surgery’review:’ surgicalnutrion, fluids’and’electrolytes’ · 2014-05-22 · chloride!...
TRANSCRIPT

Surgery Review: Surgical nutri2on,
Fluids and electrolytes
May 23, 2014

SURGERY BASICS

Essen/als for wound healing 1. Homeostasis
• Normal ECF and ICF • Op/mum balance mechanisms
2. Op/mum cell structure and func/on 3. Adequate energy provision
• Op/mum an/oxidant ac/vity 4. Adequate nutri/on
• Macronutrients • Micronutrients
5. Adequate perfusion 6. Adequate oxygena/on 7. Adequate waste removal

Homeostasis
• Essen/al for op/mum body func/on • Fluids, electrolytes, acids and bases must be balanced
• Balance = a set desired level – More than desired level = increasing excre/on – Below desired level = increasing absorp/on
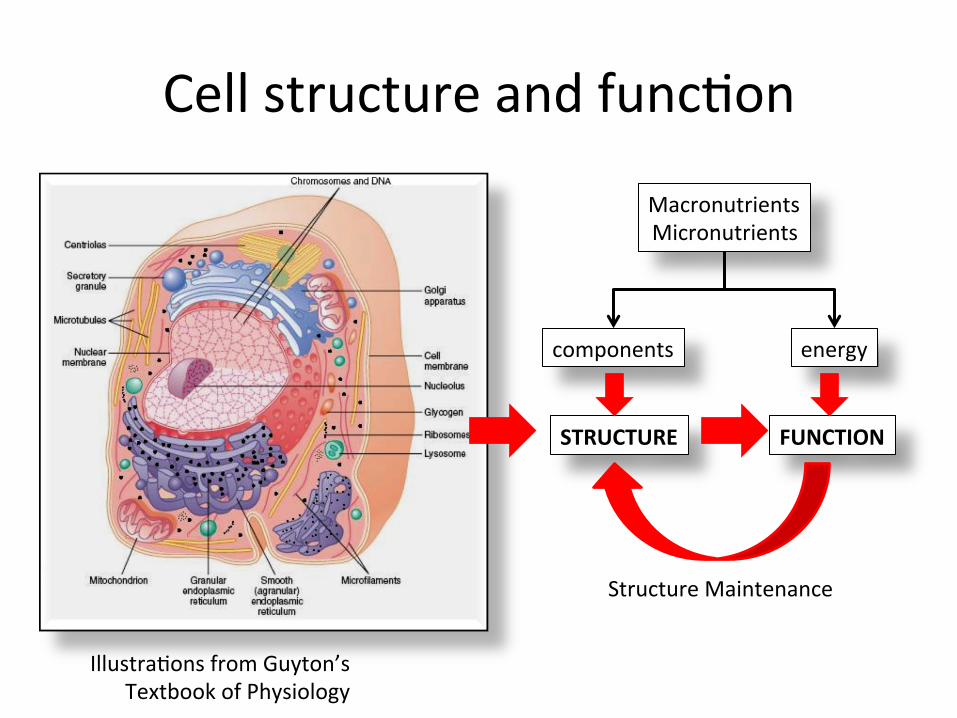
Cell structure and func/on
Illustra/ons from Guyton’s Textbook of Physiology
STRUCTURE FUNCTION
Structure Maintenance
Macronutrients Micronutrients
components energy

The cell: basic components Component Details Water 70% to 85% except in fat cells Ions major → potassium,
magnesium, phosphate, bicarbonate; minor → sodium, chloride and calcium
Protein 20% to 30% of cell mass Structural Func/onal
Lipids (mainly phospholipids and cholesterol): 2% of cell mass
Carbohydrates small part but has major role in metabolism

100 trillion cells
• Nervous system • Musculoskeletal system • Cardiovascular system • Respiratory system • Gastrointes/nal system • Genitourinary system • Reproduc/ve system • Endocrine system • Hemopoie/c system

Body composi/on and water Human body composi/on
(% of weight): • Water: 60%
– ECF (extracellular fluid): 20%
• Intravascular fluid • Extravascular inters/tal fluid
– ICF (intracellular fluid): 40%
• Mass: 40% – Lean body mass – Fat mass
TBF = ICF + ECF = 42 liters (60% of weight)
• ECF = 14 liters – Plasma – Inters//al Fluid
• ICF = 28 liters
• Computa2on of usual fluid requirement per day: – 30 ml/kg – or 1.5 to 2.5 L/day

Normal routes of water gain and loss at room temp (=230C)
Water intake ml/day Water loss ml/day Fluid 1200 Insensible 700 In Food 1000 Sweat 100 Metabolically produced from food
300 Feces 200
Urine 1500 Total 2500 2500
From: Berne R, ed. Physiology 5th ed. St. Louis, Missouri: Mosby 2004: p. 662.

