standard of practice in nephrology for pharmacy services · and hypertension, diabetes mellitus,...
TRANSCRIPT

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 1
Standard of practice in nephrology for pharmacy services 1
Michelle Nalder, BPharm(Hons), MClinPharm, MSHP 1, Carla Scuderi, BPharm, MClinPharm, MSHP 2,3, 2
Ronald Castelino, BPharm, MPharm, PhD, BCGP, MSHP 4, Matthew Cervelli, BPharm, MSHP 5,6, 3
Danielle Ironside, BPharm(Hons), GradCertClinPharm, MSHP 2, Ceridwen Jones, post nominals 7, Jess 4
Lloyd, BPharm, GDClinPharm, MSHP 8, Sanja Mirkov, B Pharm, PGDipPH, MSHP 9 and Courtney 5
Munro, BPharm, GradCertPharmPrac, MPharmPrac, MSHP, AACPA 10. 6
7
1 The Royal Melbourne Hospital, Parkville, Australia 8
2 Royal Brisbane and Women’s Hospital, suburb, Queensland 9
3 School of Pharmacy, University of Queensland, suburb, Queensland 10
4 Faculty of Health and Medicine, University of Sydney, NSW; Blacktown Hospital, WSLHD, NSW 11
5 Renal Unit, Royal Adelaide Hospital, Adelaide, Australia 12
6 13
7 14
8 The Princess Alexandra Hospital, Brisbane, Australia 15
9 Gisborne Hospital, Gisborne, New Zealand 16
10 The Society of Hospital Pharmacists of Australia, Collingwood, Victoria, Australia 17
18
Address for correspondence: 19
Carla Scuderi 2, Chair, Nephrology Leadership Committee, The Society of Hospital Pharmacists of 20
Australia, Collingwood, Victoria, Australia. Email: [email protected] 21
22
Preface 23
This Standard references and relies upon SHPA Standards of Practice for Clinical Pharmacy Services 1 24
as the foremost Standard. As kidney disease rarely occurs in isolation, this Standard may overlap with 25
others and depending on the area of specialty practice it may be advisable to refer to additional 26
Standards of Practice. 27
The use of the word ‘specialisation’ in this standard is in line with the National Competency Standards 28
Framework for Pharmacists in Australia 2 where ‘specialisation’ refers to the scope of practice rather 29
than the level of performance. ‘Specialisation’ of itself does not confer additional expertise. 30
This Standard is for professional practice and is not prepared or endorsed by Standards Australia. It is 31
not legally binding. 32
33
Introduction 34
In Australia, everyone shares a fundamental right to safe and high-quality healthcare. This is enshrined 35
in the Australian Charter of Healthcare Rights 3 by which all healthcare systems, including the provision 36
of advanced pharmacy care, must abide. The Charter summarises the basic rights that patients and 37
consumers are entitled to receive when accessing healthcare services including access, safety, respect, 38
communication, participation, privacy and comment. Additionally, Kidney Health Australia’s Charter 39

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 2
of Home Dialysis Rights and Responsibilities 4 provides guidance for patients, their carers and health 40
professionals who provide their care. The provision of pharmacy services must encompass both 41
Charters to deliver effective, efficient, timely and equitable patient-centred care for kidney disease. 42
The National Competency Standards Framework for Pharmacists in Australia 2 complements the 43
underpinnings of the Charter across five domains of competency for the pharmacy profession. These 44
include; professionalism and ethics, communication and collaboration, medicines management and 45
patient care, leadership and management, as well as education and research. 46
This Standard, produced by The Society of Hospital Pharmacists of Australia (SHPA), refers to both the 47
role of the pharmacy service and the pharmacists’ practice in nephrology (or kidney disease). It is 48
intended for both pharmacists involved in nephrology services and pharmacists whose area of 49
specialisation is nephrology services and for consistency refers to both as nephrology pharmacists. 50
The Standard predominately refers to nephrology pharmacists but does not intend to exclude suitably 51
qualified technicians where appropriate 1. SHPA supports both pharmacists and technicians to operate 52
at their full scope of practice in order to achieve optimal patient and pharmacy outcomes. 53
This Standard is intended to be used across hospital pharmacy services in Australia, irrespective of the 54
service type (public or private) or location (metropolitan, regional or rural). While this Standard is 55
