supervisors - الجامعة الإسلاميةlibrary.iugaza.edu.ps/thesis/115215.pdf · special...
TRANSCRIPT


i
Ionizing Radiation Leakage and Radiation Protection Measures in
Radio-Diagnostic Centers in Governmental Hospitals of Gaza
Governorates, Palestine
,
By:
Samer S. Abu Zer
Supervisors:
A Thesis Submitted in Partial Fulfillment of the Requirements for the Degree of
Master of Science in Environmental Health
Dec./2014
The Islamic University–Gaza
Deanship of Graduate Studies
Faculty of Science
Master of Environmental Science
Environmental Health
Prof. Mohammed R. Al Agha Dr. Samir S. Yassin Professor of Environmental Sciences Associate Prof. of Physics
The Islamic University of Gaza The Islamic University of Gaza

ii
ABSTRACT
The fact of using radiation in medicine has led to major improvements in the
diagnostic and treatment of human diseases. However, it carries some risks of
health problems. This subject has received a great concern in the recent years.
The work is based on measurement of equivalent radiation dose rate in different
locations in radio-diagnostic rooms at governmental Gaza governorates
hospitals. These include: 19 basic X-ray, 8 fluoroscopy, 3 CT scan and
mammography machines. The measurements were carried out by using the
radiation survey meter (OD-01), since there is no obvious work have been
previously done experimentally.
A questionnaire is designed for matching the study needs and 182 radio-
diagnostic workers participated in the work in order to obtain an information
about their radiation protection measures and practices.
The results indicate that the fluoroscopy and CT scan rooms were not efficiently
lead lined and the radiation protection is not well organized. The measured
values of radiation dose rate at different locations in basic X-ray and
mammography rooms are found within a permissible limits for workers and
public. However, the recommended distance between the X-ray machine and
control panel have not been achieved in some rooms.
In addition, the results of questionnaire indicate unsatisfactory practices toward
radiation protection issues, where approximately half of participants have
negative practices. The participants have reported that 35.2% of personal
radiation protection devices are available in radio-diagnostic centers. Also the
results revealed very poor of personal radiation exposure monitoring process.
Overall, the results represented in this work reflect that majority of participants
believe there is no radiation safety officer to provide the service. Therefore,
there is a desperate need for rules, regulations and radiation protection act in the
field of radiation in medical field.
Finally, recommendations in the light of the outcome of study results were
given to improve the radiation protection and safety measures.
Key Words: Ionizing radiation, Radiation protection, X-ray, Radio-diagnostic,
Equivalent radiation dose rate, Workload.

iii
ملخص الدراسة
تشخيص والعالج من األمراض التي تصيب اإلنسان. أدى استخدام اإلشعاع في الطب إلى تحسينات كبيرة في ال
من المخاطر و المشاكل الصحية. وقد حظي هذا الموضوع باهتمام كبير في اومع ذلك، فإنه يحمل كثير
السنوات األخيرة. ويستند هذا العمل على قياس معدل الجرعة اإلشعاعية في مواقع مختلفة في غرف األشعة
8، أشعة سينيةجهاز 19حكومية في محافظات غزة. حيث شملت هذه الدراسة: التشخيصية في المستشفيات ال
أجهزة أشعة مقطعية. و جهاز تصوير الثدي. وقد أجريت القياسات باستخدام جهاز 3وسكوبي، فلورأجهزة
دراسة عملية سابقةال يوجد أي ( لقياس معدل الجرعة االشعاعية المكافئة، حيث أنهOD-01المسح االشعاعي )
لقياس هذه الجرعات في المستشفيات الحكومية في محافظات غزة.
شخص يعملون في مراكز األشعة التشخيصية 182 ، حيث شاركاحتياجات الدراسة لمالئمةتم تصميم استبيان
.من اإلشعاع اجراءات وممارسات الوقايةمعلومات عن بهذه المستشفيات وذلك للحصول على
ألشعة المقطعية لم تبطن بالرصاص بكفاءة وغير و غرف ا وسكوبيالفلوررف غالنتائج إلى أن أشارت
مصممة جيدا للوقاية من االشعاع. لقد وجد أن قياس معدالت الجرعة االشعاعية في مواقع مختلفة من غرف
مسافة ال ومع ذلك فانوالجمهور. املينللثدي ضمن الحدود المسموح بها للع االشعاعيوالتصوير األشعة السينية
السنية ولوحة التحكم في بعض الغرف لم تتحقق. الموصى بها بين جهاز أشعة
ما أن من اإلشعاع، حيث الوقاية إلى ممارسات غير مرضية تجاه قضايا أشارتنتائج االستبيان فإنباإلضافة
ية الشخصية من الوقاأجهزة من٪ 35.2 المشاركين أنيقرب من نصف المشاركين لديهم ممارسات سلبية. وأفاد
ة. وكشفت النتائج أيضا ضعف في عملية مراقبة التعرض ياالشعاع متوفرة في مراكز األشعة التشخيص
.لإلشعاعالشخصي
جهة تحرص على أن غالبية المشاركين يعتقدون أنه ال يوجد تفيدممثلة في هذا العمل العموما، فإن النتائج
تتعلق ن يانولوائح وقوقواعد لوضع . ولذلك، هناك حاجة ماسةينلماجراءات الوقاية من االشعاع وسالمة العا
في المجال الطبي. بالوقاية من االشعاع
في المجال اإلشعاعاجراءات وممارسات الوقاية من لتحسين على ضوء هذه النتائج أعطيت توصيات وأخيرا،
.يطبال
، األشعة السينية، األشعة التشخيصية ، الجرعة اإلشعاع المؤين ، الوقاية من اإلشعاع ح :
اإلشعاعية المكافئة ، حمولة العمل.

iv
Dedication
I would like first and most to thank almighty
God for the blessings and power that made
my project a reality.
I would like to extend my deepest gratitude
to:
My Parents for their unending love and
support,
My lovely wife who supports me,
My beloved daughters Jana and Lana,
My brothers and sisters,
My friends and colleagues who participated
in bringing this project to the happy end.
Samer S. Abu Zer

v
Acknowledgments IN THE NAME OF ALLAH, THE MOST GRACIOUS, THE MOST MERCIFUL
I would like to express my sincere thanks and gratitude to my supervisor Prof. Dr.
Mohammed Al Agha, for his continuous guidance, support and encouragement
throughout my research, that leads to the emergence of this work in current form.
Also, my sincere thanks to my supervisor Dr. Samir Yassin, due to his initiating and
planning of this work, without whom I could not have made this progress. He was
with me step by step and he was very keen to show me everything right.
My thanks should be extended to physicist Mr. Rami Al Agha for his help in
radiation doses measurements conducting.
My thanks should be extended to Dr. Said Al Husseini (General Director Of
Radiology Unit "MOH").
I'm greatly indebted to Mr. Ibrahim Abbas, Mr. Mohammed Al Sersawy, Mr. Maher
Marzooq, Mr. Rami Dwaima, Mr. Yasser Al Ya'qoby and Mr. Ahmed Wishah for
their support, encouragement and helpful suggestions.
Special thanks and admiration to Eng. Nader Skaik, Eng. Ahmed Lolo, Eng. Hazem
Al Qasass and Eng. Abed Al Hameed Siam for their cooperation and help during my
study.
I would like to highly thank Mr. Jihad Okasha for his help in statistical analysis.
At the end, I am very grateful to those who participated and help me to complete this
study.

vi
List of Contents
ii Abstract……………………………………………………….……………..……
iii …………………………………………………..……………..…….ملخص الدراسة
iv Dedication……………………...…………………………..……………………..
v Acknowledgment……………………..…………………..………………………
vi List of contents…...…………............……....……………………………………
ix List of tables………………………….……………..…………………..………..
x List of figures………………..…………………………………………..………..
xii List of annexes……………………………………………………………………
xiii List of abbreviations……………………………………………………………...
xiv List of glossary………………………………………………………………..…
Chapter 1: Introduction
1 1.1 Overview………………………..……………………………………………
3 1.2 Problem statement……………...…………………………………………….
3 1.3 Significance……………………...…………………………………………...
4 1.4 Justification……………………...……………………………………………
5 1.5 Objectives……………………...……………………………………………..
5 1.5.1 General objectives………….……………………………...…………...
5 1.5.2 Specific objectives………..……………………………...……………..
5 1.6 Context of the study………………………………………………………….
6 1.6.1 Radio-diagnostic services in governmental hospitals of Gaza……...….
11 1.6.2 Demographic context……………..………………………………....….
11 1.6.3 Gaza Strip population………………...………………………………
12 1.6.4 Socioeconomic and political context ………...……………….………..
12 1.6.5 Environmental status………..………………...……….………….……
13 1.7 Cancer in Palestine……….……………...………………...…………………
Chapter 2: Literature Review
15 2.1 Introduction……………………………….……………………….…………
15 2.2 Conceptual framework…………………………….………….……………...
18 2.3 Ionizing radiation...……………………….………………..…………………
18 2.4 Natural ionizing radiation sources……………………………………………
19 2.5 Artificial ionizing radiation sources…………………………..……………...
20 2.6 Types of individual exposure to ionizing radiation………..……………........
20 2.7 Ionizing radiation dose and units……………..………………………………
21 2.8 Medical uses of ionizing radiation……………………………………………
21 2.8.1 Radio-therapy…………………………………………………………..
22 2.8.2 Radio-diagnostic………………………………………………………..
22 2.8.2.1 Nuclear medicine………………………………………………..
22 2.8.2.2 Diagnostic X-ray………………………………………………
24 2.9 Radiation protection………………………………………………………….
24 2.9.1 Radiation protection principle………………………………………….
24 2.9.1.1 Justification……………………………………………………...
25 2.9.1.2 Optimization…………………………………………………….
25 2.9.1.3 Individual dose limits…………………………………………...
25 2.9.2 Radiation protection techniques…………………………………….....

vii
26 2.9.3 Radiation monitoring…………………………………………………..
26 2.9.3.1 Personal radiation monitoring in radio-diagnostic centers…..…
27 2.9.3.2 Ensuring effective radiation protection of medical staff……….
27 2.9.4 Personal radiation protection devices………………………………….
28 2.9.5 Radiation protection training…………………………………………..
28 2.10 The use of radiation for medical exposure …………………………………
30 2.11 Biological effects of ionizing radiation……………………………………..
31 2.12 Previous studies related to this research…………………………………….
Chapter 3: Methodology
35 3.1 Introduction…………………………………………………………………
35 3.2 Study design………………………………………………………………..
35 3.3 Study population………………………………………………………......
35 3.4 Sample size…………………………………………………………………
36 3.5 Locations of the study………...…………………………………………….
36 3.6 Ethical considerations ………………………………………………………..
36 3.7 Study instruments ……………………………………………………………
36 3.7.1 Radiation survey meter……….…………………………..…………….
37 3.7.2 Radio-diagnostic machines and rooms specifications…..……………...
38 3.7.3 Questionnaire interview…….………………………..…………………
39 3.8 Study techniques …..…………….…………………………………………...
39 3.8.1 Locations of measurements…………………………………………..
40 3.8.2 The workload…………….………..……………………………………
41 3.8.3 The equivalent radiation dose rate ..….….……………...….…………..
43 3.9 Limitation of the study……………………………………………………….
44 3.10 Statistical tools and data analysis…………………………………………
Chapter 4: Results and Discussion
45 4.1 Introduction……………………………………….………………………….
46 Part one
46 4.2 The equivalent radiation dose rate at the selected nine hospitals………..…...
46 4.2.1 The measurements at Al Shifa Medical Complex…...............................
48 4.2.2 The measurements at Nasser Medical Complex………………..…..…..
49 4.2.3 The measurements at European Gaza hospital……………….…..…….
50 4.2.4 The measurements at Abu Yousef Al Najjar Martyr hospital….…..…..
51 4.2.5 The measurements at Kamal Adwan Martyr hospital…………..….…..
52 4.2.6 The measurements at Al Aqsa Martyrs hospital………………..…..…..
53 4.2.7 The measurements at Abdel Aziz Rantessi Martyr hospital…..…..……
54 4.2.8 The measurements at Al Naser Pediatric hospital……………...……....
54 4.2.9 The measurements at Beit Hanoun hospital……………………………
55 4.3 The equivalent radiation dose rate at the different locations………………...
55 4.3.1 The equivalent radiation dose rate at control panels……….…………..
56 4.3.2 The equivalent radiation dose rate at corridors……………….………..
57 4.3.3 The equivalent radiation dose rate at patient waiting rooms…..……….
58 4.3.4 The equivalent radiation dose rate at dark rooms……………………..
59
4.3.5 Directional equivalent radiation dose rate and at one meter from the X-
ray tube in basic X-ray and mammography rooms…………………...
61 4.3.6 Directional equivalent radiation dose rate and at one meter from the

viii
X-ray tube in fluoroscopy and CT scan rooms………………………..
62 4.4 Specifications of radio-diagnostic machines and rooms at selected hospitals.
65 Part two
65 4.5 The questionnaire contents analysis…..……………………………………..
65 4.5.1 Socio-demographic and work related information…………………..…
70 4.5.2 Participants response about the availability of radiation protection……
72 4.5.3 Participants response to awareness items about radiation protection .....
76 4.5.4 Participants response to practices items about radiation protection…....
80 4.5.5 Participants response to personal radiation exposure monitoring.…..…
86 4.6 The relationship between the independent variables and the participants……
Chapter 5: Conclusion and Recommendations
101 5.1 Conclusion……………………………………………………………………
103 5.2 Recommendations……………………………………………………………
104 5.3 Suggestions for future studies………………………………………………...
105 References………………………………………………………………………..
116 Annexes…………………………………………………………………………..

ix
List of Tables
Table No. Subject Page
Table (1.1) Population distribution in Gaza governorates 12
Table (2.1) Time evolution of the number of radiological procedures,
collective dose and annual dose per capita, worldwide 29
Table (4.1) The dependent variables according to participants age 87
Table (4.2) The dependent variables according to participants sex 90
Table (4.3) The dependent variables according to participants occupation 91
Table (4.4) The dependent variables according to participants academic
qualification 93
Table (4.5) The dependent variables according to participants practical
experience 95
Table (4.6) The dependent variables according to participants hospitals 97
Table (4.7) The dependent variables according to participants daily work
hours in radio-diagnostic rooms 100

x
List of Figures
Figure No. Subject Page
Figure (1.1) Gaza Strip map and the selected nine governmental
hospitals locations 10
Figure (2.1) Schematic representation of the study framework. 17
Figure (3.1) Radiation survey meter (OD-01) 37
Figure (3.2) The radiation parameters were taken in basic X-ray
machine 41
Figure (3.3) The reference phantom was used as a scattering medium 42
Figure (3.4) Source Image Distance (SID) is equal 100 cm 43
Figure (4:1) The equivalent radiation dose rate in basic X-ray rooms at
Al Shifa Medical Complex 46
Figure (4.2) The equivalent radiation dose rate in fluoroscopy and CT
scan rooms at Al Shifa Medical 47
Figure (4.3) The equivalent radiation dose rate in basic X-ray and
mammography rooms at Nasser Medical Complex 48
Figure (4.4) The equivalent radiation dose rate in fluoroscopy and CT
scan rooms at Nasser Medical Complex 49
Figure (4.5) The equivalent radiation dose rate at European Gaza
hospital 50
Figure (4.6) The equivalent radiation dose rate at Abu Yousef Al Najjar
Martyr hospital 50
Figure (4.7) The equivalent radiation dose rate at Kamal Adwan Martyr
hospital 51
Figure (4.8) The equivalent radiation dose rate at Al Aqsa Martyrs
hospital 52
Figure (4.9) The equivalent radiation dose rate at Abdel Aziz Rantessi
Martyr hospital 53
Figure (4.10) The equivalent radiation dose rate at Al Naser Pediatric
hospital 54
Figure (4.11) The equivalent radiation dose rate at Beit Hanoun hospital 55
Figure (4.12) The equivalent radiation dose rate at control panels 56
Figure (4.13) The equivalent radiation dose rate at corridors 57
Figure (4.14) The equivalent radiation dose rate at patient waiting rooms 58
Figure(4. 15) The equivalent radiation dose rate at dark rooms 59
Figure (4.16)
Directional equivalent radiation dose rate and at one meter
from the X-ray tube in basic X-ray and mammography
rooms
60
Figure (4.17) Directional equivalent radiation dose rate and at one meter
from the X-ray tube in fluoroscopy and CT scan rooms 61
Figure (4.18) Participants percentage according to their occupation 65
Figure (4.19) Participants percentage according to their sex 66
Figure (4.20) Participants percentage according to their age groups 66
Figure (4.21) Participants percentage according to their academic 67

xi
qualifications
Figure (4.22) Participants percentage according to their practical
experience 68
Figure (4.23) Participants percentage according to their distribution at the
hospitals 68
Figure (4.24) Participants percentage according to their dealing with
radio-diagnostic machines 69
Figure (4.25) Participants percentage according to their daily work hours
in radio-diagnostic rooms 69
Figure (4.26) Participants response about the availability of personal
radiation protection devices items 70
Figure (4.27) Participants response to radiation protection awareness
items 73
Figure (4.28) Participants response to radiation protection practices items 77
Figure (4.29) Participants response about availability of radiation
protection advisors 81
Figure (4.30) Participants response about availability of personal
radiation exposure monitoring devices 81
Figure (4.31)
Participants response about using of personal radiation
exposure monitoring device during their work in radio-
diagnostic rooms
82
Figure (4.32)
Participants response about receiving guidance about the
proper handling with the personal radiation exposure
monitoring device
82
Figure (4.33) Participants response about safety officers interest with the
devices measurements 83
Figure (4.34) Participants response about availability of new device when
the devices collect to measure of radiation dose 83
Figure (4.35) Participants response about the reasons for lack of personal
radiation exposure monitoring devices 84

xii
List of Annexes
Annex No. Annex Page
Annex (1) Sample size calculator 116
Annex (2) A permission from the Ministry of Health to perform the
study in the governmental hospitals 117
Annex (3) A consent from all participants to ensure their voluntary
participation 118
Annex (4) Arabic version of questionnaire 119
Annex (5) English version of questionnaire 123
Annex (6) Certificate of radiation survey meter (OD-01) calibration 127
Annex (7) The equivalent radiation dose rate measurements 128
Annex (8) Radio-diagnostic machines and rooms specifications data
sheet 135
Annex (9) The questionnaire analysis tables 141

xiii
List of Abbreviations
ALARA As Low As Reasonable Achievable
ANOVA Analysis Of Variance
CT Compute Tomography
DNA DeoxyriboNucleic Acid
EPA Environmental Protection Agency
HW Equivalent radiation dose for whole body
IAEA International Atomic Energy Agency
ICRP International Commission on Radiological Protection
IR Ionizing Radiation
kVp kilovolts peak (unit to describe X-ray tube voltage)
mA milliAmpere (unit to describe X-ray tube current)
MOH Ministry Of Health
MRI Magnetic Resonance Imaging
mSv milliSievert
NCRP National Council on Radiation Protection
PCBS Palestinian Central Bureau of Statistics
SPSS Statistical Package of Social Science
Sv Sievert (unit of effective dose)
UNRWA United Nations Relief and Work Agency
UNSCEAR United Nations Scientific Committee on the Effects of Atomic
Radiation
WHO World Health Organization

xiv
List of Glossary
Diagnostic radiology: the use of X-rays to diagnose disease or injury, or
provide imaging information for medical purposes.
X-ray: Ionizing electromagnetic radiation emitted by an atom when it has been
bombarded with electrons.
Diagnostic X-ray machines: any electronic device that has fast-moving
electrons is a potential source of ionizing radiation.
Radio-diagnostic worker: any person who is employed in diagnostic radiology,
whether full time, part time or temporarily, by an employer, and who has
recognized rights and duties in relation to occupational radiological protection.
Dose: a general term used to refer to the amount of energy absorbed by tissue
from ionizing radiation.
Equivalent dose: a measure of dose in organs and tissues which takes into
account the type of radiation involved. The unit of equivalent dose is J kg-1
, with
the special name Sievert (Sv).
Sievert (Sv): the special name for the SI unit of equivalent dose, effective dose,
and operational dose quantities. The unit is joule per kilogram (J/kg).
Workload: can be classified as quantitative (the amount of work to be done),
workload is a measure of the X-ray tube use.
Stochastic effects: are those in which the probability of the effect occurring
depends on the amount of radiation dose, this type of effects increases as a
radiation dose increases.

1
Chapter 1
Introduction
1.1 Overview
Ionizing radiation has always been a part of the human environment. Natural
background radiation comes from two primary sources: cosmic radiation and
terrestrial sources. The worldwide average background dose for a human being is
about 2.4 milliSievert (mSv) per year (UNSCEAR, 2008). Man-made sources also
contribute to our continuous exposure to ionizing radiation. Ionizing radiation is
radiation with enough energy so that during an interaction with an atom, it can
remove tightly bound electrons from the orbit of an atom, causing the atom to
become charged or ionized. Ionizing radiation has been putting to use in diagnosis of
various diseases and treatment since its discovery in 1895 by Wilhelm Conrad
Rontgen (WHO, 2009).
The use of radiation in medicine has led to major improvements in the diagnosis and
treatment of human diseases. Diagnostic X-rays are the largest man made sources of
radiation exposure to the population contributing to about 14% of the total annual
exposure worldwide from all sources. Although diagnostic X- ray provides great
benefits, but its use carries some risks of developing cancer (Mehta, 2005).
Monitoring of radiation doses received by staff in radiology department is a great
importance (Okaro et al., 2010). The purpose of a radiation monitoring programmed
is to identify all sources of radiation exposure within an operation area, to assess the
level of radiation exposure of the employee and members of the public so that timely
detection of changes in radiation parameters which may lead to increase the
exposures and to produce sufficient information for optimization purpose
(Olowookere et al., 2009).
The decrease in radiation dose of patients and medical staff undergoing diagnostic X-
ray has a significant value. Medical imaging has led to rapid increases in a number of
high dose X-ray examinations performed with significant consequences for

2
individual patient doses and for collective dose to the population as a whole.
Therefore, it is important to make regular assessments of the magnitude of these
large doses in each country (Gonzalez et al., 2004).
The radiological protection principles in practical field, the optimization of
protection and the individual dose limitation should be continuously performed. Dose
limitation for occupationally exposed individuals is necessary to reduce the level of
risk and ensures safety for workers. Knowledge and education have strong direct
effects in technical protection against health hazards associated with radiation
exposures (Mojiri and Moghimbeigi, 2008). It is advisable that assessing radiation
doses received by radiology workers at periodic intervals will ensure their
occupational safety (Ujah et al., 2012).
personal radiation monitoring is essential to ensure that dose limits for staff are not
exceeded. The accepted effective annual dose limits for occupational staff as
reported by the International Commission on Radiological Protection (ICRP) in 1977
was 50 mSv. Public should not be exposed to more than an average of 1 mSv per
year. A downward review was done in 1991 and an effective annual dose limit of 20
mSv was adopted as an average for a period of five years, with the further provision
that the effective dose should not exceed 50 mSv in any single year. The downward
review of annual dose limit was adopted in order to put a stricter control over the use
of ionizing radiation in medicine and minimize possible hazards, especially the
stochastic effects (Ibitoye et al., 2011).
To the best of our knowledge, there is no clear cut off evidence such a work has been
previously performed in Gaza governorates. Therefore, this study was conducted to
measure the ionizing radiation level inside and outside the radio-diagnostic rooms
and evaluation of radiation protection measures at governmental hospitals of Gaza
governorates.

3
1.2 Problem Statement
Recently, tremendous development has taken place in the radio-diagnostic field at
governmental Gaza governorates hospitals. Newer modalities are being applied in
hospitals and latest radiological machines are recently obtained. Besides, there is a
noticeable increase year after year in the frequency of radiological procedures. This
quantitative increase may have a positive impact on the health service system of the
country, but the lack of control can cause serious problem especially radiation hazard
to the radiation workers as well as public (Abbas, 2014, Personal communication).
Due to the increase of the demand on radio-diagnostic examinations, this leads to
increase the exposure of radio-diagnostic workers and patients to ionizing radiation
doses. Long term of ionizing radiation exposures may lead to biological changes and
health problems such as cancer, heritable effects and tissue reactions. Radiation
protection measures evaluation is essential to ensure that dose limits for radio-
diagnostic workers not exceed the permissible limits.
Therefore, this study should be taken seriously into consideration, so as ensure the
safety for a workers and public in governmental hospitals of Gaza governorates. This
would provide helpful recommendations for persons in charge to avoid or reduce the
exposure of workers and the public to medical ionizing radiation.
1.3 Significance
- No previous research is available about ionizing radiation levels inside and
outside of radio-diagnostic rooms at governmental hospitals at Gaza governorates.
- Ionizing radiation protection has been the concern of national and international
bodies. This is due to the potential hazardous effects associated with ionizing
radiation if not properly controlled and long term of ionizing radiation exposures
that lead to biological changes and health problems.
4
- Due to the increase of the frequency of radio-diagnostic procedures year after
year, this leads to increase the ionizing radiation doses to radio-diagnostic workers
and patients.
- In Gaza governorates hospitals, there is no radiation protection program, lack of
clear information about radiation protection measures and guidelines. Therefore,
the study results will help in implementing modification to alleviate risk factors.
In addition, to develop an action plan and new management strategies for
radiation protection enhancements and provide clear information to the decision
makers.
1.4 Justification
Measuring of the equivalent radiation dose rate at different locations in the radio-
diagnostic rooms at the selected nine hospitals. In addition obtain information about
of radio-diagnostic machines and rooms specifications.
Through the study we will get information about the availability of personal radiation
protection devices, awareness and practices regarding radiation protection issues and
evaluation of personal radiation exposure monitoring process as a dependent
variables. However, the socio-demographic and work related factors among radio-
diagnostic workers are independent variables.
The study results also help the planners and decision makers to modify the future
plans regarding radiation protection to be more effective and valuable in improving
the radiation protection knowledge among the radio-diagnostic workers in
governmental hospitals at Gaza governorates.

5
1.5 Objectives
1.5.1 General objective
The general objective of present study is to measure of ionizing radiation level inside
and outside of radio-diagnostic rooms to assess whether yearly equivalent radiation
dose received by the radio-diagnostic workers and public are within the dose limits
recommended by ICRP or not and evaluation of radiation protection measures at
governmental Gaza governorates hospitals.
1.5.2 Specific objectives
1. To identify the dangerous locations in radio-diagnostic centers.
2. To identify the availability of radiation protection devices in the radio-
diagnostic centers.
3. To measure the level of radio-diagnostic workers awareness and practices about
radiation protection issues.
4. To evaluate the personal radiation exposure monitoring process.
1.6 Context of the study
The study was conducted in governmental Gaza governorates hospitals. Therefore,
the context of the study involves some information about the place of study which
include the selected nine governmental hospitals and radio-diagnostic services in
these hospitals. In addition, information about the demographic, population,
socioeconomic, political variables and environmental status in Palestine.

6
1.6.1 Radio-diagnostic services in governmental hospitals of Gaza
governorates
In this section, we display details about the selected nine governmental hospitals and
radio-diagnostic centers according to the Ministry of Health (MOH) records (2013).
The Ministry of Health provides radio-diagnostic services mainly through eleven
hospitals from thirteen hospitals.
All of the eleven hospitals provide Ultrasound (U/S), routine X-ray, while four of
these hospitals have CT scan units, three hospitals have mammography units and
only two hospitals have panorama units. Magnetic Resonance Imaging (MRI) which
is a non-ionizing imaging unit is not available expect in one hospital.
According to the records of hospitals directorate general, about 554529 radio-
diagnostic procedures were done in 2013; of them 438016 routine X-ray procedures
and 2276 fluoroscopy procedures, 26407 CT scan procedures, 1474 panorama
procedures and 564 mammography procedures. This is a highly burden to the
workers and diagnostic machines. Thus, we have selected a nine governmental
hospitals in order to measure the equivalent radiation dose rate in different locations
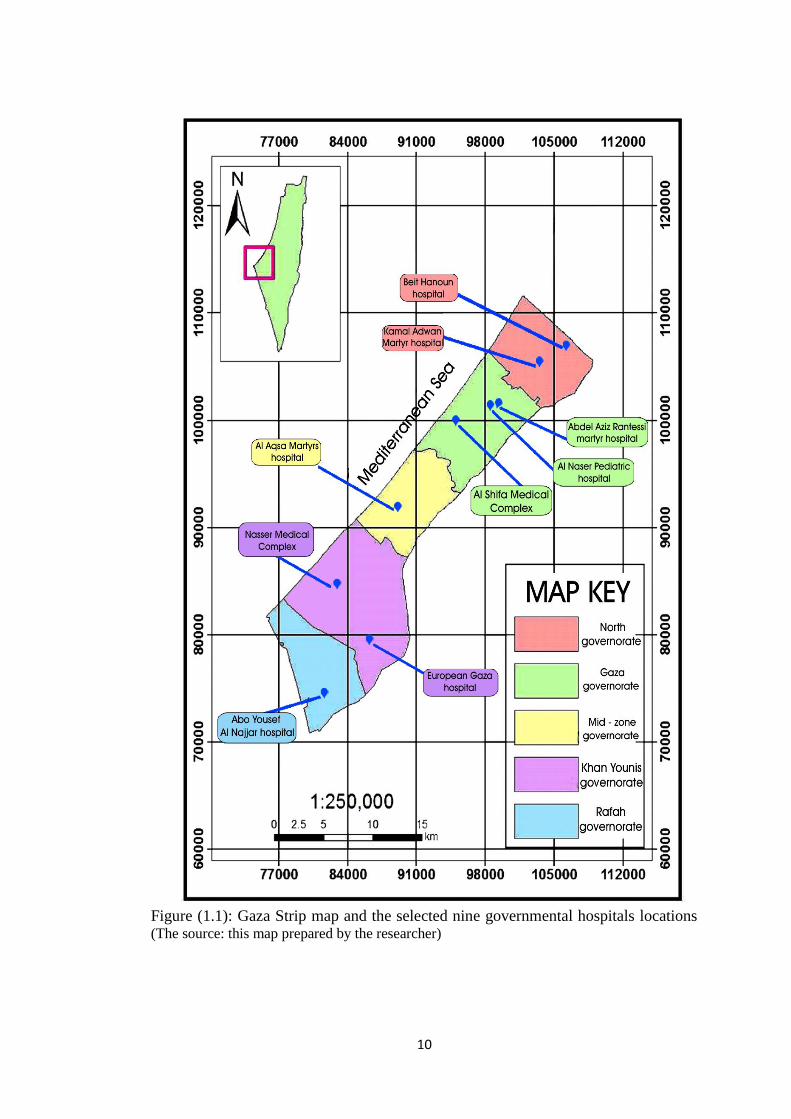
in radio-diagnostic rooms. Figure (1.1), illustrates Gaza Strip map and the selected
nine governmental hospitals locations.
1. Radio-diagnostic services in Al Shifa Medical Complex
Al Shifa Medical Complex is located in Gaza city, Gaza governorate. It includes
three hospitals: the surgery hospital, internal medicine hospital and obstetrics and
women hospital. The total clinical capacity is about 500 beds. Radio-diagnostic
center in Al Shifa Medical Complex includes: six basic X-ray, one CT scan, two
fluoroscopy, one mammography, one panorama, three portable C-Arm and some of
portable X-ray machines. This center provides approximately 169969 medical
imaging procedures per year. Fifty medical radiographers and fourteen radiologists
working in the center.

7
2. Radio-diagnostic services in Nasser Medical Complex
Nasser Medical Complex is located in Khan Younis city, Khan Younis governorate.
It contains two hospitals: Nasser and Mubarak hospitals. It is provides medical,
surgery, radiological, children and obstetrics and women services. The total clinical
capacity about 258 beds. Radio-diagnostic center in Nasser Medical Complex
includes: two basic X-ray, one CT scan, one mammography, one fluoroscopy, one
panorama, one portable C-Arm and some of portable X-ray machines. This center
provides approximately 82241 medical imaging procedures per year. Twenty eight
medical radiographers and six radiologists working in the center.
3. Radio-diagnostic services in European Gaza hospital
The European Gaza hospital is located in Khan Younis city, Khan Younis
governorate. It provides medical, surgical, pediatric and radiological services. The
total clinical capacity is about 207 beds. Radio-diagnostic center in European Gaza
hospital includes: two basic X-ray, one CT scan, one mammography, one
fluoroscopy, one fluoroscopic lithotripsy, two portable C-Arm and some of portable
X-ray machines. This center provides approximately 66980 medical imaging
procedures per year. Twenty seven medical radiographers and eight radiologists
working in the center.
4. Radio-diagnostic centers in Abu Yousef Al Najjar hospital
Abu Yousef Al Najjar Martyr hospital is located in Rafah governorate, southern
borders of Gaza Strip. It provides medical, surgical, pediatric and radiology services.
The total clinical capacity is 40 beds. Radio-diagnostic center in Abu Yousef Al
Najjar hospital includes: two basic X-ray, one fluoroscopy, one portable C-Arm and
some of portable X-ray machines. This center provides approximately 43628 medical
imaging procedures per year. Sixteen medical radiographers and three radiologists
working in the center.

