successful periodontal maintenance of a case with papillon-lefévre syndrome: 12-year follow-up and...
TRANSCRIPT

Volume 72 • Number 6
Case Report
824
Background: Various approaches to treating theperiodontal condition associated with Papillon-Lefèvresyndrome have been reported. These include oralhygiene instruction, use of mouthrinses, frequentdebridement, multiple antibiotic regimens, periodon-tal surgery, extraction of hopeless teeth, and extrac-tion of all deciduous teeth. Because Papillon-Lefèvresyndrome is rare, most publications are case reports,and very few document long-term successful treat-ment of the periodontal condition.
Methods: In 1986, a 3.5-year-old Indo-Canadianmale was diagnosed with Papillon-Lefèvre syndromeand began periodontal treatment. Initial therapy con-sisted of debridement every 3 weeks, a 0.12% chlorhex-idine mouthrinse, 2 regimens of metronidazole, andoral hygiene instruction for his parents. After 10months it became apparent that the treatment washaving little beneficial effect, since the periodontaldestruction continued and teeth 51 and 61 exfoliated.At age 4, all remaining deciduous teeth were extractedand complete dentures inserted for the following 2-year edentulous period; then a 3-month maintenanceschedule was maintained.
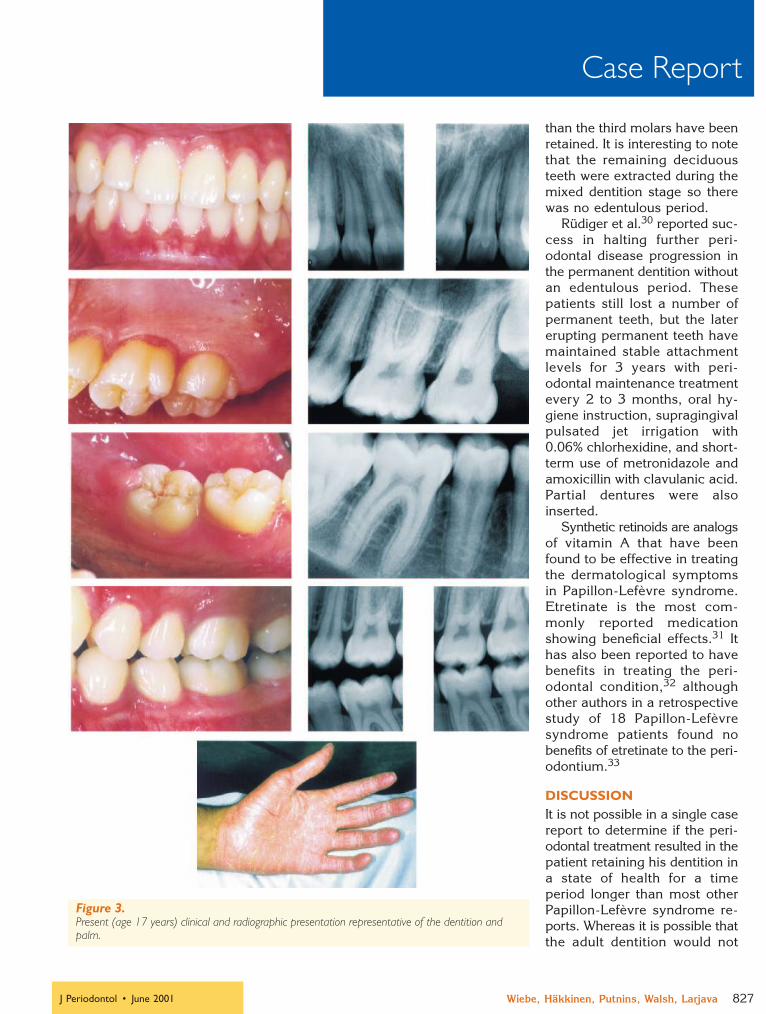
Results: The patient is now 17 years old and allhis adult teeth are present with the exception of thethird molars. His oral hygiene varies between mod-erate and good, with his most recent plaque score at80% effectiveness. There are no probing depths greaterthan 4 mm, with the exception of the distal of thelower second molars where opercula are present.