intended for hospital pharmacy services, the principles and aspects of patient management discussed 56
herein can be applied to broader pharmacy services that provide nephrology care. It is acknowledged 57
that there are significant variations in pharmacy services that are dependent on: organisational 58
capacity, patient population, nephrology service and pharmacy department priorities, and the 59
availability and scope of practice of the nephrology pharmacist; all of which may influence the scope 60
of services. 61
The Standard describes current best care for the provision of nephrology pharmacy services (see Box 62
1) by nephrology pharmacists and the pharmacy department or employer. Essential services relate to 63
services that demonstrate the full scope of current pharmacy practice. Emerging services relate to 64
services that are innovative and future focused and are provided in addition to essential services. SHPA 65
encourages all pharmacy services to strive to provide emerging services wherever possible, in addition 66
to essential services. 67
68
DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 3
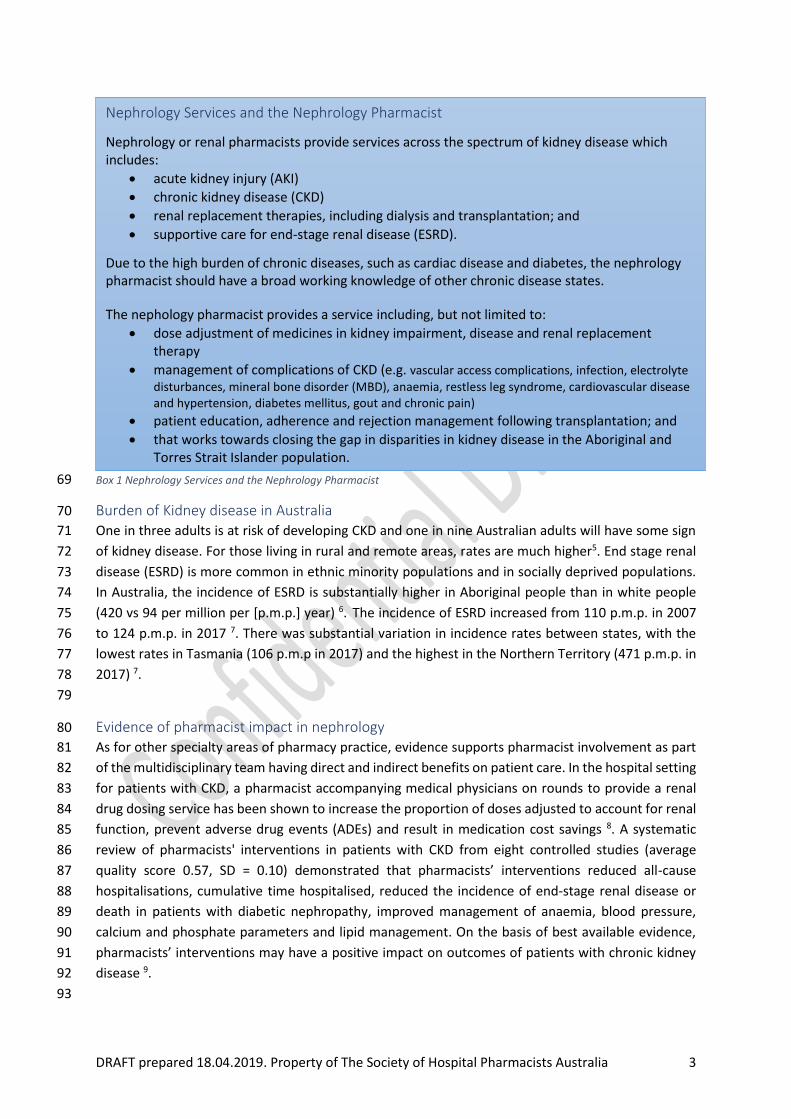
Box 1 Nephrology Services and the Nephrology Pharmacist 69
Burden of Kidney disease in Australia 70
One in three adults is at risk of developing CKD and one in nine Australian adults will have some sign 71
of kidney disease. For those living in rural and remote areas, rates are much higher5. End stage renal 72
disease (ESRD) is more common in ethnic minority populations and in socially deprived populations. 73
In Australia, the incidence of ESRD is substantially higher in Aboriginal people than in white people 74
(420 vs 94 per million per [p.m.p.] year) 6. The incidence of ESRD increased from 110 p.m.p. in 2007 75
to 124 p.m.p. in 2017 7. There was substantial variation in incidence rates between states, with the 76
lowest rates in Tasmania (106 p.m.p in 2017) and the highest in the Northern Territory (471 p.m.p. in 77
2017) 7. 78
79
Evidence of pharmacist impact in nephrology 80
As for other specialty areas of pharmacy practice, evidence supports pharmacist involvement as part 81
of the multidisciplinary team having direct and indirect benefits on patient care. In the hospital setting 82
for patients with CKD, a pharmacist accompanying medical physicians on rounds to provide a renal 83
drug dosing service has been shown to increase the proportion of doses adjusted to account for renal 84
function, prevent adverse drug events (ADEs) and result in medication cost savings 8. A systematic 85
review of pharmacists' interventions in patients with CKD from eight controlled studies (average 86
quality score 0.57, SD = 0.10) demonstrated that pharmacists’ interventions reduced all-cause 87
hospitalisations, cumulative time hospitalised, reduced the incidence of end-stage renal disease or 88
death in patients with diabetic nephropathy, improved management of anaemia, blood pressure, 89
calcium and phosphate parameters and lipid management. On the basis of best available evidence, 90
pharmacists’ interventions may have a positive impact on outcomes of patients with chronic kidney 91
disease 9. 92
93
Nephrology Services and the Nephrology Pharmacist
Nephrology or renal pharmacists provide services across the spectrum of kidney disease which includes:
• acute kidney injury (AKI)
• chronic kidney disease (CKD)
• renal replacement therapies, including dialysis and transplantation; and
• supportive care for end-stage renal disease (ESRD).
Due to the high burden of chronic diseases, such as cardiac disease and diabetes, the nephrology pharmacist should have a broad working knowledge of other chronic disease states.
The nephology pharmacist provides a service including, but not limited to:
• dose adjustment of medicines in kidney impairment, disease and renal replacement therapy
• management of complications of CKD (e.g. vascular access complications, infection, electrolyte
disturbances, mineral bone disorder (MBD), anaemia, restless leg syndrome, cardiovascular disease and hypertension, diabetes mellitus, gout and chronic pain)
• patient education, adherence and rejection management following transplantation; and
• that works towards closing the gap in disparities in kidney disease in the Aboriginal and Torres Strait Islander population.