Electrolytes
• Chemicals that can carry an electrical charge • Dissolved in the body fluids • Fluid and electrolyte levels are interdependent – Electrolyte increases, water is added – Electrolyte decreases, water is removed

Posi/ve Ions Electrolyte Extracellular
mEq/L Intracellular
mEq/L Func2on
Sodium 142 10 • Fluid balance • Osmo/c pressure
Potassium 5 100 • Neuromuscular excitability
• Acid base balance Calcium 5 -‐ • Bones
• Blood cloeng Magnesium 2 123 • Enzymes Total 154 205

Nega/ve Ions Electrolyte Extracellular
mEq/L Intracellular
mEq/L Func2on
Chloride 105 2 • Fluid balance • Osmo/c pressure
Bicarbonate 24 8 • Acid base balance Proteins 16 55 • Osmo/c pressure Phosphate 2 149 • Energy storage Sulfate 1 -‐ • Protein
metabolism Total 154 205

Osmolality
• Normal cellular func/on requires normal serum osmolality
• Water homeostasis maintains serum osmolality • The contribu/ng factors to serum osmolality are: Na, glucose, and BUN
• Sodium is the major contributor (accounts for 90% of extracellular osmolality)
• Acute changes in serum osmolality will cause rapid changes in cell volume
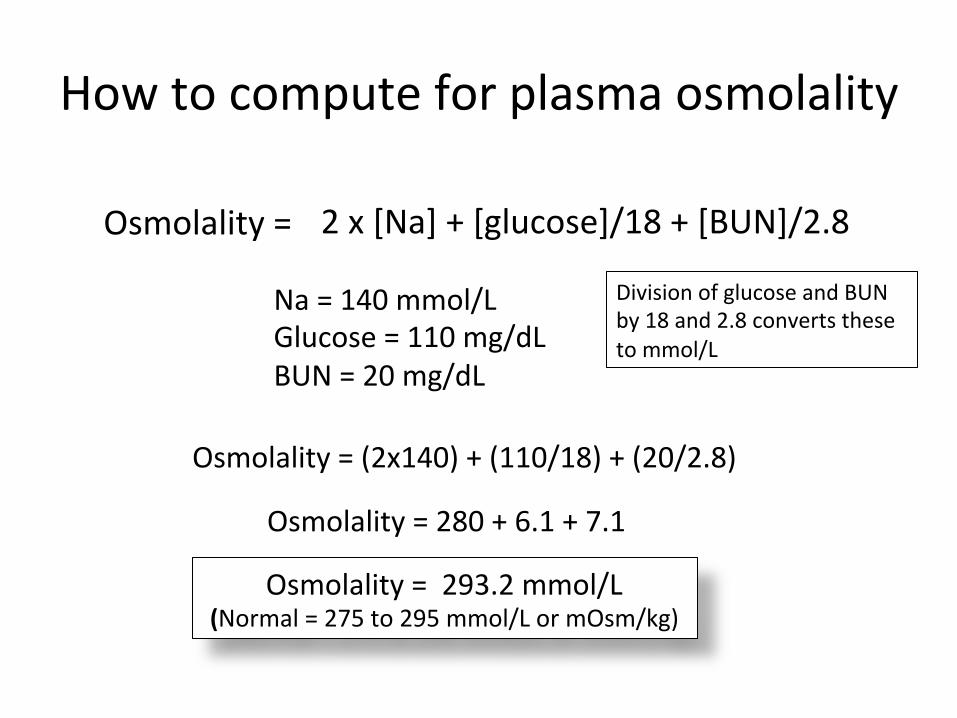
How to compute for plasma osmolality
Osmolality = 2 x [Na] + [glucose]/18 + [BUN]/2.8
Na = 140 mmol/L Glucose = 110 mg/dL BUN = 20 mg/dL
Osmolality = (2x140) + (110/18) + (20/2.8)
Osmolality = 280 + 6.1 + 7.1
Osmolality = 293.2 mmol/L (Normal = 275 to 295 mmol/L or mOsm/kg)
Division of glucose and BUN by 18 and 2.8 converts these to mmol/L


Homeostasis needs energy ECF (mmol/L) ICF (mmol/L) Mechanism
Na+ 140 10 Ac/ve transport K+ 4 140 Ac/ve transport Ca++ 2.5 0.1 Ac/ve transport Mg++ 1.5 30 Ac/ve transport Cl-‐ 100 4 Ac/ve transport HCO3-‐ 27 10 Ac/ve transport PO4-‐ 2 60 Ac/ve transport Glucose 5.5 0-‐1 Facilitated
diffusion Protein 2 gm/dL 16 gm/dL Ac/ve transport

We are living creatures made up of one trillion cells
• Each cell is living with a need for nutrients and energy
• Each cell has a structure and a purpose
• All are combined to form you and me
• When one unit suffers the rest also suffer
Nervous system Cardiovascular system Pulmonary system Muscular system Skeletal system Gastrointes/nal system Renal system Endocrine system Immune system Cutaneous system
“Fearfully and wonderfully made” Psalm 139:14
Harper Biochem Ganong Physio Guyton Physio

