su brailsford website - transfusion guidelines · su brailsford consultant in ... screening jan-dec...
TRANSCRIPT

Su Brailsford Consultant in Epidemiology and Health Protection NHS Blood and Transplant Colindale
Transfusion- The 3 R s Nottingham January 2015

Overview
What can be transmitted by transfusion ?How do we reduce the risk?
viralbacterial
How do we investigate a TTI?Are our risk reductions methods working?What does the future hold?

What can be transmitted by transfusion?
Viral infectionswindow period infectionthings we don t test forpreviously unknown infections
Parasitestravel?
Bacteriascreening of platelets-residual risk
Prionsno current screening test
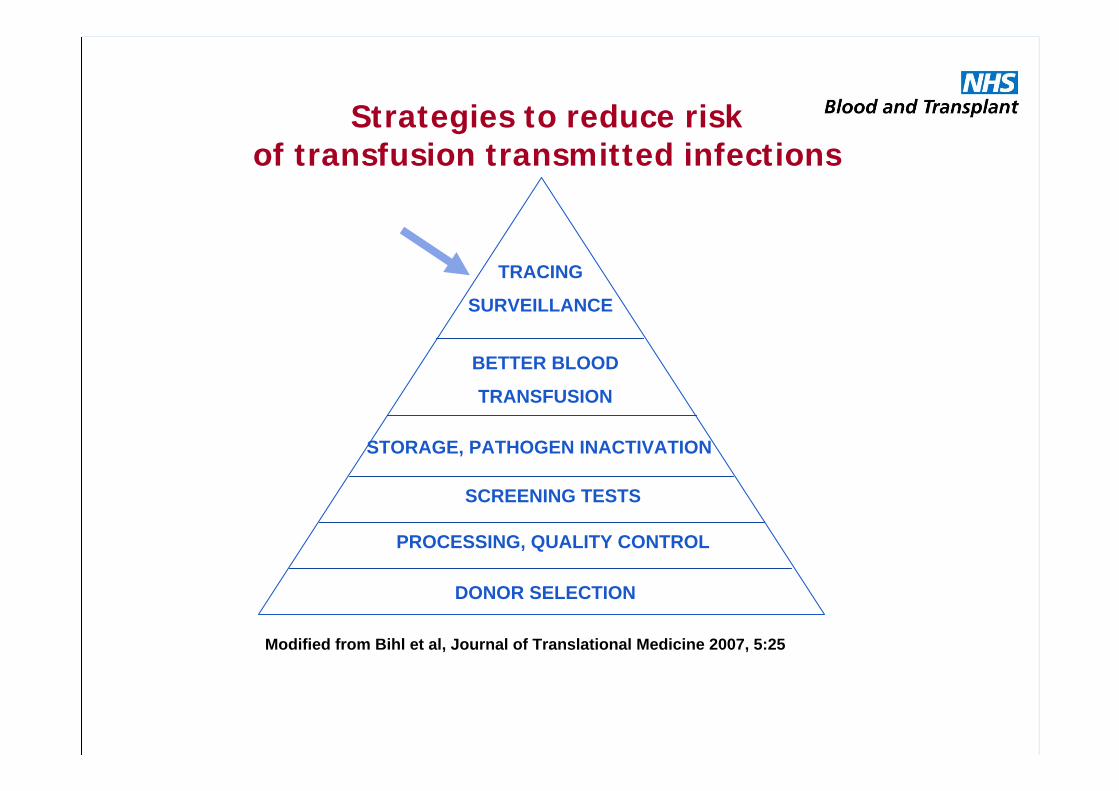
Strategies to reduce risk of transfusion transmitted infections
DONOR SELECTION
PROCESSING, QUALITY CONTROL
SCREENING TESTS
STORAGE, PATHOGEN INACTIVATION
BETTER BLOOD
TRANSFUSION
TRACING
SURVEILLANCE
Modified from Bihl et al, Journal of Translational Medicine 2007, 5:25

Donor selectionBlood from volunteers is saferDonor selection process
Known infections: BBVs
Behavioural risks
Recent risks: Piercing
Travel history: malaria, WNV, T. cruzi
MaintainingSupply & cost
Minimisingrisk

We can t always test: vCJDMajor impact on blood safety measures in UK
Donor deferralTransfused donors
Active surveillance
Other measures
UK plasma no longer used for fractionationImportation of FFP for certain groupsReduce donor exposuresLeucodepletion