8
5. Radio-diagnostic services in Kamal Adwan Martyr hospital
Kamal Adwan Martyr hospital is located in Jabalya refugee camp, North Gaza
governorate. It provides surgical, pediatrics, radiological and medical services. The
total clinical capacity is about 73 beds. Radio-diagnostic center in Kamal Adwan
Martyr hospital includes: two basic X-ray, one fluoroscopy machine, two Portable C-
Arm and some of portable X-ray machines. This center provides approximately
70733 medical imaging procedures per year. Sixteen medical radiographers and three
radiologists working in the center.
6. Radio-diagnostic services in Al Aqsa Martyrs hospital
Al Aqsa Martyrs hospital is located in Dier El Balah city, Mid-Zone governorate. It
provides medical, surgical, pediatric, radiological and women obstetrics services, the
clinical capacity is about 103 beds. Radio-diagnostic center in Al Aqsa Martyrs
hospital includes: one basic X-ray, one fluoroscopy, two portable C-Arm and some
of portable X-ray machines. This center provides approximately 53967 medical
imaging procedures per year. Sixteen medical radiographers and five radiologists
working in the center.
7. Radio-diagnostic services in Abdel Aziz Rantessi Martyr Pediatric hospital
Abdel Aziz Rantessi Martyr Pediatric hospital is located in Gaza city, Gaza
governorate. It provides specialized medical services for children. The total clinical
capacity of current operating stage is about 49 beds. Radio-diagnostic center in
Abdel Aziz Rantessi Martyr pediatric hospital includes: one fluoroscopy, one CT
scan and some of portable X-ray machines. This center provides approximately
12377 medical imaging procedures per year. Eleven medical radiographers and two
radiologists working in the center.

9
8. Radio-diagnostic services in Al Naser Pediatric hospital
Al Naser Pediatric hospital is located in Gaza city, Gaza governorate. It provides
pediatric services. The total clinical capacity is about 151 beds. Radio-diagnostic
center in Al Naser hospital includes: one basic X-ray and one fluoroscopy and some
of portable X-ray machines. This center provides approximately 21654 medical
imaging procedures per year. Twelve medical radiographers and three radiologists
working in the center.
9. Radio-diagnostic services in Beit Hanoun hospital
Beit Hanoun hospital is located in Beit Hanoun, North governorate. It provides
surgical, pediatric and medical services, the total clinical capacity is about 36 beds.
The clinical capacity is a total of 500 beds. Radio-diagnostic center in Beit Hanoun
hospital includes: one basic X-ray machine and some of portable X-ray machines.
This center provides approximately 16710 medical imaging procedures per year.
Eight medical radiographers and radiologists working in the center.
10
Figure (1.1): Gaza Strip map and the selected nine governmental hospitals locations
(The source: this map prepared by the researcher)

11
1.6.2 Demographic context
Palestine has an important geographical and strategic location in Middle East.
Palestine is surrounded by Lebanon, Syria, Egypt, and Mediterranean Sea. The total
surface area of the historical Palestine is about 27.000 Km2 (Palestine, MOH, 2006).
Palestine has been occupied in 1948 by Israel and the two remaining parts are
separated geographically (West Bank [WB] and Gaza Strip [GS]) after the war in
1967 (Palestine, MOH, 2006).
Gaza Strip an elongated zone located on the southeastern coast of Palestine with
coordination of Latitude N 31° 26' 25" and Longitude E 34° 23' 34". The area is
bounded by the Mediterranean in the west, the 1948 cease-fire line in the north and
east and by Egypt in the south. The total area of the Gaza Strip was 365 km2 with
approximately 40 km long and the width varies from 8 km in the north to 14 km in
the south (UNEP, 2003).
1.6.3 Gaza Strip population
Gaza governorates is a highly crowded populated area, where approximately
1,853,000 people live in 365 km2, of them 49.33% males and 50.67% females. The
estimated density is 4,000 people per square kilometer distributed across five
governorates. Gaza Governorates are classified into five governorates: North Gaza
governorate, Gaza governorate which is the biggest governorate, Mid-Zone
governorate, Khan Younis governorate and Rafah governorate. Table (1.1),
illustrated the distribution of people into Gaza governorates. The majority of people
live in refugee camps (PCBS, 2014).
This high population density in Gaza Strip increases the over load on the hospitals
care which stress on the great need for proving the diagnostic radiology services in
governmental hospitals of Gaza governorates.

12
Table (1.1): Population distribution in Gaza governorates [PCBS, 2014]
Governorate Population number Percentage
North Gaza 302,000 16.3%
Gaza 700,000 37.8%
Mid-Zone 260,000 14%
Khan Younis 360,000 19.4%
Rafah 231,000 12.5%
Total 1,853,000 100%
1.6.4 Socioeconomic and political context
The Palestinian economy refers to the economy of Palestinian territory, including
GS, WB and East Jerusalem (PCBS, 2009). Due to the recent political changes that
facing the GS, a very bad socio-economic situations is happened. This gives rise a
profoundly negative impact on the public health and access to basic health services.
Nowadays, 80% of families in GS currently depend on humanitarian aid. This
decline results from exceptional levels of poverty and the inability of a large majority
of the population to provide basic food (Human Rights Council, 2013). Thus, the
overall bad economic status of the Palestinians in GS increasing the load on the
governmental hospitals to provide secondary care especially in case of emergency
and violence.
1.6.5 Environmental status
Palestinian environment is experiencing from serious threats such as (Poor quality
and quantity of the water, depletion of natural resources, destruction of the land and
soil erosion, air pollution and noise, pollution of the coast and marine environment,
decline of the natural environment and biodiversity, distortion of the landscape and
threat of Palestinian heritage and historical legacy). However, handling of hazardous
waste and infectious waste mixed up with solid waste is a critical problem which
causes environmental and health risks in the Palestinian Territories (UNEP, 2013).

13
The ignorance of the ongoing environmental issues throughout the years of
occupation, which is the main reason of many environmental disasters.
Environmental problems are aggravated because of the frequent Israeli closures of
the West Bank and the Gaza Strip; they cause disabling economic and population
activities and paralyzing production and construction tools, which increases pollution
problems in every city and village in the West Bank and Gaza Strip (Palestine News
& Info Agency - WAFA, 2014).
1.7 Cancer in Palestine
Cancer is a leading cause of death in all parts of the world, the disease has caused the
deaths of 7.6 million people (about 13% of all deaths) in 2013, the world records
annually more than 11 million new cases of cancer (IARC, 2014).
Palestinian Ministry of Health confirmed that the incidence of cancer in the
Palestinian territories within the global average. The number of cancer cases
recorded in the years 1998 and 1999 in the Gaza Strip and the West Bank and East
Jerusalem, reached 3474 case where the score in the occupied Palestinian territories
more than 1,700 new cases of cancer each year, and is the incidence of cancer is 11
per cent among children of the total number of new cases recorded annually in
Palestine. Cancer considered as a leading cause of death in the Palestinian territories.
In the year 2010 cancers formed the third cause of death in Palestine (MOH, 2013).
The new cancer cases in the Palestinian territories between the 2005 and 2010 were
estimated about 1623 case, with incidence rate of 43.1 cases per 100.000 people, of
whom 49.2 cases per 100.000 people in West Bank and 32.7 cases per 100,000
people in the Gaza Strip (MOH, 2013).
Ministry of Health reported that, since 1998, established the Palestinian Ministry of
Health at the time the National Cancer Registry, where, it is clear from this record, it
is recorded annually among children under the age of 15 years, about 65 children as
new patients with cancer, noting that 49 per cent of the population in the Gaza Strip

14
under the age of 15 years, so has the incidence of cancer among children aged less
than 15 years in the Gaza Strip, 13.2 per 100 thousand inhabitants (15.5 for males
and 10.9 for females). While the number of deaths from cancer among children under
the age of 15 years in the Gaza Strip, about 30 cases a year, which accounted for 9
per cent of the annual total of deaths registered in the Gaza Strip as a result of cancer.
More than 50% of the new cases registered in Palestine are in the age group of 60
years and older
The trachea , bronchus and lung cancer is the highest cause to deaths among cancer
mortality. The incidence of cancer is higher for female than male. The breast cancer
is the highest among female Palestinian population and lung cancer is the highest
among male Palestinian population (MOH, 2014).
The rate of incidence of cancer in the Hashemite Kingdom of Jordan, for example, to
64 cases per 100 thousand inhabitants. While estimated number of people diagnosed
with cancer in Egypt by about one hundred thousand patients a year (WHO, 2013).

15
Chapter 2
Literature Review
2.1 Introduction
In this chapter, we present the study conceptual framework, then a discussion of the
different issues about ionizing radiation such as radiation sources, types of
individuals’ exposure, ionizing radiation dose and units, medical use of ionizing
radiation, radiation protection principles and techniques, ionizing radiation
monitoring and biological effects of ionizing radiation. In the last section of this
chapter, we present many studies related to ionizing radiation leakage evaluation and
radiation protection measures in radio-diagnostic centers.
2.2 Conceptual framework
Based on the review of available literature, we have designed the conceptual
framework. This is used to guide the research process and to make research finding
more meaningful. A schematic representation of the framework of the present study
is mentioned in figure (2.1). The tools of the study included radiation survey meter
(OD-01) were used to measure the equivalent radiation dose rate at different
locations in the radio-diagnostic rooms and the data sheet information collected from
radio-diagnostic machines and rooms in nine selected governmental Gaza
governorates hospitals. In addition, the questionnaire were used to obtain information
about the availability of personal radiation protection devices, awareness and
practices regarding radiation protection issues and evaluation of personal radiation
exposure monitoring process as a dependent variables. However, the socio-
demographic and work related factors among radio-diagnostic workers are
independent variables.
Ionizing radiation: is radiation with enough energy remove tightly bound
electrons from the orbit of an atom, causing the atom to become charged or
ionized (WHO, 2009).

16
Radiation protection: is the science of protecting the human population and the
environment from the harmful effects of ionizing radiation. This includes both
particle radiation and high energy electromagnetic radiation (Radiation protection
manual, 2010).
Safety measures: the measures taken when working with sources of ionizing
radiation to reduce the total dose from all types of ionizing radiation to maximum
permissible dose (Directive Council, 1996)
Radio-diagnostic centers: a places that offers diagnostic services to medical
profession or general public (Brant and Helms 2012).
Governmental hospitals: are hospitals affiliated with the Palestinian Ministry of
Health administratively, financially and technically; they provide health services
to all members of the community who have health valid insurance card (MOH,
2014).
Awareness: is the capacity to acquire, retain and use information; a mixture of
comprehension, experience, discernment and skill (Badran, 1995).
Device: is any physical item that can be used to achieve a goal, especially if the
item is not consumed in the process. Radiation protection devices are a tools made
of lead used to protect patients and staffs from ionizing radiation include: aprons,
thyroid shields, eyewear, lead curtains, and gloves (Klein et al., 2009).
Practice: means the application of rules and knowledge that leads to action.
Good practice is an art that is linked to the progress of knowledge and technology
and it’s executed in an ethical manner (Badran, 1995).
personal radiation exposure monitoring: is an important safety precaution in
the practice of radiography. Its main purpose is to measure radiation dose received

17
by radiology personal, which can indicate that radiation doses received are within
permissible limits, verify that facilities for radiation protection are adequate and
show that radiation protection techniques are acceptable (The University of
Western Australia, 2010).
Figure (2.1): Schematic representation of the study framework
Ionizing radiation leakage and radiation protection
measures in radio-diagnostic centers at
governmental Gaza governorates hospitals
Socio-demographic and work related factors
Age, sex, occupation, academic qualification,
experience, type of machine and daily work
hours
Practices Devices Awareness
Personal radiation
exposure monitoring

18
2.3 Ionizing radiation
Ionizing radiation (IR) is electromagnetic radiation that has sufficient energy to
remove electrons from atoms (WHO, 2009). Ionization results in the production of
negatively charged free electrons and positively charged ionized atoms (EPA, 2007).
IR can be classified into two categories: photons (X-ray and γ- radiation) and
particles (α and β particles and neutrons) (UNSCEAR, 2006).
X-ray is a form of short wavelength electromagnetic radiation which will penetrate
all organs of the body and are a significant external radiation hazard. The energy of
the X-ray photons is an important factor in determining the magnitude of the external
radiation hazard (Burnham, 2001). Most X-rays have a wavelength in the range of
0.01 to 10 nanometers, corresponding to frequencies in the range 30 petahertz to
30 exahertz (3×1016
Hz to 3×1019
Hz) and energies in the range 100 eV to 100 keV
X-ray is emitted by electrons, they can be generated by an X-ray tube, a vacuum
tube that uses a high voltage to accelerate the electrons released by a hot cathode to a
high velocity. The high velocity electrons collide with a metal target, the anode,
creating the X-rays (Whaites et al., 2002).
In contrast, artificial radiation sources have only been introduced in the last 100
years and although many benefits and it has been realized that exposure to these
sources can be harmful to us (IAEA, 2007).
2.4 Natural ionizing radiation sources
Throughout history, human beings are exposed to natural radiation. It is impossible
to decide whether this radiation has been harmful or beneficial to the human species
(IAEA, 2007). Radioactive material is found throughout nature in soil, rocks, water,
air, and vegetation from which it is inhaled and ingested into the body. Humans also
receive external exposure from radioactive materials that remain outside the body
and from cosmic radiation from space (UNSCEAR, 2008).

19
Ionizing radiation is present naturally in the environment from cosmic and terrestrial
sources. Cosmic radiation primarily consists of positively charged ions from protons
to iron and larger nuclei derived sources outside our solar system. This radiation
interacts with atoms in the atmosphere to create an air shower of secondary radiation,
including X-rays, protons, alpha particles, electrons, and neutrons (Feng, 2002). The
second source of natural IR is the terrestrial radiation "earth radiation'' which
includes radiation from the soil, rocks, and building materials such as radionuclides
in granite, stones, sandstone, limestone, where its amount varies geographically
(NAS, 2006).
Radon is a radioactive gas that emanates from the ground. Radon and its isotopes,
parent radionuclides, and decay products all contribute to an average inhaled dose of
1.26 mSv/yr. Radon is unevenly distributed and varies with weather, such that much
higher doses apply to many areas of the world, where it represents a significant
health hazard (UNSCEAR, 2008). Through decay of radon, it produces α and β
radiations. It enters homes through the cracks in floors and walls or building
materials which may contain radio nuclides (WHO, 2004).
2.5 Artificial ionizing radiation sources
People are also exposed to artificial radiation from medical treatments and activities
involving radioactive material. Radioisotopes are produced as a by-product of the
operation of nuclear reactors, and by radioisotope generators like cyclotrons. Many
man-made radioisotopes are used in the fields of nuclear medicine, biochemistry, the
manufacturing industry and agriculture (UNSCER, 2006).
Medical use of IR in both diagnosis and therapy has been widespread since the
discovery of X-rays by Wilhelm Conrad Roentgen in 1895, and radioactive sources
have been used in radiotherapy since 1898. Advances in the latter half of the 20th
century increased the use of medical radiation, and some newer techniques,
particularly radiotherapy, computed tomography, positron emission tomography, and

20
interventional radiation involving fluoroscopy, use higher radiation doses than do
standard diagnostic X-rays. Radiation therapy may involve use of external beams of
radiation, typically high-energy X-rays 4 to 50 MeV and low-energy cobalt-60
gamma rays 1-2 MeV (UNSCEAR, 2006).
Several industrial processes use ionizing radiation. Industrial radiography uses
gamma radiation to examine welded joints in structures. In the oil industry, gamma
radiation or neutron sources are used to determine the geological structures in a bore
hole (NCRP, 1989).
Ionizing radiation is also used to sterilize products and irradiate foods to kill bacteria
and parasites. Military uses of materials and processes that emit X-radiation and
gamma radiation include the production of materials for nuclear weapons and the
testing and use of nuclear weapons (IARC, 2000).
2.6 Types of individual exposure to ionizing radiation
The ICRP refers to three types of exposure individual; occupational exposure is the
exposure of a person in the workplace and mainly as a result of the work they
perform; medical exposure is the exposure of a person as part of a medical diagnosis
or treatment; public exposure is the exposure of a person by means other than
occupational or medical exposure (ICRP, 2008).
2.7 Ionizing radiation dose and units
The radiation dose is the amount of energy absorbed in the body from radiation
interactions. Early non quantitative measures of dose, based on skin erythema, were
replaced by measures of exposure [e.g. the ability of X-rays to ionize air, measured
in roentgens (R)] and measures of absorbed dose [e.g. energy absorption, measured
initially in radiation absorbed dose (Rad), and more recently in Gray (Gy)] (Hall and
Giaccia, 2006).

21
Different types of radiation may produce different biological effects and the
magnitude of the effect can vary according to the rate at which radiation is received
(dose rate). The dose rate is a primary factor in determining the biological effects of
a given absorbed dose. For example, as the dose rate is reduced and the exposure
time extended, the biologic effect of a given dose is generally reduced. Relative
biological effectiveness, which denotes the ability of a given type of radiation to
produce a specific biological outcome compared with X-rays or gamma rays, is taken
into account by the Sievert (Sv), a metric for biological equivalent dose that can be
used to measure mixed types of radiation exposure (ICRP, 1991 and ICRP, 2007).
The effective dose is the sum of the equivalent doses to each tissue and organ
exposed multiplied by the appropriate tissue weighting factor or, in other words, the
whole body dose of X-rays that would have to be delivered to produce the same
carcinogenic risk as the partial dose that was delivered. This quantity provides an
easy assessment of overall risk and makes the comparison of risks much simpler.
Although effective dose is emphasized in many surveys because this metric is related
to the risk of carcinogenic effects, effective dose cannot be measured and cannot be
used for individual risk assessment. Only absorbed dose to a given tissue or organ
can be used for estimating cancer risks (ICRP, 1991 and ICRP, 2007).
2.8 Medical uses of ionizing radiation
Ionizing radiation has two very different uses in medicine for diagnosis and therapy.
Both are intended to benefit patients and, as with any use of radiation, the benefit
must outweigh the risk (IAEA,2007).
2.8.1 Radio-therapy
Radiation therapy use high energy ionizing radiation to shrink tumors and kill cancer
cells. X-ray, gamma ray , and charged particles are types of radiation used for cancer
treatment. The radiation may be delivered by a machine outside the body called
external-beam radiation therapy, or it may come from radioactive material placed in

22
the body near cancer cells called internal radiation therapy, also called brachytherapy
(Lawrence et al., 2008).
2.8.2 Radio-diagnostic
Diagnostic radiography involves the use of both ionizing radiation and non-ionizing
radiation to create images for medical diagnoses (Bushberg et al., 2001).There are a
variety of imaging techniques such as nuclear medicine, X-ray radiography,
computed tomography (CT) scan, fluoroscopy, mammography, dental X-ray,
interventional radiology, ultrasound and magnetic resonance imaging (MRI) to
diagnosis of diseases (CSPH, 2006 and UNSCEAR, 2000).
2.8.2.1 Nuclear medicine
In diagnostic nuclear medicine, radiopharmaceuticals are given to patients where it
is administered either by injection, inhalation or ingestion. The type of
radiopharmaceutical is chosen according to the examined organ or tissue. These
radiopharmaceuticals emit γ rays which are detected by Gamma camera such as
sodium iodide and give a picture about the examined organ (Shrimpton, 2001,
Burnham, 2001, IAEA, 2004).
2.8.2.2 Diagnostic X-ray
Diagnostic X-ray increase the risk of developmental problems and cancer in those
exposed (Santis et al., 2007; Hall and Brenner, 2008 and Brenner, 2010).The amount
of absorbed radiation depends upon the type of X-ray examination and the body part
involved. CT scan and fluoroscopy entail higher doses of radiation than do plain X-
ray (Hall and Brenner , 2008).
Fluoroscopy is an imaging technique commonly used by physicians or radiation
therapists to obtain real-time moving images of the internal structures of a patient
through the use of a fluoroscope (Balter et al., 2010). Fluoroscopic examinations also

23
vary according to the types of exams. Most of the fluoroscopy examinations give an
effective dose higher than that for radiography examinations. Barium meal, which is
an examination for stomach, gives an effective dose of about 3 mSv. Barium enema
which is an examination for the large bowl, gives a higher effective dose of about 7
mSv (Hart and Wall, 2002), it is equal to the exposure to natural IR through 2 to 3
years (FDA, 2007).
Computed tomography scan (CT) is a medical imaging modality where tomographic
images or slices of specific areas of the body are obtained from a large series of two-
dimensional X-ray images taken in different directions. These cross-sectional images
can be combined into a three-dimensional image of the inside of the body and used
for diagnostic and therapeutic purposes in various medical disciplines (Herman and
Gabor, 2009). CT scan examinations expose patients to dose larger than any other
diagnostic radiology examinations (Golding and Shrimpton, 2002).
The effective dose to the spinal cord from a CT scan of the chest is about 5 mSv, and
the absorbed dose is about 14 mGy (Caon et al., 2000). A head CT scan (1.5 mSv, 64
mGy) that is performed once with and once without contrast agent, would be
equivalent to 40 years of background radiation to the head (Shrimpton et al., 2001).
Dosage due to dental X-rays varies significantly depending on the procedure and the
technology (film or digital). A single dental X-ray of human results in an exposure of
0.5 to 4 mRem. A full mouth series may therefore result in an exposure of up to 6
(digital) to 18 (film) mSv, for a yearly average of up to 40 mRem (Muller, 2010).
Mammograms require very small doses of radiation. The risk of harm from this
radiation exposure is extremely low, usually around 0.4 mSv to examine the human
breast, while the average annual dose from food is 0.3 mSv, the average yearly
background dose is 2.4 mSv (Biller, 2014).

24
2.9 Radiation protection
Radiation protection is defined as the science and practice of reducing harm to
human beings from radiation. In all radiological activities it is important to have
some idea of the risk associated with the use of ionizing radiation (IAEA, 2007).
Occupational radiation protection measures are necessary for all individuals who
work in the diagnostic imaging departments, radiology staffs require appropriate
monitoring continuously by common personal dosimeters like film badge and
thermo-luminescence dosimeter. They must also receive education and training
appropriate to their jobs and protect by tools and equipment (Rahman et al., 2008).
The accepted effective annual dose limits for occupational staff as reported by the
International Commission on Radiological Protection (ICRP) in 1977 was 50 mSv.
Public should not be exposed to more than an average of 1 mSv per year. A
downward review was done in 1991 and an effective annual dose limit of 20 mSv
was adopted as an average for a period of five years, with the further provision that
the effective dose should not exceed 50 mSv in any single year. The downward
review of annual dose limit was adopted in order to put a stricter control over the use
of ionizing radiation in medicine and minimize possible hazards, especially the
stochastic effects (Ibitoye et al., 2011).
2.9.1 Radiation protection principle
The radiation protection principles of justification, optimization and dose limitation
are applied to radiation protection in medicine (Street et al., 2009).
2.9.1.1 Justification
The referring medical practitioner is responsible for ensuring that a diagnostic
procedure involving ionizing radiation is necessary for a patient’s care and that the
radiation dose from the procedure is expected to do more good than harm, a concept

25
designated as justification by the ICRP (ICRP, 2007). Justification and
appropriateness of medical exposures will help reduce the imaging costs and the dose
received by the patient. However, studies under taken in some countries (Oikarinen
et al., 2009; Brenner and Hricak, 2010).
2.9.1.2 Optimization
The radiological medical practitioner is responsible for ensuring that the radiological
procedure provides images adequate for diagnosis and treatment while keeping the
radiation dose as low as reasonably achievable (ALARA), a concept designated as
optimization by the ICRP (ICRP, 2007). Dose optimization recognizes the potential
risk of any radiation and emphasizes the need for appropriate dose management for
all imaging procedures (Balter and Moses, 2007 and Stecker et al., 2009).
2.9.1.3 Individual dose limits
All medical applications of ionizing radiation must be managed in such a way that
radiation doses to occupationally exposed persons and members of the public do not
exceed the dose limits. Dose limits do not apply to the exposure of patients as part of
their diagnosis or treatment (Street et al., 2009).
2.9.2 Radiation protection techniques
There are three basic methods that control the amount of radiation dose received
from a source. Radiation exposure can be managed by a combination of these
methods: the first is the exposure time; reducing the time of an exposure is an
important method for reducing the exposure to ionizing radiation. The second
radiation protection method relates to the distance between the source of radiation
and the exposed individual, where the Radiation intensity decreases sharply with
distance, according to an inverse-square law. The third method which helps in
reducing the received dose for both patient and the staff is the shielding, which is a
material, as lead, that attenuates radiation when it is placed between the source of

26
radiation and the exposed individual. Hence, shielding strength or "thickness" is
conventionally measured in units of g/cm2. The radiation that manages to get through
falls exponentially with the thickness of the shield. In X-ray facilities, walls
surrounding the room with the X-ray generator may contain lead sheets, or the
plaster may contain barium sulfate. Almost any material can act as a shield from
gamma or X-rays if used in sufficient amounts (Lawrence, 2008 and Occupational
Safety and Health council, 2006).
2.9.3 Radiation monitoring
Radiation monitoring is an important safety precaution in the practice of
radiography. It does not in itself provide protection against ionizing radiations. Its
main purpose is to measure radiation dose received by radiology personnel, which
can indicate that radiation doses received are within permissible limits, verify that
facilities for radiation protection are adequate and show that radiation protection
techniques are acceptable (The University of Western Australia, 2010).
2.9.3.1 Personal radiation monitoring in radio-diagnostic centers
Monitoring of radiation doses received by staff in radiology department is of great
importance in efforts to protect themselves from the effect of excessive radiation
during and after radiological examinations of patients (Okaro et al., 2010). It is
advisable that assessing radiation doses received by radiology workers at periodic
intervals will ensure their occupational safety. That is the radiations exposure to a
staff are within the internationally accepted safe limits (Ujah et al., 2012).
The common devices recommended for measuring of dose rate of radiation received
by radiation workers are; Thermo-luminescence dosimeters (TLD), film badges and
pocket ionization dosimeters, etc. Okpala (2004) reported that every radiology
worker is expected to wear dosimeters always while working. The dosimeter
readings are kept as records for every staff for the purpose of evaluating their

27
radiation history and possible risks that would be involved. These records help in
improving radiation practices in radiology department.
Radiation badges are essential monitoring gadgets that must be applied and received
before starting work involving radiation exposure. Also, personal dosimetric record
and monitoring are integral parts of radiography practice in the world (Washington
State University, 2000). Dosimetric records are kept and are required to be disclosed
when workers change jobs (Jean, 1998).
2.9.3.2 Ensuring effective radiation protection of medical staff
Radiation protection programmed (RPP) is one means of implementing occupational
radiation protection by the adoption of appropriate management structures, policies,
procedures and organizational arrangements. For medical staff in X-ray imaging,
topics would include the need for local rules and procedures for personal to follow,
arrangements for the provision of personal protective tools, a programmed for
education and training in radiation protection, arrangements for individual
monitoring, and methods for periodically reviewing and auditing the performance of
the RPP (IAEA, 2006).
2.9.4 Personal radiation protection devices
Personal protective devices include aprons, thyroid shields, eyewear, lead curtains,
and gloves. Protective aprons with thyroid shields are the principal radiation
protection devices for radiology workers. They should be employed at all times. The
vest or skirt configuration is preferred by many operators in order to reduce the risk
of musculoskeletal back injury (Klein et al., 2009). This wrap-around style is
typically 0.25 mm lead-equivalent so that, when worn, the double thickness
anteriorly provides 0.5 mm lead equivalence. Operators and staff who work in the
radiology on a regular basis should be provided with properly fitted aprons, both to
reduce ergonomic hazards and to provide optimal radiation protection (Detorie et al.,
2007).

28
Aprons should be inspected fluoroscopically on an annual basis to detect
deterioration and defects in the protective material (Christodoulou et al., 2003).
Because of the ergonomic hazards of personal protective tools (particularly leaded
aprons), attempts to reduce the fatigue and injury associated with wearing heavy
protective apparel have been made (Klein et al., 2009).
The principal disadvantage of leaded eyeglasses is their weight and discomfort. In
general, the operator’s hands should be kept out of the primary radiation beam.
Leaded gloves may seem useful for radiation protection on those rare occasions
when the operator’s hands must be in the primary radiation beam, but they do not
provide protection in this situation. Because of the increased dose when any
shielding is placed in the primary beam, and the false sense of security that these
gloves provide, protective gloves can result in increased radiation dose to the hand
when the gloved hand is in the primary beam, leaded gloves are not recommended in
this situation. The best way to protect the operator’s hands is to keep them out of the
radiation field. Leaded gloves may be of benefit if the operator’s hands will be near,
but not in, the primary radiation beam (Wagner and Mulhern, 1996).
2.9.5 Radiation protection training
Education and training should be implemented to radiation protection in practice, and
most countries have regulatory requirements for such training. In X-ray imaging,
personal need training not only in occupational radiation protection, but also
inpatient radiation protection as the latter can influence occupational exposure
(European Commission, 2000).
2.10 The use of radiation for medical exposure
The use of radiation in medical applications continues to increase worldwide. Latest
UNSCEAR estimates suggest that there are about 4 billion X-ray examinations per
year, worldwide (UNSCEAR, 2008). Table (2.1), displays the time evolution through

29
two decades, from 1988 to 2008, of the number of medical radiological procedures
and the effective dose per capita, worldwide.
As is clearly seen, the number of radiological procedures more than doubled whilst
the annual effective dose per inhabitant almost doubled. Similar but more
pronounced trend scan be seen in the report NCRP-160 (NCRP, 2009), for the USA,
that pinpoints a significant increase of the population exposure to ionizing radiation
due to the medical applications of ionizing radiation, namely CT, nuclear medicine,
and interventional procedures.
In the USA the number of prescribed CT scans grew by approximately10% per
annum from the 1990s until the middle of the last decade (Bfs, 2010) pinpointing the
major role played by the increasing frequency of CT exams in the significant
increase of the mean effective dose per inhabitant.
Table (2.1): Time evolution of the number of radiological procedures, collective dose
and annual dose per capita, worldwide (UNSCEAR, 2008).
UNSCEAR
Report
No. of
examinations
(Billion)
Collective Dose
(Million man*Sv)
Annual dose
"per capita"
(mSv)
1988 1.38 1.8 0.35
1993 1.6 1.6 0.3
2000 1.91 2.3 0.4
2008 3.1 4.0 0.6
More people are exposed to ionizing radiation from medical practice than from any
other human activity, and in many cases, the individual doses are higher. In countries
with advanced healthcare systems, the annual number of radiological diagnostic
procedures approaches or exceeds 1 for every member of the population
(UNSCEAR, 2000). Furthermore, doses to patients for the same type of examination
differ widely between centers, suggesting that there is considerable scope for
management of patient dose (UNSCEAR, 2000). The use of radiation for medical
exposure of patients contributes over 95% of man-made radiation exposure and is
only exceeded world-wide by natural background as a source of exposure
(UNSCEAR, 2000).