From a nutri/on standpoint we have 3 components which func/on as one
• Water 60% → Water provides the environment for structure and func/on to occur
• Fat mass 25% → Fat mass provides both structure and func/on and is the main energy reserve for our bodies
• Carbohydrate 1% • Protein mass (fat-‐free mass) 14%
→ protein mass provides the main func/onal component of the body; it is also called the LEAN BODY MASS.
WATER (60%)
FAT (25%)
CARBO + OTHER (1%) PROTEIN (14%)
Based on the weight – we need to take the weight of the pa2ent
Harper Biochem Ganong Physio Guyton Physio
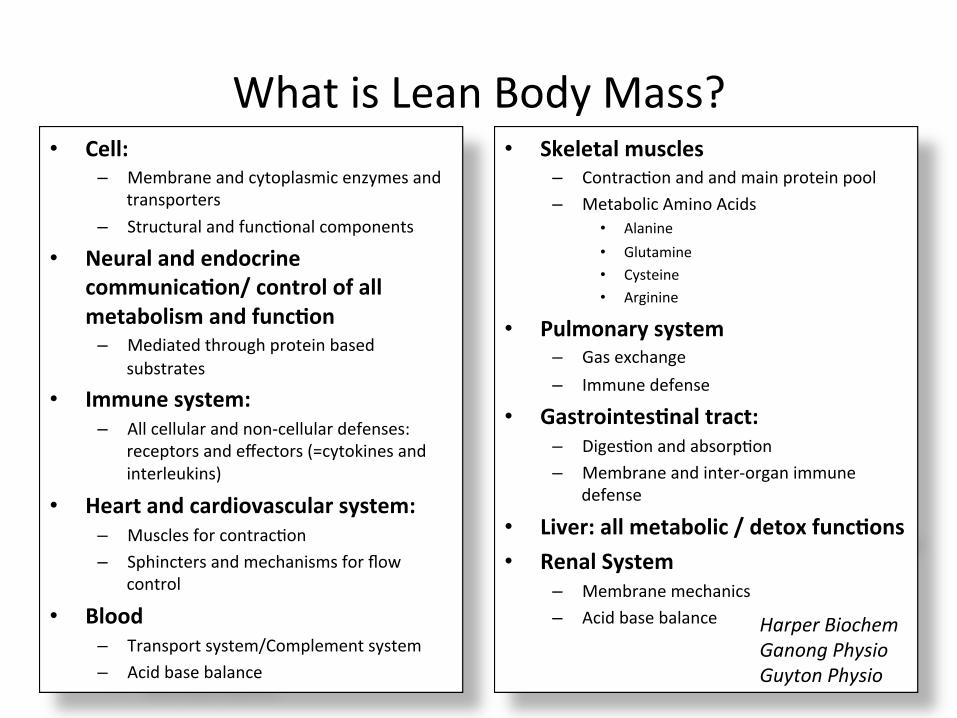
What is Lean Body Mass? • Cell:
– Membrane and cytoplasmic enzymes and transporters
– Structural and func/onal components • Neural and endocrine
communica2on/ control of all metabolism and func2on
– Mediated through protein based substrates
• Immune system: – All cellular and non-‐cellular defenses:
receptors and effectors (=cytokines and interleukins)
• Heart and cardiovascular system: – Muscles for contrac/on – Sphincters and mechanisms for flow
control
• Blood – Transport system/Complement system – Acid base balance
• Skeletal muscles – Contrac/on and and main protein pool – Metabolic Amino Acids
• Alanine • Glutamine • Cysteine • Arginine
• Pulmonary system – Gas exchange – Immune defense
• Gastrointes2nal tract: – Diges/on and absorp/on – Membrane and inter-‐organ immune
defense
• Liver: all metabolic / detox func2ons • Renal System
– Membrane mechanics – Acid base balance Harper Biochem
Ganong Physio Guyton Physio

Protein balance • Every single moment of the day there is protein synthesis
• Protein synthesis and degrada/on has a balance (= 0) → “you have to know how much protein to eat daily, including quality protein”
• If there is no protein intake, the body will recycle the old protein with the following effects: – More tendency for poor protein to be synthesized (i.e. mutaJons or degeneraJon will occur)
– increased protein breakdown with increased inflammaJon reacJon
• Protein dosage range = 0.8 – 2.5 g/day

Protein losses = Urine nitrogen losses
Long CL et al. JPEN 1979; 3: 452-‐456
0 g/day
2.5 g/day
2 g/day
1 g/day

Rela/onship between food intake and body composi/on
Liver glycogen Post-‐prandial
Amino acid pool (skeletal muscle)
Fat mass
↑Gluconeogenesis
Amino acid pool (skeletal muscle)
Fat mass
Minimum to zero feeding (=NPO for 24 to 48 hrs)
↓Gluconeogenesis
Amino acid pool (skeletal muscle)
Fat mass
Minimum to zero feeding > 5 days
Adapted from Ruderman NB. Annu Rev Med 1975; 26248.