Current Testing StrategiesTimeline of introduction of microbiological tests for blood
donations, UK
And additional tests e.g. West Nile Virus
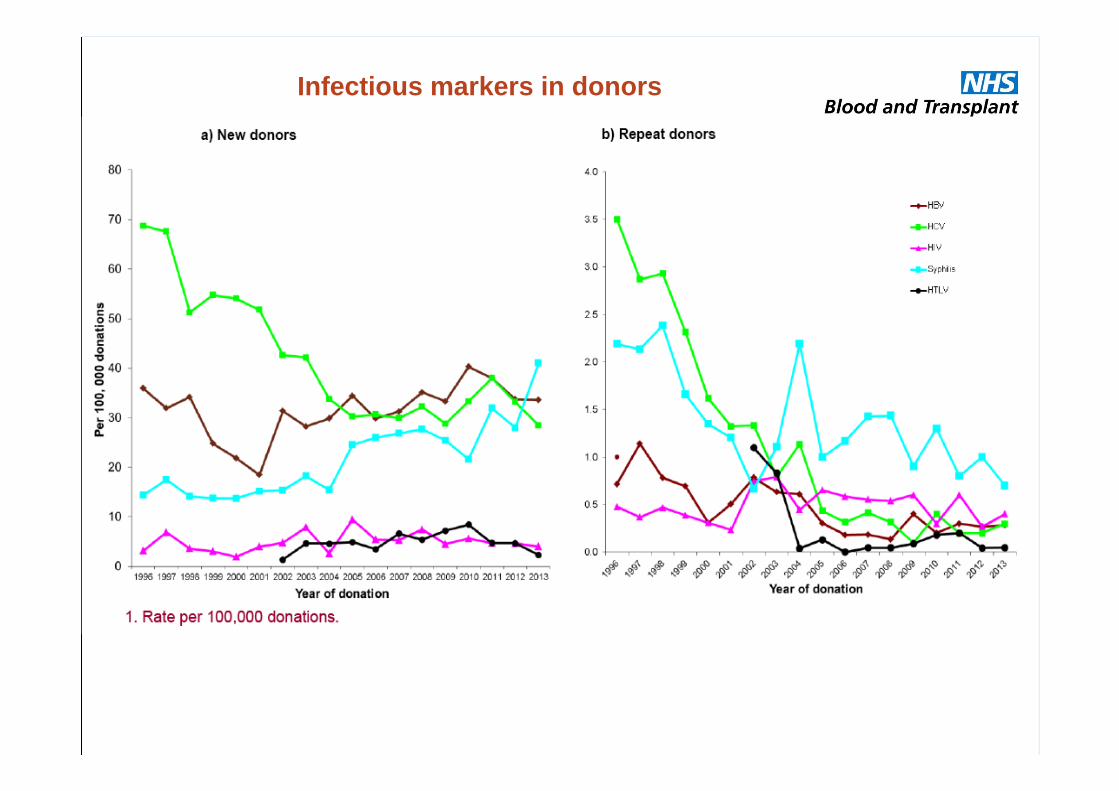
Infectious markers in donors
Infection rate in donors declining but
Viral TTIs still happen, investigated when:Post-donation illness in donorInfection in recipient with no other risk
Why?No testWindow period infectionEmerging infection

Window Periods
biggest component of risk of issuing an infectious component relates to window period
very recent infections in seroconverting donors could be missed
hepatitis B of most concern : long window period/ highest residual risk
Marker Risk (per million)
WP (days)
HBV 1: 2.2 38.3
HCV 1: 39.0 4
HIV 1: 5.9 9
Expect to miss 1 HBV/year, 1 HCV every 16.7 years and 1 HIV every 2.6 years.
Investigation of suspected TTIs
Viral (often chronic infections): May be long lag time between transfusion and diagnosis/reporting.Where there are no other known risk factors, the case is reported to clinical team at NHSBT for investigation. Re-testing of archive or subsequent samples from the donor may occur.
If possible molecular typing to prove the donor and recipient viruses are indistinguishable
Not TTI? Non-specific reactions/ Passive transfer: Parker S et al BMC Infectious Diseases. 2014:14; 99 Case report: passive transfer of hepatitis B antibodies from intravenous immunoglobulin.


What constitutes a TTI? SHOT definition
A report is classified as TTI if, following investigation:
The recipient had evidence of infection post-transfusion, and there was no evidence of infection prior to transfusion and no evidence of an alternative source of infection;
and either:At least one component received by the infected recipient was donated by a donor who had evidence of the same transmissible infection,
or:At least one component received by the infected recipient was shown to contain the agent of infection.

What is transmitted?
2005 hepatitis A and hepatitis B transmission
HAV-post-donation report/HBV early acute infection (pre-NAT)
2011 hepatitis B transmission
Things we test for and things we don t
2012/13 Parvovirus B19, HEV, HBV
B19, circulating in community
Hepatitis E genotype 3 Contaminated food

Things we don t routinely test for: hepatitis E
Widespread zoonosis, universally present in pigs
Understanding of HEV infections in England and Wales has changed
high rate of asymptomatic infectionsestimated 60 000 HEV infections/year in England and Wales
high seroprevalence: antibody positive rates of ~13%molecular characterisation studies indicate a genotype 3 virus

HEV and blood safety?
Blood components and the immunosuppressed population
Evidence of HEV turnover in blood donors in Europe
Post transfusion hepatitis linked to HEV has been reported from several countries including the UK