30
Overall, medical exposure has increased since the UNSCEAR, (2000) evaluation,
largely due to the rapid increase in the utilization of computed tomography (CT),
both in industrialized and in developing countries (ICRP, 2006 and ICRP, 2007).
Worldwide, the estimated number of medical and dental radiographic machines is
approximately 2 million. While it is difficult to estimate the number of
occupationally exposed medical workers, UNSCEAR, (2000) estimated that there are
more than 2.3 million monitored medical radiation workers.
2.11 Biological effects of ionizing radiation
Almost twenty years after the initial discovery of X-rays by Wilhelm Conrad
Roentgen in 1895, the Drosophila geneticist Herman Muller demonstrated that
ionizing radiation causes mutations in living organisms. In the 80 years since that
discovery, the biological and genetic consequences of exposure to ionizing radiation
(IR) have been investigated. The biological effects of IR exposure are mediated
through direct damage to biomolecules (e.g., energy directly deposited on the
molecule) or indirectly through the formation of Reactive Oxygen Species (ROS)
(Muller, 1927).
The biological effects of radiation can be grouped into two types: Stochastic effects
(cancer and heritable effects) and Deterministic effects (tissue reactions) (ICRP,
2007).
The first type is stochastic effects (no threshold dose): are those in which the
probability of the effect occurring depends on the amount of radiation dose, this type
of effects increases as a radiation dose increases. So, there is no threshold dose for
the stochastic effect. Stochastic effects can cause cancer, or have influence on gene-
material affecting future generations (NOHSC, 2002 and EPA, 2009).
The second type is deterministic effects (threshold dose): are those effects resulting if
the effect only results when many cells in an organ or tissue are killed, the effect will

31
only be clinically observable if the radiation dose is above some threshold. The
magnitude of this threshold will depend on the dose rate (i.e. dose per unit time),
linear energy transfer of the radiation, the organ or tissue irradiated, the volume of
the irradiated part of the organ or tissue, and the clinical effect of interest. These
effects occur because of large number of killed cells which cannot be compensated.
The degree of damage (severity) increases the more the threshold value is exceeded
(ICRP, 2007 and EPA, 2009).
The single largest contributor of manmade radiation is the medical profession. The
effects of ionizing radiation on a given population are generally divided into two
categories, acute and chronic. The acute effects are considered to be those which
happen in the immediate post irradiation periods, i.e. from the time of radiation
exposure up to 6 months to a year post exposure. Acute effects are generally the
result of long radiation exposure delivered to the whole body, or at least a major port
of it, in average short time, on the other hand the chronic effects of radiation results
from relatively low exposure levels delivered over long periods of time. Therefore
long time effects of low doses seems to be the main risk factor and that might results
from occupational exposure (Morgan, 2003).
2.12 Previous studies related to this research
A survey of Giri et al. (2007) “Radiation measurement at X-ray centers of a few
hospitals in Kathmandu city, Nepal". Radiation was measured in X-ray room of 13
different hospitals, fluoroscopy room of 2 hospitals and CT scan room of 1 hospital
in Kathmandu City, Nepal, using a portable radiation measuring instrument.
Measurement was performed during the daytime. The background radiation was
measured before the machines were switched on in respective rooms. Subsequently
after the exposure to the radiation, the fall out radiation was measured in 4 different
corners of the radiation facility room of different hospitals. The unit of measurement
was in count per minute and converted in milliSievert per year (mSv/yr). The
findings show increased exposure and in some instances very high levels of
unintentional exposure to radiation.

32
Oluwafisoye et al. (2009) conducted an environmental monitoring survey and quality
control test of X-ray diagnostic facilities of a large Nigerian hospital. The
environmental monitoring in this study was carried out using calibrated radiation
equipment. Questionnaires were also used to elicit information from the most senior
personal of the hospital. The study was carried out at the X-ray unit of the Jon-Ken
hospital, Lagos (private hospital). The results show that the facilities for safety were
grossly inadequate and the dose rates of 4.0 μSv/hr and 5.0 μSv/hr were recorded at
the reception and outside the entrance door respectively. The dose rates at the
adjacent ultrasound scan room and waiting lobby are at least a factor of 40 higher
than the background dose rate each, indicating higher health risk to the visitors and
personnel at the hospital. The results recommended to improve on the safety of the
patient and personnel were sent to the management of the X-ray unit of the hospital.
Nevertheless, follow-up studies indicate improved facilities and safety measures.
A recent study conducted by Abu Draz (2009) aimed to evaluate the radio-
technologists knowledge, attitudes and practices about radiation protection in the
eleven governmental hospitals which provide radiological services in Gaza Strip,
Palestine. Close ended structured questionnaire containing 69 questions had been
distributed among 135 radio-technologists through face to face interview. The study
showed that, the mean of knowledge was 9.5 (out of 20) while the mean attitude was
16.5 (total scores 20) and that of practice was 5.6 (total scores 18). Of studied radio-
technologists only 4.5% obtained high knowledge scores and about 87.9% have high
attitude scores while none of the study participants achieved a high practice scores.
The study has indicated that, the radio-technologists have high concern toward
radiation protection, but they have inadequate knowledge while their proper practices
were not adequate toward radiation health hazards.
Adejumo et al. (2012) evaluated compliance to radiation safety standard amongst
radiographers in radio-diagnostic centers in South West, Nigeria. The study carried
out in some selected private diagnostic centers and government hospitals. One
hundred radiographers from public and private radio-diagnostic centers administered

33
questionnaires on compliance rate of safety standard as described by national and
international commission on ionizing radiation. The result reveals high compliance
rate in majority of radio-diagnostic centers located in south west Nigeria.
Conclusively, this study showed that radiographers working in both private and
public establishments in south west, Nigeria were been monitored and they strictly
followed the radiation protection standard rules to be within radiation workers dose
limits.
The radiation survey conducted by Adhikari et al. (2012) for diagnostic radiology
was done in 28 different hospitals around Kathmandu and different parts of Nepal by
which include forty four X-ray equipment, ten CT scans, two mammography and two
catheterization laboratory to assessment of the radiation protection in medical uses of
ionizing radiation. Questionnaire for radiation workers were also used; radiation dose
levels were measured and an inventory of availability of radiation equipment made.
A corollary objective of the study was to create awareness in among workers on
possible radiation health hazard and risk. It was also deemed important to know the
level of understanding of the radiation workers in order to initiate steps towards the
establishment of Nepalese laws, regulation and code of radiological practice in this
field. The radiation workers who have participated in the questionnaire represent
more than 50% of the radiation workers working in this field in Nepal. we can say
that around 70% of the radiation workers are aware of radiation safety issue. Almost
all X-ray, CT and mammogram installations were built according to protection
criteria and hence found safe. Around 65% of the radiation workers have never been
monitored for radiation.
A survey of Ali (2013) was conducted in Iraqi Kurdistan region hospitals to evaluate
the environmental monitoring. The quality control test of X-ray facilities of
Kurdistan region hospitals was carried out. Data on the number of diagnostic
procedures using x-ray examination in year 2010- 2011 in four governmental
hospitals. Questionnaires were also used to elicit information from the most senior
personal of the hospital. The results show that the facilities for safety were grossly
inadequate and the dose rates of 11.75 μSv/hr and 10.48 μSv/hr, recorded at Place for

34
standing radiographic respectively. The dose rates at the Behind X-ray door room at
least 3.123 μSv/hr indicating higher health risk to the visitors and personnel at the
hospital. The results suggested to improve on the safety of the all staff of the X-ray
unit, patient and personnel were sent to the management of the X-ray unit of the
hospital.
Younis et al. (2014) evaluated radiation protection from radio diagnostic departments
in Erbil hospitals. Data on the number of diagnostic procedures using X-ray
examinations in five hospitals were collected. The Nuclear Radiation Meter was used
to measure radiation leakage. Questionnaire was also used to elicit information from
the most senior personnel of the hospital. The finding showed that the facilities for
safety were grossly inadequate and the dose rates of 16.4 μSv/hr and 20 μSv/hr,
recorded at places for paramedics and technician room respectively. A dose rate in
front of window of the monitor room was 113 μSv/hr and in the reception was
20μSv/hr indicating higher health risk to the paramedic, visitors and personnel at the
hospital. Radiation protection facilities in the radiological departments of Erbil
hospitals are in general poor including both public & private sectors indicating high
health risk to the paramedics, visitors and personnel at the hospitals.
Since, there is no clear cut of evidence that such a work have been done in Gaza
Strip. We present here the measurements of equivalent radiation dose rate in different
locations in radio-diagnostic rooms at a selected governmental Gaza governorates
hospitals. In addition, a questionnaire used to obtain information from the radio-
diagnostic workers in order to improve the radiation protection safety measures.

35
Chapter 3
Methodology
3.1 Introduction
In this chapter, we describe the methodology used in the present work, including the
study design, study population, sample size, location of the study, study instruments
and techniques and data analysis. Ethical considerations were also taken into
consideration through conducting the research. In addition, the obstacles and
limitations that encountered the researcher through conducting the research are also
mentioned.
3.2 Study design
The present study is a practical and descriptive analytical cross sectional study, based
on the analysis of data collected from the radiation survey meter. The data sheet
information collected from radio-diagnostic machines and rooms are also analyzed.
In addition, a questionnaire are distributed to the workers who have been working in
nine selected governmental Gaza governorates hospitals.
3.3 Study population
The target population of this study is the radio-diagnostic workers who have been
working at radio-diagnostic centers. This estimated approximately 185 medical
radiographers and 45 radiologists distributed at nine governmental hospitals
according to the MOH records (Abbas, 2014, Personal communication).
3.4 Sample size
The sample size was calculated by using sample size calculator from the survey
system on the web, with confidence level of 95% and confidence interval of 5. The
calculated sample size was 144 of the 230 radio-diagnostic workers (Annex, 1). We

36
decided to give rise this number to 182 in order to increase the response rate and to
compensate the uncertainties.
3.5 Locations of the study
The study was carried out in radio-diagnostic centers at nine selected governmental
Gaza governorates hospitals including: Al Shifa Medical Complex, Nasser Medical
Complex, European Gaza hospital, Abu Yousef Al Najjar Martyr hospital, Kamal
Adwan Martyr hospital, Al Aqsa Martyrs hospital, Abdel Aziz Rantessi Martyr
hospital , Al Naser pediatric hospital and Beit Hanoun hospital.
The hospitals were selected because of their large and diverse of their radio-
diagnostic services.
3.6 Ethical considerations
A permission from the ministry of health has been obtained to perform the study in
the governmental hospitals (Annex, 2). A consent from all participants to ensure their
voluntary participation (Annex, 3).
3.7 Study instruments
Three ways were applied to assess the status of ionizing radiation dose rate and
radiation protection measures in radio-diagnostic centers at governmental Gaza
governorates hospitals, namely:
3.7.1 Radiation survey meter
The radiation survey has been carried out to measure the radiation dose rate at
different locations in the radio-diagnostic rooms at nine selected governmental Gaza
governorates hospitals.

37
Radiation survey meter (OD-01) that designed by Step – Sensortechnik und
ElektronikPockauGmbH, Germany. Figure (3.1) displays the radiation survey meter
that used throughout the measurements. The calibration of the survey meter (OD-01)
is performed according to ISO 9001 TUV Quality Management System Certification,
headquartered in Munich, Germany by using Co-60 (photon energy 1.2 MeV), see
annex (annex, 6).
Radiation survey meter used for measurements of ambient and directional equivalent
dose of pulsed radiation fields and dose rate of X-rays, gamma and beta radiation.
Figure (3.1): Radiation survey meter (OD-01)
3.7.2 Radio-diagnostic machines and rooms specifications
Data sheets are also used to obtain information about radio-diagnostic machines and
rooms. The information was taken from medical equipment engineering department
in ministry of health and from the head of radio-diagnostic center. The data sheet
includes information about: name of hospital, radio-diagnostic room number,
manufacturer of machine, model of machine, status of machine, date of machine
installation, type of machine working (constant or portable), (electronic or manual),
(film processing digital or analogue), dimensions of radio-diagnostic room in cm,
width of the room walls in cm, material of the room walls, material of the control
panel wall, thickness and high of lead lining the room walls, the distance between the

38
radiation source and control panel, thickness of lead lining the room doors and
number of radiological procedures in the radio-diagnostic room per day. For more
details see (annex, 8).
3.7.3 Questionnaire interview
An interview was also done for filling the questionnaire that designed for matching
the study needs. All interviews were conducted face to face by the researcher
personally. During the survey the interviewer explained any of the questions that
were not clear. The questionnaire was based on the questions of a previous study
with some modifications (Abu Draz, 2009). The validity of the questionnaire was
tested by six specialists in the fields of radiology, medical physics, public health and
statistics.
The questionnaire content validity had been built in pilot study before starting real
data collection. It was served as a pre-test for the questionnaire to check the
ambiguity in the question statements and the time taken to complete the
questionnaire. Twenty radio-diagnostic workers were chosen to participate in the
pilot study. They were selected by the convenience method from the hospitals that
have been previously identified. Slight modifications were also done on the
questionnaire in corporation with the academic supervisors.
The questionnaire content reliability and internal consistency determined by using
Cronbach's Alpha in SPSS. The reliability of the second part items of the
questionnaire relating to the availability of personal radiation protection devices
equal 0.6. While the reliability of the third part items of the questionnaire relating to
awareness of radio-diagnostic workers about radiation protection issues equal 0.731.
In addition, the reliability of the fourth part items of the questionnaire relating to
practices of radio-diagnostic workers about radiation protection issues equal 0.751.

39
The questionnaire originally was constructed in English language (Annex, 4), and
then translated into Arabic language except some medical terms remained in English
(Annex, 5).
The questionnaire consists of five parts and includes the following:
Part one: consisted of eight questions about socio-demographic factors and related
work information. This includes: age, sex, occupation, academic qualification, years
of experience, name of hospital, type of radio-diagnostic machines who use it, and
daily work hours inside the radio-diagnostic rooms.
Part two: consisted of ten questions related to the availability of radiation protection
devices in the radio-diagnostic centers. This contains (lead apron, gonad shield, lead
curtains, lead shields or barrier, thyroid shields, lead glass, lead gloves, breast
shields, radiation warning signs and caution lights).
Part three: consisted of eighteen questions to measure the level of radio-diagnostic
workers awareness about radiation protection issues. This also gives some
information about the general understanding of radiation protection issues.
Part four: consisted of fifteen questions related to describe of radio-diagnostic
workers practices about radiation protection issues.
Part five: consisted of six questions to evaluate the personal radiation exposure
monitoring process.
3.8 Study techniques
3.8.1 Locations of measurements
To measure the equivalent radiation dose rate, specific locations were selected
according to radio-diagnostic rooms design and machines types. These locations are:
electrical zero balancing value, under the X-ray tube when X-ray directly fall on the

40
survey meter probe (directional dose), at one meter distance from the X-ray tube by
closing the tube collimators, at control panel, at corridor outside the X-ray room
(door closed), at dark room and behind the chest stand wall. For CT scan the
measurements also conducted at door near the control panel (door closed), in
additional to patient waiting rooms.
3.8.2 The workload
In this study the radiation level at each location was calculated using the workload.
The National Council on Radiation Protection and Measurements (NCRP report no. 49)
workloads could be used throughout this work. However, the NCRP workloads
might be more or less than the workloads at some of those rooms. For this reason,
can be calculated the workloads in each radio-diagnostic room to simulate the real
workloads in radio-diagnostic rooms at governmental Gaza governorates hospitals,
see (Annex, 7).
Workload is a measure of the X-ray tube use and is a number of electrons hitting X-
ray tube anode. It varies greatly with assumed maximum kVp of X -ray unit. It is
usually a gross overestimation (ICRP, 2007).
Workloads according to NCRP report no.49 are: for basic X-ray unit: 1000
mA.min/week, for fluoroscopy unit: 750 mA.min/week and for CT scan unit:
28.000 mA.min/week at 100 kVp. It is also noticed that spiral CT scan units or multi-
slice CT scan could have higher workloads. In addition, for mammography unit: 700
mA.min/week at 30 kVp.
The radiation level at each location in one week was calculated using the workload
mA.min/week (= mAs/60), the current workload in each room could be calculated as:
Workload = ∑ (𝐦𝐀. 𝐦𝐢𝐧)𝐢
i.Ni
Where (Ni) is the examination number of kind i and (mA.min) used techniques for
examination kind i (Adhikari, 2012).

41
3.8.3 The equivalent radiation dose rate
In order to calculate the radiation level in different locations, we have considered the
different characteristic parameters of radiation like kilo-Volt (kV), milli-Ampere
(mA) and time (s).
In basic X-ray, the radiation parameters taken to evaluate radiation level were about
100 kVp in voltage, 1 s in time (t), and tube current (I) was 100 mA, to give high
energy of radiation. Figure (3.2), displays the radiation parameters at X-ray machine
control of panel. In CT scan, the radiation parameters taken to evaluate radiation
level were about 100 kVp in voltage, 1 s in time (t), and tube current (I) was 210 mA.
In fluoroscopy, the radiation parameters taken to evaluate radiation level were about
100 kVp in voltage, tube current (I) was 3 mA. In mammography, the radiation
parameters taken to evaluate radiation level were about 30 kVp in voltage, 1 s in time
(t), and tube current (I) was 50 mA.
Figure (3.2): The radiation parameters were taken in basic X-ray machine
The measurements were performed during the daytime between 8 AM to 2 PM. The
electrical zero balancing was recorded before the radio-diagnostic machines were
switched on in respective rooms to verify the electrical zero of the measuring device.

42
Figure (3.3), illustrates the reference phantom was used as a scattering medium to
simulate physiological characteristics of patient body. The Measurements behind the
chest stand wall was done without a patient or a phantom and the distance between
X-ray tube and chest stand equal 180 cm. As shown in figure (3.4), the
measurements were conducted by using Source Image Distance (SID) is equal 100
cm.
The unit of measurements was in milliSievert per hour (mSv/hr) and converted in
milliSievert per year (mSv/year).
The equivalent radiation dose rate to whole body at each location (HW) in unit of
(mSv
week ) was calculated using:
𝐇𝐰 (mSv
week) = 𝐑 (
mSv
min) .
𝟏
𝐈𝐦(mAm) . 𝐖𝐨𝐫𝐤𝐥𝐨𝐚d (
mA.min
week)
Where (R) is the radiation dose rate reading in each location in unit of (mSv/min),
(Im) is the maximum continuous tube current possible in mA units at kVpmax and
workload in units of (mA.min
week) (Adhikari, 2012).
Figure (3.3): The reference phantom was used as a scattering medium

43
Figure (3.4): Source Image Distance (SID) is equal 100 cm
3.9 Limitation of the study
During the implementation of the study we faced some of limitations such as:
1. This study conducted only in governmental hospitals in Gaza governorates, not
primary care clinics, UNRWA or private centers, so the results can only be
generalized on this sector.
2. Lack of cooperation of Radiation Protection Department in Energy and Human
Resources Authority.
3. At some centers, it is doubtful whether the given mA or kV are actually correct
as shown in control panel because there is no measuring/verifying equipment
and no quality control program to maintain the quality of the equipment.
4. Some of radio-diagnostic machines out of services during the period of study
conducting, which led to the inability of measuring the ionizing radiation
leakage in these rooms.

44
3.10 Statistical tools and data analysis
Data checked, coded, entered and analyzed using SPSS 20 (Statistical
Package for the Social Science Inc. Chicago, Illinois USA, version 20)
statistical package.
We would utilize the following statistical tools:
Frequency .
Descriptive analysis (means and standard deviation "S.D").
Tabular and Graphical display.
Independent Samples T-test.
Analysis of Variance "ANOVA".

45
Chapter 4
Results and Discussion
4.1 Introduction
In this chapter, we presented the main results of the study based on the outcomes of
the statistical analyses and it includes two parts:
1. The results of the equivalent radiation dose rate that measured at different
locations in the radio-diagnostic rooms at the selected nine hospitals. It also
contains the radio-diagnostic machines and rooms specification data sheet
information.
2. The results of the questionnaire information analysis which includes: distribution
of the participants according to their socio-demographic characteristics and work
related information, evaluation of availability of radiation protection devices,
measure of radio-diagnostic workers awareness and practices level regarding
radiation protection issues and evaluation of the personal radiation exposure
monitoring process.
In the present work, we conducted the independent samples t- test, frequency and
one-way analysis of variance (ANOVA). These tests detect the difference between
the availability of personal radiation protection devices, awareness and practices
level regarding radiation protection issues and evaluation of personal radiation
exposure monitoring process as a dependent variables. However, the socio-
demographic and work related factors among radio-diagnostic workers are
independent variables.

46
Part one
4.2 The equivalent radiation dose rate measurements in radio-diagnostic
centers at the selected nine hospitals
The radiation survey has been carried out in radio-diagnostic centers at nine selected
governmental Gaza governorates hospitals to measure the radiation dose rate at
different locations in the radio-diagnostic rooms.
The accepted effective annual dose limits for occupational staff as reported by the
International Commission on Radiological Protection (ICRP) in 1991 was 20 mSv as
an average for a period of five years, with the further provision that the effective
dose should not exceed 50 mSv in any single year. Public should not be exposed to
more than an average of 1 mSv per year.
4.2.1 The measurements at Al Shifa Medical Complex
Figure (4:1): The equivalent radiation dose rate in basic X-ray rooms at Al Shifa
Medical Complex
Figure (4.1), shows that the equivalent radiation dose rate that measured at corridor
during closing the door, at patient waiting room and behind the chest stand wall in
the most of basic X-ray rooms are found higher than the reference limit for public
0
0.5
1
1.5
2
2.5
3
3.5
4
At control panel
At dark room
At corridor (doorclosed)
At Patient waitingroom
Behind the cheststand wall
(Hw)
mS
v/y
r
roo
m n
o. 2
Basic X-ray
room no. 6
Basic X-ray
room no. 7
Basic X-ray
emergency
room
Basic X-ray
out clinic
room no. 1
Basic X-ray
out clinic
room no. 2
1.1
mS
v/y
r
1.1
mS
v/y
r
1.7
mS
v/y
r
1.9
5 m
Sv/y
r
1.3
mS
v/y
r
1.2
mS
v/y
r
1.8
mS
v/y
r
0.9
mS
v/y
r
1.4
m
Sv/y
r
1.6
mS
v/y
r
2
.2 m
Sv/y
r
1.9
mS
v/y
r
1.8
m
Sv/y
r
1.2
mS
v/y
r
2.0
1 m
Sv/y
r
1
.9 m
Sv/y
r
3.8
mS
v/y
r
1.8
mS
v/y
r
2
.01
mS
v/y
r
2
.1 m
Sv/y
r
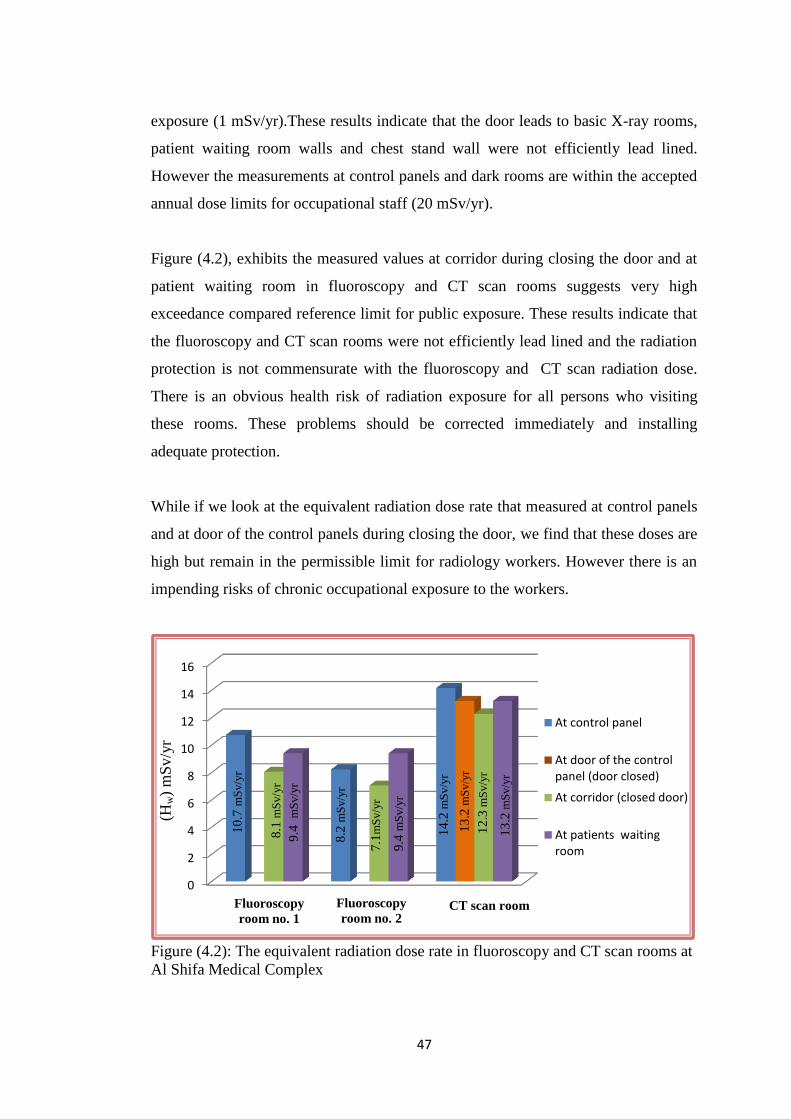
47
exposure (1 mSv/yr).These results indicate that the door leads to basic X-ray rooms,
patient waiting room walls and chest stand wall were not efficiently lead lined.
However the measurements at control panels and dark rooms are within the accepted
annual dose limits for occupational staff (20 mSv/yr).
Figure (4.2), exhibits the measured values at corridor during closing the door and at
patient waiting room in fluoroscopy and CT scan rooms suggests very high
exceedance compared reference limit for public exposure. These results indicate that
the fluoroscopy and CT scan rooms were not efficiently lead lined and the radiation
protection is not commensurate with the fluoroscopy and CT scan radiation dose.
There is an obvious health risk of radiation exposure for all persons who visiting
these rooms. These problems should be corrected immediately and installing
adequate protection.
While if we look at the equivalent radiation dose rate that measured at control panels
and at door of the control panels during closing the door, we find that these doses are
high but remain in the permissible limit for radiology workers. However there is an
impending risks of chronic occupational exposure to the workers.
Figure (4.2): The equivalent radiation dose rate in fluoroscopy and CT scan rooms at
Al Shifa Medical Complex
0
2
4
6
8
10
12
14
16
At control panel
At door of the controlpanel (door closed)
At corridor (closed door)
At patients waitingroom
CT scan room Fluoroscopy
room no. 2
(Hw)
mS
v/y
r
roo
m n
o. 2
Fluoroscopy
room no. 1
12
.3 m
Sv/y
r
9.4
mS
v/y
r
14
.2 m
Sv/y
r
7.1
mS
v/y
r
13
.2 m
Sv/y
r
8.2
mS
v/y
r
9.4
m
Sv/y
r
8.1
mS
v/y
r
10
.7 m
Sv/y
r
13
.2 m
Sv/y
r

48
4.2.2 The measurements at Nasser Medical Complex
Figure (4.3), illustrates that the values of equivalent radiation dose rate that measured
in the basic X-ray machines rooms are within the permissible limits for radio-
diagnostic workers and public.
The equivalent radiation dose rate is also measured at different locations in
mammography room, it is clearly the mammography room is very safe and built
according to protection criteria.
Figure (4.3): The equivalent radiation dose rate in basic X-ray and mammography
rooms at Nasser Medical Complex
Figure (4.4), exhibits the equivalent radiation dose rate at corridor during closing the
door and at patient waiting room in fluoroscopy room were found (5.4 mSv/yr and 6
mSv/yr) respectively. This means that the values at these locations are four times
higher than the permissible limits for the public. The equivalent radiation dose that
measured at control panel was (10.9 mSv/yr) which is also high but not exceed the
permissible occupational limits. The results indicates that this room is not efficiently
lead lined or protected well. This would give health risk due to radiation exposure.
The equivalent radiation dose rate values in CT scan room show that the equivalent
radiation dose rate at corridor during closing the door was about (1.7 mSv/yr).
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
At control panel
At dark room
At corridor (doorclosed)
Behind the cheststand wall
Portable X-ray room no. 1
(Hw)
mS
v/y
r
Basic X-ray
room no. 2
Mammography
room no. 3
Basic X-ray
Out clinic room
0.1
mS
v/y
r
0.2
mS
v/y
r
0.4
mS
v/y
r
0.1
6
mS
v/y
r
0.0
3 m
Sv/y
r
1.4
mS
v/y
r
0.0
5 m
Sv/y
r
0.0
5 m
Sv/y
r
0.2
mS
v/y
r
0.9
mS
v/y
r
0.1
mS
v/y
r
0.2
mS
v/y
r
0.4
m
Sv/y
r
0.2
mS
v/y
r
0
.4 m
Sv/y
r

49
Certainly, this is higher than the reference limit for public exposure (1 mSv/yr).This
result indicates that the doors that lead to the CT scan room and patient waiting room
are also in need for protection. However the other measurements were estimated
within the accepted annual dose limits for occupational staff (20 mSv/yr).
Figure (4.4): The equivalent radiation dose rate in fluoroscopy and CT scan rooms at
Nasser Medical Complex
4.2.3 The measurements at European Gaza hospital
Figure (4.5), shows the equivalent radiation dose rate that measured at the different
locations in basic X-ray rooms are within safe limits for radio-diagnostic workers
and public. The radiation survey in these rooms show that it is built safe according to
safety criteria.
The equivalent radiation dose rate in fluoroscopy room (ESWEL), shows the
radiation dose rate that measured at corridor during closing the door and patient
waiting room was about (2.5 mSv/yr), which is about more than 1.5 times higher
than the reference limit for public exposure (1 mSv/yr).This result indicates that the
doors that lead to the fluoroscopy room and patient waiting room was not efficiently
protected. This high dose rate could mean a higher health risk to the unsuspecting
supportive personnel such as nurses, hospital attendants and the visitors. Such dose
rate could pose more serious problem to a pregnant women. The measurements at
0
2
4
6
8
10
12
At control panel
At the entrance of controlpanel (no door)
At corridor (door closed)
At patient waiting room
(Hw)
mS
v/y
r
Fluoroscopy room no. 4
CT scan room no. 5
0.8
mS
v/y
r
1.7
m
Sv/y
r
6.3
mS
v/y
r
5.9
mS
v/y
r
6 m
Sv/y
r
5.4
mS
v/y
r
10
.9 m
Sv/y
r
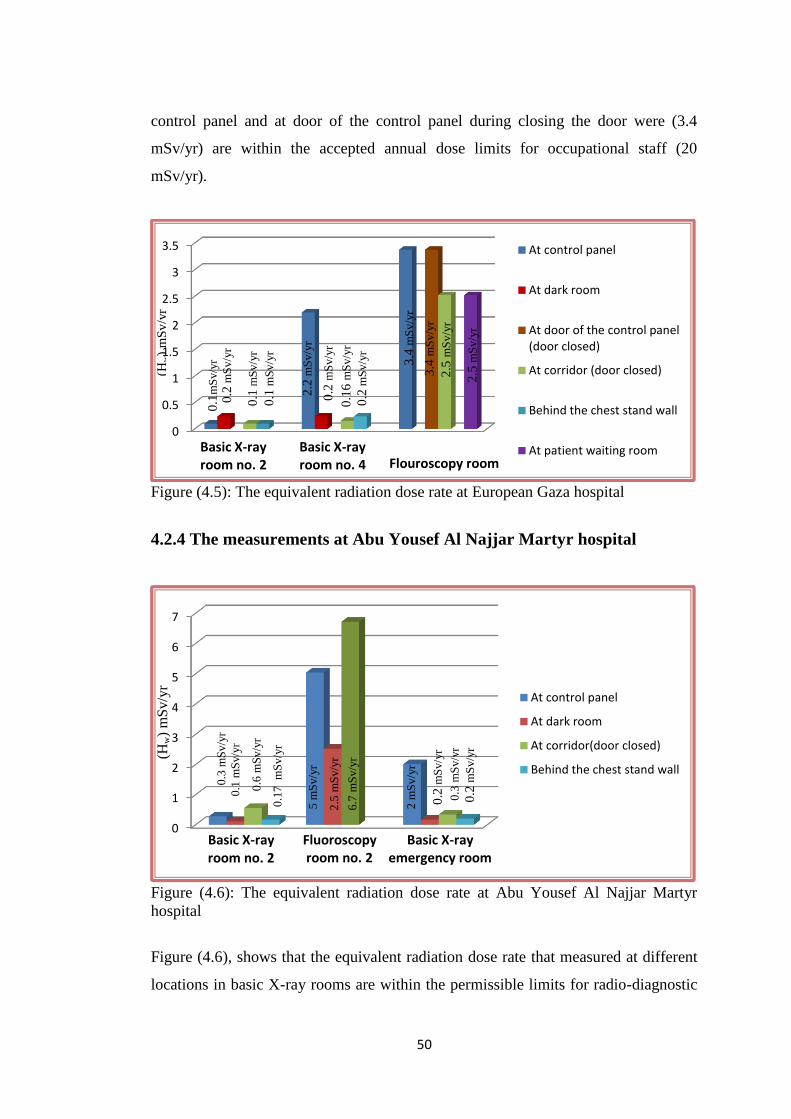
50
control panel and at door of the control panel during closing the door were (3.4
mSv/yr) are within the accepted annual dose limits for occupational staff (20
mSv/yr).
Figure (4.5): The equivalent radiation dose rate at European Gaza hospital
4.2.4 The measurements at Abu Yousef Al Najjar Martyr hospital
Figure (4.6): The equivalent radiation dose rate at Abu Yousef Al Najjar Martyr
hospital
Figure (4.6), shows that the equivalent radiation dose rate that measured at different
locations in basic X-ray rooms are within the permissible limits for radio-diagnostic
0
0.5
1
1.5
2
2.5
3
3.5 At control panel
At dark room
At door of the control panel(door closed)
At corridor (door closed)
Behind the chest stand wall
At patient waiting roomBasic X-ray room no. 2
Basic X-ray room no. 4
Flouroscopy room
0
1
2
3
4
5
6
7
At control panel
At dark room
At corridor(door closed)
Behind the chest stand wall
Basic X-ray room no. 2
Fluoroscopy room no. 2
Basic X-ray emergency room
(Hw)
mS
v/y
r
0.3
mS
v/y
r
2 m
Sv/y
r
6.7
mS
v/y
r
2.5
mS
v/y
r
5 m
Sv/y
r
0.1
7
mS
v/y
r
0.6
mS
v/y
r
0.1
mS
v/y
r
0.3
mS
v/y
r
0.2
mS
v/y
r
0
.2 m
Sv/y
r
(Hw)
mS
v/y
r
roo
m n
o. 2
2.5
mS
v/y
r
3.4
mS
v/y
r
3.4
mS
v/y
r
0.2
mS
v/y
r
0.1
6 m
Sv/y
r
0.2
mS
v/y
r
2.2
mS
v/y
r
0.1
mS
v/y
r
0.1
mS
v/y
r
0.2
mS
v/y
r
0.1
mS
v/y
r
2.5
mS
v/y
r