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 4
Objectives of the Service 94
The objectives of the nephrology service provided by pharmacists are to: optimise medicines 95
management for patients with kidney disease by assessment of renal function and appropriate 96
medicines recommendations to prevent acute kidney injury (AKI), slow progression of CKD, improve a 97
patient’s quality of life while limiting unintended consequences such as adverse drug events, 98
advancement of disease stage, burden of kidney disease and costs. Nephrology pharmacists must 99
deliver the service as part of a multidisciplinary collaboration and within the framework of evidence 100
and patient-centred healthcare ensuring optimal kidney health and patient outcomes. Where possible 101
pharmaceutical care for patients with kidney disease should be standardised to minimise variation 102
and provide equitable services, with lesser dependence on locality. 103
104
Scope 105
This Standard applies to all pharmacists working in nephrology services. The service provided by the 106
nephrology pharmacist may be delivered across several settings including both public and private 107
hospitals, in an inpatient, outpatient or ambulatory care setting, and in primary care (at patient's 108
home, Aboriginal and Torres Strait Islander health centres, community clinics). 109
In addition to providing Clinical Pharmacy services as outlined in SHPA Standards of Practice for Clinical 110
Pharmacy Services 1, nephrology pharmacists are expected to provide services relevant to their clinical 111
area and scope of practice. Whilst the range of services provided in nephrology is primarily delivered 112
by pharmacists, it may be supported by pharmacy technicians in clinical and non-clinical roles. 113
The role of the nephrology pharmacist should include: 114
• attendance on ward rounds, in outpatient consultations, at multi-disciplinary team meetings 115
and at individual patient case conferences 116
• delivery of pharmacy services that improve patient medication outcomes and adds value to 117
healthcare systems, while encouraging the financial sustainability of healthcare 118
• development of and input into policies, procedures, guidelines and resources 119
• comment on nephrology medication formulary applications and decisions 120
• provision of educational and training for healthcare professionals and students 121
• quality improvement activities; 122
• and research related to nephrology. 123
It may additionally include involvement in serving satellite centres, clinical trials and emerging 124
pharmacy services. The pharmacist should be a point of contact for other pharmacists and health 125
professionals, and for the hospital or health service for medicines enquiries related to nephrology. 126
127
Operation 128
The nephrology pharmacy service should be provided by pharmacists whose main area of 129
specialisation is nephrology and who demonstrates competence in nephrology pharmacy (refer to 130
Training and Education). Components of the service may be delegated to non-specialised 131
pharmacists after undergoing training and demonstrating an appropriate level of competence to 132
perform their tasks. 133

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 5
134
To achieve the aforementioned objectives, nephrology pharmacists need to consider both individual 135
patient factors and service provision with regard to practice settings, as detailed below. 136
Patient Factors 137
To meet the needs of the patient, the nephrology pharmacist (as part of the multidisciplinary 138
nephrology team) should: 139
• Be familiar with tools available to estimate a patient’s current kidney function and 140
understand both the applicability and limitations of these tools and the clinical situations 141
where they may be unreliable and/or misleading 142
• Consider individual patient circumstances including renal function, goals of therapy, clinical 143
presentation and comorbidities when evaluating and recommending medications 144
• Consider the impact of the varying renal replacement therapies (RRT) on medicine choice 145
and dosing along with the optimal timing of administration 146
• Understand patient risk factors for medication non-adherence for patients with renal 147
disease (including post-transplantation) and potential strategies to address these 148
• Understand risk factors for the development and progression of CKD and associated 149
comorbidities 10. 150
151
Service Provision with regard to Practice Settings 152
Service provision will vary with regard to practice setting. In the hospital setting, nephrology 153
pharmacists providing advanced pharmacy care can facilitate quality use of medicines to improve 154
outcomes for patients with kidney disease. Due to the large number of patients with kidney disease 155
and the treatment burden, the traditional inpatient model has expanded to include care for patients 156
in outpatient, ambulatory and clinic-based services. Progressively innovative services in atypical 157
settings are arising to accommodate patient need such as satellite dialysis units, Australia’s Big Red 158
Kidney Bus and GP shared care arrangements (like that for obstetrics). An ongoing challenge is 159
delivering regular nephrology pharmacy services in an outpatient setting since models of pharmacy 160
service are traditionally inpatient focused. Regardless of the setting, nephrology pharmacists have a 161
critical role in ensuring optimal kidney health. 162
Nephrology pharmacists should assess kidney function consistent with the role of a pharmacist in a 163
patient-centred and culturally responsive manner. A collaborative approach to develop a medication 164
management plan (MMP) should promote judicious use of medicine and engage patients, to convey 165
the benefits of evidence-based treatment options and establish realistic expectations. The nephrology 166
pharmacist should refer patients to services (e.g. nurse practitioner, case managers, dieticians, social 167
workers, psychologists, palliative care, credentialed advancing and advanced practice pharmacists, 168