• Catecholamines • Glucagon • Thyroid hormones • Cor2sol
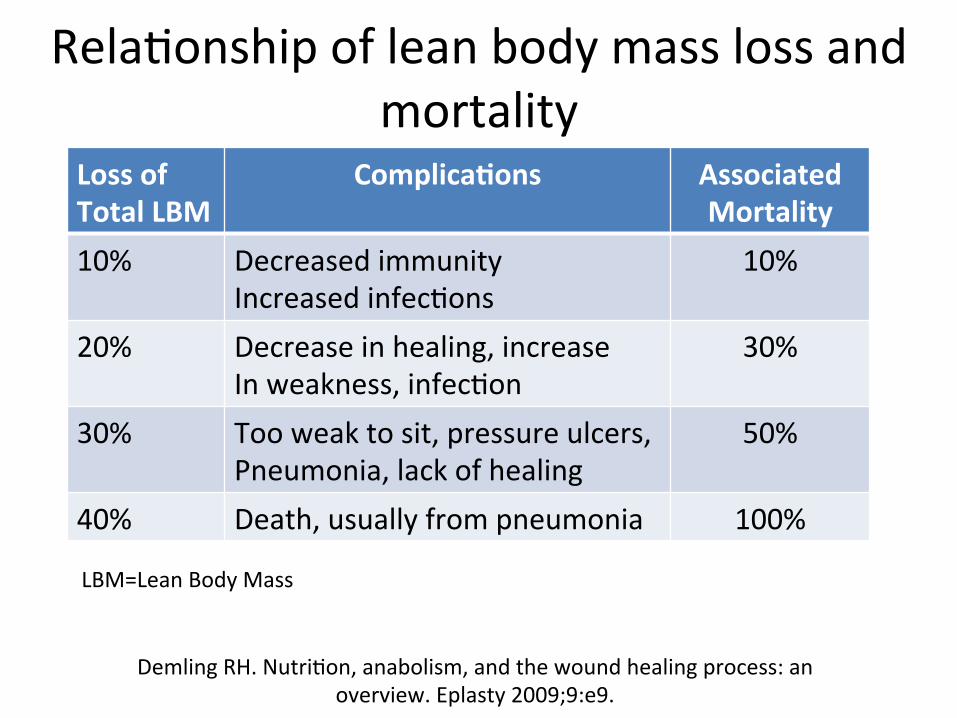
Rela/onship of lean body mass loss and mortality
Loss of Total LBM
Complica2ons Associated Mortality
10% Decreased immunity Increased infec/ons
10%
20% Decrease in healing, increase In weakness, infec/on
30%
30% Too weak to sit, pressure ulcers, Pneumonia, lack of healing
50%
40% Death, usually from pneumonia 100%
Demling RH. Nutri/on, anabolism, and the wound healing process: an overview. Eplasty 2009;9:e9.
LBM=Lean Body Mass

As we age there is a series of changes that occur in our body

As we age there is a series of changes that occur in our body
“Sarcopenia” = aging process

Lean body mass changes in elderly
COMPLICATIONS SARCOPENIA

Cancer Cachexia

Weight loss and wound healing
Demling RH. Eplasty. Nutri/on, anabolism, and the wound healing process: an overview. Eplasty 2009;9:e9. Epub 2009 Feb 3.

↓LBM, infec/on and ↑MOF
LBM
• Macrophage • T-‐cells • Ig-‐A • Mucosa integrity • Lymphoid /ssue ac/vity
Mucosa Immune System
Glutamine Alanine
9 MOF 8 Gut failure 7 Renal dysfunc2on 6 Sepsis 5 Pneumonia 4 ↑Insulin resistance 3 ↑inflamma2on 2 ↑Bacteria transloca2on 1 ↑Endotoxemia

Management
LBM
• Macrophage • T-‐cells • Ig-‐A • Mucosa integrity • Lymphoid /ssue ac/vity
Mucosa Immune System
Glutamine Alanine
9 MOF 8 Gut failure 7 Renal dysfunc2on 6 Sepsis 5 Pneumonia 4 ↑Insulin resistance 3 ↑inflamma2on 2 ↑Bacteria transloca2on 1 ↑Endotoxemia
ADEQUATE FEEDING: Macronutrients, micronutrients
LBM enhancers Early feeding, glutamine
An2bio2cs, pharmaconutri2on, pre/pro-‐bio2cs, blood purifica2on, nutrient/fluid balance

What are the LBM enhancers? • High protein intake
– Branched chain AA • Nutraceu/cals
– HMB, glutamine, arginine combina/ons – Fish oil (EPA/DHA)
• Exercise – Impact of free radicals – Not too much an/-‐oxidants
• Adequate intake • Insulin

Wound healing Essen/als: 1. Adequate protein
• Essen/al /non-‐essen/al AA 2. Adequate carbohydrate 3. Adequate fat
• Essen/al fasy acids 4. Adequate micronutrients
• Vitamins • Trace elements

eicosanoids
eicosanoids
eicosanoids
eicosanoids

Robbins Basic Pathology 7th edi/on. Kumar, Cotran, Robbins editors. 2003.
Inflamma/on

Energy requirements and an/oxidants
Glutathione reductase
Glutathione peroxidase
Glutathione peroxidase
Superoxide dismutase
• Munoz C. Trace elements and immunity: Nutri/on, immune func/ons and health; Euroconferences, Paris; June 9-‐10, 2005;
• Robbins Basic Pathology 7th edi/on 2003. Kumar, Cotran, Robbins editors.
Oxygen radicals O•2
Hydrogen peroxide H2O2
ONOO-‐
Zn Cu
2H2O
ONO-‐ + H2O
Glutathione reductase
Se
2GSH
2GSH
GSSG
GSSG
Vitamin C
Vitamin C
Catalase
2H2O

Basement membrane: 1. Cell support 2. Exchange 3. Transport 4. Development 5. Repair 6. Defense 7. Integrity of structure and
environment
Intercellular environment 1. Tissue support/shape 2. Exchange 3. Growth 4. Repair 5. Defense 6. Movement
Wound healing

Wound healing
Robbins Basic Pathology 7th edi/on. Kumar, Cotran, Robbins editors. 2003.

