent to detect an awareness case. In 330
order to get more objective data on awareness under general anesthesia, it’s necessary to perform
studies with larger number of patients but nowadays it’s becoming harder due to increased ratios of
regional anesthesia at cesarean sections.
335
CONCLUSION
In this study, magnesium infusion provided significantly lower intraoperative BIS values and lower
postoperative VAS scores. We believe that magnesium can be useful as an adjuvant to general 340
anesthesia in cesarean section patients. Larger number of sample size is needed to properly assess

Page 13 / 50
JournalAgent powered by LookUs
awareness under general anesthesia.
345
Acknowledgements
We are grateful to Prof Dr Başaran Demir from Hacettepe University Medical Faculty Department of Psychiatry for his consultancy at awareness assessment. 350
355
360
365
370
REFERENCES 375
1. Altan A, Turgut N, Yildiz F, Turkmen A, Ustun H: Effects of magnesium sulphate and clonidine on propofol consumption, haemodynamics and postoperative recovery. British journal of anaesthesia 2005, 94(4):438-441.
2. Gupta K, Vohra V, Sood J: The role of magnesium as an adjuvant during general anaesthesia. Anaesthesia 2006, 61(11):1058-1063. 380
3. Kutlesic MS, Kutlesic RM, Mostic-Ilic T: Magnesium in obstetric anesthesia and intensive care. Journal of anesthesia 2017, 31(1):127-139.
4. Barbosa FT, Barbosa LT, Juca MJ, Cunha RM: Applications of magnesium sulfate in obstetrics and anesthesia. Rev Bras Anestesiol 2010, 60(1):104-110.
5. Amer MM, Abdelaal Ahmed Mahmoud A, Abdelrahman Mohammed MK, Elsharawy AM, Ahmed 385 DA, Farag EM: Effect of magnesium sulphate on bi-spectral index (BIS) values during general anesthesia in children. BMC anesthesiology 2015, 15:126.
6. Ghoneim MM, Block RI, Haffarnan M, Mathews MJ: Awareness during anesthesia: risk factors, causes and sequelae: a review of reported cases in the literature. Anesthesia and analgesia 2009, 108(2):527-535. 390

Page 14 / 50
JournalAgent powered by LookUs
7. Lopez U, Habre W, Van der Linden M, Iselin-Chaves IA: Intra-operative awareness in children and post-traumatic stress disorder. Anaesthesia 2008, 63(5):474-481.
8. Osterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk BA: Awareness under anesthesia and the development of posttraumatic stress disorder. Gen Hosp Psychiatry 2001, 23(4):198-204.
9. Campbell J, Sultan P: Regional anaesthesia for caesarean section: a choice of three techniques. Br 395 J Hosp Med (Lond) 2009, 70(10):605.
10. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, Domino KB: The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004, 99(3):833-839, table of contents.
11. Shaygannejad V, Janghorbani M, Ashtari F, Zanjani HA, Zakizade N: Effects of rivastigmine on 400 memory and cognition in multiple sclerosis. Can J Neurol Sci 2008, 35(4):476-481.
12. Myles PS, Leslie K, McNeil J, Forbes A, Chan MT: Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004, 363(9423):1757-1763.
13. Elhakim M, Abdelhamid D, Abdelfattach H, Magdy H, Elsayed A, Elshafei M: Effect of epidural dexmedetomidine on intraoperative awareness and post-operative pain after one-lung 405 ventilation. Acta Anaesthesiol Scand 2010, 54(6):703-709.
14. Sneyd JR, Mathews DM: Memory and awareness during anaesthesia. Br J Anaesth 2008, 100(6):742-744.
15. Brice DD, Hetherington RR, Utting JE: A simple study of awareness and dreaming during anaesthesia. Br J Anaesth 1970, 42(6):535-542. 410
16. Moerman N, Bonke B, Oosting J: Awareness and recall during general anesthesia. Facts and feelings. Anesthesiology 1993, 79(3):454-464.
17. Campagna JA, Miller KW, Forman SA: Mechanisms of actions of inhaled anesthetics. The New England journal of medicine 2003, 348(21):2110-2124.
18. Bruhn J, Myles PS, Sneyd R, Struys MM: Depth of anaesthesia monitoring: what's available, what's 415 validated and what's next? British journal of anaesthesia 2006, 97(1):85-94.
19. Ghoneim MM: Awareness during anesthesia. Anesthesiology 2000, 92(2):597-602. 20. Guler T: İntraoperatif Uyanıklık. Türk Anesteziyoloji ve Reanimasyon Derneği Dergisi 2009,
37(5):265-279. 21. Kino A KR, Wakamatsu T, Hashiguchi M, Nakamura K: Awareness during anesthesia with 420
sevoflurane: a case report. Masui The Japanese journal of anesthesiology 2006, 55(10):1250-1252. 22. Kino A NK: Awareness during general anesthesia for head and neck surgery--a case report. Masui
The Japanese journal of anesthesiology 2011, 60(2):241-243. 23. Paech MJ, Scott KL, Clavisi O, Chua S, McDonnell N, Group AT: A prospective study of awareness
and recall associated with general anaesthesia for caesarean section. International journal of 425 obstetric anesthesia 2008, 17(4):298-303.
24. Lee DH, Kwon IC: Magnesium sulphate has beneficial effects as an adjuvant during general anaesthesia for Caesarean section. Br J Anaesth 2009, 103(6):861-866.
25. Samarkandi AH: The bispectral index system in pediatrics--is it related to the end-tidal concentration of inhalation anesthetics? Middle East J Anesthesiol 2006, 18(4):769-778. 430
26. Jellish WS, Owen K, Edelstein S, Fluder E, Leonetti JP: Standard anesthetic technique for middle ear surgical procedures: a comparison of desflurane and sevoflurane . Otolaryngol Head Neck Surg 2005, 133(2):269-274.
27. Miranda HF, Bustamante D, Kramer V, Pelissier T, Saavedra H, Paeile C, Fernandez E, Pinardi G: Antinociceptive effects of Ca2+ channel blockers. Eur J Pharmacol 1992, 217(2-3):137-141. 435
28. Gupta SD, Mitra K, Mukherjee M, Roy S, Sarkar A, Kundu S, Goswami A, Sarkar UN, Sanki P, Mitra R: Effect of magnesium infusion on thoracic epidural analgesia. Saudi journal of anaesthesia 2011, 5(1):55-61.
29. Mireskandari SM, Pestei K, Hajipour A, Jafarzadeh A, Samadi S, Nabavian O: Effects of preoperative magnesium sulphate on post-cesarean pain, a placebo controlled double blind study. Journal of 440 family & reproductive health 2015, 9(1):29-33.

Page 15 / 50
JournalAgent powered by LookUs
30. Frassanito L, Messina A, Vergari A, Colombo D, Chierichini A, Della Corte F, Navalesi P, Antonelli M: Intravenous infusion of magnesium sulfate and postoperative analgesia in total knee arthroplasty. Minerva anestesiologica 2015, 81(11):1184-1191.
31. Yadav M CN, Gopinath R: Effect of magnesium sulfate nebulization on the incidence of 445
postoperative sore throat. Journal of anaesthesiology, clinical pharmacology 2016, 32(2):168-171.
450
There is no conflict of interest.
455