HMR accredited pharmacists and medical staff including general practitioners) that could assist and 169
support self-care for kidney disease and escalate to the co-ordinator of the patient's medical care 170
when required. 171
Nephrology pharmacists should facilitate communication between the hospital and primary care and 172
provide education to patients. In keeping with best practice for facilitating continuity of medication 173
management on transition between care settings, there should be robust communication systems 1. 174

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 6
As detailed in the introduction, this Standard describes best care for the provision of pharmacy 175
services with essential services that relate to services that demonstrate the full scope of pharmacy 176
practice and emerging services that are innovative and future focused and are provided in addition to 177
essential services. Table 1 lists examples of services regarding practice setting and service: 178
179
DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 7
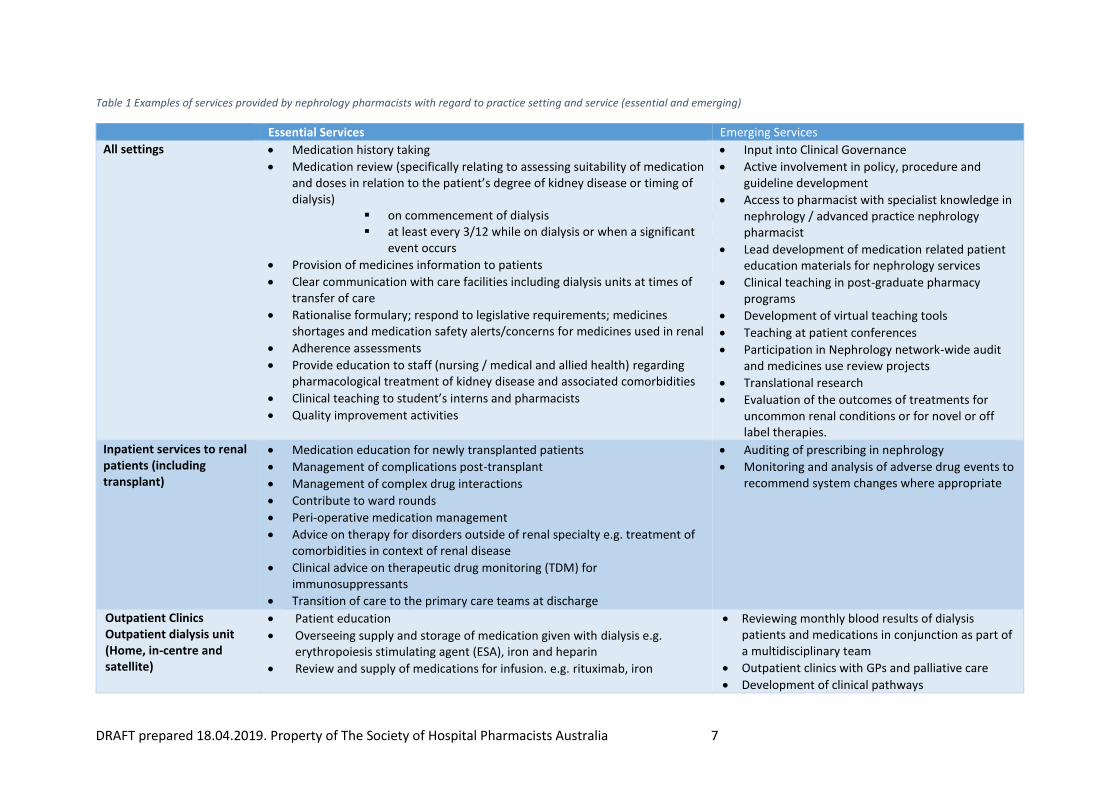
Table 1 Examples of services provided by nephrology pharmacists with regard to practice setting and service (essential and emerging)
Essential Services Emerging Services
All settings • Medication history taking
• Medication review (specifically relating to assessing suitability of medication and doses in relation to the patient’s degree of kidney disease or timing of dialysis)
▪ on commencement of dialysis ▪ at least every 3/12 while on dialysis or when a significant
event occurs
• Provision of medicines information to patients
• Clear communication with care facilities including dialysis units at times of transfer of care
• Rationalise formulary; respond to legislative requirements; medicines shortages and medication safety alerts/concerns for medicines used in renal
• Adherence assessments
• Provide education to staff (nursing / medical and allied health) regarding pharmacological treatment of kidney disease and associated comorbidities
• Clinical teaching to student’s interns and pharmacists
• Quality improvement activities
• Input into Clinical Governance
• Active involvement in policy, procedure and guideline development
• Access to pharmacist with specialist knowledge in nephrology / advanced practice nephrology pharmacist
• Lead development of medication related patient education materials for nephrology services
• Clinical teaching in post-graduate pharmacy programs
• Development of virtual teaching tools
• Teaching at patient conferences
• Participation in Nephrology network-wide audit and medicines use review projects
• Translational research
• Evaluation of the outcomes of treatments for uncommon renal conditions or for novel or off label therapies.
Inpatient services to renal patients (including transplant)
• Medication education for newly transplanted patients
• Management of complications post-transplant
• Management of complex drug interactions
• Contribute to ward rounds
• Peri-operative medication management
• Advice on therapy for disorders outside of renal specialty e.g. treatment of comorbidities in context of renal disease
• Clinical advice on therapeutic drug monitoring (TDM) for immunosuppressants
• Transition of care to the primary care teams at discharge
• Auditing of prescribing in nephrology
• Monitoring and analysis of adverse drug events to recommend system changes where appropriate
Outpatient Clinics Outpatient dialysis unit (Home, in-centre and satellite)
• Patient education
• Overseeing supply and storage of medication given with dialysis e.g. erythropoiesis stimulating agent (ESA), iron and heparin
• Review and supply of medications for infusion. e.g. rituximab, iron
• Reviewing monthly blood results of dialysis patients and medications in conjunction as part of a multidisciplinary team
• Outpatient clinics with GPs and palliative care
• Development of clinical pathways

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 8
Outpatient -other (i.e. infusions etc)
• Telehealth medication review follow up for remote /rural patients

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 9
Policies, Procedures and Governance 181
Pharmacists must have knowledge of the following documents which provide a framework within 182
which they must practice: 183
• Australian Charter of Healthcare Rights 3 184
• National Safety and Quality Health Service Standards 11 185
• Pharmacy Board of Australia Code of Conduct 12 186
• SHPA Code of Ethics 13 187
• National Competency Standards Framework for Pharmacists in Australia 2 188
• Professional Practice Standards 14 189
• Relevant legislation specifically State and Territory Acts and Regulations 190
Policies for the practice of clinical pharmacy provide a basis upon which nephrology specific policies 191
may be developed and applied. 192
Additional policies, procedures, guidelines and registries that nephrology pharmacists should be 193
familiar with include: 194
• Kidney Health Australia – Caring for Australasians with Kidney Disease (KHA – CARI) 195
• Kidney disease: Improving Global Outcomes (KDIGO) Guidelines 196
• Chronic Kidney Disease Management in General Practice 3rd Ed 2015 197
• International Society of Peritoneal Dialysis Guidelines – 198
o ISPD Peritonitis Recommendations: 2016 Update on Prevention and Treatment of 199
Peritonitis 2016 200
o ISPD Catheter-Related Infection Recommendations: 2017 Update 201
o ISPD Position Statement on Reducing the Risks of Peritoneal Dialysis-Related 202
Infections 203
• Kidney Disease Outcomes Quality Initiative 204
• International Society of Nephrology Clinical Guidelines 205
• ANZDATA Australia & New Zealand Dialysis and Transplant Registry 206
• Dialysis Outcomes and Practice Patterns Study 207
208
Local, institutional and state-based policies guiding practice may include consultation and/or 209
ownership by other professions or by the pharmacy department and should cover: 210
• Acute hypertension 211
• Anticoagulation for haemodialysis circuits including anticoagulation in the setting of heparin 212