51
workers and public. Whereas, there is a huge radiation dose at corridor during
closing the door in the fluoroscopy room, and gives (6.7 mSv/yr).These result
indicates that the door that leads to this room should be protected well. There is an
obvious health risk of radiation exposure for all persons who visiting this room. It is
interesting to note that there were no leakages experienced in the other locations
within this room, the equivalent radiation dose rate at control panel and dark room
are within the accepted annual dose limits for occupational staff, were about (5
mSv/yr and 2.5 mSv/yr) respectively. Some rooms will be fitted with more than one
X- ray tub, shielding calculations must consider the total radiation dose from the two
tubes (IAEA, 2007).
4.2.5 The measurements at Kamal Adwan Martyr hospital
Figure (4.7): The equivalent radiation dose rate at Kamal Adwan Martyr hospital
As show in figure (4.7), the equivalent radiation dose rate measured at corridor
during closing the door in basic X-ray rooms were within the reference limit for
public exposure (1 mSv/yr) except in the basic X-ray in room no. 2, the value gives
(2.4 mSv/yr). This result indicates that the door leads to this room was not efficiently
lead lined. However, the measurements at control panels and at dark rooms are
within the accepted annual dose limits for occupational staff.
0
1
2
3
4
5
6
7
8
9
At control panel
At dark room
At corridor (door closed)
Behind the chest stand wall
Basic X-ray
room no. 2 Basic X-ray
Emergency room Basic X-ray
room no.3
Fluoroscopy room no. 3
(Hw)
mS
v/y
r
roo
m n
o. 2
4.0
3 m
Sv/y
r
0
.8
mS
v/y
r
0.7
mS
v/y
r
2.3
mS
v/y
r
2
.4 m
Sv/y
r
0.9
mS
v/y
r
7.5
mS
v/y
r
6
.7 m
Sv/y
r
8.4
mS
v/y
r
0.4
mS
v/y
r
0
.5 m
Sv/y
r
0.9
mS
v/y
r
0.5
mS
v/y
r

52
The measured values in fluoroscopy room show that there is a huge radiation dose at
corridor during closing the door. This result indicates that the door leads to the
fluoroscopy room was not efficiently lead lined. It is also noticed that the equivalent
radiation dose at control panel and at dark room are within the accepted effective
annual dose limits for occupational staff.
4.2.6 The measurements at Al Aqsa Martyrs hospital
Figure (4.8): The equivalent radiation dose rate at Al Aqsa Martyrs hospital
As show in figure (4.8), the measured equivalent radiation dose rate at different
locations in basic X-ray rooms are also found within the permissible limits for radio-
diagnostic workers and public.
However, the measured values in the fluoroscopy room we found there is a huge
radiation dose at corridor during closing the door gives (10.1mSv/yr). This result
indicates that the door that leads to the fluoroscopy room was not efficiently lead
lined. There is an obvious health risk of radiation exposure for persons who visiting
this room. Radiation leakages experienced in the other locations within this room are
within the accepted annual dose limits for occupational staff, the equivalent radiation
dose rate at control panel and at dark room gives (7.7 mSv/yr and 6.7 mSv/yr).
0
2
4
6
8
10
12
Basic X-rayroom no. 1
Basic X-rayroom no. 2
Flouroscopyroom no. 2
At control panel
At dark room
At radiodiagnostic workersroom
At corridor (door closed)
Behind the chest stand wall
(Hw)
mS
v/y
r
roo
m n
o. 2
6.7
mS
v/y
r
1
0.1
mS
v/y
r
7.6
mS
v/y
r
0.1
mS
v/y
r
1.4
mS
v/y
r
0
.5 m
Sv/y
r
0.2
mS
v/y
r
0.5
mS
v/y
r
0.2
mS
v/y
r
2.0
1 m
Sv/y
r
0.2
mS
v/y
r

53
4.2.7 The measurements at Abdel Aziz Rantessi Martyr Pediatric hospital
Figure (4.9): The equivalent radiation dose rate at Abdel Aziz Rantessi Martyr
hospital
The results in figure (4.9), show that the measured radiation dose rate at corridor
during closing the door in fluoroscopy room is about (3.4 mSv/yr) and reflects a
huge radiation dose compared with reference limit for public exposure (1 mSv/yr).
These results indicate that the X-ray room was not efficiently lead lined and the
radiation protection is not commensurate with the fluoroscopy radiation doses. There
is an obvious health risk of radiation exposure for persons who visiting this room.
However, the measured values at control panel and at dark room remain in the
permissible limit for radio-diagnostic workers.
The measured values in CT scan room, show that the measured dose rate at patient
waiting room is about more than three times higher than the reference limit for public
exposure (1 mSv/yr).Whereas, the measured values at control panel and at door of
the control panel during closing the door are found high but remain in the
permissible limit for radio-diagnostic workers. These results reveals that the radio-
diagnostic center should be carefully shielded out.
0
1
2
3
4
5
6
7
At control panel
At dark room
At door of the controlpanel (door closed)
At corridor (door closed)
At patients waiting room
Fluoroscopy room no. 1
CT scan room no. 2
(Hw)
mS
v/y
r
roo
m n
o.
2
4.7
mS
v/y
r
4
.03
mS
v/y
r
6.3
mS
v/y
r
3.7
mS
v/y
r
4.2
mS
v/y
r
3.4
mS
v/y
r

54
4.2.8 The measurements at Al Naser Pediatric hospital
As shown in figure (4.10), the equivalent radiation dose rate that measured at
corridor during closing the door in basic X-ray room is found slightly beyond the
reference dose limit of 1 mSv/yr. It is interesting to note that the equivalent radiation
dose rate at control panel, at dark room are within the accepted annual dose limits
(20 mSv/yr).
Figure (4.10): The equivalent radiation dose rate at Al Naser Pediatric hospital
4.2.9 The measurements at Beit Hanoun hospital
Figure (4.11), depicts the measured radiation dose rate values at different locations
are found within the permissible limits for occupational stuff and public. The
radiation survey in this room shows that it is built safe according to safety criteria.
0
0.5
1
1.5
2
At control panel
At dark room
At corridor (door closed)
Behind the chest stand wall
(Hw)
mS
v/y
r
roo
m n
o. 2
Basic X-ray
room no. 1
room no. 2
0.5
mS
v/y
r
0.3
mS
v/y
r
1.0
08 m
Sv/y
r
1.9
mS
v/y
r

55
Figure (4.11): The equivalent radiation dose rate at Beit Hanoun hospital
4.3 The equivalent radiation dose rate at the different locations
The selected radio-diagnostic centers include: basic X-ray, fluoroscopy, CT scan and
mammography machines. The equivalent radiation dose rate were measured at the
different locations at those centers. These locations are: directional under the X-ray
tube, one meter distance from the X-ray tubes, control panels, dark rooms, corridors,
patient waiting rooms and behind the chest stand walls.
4.3.1 The equivalent radiation dose rate at control panels
The measured values of equivalent radiation dose rate at control panels are carried
out in radio-diagnostic rooms at nine selected hospitals shown in figure (4.12). The
results could be accepted and remain within permissible limit for occupational stuff.
We have also noticed that the CT scan room at Al Shifa Medical Complex ranked the
first in term of the highest radiation dose rate, and gives (14.2 mSv/yr). Then
followed by fluoroscopy room at Nasser Medical Complex, and gives (10.9 mSv/yr).
In addition , the higher values at control panels for basic X-ray rooms found in
emergency room at Kamal Adwan hospital and at emergency room at Al Shifa
0
0.2
0.4
0.6
0.8
1
1.2
1.4
At control panel
At dark room
At corridor (door closed)
Behind the chest standwall
Basic X-ray
room no. 1
(Hw)
mS
v/y
r
roo
m n
o. 2
0.3
mS
v/y
r
0.2
mS
v/y
r
0.3
mS
v/y
r
1.3
mS
v/y
r

56
hospital, and gives ( 4.03 mSv/yr and 3.8 mSv/yr) respectively. The lowest radiation
dose rate at control panel found in mammography room at Nasser Medical complex.
Figure (4.12): The equivalent radiation dose rate at control panels
4.3.2 The equivalent radiation dose rate at corridors
Figure (4.13), illustrates the measured values at corridors during closing the doors in
thirty radio-diagnostic rooms at nine selected hospitals. The results showed that the
values at CT scan , fluoroscopy, and some of basic X- ray rooms are higher than the
reference limit for public exposure and indicate that the doors that leads to these
rooms should be efficiently lead lined. Clearly, there is a health risk of radiation
0
2
4
6
8
10
12
14
16
At control panels
Mam
mo
graph
y, roo
m n
o. 3
at Nasser
Basic X
-ray, roo
m n
o. 2
at Al A
qsa
Basic X
-ray, roo
m n
o. 2
at Euro
pean
Gaza
Basic X
-ray, roo
m n
o. 2 at A
l Najjar
Basic X
-ray, ou
t clinic ro
om
at Nasser
Po
rtable X
-ray, roo
m n
o.1
at Nasser
Basic X
-ray roo
m n
o. 3
at Kam
al Aw
dw
an B
asic X-ray, ro
om
no
. 1 At B
eit Han
ou
n B
asic X-ray, o
ut clin
ic roo
m n
o.1
at Al sh
ifa B
asic X-ray, ro
om
no
. 2 at Nasser
Basic X
-ray, roo
m n
o. 6 at A
l Shifa
Basic X
-ray, roo
m n
o. 1 at A
l Naser
Basic X
-ray roo
m n
o. 7
at Al Sh
ifa B
asic X-ray, ro
om
no
. 1 at Al A
qsa
Basic X
-ray, emergen
cy roo
m at A
l Najjar
Basic X
-ray, roo
m n
o. 4 at Eu
rop
ean G
aza B
asic X-ray, o
ut clin
ic roo
m n
o. 2
at Al Sh
ifa B
asic X-ray, ro
om
no
. 2 at Kam
al Ad
wan
ESWEL, flu
oro
scop
y roo
m at Eu
rop
ean G
aza B
asic X-ray, em
ergency ro
om
at Al Sh
ifa B
asic X-ray, em
ergency ro
om
at Kam
al Ad
wan
Fluo
rosco
py, ro
om
no
. 1 at A
l Ran
tessi Flu
oro
scop
y, roo
m n
o.2
at al Najjar
CT scan
, roo
m n
o. 5
at Nasser
CT scan
, roo
m n
o. 2
at Al R
antessi
Fluo
rosco
py, ro
om
no
. 3 A
t Kam
al Ad
wan
Fluo
rosco
py, ro
om
no
. 2 at A
l Aq
sa Flu
oro
scop
y, roo
m n
o.2
at Al Sh
ifa Flu
oro
scop
y, roo
m n
o. 1
at Al Sh
ifa Flu
oro
scop
y, roo
m n
o. 4
at Nasser
CT scan
roo
m at A
l Shifa
(Hw)
mS
v/y
r
roo
m n
o. 2
0.2
mS
v/y
r
3.4
mS
v/y
r
3.8
mS
v/y
r
4.0
3 m
Sv/y
r
4.7
m
Sv/y
r
5.0
4 m
Sv/y
r
5.9
mS
v/y
r
6.3
m
Sv/y
r
7.6
mS
v/y
r
7.6
mS
v/y
r
8.2
mS
v/y
r
10
.9 m
Sv/y
r
1
0.7
mS
v/y
r
14
.2 m
Sv/y
r
0.2
mS
v/y
r
1.8
mS
v/y
r
1.9
mS
v/y
r
1.9
5 m
Sv/y
r 2
.02
mS
v/y
r
2
.01
mS
v/y
r
2.2
m
Sv/y
r
2
.2 m
Sv/y
r
2.3
mS
v/y
r
1.3
m
Sv/y
r
0.4
mS
v/y
r
0.9
mS
v/y
r
0.3
mS
v/y
r
0.4
mS
v/y
r
0.3
mS
v/y
r
1.4
mS
v/y
r
1.4
mS
v/y
r

57
exposure for people who visiting this rooms. Certainly, this would give notice to the
stakeholders for an adequate protection. However, the measured values for the rest
rooms were found within the permissible limits and the lowest radiation dose rate
was found in mammography room at Nasser Medical Complex.
Figure (4.13): The equivalent radiation dose rate at corridors
4.3.3 The equivalent radiation dose rate at patient waiting rooms
Figure (4.14), exhibits the measured values at patient waiting rooms in nine radio-
diagnostic rooms at nine selected hospitals. The results could be described the most
of equivalent radiation dose rate are higher than the reference limits for public
exposure. The results showed that the values in patient waiting room at CT scan
room at Al Shifa Medical complex are the higher compared the reference limit for
public exposure and indicate that the doors that leads to these rooms should be
0
2
4
6
8
10
12
14
At corridors
Mam
mo
graph
y, roo
m n
o. 3
at Nasser
Po
rtable X
-ray, roo
m n
o. 1
at Nasser
Basic X
-ray, roo
m n
o. 2
at Euro
pean
Gaza
Basic X
-ray, roo
m n
o. 4
at Euro
pean
Gaza
Basic X
-ray, roo
m n
o. 1
at Al A
qsa
Basic X
-ray, roo
m n
o. 1
At B
eit Han
ou
n
Basic X
-ray, emergen
cy roo
m at A
l Najjar
Basic X
-ray, ou
t clinic ro
om
at Nasser
Basic X
-ray, roo
m n
o. 2
at Al A
qsa
Basic X
-ray, roo
m n
o. 3
at Kam
al Ad
wan
Basic X
-ray, roo
m n
o. 2
at Al N
ajjar B
asic X-ray, em
ergen
cy roo
m at K
amal A
dw
an
Basic X
-ray, roo
m n
o. 2
at Nasser
Basic X
-ray, roo
m n
o. 1
at Al N
aser B
asic X-ray, ro
om
no
. 7 at A
l Shifa
Basic X
-ray roo
m n
o. 6
at Al Sh
ifa
Basic X
-ray, emergen
cy roo
m at A
l Shifa
Basic X
-ray, ou
t clinic ro
om
no
.1 at A
l shifa
Basic X
-ray, ou
t clinic ro
om
no
. 2 at A
l Shifa
B
asic X-ray ro
om
no
. 2 at K
amal A
dw
an
ESWEL, flu
oro
scop
y roo
m at Eu
rop
ean G
aza
Fluo
rosco
py, ro
om
no
. 1 at A
l Ran
tessi Flu
oro
scop
y, roo
m n
o.4
at Nasser
CT scan
, roo
m n
o. 5
at Nasser
Fluo
rosco
py, ro
om
no
. 3 A
t Kam
al Ad
wan
Fluo
rosco
py, ro
om
no
.2 at al N
ajjar Flu
oro
scop
y, roo
m n
o.2
at Al Sh
ifa
Fluo
rosco
py, ro
om
no
. 1 at A
l Shifa
Fluo
rosco
py, ro
om
no
. 2 at A
l Aq
sa
CT scan
roo
m at A
l Shifa
(Hw)
mS
v/y
r
roo
m n
o.
2 8.1
mS
v/y
r
10
.08
mS
v/y
r
12
.3 m
Sv/y
r
1.8
mS
v/y
r
1.9
mS
v/y
r
1.1
2 m
Sv/y
r
1
.01
mS
v/y
r
0
.9 m
Sv/y
r
0
.8 m
Sv/y
r
0
.6 m
Sv/y
r
0
.5 m
Sv/y
r
0
.5 m
Sv/y
r
0
.4 m
Sv/y
r
0
.3 m
Sv/y
r
0
.3 m
Sv/y
r
0
.2 m
Sv/y
r
0
.2 m
Sv/y
r
0
.1 m
Sv/y
r
0
.09
mS
v/y
r
0
.05
mS
v/y
r
2.5
mS
v/y
r
2.0
2 m
Sv/y
r
2.4
mS
v/y
r
4.0
3 m
Sv/y
r
5.4
mS
v/y
r
6.3
mS
v/y
r
6.7
mS
v/y
r
6.7
mS
v/y
r
7.1
mS
v/y
r
1.7
mS
v/y
r

58
efficiently lead lined. However, the lowest radiation dose rate was found in patient
waiting room at CT scan room at Nasser Medical Complex.
Figure (4.14): The equivalent radiation dose rate at patient waiting rooms
4.3.4 The equivalent radiation dose rate at dark rooms
Figure (4.15), describes the measured values in twenty first dark rooms at nine
selected hospitals. It is noticed that the dark rooms near the fluoroscopy rooms
ranked the first in terms of the highest radiation dose rate.
0
2
4
6
8
10
12
14
At patient waiting rooms
CT scan
, roo
m n
o. 5
at Nasser
Basic X
-ray, roo
m n
o. 7 at A
l Shifa
Basic X
-ray, roo
m n
o. 6 at A
l Shifa
ESWEL, flu
oro
scop
y roo
m at Eu
rop
ean G
aza C
T scan, ro
om
no
. 2 at A
l Ran
tessi Flu
oro
scop
y, roo
m n
o. 4
at Nasser
Fluo
rosco
py, ro
om
no
.2 at A
l Shifa
Fluo
rosco
py, ro
om
no
. 1 at A
l Shifa
CT scan
roo
m at A
l Shifa
(Hw)
mS
v/y
r
roo
m n
o. 2
13
.2
mS
v/y
r
9.4
mS
v/y
r
9.4
mS
v/y
r
6.0
5 m
Sv/y
r
4.2
mS
v/y
r
2.5
mS
v/y
r
1.2
mS
v/y
r
1.1
2 m
Sv/y
r
0.8
mS
v/y
r

59
Figure (4. 15): The equivalent radiation dose rate at dark rooms
4.3.5 Directional equivalent radiation dose rate and at one meter from the
X-ray tube in basic X-ray and mammography rooms
Figure (4.16), illustrates the difference between the directional radiation dose rate
and the radiation dose rate at one meter distance from the X-ray tube by closing the
collimators in basic X-ray and mammography machines. This indicates to the
importance of using radiation protection techniques such as the distance from the X-
ray source and X-ray beam collimators.
All X-ray tubes have some radiation leakage, there is only 2-3 mm lead in the
housing. Radiation leakage is limited in most countries to 1 mGy/hr at 1 meter, so
this can be used as the actual leakage value for shielding calculations (ICRP, 2007).
0
2
4
6
8
10
At dark rooms
(Hw)
mS
v/y
r
0.1
1 m
Sv/y
r
0
.06
mS
v/y
r
0.2
mS
v/y
r
0.2
mS
v/y
r
0
.2 m
Sv/y
r
0.2
mS
v/y
r
0.2
mS
v/y
r
0.3
mS
v/y
r
0.4
mS
v/y
r
0.7
mS
v/y
r
0.9
mS
v/y
r
1.2
m
Sv/y
r
1.4
mS
v/y
r
1.8
mS
v/y
r
2.0
2 m
Sv/y
r
2.5
mS
v/y
r
3.4
mS
v/y
r
6.7
mS
v/y
r
8.4
mS
v/y
r
0.2
mS
v/y
r
0
.16
mS
v/y
r
Mam
mo
graph
y roo
m n
o.3
at Nasser
Po
rtable X
-ray, roo
m n
o.1
at Nasser
Basic X
-ray ,roo
m n
o. 2 at A
l Najjar
Basic X
-ray, roo
m n
o. 2 at N
asser
Basic X
-ray, emergen
cy roo
m at A
l Najjar
Basic X
-ray, roo
m n
o. 1 at A
l Aq
sa
Basic x-ray, o
ut clin
ic roo
m at N
asser
Basic X
-ray, roo
m n
o. 1
At B
eit Han
ou
n
Basic X
-ray, roo
m n
o. 4 at Eu
rop
ean G
aza
Basic X
-ray, roo
m n
o. 2
at Euro
pean
Gaza
Basic X
-ray, roo
m n
o. 1 at A
l Naser
Basic X
-ray, roo
m n
o. 3 at K
amal A
dw
an
Basic X
-ray, emergen
cy roo
m at K
amal A
dw
an
Basic X
-ray, roo
m n
o. 2 at K
amal A
dw
an
Basic X
-ray , ou
t clinic ro
om
no
.1 at A
l shifa
Basic X
-ray, roo
m n
o. 2
at Al A
qsa
Basic X
-ray, ou
t clinic ro
om
no
. 2 at A
l Shifa
Basic X
-ray, emergen
cy roo
m at A
l Shifa
Fluo
rosco
py, ro
om
no
.2 at al N
ajjar
Fluo
rosco
py, ro
om
no
. 1 at A
l Ran
tessi
Fluo
rosco
py, ro
om
no
. 2 at A
l Aq
sa
Fluo
rosco
py, ro
om
no
. 3 A
t Kam
al Ad
wan
0.0
3 m
Sv/y
r

60
The directional radiation dose rate in basic X-ray machine in room no. 2 at Kamal
Adwan martyr hospital was about (162.9 mSv/yr), while the radiation leakage at one
meter distance from the X-tube by closing the collimators about (4.4 mSv/yr).This
reflects the importance of using the distance from the X-ray source and X-ray tube
collimators to protect the patients and their escorts.
Figure (4.16): Directional equivalent radiation dose rate and at one meter from the X-
ray tube in basic X-ray and mammography rooms
-10
10
30
50
70
90
110
130
150
170
Directional dose rate
At one meter from the X-ray tube by closing the collimators
Mam
mo
grap
hy, ro
om
no
. 3 at N
asser
Po
rtable X
-ray, ro
om
no
.1 at N
asser
Basic X
-ray, ro
om
no
. 2 at E
uro
pean
Gaza
Basic X
-ray, e
merg
ency ro
om
at A
l Najjar
Basic X
-ray, ro
om
no
. 3 at K
amal A
dw
an
Basic X
-ray, ro
om
no
. 2 at A
l Aq
sa
Basic X
-ray, ro
om
no
. 1 at A
l Naser
Basic X
-ray, ro
om
no
. 1 A
t Beit H
ano
un
Basic X
-ray, ro
om
no
. 7 at A
l Sh
ifa
Basic X
-ray, ro
om
no
. 2 at A
l Najjar
Basic X
-ray, e
merg
ency ro
om
at A
l Sh
ifa
Basic X
-ray, o
ut clin
ic roo
m n
o. 2
at Al S
hifa
Basic X
-ray, o
ut clin
ic roo
m n
o.1
at Al sh
ifa
Basic X
-ray. ro
om
no
. 1 at A
l Aq
sa
Basic X
-ray, ro
om
no
. 2 at N
asser
Basic X
-ray, ro
om
no
. 6 at A
l Sh
ifa
Basic X
-ray, o
ut clin
ic roo
m at N
asser
Basic X
-ray, ro
om
no
. 4 at E
uro
pean
Gaza
Basic X
-ray, e
merg
ency ro
om
at K
am
al Ad
wan
Basic X
-ray, ro
om
no
. 2 at K
amal A
dw
an
(Hw)
mS
v/y
r
roo
m n
o. 2
10
5.3
mS
v/y
r
29
.1m
Sv/y
r
30
.7 m
Sv/y
r
52
.1 m
Sv
/yr
4
6.6
mS
v/y
r
55
.6 m
Sv/y
r
58
.8 m
Sv/y
r
64
.4 m
Sv/y
r
67
.8 m
Sv/y
r
79
.1 m
Sv/y
r
83
.6 m
Sv/y
r
98
.8 m
Sv/y
r
10
3.7
mS
v/y
r
10
6.5
mS
v/y
r
10
7.2
mS
v/y
r
10
7.5
mS
v/y
r
12
8.7
m
Sv/y
r
15
0.4
mS
v/y
r
15
4.9
mS
v/y
r
16
2.9
mS
v/y
r
0.3
mS
v/y
r
6
.7 m
Sv/y
r
0
.5 m
Sv/y
r
2.6
mS
v/y
r
0.9
m
Sv/y
r
1.7
mS
v/y
r
0.6
mS
v/y
r
2.0
1m
Sv/y
r
2.4
mS
v/y
r
4.2
mS
v/y
r
3.2
mS
v/y
r
1.1
mS
v/y
r
2.5
mS
v/y
r
1.2
mS
v/y
r
2.7
mS
v/y
r
1.5
mS
v/y
r
4.4
mS
v/y
r
0.7
mS
v/y
r
0.8
mS
v/y
r
0.4
mS
v/y
r

61
4.3.6 Directional equivalent radiation dose rate and at one meter from the
X-ray tube in fluoroscopy and CT scan rooms
Figure (4.17): Directional equivalent radiation dose rate and at one meter from the X-
ray tube in fluoroscopy and CT scan rooms
The measurements are also performed for both fluoroscopy and CT scan machines at
the selected hospitals. Figure (4.17), describes the deference between the directional
radiation dose rate and the radiation dose rate at one meter distance from the X-ray
tube by closing the collimators in fluoroscopy rooms.
The difference between the directional radiation dose rate in CT scan machine at Al
Shifa Medical complex (1338.12 mSv/yr), and the radiation dose rate at one meter
distance from the X-ray tube (752.976 mSv/yr), refers to a huge radiation dose
inside the CT scan rooms during imaging the patient. This high dose rate indicates a
-200
300
800
1300
1800
2300
Directional dose rate
At one meter from X-ray tube
CT scan
, roo
m n
o. 5
at Nasser
Fluo
rosco
py, ro
om
no
. 4 at Nasser
CT scan
, roo
m n
o. 2
at Al R
ante
ssi
Fluo
rosco
py, ro
om
no
. 1 at A
l Ran
tessi
ESWEL, flu
oro
scop
y roo
m at Eu
rop
ean G
aza
CT scan
roo
m at A
l Shifa
Fluo
rosco
py, ro
om
no
.2 at al N
ajjar
Fluo
rosco
py, ro
om
no
. 2 at A
l Aq
sa
Fluo
rosco
py, ro
om
no
. 3 A
t Kam
al Ad
wan
Fluo
rosco
py, ro
om
no
. 2 at A
l Shifa
Fluo
rosco
py, ro
om
no
. 1 at A
l Shifa
(Hw)
mS
v/y
r
roo
m n
o. 2
12
.6
mS
v/y
r
16
.1 m
Sv/y
r
26
2.5
mS
v/y
r
60
6.1
mS
v/y
r
89
9.1
mS
v/y
r
98
3.8
mS
v/y
r
98
7.8
mS
v/y
r
12
90
.2 m
Sv/y
r
13
38
.1 m
Sv/y
r
13
38
.1 m
Sv/y
r
13
67
.5 m
Sv
/yr
15
72
.5 m
Sv/y
r
21
09
.7 m
Sv/y
r
22
96
.9 m
Sv/y
r
48
3.5
mS
v/y
r
17
.6 m
Sv/y
r
14
8.7
mS
v/y
r
75
2.9
8 m
Sv
/yr
17
.6
mS
v/y
r
18
.5 m
Sv/y
r
41
.2 m
Sv/y
r
45
.7 m
Sv
/yr

62
high health risk to the unsuspecting supportive persons such as nurses, hospital
attendants and patient escorts. Such dose rate could pose more serious problem to a
pregnant women. So, it is importance of evacuating the CT scan room from the
patient escorts before giving the X-ray dose.
For more details about the equivalent radiation dose rate measurements in radio-
diagnostic centers, see annex (7).
4.4 Specifications of radio-diagnostic machines and rooms at the selected
hospitals
Data sheet information were collected and analyzed for all radio-diagnostic machines
and rooms that available in the selected hospitals. The information was taken from
medical equipment engineering department in ministry of health and from the head
of radio-diagnostic center. Most of these machines are analogue, this leads to
increase the possibility of X-ray images repeating. Thereby leads to increase the
work load in those rooms.
The analysis shows the presence of thirty-five radio-diagnostic machines in the
radio-diagnostic centers. Most of these machines are installed recently, working
electronically and constant except one of them is a portable and nine of them out of
services.
The results of analysis show that all of radio-diagnostic rooms space less than the
ideal X-ray rooms space, that should not be less than 36 m2 according to (NCRP,
report no. 147). The recommended distance between the X-ray machine and control
panels have not been achieved in some rooms such as: emergency basic X-ray room
at Al Shifa Medical Complex, fluoroscopy room at Nasser Medical Complex, basic
X-ray room no. 4 at European Gaza hospital, emergency basic X-ray room at Abu
Yousef Al Najjar Martyr hospital, basic X-ray in emergency room and fluoroscopy
room at Kamal Adwan Martyr hospital, basic X-ray room at Al Naser Pediatric
hospital and basic X-ray room at Beit Hanoun hospital.

63
The thickness and materials of the X-ray rooms walls (20 cm and cement)
respectively. The thickness and height of lead lining of room walls (2 mm and 200-
210 cm) respectively. The thickness of lead lining the room doors (2 mm), this is in
conformity with safety standards. However, we found that the wall of the control
panel in some rooms made of wood lined with lead thickness 2 mm, this is not
compatible with ALARA principle.
For more details about the radio-diagnostic machines and rooms data sheet, see
annex (8).
These findings are consistent with the study of Giri et al. (2007), which was
conducted to measure of radiation at X-ray centers of a few hospitals in Kathmandue
city, Nepal. Their results revealed that the maximum radiation level noted at 4
different corners of radiation machine room was considered for the purpose of
statistical analysis.
These findings are also in line with Younis et al. (2014), which was conducted to
evaluation of radiation protection in radio-diagnostic departments in Erbil hospitals,
his results showed that the facilities for safety were grossly inadequate at places for
paramedics and technician room. Dose rates in front of window of the monitor room
and in the reception indicating higher health risk to the paramedic, visitors and
personnel at the hospital.
The results in the present work could be described in consistent with Adhikari et al.
(2012),which was conducted to evaluate the status of radiation protection at different
hospitals in Nepal. They observed the maximum calculated equivalent radiation level
(HW) is 0.006 mSv/week, which is within the safe limit. Radiation dose level
measurement, was also done at patient waiting area and inside the dark room. In
addition, leakage radiation test was performed by closing the collimators and reading
were obtained at one meter distance from the tube. There is a leakage in almost all
units which is not good in view of protection of the patients and average reading was

64
0.0075 mSv/week. Dose level at different reference point around CT scan unit shows
a maximum value of 0.057 mSv/week at door near the control console. Radiation
survey around the mammogram unit shows that all the area is very safe and built
according to protection criteria.
Furthermore, Ali (2013), study which conducted in X-ray diagnostic facility of
hospitals in Iraqi Kurdistan region. The results show that the facilities for safety were
grossly inadequate and the dose rates at the behind X-ray door room indicating
higher health risk to the visitors and personnel at the hospital. Similar results were
found in the study of Oluwafisoye et al. (2009), which was conducted in X-ray
diagnostic facility of a large Nigerian hospital. The results revealed that the dose rate
measured at the patient waiting room was far above the background radiation dose
rate, while at the reception, the dose rate was greater than the background dose rate
by factor of 20 mSv/yr. This high dose rate indicates a higher health risk to the
unsuspecting supportive personnel such as nurses, hospital attendants and visitors.
In brief, our results and findings are consistent and adequate with the results of
previous studies that above mentioned. This reveals the presence of ionizing
radiation leakage in different locations in radio-diagnostic centers and suggested to
be remediated.

