supracondylar humeral fractures in children - have … humeral fractures in children - have we...
TRANSCRIPT
Volume 04 / Issue 02 / June 2016 boa.ac.uk Page 48
JTO Peer-Reviewed Articles
Supracondylar humeral fractures in children - have we stopped thinking?
Christopher Colton
Neurovascular Injury
The management of neurovascular complications of this fracture generates much heated debate, which is perhaps not surprising, as the consequences of permanent neurological injury, or a critically ischaemic limb, are devastating.
Nerve injuries are common and are estimated to occur in 12% to 20% of all such displaced fractures, with the anterior interosseous nerve predominating2-5.
The majority will recover without treatment and the difficulty arises in identifying those that require exploration. Formal documentation of neurological and vascular function at the time of presentation is the first standard for practice in BOAST 116. Frequent reassessment during the period following reduction and stabilisation, whether by open or closed means, is also necessary to identify an iatrogenic injury, which has a reported incidence of 2% to 6% in some series7,8.
Ramachandran et al.9 recommended exploration of any nerve injured during reduction and stabilisation of fracture, in the presence of neuropathic pain, a complete lesion with sympathetic paralysis, or a nerve lesion with progressive acute deterioration. Single assessment provides but a snapshot, whereas it is a trend towards deterioration that
Christopher Colton & Fergal Monsell
Although it is unlikely that Hippocrates corresponded in Latin, we respect his attributed primum non nocere as a central tenet of medical practice. Those of us who undertake the management of distal humeral fractures in children would do well to hold to this.
Fergal Monsell
We also benefit from the wisdom of Santayana1 who told us that “Those who cannot remember the past are condemned to repeat it”, yet supracondylar humeral fractures in children appear to be exempt from the rules and reason that govern the contemporary management of other injuries.
The purpose of this essay is to examine the conventional dogma associated with this common fracture, and to question some of its firmly-held beliefs, even should this require the sacrifice of sacred cows.
The authors’ view is that preservation of neurological function, the prevention of further neurological injury and the avoidance of ischaemic muscular damage are of fundamental importance in management.
Good function is to be expected in the majority of cases and the current paradigm of prevention of cosmetic deformity at all costs is not only illogical, but also potentially harmful.
Volume 04 / Issue 02 / June 2016 boa.ac.uk Page 49
>>
and pulseless hand following supracondylar humeral fracture, at a mean interval of three months following injury, were found to have an established ischaemic contracture of the forearm and hand.
They recommended “urgent exploration of the vessels and nerve in the child with pink, pulseless hand, not relieved by reduction, with persistent and increasing pain, suggestive of a deteriorating neurological injury and critical ischaemia”.
The authors’ view is that the majority of the recommendations made by Ramachandran et al.
should inform decisions on nerve exploration9.
The controversy surrounding the limb with potential ischaemia is in our view, due in part, to the surrogate methods of assessment of limb perfusion. The fundamental goal is to avoid muscle ischaemia with consequent contracture, and assessment must assess muscle perfusion, albeit indirectly.
Pulse, digital colour, capillary refill and mechanical methods, including pulse oximetry, do not satisfy this requirement. The simplest clinical test for evolving
muscle ischaemia is pain on passive digital extension and/or flexion.
In our view, the decision to explore a vascular injury or decompress a muscle compartment should be based largely on the presence and deterioration of muscle stretch pain in the period following injury or reduction of the fracture.
We consider that the majority of fractures can be managed without exploration of the neurovascular structures and have highlighted specific clinical situations in which rapid exploration is required.
frequently determines the need for surgical exploration.
Mangat et al.10 suggested management strategies for the perfused, pulseless hand, following stabilisation of displaced fractures. They reported a sub-group with tethering, or entrapment, of nerve and vessel at the fracture site and their recommendation was that the patient presenting with co-existing anterior interosseous, or median nerve palsy and a pink, pulseless hand warranted early neurovascular exploration.