Page 16 / 50
JournalAgent powered by LookUs
Kaynaklar 460 References
Kayıt Tarihi: 03.10.2017 03:46:34
REFERENCES 465
1. Altan A, Turgut N, Yildiz F, Turkmen A, Ustun H: Effects of magnesium sulphate and clonidine on propofol consumption, haemodynamics and postoperative recovery. British journal of anaesthesia 2005, 94(4):438-441.
2. Gupta K, Vohra V, Sood J: The role of magnesium as an adjuvant during general anaesthesia. 470 Anaesthesia 2006, 61(11):1058-1063.
3. Kutlesic MS, Kutlesic RM, Mostic-Ilic T: Magnesium in obstetric anesthesia and intensive care. Journal of anesthesia 2017, 31(1):127-139.
4. Barbosa FT, Barbosa LT, Juca MJ, Cunha RM: Applications of magnesium sulfate in obstetrics and anesthesia. Rev Bras Anestesiol 2010, 60(1):104-110. 475
5. Amer MM, Abdelaal Ahmed Mahmoud A, Abdelrahman Mohammed MK, Elsharawy AM, Ahmed DA, Farag EM: Effect of magnesium sulphate on bi-spectral index (BIS) values during general anesthesia in children. BMC anesthesiology 2015, 15:126.
6. Ghoneim MM, Block RI, Haffarnan M, Mathews MJ: Awareness during anesthesia: risk factors, causes and sequelae: a review of reported cases in the literature. Anesthesia and analgesia 2009, 480 108(2):527-535.
7. Lopez U, Habre W, Van der Linden M, Iselin-Chaves IA: Intra-operative awareness in children and post-traumatic stress disorder. Anaesthesia 2008, 63(5):474-481.
8. Osterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk BA: Awareness under anesthesia and the development of posttraumatic stress disorder. Gen Hosp Psychiatry 2001, 23(4):198-204. 485
9. Campbell J, Sultan P: Regional anaesthesia for caesarean section: a choice of three techniques. Br J Hosp Med (Lond) 2009, 70(10):605.
10. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, Domino KB: The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004, 99(3):833-839, table of contents. 490
11. Shaygannejad V, Janghorbani M, Ashtari F, Zanjani HA, Zakizade N: Effects of rivastigmine on memory and cognition in multiple sclerosis. Can J Neurol Sci 2008, 35(4):476-481.
12. Myles PS, Leslie K, McNeil J, Forbes A, Chan MT: Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004, 363(9423):1757-1763.
13. Elhakim M, Abdelhamid D, Abdelfattach H, Magdy H, Elsayed A, Elshafei M: Effect of epidural 495 dexmedetomidine on intraoperative awareness and post-operative pain after one-lung ventilation. Acta Anaesthesiol Scand 2010, 54(6):703-709.
14. Sneyd JR, Mathews DM: Memory and awareness during anaesthesia. Br J Anaesth 2008, 100(6):742-744.
15. Brice DD, Hetherington RR, Utting JE: A simple study of awareness and dreaming during 500 anaesthesia. Br J Anaesth 1970, 42(6):535-542.
16. Moerman N, Bonke B, Oosting J: Awareness and recall during general anesthesia. Facts and feelings. Anesthesiology 1993, 79(3):454-464.
17. Campagna JA, Miller KW, Forman SA: Mechanisms of actions of inhaled anesthetics. The New England journal of medicine 2003, 348(21):2110-2124. 505
18. Bruhn J, Myles PS, Sneyd R, Struys MM: Depth of anaesthesia monitoring: what's available, what's validated and what's next? British journal of anaesthesia 2006, 97(1):85-94.
19. Ghoneim MM: Awareness during anesthesia. Anesthesiology 2000, 92(2):597-602. 20. Guler T: İntraoperatif Uyanıklık. Türk Anesteziyoloji ve Reanimasyon Derneği Dergisi 2009,
37(5):265-279. 510

Page 17 / 50
JournalAgent powered by LookUs
21. Kino A KR, Wakamatsu T, Hashiguchi M, Nakamura K: Awareness during anesthesia with sevoflurane: a case report. Masui The Japanese journal of anesthesiology 2006, 55(10):1250-1252.
22. Kino A NK: Awareness during general anesthesia for head and neck surgery--a case report. Masui The Japanese journal of anesthesiology 2011, 60(2):241-243.
23. Paech MJ, Scott KL, Clavisi O, Chua S, McDonnell N, Group AT: A prospective study of awareness 515 and recall associated with general anaesthesia for caesarean section. International journal of obstetric anesthesia 2008, 17(4):298-303.
24. Lee DH, Kwon IC: Magnesium sulphate has beneficial effects as an adjuvant during general anaesthesia for Caesarean section. Br J Anaesth 2009, 103(6):861-866.
25. Samarkandi AH: The bispectral index system in pediatrics--is it related to the end-tidal 520 concentration of inhalation anesthetics? Middle East J Anesthesiol 2006, 18(4):769-778.
26. Jellish WS, Owen K, Edelstein S, Fluder E, Leonetti JP: Standard anesthetic technique for middle ear surgical procedures: a comparison of desflurane and sevoflurane. Otolaryngol Head Neck Surg 2005, 133(2):269-274.
27. Miranda HF, Bustamante D, Kramer V, Pelissier T, Saavedra H, Paeile C, Fernandez E, Pinardi G: 525 Antinociceptive effects of Ca2+ channel blockers. Eur J Pharmacol 1992, 217(2-3):137-141.
28. Gupta SD, Mitra K, Mukherjee M, Roy S, Sarkar A, Kundu S, Goswami A, Sarkar UN, Sanki P, Mitra R: Effect of magnesium infusion on thoracic epidural analgesia. Saudi journal of anaesthesia 2011, 5(1):55-61.
29. Mireskandari SM, Pestei K, Hajipour A, Jafarzadeh A, Samadi S, Nabavian O: Effects of preoperative 530 magnesium sulphate on post-cesarean pain, a placebo controlled double blind study. Journal of family & reproductive health 2015, 9(1):29-33.
30. Frassanito L, Messina A, Vergari A, Colombo D, Chierichini A, Della Corte F, Navalesi P, Antonelli M: Intravenous infusion of magnesium sulfate and postoperative analgesia in total knee arthroplasty. Minerva anestesiologica 2015, 81(11):1184-1191. 535
31. Yadav M CN, Gopinath R: Effect of magnesium sulfate nebulization on the incidence of
postoperative sore throat. Journal of anaesthesiology, clinical pharmacology 2016, 32(2):168-171.
540

Page 18 / 50
JournalAgent powered by LookUs
Tablolar Tables
Kayıt Tarihi: 03.10.2017 03:46:58
545 TABLES:
Table 1. Patient and Surgery Characteristics:
*Sevo: sevoflurane, des: desflurane, mg: magnesium sulphate
The patient characteristics and surgery characteristics were similar in each group. 550
555
560
565
570 Table 2. BIS Values at Different Time-Points Amoung Groups
BIS Sevo Des Sevo+Mg Des+Mg p
BIS 0 95.9±2.76 95.2±3.05 95.3±2.88 96.28±2.4 0.504
BIS 5 50.8±7.8 45.96±6.5 39.2±5.5 35.96±5.1 < 0.001
Sevo Sevo + Mg Des Des + Mg p
Age (Year) 29.7 ± 5.1 30.2 ± 5.8 30.2 ± 4.3 29.7 ± 4.78 0.976
Weight (kg) 73.4 ± 14.7 77.5 ± 11.8 79.9 ± 14.7 77.1 ± 14 0.415
Operation time
(min)
47.4 ± 11.19 44.8 ± 7.96 47.6 ± 10.7 41.4 ± 9.6 0.103

Page 19 / 50
JournalAgent powered by LookUs
BIS Med 55.6±6.08 52.6±7.1 40.9±7.4 41.1±9.78 < 0.001
BIS End 64.8±7.5 62.88±4.5 53.0±8.2 50.88±8.3 < 0.001
BIS: bispectral index score, sevo: sevoflurane, des: desflurane, mg: magnesium sulphate,
BIS 0: BIS value before induction, BIS 5: BIS value 5 minutes after induction,
BIS Med: BIS value at the medium point of operation, BIS End: BIS value at the end of the 575
operation
580
585
590
595
600
Table 3. Hemodynamic Parameters Amoung Groups

Page 20 / 50
JournalAgent powered by LookUs
HR
Sevo
Des
Sevo+M
g
Des+Mg
P
MAP
Sevo
Des Sevo+Mg Des+Mg P
0.Min 102 ±17.1 97.3±19.7 106±16.6 106.4±13.8 0.222 98±13.8 92.3±11.5 91.3±71. 91.4±14.8 0.165
5.Min 113.8±14 106±18.3
111.4±12.9 108.7±11.2 0.297 92.3±16.5 86.9±13 84.9±12 86.1±13.4 0.259
Med 91.5±14.4 88±16.9 96.7±18.3 89.2±13.4 0.229 83.8±12.9 83.2±10.6 84.9±12.5 83.2±14.5 0.962
End 93.8±14.8 89.9±16.4 96.4±14.1 89.2±10.2 0.257 88.1±15.6 82.8±11.6 83.4±12.5 85±12.3 0.486
HR: Heart Rate, MAP: Mean arterial pressure 605
610
615
620