Conclusions: Extraction of all the deciduous teethfollowed by a period of edentulousness may partiallyexplain the fact that there has been no recurrentattachment loss in the permanent teeth up to age 17.Other explanations are discussed as part of the liter-ature review of Papillon-Lefèvre syndrome. J Peri-odontol 2001;72:824-830.
KEY WORDSPapillon-Lefèvre disease; follow-up studies; toothextraction; tooth, deciduous.
Papillon-Lefèvre syndrome is a very rare (1 to 4cases per million) autosomal recessive disorder char-acterized by well-demarcated hyperkeratosis of thepalms and soles, which usually develops between theages of 2 and 4. At this age, prepubertal periodonti-tis with considerable inflammation develops and pro-ceeds until all deciduous teeth are lost around 4 yearsof age. The inflammation disappears during the eden-tulous period but the process repeats itself when thepermanent dentition erupts.1 Most teeth are lost bythe early teen years, although late-erupting wisdomteeth have often been spared.2 Severe destruction ofthe alveolar bone often occurs, leaving atrophied jaws.Other findings reported in Papillon-Lefèvre casesinclude increased susceptibility to infections in 20%of cases,3 decreased PMN function,4,5 intracranialcalcifications,6 and onychogryphosis.7 No referencesuggesting a decreased life expectancy in these indi-viduals was noted.8
CASE REPORTThe initial periodontal findings have been previouslydocumented.9 The patient is now 17 years old, wellpast the normal age that loss of permanent teeth isexpected in patients with Papillon-Lefèvre syndrome.It is uncertain whether there is consanguinity betweenthe parent families, although both were raised in thesame small village in India and members in both ofthese families are blind as a result of retinitis pig-mentosa, an autosomal recessive degenerative ocu-lar disease. The patient’s mother died of leukemia in1994 and his father of kidney failure in 1996.
A brief history of the case is summarized here. In1986, a 3-and-a-half year old Indo-Canadian malewas referred for periodontal treatment and was diag-nosed with Papillon-Lefèvre syndrome. Initial therapyconsisted of debridement every 3 weeks, a 0.12%chlorhexidine mouthrinse, 2 rounds of metronidazole,and oral hygiene instruction for his parents. Bacter-ial testing was not conducted around the deciduousteeth. After 10 months it became apparent that thetreatment was having little beneficial effect as theperiodontal destruction continued and the mandibu-lar deciduous central incisors exfoliated (Fig. 1). At
Successful Periodontal Maintenance of a Case WithPapillon-Lefèvre Syndrome: 12-Year Follow-Up and Review of the Literature*Colin B. Wiebe, Lari Häkkinen, Edward E. Putnins, Priscilla Walsh, and Hannu S. Larjava
* Department of Oral Biological and Medical Sciences, The University ofBritish Columbia, Vancouver, BC.
0227_IPC_AAP_553301 6/4/01 9:38 AM Page 824

J Periodontol • June 2001
Case Report
Wiebe, Häkkinen, Putnins, Walsh, Larjava 825
age 4, all remaining deciduous teeth were extractedand complete dentures inserted for the following 2-year edentulous period. DNA probe analysis of plaquesamples from the sulcus of the first molars was con-ducted as these teeth erupted. A weak signal (0.2%of the total signal) was found for Porphyromonas gin-givalis and a strong signal (5%) for Bacteroidesforsythus. A 3-month maintenance schedule wasestablished, but from age 10 to 13 years, he wouldhave times of poor oral hygiene and, for much of thistime, he was brought in for de-plaquing on a 6-weekschedule. No further antibiotic treatment was admin-istered during the time the permanent teeth wereerupting. He has never received etretinate or otherretinoid therapy for either his skin or periodontal con-dition. The patient is now 17 years old and all hisadult teeth are present with the exception of the thirdmolars. His oral hygiene varies between moderateand good, with his most recent plaque score at 80%effectiveness. There are no probing depths greaterthan 4 mm with the exception of the distal of thelower second molars where opercula are present.