induced thrombocytopenia 213
• Locking solutions for venous catheters for dialysis 214
• Blocked lines e.g. alteplase or urokinase administered via venous catheter (or vas cath) 215
• Calciphylaxis including use and adverse effects of sodium thiosulfate 216
• Prevention of Contrast Induced Nephropathy (CIN) 217
• Empiric and directed treatment of peritonitis 218
• Prevention and management of PD exit site infections 219
• Pharmacological management of acute hyperkalaemia 220
• Pharmacological management of anaemia in renal disease 221

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 10
• Prophylactic antibiotics pre-colonoscopy and invasive gynaecologic procedures in patients 222
on peritoneal dialysis 223
• Medications requiring substantial dose adjustment in renal disease such as aminoglycosides 224
and vancomycin 225
• Treatment of bacteraemia in patients on haemodialysis 226
• Vaccination pre-dialysis including hepatitis B, influenza and pneumococcal disease 227
• Medications used for kidney transplantation and management of complications after 228
transplant (e.g. acute rejection, BK, CMV, bone disease) 229
• Advice on dosing and monitoring of chemotherapy and immunological therapy. 230
231
Recommended Staffing 232
As per the Clinical Pharmacy Standards 1 there are three major factors driving staffing levels for clinical 233
pharmacy services including: the range of clinical pharmacy services, the complexity of care required, 234
and hospital throughput. Recommended nephrology pharmacist staffing levels for pharmacy services 235
are presented in Table 2 andTable 3 and should be interpreted with consideration of the health 236
service, activities performed by the nephrology pharmacist, and those that are undertaken by other 237
pharmacists and pharmacy technicians. 238
The roles of nephrology pharmacists are varied and dependent on the model of care and size of the 239
health service and recommended staffing levels is, therefore, a reflection of this. Whereas the 240
traditional model has been that ward-based pharmacists are wholly responsible for an individual 241
patient, pharmacists are increasingly practicing in team-based models and with specialisation, 242
consultant-type roles. As the models change and roles grow, provision of advanced pharmacy care for 243
an individual patient may be shared between pharmacists. 244
There should be at least one pharmacist responsible for the coordination of all aspects of the 245
nephrology pharmacy service. Staffing ratios should consider dedicated time for the lead nephrology 246
pharmacist to perform these coordination duties. 247
Table 2 Recommended pharmacist staffing levels for provision of clinical pharmacy services based on ‘overnight beds’. 248 Adapted from Table 9.1 Staffing Levels and Structure for the Provision of Clinical Pharmacy Services 1. 249
Category Service-related group / bed
type
Beds to 1 FTEi pharmacist for
clinical pharmacy services 5
days / weekii
1
Specialist units, high
dependence on medicines
Renal Medicine,
Transplantation
15
Consideration should be given to adjustment of this ratio for sites who manage a high number of 250
patients following acute renal transplantation (refer to Appendix H, TSANZ 15). 251
i FTE = full-time equivalent. ii Service on a weekend (assuming few admissions and discharges and medication chart review only) would require an additional 2 to 2.5 hours per day.

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 11
Table 3 Recommended pharmacist staffing levels for provision of clinical pharmacy services based on the number of 252 patients per day. Adapted from Table 9.2 Staffing Levels and Structure for the Provision of Clinical Pharmacy Services 1. 253
Category Patient/service type No. of patients to 1 FTE
pharmacist for clinical
pharmacy services per dayiii
9
Review and advice on
medicine usage – ambulatory
Pharmacists providing review
and advice on medicine usage
in Allied Health and/or Clinical
Nurse Specialist Interventions
clinics – Tier 2 Non-admitted
Service 40.04
5
10
Review and advice on
medicine usage – outreach
services
Pharmacists providing review
and advice on medicine usage
in Allied Health and/or Clinical
Nurse Specialist Interventions
clinics – Tier 2 Non-admitted
Service 40.04 as an outreach
service or in the patient’s
home
3
254
Owing to increasing demand there have been changes in the operation of dialysis units, increasing 255
sessions provided over a seven-day week and a push towards home-based therapies. In recognition 256
of the changing model of care provision the LC recommends ratios based on actual patient numbers 257
as opposed to bed numbers or day admissions as follows: 258
• For outpatient haemodialysis patientsiv: a ratio of 200 patients to 1 FTE pharmacist (not 259
eligible for Tier 2 funding) 260
• For nephrology outpatient clinics (category 12), a ratio of 5-7 patients to 1 FTE pharmacist 261
per day (eligible for Tier 2 funding). 262
Further to these ratios, it is recommended that support is provided for pharmacist to travel to 263
satellite centres and for home visits. 264
265
Training and Education 266
It is essential to develop the pharmacy workforce enabling delivery of advanced pharmacy care in 267
nephrology through training and education of pharmacists and technicians. Nephrology pharmacists 268
should have a scope of practice competency profile with a Continuing Professional Development (CPD) 269
plan that covers the five domains of professional performance as per the National Competency 270
Standards Framework for Pharmacists in Australia 2016 2. Whilst the framework itself is not tied to 271
any area of specialisation, for nephrology pharmacists there are qualifications, educational activities, 272
knowledge and skills that are recommended in addition to those of a clinical pharmacist. These have 273
been informed by the SHPA Nephrology Leadership Committee. 274
iii Includes services on weekdays and weekends. iv Described previously in Clinical Pharmacy Standards 1 as category 11 same day admission, renal dialysis.