Blakey et al.11 reported that 23/26 children with a pink
Journal of Trauma and Orthopaedics: Volume 04, Issue 02, pages 48-51Title: Supracondylar humeral fractures in children – have we stopped thinking?
Authors: Christopher Colton & Fergal Monsell
© 2016 British Orthopaedic Association
MCh OrthopaedicsFaculty of Medical Science
Our Masters course is ideal for surgeons who wish to develop their expertise at postgraduate level. It’s designed to fit flexibly around your career commitments through blended learning. We are still accepting applications for this September. • Leadership and management • Observership with Addenbrooke’s University Hospital
in Cambridge• Research opportunities
For full course details and an application form visit
anglia.ac.uk/orthopaedics
facebook.com/FHSCEnews@FHSCEnews@angliaruskinFMS
01245 68 68 68
Volume 04 / Issue 02 / June 2016 boa.ac.uk Page 50
JTO Peer-Reviewed Articles
structures, as well as increasing the chances of a failed fixation. For this reason alone, reduction must be achieved to an anatomical, or near-anatomical position and requires careful monitoring with image intensification. Whereas these problems need not necessarily contraindicate closed reduction and intraosseous pinning, such valid caveats are rarely stressed.
Powered insertion of Kirschner wires generates heat in the tissues and an important point that passes largely unstated is that the pins should be inserted with an oscillating drill or by hand in health systems where such equipment is unavailable. Thermal injury of the physis, through which the pins are inserted is a danger, especially if multiple attempts are made to insert any one pin.
Hunter and Slongo stated: “When placing (inserting) wires across the growth plate, repeated drilling, starting several wires from a single point, and very peripheral insertion must be avoided to minimise damage to the proliferation zone.”15
As educators of future generations of orthopaedic and fracture surgeons, we must condemn
multiple passes of a wire across the physis in an attempt to stabilise an imperfectly reduced fracture. Such a technique of multiple physeal penetrations, in other anatomical situations, is sometimes exploited to secure epiphysiodesis.
Cubitus varus
It is not unreasonable to examine current practice in the context of why reduction and fixation are so strongly advocated. With the exception of cases with vascular and neurological deficits, surgery is performed exclusively to avoid cubitus varus following malreduction.
Cubtius varus rarely, if ever, results in any functional deficit. It is purely a cosmetic problem in most, if not all cases and usually only evident when the patient is standing in the “anatomical position”.
In 1986, Ippolito et al. reviewed 22 patients with cubitus varus following such fractures treated non-operatively, and none had a functional deficit16. Similarly, Labelle et al. found no functional deficit in 63 patients with residual cubitus varus17.
Reduction and Fixation
As early as 1903, Prof. Niehans of Bern used intramedullary pinning to stabilise displaced supracondylar humeral fractures in children, but after open reduction12.
In 1988, Pirone stated: “Percutaneous Kirschner-wire fixation is advocated as the method of choice for the majority of (such) displaced fractures”13.
In 2014, Ladenhauf stated: “Today, the preferred treatment of displaced supracondylar humerus fractures in children is immediate closed reduction and percutaneous fixation with two or three lateral pins. In case of instability of the medial column, a medial pin may be used, but possibility of iatrogenic ulnar nerve injury should be considered”14.
Closed reduction with transcutaneous pinning has now become the promulgated orthodoxy for such fractures and BOAST states that: “These injuries require early surgical treatment; ideally on the day of admission…surgical stabilisation should be with bicortical wire fixation”6.
Such dogma deserves careful and thoughtful re-examination as the therapeutic pendulum appears to have become stuck at one of its poles.