A holding arch was placed on the first molars oncethey erupted but there was no guidance for theseteeth as they erupted, since all the deciduous teethexfoliated or were extracted prematurely. As a result,the patient has an end-to-end occlusion. Orthodon-tic treatment was avoided during his early and mid-teens to avoid creating plaque-retentive areas andencouraging recurrent disease. As it is now apparentthat his condition is stable, approval for orthodontictreatment has been given, assuming the patient isagreeable to continuing with 3-month maintenancevisits during this phase.
The patient’s third molars are likely to becomeimpacted. Presently, the roots are one-third devel-oped, a thin layer of bone is present over the occlusalsurface, and there is no connection to the oral cav-ity. It has been recommended that all 4 third molarsbe extracted in 1 year’s time.
The hyperkeratosis on his hands and feet still exists,but the severity appears to have decreased with ageand the patient states it is not a problem for him(Figs. 2 and 3).
It appears that extraction of all the deciduous teethfollowed by a period of edentulousness was effec-tive in this patient since there has been no recurrentattachment loss in the permanent teeth up to age17. The degree of involvement on his hands and feethas also decreased and it is possible that some fac-tor, other than the periodontal treatment, hasdecreased his risk for clinical attachment loss. Con-sidering the poor success rate of controlling peri-odontal disease in Papillon-Lefèvre patients,10 itseems justifiable to extract all of the deciduous teethbefore any permanent teeth erupt. Although itappears extreme, alternative periodontal treatmentoptions have mainly been unsuccessful and attach-ment loss has continued.11
LITERATURE REVIEWTheories on the etiology of the periodontal lesionsseen in Papillon-Lefèvre syndrome have examinedanatomical defects (cemental, epithelial and sali-vary),12 microbiological factors (Actinobacillus actin-omycetemcomitans13 and other putative periodontalpathogens14), viral agents (cytomegalovirus andEpstein-Barr type 1 virus15), and host response (PMNfunction16 and lymphocyte functional defects17) ascausative factors. Interestingly, Lundgren et al.18 usingcheckerboard DNA-DNA hybridization in 12 Papil-lon-Lefèvre patients were unable to demonstrate aspecific bacterial profile associated with the peri-odontal condition. Kleinfelder et al.13 also did not findany morphological abnormalities of the root cemen-tum. It is likely that many of the above reported fac-tors are not necessary for the periodontal lesions todevelop, but rather are a result of the disease or arecontributory to the attachment loss.
Recently, 3 groups have mapped the gene forPapillon-Lefèvre syndrome to chromosome 11q14-q21.19-21 This major gene locus includes 6 genesincluding cathepsin C. Cathepsin C (dipeptidylaminopeptidase I) is a lysosomal cysteine proteinasewhich plays an important role in the intracellulardegradation of proteins and also processes and acti-
Figure 1.Appearance of dentition at initial presentation; age 3.5 years.
0227_IPC_AAP_553301 6/4/01 9:38 AM Page 825

Volume 72 • Number 6
Case Report
826 Twelve-Year Periodontal Maintenance in Papillon-Lefèvre Syndrome
TREATMENT OF PERIODONTAL DISEASE INPAPILLON-LEFÈVRE PATIENTSBaer and McDonald26 recommended treatment ofperiodontal disease associated with Papillon-Lefèvresyndrome by extraction of all the deciduous teeth by3 years of age, followed by an edentulous period withcomplete dentures inserted 3 months after the extrac-tions. Tetracycline was given at the time of dentureinsertion and as the permanent teeth were erupting.Similar protocols have been advocated by Tinanoffet al.27 and Preus.28 Tinanoff et al.29 published a 15-year follow-up of a variant on this protocol in onepatient. Conventional debridement and regimens oftetracycline and erythromycin were unsuccessful inreducing inflammation or tooth mobility. Because thepatient was 9 years old, all the primary teeth hadexfoliated and 14 permanent teeth (incisors, firstmolars, and mandicular cuspids) had erupted. Theseteeth were extracted to create the edentulous period.As the remaining permanent teeth erupted, a castpartial denture was placed. Although the patient’soral hygiene was poor, she had not lost any moreteeth at age 24 and her clinical attachment appearsstable.