65
Part two
4.5 The questionnaire contents analysis
Our study consists of 182 radio-diagnostic workers from nine selected hospitals,
where a questionnaire were distributed to obtain information for matching the study
needs. The questionnaire includes five parts as follows.
4.5.1 Socio-demographic and work related information
The first part of the questionnaire contained eight items about the socio-demographic
and work related information of participants who completed the questionnaire. The
results reveals an information about the participants percentage according to the
following items:
i. Participants occupation
Figure (4.18), shows 79.1% (n=144) of participants are medical radiographers and
20.9% (n=38) are radiologists.
Figure (4.18): Participants percentage according to their occupation
Radiologists
Medical radiographers
20.9%
79.1%

66
ii. Participants sex
There is a wide variation in sex of radio-diagnostic workers, where 76.1% (n=144) of
the study participants are males and 23.9% (n=43) females as illustrated in figure
(4.19). This result indicates that the most of radio-diagnostic workers are males and
this is attributed to the community culture towards women who working in radiology
field and their fear from transmitting the risk of radiation to their future generations.
A pproximatlely180 participant answered this question.
Figure (4.19): Participants percentage according to their sex
iii. Participants age groups
Figure (4.20): Participants percentage according to their age groups
0%
10%
20%
30%
40%
50%
60%
70%
80%
Male Female
76.1%
23.9%
Par
tici
pan
ts p
erce
nta
ge
0%
10%
20%
30%
40%
50%
From 20-29years
From 30-39years
From 40-49years
More than 50years
Par
tici
pan
ts p
erce
nta
ge
8.3%
21%
46.4%
24.3%

67
The study shows that the participants ages were between 30 and 39 years which
formulates 46.4% (n=84) of the participants. Figure (4.20), illustrates the percentage
of participates due to their ages. This indicates that the radio-diagnostic population
are young labors.
iv. Participants academic qualifications
About 174 participants out of 182 participants answered this question and gives a
result as illustrated in figure (4.21).
Figure (4.21): Participants percentage according to their academic qualifications
v. Participants practical experience
It is also about 178 participants from 182 persons answered the question related to
the practical experience. Figure (4.22), shows that the study population was
categorized into four groups according to their practical experience and refers that
most of the radio-diagnostic workers have sufficient practical experience in radio-
diagnostic field.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Diploma Bachelor Higher degrees
Par
tici
pan
ts p
erce
nta
ge
9.2% 8%
82.8%

68
Figure (4.22): Participants percentage according to their practical experience
vi. Participants distribution at the hospitals
Figure (4.23): Participants percentage according to their distribution at the hospitals
Clearly, it is found that the largest number of study participants from Al Shifa
Medical Complex, who formulates 31.3% (n=57) of the study participants. However,
the lowest number of study participants from Abdel Aziz Rantessi hospital who
formulates 4.9% (n=9) of the participants. Participants distribution in other hospitals
are illustrated in figure (4.23).
This result is not a surprise since the participants proportions depend on the number
of radio-diagnostic workers in each hospital, where Al Shifa Medical Complex is a
major one.
0%
5%
10%
15%
20%
25%
30%
35%
40%
1-4 years 5-9 years 10-14 years 15-20 years
36%
27%
19.1% 18% P
arti
cip
ants
per
cen
tage
0%5%
10%15%20%25%30%35%
Par
tici
pan
ts p
erce
nta
ge 31.3%
8.8% 9.3% 11%
15.9%
5.5% 6.6% 6.6% 4.9%

69
vii. Participants dealing with radio-diagnostic machines
As shown in figures (4.24). Basic X-ray machines is the most common used, which
formulates 83% (n=151) of participants. While 14.8% (n=27) of participants used
with mammography machines. We find that this result is reasonable because the
basic X-ray machines are the most prevalent in terms of the number and use in the
hospitals. Whereas, the dealing with the mammography machines restricted to
females workers.
Figure (4.24): Participants percentage according to their dealing with radio-
diagnostic machines
viii. Participants daily work hours in radio-diagnostic rooms
Figure (4.25): Participants percentage according to their daily work hours in radio-
diagnostic rooms
0
50
100
Radio-diagnosticmachines
0%
20%
40%
1-2 hours2-3 hours
3-4 hours4-5 hours
More than5 hours
14.8% 24.2%
58.8% 44%
83%
41.8%
8%
34.1% 27.8%
18.2% 11.9%
%
%
%

70
Most of radio-diagnostic workers that formulate 34.1% (n=60) working between 3
and 4 hours inside the radio-diagnostic rooms per day, while 27.8% (n=49) of the
participants working between 2 and 3 hours per day. Figure (4.25) exhibits the
participant percentage concerning daily work hours in radio-diagnostic rooms.
For more details about the socio-demographic and related work factors of the study
participants, see table no. (1) in annex (9).
4.5.2 Participants response to availability of personal radiation protection
devices items
The second part of the questionnaire contained ten items that reflects the current
level of availability of personal radiation protection devices and warning signs in
radio-diagnostic centers. The results about the availability of such devices in radio-
diagnostic centers according to the participants response are illustrated in figure
(4.26).
Figure (4.26): Participants response about the availability of personal radiation
protection devices items
0%10%20%30%40%50%60%70%80%90%
100%
Ava
ilab
ility
of d
evic
es
pe
rce
nt.
95.6%
41.8%
75.8%
26.4%
40.1%
22.5% 20.9% 15.9%
5.5% 7.1%
35.2%

71
The personal radiation protection devices are the principal for radiology workers
(Klein et al., 2009). A visible warning sign and caution light required to alert
individuals to radiological conditions (Radiation protection manual, 2010). However,
according to the participants knowledge, it is about 35.2% of personal radiation
protection devices are available in the radio-diagnostic centers at governmental Gaza
governorates hospitals.
As it displays in the figure (4.26), the maximum rate about the availability of
personal radiation protection devices specified to lead aprons and thyroid shields by
95.6% (n=174) and 75.8% (n=138) respectively. The minimum rate that related to
the availability of personal radiation protection devices specified to lead curtains,
breast shields and gonad shields by 5.5% (n=10), 7.1% (n=13) and 15.9% (n=29)
respectively.
In addition, There are a few participants have no idea about the availability of
personal radiation protection devices in radio-diagnostic centers such as lead
curtains, lead barriers and breast shields by 20.3% (n=37), 9.3% (n=17) and 7.7%
(n=14) respectively.
The percentage of participants who know that the lead glass available in radio-
diagnostic centers was about 41.8% (n=76). However, less percentage of participants
reported the availability of radiation warning signs and caution lights respectively.
These findings are in line with results of a study which was conducted by Adejumo
et al. (2012) in South West Nigeria. Their results revealed that some radiation
protection devices are available in large proportion in radio-diagnostic centers such
as: lead apron 96%,caution lights 98%, lead glass 19% and shield lead shields/barrier
77%. However, other radiation protection devices are available in low proportion in
radio-diagnostic centers such as: lead gloves 19%, breast shields 19%, lead curtains
36% and thyroid shields 24%.
72
In addition, these results are in an agreement with the study of Mojiri and
Moghimbeigi (2011) which conducted in various hospitals in Hamadan city, Iran.
They observed that different percent of radiographers awareness about the existence
of personal radiation protective devices in radiology centers, where that lead apron,
radiation signs and gonad shields are available in radiology centers by 98.6%, 80.3%
and 78.9% respectively. While lead glass, lead gloves and thyroid shields are
available in radiology centers by 28.2%, 35.2% and 67.6% respectively. In addition,
These findings are in adequate with Younis et al. (2014) which conducted to
radiation protection evaluation from radio-diagnostic departments in Erbil hospitals.
They showed that the facilities for safety were grossly inadequate at places for
paramedics and technician room.
For more details about the response of study participants to the availability of
personal radiation protection devices items, see table no. (2), in annex no. (9).
4.5.3 Participants response to awareness items about radiation protection
issues
The third part of the questionnaire contained eighteen items to measure the current
level of radio-diagnostic workers awareness about radiation protection issues.
Descriptive statistics include mean and percentage; where yes answers reflecting the
level of study participants awareness about radiation protection issues.
According to the results displayed in figure (4.27), about 74.8% of participants have
awareness toward radiation protection issues. This result indicates that the majority
of radio-diagnostic workers in governmental Gaza governorates hospitals have
relatively adequate awareness regarding radiation protection issues. This would not
surprise us since there is an educational lectures established recently in governmental
Gaza governorates hospitals regarding radiation protection and safety issues. Despite
this result is obtained, there is a dare need to increase the radio-diagnostic workers
awareness about some of radiation protection issues, which will be mentioned later.

73
Figure (4.27): Participants response to radiation protection awareness items
Clearly, the radio-diagnostic workers have a relatively well awareness about
radiation protection techniques. The highest value of percentage of participants who
know that short radiation exposure time during radiological examinations leads to
less patient radiation dose, and gives 97.8% (n=178). The participants awareness
about increase the distance from the radiation source to double the received dose will
be reduced to its half was about 74.2% (n=135).The rest either they said the opposite
or they did not know. While those who know that the thickness of the X-ray room
wall, which is exposed to primary X-rays should be 2 mm based on the principle of
ALARA about 64.3% (n=117) of participants response.
The item about the recommended distance between the X-ray source and radiology
workers is two meter have the lowest percentage of participants awareness and gives
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Sho
rt r
adia
tio
n e
xpo
sure
tim
e d
uri
ng…
The
per
iod
ic m
ain
ten
ance
fo
r X
-ray
…
The
mai
nte
nan
ce a
nd
cal
ibra
tio
n f
or
X-…
Pro
tect
ion
of
the
pat
ien
t an
d t
he
pu
blic
…
The
err
or
in t
he
sele
ctio
n o
f ap
pro
pri
ate…
The
exp
eri
ence
of
wo
rke
rs m
ust
be
take
n…
The
use
of
colli
mat
ion
du
rin
g…
Uti
lizin
g h
igh
kV
du
rin
g th
e gi
ven
…
Pro
tect
ive
lead
mu
st p
eri
od
ical
ly…
If t
he
dis
tan
ce in
cre
ase
d f
rom
th
e…
The
pri
mar
y ra
dia
tio
n b
arri
er
mu
st b
e…
The
an
nu
al a
vera
ge d
ose
ove
r fi
ve y
ear
s…
The
th
ickn
ess
of
the
X-r
ay r
oo
m w
all,…
Pu
blic
sh
ou
ld n
ot
be
exp
ose
d t
o m
ore
…
X-r
ay r
oo
m d
oo
rs m
ust
be
lin
ed o
n o
ne
…
The
idea
l Sp
ace
fo
r X
-ray
ro
om
sh
ou
ld…
Rad
iati
on
do
se li
mit
s fo
r p
regn
ant…
The
rec
om
men
ded
dis
tan
ce b
etw
een
th
e…
Ave
rage
Par
tici
pan
ts a
war
nes
s p
erce
nt.
89
.6%
93
.4%
94%
94
.5%
97
.8%
95
.1%
95
.6%
96
.7%
49
.5%
36
.8%
33
.5%
74
.8%
68
.7%
64
.3%
58
.8%
56
.6%
76
.4%
74
.2%
70
.9%

74
about 33.5% (n=61) of participants. Then it is followed by the item about radiation
dose limits for pregnant women which worked in radiation field and gives about
36.8% (n=67) of participants. Only 49.5% (n=90) of participants knew that the ideal
space for X-ray room should not be less than 36 m2, the ceiling height of 3.6 m and
the exterior windows must have a height of 2.2 m above the X-ray room floor. These
findings revealed that the radio-diagnostic workers in governmental hospitals in
Gaza governorates have limited awareness about specific radiation protection issues
in spite of their work in a radio-diagnostic field.
In the items regarding awareness about the annual average dose over five years
should not exceed (20 mSv) for occupational exposure, the responses were almost
68.7% (n=125) are aware of the annual average dose. While 19.8% (n=36) did not
aware that and 11.5% (n=21) said the opposite. About 58.8% (n=107) are aware on
public should not be exposed to more than an average of (1 mSv per year). Clearly
that the radio-diagnostic workers in governmental Gaza governorates hospitals have
inadequate awareness regarding permissible radiation dose limits in spite of their
work in a radio-diagnostic field.
Participants awareness was relatively high in a few issues. Most of them aware that
periodic maintenance for X-ray room walls, doors and radiation protection devices
should be tested to ensure their efficiency with a percentage of about 96.7% (n=176).
While only 2.2% (n=4) of them answered the opposite and 1.1% (n=2) they did not
know. Regarding the maintenance and calibration for X-ray machines must be
periodically performed to prevent radiation leakage by 95.6% (n=174). However,
about 95.1% (n=173) know that the protection of the patient and the public from
unnecessary radiation during radiological examinations are the responsibility of
radiology staff, while about 1.1% (n=2) of participants have no idea, and 3.8% (n=7)
said the opposite. Almost 94.5% (n=172) aware that the error in the selection of
appropriate kilovolts due to technical error or malfunction in the X-ray machine
leads to excessive radiation dose to the patient.

75
Approximately 94.0% (n=171) of the participants responded that the radio-diagnostic
workers should be involved in the X-ray machines purchase. The participants
awareness about the use of collimation during radiography has a great benefit in
reducing patient dose were about 93.4% (n=170) of the study participants. These
results indicate that the majority of the participants have positive awareness
regarding the numerous radiation protection issues.
In comparison of our results with others due to awareness level. There is an
agreement with the study of Mojiri and Moghimbeigi (2011) which was conducted in
various hospitals in Hamadan city, Iran. They revealed that the medical
radiographers have a good awareness about radiation protection issues. The same
results have been reported in the study of Amirzadeh and Tabatabaee (2005) in Iran
which was conducted to evaluate the awareness of employees about radiation
protection in Shiraz hospitals.
In comparison with other study performed by Adejumo et al. (2012) to evaluate the
compliance to radiation safety standard amongst radiographers in radio-diagnostic
centers in south west, Nigeria. The study reported that about 98% of respondents
have good knowledge of radiation protection issues.
The same results have been also reported in the study of Shah et al. (2007) which
conducted in Campus Peshawar, Pakistan, to assess the radiation protection
awareness levels in medical radiation technologists. They observed that the radiation
awareness knowledge levels in the sample group varied widely with a range of
median score of 75%. In addition, these findings are in line with Adhikari et al.
(2012) which conducted to evaluate the status of radiation protection at different
hospitals in Nepal. They observed that around 70% of the radiation workers are
aware of radiation safety issue.
However, the present work disagrees with the results of Abu Draz (2009) which
showed that the level of radiation protection knowledge among radio-technologists in
governmental hospitals in Gaza governorates almost 47.41%. This value indicates

76
that the majority of radio-technologists haven't high knowledge regarding radiation
protection issues of that time. These variations can be attributed to the educational
lectures established recently in governmental Gaza governorates hospitals that
regarding about radiation protection and safety issues.
There is also an disagreement with results reported in Mutyabule and Whaites (2002)
in Uganda. and in that of Salti and Whaites (2002) in Syria. This disagreement with
our results may be due to the difference in the cultures among various communities.
For more details about the response of study participants to awareness items about
radiation protection issues, see table no. (3), in annex no. (9).
4.5.4 Participants response to practices items about radiation protection
issues
The fourth part of the questionnaire contained fifteen items describe current level of
radio-diagnostic workers practices about radiation protection issues.
The results in figure (4.28), illustrates that, in spite the fact that 74.8% of participants
have awareness about radiation protection issues, but it is only about 53.4% of
participants follows the radiation protection practices. This result is surprising and
alarming. Clearly it seems unsatisfactory and indicates that the approximately half of
participants have negative practices toward radiation protection issues.
The statistical strength of these relationships are in line with the study carried out by
Slechta and Reagan (2008) which conducted to examination of factors related to
radiation protection practices in American society of radiologic technologists. They
reported that the mean scores for knowledge and compliance with safety practices
were 82% and 72%, respectively.

77
Figure (4.28): Participants response to radiation protection practices items
At the present work, the results of participants practices regarding of radiation
protection issues during their work in the radio-diagnostic centers, have shown the
majority of the participants 94.0% (n=171) stand behind the lead barrier when give
the radiation dose. However, 73.6% (n=134) of participants used the X-ray tube
collimation during the radiography in order to reduce patient surface that exposed to
X-ray, this means the radio-diagnostic workers interested in protecting themselves
and their patients from ionizing radiation. Also 74.7% (n=136) of participants make
sure that the X-ray door is closed during the examination. These results reflect that
the study participants follows some of positive radiation protection practices.
When the radio-diagnostic workers were asked if they explain the radiological
examination instructions to the patient before the exam, just about 52.2% (n=95) of
participants answered yes. While low percentage of participants don’t protect patient
escorts who holds the child during the radiological examination were about 31.3%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Par
tici
pan
ts p
ract
ices
per
cen
t.
34
.6%
36
.3%
3
6.8
%
52
.2%
55
.5%
59%
66
.5%
67
.6%
73
.6%
74
.7%
76
.4%
94%
31
.3%
25
.8%
16
.5%
53
.4%

78
(n=57). In addition, about 67.6% of participants wear and use the radiation protection
devices in order to protect themselves from ionizing radiation. We found only about
16.5% (n=30) of participants use the gonadal shield to protect the patients gonads
even if the doctor did not ask to protect these organs. This results may be due to only
15.9% of participants reported the availability of gonadal shield in radio-diagnostic
centers.
Approximately 55.5% (n=101) of participants reported that they asked the patient
escorts to evacuate the X-ray room before giving the X-ray dose. We also found that
this result is un satisfactory when compared with participants awareness about
radiation protection issues. This result reflects that the study participants follow
some of negative practices toward radiation protection issues.
The responses related to item about radiation protection course, show less than half
of radio-diagnostic workers have participated in a radiation protection course
(34.6%). Similar studies such as Mojiri and Moghimbeigi (2011) which was
conducted in in various hospitals in Hamadan city, reported that there less than half
of the technicians have participated in a radiation protection course (43.7%). In
comparison with the other study performed by Noohi (2009) in Kerman (Iran)
revealed that half of the radiographers in diagnostics radiology centers have
participated in a radiation protection course (50%).
Regarding responses to using of portable X-ray items, only 66.5% (n=121) of
participants take the necessary precautions to protect patient escorts and other
patients in the room when using the portable X-ray machine. When the participants
were asked if they keep the recommended distance from the radiation source, a
relatively high percentage of participants 76.4% (n=139) answered positively.
When the participants were asked if they believe that your radio-diagnostic centers
conformity with the safety and radiation protection standards, the responses were
55.5% (n=101) response negatively. While 36.3% (n=66) answered positive and
8.2% (n=15) answered don’t know. The importance of this study was to determine

79
whether the radio-diagnostic centers safe or not. This result contradict by Adejumo et
al. (2012) study, which reported that 65% of radiographers believe that there is a
radiation safety in the workplace. This disagreement possibly because of differences
in the design, construction and lead lined of X-ray rooms.
When the participants were asked if they participants interested in maintenance
conducting for X-ray machines when the defect related with radiation protection,
59.0% (n=109) answered yes. While about 58.8% (n=107) of participants show
carelessly to check the radiology center when there is suspicion of radiation leakage.
However, about 50.5% (n=92) of participants answered that the administration does
not respond to the demands of workers related to check the X-ray rooms to make
sure of their safety. This result is highly associated with opinion of 64.9% of
participants that the negligence in radiation protection issues caused by the lack of
radiation safety officer to provide the service.
These results are agreement with the study of Abu Draz (2009) which showed that
the level of radiation protection practices among radio-technologists in governmental
hospitals in Gaza governorates was about 45%. Clearly, this result indicates that the
majority of radio-technologists have low practices level regarding radiation
protection issues..
This result is also adequate with Tavakoli et al. (2003) which was conducted in Iran,
who revealed that the medical students in Birjand University of medical sciences
have low level of practices regarding radiation protection.
For more details about the responses of study participants to practices items about
radiation protection issues, see table no. (4), in annex no. (9).

80
4.5.5 Participants response to personal radiation exposure monitoring
process items
The fifth part of the questionnaire contained seven items to evaluate current level of
personal radiation exposure monitoring process.
Descriptive statistics include mean and percentage were carried out. According to the
study results, just about 29.9% of study participants have positive evaluation toward
personal radiation monitoring process. This result indicates that the majority of
radio-diagnostic workers in governmental Gaza governorates hospitals undergoes to
radiation risks. Certainly, this cannot be purposely assessed and corrective measures
will become difficult.
These results are in an agreement with the study of Iortile et al. (2013), the study has
revealed that the levels of monitoring the absorption of radiation by radiology
workers in most hospitals surveyed in Makurdi metropolis are very poor. These
findings are in line with Okaro et al. (2010) study which reported that personal
radiation monitoring radio-diagnostic centers in South Eastern Nigeria is abysmally
poor.
i. Availability of radiation protection adviser
The results in figure (4.29), show that the radiation protection advisers or supervisors
are not available in the radio-diagnostic centers surveyed. About 95.6% (n=174) of
study participants don't have radiation protection adviser in radio-diagnostic centers.
This result agrees with the results of Okaro et al. (2010) which conducted to
evaluation of personal radiation monitoring in radio-diagnostic centers in south
eastern Nigeria, which showed that radiation protection advisers are hardly available
in the centers surveyed. They were found only in four centers when ideally they
should be in every radiology centers.

81
Figure (4.29): Participants response about availability of radiation protection
advisors
ii. Availability of personal radiation exposure monitoring devices
As shown in figure (4.30), about 60.4% (n=111) of study participants have a personal
radiation exposure monitoring device.
Figure (4.30): Participants response about availability of personal radiation exposure
monitoring devices
iii. Use of personal radiation exposure monitoring devices during their work in
radio-diagnostic rooms
As shown in figure (4.31), about 55% (n=61) of participants who have personal
radiation exposure monitoring device use this device during their work in radio-
diagnostic rooms. While 31.5% (n=35) of participants sometimes use this device.
About 13.5% (n=15) of participants who have personal radiation exposure
monitoring device don’t use this device during their work in radio-diagnostic rooms.
Yes
No
Yes
No
Participants response
95.6%
4.4%
60.4%
39.6%

82
.
Figure (4.31): Participants response about using of personal radiation exposure
monitoring device during their work in radio-diagnostic rooms
iv. Receive of guidance about using the devices
As shown in figure (4.32), the most of participants who have a dosimeter don't
receive guidance about the proper handling with the personal radiation exposure
monitoring devices, this represents about 75.7% (n=84) of participants.
Figure (4.32): Participants response about receiving guidance about the proper
handling with the personal radiation exposure monitoring device
v. Safety officers interest with the devices measurements
As shown in figure (4.33), there are a big problem in personal radiation exposure
monitoring process, majority of the participants 64.9% (n=72) believe that the
measurements results doesn’t take into consideration by the safety officers.
0%
20%
40%
60%
Yes Sometimes No
Per
cen
tage
of
resp
on
se
0%
20%
40%
60%
80%
YesNo
55%
13.5%
31.5%
24.3%
75.7%

83
Figure (4.33): Participants response about safety officers interest with the devices
measurements
vi. Availability of another personal radiation exposure monitoring device
As shown in figure (4.34), there is no one of radio-diagnostic workers receive a new
personal radiation exposure monitoring device when the devices collect to measure
of radiation dose.
Figure (4.34): Participants response about availability of new device when the
devices collect to measure of radiation dose
vii. The reasons for lack of these devices
As shown in figure (4.35), there are a miscellaneous reasons advanced by the study
participants about the negligence in personal radiation exposure monitoring process.
Majority of participants 64.9% (n=63) believe that there is no radiation safety officer
to provide the service. While about 57.7% (n=56) believe that another reason was put
0%
20%
40%
60%
80%
YesNo
Per
cen
tage
of
resp
on
se
Yes 0%
No 100%
100%
Participants response
64.9%
35.1%

84
forward by the participants. This is due to the carelessly of hospital management, that
represent about 57.7% (n=56). Another opinion reports that there is lack of fund to
purchase these devices and this represents about 32.0% (n=31). Finally, 24.7%
(n=24) of participants believe that the radio-diagnostic workers do not request the
dosimeters.
Figure (4.35): Participants response about the reasons for lack of personal radiation
exposure monitoring devices
Almost similar reasons with different in ratios were found in the Iortile et al. (2013)
study, which conducted in Makurdi Metropolis, and reported the percentages of
7.5%, 17.5%, 10%, 32.5% and 32.5% for various reasons as: unavailability of
radiation safety officers, lack of funds, radiology workers do not request for personal
radiation monitoring, hospital management do not provide for it and others,
respectively.
In addition, almost similar reasons with different values were found in the Okaro et
al. (2010) study, which conducted in South Eastern Nigeria. They reported that about
(9.8%) of participants believe that there is no radiation safety officer to provide the
service, (14%) of participants reports that there is lack of funds, (4.9%) of
participants believe that the radiographers do not request for personal radiation
monitoring and (41.5%) of participants believe that the hospital management do not
provide for it in its budget. However, about (29.2%) of participants reports other
reasons for lack of these devices.
0
20
40
60
80No radiation safety officer toprovide the service
Carelessly of hospitalmanagement
Lack of fund to purchasethese devices
Radiology workers do notrequest these devices
64.9%
24.7%
32%
57.7% %
%
%
%
%

85
The results of present work agree with the safety policies and procedures manual on
radiation safety conducted in Washington State University (2000). This manual
reported that the employees should receive a radiation monitoring device for
monitoring radiation exposure.
In addition, our results are found in line with Okaro et al. (2010) study who show
that personal radiation monitoring is available only in a few hospitals and in most
cases does not cover all the radiographers on employment. This finding agrees with
the result of a previous survey which carried by Okpala (2004) which covered 28 X-
ray centers in two states of south eastern Nigeria. The survey result showed that
radiation monitoring was almost non-existent in the centers. Furthermore, the
obtained results are in line with Younis et al. (2014) who carried out his work in
radio-diagnostic departments in Erbil hospitals. His results revealed that the personal
monitoring (TLD badges) were not provided in the majority of departments. Our
results are also agrees well with Adhikari et al. (2012) which conducted to evaluate
the status of radiation protection at different hospitals in Nepal, which observed the
personal monitoring for radiation workers cannot be easily determined. This is due to
around 65% of radiation workers are not monitored for radiation exposure owing
insufficient of monitoring devices.
In comparison with the other study performed similar results were found in the study
of Ali (2013) which was conducted in X-ray diagnostic facility of hospitals in Iraqi
Kurdistan region, and its results revealed that the personal monitoring (TLD badges)
were not provided for radiographers.
Our results, also give a good agreement with Iortile et al. (2013) study, which
observed that personal radiation monitoring is available only in one hospital. This
indicates that, radiation monitoring devices are not easily provided in most of radio-
diagnostic centers of hospitals.
Clearly, a poor level of personal radiation exposure monitoring is found in the
present work. This is due to radiation monitoring insufficient to cover all the radio-

86
diagnostic workers, where the results shows that the devices are available for only
60.4% (n=110) of study participants. Rosenbloom (2007), revealed in his article that
the risk level from radiation exposure could not be assessed perfectly. Since we are
in dare need for a sensitive devices for radiation exposure monitoring.
For more details about the responses of study participants to evaluation of personal
radiation exposure monitoring process items, see table no. (5), in annex no. (9)
4.6 The relationship between the independent variables and the
participants response to radiation protection issues
The independent samples t-test, frequency, one-way analysis of variance (ANOVA),
mean and the standard deviation were carried out and developed in order to meet the
study purpose.
Therefore, the relationship between the level of availability the personal radiation
protection devices, awareness and practices regarding radiation protection issues and
evaluation of personal radiation exposure monitoring process as a dependent
variables. However, the socio-demographic and work related factors for workers as
independent variables will be discussed in the following section.
i. Age effect
The radio-diagnostic workers who participated in this study were categorized into
four groups according to their age groups as mentioned previously. The following
table (4.1), shows the results of dependent variable throughout the participants
according to their age groups.

87
Table (4.1): The dependent variables according to participants age
Items Age No. Mean Std. F Sig.
Availability of
devices
From 20-29 years 44 40.00 21.67
2.024
0.112
From 30-39 years 84 34.29 19.59
From 40-49 years 38 30.26 15.85
More than 50 years 15 39.33 18.31
Awareness
From 20-29 years 44 73.61 14.68
2.18
0.092
From 30-39 years 84 74.07 14.26
From 40-49 years 38 74.42 14.47
More than 50 years 15 83.70 9.73
Practices
From 20-29 years 44 53.03 21.23
4.721
0.003
From 30-39 years 84 49.05 21.45
From 40-49 years 38 55.44 25.66
More than 50 years 15 72.00 18.55
Radiation
monitoring
From 20-29 years 44 23.11 26.22
2.879
0.037
From 30-39 years 84 33.93 25.67
From 40-49 years 38 25.00 26.78
More than 50 years 15 41.11 33.85
The above table illustrates that age group between 20 and 29 years has the highest
mean value (40). This means that the participants in this age group recorded highly
availability of personal radiation protection devices in the radio-diagnostic centers.
While the age group between 40 and 49 years has the lowest mean value (30.26).
According to one-way variance (ANOVA) analysis, (P value=0.112), there are no
statistically significant differences between availability and age groups. Clearly that
the calculated p-value is greater than the significant level which is equal 0.05 (p-
value > 0.05).This indicates that there is no effect of age groups on the evaluation of
the availability of personal radiation protection devices in radio-diagnostic centers.
So, the null hypothesis that there is no differences between the evaluation of the
availability of radiation protection devices in radio-diagnostic centers and their age
groups is accepted and the researcher hypothesis is rejected.
Regarding the awareness items. It is noticed that the age group more than 50 years
has higher awareness than the other age groups, and gives mean value (83.70).

88
Moreover, there is no statistically significant differences among age groups and
participants awareness (p-value=0.092). So, the null hypothesis "there is no
relationship between the awareness of radio-diagnostic workers about radiation
protection issues and their age groups is accepted and the researcher hypothesis
rejected. This result may be attributed to the older age radio-diagnostic workers are
more careful about their health, while the younger workers careless. This result are in
line with Su, et al., (2000) study result, which observed there is a significant
difference shown between radiation safety knowledge and the growth of the age and
the career period of radiological technologists who work at medical centers in
Taiwan.
Regarding the practices items. According to one-way variance (ANOVA) analysis,
(P value=0.003), the results reflect there is a difference in the practices mean among
the radio-diagnostic workers according to their age groups. The highest mean value
(72) was for age group more than 50 years, while the lowest mean value (49.05) was
for age group between 30 and 39 years. So, the alternative hypothesis that there is
statistically significant relationship between the participants practices regarding
radiation protection and their age groups is accepted.
Regarding the evaluation of personal radiation exposure monitoring process items.
Clearly that there is a statistically significant difference according to the participants
age groups (p-value=0.037), this difference is highest among radio-diagnostic
workers with age groups more than 50 years, with mean value (41.11). The lowest
mean (23.11) is among age group between 20 and 29 years. This is logical result and
reflects that the new employees are not included in the personal radiation exposure
monitoring process. So, the alternative hypothesis that there is statistically significant
relationship between the radio-diagnostic workers evaluation of monitoring process
and their age groups is accepted.