Quality of reduction
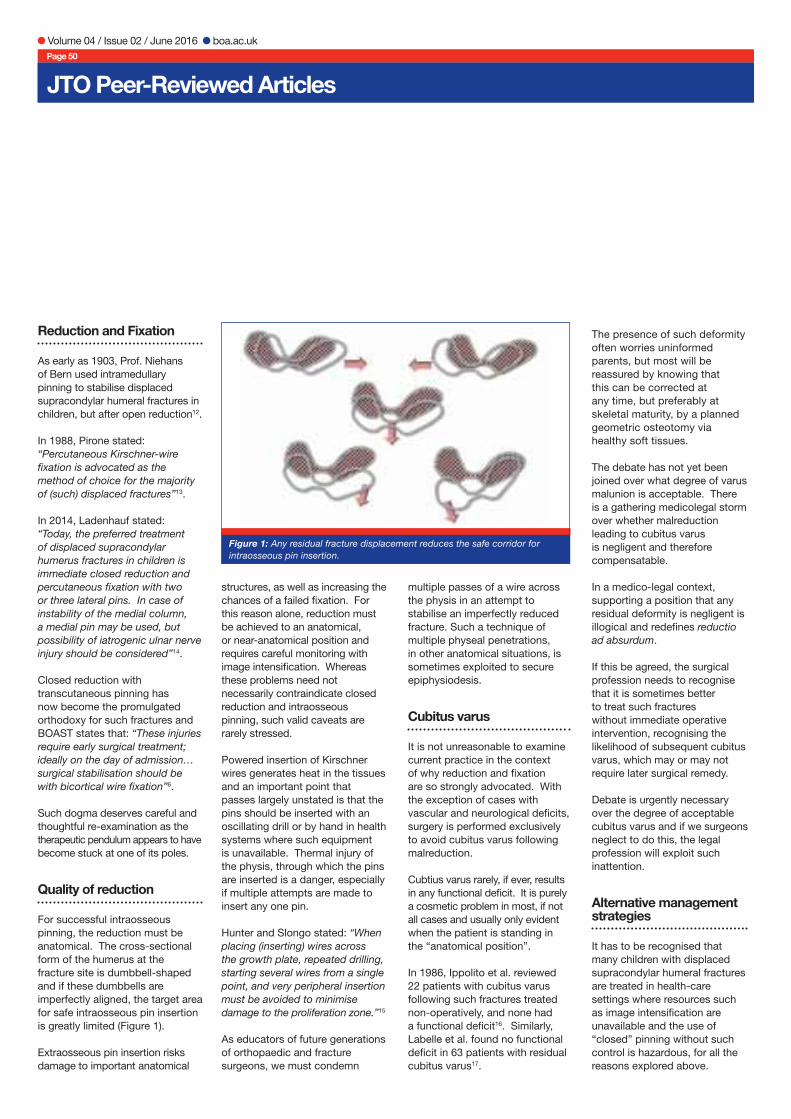
For successful intraosseous pinning, the reduction must be anatomical. The cross-sectional form of the humerus at the fracture site is dumbbell-shaped and if these dumbbells are imperfectly aligned, the target area for safe intraosseous pin insertion is greatly limited (Figure 1).
Extraosseous pin insertion risks damage to important anatomical
The presence of such deformity often worries uninformed parents, but most will be reassured by knowing that this can be corrected at any time, but preferably at skeletal maturity, by a planned geometric osteotomy via healthy soft tissues.
The debate has not yet been joined over what degree of varus malunion is acceptable. There is a gathering medicolegal storm over whether malreduction leading to cubitus varus is negligent and therefore compensatable.
In a medico-legal context, supporting a position that any residual deformity is negligent is illogical and redefines reductio ad absurdum.
If this be agreed, the surgical profession needs to recognise that it is sometimes better to treat such fractures without immediate operative intervention, recognising the likelihood of subsequent cubitus varus, which may or may not require later surgical remedy.
Debate is urgently necessary over the degree of acceptable cubitus varus and if we surgeons neglect to do this, the legal profession will exploit such inattention.
Alternative management strategies
It has to be recognised that many children with displaced supracondylar humeral fractures are treated in health-care settings where resources such as image intensification are unavailable and the use of “closed” pinning without such control is hazardous, for all the reasons explored above.