De Vree et al.11 also published a 15-year follow-up of 2 patients treated by extraction of all decidu-ous teeth, doxycycline and metronidazole therapy,oral hygiene instruction, chlorhexidine rinses, bi-weekly professional prophylaxis, and scaling and rootplaning and periodontal surgery as indicated. Thiswas unsuccessful in one case that required all teethexcept the third molars to be extracted. The othercase was moderately successful and 12 teeth other
Figure 2.Appearance of dentition and hand during dental treatment; age from left to right: 4, 10, 12, and 14.
vates several leukocyte and mast cell granule ser-ine proteinases critical to immune and inflammatoryresponses including cathepsin G, leukocyte elastase,mast cell chymase, and tryptase and lymphocytegranzymes B and H.22 It is expressed in the lungs,kidneys, and in keratinized epithelial areas normallyaffected in Papillon-Lefèvre syndrome, namely thepalms, soles, knees, and oral keratinized gingiva.23
It is also expressed in polymorphonuclear leuko-cytes, alveolar macrophages, and osteoclasts.22 Hartet al.23 carried out sequence analysis in 5 consan-guineous families and found 4 different cathepsin Cmutations that resulted in premature stop codonsand produced the same clinical outcome in subjectsthat were homozygous for these mutations. Parentsand siblings who were heterozygous for the cathep-sin C mutations did not develop Papillon-Lefèvre syn-drome. Although the pathogenesis of Papillon-Lefèvreis not established, it appears that cathepsin C isimportant in the normal development/maintenanceof the skin and immune and inflammatory cells. Whythe lesions develop in certain areas of the body isstill a mystery. Of particular interest in consideringthe periodontal condition is whether a cathepsin Cmutation also affects the junctional epithelium aroundthe teeth.
Hart and coworkers have described similar muta-tions on chromosome 11q14 involving the cathepsinC gene in cases with non-syndromic prepubertal peri-odontitis24 and in Haim-Munk syndrome,25 which issimilar to Papillon-Lefèvre syndrome although it alsoinvolves arachnodactly, acroosteolysis, atrophy of thenails, and deformity of the phalanges of the hand.
0227_IPC_AAP_553301 6/4/01 9:38 AM Page 826
J Periodontol • June 2001
Case Report
Wiebe, Häkkinen, Putnins, Walsh, Larjava 827
than the third molars have beenretained. It is interesting to notethat the remaining deciduousteeth were extracted during themixed dentition stage so therewas no edentulous period.
Rüdiger et al.30 reported suc-cess in halting further peri-odontal disease progression inthe permanent dentition withoutan edentulous period. Thesepatients still lost a number ofpermanent teeth, but the latererupting permanent teeth havemaintained stable attachmentlevels for 3 years with peri-odontal maintenance treatmentevery 2 to 3 months, oral hy-giene instruction, supragingivalpulsated jet irrigation with0.06% chlorhexidine, and short-term use of metronidazole andamoxicillin with clavulanic acid.Partial dentures were alsoinserted.
Synthetic retinoids are analogsof vitamin A that have beenfound to be effective in treatingthe dermatological symptomsin Papillon-Lefèvre syndrome.Etretinate is the most com-monly reported medicationshowing beneficial effects.31 Ithas also been reported to havebenefits in treating the peri-odontal condition,32 althoughother authors in a retrospectivestudy of 18 Papillon-Lefèvresyndrome patients found nobenefits of etretinate to the peri-odontium.33
DISCUSSIONIt is not possible in a single casereport to determine if the peri-odontal treatment resulted in thepatient retaining his dentition ina state of health for a timeperiod longer than most otherPapillon-Lefèvre syndrome re-ports. Whereas it is possible thatthe adult dentition would not
Figure 3.Present (age 17 years) clinical and radiographic presentation representative of the dentition andpalm.