Inflamma/on: surgery
ADAPTED FROM:

Surgery induced immunosuppression
Ogawa K et al. Suppression of cellular immunity by surgical stress. Surgery 2000; 127 (3): 329-‐36
Surgical stress
↓Lymphocyte number and func/on up to 2 weeks post-‐op
↓T-‐helper cells ↓Cytotoxic T-‐cells ↓NK cells ↓IL2 receptor+ cells
↑T-‐suppressor cells ↑cor/sol ↑immuno -‐ suppressive
acidic protein?
?

Surgery induced immunosuppression
PRACTICAL SURGERY

Pre-‐opera/ve checklist • Check nutri/onal and fluid status (nutri/onal assessment)
• Check fluid and electrolyte status (=homeostasis): – Na, K, Cl (then may add Mg, Ca if needed) – Glucose, BUN, serum osmolality – Fluid intake and output record
• Wound healing capacity – Energy and protein requirements – Micronutrient requirements – Need for pharmaconutri/on

1. DETECT MALNUTRITION

Nutri/on screening & assessment Nutri2on screening Nutri2onal assessment

Malnutri/on and complica/ons Surgical pa2ents • 9% of moderately
malnourished pa/ents → major complica/ons
• 42% of severely malnourished pa/ents → major complica/ons
• Severely malnourished pa2ents are four 2mes more likely to suffer postopera2ve complica2ons than well-‐nourished pa2ents
Detsky et al. JAMA 1994 Detsky et al. JPEN 1987

Malnutri/on and complica/ons
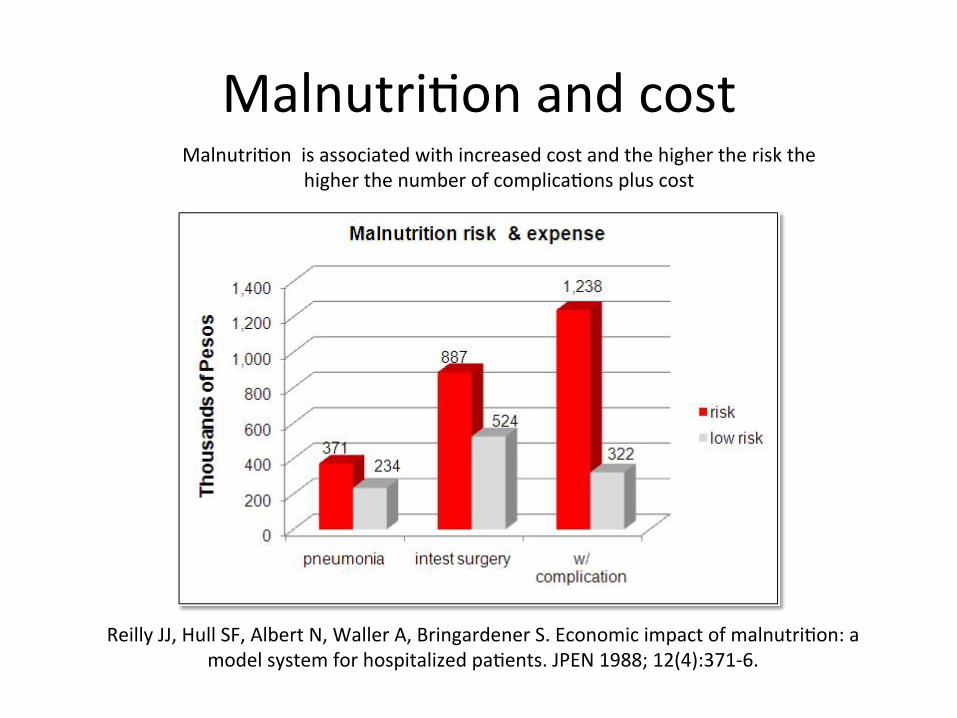
Malnutri/on and cost Malnutri/on is associated with increased cost and the higher the risk the
higher the number of complica/ons plus cost
Reilly JJ, Hull SF, Albert N, Waller A, Bringardener S. Economic impact of malnutri/on: a model system for hospitalized pa/ents. JPEN 1988; 12(4):371-‐6.

2. DETERMINE REQUIREMENTS

Nutri/on Care Plan Form

How much calories? Usual: 20-‐25 kcal/kg/day
Very sick: 15-‐20 kcal/kg/day
Jeejeebhoy K. 4th Asia Pacific Parenteral Nutri/on Workshop. June 7-‐9, 2009; Kuala Lumpur, Malaysia


How much protein?

How much carbohydrate and fat?