Figure 1: Any residual fracture displacement reduces the safe corridor for intraosseous pin insertion.

Volume 04 / Issue 02 / June 2016 boa.ac.uk Page 51
The alternative options would then be open reduction and pinning, splintage after attempted reduction (accepting the risk of cubitus varus), or traction, involving methods that include straight-arm and overhead olecranon traction (Figure 2).
The latter two therapeutic options should not be allowed to fall into the oubliette of paediatric orthopaedic history, for want of a rather broader approach than the current dogma of Pirone, Ladenhauf and the BOA’s standard treatment protocol.
Correction of cubitus varus malunion
In 1959, French described a somewhat crude valgus osteotomy for the correction of cubitus varus18. It unfortunately produced the so-called “chicane” deformity, with excessive lateral condylar prominence, as does any such osteotomy that fails to translate medially the distal humeral fragment.
Regrettably, such ugly corrections are still practised today, thereby exchanging one cosmetic deformity
for another. Yun et al. described an ingenious technique19 that corrects distal humeral deformity, without secondary lateral translation (Figure 3).
There is no place in modern surgery for corrective osteotomies to be conducted without detailed preoperative planning and geometric precision. The correction of a cosmetic deformity demands a cosmetically perfect result.
Some authors advocate stabilisation of such osteotomies using external fixation20 and whilst this provides a potentially attractive alternative; it has not become an established part of contemporary practice.
Summary
The majority of perfused but pulseless hands can be managed expectantly, provided there is no evidence of evolving muscular ischaemia.
The majority of peripheral nerve injuries, which are caused at the time of injury and present at the time of first assessment, can also be managed expectantly,
provided there is no evidence of neuropathic pain, or deterioration over a period of 8 to 12 hours.
The current dogma of reduction and transcutaneous pinning of all displaced supracondylar humeral fractures in children should be approached in a more analytical fashion than the simple ex cathedra statements that abound. It is a demanding surgical procedure with risks for patients of the unwary and formulaic surgeon, and there are alternative management strategies for under-resourced health care systems.
Attitudes to cubitus varus malunion, in both surgical and medicolegal contexts, bear careful scrutiny and osteotomies to correct cubitus varus malunion require meticulous planning and precise, geometric execution.
Christopher Colton is Professor Emeritus in Orthopaedic and Accident Surgery at the University of Nottingham and was a Consultant Orthopaedic, Trauma and Paediatric Orthopaedic Surgeon at Nottingham University Hospital for more than 20 years. He was an ABC Travelling fellow, BOA President, Founding Trustee and Lifetime Honorary Member of the Board of Trustees of
the AO Foundation. He is currently enjoying life as an educator, boulevardier and master diver.
Fergal Monsell is a Consultant Orthopaedic Surgeon at the Royal Hospital for Children in Bristol. He was an ABC travelling fellow, Past President of the British Limb Reconstruction Society and a Member of the Politburo of the Society for Children’s Orthopaedic Surgery. He is a member of the editorial board of the Bone and Joint Journal and specialty editor for paediatrics. He is married to Ros, has three grown-up children and to his credit is a lifelong Spurs supporter.
Correspondence
Email: [email protected]: [email protected]
References
References can be found online at www.boa.ac.uk/publications/JTO or by scanning the QR Code.
Figure 2: Overhead traction via an olecranon screw. The arm is elevated, thereby reducing pain and swelling: the forearm falls naturally into pronation, encouraging the correction of varus.
Figure 3: Yun osteotomy: A triangle of bone is excised as shown in the left hand diagram: the angle at B is the desired angle of valgus correction. The distal humeral fragment is then rotated and medially translated so that the original point A is moved to point C. The pair of diagrams on the right show how the longitudinal axis of the humeral diaphysis now passes through the lateral portion of the trochlea – the anatomical norm – and the osteotomy if stabilised with crossed pins.