Page 21 / 50
JournalAgent powered by LookUs
Table 4. TOF Values at Different Time-Points Amoung Groups
625 Sevo: sevoflurane, des: desflurane, mg: magnesium sulphate, TOF: Train of four TOF 5: TOF value 5 min after induction, TOF 10: TOF value 10 minutes after induction
TOF Med: TOF value at the medium point of operation, TOF End: TOF value at the end of the operation
630
635
640
TOF Sevo Des Sevo+Mg Des+Mg p
TOF 5 2.5±1.6 1.7±1.7 0.5±0.8 1±1.5 < 0.01
TOF 10 2.3±1.2 1.5±1.4
0.3±0.6 0.6±0.7 0.024
TOF Med 2.4±1.1 2.3±1.2 0.7±0.7 0.8±0.8 0.036
TOF End 3.8±0.4 3.9±0.2 2.8±1.1 2.5±1.2 0.01

Page 22 / 50
JournalAgent powered by LookUs
645
Table 5. VAS Scores at Different Time Points Amoung Groups
Sevo: sevoflurane, des: desflurane, mg: magnesium sulphate, SD: standart deviation, VAS1: VAS
score at postoperative first hour, VAS2: VAS score at postoperative second hour, VAS24: VAS score 650
at postoperative 24th hour
655
660
665
VAS Sevo Des Sevo+Mg Des+Mg p
VAS 1 8.1±0.9 8.1±0.8 7.1±0.6 7.1±0.6 < 0.01
VAS 2 5.1±0.6 4.8±0.8
3.5±0.6 3.5±0.6 0.024
VAS 24 4.0±0.6 3.8±0.7 3.0±0.6 03±0.4 0.036

Page 23 / 50
JournalAgent powered by LookUs
Table 6. Dreaming Amoung Groups At the End of the First Month
Dream Sevo Des Sevo+Mg Des+Mg p
Yes 1 2 0 1 0.9
No 24 23 25 4
670
675
680

Page 24 / 50
JournalAgent powered by LookUs
Resimler Figures
Kayıt Tarihi: 03.10.2017 03:47:38 685
Figure 1. BIS Values Measured in Different Time Points Among the Groups
Sevo; sevoflurane, des; desflurane, mg; magnesium sulphate, BIS; bispectral index 690
Page 25 / 50
JournalAgent powered by LookUs
Revizyon Notu Response
Kayıt Tarihi: 03.10.2017 03:49:00 695
RESPONSE TO THE REVIEWER COMMENTS:
Reviewer 1. 700
Comment 1. “Sample size may not be enough for this kind of study. Power analysis of the study should be
included in statistical analysis section. “
Answer 1. Sample size is not enough to detect an awareness case, but in the current study power analysis
was calculated to obtain a significant difference in BIS values between control and study groups. 705
The title of the study is changed and the following part is inserted to the statistical analysis:
“Calculation of sample size was based on previous investigations conducted about the effects of Mg
sulphate on BIS values and propofol consumption. Assuming α error = 0.05 (two-tailed) and β
error = 0.1. sample size of totally 45 patients, allocated into one group, will have a power of 90 % 710
to determine an assumed clinically significant difference of 5 % (effect size d = 0.6) between the
paired measurements of BIS value in groups with and without magnesium infusion. The sample size
was calculated using Power Analysis and Sample Size 12 software (NCSS, Kaysville, UT, USA).
Comment 2. “Statistical significances (as * P values) must be included in tables and on figures.” 715
Answer 2. All of the tables are revised with “p” values.
Comment 3. “ Conclusion paragraph must be revised.”
720
Answer 3. Conclusion paragraph is revised as below:
“In this study, magnesium infusion provided significantly lower intraoperative BIS values and
lower postoperative VAS scores. We believe that magnesium can be useful as an adjuvant to general
anesthesia in cesarean section patients. Larger number of sample size is needed to properly assess 725
awareness under general anesthesia. “

Page 26 / 50
JournalAgent powered by LookUs
730
Reviewer 2.
Comment 1. “Power analysis? There are multiple endpoints but no power analysis. The proper
power analysis should be made for the main endpoints of this study.” 735
Answer 1. The power analysis of the study was calculated to obtaine a significant difference in BIS values
between control and study groups.
The primary end point of the study is changed and the following part is added to the statistical analysis:
“Calculation of sample size was based on previous investigations conducted about the effects of Mg 740
sulphate on BIS values and propofol consumption. Assuming α error = 0.05 (two-tailed) and β
error = 0.1. sample size of totally 45 patients, allocated into one group, will have a power of 90 %
to determine an assumed clinically significant difference of 5 % (effect size d = 0.6) between the
paired measurements of BIS value in groups with and without magnesium infusion. The sample size
was calculated using Power Analysis and Sample Size 12 software (NCSS, Kaysville, UT, USA). 745
Comment 2. “Did MgSO4 administration lead to significant changes in the hemodynamic status
between groups?”
Answer 2. In our study magnesium sulphate had no significant effect between groups, so we didn’t 750
need to mention it in the text. But after the reviewer’s comment, we added the following sentence
and related table into the results section:
“There was no significant difference at MAP and heart rate between the groups throughout the
operation ( p > 0.05) (Table 3).”
755
Comment 3. “Was there any significant difference in duration of emergence, recovery and PACU
stay between groups?”
Answer 3. Regarding the TOF values, we inserted the following part and related table into the
result section: 760
“At all time points, TOF values of group S and D were found to be higher than study groups. There
was no significant difference between the groups S-M and D-M or between control groups at any
time-point (Table 4).”

Page 27 / 50
JournalAgent powered by LookUs
Unfortunatelly duration of emergence and recovery was not an end point of our study and we didn’t 765
collect data.
Comment 4. “ Mean VAS scores were above 4 in almost all patients until 1 hour after operations.
Ethically, the aim of postoperative analgesia should be keeping the pain scores below 3-4.
Additionally, there is no comment about the amount of the rescue analgesic. Did all the patients
receive only diclofenac 75 mg?” 770
Answer 4. Dear reviewer, VAS1 is the pain score of patients at the first evaluation. The rescue
analgesic (first step diclofenac 75 mg im, second step tramadol 1 mg/kg iv) was added at the end of
this first evaluation. So, VAS values were significantly lower in the second hour. The following
sentence is inserted into the methodology part: “For postoperative analgesia, 1000 mg paracetamol 775
was applied intravenously 15 minutes before the end of the surgery and 75 mg diclofenac sodium
was applied at every 8 hours in the ward. When Visual Analogue Scale (VAS) scores were 4 or
more, tramadol 1 mg kg ֿ ¹ i.v was applied as rescue analgesic.”
Although the data about resque analgesic was recorded, no significant difference was found. So, we
didn’t mention it in the text. 780
Comment 5. “Table 1: Is the duration of operation in Des+Mg Group 4,4±9,6 minutes (I think
44±9,6)
Answer 5. All of the tables are revised. The correct duration is 41.4 ±9.6 minutes.
785
Comment 6. “I wonder if all the patients in Table 4 received only a single dose fentanyl. If not, the
dose of fentanyl requirement between groups will be more important (may be significant).”
Answer 6. When needed, fentanyl was administered as 1 mcg/kg iv to very patients. As there was
no significant difference between groups, we deleted the part about intraoperative analgesic 790
requirements and the related table.
Comment 7. “The authors should discuss their results in terms of fentanyl consumption,
hemodynamic status, emergence-recovery time and postoperative analgesia with the recent studies
in which similar methodology used in adult patients underwent caesarean section under general 795
anaesthesia.”