3. DETERMINE ROUTE OF FEEDING

Feeding algorithm Can the GIT be used?
Yes No
Parenteral nutrition Oral
< 75% intake
Tube feed
Short term Long term
Peripheral PN Central PN More than 3-4 weeks
No Yes
NGT
Nasoduodenal or nasojejunal
Gastrostomy
Jejunostomy
“inadequate intake”
“Inability to use the GIT”
A.S.P.E.N. Board of Directors. Guidelines for the use of parenteral and enteral
nutrition in adult and pediatric patients, III: nutritional assessment – adults. J
Parenter Enteral Nutr 2002; 26 (1 suppl): 9SA-12SA.

malnutri2on Scheduled • esophageal resec2on • gastrectomy • pancrea2coduodenectomy
Enteral nutri2on for 10-‐14 days
oral immunonutri2on for 6-‐7 days
Early oral feeding within 7 days
yes no
within 4 days
yes
“Fast Track”
no
Parenteral hypocaloric
Adequate calorie intake within 14 days
Enteral access (NCJ)
yes no
enteral nutri2on immunonutri2on for 6-‐7 days
Oral intake of energy requirements
yes no
combined enteral / parenteral
no slight, moderate severe
SURGERY
PRE-‐OPERATIVE PHASE
POST-‐OP
EARLY DAY 1 -‐ 14
LATE DAY 14
Oral intake of energy requirements
yes no supplemental enteral diet

Surgical nutri/on pathways: Pre-‐opera/ve phase
Normal to moderate malnutri/on
SURGERY
Severe Malnutri/on • Esophageal resec/on • Gastrectomy • Pancrea/coduodenectomy
Parenteral nutri/on + Omega-‐3-‐Fasy Acids + An/oxidants (+ glutamine); 6-‐7 days
Nutri/onal Assessment
ESPEN Guidelines on Parenteral Nutri/on (2009)
Condi/on: When oral or enteral feeding not possible

Enteral nutri/on STOMACH JEJUNUM
Nasogastric tube Nasojejunal tube
PEG PEJ
BUTTON
PLG
JET-‐PEG
PLJ
NCJ
PSJ
PFJ
PSG
PFG
Witzel, Stamm, Janeway
Loser C et al. ESPEN guidelines on arJficial enteral nutriJon – Percutaneous endoscopic gastrostomy
(PEG)
E: Endoscopic G: Gastrostomy J: Jejunostomy
L: Laparoscopic NC: Needle Catheter S: Sonographic F: Fluoroscopic

Parenteral nutri/on
• Central PN • Peripheral / peripheral central PN (PICC)
PICC =peripherally inserted central catheter
EARLY ENTERAL NUTRITION
• Enteral feeding 24 to 72 hours azer surgery or when pa/ent is hemodynamically stable
• Provide nutrients required during metabolic stress
• Maintain GI integrity • Reduce morbidity compared with parenteral nutri/on
• Reduce cost compared with parenteral nutri/on
Ra/onale

Early enteral nutri/on vs standard nutri/onal support on mortality
Comparison: mortality Outcome: early enteral nutri/on vs. control
Study Treatment n/N
Control n/N
Cerra et al 1990
Gosschlich et al, 1990
Brown et al, 1994 Moore et al, 1994 Bower et al, 1996 Kudsk et al, 1996
Engel et al, 1997
Weimann et al, 1998
1/11
2/17
0/19 1/51
24/163 1/16
7/18
2/16
1/9
1/14
0/18 2/47
12/143 1/17
5/18
4/13
0.01 0.1 10 100 Higher for control Higher for treatment
Ross Products, 1996 20/87 8/83
Mendez et al, 1997 1/22 1/21 Rodrigo et al, 1997 2/16 2/13
Atkinson et al, 1998 96/197 86/193
Galban et al, 2000 17/89 28/87
Heyland et al. JAMA, 2001
Pooled Risk Ra2o 1

4. DETERMINE ADEQUACY OF INTAKE

Calorie Count

Monitor actual nutrient intake

Effect of nutri/on intake on outcome Nutrition care led to reduced morbidity and mortality of surgical patients assessed
as severely malnourished and high risk (n=103)
Effect of nutrition care on post-operative complications predicted by surgical nutrition risk assessment: St. Luke’s Medical Center experience. Del Rosario D, Inciong JF, et al. 2008.