Journal of Trauma and Orthopaedics: Volume 04, Issue 02, pages 48-51Title: Supracondylar humeral fractures in children – have we stopped thinking?
Authors: Christopher Colton & Fergal Monsell
© 2016 British Orthopaedic Association
References 1. Santayana G. Life of Reason Vol 1, Ch XII. Flux and Constancy in Human Nature,1905 2. Culp RW, Osterman AL, Davidson RS, Skirven T, Bora FW Jr. Neural injuries associated with supracondylar
fractures of the humerus in children.J Bone Joint Surg [Am] 1990;72-A:1211-15. 3. Dormans JP, Squillante R, Sharf H. Acute neurovascular complications with supracondylar humerus fractures in
children. J Hand Surg [Am] 1995;20:1-4. 4. Cramer KE, Green NE, Devito DP. Incidence of anterior interosseous nerve palsy in supracondylar humerus
fractures in children. J Pediatr Orthop 1993;13:502-5. 5. Campbell CC, Waters PM, Emans JB, Kasser JR, Millis MB. Neurovascular injury and displacement in type III
supracondylar humerus fractures. J Pediatr Orthop 1995;15:47-52. 6. http://www.boa.ac.uk/publications/boa-standards-trauma-boasts/#toggle-id 7. Rasool MN.Ulnar nerve injury after K-wire fixation of supracondylar humerus fractures in children. J Pediatr
Orthop 1998;18:686-90. 8. Birch R, Achan P. Peripheral nerve repairs and their results in children. 9. Hand Clin 2000;16:579-95. 10. Ramachandran M, Birch R, Eastwood. Clinical outcome of nerve injuries associated with supracondylar fractures
of the humerus in children. The experience of a specialist referral centre. J Bone Joint Surg [Br] 2006;88-B:90-4. 11. Mangat KS, Martin A, Bache CE. The ‘pulseless pink’ hand following supracondylar fractures of the humerus in
children: the predictive value of nerve palsy. J Bone Joint Surg [Br] 2009;91-B:1521-5. 12. Blakey CM, Biant LC, Birch R. Ischaemia and the pink, pulseless hand complicating supracondylar fractures of the
humerus in childhood: long-term follow-up. J Bone Joint Surg [Br] 2009;91-B:1487-92. 13. Niehans P, Zur Fracturebehandlung durch temporäre Annagelung. Arch Klin Chir 1904; 73: 167-78 14. Pirone A M, Krajbich J, Graham H K. Managment of displaced extension type supracondylar fractures of the
humerus in children. J Bone Joint Surg (Am) 1988; 70: 641-50. 15. Ladenhauf, H.,Schaffert, M., Bauer, J.The displaced supracondylar humerus fracture: indications for surgery and
surgical options: a 2014 update. Current Opinion in Pediatrics: 2014, 26: 64–69 16. Hunter J, Slongo T Principles of Fracture Management AO Publishing, Zurich, Distributed Thieme Verlag, 2007. 17. Ippolito, E., R. Caterini, and E. Scola. Supracondylar fractures of the humerus in children. Analysis at maturity of
fifty-three patients treated conservatively. Journal of Bone & Joint Surgery 68.3 (1986): 333-344. 18. Labelle, Hubert, et al. Cubitus varus deformity following supracondylar fractures of the humerus in children.
Journal of Pediatric Orthopaedics 2.5 (1982): 539-546. 19. French P. Varus deformity of the elbow following supracondylar fractures of the humerus in children. Lancet
(1959) 274, p439–441, 20. Yun, Y-H., S-J. Shin, and J-G. Moon. Reverse V osteotomy of the distal humerus for the correction of cubitus
varus. Journal of Bone & Joint Surgery, British Volume 89.4 (2007): 527-531. 21. Slongo T. Behandlung des posttraumatischen Cubitus varus bei Kindern und Jugendlichen. Suprakondyläre
Humerusosteotomiemit radialem Fixateur externe 22. Oper Orthop Traumatol 2015, 27:194–209.