Page 28 / 50
JournalAgent powered by LookUs
Answer 7. We dicussed fentanyl consumption and postoperative analgesia with some of the refered
studies. Some of the old references are replaced with latest ones.
800
Reviewer 3:
805
Comment 1. “I think that the sentence in P5 L 135 '' 3) Do you remember anything in
between?.''may be little confused. The sentence can be made more clear.”
Answer 1. Dear Editor, this sentence is a part of “Modified Brice interviews” which is still accepted
as the gold-standart for postoperative awareness screening. We didn’t make any difference in the 810
original questionarre.
Comment 2. “It would be better to add a table for awareness results.”
Answer 1. A table about dreaming insidence amoung groups is added to the Results section (Table 815
6). None of the patients could remember any words from Wechsler Memory Scale, so we didn’t
make any tables about that data.
Comment 3. “Why cesarean patients were evaluated for study? Does the gynecology clinic have an
indication for the use of magnesium?” 820
Answer 3. Both in the “Introduction” and “Discussion” sections, we tried to mention the
importance of obstetric surgery for awareness:
“As low doses of general anaesthetic agents have traditionally been used in caesarean sections, 825
obstetric patients are reported to have a higher incidence of intraoperative awareness than other
surgical patients, especially during the period before delivery [10].”
“Awareness under general anesthesia is a rare complication seen between 0.1%-0.2% of all patients
[6]. However, some publications reported that these numbers can rise upto 7-28% in obstetric
surgeries [6, 23].” 830
Although in obstetric intensive care, magnesium represents a first-choice medication in the

Page 29 / 50
JournalAgent powered by LookUs
treatment and prevention of eclamptic seizures, we didn’t allocate eclamptic patients into the
study.
Comment 4. “The sentence in P9 L 215; '' We believe that magnesium infusion in cesarean section
can be useful by reducing patients’ inoperative anesthetic and postoperative analgesic need and 835
prevent depressant effects on fetus.'' But, there is no clinical result about the fetus at article. How
accurate can be your result? If you have data with the fetus, you should add.”
Answer 4. The comment regarding the fetus is deleted from the text. Conclusion paragraph is
revised as below: 840
“In this study, magnesium infusion provided significantly lower intraoperative BIS values and
lower postoperative VAS scores. We believe that magnesium can be useful as an adjuvant to general
anesthesia in cesarean section patients. Larger number of sample size is needed to properly assess
awareness under general anesthesia. “ 845
850

Page 30 / 50
JournalAgent powered by LookUs
Original Files Tam Metin
Main TEXT awareness Kayıt Tarihi: 09.09.2016 11:15:12 855
INTRODUCTION
The term “awareness” under anesthesia is used in literature as the wakening of brain by a stimulant 860
under general anesthesia and storing this information in order to recall it in the future (1). Although
most of the patients experienced awareness may seem to have no complaint in the long time period
postoperatively (2), symptoms like nightmares, daytime anxiety and flashbacks can be seen and in
some cases, even patients may develop posttraumatic stress disorder (2, 3).
Over the last 20 years, there has been a large increase in the proportion of caesarean section 865
performed under regional anaesthesia. But in emergency situations, when there is a contraindication
for regional anesthesia or in the situation of patient’s refusal, general anesthesia is applied (4).
Therefore general anesthesia is still frequently prefered in some clinics.
Low concentrations of anaesthetic agents until delivery have traditionally been used for caesarean
section under general anesthesia to prevent uterine atony and neonatal respiratory depression. As a 870
result, obstetric patients have a higher incidence of intraoperative awareness than other surgical
patients, especially during the period before delivery (5).
Over the recent years, magnesium has been widely used in anesthesia management. It was reported
to regulate cardiovascular response by reducing cathecolamin release associated with tracheal
intubation, block acetylcholine discharge from neuromuscular junction and potentiate the effect of 875
non-depolarizing neuromuscular blockers (6). Recently magnesium sulphate was reported to reduce
anaesthetic requirements and shorten anaesthetic induction with propofol (7-9). It has potential
analgesic and sedative properties, therefore it may be used as adjuvant during general anesthesia
(10).
In this study our primary hypothesis was magnesium infusion has positive effects on awareness 880
under general anesthesia. Our secondary hypothesis was magnesium infusion can reduce pain at

Page 31 / 50
JournalAgent powered by LookUs
both intraoperative and postoperative period.
MATERIAL AND METHOD
After receiving hospital Clinical Trials Local Ethic Committee approval (reference Number: LUT-
10/60) and patients’ informed consent, 100 patients (American society of anesthesiologists status I-885
II and between 17-41 years old) undergoing cesarean section with general anesthesia were included
in the study. The study was conducted in accordance with the Helsinki declaration in Ankara
Hacettepe University Hospital between 2010-2011 and patient follow-up has been continued untill
2016 via phone calls. Patients with known history of magnesium sulphate hypersensivity,
hypermagnesemia, any degree of heart block, hypertension, diabetus mellitus, preterm or multiple 890
pregnancy, preoperative fetal distress or other medical conditions were excluded from the study. In
the operating room, electrocardiogram, non invasive blood pressure, peripheral oxygen saturation,
train of four (Datex-Ohmeda N-NMT Sensors) and bispectral index scoring (BIS) (Datex-Ohmeda
S/5TM) measurements were monitored. Patients were randomized into four groups by using a
computer-generated randomization schedule and each group included 25 patients. The study drug 895
solutions were prepared into 20-mL identical syringes for bolus doses and 500-mL serum
physiologic solutions for intraoperative infusions and labeled by an anesthetist who did not
participate in the study. The investigators and patients were blinded to group allocation. The first
and the second groups were planed to receive sevoflurane and desflurane as inhalation anesthetic
agent respectively. They were planed to receive serum physiologic in 20-mL syringes and serum 900
physiologic as infusion solution (Group S and D). In the third and fourth groups, patients were
planed to receive sevoflurane and desflurane as inhalation anesthetic agent respectively. They were
planed to receive 30 mg kg ֿ ֿ ¹ magnesium sulfate in 20-mL syringes and magnesium sulfate plus
serum physiologic as infusion solution (Group S-M and D-M).
Induction was performed with 2-3 mg kg ֿ ¹ i.v propofol and 0.6 mg kg ֿ ֿ i.v rocronium bromide in 905
all groups. After induction, in groups S-M and D-M, 30 mg kg ֿ ¹ i.v magnesium sulfate was
applied as bolus in 15-20 seconds and then 10 mg kg ֿ ֿ hour ֿ ¹ magnesium sulfate infusion in 500-

Page 32 / 50
JournalAgent powered by LookUs
mL serum physiologic solution was started.
At the maintenance of anesthesia 2% end-tidal sevoflurane and 4 lt min ֿ ֿ ֿ ¹ 40% O2-60% N2O
were used in group S and group S-M, and 6% end-tidal desflurane and 4 lt min ֿ ¹ 40% O2-60% 910
N2O were used in group D and group D-M. When heart rate or blood pressure increased more than
20% of baseline values, fentanyl 1 mcg kg ֿ ֿ ¹ was applied intravenously while minimum alveolar
concentration (MAC) remained constant. In all groups BIS values were recorded before induction,
right after induction and at five minute intervals throughout the operation. Intraoperative opioid
need was recorded following induction and throughout the operation. For postoperative analgesia, 915
1000 mg paracetamol was applied intravenously 15 minutes before the end of the surgery and 75
mg diclofenac sodium was applied at every 8 hours as rescue analgesic in the ward. Patients were
evaluated at the postoperative 1st , 2nd and 24th hours via Visual Analogue Scale (VAS).
Following anesthesia induction, a text chosen with the consultancy of Hacettepe University Medical
Faculty Psychiatry Department was listened to all patients via earphones. This text was a story 920
included in the “Wechsler Memory Scale” used for neurophysiological examination of the patients
and there were 24 key words in this single line text (11).
Similar to previous studies (12, 13), all patients were questioned about awareness under general
anesthesia at postoperative 1st, 6th, 24th hours, at the end of the 1st month by the same anesthesiogist.
As an addition to previous studies, we interviewed with the patients at the end of the first, second, 925
third, fourth and fifth year in order to evaluate long term effects of general anesthesia. First all
patients were given some clues about the story and then they were asked whether if they recalled
anything about the text or not. Besides Wechsler Memory Scale, questions from “Modified Brice
interviews” which is still accepted as the gold-standart for postoperative awareness screening were
also asked (14). The interview is consisted of five simple questions which were first defined by 930
Brice et al. (15) and then modified by Moerman et al. (16). These questions are listed as – “1) What
is the last thing you remember before sleeping? 2) What is the first thing you remember at awaking
after the surgery? 3) Do you remember anything in between? 4) Did you see any dreams? 5) What