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 12
In addition, pharmacists and pharmacy technicians commencing practice in nephrology services must 275
undertake a relevant orientation and training program as determined by the health service. This 276
should include credentialing relative to their role as implemented by local or state-based health 277
service. 278
Nephrology pharmacists must contribute to the education and development of procedures for non-279
specialist pharmacists caring for nephrology patients. 280
Credentialing and Qualificationsv 281
Desirable certification, credentialing and qualifications for nephrology pharmacists include: 282
• a postgraduate qualification in clinical pharmacy or public health e.g. 283
o Master of Clinical Pharmacy 284
o Master of Public Health 285
• credentialing as an Advancing or Advanced Practice Pharmacist is provided by Pharmacy 286
Development Australia 16 287
• other relevant postgraduate degrees which may be available nationally or 288
internationally. Examples include: 289
o Postgraduate Diploma in Renal Medicine currently offered by University of 290
South Wales. 291
Educational Activities 292
Further to the Pharmacy Board of Australia Guidelines on Continuing Professional Development 17 it 293
is recommended that nephrology pharmacists have a significant proportion of their continuing 294
professional development per year tailored to nephrology services. There is a dearth of specific 295
pharmacist training for nephrology however any training on chronic disease e.g. cardiac disease or 296
diabetes is worthwhile for nephrology pharmacists. Recommended continuing education for 297
nephrology pharmacists include the following; 298
Attendance at local or national courses: 299
• SHPA Seminars and related CPD activities e.g. extension seminar internal medicine, state 300
branch CEs or symposiums 301
• ANZSN Kidney School online educational website 302
• Virtual simulation on AKI ‘Ready to Practice’ 18 303
• General medicine/ chronic disease training e.g. NPS webinars and CPD activities for 304
pharmacists 305
• In house journal clubs 306
• Kidney Health Australia 307
International courses: 308
• ISN Academy Online Learning 309
• University College London (UCL) renal short courses 310
Joining professional organisations: 311
• Australian and New Zealand Society of Nephrology (ANZSN) 312
v This is a limited list offered for general information and does not represent endorsement of any provider; new providers may emerge, and this is list is current as of April 2019.

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 13
• Renal Society of Australasia (RSA) 313
• International Society of Nephrology (ISN) 314
• UK Renal Pharmacy Group (UKRPG) 315
The leadership committee consider the ability to undertake preceptorships and/or site visits to health 316
services in either geographically diverse areas or areas of diverse practise to be a useful way of 317
expanding knowledge and skills, particularly for those nephrology pharmacists practising alone or at 318
smaller sites. 319
Educational material and resources are provided on the SHPA Specialty Practice Nephrology stream 320
page on the SHPA eCPD website. For nephrology pharmacists, joining and actively participating in the 321
SHPA Specialty Practice Nephrology stream at the Practice Group level is strongly recommended. 322
Attendance at specialist conferences and educational meetings should be supported to maintain and 323
update specialist knowledge in nephrology. Relevant domestic conferences include those organised 324
by SHPA, the Australian and New Zealand Society of Nephrology (ANZSN) Annual Meeting, and the 325
Renal Society of Australasia (RSA). International conferences in conferences in nephrology include the 326
American Society of Nephrology (ASN) Kidney Week, International Society of Nephrology (ISN) World 327
Congress of Nephrology (WCN), and the European Society of Paediatric Nephrology (ESPN) Annual 328
Meeting. 329
Knowledge, Skills and Experiential Learning 330
The role of a nephrology pharmacist, like any clinician with specialised expertise, is based on a high 331
level of skill in general pharmacy with the later addition of specialty specific experience. Pharmacists’ 332
working in this area should have high levels of personable skills including confidence, empathy and 333
effective patient communication skills, in order to provide personalised care. Underpinning knowledge 334
related to key areas of pharmacy practice in nephrology are the skills and application of clinical 335
pharmacy, which may be advanced by experiential learning. This Standard does not list the 336
competencies that the individual nephrology pharmacist should address as this will be dependent 337
upon their scope of practice. 338
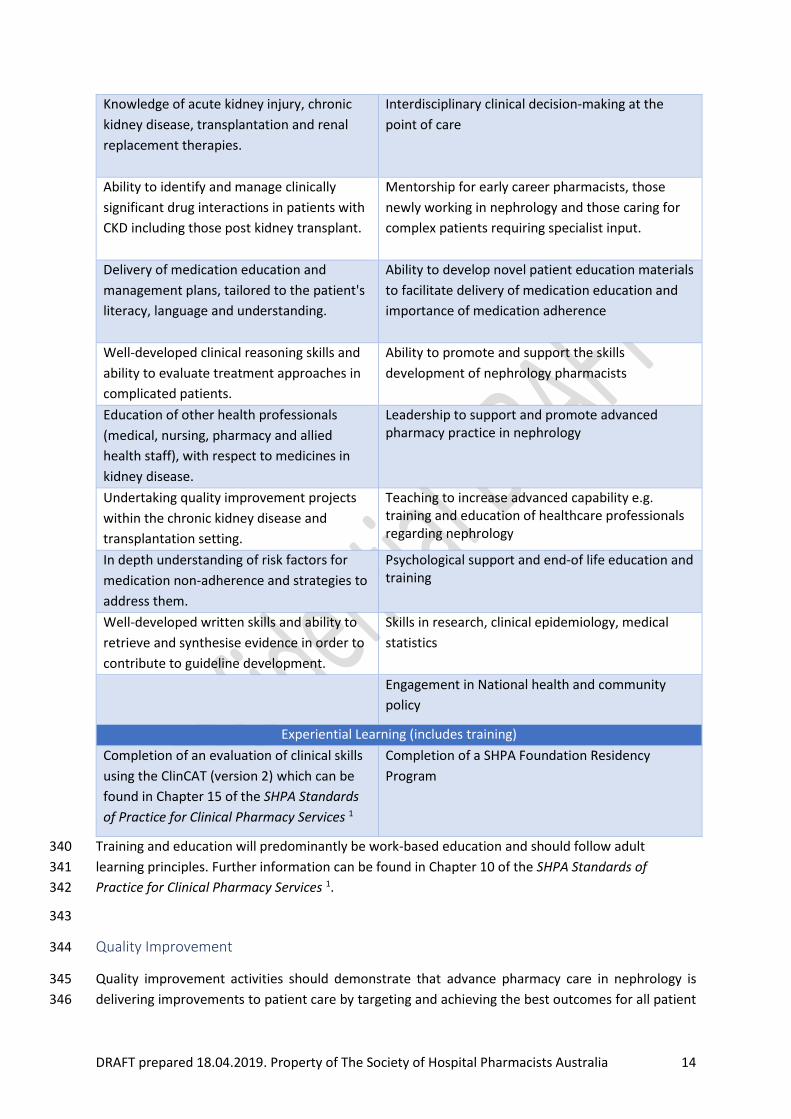
Table 4 Essential and desirable knowledge and skills and experiential learning for nephrology pharmacists 339
Knowledge and Skills
Essential Desirable
Understanding of the various equations and
method used to estimate kidney function
and the limitations associated with these
equations and methods.