0227_IPC_AAP_553301 6/4/01 9:38 AM Page 827

Volume 72 • Number 6
Case Report
have been affected, this is unlikely considering it iswell documented that Papillon-Lefèvre syndromecommonly affects both the deciduous and perma-nent teeth and generally results in their loss at a laterstage in the order of eruption.2 Of particular rele-vance for comparison are the cases documented byBaer and McDonald26 and Tinanoff et al.29 Baer andMcDonald recommended the treatment protocol usedfor our patient. They published a very brief follow-upreport34 when the patient was 25 years old andreported periodontal health.
Tinanoff et al.29 provide significantly more infor-mation on the long-term follow-up of their patient.After all the permanent incisors, first molars, andlower canines were extracted when the patient was9 years old, she then went through an edentulousperiod. Eventually, all the remaining permanent teetherupted and a cast partial denture was inserted. Thepatient continued to have poor oral hygiene and gen-eralized gingivitis, yet at age 24, the remaining 16 per-manent teeth appeared to have normal radiographicalveolar bone levels and only 3 probing sites were 5mm, with all the others in the 2 to 4 mm range.
In the case reported here and in others, it appearsthat the palmar plantar hyperkeratosis decreased inseverity with age.29,35 It has been reported in somechildren that palmar plantar keratosis develops at thesame time as the periodontal disease affecting theprimary dentition and then decreases once the decid-uous teeth are lost.35 It is interesting to note that var-ious other genetic dermatological disorders also havebeen reported to decrease in severity with age. Pear-son36 has reported decreased blistering at puberty,especially in females, in patients with epidermolysisbullosa simplex. Epidermolysis bullosa simplexinvolves tissue cleavage within the epidermal celllayer or at the level of the basal keratinocytes.37 Thereare many types, with the majority having an autoso-mal dominant mode of inheritance.38 Gene defectscoding for keratins 5 and 14 have been reported.39
Decreased blistering and skin fragility also have beenreported in Kindler syndrome, a rare genetic vesicu-lobullous disorder that may also involve aggressiveperiodontitis.40 Since these are genetic disorders, itis unknown why symptoms would decrease with age.One possibility is that missing or mutated proteinsare compensated for by other components over time.It is also possible that proteins necessary duringdevelopmental stages are replaced by others in adult-hood. The fact that wisdom teeth are often spared2
suggests that aging, rather than development andtooth eruption, is associated with improved expected
outcome in these patients. Since different studiesreport different clinical outcomes, it is possible thatthe timing of the disease burst is different betweenindividual patients. If this is the case, the clinical out-come is more dependent on the maturation or agingof the individual (i.e., replacement of developmentalproteins with more stable ones) than the periodontalcare provided. In the case reported here, a possibleexplanation for the lack of disease recurrence may bethat this unknown effect has started at a younger agethan normal and possibly he is much less suscepti-ble to periodontal disease now.
A case of severe early-onset periodontitis with ahistory of prepubertal periodontitis associated withKindler syndrome has been previously published.40,41
Kindler syndrome is an extremely rare and poorlyunderstood disorder that demonstrates the cutaneousmanifestations of epidermolysis bullosa and poikilo-derma congenitale.42 The periodontal condition pre-sentation is not unlike that found in Papillon-Lefèvresyndrome, although this patient has managed toretain over half her permanent dentition with regularperiodontal maintenance. The suggestion was pre-sented that the periodontal condition may have moreto do with a weakened attachment of the gingiva tothe tooth due to a basement membrane defect ratherthan as a result of a particular virulent microbial infec-tion. It is possible that a structural defect of the junc-tional epithelium in Papillon-Lefèvre syndrome, ratherthan a particular periodontal pathogen, results in thesevere periodontal condition observed. A potentialstructural defect in the gingiva and junctional epithe-lium in Papillon-Lefèvre syndrome remains to beshown. Additionally, it is possible that the mutationsin the cathepsin C gene may also affect immunedefense of the periodontal sulcus through its involve-ment as a regulator of inflammatory cells.22 Numer-ous reports of immunological dysfunction have beennoted including reduced chemotaxis, low integrinexpression, increased superoxide production, andimpaired phagocytosis by neutrophils (see reference43 for review). The case report by Tinanoff et al.29
found decreased neutrophil chemotaxis and adher-ence in the patient at age 9, but these abnormalitieswere no longer present at age 24. This raises thequestion of whether the neutrophil defects are causedby periodontal pathogens and whether the patient’srisk for periodontal disease decreases with age as theimmune response develops to handle the antigenicchallenge.