Intra-‐opera/ve checklist
• Fluid intake – Monitor and es/mate fluid losses – Only infuse what is required – Determine whether to give balanced electrolyte solu/ons or colloids; avoid saline and “water only” infusions like D5W or D10W
• Nutri/on access – Determine the need for long term enteral nutri/on (jejunostomy: surgical jejunostomy or nasojejunostomy)
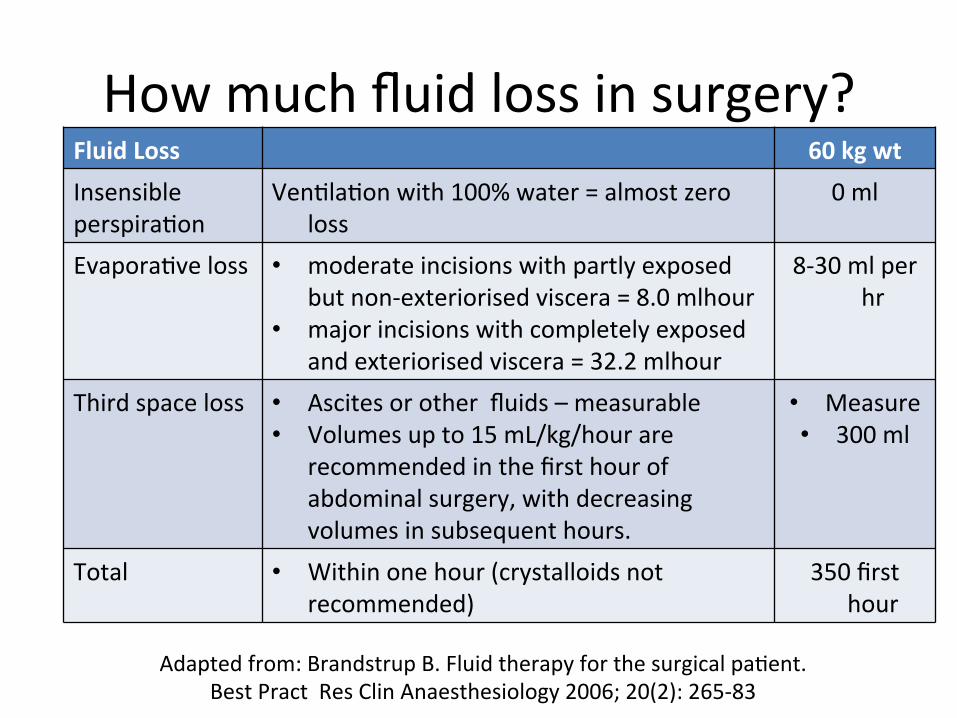
How much fluid loss in surgery? Fluid Loss 60 kg wt Insensible perspira/on
Ven/la/on with 100% water = almost zero loss
0 ml
Evapora/ve loss • moderate incisions with partly exposed but non-‐exteriorised viscera = 8.0 mlhour
• major incisions with completely exposed and exteriorised viscera = 32.2 mlhour
8-‐30 ml per hr
Third space loss • Ascites or other fluids – measurable • Volumes up to 15 mL/kg/hour are
recommended in the first hour of abdominal surgery, with decreasing volumes in subsequent hours.
• Measure • 300 ml
Total • Within one hour (crystalloids not recommended)
350 first hour
Adapted from: Brandstrup B. Fluid therapy for the surgical pa/ent. Best Pract Res Clin Anaesthesiology 2006; 20(2): 265-‐83

Which fluid is the most appropriate?

71
Fluid management Use Compartment Composition Examples
Volume Replacement
Intravascular fluid volume
Iso-oncotic Isotonic Iso-ionic
6% HES 130 in balanced solution
Fluid Replacement
Extracellular fluid volume
Isotonic Iso-ionic
Balanced solution: normal saline; ringer’s lactate
Electrolyte or osmotherapy (solutions for correction)
Total body fluid volume
According to need for correction
KCL Glucose 5% Mannitol
Reference: Zander R, Adams Ha, Boldt J. 2005; 40; 701-‐719

Post-‐opera/ve checklist
• Fluids and electrolytes – Daily accumulated fluid balance – Goal: “zero” fluid balance – Serum electrolytes – Give balanced electrolyte solu/ons
• Adequacy of nutrient intake – Early enteral nutri/on – Daily nutrient balance (=nutrient intake) – Good glucose control

SURGICAL COMPLICATIONS

Common peri-‐opera/ve surgical complica/ons
• Fluid and electrolyte problems • Wound infec/on and sepsis • Wound dehiscence

Fluid management
• Average periopera/ve fluid infusion: – Intra-‐op = 3.5 to 7 liters – 3 liters/day for the next 3 to 4 days – Average gain post-‐op = 3 to 6 kg weight gain
• Leads to: – Delay of gastrointes/nal func/on – Impair wound anastomosis healing – Affects /ssue oxygena/on – Prolonged hospital stay
Lassen et al. Arch Surg 2009

Fluid and electrolyte imbalance INJURY = SURGERY
↑albumin escape from intravascular
space
Inflammatory mediators ↑vasodila/on effect of anesthe/c agents
↑K+ release from cells
↓K+ and ↑ Na intracellular
Sick cell syndrome of cri/cal illness
↑hypotonic fluid infusion
90% cause of hyponatremia in
surgery
Fluid Reten2on + Electrolyte Imbalance
Lobo D, Macafee DL, Allison S. How periopera/ve fluid balance influences postopera/ve outcomes. Best Pract Res Clin Anaesthesiology 2006; 20(3): 439–55.

Ileus and dehiscence Salt and water overload
↑intra-‐abdominal pressure
↓mesentery blood flow
Intes/nal edema
↓/ssue OH-‐proline
STAT3 ac/va/on ↓myosin phosphoryla/on
ILEUS
Impaired wound healing
DEHISCENCE
Intramucosal acidosis
↓muscle contrac/lity
Chowdhury and Lobo. Curr Opinion Clin Nutr Metab 2011

Anastomosis leak
• Points to bowel prepara/on: – meta-‐analyses show that bowel prepara/on is not beneficial
– in elec/ve colonic surgery, and 2 smaller recent RCTs suggest that it increases the risk for anastomo/c leak
– Promote longer ileus dura/on
• Points to fluid management Lassen K et al. Consensus Review of Op/mal Periopera/ve Care in Colorectal Surgery: Enhanced Recovery Azer Surgery (ERAS) Group Recommenda/ons.
Arch Surg 2009; 144 (10): 961-‐9.