Specialist knowledge of pharmacotherapeutics to
support comprehensive medicines use e.g. drug
dosing in CRRT, TDM post transplantation
Ability to identify medicines that need dose
adjustment in kidney disease and be able to
recommend appropriate dose adjustments
considering clinical picture and patient
characteristics.
Ability to select dose regimens for medicines in renal disease in the absence of published recommendations.
Understanding of drug removal by
haemodialysis and peritoneal dialysis and
implications for drug dosing.
Motivational interviewing to support changes in
medication adherence for transplant medications.
DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 14
Knowledge of acute kidney injury, chronic
kidney disease, transplantation and renal
replacement therapies.
Interdisciplinary clinical decision-making at the
point of care
Ability to identify and manage clinically
significant drug interactions in patients with
CKD including those post kidney transplant.
Mentorship for early career pharmacists, those
newly working in nephrology and those caring for
complex patients requiring specialist input.
Delivery of medication education and
management plans, tailored to the patient's
literacy, language and understanding.
Ability to develop novel patient education materials
to facilitate delivery of medication education and
importance of medication adherence
Well-developed clinical reasoning skills and
ability to evaluate treatment approaches in
complicated patients.
Ability to promote and support the skills
development of nephrology pharmacists
Education of other health professionals
(medical, nursing, pharmacy and allied
health staff), with respect to medicines in
kidney disease.
Leadership to support and promote advanced pharmacy practice in nephrology
Undertaking quality improvement projects
within the chronic kidney disease and
transplantation setting.
Teaching to increase advanced capability e.g. training and education of healthcare professionals regarding nephrology
In depth understanding of risk factors for
medication non-adherence and strategies to
address them.
Psychological support and end-of life education and training
Well-developed written skills and ability to
retrieve and synthesise evidence in order to
contribute to guideline development.
Skills in research, clinical epidemiology, medical
statistics
Engagement in National health and community
policy
Experiential Learning (includes training)
Completion of an evaluation of clinical skills
using the ClinCAT (version 2) which can be
found in Chapter 15 of the SHPA Standards
of Practice for Clinical Pharmacy Services 1
Completion of a SHPA Foundation Residency
Program
Training and education will predominantly be work-based education and should follow adult 340
learning principles. Further information can be found in Chapter 10 of the SHPA Standards of 341
Practice for Clinical Pharmacy Services 1. 342
343
Quality Improvement 344
Quality improvement activities should demonstrate that advance pharmacy care in nephrology is 345
delivering improvements to patient care by targeting and achieving the best outcomes for all patient 346

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 15
groups, including those at greatest risk for medicines. Examples of quality improvement activities 347
which may be considered within a plan, do, study, act (PDSA) cycle for quality improvement activities 348
are listed below: 349
• Assessment of practice against CARI guidelines e.g. iron management, preventing infection 350
in peritoneal dialysis, exit site infection avoidance 351
• Assisting nursing staff with accuracy of medicines data input into ANZDATA registry 352
• Evaluation of anaemia management 19,20 353
• Proportion of guidelines (e.g. PD, HD, kidney transplant) that have been reviewed and 354
updated within designated expiry period. 355
Further information on quality improvement can be found in Chapter 14 of the SHPA Standards of 356
Practice for Clinical Pharmacy Services 1 and ACSQHC Selected best practices and suggestions for 357
improvement for clinicians and health system managers hospital-acquired complication renal failure 358 21. 359
360
Research 361
Systematic reviews of randomised controlled trials (RCTs) are commonly used in evidence-based 362 policy making.22 However, the number of RCTs is fewer in nephrology than other specialties of internal 363 medicine and low in quality.23 Furthermore, public health systematic reviews of interventions are 364 much more likely to be evaluated using observational and other study designs - the best available 365 evidence wherever this may be found.24 366
Translational research in nephrology should include pharmacogenomics studies for renal kinetics, 367 pharmacokinetic studies on drug dosing in RRT, pharmacoepidemiology studies on drug use and 368 treatment outcomes in patients in CKD, dialysis and kidney transplantation, medication adherence 369 post kidney transplantation and evaluation of the outcomes of treatments for uncommon renal 370 conditions or for novel or off label therapies. 371
Consideration should be given to research priorities from the patient and carer’s perspective such as 372 those for chronic kidney disease published by CARI 25 e.g.’ what can we do to improve individual drug 373 therapy in terms of better management of side effects?’ and ‘what interventions can improve long 374 term post-transplant outcomes?’ 375
Research is vital for developing the pharmacy profession and may inform pharmacy services current 376 level of, and future contributions to, advancing pharmacy and patient care. Nephrology pharmacists 377 should initiate, conduct and supervise research that contributes to the body of knowledge providing 378 evidence of impact in support of optimal use of medicines and advanced pharmacy care in nephrology 379 as well as evaluating novel treatments and ensuring patient safety. Research Ethics Committee 380 approval should be sought where applicable. 381