Evidence continues to mount about the role ofgenetic factors in early-onset periodontal disease. It
828 Twelve-Year Periodontal Maintenance in Papillon-Lefèvre Syndrome
0227_IPC_AAP_553301 6/4/01 9:38 AM Page 828

J Periodontol • June 2001
Case Report
is interesting to consider whether these factors affectthe host immune response or also affect the struc-tural defenses of the periodontium including thebasement membrane and the junctional epitheliumattachment to the tooth.
CONCLUSIONSIt is not understood why certain genetic diseasesdecrease in severity with age. In Papillon-Lefèvre syn-drome, case reports have shown that no periodontaltreatment or standard non-surgical and surgical peri-odontal treatment result in the loss of all permanentteeth by age 20, with the exception of the thirdmolars.44 Maintaining periodontal health of some ofthe adult dentition has been reported when continu-ous antibiotic therapy28 or extraction followed by anedentulous period29 has been employed. This hasbeen the case even when the oral hygiene is poor, i.e.,Tinanoff et al.29 and the present case report. Itappears that success in retaining adult teeth dependson the timing of these unconventional therapies (con-tinuous antibiotics, extraction of all erupted teeth)when Papillon-Lefèvre syndrome symptoms are thestrongest. With increasing age, the symptoms asso-ciated with the syndrome decrease, and if any teetherupt after that period into a mouth that is free ofperiodontal disease, patients have a good chance ofremaining periodontally healthy, even if oral hygieneand maintenance are not optimal.
ACKNOWLEDGMENTThe authors gratefully acknowledge the contribution ofMr. Bruce McCaughey in preparing Figures 1 and 2.
REFERENCES1. Gorlin RJ, Cohen MM Jr., Levin LS. Syndromes of the
Head and Neck, 3rd ed. New York: Oxford UniversityPress;1990:853-854.
2. Haneke E. The Papillon-Lefèvre syndrome: Keratosispalmoplantaris with periodontopathy. Report of a caseand review of the cases in the literature. Hum Genet1979;51:376-382.
3. Haneke E, Hornstein OP, Lex C. Increased suscepti-bility to infections in Papillon-Lefèvre syndrome. Der-matologica 1975;150:283-286.
4. Firatli E, Gurel N, Efeoglu A, Badur S. Clinical andimmunological findings in 2 siblings with Papillon-Lefèvre syndrome. J Periodontol 1996;67:1210-1215.
5. Ghaffar KA, Zahran F, Fahmy HM, Brown RS. Papillon-Lefèvre syndrome. Neutrophil function in 15 cases from4 families in Egypt. Oral Surg Oral Med Oral PatholOral Radiol Endod 1999;88:320-325.
6. Brownstein MM, Skolnik P. Papillon-Lefèvre syndrome.Arch Dermatol 1972;106:533-534.
7. Ziprkowski L, Ramon Y, Brish M, Hashomer T. Hyper-keratosis palmoplantaris with periodontosis (Papillon-Lefèvre). Arch Dermatol 1963;88:207-209.
8. OMIM, Online Mendelian Inheritance in Man [databaseonline]. Baltimore, MD: Johns Hopkins University. OMIMnumber: {245000}: {7/27/00}. Available at: http://www.ncbi.nlm.nih.gov/omim/. Accessed in March 2000.