89
ii. Sex effect
As shown in Table (4.2), the mean of availability of personal radiation protection
devices among participants males (34.67) is slightly more than females (36.28).
According to one-way variance (ANOVA) analysis, (p-value=0.636), there are no
statistically significant differences due to their sex. So, the null hypothesis that there
is no relationship between the evaluation of the availability of personal radiation
protection devices and their sex is accepted and the researcher hypothesis is rejected.
Regarding the awareness items. The mean of awareness among participants males
(74.53) is slightly less than females (75.19). According to one-way variance
(ANOVA) analysis, (p-value=0.791), there is no relationship between the awareness
of radio-diagnostic workers regarding radiation protection and their sex. So, the null
hypothesis that there is no relationship between the awareness of radio-diagnostic
workers regarding radiation protection issues and their sex is accepted and the
researcher hypothesis is rejected. These findings are in line with Su et al., (2000)
study results, there is no significant difference shown between radiation safety
knowledge and gender of radiological technologists who work at medical centers in
Taiwan.
Regarding the practices items. The results demonstrate that there is a slight
difference in the mean of participants due to their sex. The practices mean among
males (52.99) slightly higher than females (53.18). According to one-way variance
(ANOVA) analysis, there are no relationship between the participants practices
regarding radiation protection and the sex. So, the null hypothesis that there are no
relationship between the practices of radio-diagnostic workers regarding radiation
protection issues and their sex is accepted and the researcher hypothesis is rejected.
Regarding the evaluation of personal radiation exposure monitoring process items.
The results reflect that the mean among males (29.56) is slightly less than among
females (32.17). According to one-way variance (ANOVA) analysis, (p-
value=0.584), there is no relationship between the evaluation regarding personal

90
radiation monitoring process and the gender of radio-diagnostic workers. So, the null
hypothesis that there is no relationship between the evaluation regarding personal
radiation monitoring process and their sex is accepted and the researcher hypothesis
is rejected.
Table (4.2): The dependent variables according to participants sex
Items Sex No. Mean Std. t Sig.
Availability of
devices
Male 137 34.67 18.87 -0.474
0.636
Female 43 36.28 21.05
Awareness Male 137 74.53 14.72 -0.266
0.791
Female 43 75.19 12.32
Practices Male 137 52.99 23.25 -0.047
0.963
Female 43 53.18 21.01
Radiation
monitoring
Male 137 29.56 27.34 -0.548
0.584
Female 43 32.17 26.82
iii. Occupation effect
As shown in table (4.3), the mean of availability of personal radiation protection
devices among medical radiographers (35.83) is slightly higher than that among
radiologists (32.63). According to one-way variance (ANOVA) analysis, (p-
value=0.368 ). There are no statistically significant differences in the evaluation of
the availability of personal radiation protection devices due to their occupation. So,
the null hypothesis that there is no relationship between the evaluation of the
availability of personal radiation protection devices and their occupation is accepted
and the researcher hypothesis is rejected.
Regarding the awareness items. The mean of awareness among medical
radiographers (75.96) is slightly higher than that among radiologists (70.32).
According to one-way variance (ANOVA) analysis, (p-value=0.029).There is a
statistically significant relationship between radio-diagnostic workers awareness
toward radiation protection issues due to their occupation. So, the alternative
hypothesis that there is a statistically significant relationship between the radio-

91
diagnostic workers awareness regarding radiation protection issues and their
occupation is accepted.
Regarding the practices items. Clearly that the radiation protection practices mean
among medical radiographers (54.86) is higher than among radiologists (48.07).
According to (p-value=0.104). There are no statistically significant differences. So,
the null hypothesis that there is no statistically significant relationship between the
radio-diagnostic workers practices regarding radiation protection issues and their
occupation is accepted and the researcher hypothesis is rejected.
Regarding the evaluation of personal radiation exposure monitoring process items.
The medical radiographers have a highest mean (35.88), while the radiologists have a
lowest mean (8.77). According to (p-value=0.000). There are a highly statistically
significant differences. So, the alternative hypothesis that there is statistically
significant relationship between the radio-diagnostic workers evaluation regarding
personal radiation exposure monitoring process and their occupation is accepted.
Table (4.3): The dependent variables according to participants occupation
Items Occupation No. Mean Std. t Sig.
Availability of
devices
Radiologist 38 32.63 17.96 -0.902
0.368
Medical radiographer 144 35.83 19.84
Awareness Radiologist 38 70.32 15.30 -2.199
0.029
Medical radiographer 144 75.96 13.73
Practices Radiologist 38 48.07 25.94 -1.635
0.104
Medical radiographer 144 54.86 21.89
Radiation
monitoring
Radiologist 38 8.77 16.32 -5.952
0.000
Medical radiographer 144 35.88 26.76
iv. Academic qualification effect
As show in table (4.4), the results reflect some differences between the means of
availability of personal radiation protection devices among radio-diagnostic workers
due to their academic qualification. The mean of radio-diagnostic workers who have

92
bachelor degrees (36.11) is slightly higher than the mean for those who have higher
degree (35.71) and those who have diploma is (31.25). According to (p-
value=0.648). There are no statistically significant differences. So, the null
hypothesis that there is no relationship between the evaluation of the availability of
personal radiation protection devices among radio-diagnostic workers and their
academic qualification is accepted and the researcher hypothesis is rejected.
Regarding the awareness items. The results demonstrate that there is slightly
differences in the mean of radio-diagnostic workers awareness between those who
have diploma (78.13), those who have higher degree (75.00) and those who have
bachelor degrees (74.50). According to (p-value=0.631). There is no relationship
between the awareness level regarding radiation protection issues and the academic
qualification of radio-diagnostic workers. So, the null hypothesis that there is no
statistically significant relationship between the radio-diagnostic workers awareness
level regarding radiation protection issues and their academic qualification is
accepted and the researcher hypothesis is rejected. There is an agreement with Abu
Draz (2009) study, which revealed that there is no statistically significant difference
in knowledge level due to the educational level of radio-technologists in
governmental Gaza governorates hospitals.
Regarding the practices items. According to one-way variance (ANOVA) analysis,
(p-value=0.008). Clearly that there is a statistically significant difference in the radio-
diagnostic workers practices according to their academic qualification. So, the
alternative hypothesis there is a statistically significant relationship between the
radio-diagnostic workers practices regarding radiation protection issues and their
academic qualification is accepted. This result may be attributed to the quality of
education materials and curriculum given to the three different groups. This result is
also commensurate with the level of radiation protection awareness of each group as
mentioned above.
Regarding the evaluation of personal radiation exposure monitoring process items.
The mean of radio-diagnostic workers who have diploma (47.92) is higher than those

93
who have bachelor degrees (30.09) ) and those who have higher degree (20.24).
According to (p-value=0.013). There is statistically significant difference. So, the
alternative hypothesis there is relationship between the evaluation regarding personal
radiation exposure monitoring process among radio-diagnostic workers and their
academic qualifications is accepted and the researcher hypothesis is rejected.
Table (4.4): The dependent variables according to participants academic qualification
Items Education No. Mean Std. F Sig.
Availability of
devices
Diploma 16 31.25 19.28 0.435
0.648
B.Sc. 144 36.11 20.11
Higher degree 14 35.71 16.51
Awareness
Diploma 16 78.13 10.44 0.462
0.631
B.Sc. 144 74.50 14.68
Higher degree 14 75.00 14.25
Practices
Diploma 16 70.42 19.62 4.967
0.008
B.Sc. 144 52.04 22.32
Higher degree 14 55.24 23.45
Radiation
monitoring
Diploma 16 47.92 27.13 4.433
0.013
B.Sc. 144 30.09 26.76
Higher degree 14 20.24 25.47
v. Practical experience effect
From table (4.5), The availability of personal radiation protection devices differs
according to the participants practical experience. The radio-diagnostic workers who
have between 15 and 19 years of practical experience have a highest mean value
(39.47) , while the lowest mean value (30.83) for those who have between 10 and 14
years. According to the one-way (ANOVA) test results (p-value=0.287).This
indicates that, there is no relationship between level of evaluation of the availability
of radiation protection devices among radio-diagnostic workers and their practical
experience years. So, the null hypothesis that there is no relationship between level
of evaluation of the availability of radiation protection devices among the radio-

94
diagnostic workers and their years of practical experience is accepted and the
researcher hypothesis is rejected.
Regarding the awareness items. The radio-diagnostic workers who have more than
20 years of practical experience have a highest mean value (81.48), while the lowest
mean value (71.09) for those who have between 5 and 9 practical experience years.
According to the one-way (ANOVA) test results (p-value=0.017). There is a
statistically significant difference in the radio-diagnostic workers awareness level
due to their years of practical experience. So, the alternative hypothesis that there is a
relationship between the radio-diagnostic workers awareness level regarding
radiation protection issues and their practical experience years is accepted and the
researcher hypothesis is rejected.
There is an agreement with Mojiri and Moghimbeigi (2011) study result, which was
conducted in various hospitals in Hamadan city. The result revealed that there is a
statistically significant relationship between the work experiences and awareness of
radiation protection. The low experiences workers have less information about
radiation protection issues.
In addition, this result in line with Su et al. (2000) study result, which observed there
is a significant difference was shown between radiation safety knowledge and years
of practical experience of radiological technologists who work at medical centers in
Taiwan. Radiation safety knowledge of the college level for radiological
technologists is significant better than the junior college level ones.
Regarding the practices items. The radio-diagnostic workers who have more than 20
years of practical experience have a highest mean value (75.11), while the lowest
mean value (47.19) for those who have between 5 and 9 years of practical
experience. According to the one-way (ANOVA) test results (p-value=0.000).There
is a highly statistically significant difference in the radio-diagnostic practices due to
their practical experience years. So, the alternative hypothesis that there is a
statistically significant relationship between the radio-diagnostic workers practices

95
regarding radiation protection issues and their years of practical experience is
accepted. This result may be attributed to long-term of occupational radiation doses
for those who have more than 20 years of work. So, this group of radio-diagnostic
workers has become more concerned about the health impacts from radiation
exposures than those who have less period of experience. Hence, they applied the
protection procedures more carefully to decrease the probability of radiation risks on
their health.
Regarding the evaluation of personal radiation exposure monitoring process items.
The radio-diagnostic workers who have more than 20 years of practical experience
have a highest mean value (48.89), while those who have between 1 and 4 years of
practical experience have the lowest mean value (13.54). This result is surprising and
alarming. It should be strongly recommended to improve the personal radiation
exposure monitoring process for them. According to the one-way (ANOVA) test
results (p-value=0.000).There are a highly statistically significant differences in the
evaluation of personal radiation exposure monitoring process due to their practical
experience years. So, the alternative hypothesis that there is a statistically significant
relationship between the participants evaluation regarding personal radiation
exposure monitoring process and their years of practical experience is accepted.
Table (4.5): The dependent variables according to participants practical experience
Items Experience No. Mean Std. F Sig.
Availability of
devices
From 1-4 years 32 39.06 24.14
1.261
0.287
From 5-9 years 64 35.31 19.92
From 10-14 years 48 30.83 15.96
From 15-19 years 19 39.47 17.79
More than 20 years 15 32.00 16.56
Awareness
From 1-4 years 32 78.99 12.91
3.088
0.017
From 5-9 years 64 71.09 14.21
From 10-14 years 48 73.61 14.24
From 15-19 years 19 78.07 13.67
More than 20 years 15 81.48 13.55
Practices From 1-4 years 32 53.13 18.97 7.493 0.000

96
From 5-9 years 64 47.19 22.04
From 10-14 years 48 49.72 22.04
From 15-19 years 19 67.02 22.50
More than 20 years 15 75.11 19.76
Radiation
monitoring
From 1-4 years 32 13.54 20.93
5.414
0.000
From 5-9 years 64 32.29 25.70
From 10-14 years 48 30.21 25.65
From 15-19 years 19 33.33 31.43
More than 20 years 15 48.89 29.86
vi. Hospitals effect
From table (4.6), shows clear differences between the radio-diagnostic workers
evaluation of the availability of personal radiation protection devices according to
their hospitals. Abdel Aziz Rantessi Martyr Pediatric hospital obtain the highest
mean value (63.33), while Beit Hanoun hospital obtain the lowest mean value
(15.00). According to the one-way (ANOVA) test results (p-value=0.000), there are
highly statistically significant differences in the availability due to their hospitals. So,
the alternative hypothesis that there is a statistically significant relationship between
the evaluation of the availability of personal radiation protection devices and their
hospitals is accepted.
Regarding the awareness items. Al Naser Pediatric hospital obtain the highest mean
value (85.65), while Abdel Aziz Rantessi Martyr Pediatric hospital obtain the lowest
mean value (69.14). According to the one-way (ANOVA) test results (p-
value=0.028), there are a statistically significant differences in the awareness level
due to their hospitals. So, the alternative hypothesis that there is a statistically
significant relationship between the awareness level regarding radiation protection
issues and their hospitals is accepted.
These findings contradict the Su et al. (2000) study results, that revealed there is no
significant difference was shown between radiation safety knowledge and work place
of radiological technologists who work at medical centers in Taiwan. This difference

97
in the outcomes of the studies may be attribute to the existence of a difference in the
nature of work in hospitals between the two countries.
Regarding the awareness items. The mean of radio-diagnostic workers practices in
Al Naser Pediatric hospital (67.22) is higher than other hospitals. According to (p-
value=0.001). There is a highly statistically significant difference. So, the alternative
hypothesis that there is a relationship between the radio-diagnostic workers practices
regarding radiation protection issues is accepted and the researcher hypothesis is
rejected.
Regarding the evaluation of personal radiation exposure monitoring process items.
Abu Yousef Al Najjar Martyr hospital obtain the highest mean value (45.83), while
Nasser Medical Complex obtain the lowest mean value (24.71). According to the
one-way ANOVA test results (p-value=0.134),there is no relationship between level
of evaluation of personal radiation exposure monitoring process and their hospitals.
So, the null hypothesis that there is no relationship between the evaluation of
personal radiation exposure monitoring process among the radio-diagnostic workers
and their hospitals is accepted and the researcher hypothesis is rejected.
Table (4.6): The dependent variables according to participants hospitals
Items Hospital No. Mean Std. F Sig.
Availability of
devices
European Gaza hospital 16 31.25 10.25
8.337
0.000
Nasser Medical Complex 29 43.45 20.58
Abu Yousef Al Najjar hospital 12 22.50 6.22
Al Aqsa Martyrs hospital 20 34.00 11.42
Al Shifa Medical Complex 57 38.77 19.28
Abdel Aziz Rantessi hospital 9 63.33 11.18
Al Naser hospital 12 31.67 23.29
Kamal Adwan hospital 17 22.35 16.78
Beit Hanoun hospital 10 15.00 9.72
Awareness
European Gaza hospital 16 70.83 15.52 2.221
0.028
Nasser Medical Complex 29 71.26 13.03
Abu Yousef Al Najjar hospital 12 70.37 17.14

98
Al Aqsa Martyrs hospital 20 74.17 16.74
Al Shifa Medical Complex 57 78.36 12.93
Abdel Aziz Rantessi hospital 9 69.14 14.46
Al Naser hospital 12 85.65 14.88
Kamal Adwan hospital 17 73.53 8.68
Beit Hanoun hospital 10 71.67 13.21
Practices
European Gaza hospital 16 43.33 26.22
3.484
0.001
Nasser Medical Complex 29 42.76 21.49
Abu Yousef Al Najjar hospital 12 56.11 16.69
Al Aqsa Martyrs hospital 20 42.00 25.05
Al Shifa Medical Complex 57 59.53 21.19
Abdel Aziz Rantessi hospital 9 54.81 22.80
Al Naser hospital 12 67.22 13.77
Kamal Adwan hospital 17 56.08 19.73
Beit Hanoun hospital 10 63.33 25.39
Radiation
monitoring
European Gaza hospital 16 25.0 21.08
1.58
0.134
Nasser Medical Complex 29 24.71 28.74
Abu Yousef Al Najjar hospital 12 45.83 18.97
Al Aqsa Martyrs hospital 20 27.50 26.64
Al Shifa Medical Complex 57 26.90 28.65
Abdel Aziz Rantessi hospital 9 42.59 22.22
Al Naser hospital 12 38.89 32.05
Kamal Adwan hospital 17 27.45 25.65
Beit Hanoun hospital 10 43.33 26.29
vii. Daily work hours in radio-diagnostic rooms effect
The above table shows that the participants who work more than 5 hours have the
highest mean value (40). This means that the participants in this group is the most
recorded about the availability of personal radiation protection devices in their radio-
diagnostic centers. While the participants who work between 1 and 2 hours have the
lowest mean value (32.4). There are no statistically significant differences between
availability and daily work hours (P value=0.733). So, the null hypothesis that there
is no differences between the evaluation of the availability of radiation protection

99
devices in radio-diagnostic centers and their daily work hours is accepted and the
researcher hypothesis is rejected.
Regarding the awareness level items. It is clearly that the radio-diagnostic workers
who work between 2 and 4 hours have lowest mean value (72.3).While the radia-
diagnostic workers who work between 4 and 5 hours have a highest mean value
(80.7).This means that they have higher awareness level than the other groups.
Moreover, there is no statistically significant differences between the daily work
hours and participants awareness level (p-value=0.108). So, the null hypothesis
"there is no relationship between the awareness level of radio-diagnostic workers
about radiation protection issues and their daily work hours is accepted and the
researcher hypothesis is rejected .
Regarding the awareness items. Clearly that there is a statistically significant
difference in the radio-diagnostic workers practices according to their daily work
hours (p-value=0.008). This difference is high among radio-diagnostic workers who
work more than 5 hours (67.1), the lowest is among radio-diagnostic workers who
work between 2 and 4 hours (46.7). So, the alternative hypothesis there is a
statistically significant relationship between the radio-diagnostic workers practices
regarding radiation protection issues and their daily work hours is accepted .
Regarding the evaluation of personal radiation exposure monitoring process items.
The mean among participants who work between 4 and 5 hours is (35.9), slightly
more than other participants groups, where (p-value=0.048).This indicates there is no
statistically significant differences. So, the null hypothesis that there is no
relationship between the evaluation of personal radiation exposure monitoring
process and their daily work hours is accepted and the researcher hypothesis is
rejected.

100
Table (4.7): The dependent variables according to participants daily work hours in
radio-diagnostic rooms
Items Daily work hours No. Mean Std. F Sig.
Availability of
devices
From 1-2 hours 21 32.4 21.2
0.504
0.733
From 2-3 hours 49 36.9 22.7
From 2-4 hours 60 36.0 18.5
From 4-5 hours 32 33.1 17.5
More than 5 hours 14 40.0 15.2
Awareness
From 1-2 hours 21 74.6 13.6
1.928
0.108
From 2-3 hours 49 73.7 15.9
From 2-4 hours 60 72.3 14.8
From 4-5 hours 32 80.7 11.3
More than 5 hours 14 75.0 11.9
Practices
From 1-2 hours 21 56.2 20.5
4.192
0.003
From 2-3 hours 49 52.9 21.9
From 2-4 hours 60 46.7 21.7
From 4-5 hours 32 62.3 22.8
More than 5 hours 14 67.1 21.8
Radiation
monitoring
From 1-2 hours 21 31.0 29.5
1.002
0.408
From 2-3 hours 49 32.7 26.1
From 2-4 hours 60 25.6 27.7
From 4-5 hours 32 35.9 28.4
More than 5 hours 14 25.0 25.9

101
Chapter 5
Conclusion and Recommendations
5.1 Conclusion
In the present work, radiation level measurements for radio-diagnostic centers was
carried out in nine selected governmental hospitals at Gaza governorates. These
include: 19 basic X-ray, 8 fluoroscopy, 1 mammography and 3 CT scan machines.
The equivalent radiation dose rate were measured experimentally at different
locations in the radio-diagnostic rooms at the selected hospitals. These locations are:
directional dose rate , at one meter distance from the X-ray tube, at control panel, at
corridor outside the X-ray room, at dark room , behind the chest stand wall and at
patient waiting rooms. In addition, data sheets are used to obtain information about
the radio-diagnostic machines and rooms specifications.
In general, the results indicate that the fluoroscopy and CT scan rooms were not
efficiently lead lined and the radiation protection is not well organized. Since, the
measured values at corridors during closing the doors and at patient waiting rooms in
fluoroscopy and CT scan rooms suggests very high exceedance compared to the
reference limit for public exposure. Thus, it is noticed that a health risk of radiation
exposure for all persons who visiting these rooms. Also, the measured equivalent
radiation dose rate at control panels give high doses values, but remain in the
permissible limit for radiology workers. However, there is an impending risk of
chronic occupational exposure to the employees. In addition, we have noticed that
the CT scan room at Al Shifa Medical Complex ranked the first in term of the
highest radiation dose rate, and gives (14.2 mSv/yr). Then followed by fluoroscopy
room at Nasser Medical Complex, and gives (10.9 mSv/yr).
Moreover, the equivalent radiation doses rate that measured at a different locations in
basic X-ray and mammography rooms are found within the permissible limits for
radio-diagnostic workers and public. This indicates that these rooms are built safe
and well organized according to safety criteria. Also, the results suggest that the

102
importance of using radiation protection techniques such as the distance from the X-
ray source and X-ray beam collimators. Whereas, the recommended distance
between the X-ray machines and control panels have not been achieved in some
rooms.
A second part of this research is a questionnaire, which designed for matching the
study needs and 182 radio-diagnostic workers participated in the work. We
conducted the independent samples t-test, frequency and one-way analysis of
variance (ANOVA). These tests detect the difference between the availability of
personal radiation protection devices, awareness and practices level regarding
radiation protection issues and evaluation of personal radiation exposure monitoring
process as a dependent variables. However, the socio-demographic and work related
factors among radio-diagnostic workers are independent variables.
According to the results displayed in chapter four, the participants reported that
35.2% of personal radiation protection devices are available in the radio-diagnostic
centers at governmental Gaza governorates hospitals.
The results indicate unsatisfactory practices toward radiation protection issues, where
approximately half of participants have negative practices. In general, the results
revealed that there is an obvious poor of personal radiation exposure monitoring
process. There is also a statistically significant difference in the participants
awareness level due to their years of practical experience and occupation.
Overall, the results represented in this work reflect that majority of
participants believe there is no radiation safety officer to provide the service.
Therefore, there is a desperate need for rules, regulations and radiation
protection act in the field of radiation in medical field.

103
5.2 Recommendations
The outcome of the results in this research, the following recommendations
should be taken into account to improve the radiation protection measures
and reduce the radiation doses for the radio-diagnostic workers and public:
The basic radiation protection principles of Justification and Optimization
should be taken into consideration, in this period of rapid increase of
radio-diagnostic procedures following the availability of new machines.
The stakeholders should provide the radiation protection devices in all
radio-diagnostic centers in Gaza governorates hospitals.
Re-shielding the locations where the annual equivalent radiation dose
exceed of the permissible limits should be taken into consideration.
There is a dare need for rules, regulation and radiation protection act in
the field of radiation in medical field.
Conducting continuous training programs that may help in improving the
awareness of workers about radiation protection issues.
The hospitals should provide a radiation protection advisers for a routine
daily monitor the radiation protection measures, practices and inspection
of radiation dose rate levels in Gaza governmental hospitals.
Establishing radiation protection department in the country in order to
ensure the regular monitoring of radio-diagnostic workers doses.
Designing the radio-diagnostic centers according to the internationally
safety criteria.

104
5.3 Suggestions for future studies
The present study suggests to conduct further researches in West Bank
governorates hospitals, UNRWA and private radiology centers to measure
radiation leakage and evaluating the radiation protection measures.

105
References
Abu Draz S., 2009 - Knowledge, attitudes and practices regarding radiation
protection among radio-technologists in governmental hospitals in Gaza
governorates. MPH thesis, Al-Quds university.
Adejumo B.; Irurhe K.; Olowoyey A.; Ibitoye Z.; Eze U.; and Omiyi D., 2012 -
Evaluation of compliance to radiation safety standard amongst radiographers in
radio-diagnostic centers in South West, Nigeria. World Journal of Medical Sciences.
Vol: 7, No: 3, P: 194-196.
Adhikari K.; Jha L.; and Galan M., 2012 - Status of radiation protection at different
hospitals in Nepal. Journal of Medical Physics, Association of Medical Physicists of
India. Vol: 37, No: 4, P: 240-4.
Ali R., 2013 - Environmental survey and quality control tests of X-ray diagnostic
facility of hospitals in Iraqi Kurdistan region. International Journal of Enhanced
Research in Science Technology & Engineering. Vol: 2, No: 11, P: 64-70.
Amirzadeh.; and Tabatabaie S., 2005 - Survey of radiation protection awareness
among radiation workers in Shiraz hospitals. Iranian Journal of Nuclear Medicine.
Vo: 13, No: 2, P: 38-43.
Badran I., 1995 - Knowledge, attitude and practices the three pillars of excellence
and wisdom: a place in the medical profession. Eastern Mediterranean Health
Journal. Vol: 1, No:1, P: 7.
Balter S.; and Moses J., 2007 - Managing patient dose in interventional cardiology.
Catheterization and Cardiovascular Interventions. Vol: 70, No:2, P: 244-249.

106
Balter S.; Hopewell J.; Miller D.; Wagner L.; and Zelefsky M., 2010 -
Fluoroscopically guided interventional procedures. A review of radiation effects on
patients' skin and hair. Radiology Journal. Vol: 254, No:2, P: 326–341.
Biller N., 2014 - Abolishing Mammography Screening Programs? A View from the
Swiss Medical Board. The New England Journal of Medicine. Vol: 370, P: 1965–
1967.
Brant E.; and Helms A., 2012 - Fundamentals of diagnostic radiology. Lippincott
Williams & Wilkins. Vol: 4, P: 1 .
Brenner D., 2010 - Should we be concerned about the rapid increase in CT usage?.
Reviews on environmental health. Vol: 25, No: 1, P: 63-68.
Brenner J.; and Hricak, H., 2010 - Radiation exposure from medical imaging: time
to regulate?. Jama. Vol: 304, No: 2, P: 208-209.
Burnham J., 2001 - Radiation protection, NB Power Corporation. Point Lepreau,
New Brunswick Power Corporation. Fourth edition.
Bushberg J.; Seibert A.; Leidholdt J.; Edwin M.; and Boone M., 2001 - The essential
physics of medical imaging. Lippincott Williams & Wilkins. 2nd
edition.
Caon M.; Bibbo G.; and Pattison J., 2000 - Monte Carlo calculated effective dose to
teenage girls from computed tomography examinations. Radiation Protection
Dosimetry. Vol: 90, No: 4, P: 445–448.
Christodoulou G.; Goodsitt M.; Larson C.; Darner L.; Satti J.; and Chan P., 2003 -
Evaluation of the transmitted exposure through lead equivalent aprons used in a
radiology department, including the contribution from backscatter. Medical Physics.
Vol: 30, P: 1033–1038.

107
Complex Systems Approaches to Population Health (CSAPH)., 2006 - Ionizing
radiation exposure in the medical setting. Scientific report no. 2. American medical
association.
Detorie N.; Mahesh M.; and Schueler A., 2007 - Reducing occupational exposure
from fluoroscopy. J Am Coll Radiol. Vol: 4, P: 335–337.
Directive Council., 1996 - laying down basic safety standards for the protection of
the health of workers and the general public against the dangers arising from
ionizing radiation. Official Journal. P: 1-114.
Environmental Protection Agency (EPA)., 2007 - Ionizing Radiation (Fact Book).
United States. (http://www.epa.gov/repweb00/doc/402-f-06-061.pdf.).
Environmental Protection Agency (EPA)., 2009 - Radiation and Health..
(http://www.epa.gov/radiation/understand/health_effects.html).
Food and Drug Administration (FDA) ., 2007 - What Are the Radiation Risks From
CT? United States. (http://www.fda.gov/cdrh/ct/risks.html).
Feng J.; Chen R.; Sun P.; Duan Y.; Jia S.; and Zhang L., 2002 - Estimated cosmic
radiation doses for flight personal. Space Med Eng. Vo: 15, No: 4, P: 265–269.
European Commission., 2000 - Radiation Protection 116: Guidelines on education
and training in radiation protection for medical exposures.
Giri K.; Dhiraj G.; and Krishna M., 2007 - Radiation measurement at X-ray centers
of a few hospitals in Kathmandu city, Nepal. Kathmandu University Journal of
Science, Engineering and Technology. Vol: 3, No: 2, P: 31-34.
Golding S.; and Shrimpton P., 2002 - Radiation Dose in CT: Are We Meeting the
Challenge?. The British Journal Radiology. P: 75: 1-4.

108
Gonzalez d.; Berrington A.; and Darby S., 2004 - Risk of cancer from diagnostic X-
rays: estimates for the UK and 14 other countries. The lancet. Vol: 363. No: 9406, P:
345-351.
Hall J.; and Brenner D., 2008 - Cancer risks from diagnostic radiology. The British
Journal of Radiology. Vol: 81, P: 362–378.
Hall J.; and Giaccia A., 2006 - Clinical response of normal tissues. Radiobiology for
the Radiologist. Vol: 6, P: 333-337.
Hart D.; and Wall B., 2002 - Radiation exposure of the UK population from medical
and dental X-ray examinations. Report.W4. National Radiation Protection Board.
Chiton.
Herman T.; and Gabor T., 2009 - Fundamentals of Computerized Tomography:
Image Reconstruction from Projections (2nd ed.). Springer.
Human Rights Council (HRC)., 2013 - Annual report. Ramallah, Palestine.
International agency for research on cancer (IARC)., 2000 - Monographs on the
evaluation of carcinogenic risk to humans. Ionizing Radiation, Part 1: X and gamma
radiation, and neutrons. Lyons, France. Vol: 750.
International agency for research on cancer (IARC)., 2013 - Latest world cancer
statistics - GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and
Prevalence Worldwide in 2012.
International Atomic Energy Agency (IAEA)., 2004 - Radiation, people and
environment.. Australia.
International Atomic Energy Agency (IAEA)., 2007 - Dosimetry in diagnostic
radiology.. An International Code of Practice IAEA Vienna. P:113-125.

109
Ibitoye Z.; Aweda M.; and Irurhe N., 2011 - Annual effective dose status among the
radiation staff of Lagos university teaching hospital, Lagos, Nigeria. African
Journal. Basic and Appl. Vol: 3, P: 126-130.
International Commission on Radiological Protection (ICRP)., 1991 -
recommendations of the international commission on radiological protection.
Publication No.60.
International Commission on Radiological Protection (ICRP)., 2006 – Draft
recommendations of the international commission on radiological protection.
Sweden.
International Commission on Radiological Protection (ICRP)., 2007 – Draft
recommendations of the international commission on radiological protection.
Sweden.
Iortile T.; Archibong B.; and Chelen J., 2013 - Assessment of the levels of radiation
absorbed by radiology personnel in some hospitals in Makurdi Metropolis. Journal
of hospital management. Vol: 13, P: 32-5.
Jean, M.C., 1998 - Community legislation on medical radiation protection in the
context of internal market. Radiation Protection Division, DG XI, Commission of the
European Communities, Luxembourg.
Klein W.; Miller L.; Balter S.; Laskey W.; Haines D.; Norbash A.; and Goldstein J.,
2009 - Occupational health hazards in the interventional laboratory: time for a safer
environment. Catheterization and Cardiovascular Interventions Journal. Vol: 73, No:
3, P: 432-438.

110
Lawrence S.; Haken K.; and Giaccia A., 2008 - Principles of radiation oncology. In:
Vita T. ; Lawrence S., Rosenberg A., editors. Cancer: Principles and Practice of
Oncology. 8th
edition. Philadelphia: Lippincott Williams and Wilkins.
Mehta S., 2005 - Health risks of low level radiation exposures: a review. Indian
Journal of Nuclear Medicine. Vol: 20, No: 2, P: 29-41.
Morgan F., 2003 - Non-targeted and delayed effects of exposure to ionizing
radiation: II. Radiation-induced genomic instability and bystander effects in vivo,
clastogenic factors and transgenerational effects. Radiation research. Vol: 159, No:
5, P: 581-596.
Ministry Of Health (MOH)., 2006 - Health status in Palestine. Annual report,
Palestinian National Authority: Palestinian health information center.
Ministry Of Health (MOH)., 2011 - Cancer in Palestine. Annual report. Palestinian
National Authority: Palestinian health information center.
Mojiri M.; and Moghimbeigi A., 2008 - Awareness and attitude of radiographers
towards radiation protection. Journal of Paramedical Sciences. Vol: 2, No: 4, P: 497.
Muller J., 1927 - Artificial transmutation of the gene. Science. Vol: 46, P: 84-87.
Muller S.; and Richard T., 2010 - Physics for Future Presidents, Princeton
University Press.
Mutyabule K.; and Whaites J., 2002 - Survey of radiography and radiation
protection in general dental practice in Uganda. Dentomaxillofacial Radiology. Vol:
31, No: 3, P: 164-169.