Page 33 / 50
JournalAgent powered by LookUs
was the most disturbing thing you remember about the operation and anesthesia?.
STATISTICAL ANALYSIS 935
The statistical anaylsis was made by using the Statistical Package for Social Science, version 17.0
(SPSS Inc., Chicago, IL). All demographic datas and perioperative periods were evaluated with One
Way Variance Analysis. Turkey-HSD test was used for the multiple comparison between groups.
For evaluation of VAS values non-parametric Kruskal-Wallis test was performed. Exact chi-square
test was used to compare additional analgesic need, dreaming, remembering and recalling the story. 940
“P < 0,05” was accepted as statistically significant and all datas was defined as “mean±SD”.
RESULTS
A hundred and twenty patients were included into the study. Two of the patients excluded due to
intraoperative allergic symptoms. Six patients declined to participitate in the study postoperatively
and twelve patients excluded from the study due to intraoperative faults. The characteristics of 100 945
patients and surgery characteristics were similar in each group (Table 1). There was no significant
difference in the frequency of comorbidities between groups.
For analysis of BIS values, before induction (BIS 0), 5 minutes after the induction (BIS 5), total
operation median time (BIS Median) and end of operation (BIS End) time-points were chosen
(Table 2). 950
BIS values before the induction were similar in all groups (p > 0.05) whereas BIS values at BIS 5 is
significantly higher in the sevoflurane group (p < 0.001) (Figure 1). At the BIS Median point; BIS
values in Group S and Group D are similar to each other and statistically significantly higher than
the groups with magnesium infusion ( p < 0.001) (Figure 2). Likewise when BIS End values are
observed; Group S and Groups D were found to be similar to each other and significantly higher 955
than magnesium groups ( p < 0.001). There was no statistically significant difference amoung
magnesium groups ( p > 0.05). (Figure 3). BIS value ranges measured throughout the operation is
shown in Figure 4.
VAS scores were questioned at 1st, 2nd and 24th hour. VAS scores in all time points were

Page 34 / 50
JournalAgent powered by LookUs
significantly lower in magnesium groups (p < 0.05). VAS scores of group S and D were similar, 960
while groups S-M and D-M were similar to each other (Table 3).
Although intraoperative additional analgesic requirement was higher in non-magnesium groups, the
difference was not statistically significant (p = 0.307) (Table 4).
At the interviews performed at the end of 1st, 6th and 24th hour, one patient in groups S, two in group
D and one in group D-M were found to dream intraoperatively. They stated that their dreams were 965
not related to their surgeries. At the end of the first month, same four patients reported that they
dreamed intraoperatively but couldn’t remember anything about their dreams. This difference
amoung groups was not statistically significant (p > 0.05).
At the end of the first and second years we managed to interview with all patients and non of them
could remember anything new. At the end of the third, fouth and fifth years we couldn’t contact 970
with two patients in group S and three patients in each group S-M and group D-M. None of the
patients reported to hear any sound during the operation nor remember anything. None of the
patients could give a significant answer to the questions of Modified Brice interviews by means of
intraoperative awareness. Likewise, none of the patients could remember the story played through
earphones, or find any of the key words. None of the patients had any signs of posttraumatic stres 975
disorder meanwhile.
DISCUSSION
Our primary hypothesis was magnesium infusion has positive effects on awareness under general
anesthesia. We aimed to assess this effect by BIS measurements and postoperative interviews. In the
present study none of the patients had awareness under general anesthesia, while BIS scores were 980
significantly lower in groups with magnesium infusion.
Our secondary hypothesis was magnesium infusion can reduce pain at both intraoperative and
postoperative period. Although intraoperative opioid need was similar in all groups, VAS scores
were significantly lower in groups with magnesium infusion.
Awareness under general anesthesia is often experienced due to inadequate levels of anesthesia 985

Page 35 / 50
JournalAgent powered by LookUs
(17). It’s been reported in the literature that serious psycological problems which leads to
posttraumatic stress disorder may occur during long-term follow up of these patients (1). Today
intraoperative awareness is mostly observed when opioids and benzodiazepines or weak anesthetics
like nitrous oxide are used seperately or together. Contrary to this, inhalation anesthethics like
sevoflurane, desflurane, isoflurane and potent intravenous anesthetics used in proper concentrations 990
are believed to prevent intraoperative perception succesfully (18). However, there are plenty of
intraopertive awareness cases experienced with inhalation anesthetics in the literature (19, 20). In
the light of these informations, we suggest that adding an adjuvant agent to general anesthesia may
help preventing intraoperative awareness. In this study, we prefered to add magnesium infusion to
general anesthesia provided by sevoflurane or desflurane anesthetics and none of our patients 995
experienced awareness. Dreaming which is believed to be related with awareness was detected at
four patients but when we compared the groups by means of dreaming, there was no statistically
significant difference. Awareness under general anesthesia is a rare complication seen between
0.1%-0.2% of all patients (1). Some publications show that these numbers can rise upto 7-28% in
obstetric surgeries (1, 21, 22). Although the current study was held with obstetric patients, no one 1000
reported to experience awareness. The most likely reason is our sample size may lack to detect an
awareness case. Secondly constant and reasonable MAC values may prevent to see awareness under
general anesthesia.
In the study of Lee et al, different dosages of magnesium were compared with control group and it
was shown that BIS values were significantly lower in the groups with magnesium infusion (23). In 1005
the current study, BIS values were also significantly lower in the groups with magnesium infusion
througout the operation. This result supports our suggestion about magnesium being a good
advujant for general anesthesia. Beside this, BIS values of the groups with magnesium infusion
didn’t differ significantly. This brings the idea that magnesium may deepen the level of anesthesia
with regardless of type of inhalated anesthetic agent. On the other hand, when we look at the non-1010
magnesium groups; BIS values in the 5th minute after induction was higher in sevolfurane group

Page 36 / 50
JournalAgent powered by LookUs
than desflurane group. According to previous studies performed with similar inhalation anesthetics,
this difference between sevoflurane and desflurane is not suprising. It is known that different
inhalation anesthetics given at the end-tidal concentration levels providing same potency can result
in different BIS values of patients (24). Jellish et al. compared sevoflurane and desflurane effects 1015
and reported that BIS values were significantly lower in the desflurane group (25).
The analgesic effect mechanism of magnesium sulfate has not been shown clearly yet, but
inhibition of calcium channels and N-methyl-D-aspartate receptors are believed to have an
important role (26). In previous studies, bolus dosage of magnesium was shown to reduce
postoperative pain scores and additional analgesic need significantly (27, 28). Whereas, in 2001 Ko 1020
et al. reported that magnesium had no effect on postoperative pain in their study. They claimed that
even in increased serum concentrations, magnesium slightly passes the blood-brain barrier, so
intravenous magnesium has minimal effect on postoperative pain (29). In the current study, contrary
to Ko et al. we found VAS scores of magnesium groups were significantly lower at all time points.
Nowadays magnesium is in the focus of studies analyzing post operative inflammation. It was 1025
recently reported to reduce postoperative sore throat significantly (30).
The major limitation of our study is the relatively small sample size. In order to get more objective
data on awareness under general anesthesia, it’s necessary to perform studies with larger number of
patients but nowadays it’s becoming harder due to increased ratios of regional anesthesia at
cesarean sections. 1030
CONCLUSION
In this study, although magnesium infusion didn’t make a significant difference on awareness under
general anesthesia, it provided lower intraoperative BIS and postoperative VAS values. Therefore,
we believe that magnesium infusion in cesarean section can be useful by reducing patients’ 1035
inoperative anesthetic and postoperative analgesic need and prevent depressant effects on fetus.