9. French D, Scott H, Overall CM. Papillon-Lefèvre syn-drome associated with early onset periodontitis: Areview and case study. J Can Dent Assoc 1995;61:432-438.
10. Posteraro AF. Papillon-Lefèvre syndrome. J Ala DentAssoc 1992;76:16-19.
11. De Vree H, Steenackers K, De Boever JA. Periodontaltreatment of rapid progressive periodontitis in 2 siblingswith Papillon-Lefèvre syndrome: 15-year follow-up. JClin Periodontol 2000;27:354-360.
12. Lundgren T, Twetman S, Johansson I, Crossner CG,Birkhed D. Saliva composition in children and youngadults with Papillon-Lefèvre syndrome. J Clin Peri-odontol 1996;23:1068-1072.
13. Kleinfelder JW, Topoll HH, Preus HR, Muller RF, LangeDE, Bocker W. Microbiological and immunohisto-chemical findings in a patient with Papillon-Lefèvresyndrome. J Clin Periodontol 1996;23:1032-1038.
14. Clerehugh V, Drucker DB, Seymour GJ, Bird PS. Micro-biological and serological investigations of oral lesionsin Papillon-Lefèvre syndrome. J Clin Pathol 1996;49:255-257.
15. Velazco CH, Coelho C, Salazar F, Contreras A, Slots J,Pacheco JJ. Microbiological features of Papillon-Lefèvresyndrome periodontitis. J Clin Periodontol 1999;26:622-627.
16. Liu R, Cao C, Meng H, Tang Z. Leukocyte function in2 cases of Papillon-Lefèvre syndrome. J Clin Peri-odontol 2000;27:69-73.
17. Firatli E, Gurel N, Efeoglu A. Papillon-Lefèvre syn-drome. Analysis of peripheral blood lymphocyte sub-sets. J Clin Periodontol 1996;23:823-825.
18. Lundgren T, Renvert S, Papapanou PN, Dahlen G. Sub-gingival microbial profile of Papillon-Lefèvre patientsassessed by DNA probes. J Clin Periodontol 1998;25:624-629.
19. Fischer J, Blanchet-Bardon C, Prud’homme JF, et al.Mapping of the Papillon-Lefèvre syndrome to chro-mosome 11q14 region. Eur J Hum Genet 1997;5:156-160.
20. Laass MW, Hennies HC, Preis S, et al. Localization ofa gene for Papillon-Lefèvre syndrome to chromosome11q14-q21 by homozygous mapping. Hum Genet1997;101:376-382.
21. Hart TC, Bowden DW, Ghaffar KA, et al. Sublocaliza-tion of the Papillon-Lefèvre syndrome locus on 11q14-q21. Am J Med Genet 1998;79:134-139.
22. Rao NV, Rao GV, Hoidal JR. Human dipeptidyl-pepti-dase I. J Biol Chem 1997;272:10260-10265.
23. Hart TC, Hart S, Bowden DW, et al. Mutations of thecathepsin C gene are responsible for Papillon-Lefèvresyndrome. J Med Genet 1999;36:881-887.
24. Hart TC, Hart PS, Michalec MD, et al. Localization ofa gene for prepubertal periodontitis to chromosome11q14 and identification of a cathepsin C gene muta-tion. J Med Genet 2000;37:95-101.
25. Hart TC, Hart PS, Michalec MD, et al. Haim-Munk syn-drome and Papillon-Lefèvre syndrome are allelic muta-
Wiebe, Häkkinen, Putnins, Walsh, Larjava 829
0227_IPC_AAP_553301 6/4/01 9:38 AM Page 829

Volume 72 • Number 6
Case Report
830 Twelve-Year Periodontal Maintenance in Papillon-Lefèvre Syndrome
tions in cathepsin C. J Med Genet 2000;37:88-94.26. Baer PN, McDonald RE. Suggested mode of periodontal
therapy for patients with Papillon-Lefèvre syndrome.Periodontol Case Rep 1981;1:10.