111
National Research Council (NRC)., 2006 - Health risks from exposure to low levels
of ionizing radiation: BEIR VII- Phase 2. National Academy of Sciences.
Committee to assess health risks from exposure to low levels of ionizing radiation,
National council on Radiation Protection and Measurements (NCRP)., 1976 -
Structural shielding designs and evaluation for medical use of X-ray and gamma rays
of energies up to 10MeV. Report No.49.
National council on Radiation Protection and Measurements (NCRP)., 1989 - Report
on carcinogens.12th
edition.
National council on Radiation Protection and Measurements (NCRP)., 2009 -
Ionizing radiation exposure of the population of the united states. Bethesda, MD.
Report No. 160.
National Occupational Health and Safety Commission (NOHSC)., 2002 - Code of
practice for the safe removal of asbestos. 2nd
edition.
Noohi J., 2009 - Evaluation of personal protection among radiographers in
diagnostics radiology centers in Kerman (Iran). Environmental Health Conference
Iran.
Occupational Safety and Health Council (OSHC)., 2006 - The ocular radiation
hazard for health care practitioners involving radiation exposure and the solutions
for reducing this hazard.
Oikarinen H.; Meriläinen S.; Paakko E.; Karttunen A.; Nieminen T.; and Tervonen
O., 2009 - Unjustified CT examinations in young patients. European radiology. Vol:
19, No: 5, P: 1161-1165.

112
Okaro O.; Ohagwu C.; and Njoku J., 2010 - Evaluation of personal radiation
monitoring in radio-diagnostic centers in South Eastern Nigeria. African Journal of
Basic and Applied Sciences. Vol: 2, P: 49-53.
Okpala, C., 2004 - Survey of radiation protection facilities in some parts of Nigeria
(Enugu and Anambra States). Journal of Biomedical Investigation. Vol: 2, No:1, P:
17-21.
Olowookere J.; Obed I.; Adefisoye A.; and Vincent U.E., 2009 - Medical Physicist:
Missing component of Nigerian Radiological Crew. Journal of Scientific and
Industrial Studies. Vol: 7, No: 1, P: 110-117.
Oluwafisoye A.; Olowookere J.; Obed I.; Efunwole O.; and Akinpelu A., 2009 -
Environmental survey and quality control test of X-ray diagnostic facility of a large
Nigerian hospital. International Journal of Research and Reviews in Applied
Science. Vol: 1, No: 2, P: 157-162.
Palestinian Central Bureau of Statistics (PCBS)., 2009 - Annual report. Ramallah,
Palestine.
Palestinian Central Bureau of Statistics (PCBS)., 2014 - Population and housing and
establishment census rep. Ramallah, Palestine.
Radiation Protection Manual., 2010 - A publication of institute of Nuclear Medicine
and Allied Science (INMAS), DRDO, Delhi, India. Radiological Protection Bulletin.
Vol: 231, P: 18-23.
Rahman N.; Dhakam S.; Shafqut A.; Qadir S.; and Tipoo A., 2008 - Knowledge and
practice of radiation safety among invasive cardiologists. Journal of the Pakistan
Medical Association. Vol: 58, No:3, P: 119.

113
Rosenbloom M., 2007 - Theoretical background to radiation protection, In: Mayles
P.; Nahun A.; and Rosenwald J., (Eds). Handbook of radiotherapy physics: Theory
and practice. Florida, USA: Taylor and Francis Group.
Salti, L.; and Whaites E., (2002). Survey of dental radiographic services in private
dental clinics in Damascus, Syria. Dentomaxillofacial Radiology Journal. Vol: 31,
No: 2, P: 100-105.
Santis M.; Cesari E.; Nobili E.; Straface G.; Cavaliere F.; and Caruso A., (2007).
Radiation effects on development. Birth Defects Research Part C: Embryo Today:
Reviews. Vol: 81, No: 3, P:177-182.
Shah S.; Begum N.; Shahida N.; and Khan A., 2007 - Assessment of radiation
protection awareness levels in medical radiation science technologists.
Postgraduate Medical Institute Journal. Vol: 21, No: 3, P: 169-179.
Shrimpton P., 2001 - The world of medical radiation exposures. Radiological
Protection Bulletin. Vol: 231, P: 18-23.
Slechta M.; and Janet R., 2008 - An examination of factors related to radiation
protection practices. Radiologic technology Journal. Vol: 79, No: 4, P: 297-305.
Stecker S.; Balter S.; Towbin B.; Miller L.; Vano E.; Bartal G.; Angle F.; Chao P.;
Cohen M.; Dixon G.; Gross K.; Hartnell G.; Scheuler B.; Statler D.; Baere T.; and
Cardella F., 2009 - Gidelines for patient radiation management. Journal Vascular
International Radiology. Vol: 20, P: 263–S273.
Street M.; Brady Z.; Van B.; and Thomson R., 2009 - Radiation exposure and the
justification of computed tomography scanning in an Australian hospital emergency
department. Internal medicine journal. Vol: 39, No:11, P: 713-719.

114
Su C.; Huang F.; Chen C.; and Chang S., 2000 - Radiation safety knowledge of
medical center radiological technologists in Taiwan. Radiation Oncology Journal.
Vol: 50, P:1-3.
Tavakoli R.; Seilanian F.; and Saadatjou A., 2003 - Knowledge of medical students
on hazards of ionizing radiation. Journal of Medical Education. Vol: 3, No: 1, P: 3-6.
The University of Western Australia., 2010 - Achieving international excellence.
School of Plant Biology M084. Safety manual.
(http://www.safety.uwa.edu.au/policies/occupational_safety_and_health.html).
Ujah F.; Akaagerger N.; Agba E.; and Iortile J., 2012 - A comparative study of
patients radiation levels in federal standard diagnostic reference levels in federal
medical center and bishop Murray hospitals in Makurdi. Archives of Applied
Science Research. Vol: 4, P: 800-804.
United Nation Environment Program (UNEP)., 2013 - Desk study on the
environment in the occupied Palestinian territories rep. P: 194.
United Nations Scientific Committee on the Effects of Atomic Radiation
(UNSCEAR)., 2000 - Sources and effects of ionizing radiation . United Nations
Scientific Committee on the Effect of Atomic Radiation. United Nation, New York.
United Nations Scientific Committee on the Effects of Atomic Radiation
(UNSCEAR)., 2006 - Sources-to-effects assessment for radon in homes and
workplaces. effects of ionizing radiation. New York: United Nations. Annex E.
United Nations Scientific Committee on the Effects of Atomic Radiation
(UNSCEAR)., 2008 - medical radiation exposures. Annex A.
Wagner K.; and Mulhern R., 1996 - Radiation attenuating surgical gloves: effects of
scatter and secondary electron production. Radiology. Vol: 200, P: 45–48.

115
Washington State University., 2000 - Safety policies and procedures manual on
radiation safety.
Whaites E.; and Roderick C., 2002 - Essentials of dental radiography and radiology.
Elsevier Health Sciences. P: 15–20.
World Health Organization (WHO)., 2009 - What Is Ionizing Radiation?.
(http://www.who.int/ionizing_radiation/about/what_is_ir/en/index.html)
Younis S.; Ali R.; Rashid S., 2014 - Radiation protection evaluation from radio
diagnostic departments in Erbil hospitals. Zanco Journal of Medical Sciences. Vol:
18, No: 1, P: 625-631.
Web sites
http://www.bfs.admin.ch/bfs/portal/de/index.html.
Personal communication
Ibrahim Abbas, deputy director of radiology department in Ministry of Health
(October 2014): Data about numbers and distribution of the radio-diagnostic workers
and radio-diagnostic services in Gaza governmental hospitals.

116
Annexes
Annex (1): Sample size calculator
Sample Size Calculator Terms: Confidence Interval & Confidence Level
The confidence interval (also called margin of error) is the plus-or-minus figure
usually reported in newspaper or television opinion poll results. For example, if you
use a confidence interval of 4 and 47% percent of your sample picks an answer you
can be "sure" that if you had asked the question of the entire relevant population
between 43% (47-4) and 51% (47+4) would have picked that answer.
The confidence level tells you how sure you can be. It is expressed as a percentage
and represents how often the true percentage of the population who would pick an
answer lies within the confidence interval. The 95% confidence level means you can
be 95% certain; the 99% confidence level means you can be 99% certain. Most
researchers use the 95% confidence level.
When you put the confidence level and the confidence interval together, you can say
that you are 95% sure that the true percentage of the population is between 43% and
51%. The wider the confidence interval you are willing to accept, the more certain
you can be that the whole population answers would be within that range.
For example, if you asked a sample of 1000 people in a city which brand of cola they
preferred, and 60% said Brand A, you can be very certain that between 40 and 80%
of all the people in the city actually do prefer that brand, but you cannot be so sure
that between 59 and 61% of the people in the city prefer the brand.
http://www.surveysystem.com/sscalc.htm

117
Annex (2): A permission from the Ministry of Health to perform the study in
the governmental hospitals

118
Annex (3): A consent from all participants to ensure their voluntary
participation
بسم هللا الرحمن الرحيم
السيد/ة المشارك:
تحية طيبة وبعد...
أدرس بكلية العلوم بالجامعةة اسالةيمية بةة ة و طمبطلةب للح ةو سامر سليم عبد أبو زرأنا الطالب
على درجة الماجسبير أقوم بإعداد بحث بعنوان:
تسرب اإلشعاع المؤين وإجراءات الوقاية من اإلشعاع في مراكز األشعة التشخيصية في مستشفيات "
"محافظات غزة الحكومية, فلسطين
"Ionizing radiation Leakage and Radiation Protection Measures in
Radio-Diagnostic Centers in Governmental Hospitals of Gaza
Governorates, Palestine"
إلةى قيةاس مسةبو اإل اسعةعام المةا ت والبعةرء إجةراقاإل الوقا ةة مةت اسعةعام و تهدف هذه الدراسذة
الخروج ببوصياإل تساعد صانعي القرار في تحسيت خططهم المسبقبلية المبعلقة بالوقا ة مت اسععام.
أرجو المشارطة في هذه الدراالة باسجابة على بعض األالئلة خةي المقابلةة البةي لةت تسةبةرر أط ةر مةت
دقيقة تقر با المشارطة طوعية و حق لك االمبنام عت إجابة أي الاا . 15
أرغب أن أنوه أن المعلوماإل البي الوء بم جمعها الةبكون م ةدر ةقةة والةر ة تامةة و الةوء تسةبخدم
فقط بةرض البحث العلمي وبدون ذطر أالماق لذلك أرجوا منك أن تكون اسجاباإل دقيقة.
على أي االبفسار مت طرفك.أنا مسبعد لإلجابة
هل توافق على المشارطة في هذه الدراالة؟
ال نعم
شكرا على حسن تعاونك
الباحث: سامر سليم أبو زر
0599309702جوال:

119
Annex (4): Arabic version of questionnaire
-----رقم البسلسل:
أوال: األسئلة المتعلقة بالبيانات الديموغرافية و أخرى تتعلق بالعمل :
النة 50أط ر مت 49-40 39-30 29-20 العمر:
أن ى ذطر :الجنس
فني ت و ر طبي طبيب أخ ائي أععة المهنة:
دراالاإل عليابكالور وس دبلوم مبوالط المؤهل العلمي:
النة 20أط ر مت 19-15 14-10 9-5 4-1سنوات الخبرة العملية:
مسبشفى غ ة األوروبي مجمع ناصر الطبي مجمع الشفاق الطبي المستشفى الهي تعمل به:
مسبشفى مسبشفى عهداق األق ى مسبشفى الشهيد طما عدوان مسبشفى الشهيد أبو والف النجار
مسبشفى بيت حانون مسبشفى الن ر لألطفا الرنبيسي البخ ي لألطفا الشهيد عبد الع
-األجهزة التي عادة ما تعمل عليها:
-ray
عدد ساعات العمل اليومي داخل غرف األشعة التشخيصية:
الاعاإل 6أط ر مت 5-6 4-5 4 -3 2-3 1-2
ثانيا: األسئلة المتعلقة بتوفر أدوات الوقاية من اإلشعاع في القسم الهي تعمل به:
م أداة الوقاية من اإلشعاع
ال نعم
ال
أعرف
1 Lead Apron
2 Gonad shields
3 Lead curtains
4 Lead shields/barrier
5 Thyroid shields
6 Lead glass
7 Lead gloves
8 Breast shields
9 Radiation warning signs
10 Caution lights

120
ثالثا: األسئلة المتعلقة بقياس مستوى معرفة العاملين حول طرق الوقاية من اإلشعاع:
ال نعم السؤال مال
أعرف
1 الجرعة اسععاعية السنو ة المسموح بها للعامليت في مجا األععة هي
20 mSv/yr
1mSv/yrالجرعة اسععاعية المسموح بها للجمهور هي 2
3 حدود الجرعة اسععاعية للمرأة الحامل العاملة في مجا االععة هي
2mSv خي فبرة الحمل
4 والجمهور مت األععة الةير ضرور ة أةناق الفحوصاإل حما ة المر ض
اسععاعية قع على عاتق العامليت في مجا األععة
5
االبخدام طيلو فولت عالي أةناق إعطاق الجرعة اسععاعية ادي إلى ز ادة
في نفوذ ة الح مة اسععاعية البي تادي إلى تخفيض الجرعة الممب ة في
جسم المر ض
6 قل وقت البعرض لألععة أةناق الفحوصاإل اسععاعية فإن جرعة إذا
المر ض الوء تقل
7 إذا زادإل المسافة مت م در األععة إلى الضعف فإن جرعة المسبلمة الوء
تقل إلى الن ف
مبر 2المسافة الموصى ترطها بيت جهاز األععة والعامليت هي 8
9 أةناق الب و ر اسععاعي له فائدة طبيرة " "Collimationاالبخدام المحدد
في تقليل جرعة األععة للمر ض
واقي الرصاص جب فح ه بشكل دوري لبجنب حدوث أي تشققاإل فيه 10
11 primary x- ray roomالمك الرصاص في جدار غرفة األععة األولي
ALARAملي مبر بناق على مبدأ 2 جب أن كون
12 أبواب مت جهة واحدة أو مت جهبيت بطبقة مت الرصاص المكها جب تبطيت
ملي مبر1
13
3.6مبر مربع وارتفام السقف 36ال تقل عت المساحة الم الية لةرء أععة
مبر فور 2.2مبر وبالنسبة للنوافذ الخارجية جب أن كون ارتفاعها
مسبوى أرضية الةرفة
14 " جب أن Primary radiation barrierالحاج اسععاعي األولي"
مبر 2 كون على ارتفام
جب أن بم عمل صيانة و معا رة دور ة ألجه ة األععة لمنع البسرب 15
16 جب أن بم عمل فحص دوري لجدران و أبواب غرء األععة ووالائل
الوقا ة للبأطد مت طفاقتها
17 أجه ة األععة في عيت االعببار عند عرائها جب أخذ خبرة العامليت على
واعراطهم في مواصفاإل الشراق
الكيلو فولت المناالب الناتج عت خطأ الفني أو وجود عطل الخطأ في اخبيار 18
في جهاز األععة قد ادي إلى جرعة إععاعية زائدة للمر ض

121
حذول الوقايذذة مذذن ةالمتعلقذة بوفذذم ممارسذذات العذاملين فذذي مجذال األشذذعة التشخيصذذي ةرابعذا: األسذذئل
:اإلشعاع
خامسا: مجموعة أسئلة لتقييم عملية مراقبة التعرض الشخصي لإلشعاع المؤين:
. هل يوجد مشرف مختص في الوقاية من اإلشعاع في المستشفى الهي تعمل به؟1
ال نعم
. هل تملك جهاز قياس لمراقبة التعرض لإلشعاع ؟2
ال نعم
(7)اذا طانت االجابة ب )ال( فقط اجب عت الساا رقم
", هل تقوم باستخدامه أُثناء عملك في غرف األشعة؟ة " نعمإذا كانت اإلجاب .3
ال أحيانا نعم
أحيانا ال نعم السؤال م
هل عارطت في دوراإل حو الوقا ة مت اسععام؟ 1
هل تقوم ببوضيح تعليماإل الفحص اسععاعي للمر ض قبل ت و ره؟ 2
3 لبقليل collimationأةناق قيامك بالب و ر اسععاعي هل تقوم باالبخدام
الطح المر ض المعرض لإلععام؟
هل تقف خلف الحاج المرصص عند ت و رك للمر ض؟ 4
5 هل تقوم باالبخدام Gonadesفي حالة عدم احبواق طلب الطبيب ت و ر
Gonadal shield لحما ة هذه األعضاق؟
6 هل تقوم بإفراغ غرفة األععة مت مرافقي المر ض قبل اعطاق الجرعة
االععاعية؟
هل تبأطد مت إغير باب غرفة األععة جيدا أةناق الب و ر؟ 7
8 أةناق عملك باالبخدام جهاز أععة مبنقل هل تقوم بالحفاظ على المسافة
المطلوبة بينك وبيت م در األععة؟
9 باالبخدام جهاز أععة مبنقل هل تقوم بأخذ االحبياطاإل اليزمة أةناق عملك
لحما ة مرافقي المر ض والمرضى اآلخر ت داخل الةرفة؟
10 هل تقوم بارتداق و االبخدام أدواإل الوقا ة مت اسععام لحما ة نفسك مت
االععام؟
الب و ر؟هل تقوم بحما ة مرافق المر ض الذي قوم بب بيت الطفل أةناق 11
12 هل البق و أن طلبت فحص للموقع الذي تعمل به عند االعبباه بوجود تسر ب
لألععة؟
13 هل تهبم بإجراق ال يانة للجهاز في حا وجود خلل بعلق بالوقا ة مت
اسععام؟
14 هل تسبجيب اسدارة لمطالب العامليت سجراق فحوصاإل للبأطد مت اليمة
غرء األععة؟
15 هل تعبقد أن قسم األععة الذي تعمل به مطابق لمعا ير السيمة والوقا ة مت
اسععام؟

122
. هل تلقيت إرشادات من قبل مسئول الوقاية من اإلشعاع حول كيفية استخدام وحفظ جهاز قياس اإلشعاع؟ 4
ال نعم
. هل يتم أخه قياسات أجهزة مراقبة التعرض الشخصي لإلشعاع بعين االعتبار من قبل الجهات المختصة؟ 5
ال نعم
؟اإلشعاعية أخر عند تسليمك للجهاز القديم لقياس الجرعة جهاز قياس تسليمك. هل يتم 6
ال نعم
", إلى ما تعزو هها اإلهمال ؟إذا كانت اإلجابة "ال .7
غير مهبمة اسدارة عت الوقا ة مت اسععام مسئولةعدم وجود جهة
العامليت في مجا األععة ال طلبون هذه األجه ة لبوفير هذه األجه ة ةالمي انيعدم توفر

123
Annex (5): English version of questionnaire
Serial number:………..
Part one: The following questions about socio-demographic and related work
information:
Age: - - -
Sex:
Occupation: Medical radiographer
Academic qualification: ploma Bachelor higher degrees
Years of practical experience - - - -
15 years
Name of hospital
a Martyrs hospital
Types of your radio-diagnostic machines: Basic X-
-ray
Daily work hours in radio-diagnostic rooms:
- - - -

124
Part two: The availability of radiation protection devices in radio-diagnostic
center:
No idea
NO
Yes
Radiation protection devices No.
Lead Apron 1
Gonad shields 2
Lead curtains 3
Lead shields/barrier 4
Thyroid shields 5
Lead glass 6
Lead gloves 7
Breast shields 8
Radiation warning signs 9
Caution lights 10
Part three: Measure of the radio-diagnostic workers awareness level regarding
radiation protection issues:
No
idea No Yes Question No.
The annual average dose over five years should not
exceed 20 mSv for occupational exposure 1
Public should not be exposed to more than an average of
1 mSv per year 2
Radiation dose limits for pregnant woman who work in
radiation field is 2 mSv during pregnancy period 3
Protection of patient and public from unnecessary
radiation during radiological examinations are the
responsibility of radiology staff
4
Utilizing high kV during radiological examinations leads
to an increase the permeability of the radiation beam and
reduce the absorbed dose in the patient body
5
Short radiation exposure time during radiological
examinations, leads to less patient radiation dose 6
Increasing the distance from the radiation source to
double, leads to reduce the received dose to half 7
The recommended distance between X-ray source and
radiology workers is two meter 8
Using the collimators during medical radiography has a
great benefits and reduce the patient dose 9
Protective lead must periodically examined to avoid any
cracks in the lead 10
Thickness of the lead lined the X-ray room wall, which is
exposed to primary X-rays should be 2 mm based on the
principle of ALARA
11
The doors of X-ray room must be lined from one or two
sides with a lead layer thickness of 1 mm 12

125
The ideal X-ray room space should not be less than 36 m2,
the ceiling height is 3.6 m and the exterior windows
height is 2.2 m above the X-ray room floor
13
The primary radiation barrier must be height 2m from the
X-ray room floor 14
The X-ray machines maintenance and calibration must be
periodically carried out to prevent radiation leakage 15
The periodic maintenance for X-ray rooms walls, doors
and radiation protection tools should be performed to
ensure their efficiency
16
The experience of workers must be taken into
consideration when X-ray machines were imported and
involved them in the specification of the purchase
17
The error in the selection of appropriate kilo volts due to
technical error or malfunction of X-ray machine leads to
excessive radiation dose to the patient
18
Part four: Description of radio-diagnostic workers practices about radiation
protection issues:
Som-
etimes NO Yes Question No.
Have you ever received any training in radiation
protection? 1
Do you explain the radiological examination instructions
to the patient before the exam? 2
Do you use X-ray tube collimation during the
radiography in order to reduce patient body dose?
3
Do you stand behind the lead barrier during giving the
radiation dose? 4
If the doctor doesn't ask for imaging the Gonads, do you
use the gonadal shield to protect these organs? 5
Do you ask the patient escorts to evacuate the X-ray
room before giving the X-ray dose?
6
Do you make sure that the X-ray door is closed during
the radiological examination?
7
Do you keep the requierd distance between the X-ray
source and yourself during using a mobile X-ray
machine?
8
Do you take the necessary precautions to protect patient
escorts and other patients in the room during using a
mobile X-ray machine?
9
Do you wear the radiation protection devices to protect
yourself from ionizing radiation? 10
Do you protect the patient escort, who hold the child
during the radiological examination? 11
Have you been asked to check your radiology center
when there is suspicion of radiation leakage? 12
Are you interested in maintenance conducting for X-ray
machines when the defect related with radiation 13

126
protection?
Does the administration respond to workers' demands
regarding to check the X-ray rooms to make sure about
of their safety?
14
Do you think that your radiology center conformity with
the safety and radiation protection standards? 15
Part five: Evaluating the personal radiation exposure monitoring process:
1. Does the hospital have Radiation Protection Adviser (RPA) or departmental
Radiation Protection Supervisor (RPS)?
2. Does the hospital provide you with any personal radiation monitoring
device?
(If no, only answer question no. 7)
3. If yes, do you use it during your work in the radio-diagnostic rooms?
4. Did you receive a guidance about the proper handling with the personal radiation monitoring device?
5. Are the measurements results taken into consideration by the safety officers?
6. Do you receive another personal radiation monitoring device when the device
collect to measure of radiation dose?
7. If no, what is the reason for non-provision of the device?
carelessly of hospital
management
not request for it

127
Annex (6): Certificate of radiation survey meter (OD-01) calibration

128
Annex (7): The equivalent radiation dose rate measurements
Eq
uiv
alen
t
rad
iati
on
do
se H
W
mS
v/y
ear
Eq
uiv
alen
t
rad
iati
on
do
se H
W m
Sv
/wee
k
Wo
rklo
ad
in t
he
roo
m
mA
.min
/w
-eek
Rad
iati
on
do
se r
ate
mS
v/m
in R
adia
tio
n
do
se r
ate
mS
v/h
r L
oca
tio
ns
of
rad
iati
on
do
se r
ate
mea
sure
m
ents
Nam
e o
f
mac
hin
e
and
roo
m
nu
mb
er N
ame
of
ho
spit
al
0.04 Electrical zero
balancing value
Flu
oro
sco
py
roo
m n
o.1
Al
Sh
ifa
Med
ical
Co
mp
lex
2296.9 47.85144
840
0.28483 17.09 Directional
45.7 0.952056 0.00567 0.34
At 1 meter distance from the tube by
closing the collimators
10.7 0.223944 0.00133 0.08 At control panel
8.1 0.168 0.001 0.06 At corridor (door
closed)
9.4 0. 196056 0.00117 0.07 At Patient waiting
room
0.03 Electrical zero
balancing value
Flu
oro
sco
py
roo
m n
o. 2
2109.7 43.953
735
0.299 17.94 Directional
41.2 0.857451 0.00583 0.35
At 1 meter distance from the tube by
closing the collimators
8.2 0.171402 0.00117 0.07 At control panel
7.1 0.147 0.001 0.06 At corridor (door
closed)
9.4 0.195951 0.00133 0.08 At Patient waiting
room
0.03 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o. 6
107.5 2.24
1750
0.32 19.20 Directional
2.5 0.0525 0.0075 0.45
At 1 meter distance from the tube by
closing the collimators
1.8 0.03731 0.00533 0.32 At control panel
1.7 0.036169 0.00517
0.31
At corridor (door closed)
1.2 0.025669 0.00367 0.22 At Patient waiting
room
1.3 0.02681 0.00383 0.23 Behind the chest
stand wall
0.04 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o. 7
79.1 1.6485
1750
0.2355 14.13 Directional
1.7 0.036169 0.00517 0.31
At 1 meter distance from the tube by
closing the collimators
1.95 0.04081 0.00583 0.35 At control panel
1.1 0.02331 0.00333 0.20 At corridor (door
closed)
1.1 0.02331 0.00333 0.20 At Patient waiting
room
0.9 0.018669 0.00267 0.16 Behind the chest
stand wall

129
0.02 Electrical zero
balancing value
Bas
ic X
-ray
emer
gen
cy r
oo
m
98.8 2.058
2100
0.245 14.7 Directional
2.02 0.042 0.005 0.30
At 1 meter distance from the tube by
closing the collimators
3.8 0.0798 0.0095 0.57 At control panel
1.8 0.0378 0.0045 0.27 At corridor (closed
door)
2.02 0.042 0.005 0.30 At dark room
1.9 0.040572 0.00483 0.29 Behind the chest
stand wall
0.04 Electrical zero
balancing value
CT
sca
n
CT
sca
n r
oo
m
1338.1 27.8775
33075
0.236 14.16 Directional
752.97 15.687 0.1328 7.97
At 1 meter distance from the C.T scan
gantry
14.2 0.2953125 0.0025 0.15 At control panel
13.2 0.2755856 0.00233 0.14 At door of the control
panel (door closed)
12.3 0.2559769 0.00217 0.13 At corridor (closed
door)
13.2 0.2755856 0.00233 0.14 At patients waiting
room
0.04 Electrical zero
balancing value
Bas
ic X
-ray
ou
t cl
inic
roo
m n
o. 1
105.3 2.19408
2100
0.2612 15.67 Directional
4.2 0.0882 0.0105 0.63
At 1 meter distance from the tube by
closing the collimators
1.4 0.0294 0.0035 0.21 At control panel
1.9 0.039228 0.00467 0.28 At corridor (door
closed)
1.2 0.0252 0.003 0.18 At dark room
1.6 0.0336 0.004 0.24 Behind the chest
stand wall
0.04 Electrical zero
balancing value
Bas
ic X
-ray
ou
t cl
inic
roo
m n
o. 2
103.7 2.16048
2100
0.2572 15.43 Directional
2.4 0.0489997 0.00583
3 0.35
At 1 meter distance from the tube by
closing the collimators
2.2 0.0462 0.0055 0.33 At control panel
2.02 0.042 0.005 0.30 At corridor (door
closed)
1.8 0.0378 0.0045 0.27 At dark room
2.1 0.043428 0.00517 0.31 Behind the chest
stand wall
0.02 Electrical zero
balancing value
Po
rt-a
ble
X-r
ay
roo
m 1
Nas
ser
Med
ical
Co
mp
lex
30.7 0.6400125
262.5
0.17067 10.24 Directional
6.7 0.140602 0.0857 5.14
At 1 meter distance from the tube by
closing the

130
collimators
0.4 0.0087375 0.00233 0.14 At control panel
0.09 0.001875 0.0005 0.03 At corridor (door
closed)
0.06 0.0012375 0.00033 0.02 At dark room
0.09 0.001875 0.0005 0.03 Behind the chest
stand wall
0.02 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o. 2
107.3 2.2344
2450
0.228 13.68 Directional
1.1 0.022834 0.00233 0.14
At 1 meter distance from the tube by
closing the collimators
1.4 0.0294 0.003 0.18 At control panel
0.9
0.0196 0.002 0.12
At corridor (door closed)
0.16 0.003234 0.00033 0.02 At dark room
0.2 0.0049 0.0005 0.03 Behind the chest
stand wall
0.03 Electrical zero
balancing value
Mam
mo
gra
phy
roo
m n
o. 3
29.1 0.606309
87.5
0.27717 16.63 Directional
0.5 0.0105656 0.00483 0.29
At 1 meter distance from the tube by
closing the collimators
0.2 0.0040031 0.00183 0.11 At control panel
0.05 0.0010938 0.0005
0.03
At corridor (door closed)
0.03 0.0007219 0.00033 0.02 At dark room
0.02 Electrical zero
balancing value
Flu
oro
sco
py
roo
m n
o. 4
899.1 18.732
420
0.223 13.38 Directional
16.1 0.336 0.004 0.24
At 1 meter distance from the tube by
closing the collimators
10.9 0.2268 0.0027 0.12 At control panel
5.4 0.11172 0.00133 0.08 At corridor (door
closed)
6.05 0.126 0.0015 0.09 At Patient waiting
room
0.02 Electrical zero
balancing value
CT
sca
n ro
om
no
. 5
606.1 12.62625
14700
0.2405 14.43 Directional
262.5 5.468925 0.10417
6.25
At 1 meter distance from the C.T scan
gantry
5.9 0.1224825 0.00233 0.14 At control panel
6.3 0.13125 0.0025 0.15 At door of the control
panel (No door)
1.7 0.0350175 0.00067 0.04 At corridor (door
closed)
0.8 0.0174825 0.00033 0.02 At patients waiting
room

131
0.03
Electrical zero balancing value
Bas
ic X
-ray
ou
t cl
inic
ro
om
128.7 2.68177
2275
0.2947 17.68 Directional
1.2 0.025753 0.00283 0.17
At 1 meter distance from the tube by
closing the collimators
0.4 0.007553 0.00083 0.05 At control panel
0.4 0.007553 0.00083 0.05 At corridor (door
closed)
0.2 0.00455 0.0005 0.03 At dark room
0.2 0.00455 0.0005 0.03 Behind the chest
stand wall
0.02 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o. 2
Eu
rop
ean
Gaz
a h
osp
ital
46.6 0.9702
1050
0.231 13.86 Directional
0.3 0.0063 0.0015 0.09
At 1 meter distance
from the tube by
closing the
collimators
0.1 0.0021 0.0005 0.03 At control panel
0.1 0.0021 0.0005 0.03 At corridor (door
closed)
0.2 0.004914 0.00117 0.07 At dark room
0.1 0.0021 0.0005 0.03 Behind the chest
stand wall
.02 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o. 4
150.4 3.134334
2450
0.31983 19.19 Directional
2.7 0.057134 0.00583 0.35
At 1 meter distance
from the tube by
closing the
collimators
2.2 0.045766 0.00467 0.28 At control panel
0.16 0.003234 0.00033 0.02 At corridor (door
closed)
0.2 0.0049 0.0005 0.03 Dark room
0.2 0.0049 0.0005 0.03 Behind the chest
stand wall
0.01 Electrical zero
balancing value
ES
WE
L
Flu
oro
sco
py
ro
om
1290.2 26.88
525
0.256 15.36 Directional
148.7 3.0975 0.0295 1.77
At 1 meter distance
from the tube by
closing the
collimators
3.4 0.07035 0.00067 0.04 At control panel
2.5 0.0525 0.0005 0.03 At corridor (door
closed)
2.5 0.0525 0.0005 0.03 At patient waiting
room
3.4 0.07035 0.00067 0.04 At door of the control
panel(door closed)
0.02 Electrical zero
balancing value
Bas
ic X
-
ray
roo
m n
o. 2
Ab
u Y
ou
sef
Al
Naj
jar
Mar
tyr
ho
spit
al
83.6 1.74181
1750
0.24883 14.93 Directional
0.6 0.011669 0.00167 0.1 At 1 meter distance
from the tube by