Page 37 / 50
JournalAgent powered by LookUs
1040
REFERENCES
1. Ghoneim MM, Block RI, Haffarnan M, Mathews MJ. Awareness during anesthesia: risk 1045
factors, causes and sequelae: a review of reported cases in the literature. Anesth Analg. 2009 Feb;108(2):527-35. PubMed PMID: 19151283. Epub 2009/01/20. eng.
2. Lopez U, Habre W, Van der Linden M, Iselin-Chaves IA. Intra-operative awareness in children and post-traumatic stress disorder. Anaesthesia. 2008 May;63(5):474-81. PubMed PMID:
18412644. Epub 2008/04/17. eng. 1050
3. Osterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk BA. Awareness under anesthesia and the development of posttraumatic stress disorder. Gen Hosp Psychiatry. 2001 Jul-Aug;23(4):198-204. PubMed PMID: 11543846. Epub 2001/09/07. eng. 4. Campbell J, Sultan P. Regional anaesthesia for caesarean section: a choice of three techniques. Br J Hosp Med (Lond). 2009 Oct;70(10):605. PubMed PMID: 19966715. 1055
5. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, et al. The incidence of
awareness during anesthesia: a multicenter United States study. Anesth Analg. 2004 Sep;99(3):833-9, table of contents. PubMed PMID: 15333419. Epub 2004/08/31. eng.
6. James MF, Beer RE, Esser JD. Intravenous magnesium sulfate inhibits catecholamine release associated with tracheal intubation. Anesthesia and analgesia. 1989 Jun;68(6):772-6. PubMed 1060
PMID: 2735543. 7. Gupta K, Vohra V, Sood J. The role of magnesium as an adjuvant during general anaesthesia.
Anaesthesia. 2006 Nov;61(11):1058-63. PubMed PMID: 17042843. Epub 2006/10/18. eng. 8. Altan A, Turgut N, Yildiz F, Turkmen A, Ustun H. Effects of magnesium sulphate and
clonidine on propofol consumption, haemodynamics and postoperative recovery. Br J Anaesth. 1065
2005 Apr;94(4):438-41. PubMed PMID: 15653705. Epub 2005/01/18. eng.
9. Telci L, Esen F, Akcora D, Erden T, Canbolat AT, Akpir K. Evaluation of effects of magnesium sulphate in reducing intraoperative anaesthetic requirements. Br J Anaesth. 2002 Oct;89(4):594-8. PubMed PMID: 12393361. Epub 2002/10/24. eng. 10. Barbosa FT, Barbosa LT, Juca MJ, Cunha RM. Applications of magnesium sulfate in obstetrics 1070
and anesthesia. Rev Bras Anestesiol. 2010 Jan-Feb;60(1):104-10. PubMed PMID: 20169270. Epub
2010/02/20. eng por.
11. Shaygannejad V, Janghorbani M, Ashtari F, Zanjani HA, Zakizade N. Effects of rivastigmine on memory and cognition in multiple sclerosis. Can J Neurol Sci. 2008 Sep;35(4):476-81. PubMed 1075
PMID: 18973065. Epub 2008/11/01. eng. 12. Myles PS, Leslie K, McNeil J, Forbes A, Chan MT. Bispectral index monitoring to prevent
awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet. 2004 May 29;363(9423):1757-63. PubMed PMID: 15172773. Epub 2004/06/03. eng.

Page 38 / 50
JournalAgent powered by LookUs
13. Elhakim M, Abdelhamid D, Abdelfattach H, Magdy H, Elsayed A, Elshafei M. Effect of 1080
epidural dexmedetomidine on intraoperative awareness and post-operative pain after one-lung
ventilation. Acta Anaesthesiol Scand. 2010 Jul;54(6):703-9. PubMed PMID: 20085547. Epub 2010/01/21. eng.
14. Sneyd JR, Mathews DM. Memory and awareness during anaesthesia. Br J Anaesth. 2008 Jun;100(6):742-4. PubMed PMID: 18483111. Epub 2008/05/17. eng. 1085
15. Brice DD, Hetherington RR, Utting JE. A simple study of awareness and dreaming during anaesthesia. Br J Anaesth. 1970 Jun;42(6):535-42. PubMed PMID: 5423844. Epub 1970/06/01. eng.
16. Moerman N, Bonke B, Oosting J. Awareness and recall during general anesthesia. Facts and feelings. Anesthesiology. 1993 Sep;79(3):454-64. PubMed PMID: 8363069. Epub 1993/09/01. eng.
17. Ghoneim MM. Awareness during anesthesia. Anesthesiology. 2000 Feb;92(2):597-602. 1090
PubMed PMID: 10691248. Epub 2000/02/26. eng.
18. Guler T. İntraoperatif Uyanıklık. Türk Anesteziyoloji ve Reanimasyon Derneği Dergisi 2009;37(5):265-79. 19. Kino A KR, Wakamatsu T, Hashiguchi M, Nakamura K. Awareness during anesthesia with sevoflurane: a case report. Masui The Japanese journal of anesthesiology. 2006;55(10):1250-2. 1095
20. Kino A NK. Awareness during general anesthesia for head and neck surgery--a case report. Masui The Japanese journal of anesthesiology. 2011;60(2):241-3. 21. Paech MJ, Scott KL, Clavisi O, Chua S, McDonnell N. A prospective study of awareness and recall associated with general anaesthesia for caesarean section. Int J Obstet Anesth. 2008 Oct;17(4):298-303. PubMed PMID: 18617387. Epub 2008/07/12. eng. 1100
22. Crawford JS. Awareness during operative obstetrics under general anaesthesia. Br J Anaesth. 1971 Feb;43(2):179-82. PubMed PMID: 5550849. Epub 1971/02/01. eng.
23. Lee DH, Kwon IC. Magnesium sulphate has beneficial effects as an adjuvant during general anaesthesia for Caesarean section. Br J Anaesth. 2009 Dec;103(6):861-6. PubMed PMID:
19783538. Epub 2009/09/29. eng. 1105
24. Samarkandi AH. The bispectral index system in pediatrics--is it related to the end-tidal
concentration of inhalation anesthetics? Middle East J Anesthesiol. 2006 Feb;18(4):769-78. PubMed PMID: 16749571. Epub 2006/06/06. eng.
25. Jellish WS, Owen K, Edelstein S, Fluder E, Leonetti JP. Standard anesthetic technique for middle ear surgical procedures: a comparison of desflurane and sevoflurane. Otolaryngol Head 1110
Neck Surg. 2005 Aug;133(2):269-74. PubMed PMID: 16087026. Epub 2005/08/10. eng. 26. Miranda HF, Bustamante D, Kramer V, Pelissier T, Saavedra H, Paeile C, et al. Antinociceptive effects of Ca2+ channel blockers. Eur J Pharmacol. 1992 Jul 7;217(2-3):137-41. PubMed PMID: 1425934. Epub 1992/07/07. eng. 27. Gupta SD MK, Mukherjee M, Roy S, Sarkar A, Kundu S, et al. Effect of magnesium infusion 1115
on thoracic epidural analgesia. Saudi journal of anaesthesia. 2011;5(1):55-61. 28. Kiran S GR, Verma D. Evaluation of a single-dose of intravenous magnesium sulphate for prevention of postoperative pain after inguinal surgery. Indian journal of anaesthesia. 2011;55(1):31-5.
29. Ko SH, Lim HR, Kim DC, Han YJ, Choe H, Song HS. Magnesium sulfate does not reduce 1120
postoperative analgesic requirements. Anesthesiology. 2001 Sep;95(3):640-6. PubMed PMID:
11575536. Epub 2001/09/29. eng. 30. Yadav M CN, Gopinath R. Effect of magnesium sulfate nebulization on the incidence of
postoperative sore throat. Journal of anaesthesiology, clinical pharmacology. 2016;32(2):168-71. 1125 There is no conflict of interest.