SE England study: Lancet
9382 minipools tested (x24) = 225,168 individual donations
78 HEV RNA repeat reactive (positive) donations
= 0.03% of donations HEV RNA positive
= 1:2900 donations HEV RNA positive
Hewitt PE, Ijaz S et al Hepatitis E virus in blood components: a prevalence and transmission study in southeast England. Lancet 2014:15;384:1766-73

Outcome in HEV infected recipients
immunocompetent infected recipients generally cleared infection rapidlyimmunosuppressed infected recipients exhibited prolonged viraemia of 4 to 35 weeks one immunosuppressed recipient treated successfully with Ribavirin in between cycles of chemotherapy, two cleared on reduction of immunosuppressionsome recipients did not become infected when expected to be so: ?? protective role of other transfused components with HEV antibodies

Do we need to test?
SaBTO working group considering impact of HEV on blood, tissues and organs
Report later in 2015 with recommendation to DH
Watch this space .

Bacterial v viral infections
Bacterial Viral
Time to report Hours-days May be years
Symptoms Usually acute May not be recognised
Outcome Serious morbidity/fatal May clear or become chronic
Reported after hospital discharge
Rarely Often
Risk reduction
In recent years bacteria main cause of TTIsStaphylococcus aureusStreptococcus pneumoniaePseudomonas spp.
Number of risk reduction measuresDonor selectionSkin cleansingDiversion pouchIPC

Bacterial screening
Bacterial screening of all platelets
Sample taken after a minimum hold of 36 hours
Released after 6 hours on BacTAlert
Bottles remain on machine until end of shelf-life or until they go ping i.e. initial reactive
Slow growing bugs may result in an initial reactive post issue: recall/transfusion

Recall
All initial reactives are recalled
Do not know if reaction is real at this point
Bottles and packs returned for testing
Not all will be positive for growth
But any patient adverse events should be reported

Does the current method work?
Type Number of packs
Initial reactive(%)
Confirmed positive (%)
Indeterminate positive (%)
Apheresis 771785 3441 (0.45) 159 (0.02) 280 (0.04)
Pool 177236 575 (0.32) 123 (0.07) 111 (0.06)
False negatives-not initial reactive by end of platelet shelf-life
2 packs September 2013 Staphylococcus aureus- not transfused
1 pack May 2014 Staphylococcus aureus- not transfused
Number of packs screened between Feb 2011 and Sept 2014

Numbers and type of organisms isolated on bacterial screening Jan-Dec 2013 (Apheresis)
0
10
20
30
40
50
60
70
GPRCNS
S. sacc
S. aur
eus
oral
strp
S. pne
u
oro-
phar
yn gut
envir
o
Bacterium
Nu
mb
ers
AphCP
AphIP
Numbers and type of organisms isolated on bacterial screening Jan -Dec 2013 (Pool)
0
5
10
15
20
25
GPRCNS
S. sacc
S. aur
eus
oral
strp
S. pne
u
oro-
phar
yn gut
envir
o
Bacterium
Nu
mb
er PoolCP
PoolIPMaximum growth time
Propionibacteria 138 hrs
S. aureus 12 hrs
S. pneumoniae 14 hrs
E. coli 10 hrs

Potential sources of contamination
DonorVenepuncture siteBloodstreamOral cavityGut
EnvironmentalSamplingComponent processing

Likely source of organisms
Skin
Failure of cleansing e.g. Staphylococcus aureus
Follicles/deeper layers anaerobes e.g. Propionibacteria
Transient bacteraemia
Gut e.g. E. coli, Streptococcus bovis
Oropharynx e.g. Streptococcus oralis, S. pneumoniae

Gut flora
Streptococcus bovis
Ca colon
non-malignant conditions of gut
E. coli
Part of normal microflora of the gut
Listeria monocytogenes
Pates, cheeses, poor outcome in immunosuppressed
? Carriage in healthy individuals

Near-missFirst known bacterial screening miss reported by NHSBT since screening began September 2013 Two apheresis platelet packs-one donorIssued to two separate hospitalsClumps observed in one packStaphylococcus aureus isolated from both packs

0
1
2
3
4
5
6
7
1996
-97
1997
-98
1998
-99
1999
-00
2000
-01
2000
-02 (
15 m
onth
s)20
0320
0420
0520
0620
0720
0820
0920
1020
11
Year of report
Nu
mb
er o
f In
cid
ents
Red Cells
Platelets
Confirmed TTIs platelets v red cells(SHOT report)

SaBTO review 2013
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/324354/SaBTO_platelets_report.pdf

Source: Public Health England

Summary
Risk of a TTI is smallDonor selection, testing and processing decrease the
riskNeed for vigilanceSuspected TTIs should be reported to NHSBTSurveillance informs current policies

Acknowledgments
NHSBT/HPA Epidemiology teamColleagues in Transfusion Microbiology