What is the worst fluid to give?
Plasma 0.9% saline Na (mmol/L) 135 – 145 154 Cl (mmol/L) 95 – 105 154 K (mmol/L) 3.5 – 5.3 0 HCO3 (mmol/L)
24 – 32 0
Osmolality (mOsm/kg) 275 – 295 308 pH 7.35 – 7.45 5.4
Lobo D, Macafee D, and Allison S. How periopera/ve fluid balance influences postopera/ve outcomes. Best Pract Res Clin Anaesthesiology 2006; 20(3):
439-‐55.

Inflamma/on: surgery
ADAPTED FROM:

Inflamma/on: sepsis

Inflamma/on & organ failure in the ICU
SIRS TNFα, IL-1β, IL-6, IL-12, IFNγ, IL-3
IL-10, IL-4, IL-1ra, Monocyte HLA-DR
suppression
CARS
days
Insult (trauma, sepsis)
Infla
mm
ator
y ba
lanc
e
AN
TI
PR
O
Tissue inflammation, Early organ failure and death
weeks
Immunosuppression
2nd Infections Delayed MOF and death
Griffiths, R. “Specialized nutrition support in the critically ill: For whom and when? Clinical Nutrition: Early Intervention; Nestle
Nutrition Workshop Series
Goal of nutri2on/ pharmaconutri2on

Inflamma/on & organ failure in the ICU
SIRS TNFα, IL-1β, IL-6, IL-12, IFNγ, IL-3
IL-10, IL-4, IL-1ra, Monocyte HLA-DR
suppression
CARS
days
Insult (trauma, sepsis)
Infla
mm
ator
y ba
lanc
e
AN
TI
PR
O
Tissue inflammation, Early organ failure and death
weeks
Immunosuppression
2nd Infections Delayed MOF and death
Griffiths, R. “Specialized nutrition support in the critically ill: For whom and when? Clinical Nutrition: Early Intervention; Nestle
Nutrition Workshop Series
Goal of nutri2on/ pharmaconutri2on
1. Early enteral nutri2on 2. Supplement with
parenteral nutri2on 3. Pharmaconutri2on: Fish
oils and glutamine 4. Zero fluid balance

Sarcopenia in elderly COMPLICATIONS

Sarcopenia in elderly COMPLICATIONS
1. Early enteral nutri2on 2. Supplement with
parenteral nutri2on 3. Adequate nutrient
intake 4. Pharmaconutri2on: Fish
oils and glutamine 5. Zero fluid balance

Cancer Cachexia

Cancer Cachexia
1. Early enteral nutri2on 2. Supplement with
parenteral nutri2on 3. Adequate nutrient
intake 4. Pharmaconutri2on: Fish
oils and glutamine 5. Zero fluid balance

CASE DISCUSSION

Surgical case • 62 y/o male • Height=1.6 m, weight=52 kg, weight two months ago=60 kg
• Anorexia, vomi/ng; weight loss • Diagnosis: head of pancreas cancer • Referred for surgery: • Labs: Hb=11, WBC=5600, N=60%, L=6%, platelet=240k; Na=135 mmol/L; K=3.2 mmol/L; glucose=160 mg/dL; BUN=6 mmol/L; albumin=3 gm/dL; crea/nine=1.1 mg/dL
Ques/ons
• Will you operate on this pa/ent tomorrow?

Available data
• BMI=21 • Weight loss in two months=13% • Cancer, head of pancreas • Albumin=3 gm/dL • Total lymphocyte count (TLC)=336 • Na=135, K=3.2 • Compute for the osmolality
– ([2x135] + [160/18] + [6] = 284.8 mOsm/kg H2O)

Ques/on
• If you plan to build up the pa/ent how?

Build up
• Total fluid (ml)/day = 52 kg x 30 ml/day = 1560-‐1600 ml/day
• Total calories/day = 52 kg x 30 kcal/day = 1560 kcal/day
• Total protein/day = 52 kg x 1.5 gm/day = 78 gm/day • Total carbo and fat: get the non-‐protein calories: 1560 – (78x4kcal/gm) = 1248 NPC – Carbo (60%): 1248 x 0.60 = 748.8 kcal/(4kcal/g) = 187 gm – Fat (40%): 1248 x 0.40 = 499.2 kcal/(9kcal/g) = 55.5 gm
• Vitamins and trace elements?

Build up
• What is the route? – Oral? Tube feed? Parenteral nutri/on? Combina/on?
• Dura/on of build up? • How to ensure adequate intake?
– Measure calorie count daily – Monitor and ensure normaliza/on of the electrolyte and fluid status

Build up
• What are the indicators of build up success? – Normaliza/on of abnormal values?
• TLC? Albumin? Na? K?
– “zero” fluid balance? – Adequate nutri/on intake?

Intra-‐opera/ve
• Will you monitor the fluid input? • How much fluid loss do you expect?
– Will you leave everything to the anesthesiologist?
• What are your choices of fluids? • Will you place a jejunostomy?

Post-‐opera/ve
• Will you place an NGT? • Will you place drains? • How will you monitor the post-‐op course?
– Will you place on NPO? How long? – How ozen will you check the electrolytes? Glucose?
• When will you start enteral feeding? Oral feeding? – How? When?
• Will you give parenteral nutri/on?

Take home message
• Fluid and nutri/onal status • Fluid and electrolyte balance • Nutrient balance/adequate nutrient intake

THANK YOU