Page 39 / 50
JournalAgent powered by LookUs
1130
TABLES: 1135
Table 1. Patient and Surgery Characteristics:
*Sevo: sevoflurane, des: desflurane, mg: magnesium sulphate
Table 2. BIS at Different Time-Points Amoung Groups 1140
1145
*BIS: bispectral index score, sevo: sevoflurane, des: desflurane, mg: magnesium sulphate, SD:
standart deviation, BIS Med: BIS at the medium point of operation
Sevo. Sevo + Mg Des. Des + Mg Total
Age (Year) 29.7 ± 5.1 30.2 ± 5.8 30.2 ± 4.3 29.7 ± 4.78 29.97 ± 4.97
Weight (kg) 73.4 ± 14.7 77.5 ± 11.8 79.9 ± 14.7 77.1 ± 14 77.0 ± 13.7
Operation time
(min)
47.4 ± 11.19 44.8 ± 7.96 47.6 ± 10.7 4.4 ± 9.6 45.3 ± 10.1
Group BIS 0 BIS 5 BIS Med BIS End
sevo Mean 95.9 50.8 55.6 64.8
SD 2.76 7.8 6.08 7.5
sevo+mg Mean 95.3 39.2 40.9 53.0
SD 2.88 10.5 7.4 8.2
des Mean 95.2 38.96 52.6 62.88
SD. 3.05 6.5 7.1 4.5
des+mg Mean 96.28 35.96 41.1 50.88
SD 2.4 10.1 9.78 8.3

Page 40 / 50
JournalAgent powered by LookUs
1150
1155
1160
Tablo 3. VAS scores amoung groups
Group VAS1 VAS2 VAS24
sevo Mean 8.16 5.12 4.00
N 25 25 25
SD .898 .666 .6455
des Mean 8.12 4.88 3.80
N 25 25 25
SD .833 .881 .707
sevo+mg Mean 7.16 3.52 3,00
N 25 25 25
SD .624 .653 .645
des+mg Mean 7.12 3.56 3.00
N 25 25 25
SD .600 .651 .408
*Sevo: sevoflurane, des: desflurane, mg: magnesium sulphate, SD: standart deviation, VAS1: VAS
score at postoperative first hour, VAS2: VAS score at postoperative second hour, VAS24: VAS score
at postoperative 24th hour
1165
Table 4. Intraoperative Additional Analgesic Requirement
Group
Total sevo des sevo+mg des+mg
fentanyl yes 15 14 9 11 49
no 10 11 16 14 51
Total 25 25 25 25 100

Page 41 / 50
JournalAgent powered by LookUs
Sevo: sevoflurane, des: desflurane, mg: magnesium sulphate
1170
Figure 1. BIS Values Among Groups at 5 Minutes After the Induction
*sevo; sevoflurane, des; desflurane, mg; magnesium sulphate, BIS; bispectral index, SD; Standard
deviation
Figure 2. BIS Values Among Groups at BIS Median Point 1175
*sevo; sevoflurane, des; desflurane, mg; magnesium sulphate, BIS; bispectral index, SD; Standard
deviation

Page 42 / 50
JournalAgent powered by LookUs
At the BIS Median point; BIS values in Group S and Group D are similar to each other and
statistically significantly higher than the groups with magnesium ( p < 0.001) 1180
Figure 3. BIS Values Among Groups at BIS End Point
*sevo; sevoflurane, des; desflurane, mg; magnesium sulphate, BIS; bispectral index, SD; Standard
deviation
BIS values of group S and group D at the end of the operation were similar to each other and 1185
significantly higher than magnesium groups ( p < 0.001). There was no statistically significant
difference amoung magnesium groups ( p > 0.05)
Figure 4. BIS Values Measured in Different Time Points Among the Groups
1190 Sevo; sevoflurane, des; desflurane, mg; magnesium sulphate, BIS; bispectral index


Page 44 / 50
JournalAgent powered by LookUs
Kaynaklar References
Kayıt Tarihi: 08.09.2016 23:59:36 1195
REFERENCES
1. Ghoneim MM, Block RI, Haffarnan M, Mathews MJ Awareness during anesthesia: risk
factors, causes and sequelae: a review of reported cases in the literature. Anesth Analg 1200
2009, 108(2):527-35.
2. Lopez U, Habre W, Van der Linden M, Iselin-Chaves IA Intra-operative awareness in children and post-traumatic stress disorder. Anaesthesia 2008, 63(5):474-81.
3. Osterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk Awareness under anesthesia and
the development of posttraumatic stress disorder. Gen Hosp Psychiatry 2001, 23(4):198-1205
204.
4. Campbell J, Sultan P Regional anaesthesia for caesarean section: a choice of three techniques. Br J Hosp Med (Lond) 2009, 70(10):605.
5. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, et al. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004, 1210
99(3):833-9 6. James MF, Beer RE, Esser JD Intravenous magnesium sulfate inhibits catecholamine release
associated with tracheal intubation. Anesth analg 1989, 68(6):772-6 7. Gupta K, Vohra V, Sood J The role of magnesium as an adjuvant during general anaesthesia.
Anaesthesia 2006, 61(11):1058-63. 1215
8. Altan A, Turgut N, Yildiz F, Turkmen A, Ustun H Effects of magnesium sulphate and clonidine
on propofol consumption, haemodynamics and postoperative recovery. Br J Anaesth 2005, 94(4):438-41.
9. Telci L, Esen F, Akcora D, Erden T, Canbolat AT, Akpir K Evaluation of effects of magnesium sulphate in reducing intraoperative anaesthetic requirements. Br J Anaesth 2002, 1220
89(4):594-8.
10. Barbosa FT, Barbosa LT, Juca MJ, Cunha RM Applications of magnesium sulfate in obstetrics and anesthesia. Rev Bras Anestesiol 2010, 60(1):104-10.
11. Shaygannejad V, Janghorbani M, Ashtari F, Zanjani HA, Zakizade N Effects of rivastigmine on memory and cognition in multiple sclerosis. Can J Neurol Sci 2008, 35(4):476-81. 1225
12. Myles PS, Leslie K, McNeil J, Forbes A, Chan MT Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004,
363(9423):1757-63. 13. Elhakim M, Abdelhamid D, Abdelfattach H, Magdy H, Elsayed A, Elshafei M Effect of
epidural dexmedetomidine on intraoperative awareness and post-operative pain after one-1230
lung ventilation. Acta Anaesthesiol Scand 2010, 54(6):703-9.
14. Sneyd JR, Mathews DM Memory and awareness during anaesthesia. Br J Anaesth 2008, 100(6):742-4.
15. Brice DD, Hetherington RR, Utting JE A simple study of awareness and dreaming during anaesthesia. Br J Anaesth 1970, 42(6):535-42. 1235
16. Moerman N, Bonke B, Oosting J Awareness and recall during general anesthesia. Facts and feelings. Anesthesiology 1993, 79(3):454-64.
17. Ghoneim MM Awareness during anesthesia. Anesthesiology 2000, 92(2):597-602. 18. Guler T İntraoperatif Uyanıklık. Turk J Anesthesiol Reanim 2009, 37(5):265-79. 19. Kino A KR, Wakamatsu T, Hashiguchi M, Nakamura K Awareness during anesthesia with 1240
sevoflurane: a case report. Masui The Japanese journal of anesthesiology 2006,

Page 45 / 50
JournalAgent powered by LookUs
55(10):1250-52. 20. Kino A NK: Awareness during general anesthesia for head and neck surgery--a case report.
Masui The Japanese journal of anesthesiology 2011, 60(2):241-3. 21. Paech MJ, Scott KL, Clavisi O, Chua S, McDonnell N A prospective study of awareness and 1245
recall associated with general anaesthesia for caesarean section. Int J Obstet Anesth 2008, 17(4):298-303.
22. Crawford JS Awareness during operative obstetrics under general anaesthesia. Br J Anaesth 1971, 43(2):179-82.
23. Lee DH, Kwon IC Magnesium sulphate has beneficial effects as an adjuvant during general 1250
anaesthesia for Caesarean section. Br J Anaesth 2009, 103(6):861-6.
24. Samarkandi AH The bispectral index system in pediatrics--is it related to the end-tidal concentration of inhalation anesthetics? Middle East J Anesthesiol 2006, 18(4):769-78.
25. Jellish WS, Owen K, Edelstein S, Fluder E, Leonetti JP Standard anesthetic technique for middle ear surgical procedures: a comparison of desflurane and sevoflurane. Otolaryngol 1255
Head Neck Surg 2005, 133(2):269-74. 26. Miranda HF, Bustamante D, Kramer V, Pelissier T, Saavedra H, Paeile C, et al. Antinociceptive
effects of Ca2+ channel blockers. Eur J Pharmacol 1992, 217(2-3):137-41. 27. Gupta SD, Mitra K, Mukherjee M, Roy S, Sarkar A, Kundu S, et al.: Effect of magnesium
infusion on thoracic epidural analgesia. Saudi journal of anaesthesia 2011, 5(1):55-61. 1260
28. Kiran S GR, Verma D Evaluation of a single-dose of intravenous magnesium sulphate for prevention of postoperative pain after inguinal surgery. Indian journal of anaesthesia 2011,
55(1):31-5. 29. Ko SH, Lim HR, Kim DC, Han YJ, Choe H, Song HS: Magnesium sulfate does not reduce
postoperative analgesic requirements. Anesthesiology 2001, 95(3):640-6. 1265
30. Yadav M CN, Gopinath R Effect of magnesium sulfate nebulization on the incidence of
postoperative sore throat. Journal of anaesthesiology, clinical pharmacology 2016, 32(2):168-71.
1270