27. Tinanoff N, Tanzer J, Kornman KS, Maderazo EG.Treatment of the periodontal component of Papillon-Lefèvre syndrome. J Clin Periodontol 1986;13:6-10.
28. Preus HR. Treatment of rapidly destructive periodon-titis in Papillon-Lefèvre syndrome. Laboratory and clin-ical observations. J Clin Periodontol 1988;15:639-643.
29. Tinanoff N, Tempro P, Maderazo EG. Dental treatmentof Papillon-Lefèvre syndrome: 15-year follow-up. J ClinPeriodontol 1995;22:609-612.
30. Rüdiger S, Petersilka G, Flemmig TF. Combined sys-temic and local antimicrobial therapy of periodontaldisease in Papillon-Lefèvre syndrome. A report of 4cases. J Clin Periodontol 1999;26:847-854.
31. Siragusa M, Romano C, Batticane N, Batolo D, SchepisC. A new family with Papillon-Lefèvre syndrome: Effec-tiveness of etretinate treatment. Cutis 2000;65:151-155.
32. Gelmetti C, Nazzaro V, Cerri D, Fracasso L. Long-termpreservation of permanent teeth in a patient with Papil-lon-Lefèvre syndrome treated with etretinate. PediatrDermatol 1989;6:222-225.
33. Lundgren T, Crossner CG, Twetman S, Ullbro C. Sys-temic retinoid medication and periodontal health inpatients with Papillon-Lefèvre syndrome. J Clin Peri-odontol 1996;23:176-179.
34. Baer PN. Preventing loss of teeth in patients with Papil-lon-Lefèvre syndrome. J Pedodontics 1989;13:182-183.
35. Gorlin RJ, Sedano H, Anderson VE. The syndrome ofpalmar-plantar hyperkeratosis and premature peri-odontal destruction of the teeth. J Pediatr 1964;65:895-908.
36. Pearson RW. Clinicopathologic types of epidermolysisbullosa and their nondermatologic complications. ArchDermatol 1988;124:718-725.
37. Wiebe CB, Larjava HS. Do mutations in the basementmembrane zone affect the human periodontium?Review with special reference to epidermolysis bullosa.J West Soc Periodontol 1998;46:5-18.
38. Fine JD, Bauer EA, Briggaman RA, et al. Revised clin-ical and laboratory criteria for subtypes of inheritedepidermolysis bullosa. J Am Acad Dermatol 1991;24:119-135.
39. Vassar R, Coulombe PA, Degenstein L, Albers K, FuchsE. Mutant keratin expression in transgenic mice causesmarked abnormalities resembling a human genetic skindisease. Cell 1991;64:365-380.
40. Wiebe CB, Sliver JG, Larjava HS. Early-onset peri-odontitis associated with Weary-Kindler syndrome: Acase report. J Periodontol 1996;67:1004-1010.
41. Wiebe CB, Larjava HS. Abnormal deposition of type VIIcollagen in Kindler syndrome. Arch Dermatol Res1999;291:6-13.
42. Kindler T. Congenitale poikiloderma with traumaticbulla formation and progressive cutaneous atrophy. BrJ Dermatol 1954;66:104-111.
43. Hart TC, Shapira L. Papillon-Lefèvre syndrome. Peri-odontol 2000 1994;6:88-100.
44. Baer PN, Benjamin SD. Periodontal Disease in Chil-dren and Adolescents. Toronto: J.B. Lippincott Com-pany; 1974:206-208.
Send reprint requests to: Dr. Colin B. Wiebe, Oral Biolog-ical and Medical Sciences, Faculty of Dentistry, Universityof British Columbia, 2199 Wesbrook Mall, Vancouver, BC,V6T 1Z3. Telephone: 604/822-3562; e-mail: [email protected]
Accepted for publication January 5, 2001.
0227_IPC_AAP_553301 6/4/01 9:38 AM Page 830