132
closing the
collimators
0.3 0.005831 0.00083 0.05 At control panel
0.6 0.011669 0.00167 0.1 At corridor
(door closed)
0.1 0.00231 0.00033 0.02 At dark room
0.2 0.0035 0.0005 0.03 Behind the chest
stand wall
0.02 Electrical zero
balancing value
Flu
oro
sco
py
roo
m n
o. 2
1338.1 27.8775
525
0.2655 15.93 Directional
17.6 0.3675 0.0035 0.21
At 1 meter distance
from the tube by
closing the
collimators
5.04 0.105 0.001 0.06 At control panel
6.7 0.139965 0.00133 0.08 At corridor (door
closed)
2.5 0.0525 0.0005 0.03 At dark room
.04 Electrical zero
balancing value
Bas
ic X
-ray
emer
gen
cy r
oo
m
52.1 1.08486
1050
0.2583 15.15 Directional
0.7 0.013986 0.00333 0.2
At 1 meter distance
from the tube by
closing the
collimators
2.02 0.042 0.01 0.6 At control panel
0.3 0.007056 0.00168 0.1 At corridor (door
closed)
0.2 0.003486 0.00083 0.05 At dark room
0.2 0.0042 0.001 0.06 Behind the chest
stand wall
0.04
Electrical zero balancing value
Bas
ic X
-ray
emer
gen
cy r
oo
m
Kam
al A
dw
an M
arty
r ho
spit
al
154.9 3.227742
3150
0.25617 15.37 Directional
1.5 0.0315 0.0025 0.15
At 1 meter distance from the tube by
closing the collimators
4.03 0.084042 0.00667 0.4 At control panel
0.8 0.016758 0.00133 0.08 At corridor (door
closed)
0.7 0.0147042 0.00117 0.07 At dark room
0.03 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o. 2
162.9 3.393558
3150
0.26933 16.16 Directional
4.4 0.092358 0.00733 0.44
At 1 meter distance from the tube by
closing the collimators
2.3 0.048258 0.00383 0.23 At control panel
2.4 0.0504 0.004 0.24 At corridor (door
closed)
0.9 0.0189 0.0015 0.09 At dark room
0.04 Electrical zero
balancing value
Flu
oro
sc-
op
y
roo
m n
o. 3
1572.5 32.76
525
0.312 18.72 Directional
12.6 0.2625 0.0025 0.15 At 1 meter distance
from the tube by

133
closing the collimators
7.6 0.1575 0.0015 0.09 At control panel
6.7 0.13965 0.00133 0.08 At corridor (door
closed)
8.4 0.17535 0.00167 0.07 At dark room
0.04 Electrical zero
balancing value B
asic
X-r
ay
roo
m n
o. 3
55.6 1.157814
1050
0.27567 16.54 Directional
0.8 0.0168 0.004 0.24
At 1 meter distance from the tube by
closing the collimators
0.9 0.018186 0.00433 0.26 At control panel
0.5 0.0105 0.0025 0.15 At corridor (door
closed)
0.4 0.0091014 0.00217 0.13 At dark room
0.5 0.0105 0.0025 0.15 Behind the chest
stand wall
0.01 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o. 1
Al
Aq
sa M
arty
rs h
osp
ital
106.5 2.219742
3150
0.17617 10.57 Directional
3.2 0.067158 0.00533 0.32
At 1 meter distance from the tube by
closing the collimators
2.01 0.041958 0.00333 0.2 At control panel
0.2 0.0041958 0.00033 0.02 At corridor (door
closed)
0.2 0.0041958 0.00033 0.02 At dark room
0.5 0.0104958 0.00083 0.05 At radio-diagnostic
workers room
0.01 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o.2
58.8 1.2243
1050
0.2915 17.49 Directional
0.4 0.0084 0.002 0.12
At 1 meter distance from the tube by
closing the collimators
0.2 0.004914 0.00117 0.07 At control panel
0.5 0.009786 0.00233 0.14 At corridor (door
closed)
1.4 0.02814 0.0067 0.16 At dark room
0.1 0.0021 0.0005 0.03 Behind the chest
stand wall
0.01 Electrical zero
balancing value
Flu
oro
sco
py
roo
m n
o. 2
1367.5 28.48965
525
0.27133 16.28 Directional
18.5 0.385035 0.00367 0.19
At 1 meter distance from the tube by
closing the collimators
7.6 0.1575 0.0015 0.09 At control panel
10.1 0.21 0.002 0.12 At corridor (door
closed)
6.7 0.139965 0.00133 0.08 At dark room

134
0.03 Electrical zero
balancing value
Flu
oro
sco
py
roo
m n
o. 1
Ab
del
Azi
z R
ante
ssi
Mar
tyr
Ped
iatr
ic h
osp
ital
987.8 20.58
420
0.245 14.7 Directional
17.5 0.36372 0.00433 0.26
At 1 meter distance from the tube by
closing the collimators
4.7 0.0980028 0.00117 0.07 At control panel
4.03 0.084 0.001 0.06 At corridor (door
closed)
3.4 0.069972 0.00083 0.05 At dark room
0.04 Electrical zero
balancing value
CT
sca
n ro
om
no
. 2
983.8 20.49666
18375
0.31233 18.74 Directional
483.5 10.073438 0.1535 9.21
At 1 meter distance from the C.T scan
gantry
6.3 0.13125 0.002 0.12 At control panel
3.7 0.0767813 0.00117 0.07 At door of the control
panel (door closed)
4.2 0.0872813 0.00133 0.08 At patients waiting
room
0.04 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o. 1
Al
Nas
er P
edia
tric
ho
spit
al
64.4 1.3412028
2100
0.15967 9.04 Directional
2.6 0.0546 0.0065 0.39
At 1 meter distance from the tube by
closing the collimators
1.9 0.0392028 0.00467 0.28 At control panel
1.01 0.021 0.0025 0.15 At corridor (door
closed)
0.3 0.0069972 0.00083 0.05 At dark room
0.5 0.0098028 0.00117 0.07 Behind the chest
stand wall
0.05 Electrical zero
balancing value
Bas
ic X
-ray
roo
m n
o. 1
Bei
t H
ano
un
ho
spit
al
67.8 1.41288
1400
0.2523 15.14 Directional
0.9 0.018648 0.00333 0.2
At 1 meter distance from the tube by
closing the collimators
1.3 0.028 0.005 0.3 At control panel
0.3 0.0056 0.001 0.06 At corridor (door
closed)
0.2 0.004648 0.00083 0.05 At dark room
0.3 0.0056 0.001 0.06 Behind the chest
stand wall

135
Annex (8): Radio-diagnostic machines and rooms specifications data sheet
No
. o
f ra
dio
log
ica
l
pro
ced
ure
s p
er d
ay
Th
ick
nes
s o
f le
ad
lin
ing
th
e
roo
m d
oo
rs
Dis
tan
ce b
etw
een
th
e X
-ra
y
tub
e a
nd
co
ntr
ol
pa
nel
Th
ick
nes
s a
nd
hei
gh
t o
f le
ad
lin
ing
o
f ro
om
wa
lls
Width of room
walls/cm
Dim
ensi
on
s o
f ra
dio
log
y
roo
m/c
m
Type of machine
working (constant or
portable)
Da
te o
f in
sta
lla
tio
n
Sta
tus
Mo
del
No
. M
an
ufa
ctu
rer
com
pa
ny
Na
me
of
ma
chin
e a
nd
ro
om
nu
mb
er
Na
me
of
ho
spit
al
Material of room
walls (electronic or manual)
Material of control
panel wall
(Film processing
digital or analogue)
------- 2 mm 150
cm
2 mm
200-210
cm
20 cm
550 X 330
cm
Constant
20
05
Mal
fun
ctio
n
-in
g
SH
F-5
35
Sed
ecal
Bas
ic X
-ray
roo
m n
o.1
Ab
u Y
ou
sef
Al
Naj
jar
Mar
tyr
ho
spit
al
Cement Electronic
Wood
Analog
5
fluorosc-
opy.
50 basic
X-rays
2 mm 200
cm
2 mm
200-210
cm
20 cm
490 X 380
cm
Constant
20
07
Fu
nct
ion
-
ing
UD
15
OB
-
30
Sh
imad
zu F
luo
rosc
o-
py
an
d
bas
ic X
-
ray
roo
m n
o. 2
Cement Electronic
wood Analog
30 2 mm 150
cm
2 mm
200-210
cm
20 cm
410 X 410
cm
Constant
20
05
Fu
nct
ion
-
ing
UD
15
0L
40
E
Sh
imad
zu
Bas
ic X
-
ray
Em
erg
en-
cy r
oom
Cement Electronic
Wood
Analog
------- 2 mm 300
cm
2 mm
200-210
cm
20 cm
700 X 500
Constant
20
00
Mal
fun
-
ctio
nin
g S
ires
ko
-pe
CX
Sie
men
s F
luo
rosc
o-
py
roo
m n
o. 1
Eu
rop
ean
Gaz
a
ho
spit
al
Cement Electronic
Cement
Analog
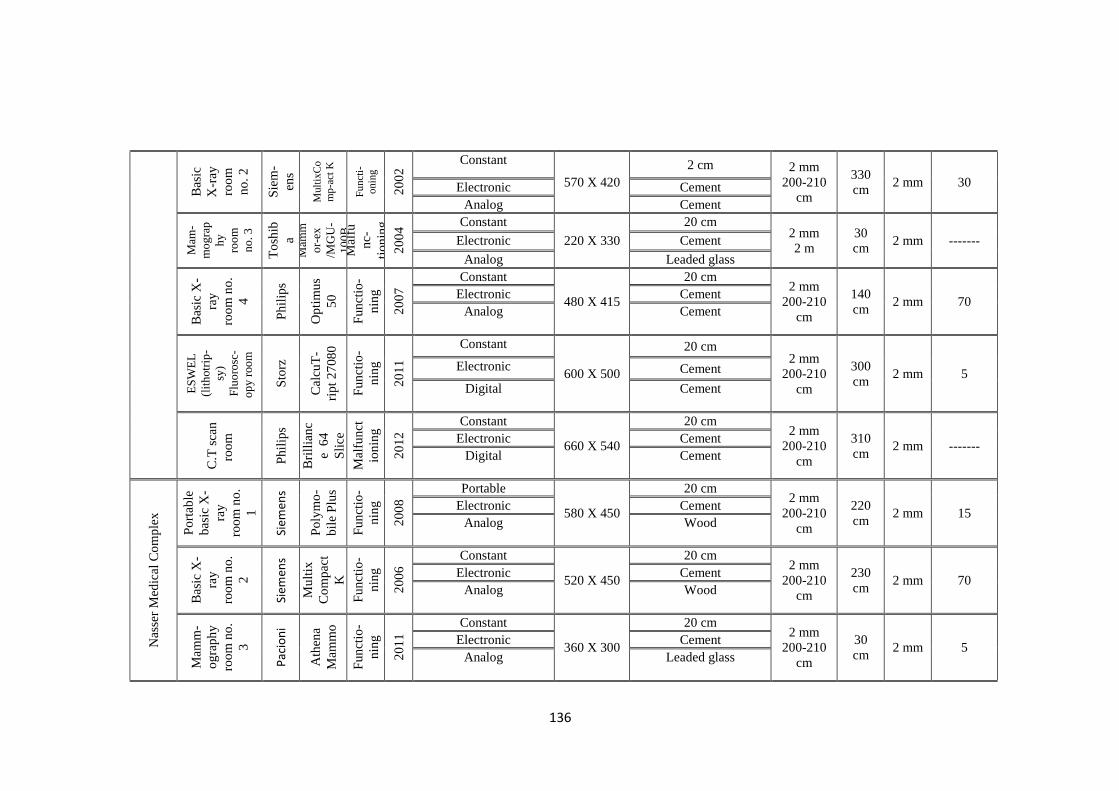
136
30 2 mm 330
cm
2 mm
200-210
cm
2 cm
570 X 420
Constant
20
02
Fu
nct
i-
onin
g M
ult
ixC
o
mp
-act
K
Sie
m-
ens
Bas
ic
X-r
ay
roo
m
no
. 2
Cement Electronic
Cement Analog
------- 2 mm 30
cm
2 mm
2 m
20 cm
220 X 330
Constant
20
04
Mal
fu
nc-
tio
nin
g
Mam
m
or-
ex
/MG
U-
10
0B
To
shib
a Mam
-
mo
gra
p
hy
roo
m
no
. 3
Cement Electronic
Leaded glass Analog
70 2 mm 140
cm
2 mm
200-210
cm
20 cm
480 X 415
Constant
20
07
Fu
nct
io-
nin
g Op
tim
us
50
Ph
ilip
s B
asic
X-
ray
roo
m n
o.
4
Cement Electronic
Cement
Analog
5 2 mm 300
cm
2 mm
200-210
cm
20 cm
600 X 500
Constant
20
11
Fu
nct
io-
nin
g Cal
cuT
-
rip
t 2
708
0
Sto
rz E
SW
EL
(lit
hotr
ip-
sy)
Flu
oro
sc-
op
y r
oo
m
Cement Electronic
Cement
Digital
------- 2 mm 310
cm
2 mm
200-210
cm
20 cm
660 X 540
Constant
20
12
Mal
fun
ct
ion
ing
Bri
llia
nc
e 6
4
Sli
ce P
hil
ips
C.T
sca
n
roo
m
Cement Electronic
Cement
Digital
15 2 mm 220
cm
2 mm
200-210
cm
20 cm
580 X 450
Portable
20
08
Fu
nct
io-
nin
g Po
lym
o-
bil
e P
lus
Siem
ens
Po
rtab
le
bas
ic X
-
ray
roo
m n
o.
1
Nas
ser
Med
ical
Co
mp
lex
Cement Electronic
Wood
Analog
70 2 mm 230
cm
2 mm
200-210
cm
20 cm
520 X 450
Constant
20
06
Fu
nct
io-
nin
g M
ult
ix
Co
mp
act
K
Siem
ens
Bas
ic X
-
ray
roo
m n
o.
2
Cement Electronic
Wood
Analog
5 2 mm 30
cm
2 mm
200-210
cm
20 cm
360 X 300
Constant
20
11
Fu
nct
io-
nin
g A
then
a
Mam
mo
Pac
ion
i
Mam
m-
og
raph
y ro
om
no
.
3
Cement Electronic
Leaded glass
Analog

137
------- 2 mm 230
cm
2 mm
200-210
cm
20 cm
360 X 300
Constant
20
08
Mal
fun
-
ctio
nin
g
Ex
plo
r -
X FI
AD
Pan
ora
-
ma
roo
m n
o.
3
Cement Electronic
Cement
Analog
4 2 mm 160
cm
2 mm
200-210
cm
20 cm
580 X 430
Constant
20
11
Fu
nct
io-
nin
g
Du
o
Dia
gn
ast
Ph
ilip
s
Flu
oro
s-
cop
y roo
m n
o.
4
Cement Electronic
Cement
Digital
20 2 mm 290
cm
2 mm
200-210
cm
20 cm
480 X 430
Constant
20
06
Fu
nct
io-
nin
g So
mat
o
m S
pir
it Si
emen
s
C.T
Sca
n
roo
m n
o.
5
Cement Electronic
Cement
Digital
65 2 mm 240
cm
2 mm
200-210
cm
20 cm
500 X 370
Constant
20
12
Fu
nct
io-
nin
g In
con
ia
65
/R P
hili
ps
Bas
ic X
-
ray
ou
t cl
inic
roo
m
Cement Electronic
Wood
Analog
90 2 mm 310
cm
2 mm
200-210
cm
20 cm
500 X 450
Constant
20
02
Fu
nct
io-
nin
g UD
15
0L
-30
E Sh
imad
zu
Bas
ic X
-
ray
roo
m n
o.
1
Al
Aq
sa M
arty
rs
ho
spit
al
Cement Electronic
Wood
Analog
5
fluorosco
py
30 X-
rays
2 mm 330
cm
2 mm
200-210
cm
20 cm
450 X 360
Constant
20
07
Fu
nct
ion
ing
UD
15
0B
-30
Shim
adzu
Flu
oro
sco
-
py
an
d
bas
ic X
-ray
roo
m n
o.2
Cement Electronic
Wood
Analog
8 2 mm 280
cm
2 mm
200-210
cm
20 cm
600 X 580
Constant
20
09
Fu
nct
ion
ing
AX
IOM
Ico
ns
R2
00
Siem
ens
Flu
oro
sco
py
roo
m n
o. 1
Al
Sh
ifa
Med
ical
Co
mp
lex
Cement t Electronic
Cement t
Digital

138
7 2 mm 300
cm
2 mm
200-210
cm
20 cm
460 X 450
Constant
20
13
Fu
nct
ion
in
g
Ap
olo
Vill
a
Flu
oro
s-
cop
y
roo
m n
o. 2
Cement Electronic
Cement t
Digital
------- 2 mm 30
cm
2 mm
200-210
cm
20 cm
430 X 190
Constant
20
03
Mal
fun
ct
ion
ing
lora
d
Aff
init
y
Ho
logi
c
Mam
m-
og
raph
y
roo
m
no
.3
Cement Electronic
Leaded glass
Analog
------- 2 mm 260
m
2 mm
200-210
cm
20 cm
450 X 430
Constant
20
09
Mal
fun
ct
ion
ing
UD
15
0L
40
E Sh
imad
z
u
Bas
ic X
-
ray
roo
m n
o.
5
Cement Electronic
Cement
Analog
50 2 mm 240
cm
2 mm
200-210
cm
20 cm
450 X 350
Constant
20
12
Fu
nct
ion
ing
----
----
-
Hit
ach
i
Bas
ic X
-
ray
roo
m n
o.
6
Cement Electronic
Cement
Analog
50 2 mm 250
cm
2 mm
200-210
cm
20 cm
580 X 340
Constant
19
97
Fu
nct
ion
ing
UD
15
0L
-RII
Shim
adzu
Bas
ic X
-
ray
roo
m n
o.
7
Cement Electronic
Wood
Analog
-------
No
lead
lining the
room
door
250
cm
2 mm
200-210
cm
20 cm
250 X 230
Constant
20
09
Mal
fun
cti
on
ing
Ort
ho
pho
s
3
Siro
na
Pan
ora
ma
roo
m n
o. 7
Cement Electronic
Cement Analog
45 2 mm 330
cm
2 mm
200-210
cm
20 cm
500 X 450
Constant
20
11
Fu
nct
ion
ing
Bri
llia
nce
CT
6 S
lice
Ph
ilip
s
C.T
sca
n r
oo
m
Cement Electronic
Cement
Digital

139
60 2 mm 180
cm
2 mm
200-210
cm
20 cm
600 X 400
Constant
20
11
Fu
nct
ion
in
g
Mu
ltix
pro
Siem
ens
Bas
ic X
-
ray
Em
erg
e-
ncy
roo
m
Cement Electronic
Cement
Analog
60 2 mm 260
cm
2 mm
200-210
cm
20 cm
400 X 380
Constant
20
09
Fu
nct
ion
ing
UD
15
0L
40
E
Shim
adzu
Bas
ic X
-
ray
ou
t cl
inic
roo
m n
o.1
Cement Electronic
Cement
Analog
60 2 mm 250
cm
2 mm
2 m
20 cm
400 X 360
Constant
20
05
Fu
nct
ion
ing
UD
15
0L
40
E
Shim
adzu
Bas
ic X
-ray
ou
t cl
inic
roo
m n
o. 2
Cement Electronic
Cement
Analog
60 2 mm 100
cm
2 mm
200-210
cm
20 cm
500 X 400
Constant 2
01
1 Fu
nct
io-
nin
g In
con
ia
65
/R P
hili
ps
Bas
ic X
-
ray
roo
m
no
.1
A
l N
aser
Ped
iatr
ic
ho
spit
al
Cement Electronic
Wood
Analog
4 2 mm 230
cm
2 mm
200-210
cm
20 cm
480 X 440
Constant
20
11
Fu
nct
ion
i
ng
Fle
xa
Vis
ion
HB
Shim
adzu
Flu
oro
-
sco
py
roo
m n
o.
1
Ab
del
Azi
z R
ante
ssi
Mar
tyr
Ped
iatr
ic h
osp
ital
Cement Electronic
Cement
Digital
25 2 mm 280
cm
2 mm
200-210
cm
20 cm
550 X 450
Constant
20
08
Fu
nct
ion
-
ing
So
mat
om
-Em
oti
on
Siem
ens
C.T
sca
n
roo
m n
o.
2
Cement Electronic
Cement Digital
90 2 mm 150
cm
2 mm
200-210
cm
20 cm
550 X 390
Constant
20
11
Fu
nct
ion
ing
Mu
ltix
Pro
Siem
ens
Bas
ic X
-ray
E
mer
gen
cy
roo
m
Kam
al A
dw
an
Mar
tyr
ho
spit
al
Cement Electronic
Wood
Analog

140
90 2 mm 200
cm
2 mm
200-210
cm
20 cm
500 X 390
Constant
20
10
Fu
nct
ion
ing
RA
D-
ES
SE
NT
A Ph
ilip
s
Bas
ic X
-
ray
roo
m n
o.
2
Cement Electronic
Wood
Analog
5
fluorosco
py
30 X-
rays
2 mm 170
cm
2 mm
200-210
cm
20 cm
500 X 390
Constant
20
06
Mal
fun
ctio
nin
g
UD
15
0B
-
30
Shim
adzu
Flu
oro
sco
-
py
and
bas
ic
X-r
ay
roo
m n
o. 3
Cement Electronic
Cement
Analog
40 2 mm 160
cm
2 mm
200-210
cm
20 cm
400 X 260
Constant
20
11
Fu
nct
ion
ing
V2
W2
93
0R
BZ
-
65
Vila
Bas
ic X
-
ray
roo
m n
o.
1 B
eit
Han
ou
n
ho
spit
al
Cement Electronic
Wood
Analog

141
Annex (9): The questionnaire analysis tables
Table (1): Socio-demographic and related work factors of the study participants
Item Frequency Percentage
1. Age
From 20-29 years 44 24.3
From 30-39 years 84 46.4
From 40-49 years 38 21.0
More than 50 years 15 8.3
Total 181 100
2. Sex
Male 137 76.1
Female 43 23.9
Total 180 100
3. Occupation
Radiologist 38 20.9
Medical radiographer 144 79.1
Total 182 100
4. Academic qualification
Diploma 16 9.2
Bachelor 144 82.8
Higher degree 14 8.0
Total 174 100
5. Practical experience
1-4 years 32 18.0
5-9 years 64 36.0
10-14 years 48 27.0
15-20 years 34 19.1
Total 178 100
6. Name of hospital
Abu Yousef Al Najjar hospital 12 6.6
European Gaza hospital 16 8.8
Nasser medical complex 29 15.9
Al Aqsa Martyrs hospital 20 11.0
Al Shifa Medical complex 57 31.3
Al Naser pediatric hospital 12 6.6
Abdel Aziz Rantessi Martyr 9 4.9
Kamal Adwan Martyr hospital 17 9.3
Beit Hanoun hospital 10 5.5
Total 182 100
7. Type of radio-diagnostic machine
Basic X-ray 151 83.0
CT scan 80 44.0
Fluoroscopy 107 58.8
Panorama 44 24.2
Mammography 27 14.8
Portable X-ray 76 41.8
8. Daily work hours in radio-diagnostic rooms
1-2 hours 21 11.9
2-3 hours 49 27.8

142
3-4 hours 60 34.1
4-5 hours 32 18.2
More than 5 hours 14 8.0
Total 176 100.0
Table (2): Responses of study participants about the availability of personal
radiation protection devices items
Radiation protection devices
Yes No Don't Know
No. % No. % No. %
Lead aprons 174 95.7 7 3.8 1 0.5
Gonadal shields 29 16 142 78.0 11 6.0
Lead curtains 10 5.5 135 74.2 37 20.3
Lead shields / barriers 73 40.2 92 50.5 17 9.3
Thyroid shields 138 75.9 41 22.5 3 1.6
Lead glass 76 41.8 98 53.8 8 4.4
Lead gloves 38 20.9 134 73.6 10 5.5
Breast shields 13 7.1 155 85.2 14 7.7
Radiation warning signs 41 22.5 132 72.5 9 4.9
Caution lights 48 26.4 122 67.0 12 6.6
Average 35.2% 58.1% 6.7%
Table (3): Responses of study participants to radiation protection awareness
items
Items Yes No
Don't
Know
No. % No. % No. %
1.The annual average dose over five
years should not exceed 20 mSv for
occupational exposure
125 68.7 21 11.5 36 19.8
2.Public should not be exposed to more
than an average of 1 mSv per year 107 58.8 20 11.0 55 30.2
3. Radiation dose limits for pregnant
woman who work in radiation field is 2
mSv during pregnancy period
67 36.8 44 24.2 71 39.0
4. Protection of patient and public from
unnecessary radiation during
radiological examinations are the
responsibility of radiology staff
173 95.1 7 3.8 2 1.1
5. Utilizing high kV during radiological
examinations leads to an increase the
permeability of the radiation beam and
reduce the absorbed dose in the patient
body
163 89.6 10 5.5 9 4.9
6. Short radiation exposure time during
radiological examinations, leads to less 178 97.8 3 1.6 1 0.5

143
patient radiation dose
7. Increasing the distance from the
radiation source to double, leads to
reduce the received dose to half
135 74.2 36 19.8 11 6.0
8. The recommended distance between
X-ray source and radiology workers is
two meter
61 33.5 99 54.4 22 12.1
9. Using the collimators during medical
radiography has a great benefits and
reduce the patient dose
170 93.4 9 4.9 3 1.6
10. Protective lead must periodically
examined to avoid any cracks in the
lead
139 76.4 33 18.1 10 5.5
11. Thickness of the lead lined the X-
ray room wall, which is exposed to
primary X-rays should be 2 mm based
on the principle of ALARA
117 64.3 21 11.5 44 24.2
12. The doors of X-ray room must be
lined from one or two sides with a lead
layer thickness of 1 mm
103 56.6 40 22.0 39 21.4
13. The ideal X-ray room space should
not be less than 36 m2, the ceiling
height is 3.6 m and the exterior
windows height is 2.2 m above the X-
ray room floor
90 49.5 24 13.2 68 37.4
14. The primary radiation barrier must
be height 2m from the X-ray room
floor
129 70.9 11 6.0 42 23.1
15. The X-ray machines maintenance
and calibration must be periodically
carried out to prevent radiation leakage
174 95.6 4 2.2 4 2.2
16. The periodic maintenance for X-
ray rooms walls, doors and radiation
protection tools should be performed to
ensure their efficiency
176 96.7 4 2.2 2 1.1
17. The experience of workers must be
taken into consideration when X-ray
machines were imported and involved
them in the specification of the
purchase
171 94.0 5 2.7 6 3.3
18. The error in the selection of
appropriate kilo volts due to technical
error or malfunction of X-ray machine
leads to excessive radiation dose to the
patient
172 94.5 6 3.3 4 2.2
Average 74.8% 12.1% 13.1%

144
Table (4): Responses of study participants to radiation protection practices
items
Items Yes No
Don't
Know
No. % No. % No. %
1. Have you ever received any training
in radiation protection? 63 34.6 119 65.4 0 0.0
2. Do you explain the radiological
examination instructions to the patient
before the exam?
95 52.2 48 26.4 39 21.4
3. Do you use X-ray tube collimation
during the radiography in order to
reduce patient body dose?
134 73.6 23 12.6 25 13.7
4. Do you stand behind the lead barrier
during giving the radiation dose? 171 94.0 5 2.7 6 3.3
5. If the doctor don't ask for imaging the
Gonads, do you use the gonadal shield
to protect these organs?
30 16.5 140 76.9 12 6.6
6. Do you ask the patient escorts to
evacuate the X-ray room before giving
the X-ray dose?
101 55.5 30 16.5 51 28.0
7. Do you make sure that the X-ray door
is closed during the radiological
examination?
136 74.7 18 9.9 28 15.4
8. Do you keep the requierd distance
between the X-ray source and yourself
during using a mobile X-ray machine?
139 76.4 18 9.9 25 13.7
9. Do you take the necessary precautions
to protect patient escorts and other
patients in the room during using a
mobile X-ray machine?
121 66.5 25 13.7 36 19.8
10. Do you wear the radiation protection
devices to protect yourself from ionizing
radiation?
123 67.6 18 9.9 41 22.5
11. Do you protect the patient escort,
who hold the child during the
radiological examination?
57 31.3 86 47.3 39 21.4
12. Have you been asked to check your
radiology center when there is suspicion
of radiation leakage?
67 36.8 107 58.8 8 4.4
13. Are you interested in maintenance
conducting for X-ray machines when the
defect related with radiation protection?
109 59.0 51 28.0 22 12.1
14. Does the administration respond to
workers' demands regarding to check the
X-ray rooms to make sure about of their
safety?
47 25.8 92 50.5 43 23.6
15. Do you think that your radiology
center conformity with the safety and
radiation protection standards?
66 36.3 101 55.5 15 8.2
Average 53.4 32.3 14.3
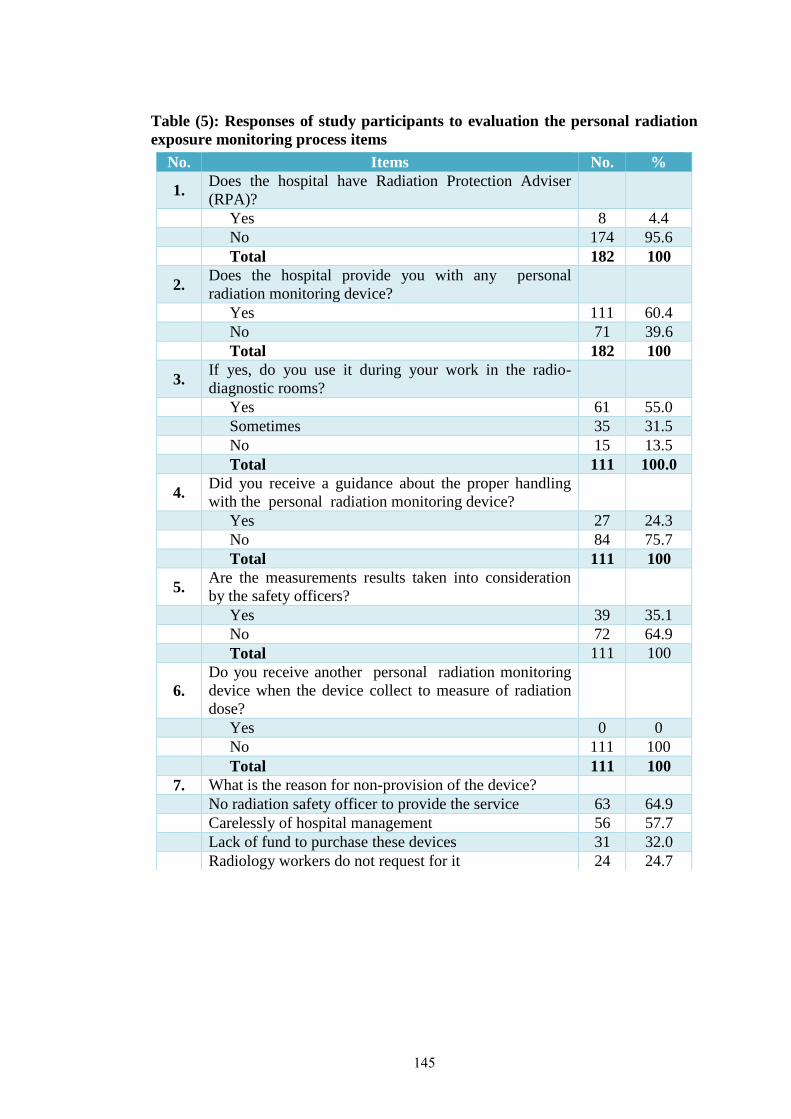
145
Table (5): Responses of study participants to evaluation the personal radiation
exposure monitoring process items
No. Items No. %
1. Does the hospital have Radiation Protection Adviser
(RPA)?
Yes 8 4.4
No 174 95.6
Total 182 100
2. Does the hospital provide you with any personal
radiation monitoring device?
Yes 111 60.4
No 71 39.6
Total 182 100
3. If yes, do you use it during your work in the radio-
diagnostic rooms?
Yes 61 55.0
Sometimes 35 31.5
No 15 13.5
Total 111 100.0
4. Did you receive a guidance about the proper handling
with the personal radiation monitoring device?
Yes 27 24.3
No 84 75.7
Total 111 100
5. Are the measurements results taken into consideration
by the safety officers?
Yes 39 35.1
No 72 64.9
Total 111 100
6.
Do you receive another personal radiation monitoring
device when the device collect to measure of radiation
dose?
Yes 0 0
No 111 100
Total 111 100
7. What is the reason for non-provision of the device?
No radiation safety officer to provide the service 63 64.9
Carelessly of hospital management 56 57.7
Lack of fund to purchase these devices 31 32.0
Radiology workers do not request for it 24 24.7