Page 46 / 50
JournalAgent powered by LookUs
Tablolar Tables
Kayıt Tarihi: 09.09.2016 11:15:36
1275
TABLES:
Table 1. Patient and Surgery Characteristics:
*Sevo: sevoflurane, des: desflurane, mg: magnesium sulphate
1280
Table 2. BIS at Different Time-Points Amoung Groups
1285
*BIS: bispectral index score, sevo: sevoflurane, des: desflurane, mg: magnesium sulphate, SD:
standart deviation, BIS Med: BIS at the medium point of operation 1290
1295
1300
Sevo. Sevo + Mg Des. Des + Mg Total
Age (Year) 29.7 ± 5.1 30.2 ± 5.8 30.2 ± 4.3 29.7 ± 4.78 29.97 ± 4.97
Weight (kg) 73.4 ± 14.7 77.5 ± 11.8 79.9 ± 14.7 77.1 ± 14 77.0 ± 13.7
Operation time
(min)
47.4 ± 11.19 44.8 ± 7.96 47.6 ± 10.7 4.4 ± 9.6 45.3 ± 10.1
Group BIS 0 BIS 5 BIS Med BIS End
sevo Mean 95.9 50.8 55.6 64.8
SD 2.76 7.8 6.08 7.5
sevo+mg Mean 95.3 39.2 40.9 53.0
SD 2.88 10.5 7.4 8.2
des Mean 95.2 38.96 52.6 62.88
SD. 3.05 6.5 7.1 4.5
des+mg Mean 96.28 35.96 41.1 50.88
SD 2.4 10.1 9.78 8.3

Page 47 / 50
JournalAgent powered by LookUs
Tablo 3. VAS scores amoung groups
Group VAS1 VAS2 VAS24
sevo Mean 8.16 5.12 4.00
N 25 25 25
SD .898 .666 .6455
des Mean 8.12 4.88 3.80
N 25 25 25
SD .833 .881 .707
sevo+mg Mean 7.16 3.52 3,00
N 25 25 25
SD .624 .653 .645
des+mg Mean 7.12 3.56 3.00
N 25 25 25
SD .600 .651 .408
*Sevo: sevoflurane, des: desflurane, mg: magnesium sulphate, SD: standart deviation, VAS1: VAS
score at postoperative first hour, VAS2: VAS score at postoperative second hour, VAS24: VAS score
at postoperative 24th hour 1305
Table 4. Intraoperative Additional Analgesic Requirement
Group
Total sevo des sevo+mg des+mg
fentanyl yes 15 14 9 11 49
no 10 11 16 14 51
Total 25 25 25 25 100
Sevo: sevoflurane, des: desflurane, mg: magnesium sulphate
1310

Page 48 / 50
JournalAgent powered by LookUs
Resimler Figures
Kayıt Tarihi: 09.09.2016 11:16:01
1315 Figure 1. BIS Values Among Groups at 5 Minutes After the Induction
*sevo; sevoflurane, des; desflurane, mg; magnesium sulphate, BIS; bispectral index, SD; Standard
deviation
Figure 2. BIS Values Among Groups at BIS Median Point 1320
*sevo; sevoflurane, des; desflurane, mg; magnesium sulphate, BIS; bispectral index, SD; Standard
deviation
At the BIS Median point; BIS values in Group S and Group D are similar to each other and
statistically significantly higher than the groups with magnesium ( p < 0.001) 1325
Figure 3. BIS Values Among Groups at BIS End Point

Page 49 / 50
JournalAgent powered by LookUs
*sevo; sevoflurane, des; desflurane, mg; magnesium sulphate, BIS; bispectral index, SD; Standard
deviation
BIS values of group S and group D at the end of the operation were similar to each other and 1330
significantly higher than magnesium groups ( p < 0.001). There was no statistically significant
difference amoung magnesium groups ( p > 0.05)
Figure 4. BIS Values Measured in Different Time Points Among the Groups
1335 Sevo; sevoflurane, des; desflurane, mg; magnesium sulphate, BIS; bispectral index
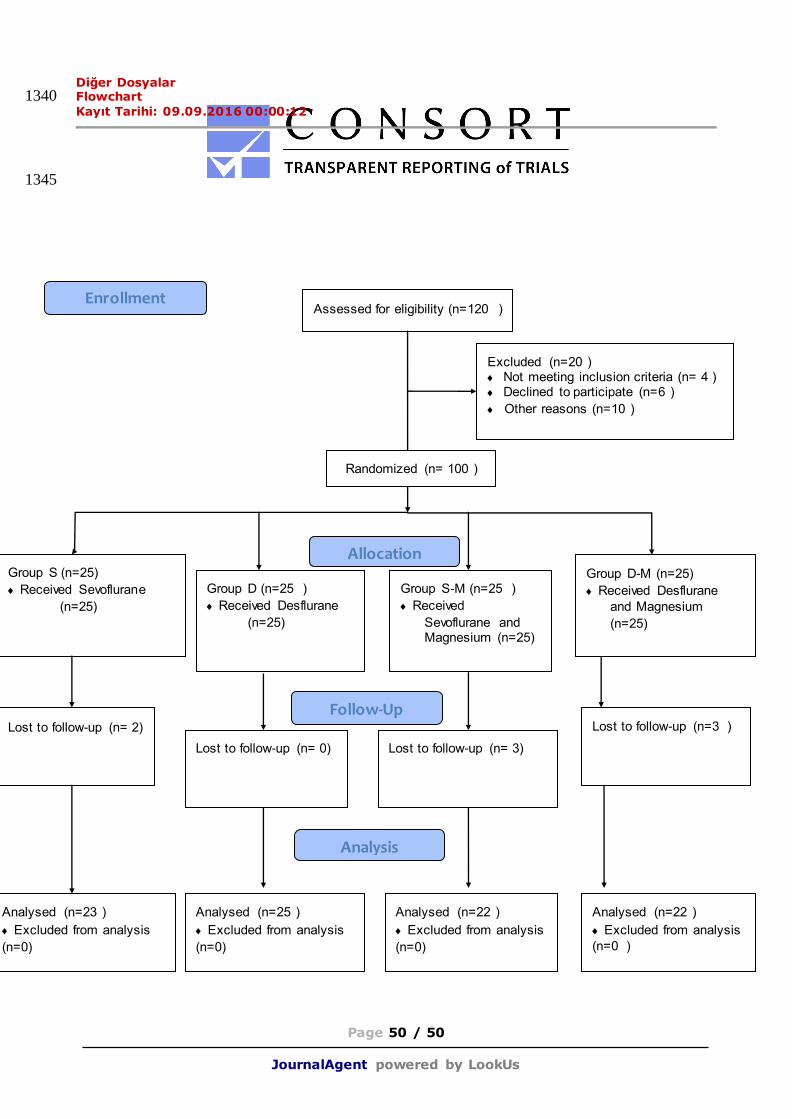
Page 50 / 50
JournalAgent powered by LookUs
Diğer Dosyalar Flowchart 1340 Kayıt Tarihi: 09.09.2016 00:00:12
1345
Assessed for eligibility (n=120 )
Excluded (n=20 ) Not meeting inclusion criteria (n= 4 ) Declined to participate (n=6 )
Other reasons (n=10 )
Analysed (n=23 )
Excluded from analysis
(n=0)
Lost to follow-up (n= 2)
Group S (n=25)
Received Sevoflurane
(n=25)
Lost to follow-up (n=3 )
Group D-M (n=25)
Received Desflurane
and Magnesium
(n=25)
Analysed (n=22 )
Excluded from analysis
(n=0 )
Allocation
Analysis
Follow-Up
Randomized (n= 100 )
Enrollment
Group D (n=25 )
Received Desflurane
(n=25)
Group S-M (n=25 )
Received
Sevoflurane and Magnesium (n=25)
Lost to follow-up (n= 0) Lost to follow-up (n= 3)
Analysed (n=25 )
Excluded from analysis
(n=0)
Analysed (n=22 )
Excluded from analysis
(n=0)