Cross-sector, inter-sectoral and interdisciplinary research is advocated to ensure the input of key 382 stakeholders and that research is relevant to the Australian community. Medical teams external to 383 nephrology may be involved, depending on subject choice. Liaising with medical staff may identify 384 medicine-related aspects of existing nephrology projects. Students, pre-registration pharmacists or 385 doctors in training may assist with data collection. To improve the chance of project success, the data 386 collection should be achievable in a timely manner and the topic should be of interest to the 387 nephrology team. Collaborations with research institutes and groups such as the Australian Kidney 388 Trials Network (AKTN) and CKD-centre for research excellence are also advocated. 389

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 16
External funding enables larger and feasibly multi-centre studies to be conducted. The SHPA National 390 Translational Research Collaborative (NTRC) funds research grants, practitioner grants and 391 educational grants to develop research capacity. Grants are also available from other organisations 392 including Kidney Health Australia and the Australian and New Zealand Society of Nephrology. 393 Presentation and publication of studies by Australian pharmacists practicing in nephrology is 394 imperative, to aid others in the implementation of innovative and evidence-based nephrology 395 pharmacy services and illustrate where nephrology pharmacists are involved in research and how they 396 are improving patient care. 397
The choice of journal to publish in depends on consideration of the best audience for the study 398 results. The Journal of Pharmacy Practice and Research (JPPR) presents findings to primarily an 399 Australian pharmacy audience. Journals specific to nephrology that may be appropriate are listed in 400 Appendix 1: Resources. 401
Further information on research can be found in Chapter 11 of the SHPA Standards of Practice for 402 Clinical Pharmacy Services 1. 403
404
References 405
1. SHPA Committee of Specialty Practice in Clinical Pharmacy. SHPA Standards of Practice for 406 Clinical Pharmacy Services. Journal of Pharmacy Practice and Research 2013; 43(No. 2 407 Supplement): S1-69. 408
2. Pharmaceutical Society of Australia. National Competency Standards Framework for 409 Pharmacists in Australia. Deakin West ACT 2600; 2016. 410
3. The Australian Commission on Safety and Quality in Health Care. Australian Charter of 411 Healthcare Rights. 2008. 412
4. Home Dialysis Advisory Committee of Dialysis Nephrology and Transplant. The Australian 413 Charter of Home Dialysis Rights and Responsibilities. Australia; 2012. p. 2. 414
5. National Rural Health Alliance. Kidney disease in rural Australia. In: Australia KH, Inc. NRHA, 415 editors. Fact Sheet 35 ed. ACT: National Rural Health Alliance; 2013. 416
6. El Nahas M. The global challenge of chronic kidney disease. Kidney Int 2005; 68(6): 2918-29. 417 7. ANZDATA Registry. Chapter 1 Incidence of Renal Replacement Therapy for End Stage Kidney 418
Disease. Adelaide, Australia, 2018. 419 8. Hassan Y, Al-Ramahi RJ, Aziz NA, Ghazali R. Impact of a renal drug dosing service on dose 420
adjustment in hospitalized patients with chronic kidney disease. The Annals of 421 pharmacotherapy 2009; 43(10): 1598-605. 422
9. Salgado TM, Moles R, Benrimoj SI, Fernandez-Llimos F. Pharmacists' interventions in the 423 management of patients with chronic kidney disease: a systematic review. Nephrol Dial 424 Transplant 2012; 27(1): 276-92. 425
10. Raymond CB, Wazny LD, Sood AR. Standards of clinical practice for renal pharmacists. Can J 426 Hosp Pharm 2013; 66(6): 369-74. 427
11. Australian Commission on Safety and Quality in Health Care. National Safety and Quality 428 Health Service Standards. Medication Safety. Sydney: Australian Commission on Safety and 429 Quality in Health Care; 2017. p. 86. 430
12. Pharmacy Board of Australia. For Pharmacists Code of Conduct. March 2014 ed; 2014. 431 13. The Society of Hospital Pharmacists Australia. SHPA Code of Ethics. Governance. 432
Collingwood: The Society of Hospital Pharmacists of Australia; 2016. p. 1. 433 14. Pharmaceutical Society of Australia. Professional Practice Standards Version 5. Deakin West 434
ACT 2600.; 2017. p. 116. 435 15. The Transplantation Society of Australia and New Zealand. Clinical Guidelines for Organ 436
Transplantation from Deceased Donors, 2018. 437

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 17
16. Pharmacy Development Australia. Advancing Practice Background and Guiding Principles, 438 2018. 439
17. Pharmacy Board of Australia. Guidelines on Continuing Professional Development. 2015. 440 18. Martini N, Farmer K, Patil S, et al. Designing and Evaluating a Virtual Patient Simulation—The 441
Journey from Uniprofessional to Interprofessional Learning. Information 2019; 10(1). 442 19. Fishbane S, Spinowitz B. Update on Anemia in ESRD and Earlier Stages of CKD: Core 443
Curriculum 2018. Am J Kidney Dis 2018; 71(3): 423-35. 444 20. Bosch JP, Walters BA. Continuous quality improvement for a hemodialysis network. Contrib 445
Nephrol 2002; (137): 300-10. 446 21. Australian Commision on Safety and Quality in Health Care. Hospital-Acquired Complication 447
8 RENAL FAILURE, 2018. 448 22. Barton S. Which clinical studies provide the best evidence? The best RCT still trumps the best 449
observational study. British Medical Journal 2000; 321: 255-6. 450 23. Strippoli GF, Craig JC, Schena FP. The number, quality, and coverage of randomized 451
controlled trials in nephrology. J Am Soc Nephrol 2004; 15(2): 411-9. 452 24. Bambra C. Real world reviews: a beginner's guide to undertaking systematic reviews of 453
public health policy interventions. J Epidemiol Community Health 2011; 65(1): 14-9. 454 25. Tong A. Exploring Research Priorities in Chronic Kidney Disease. Centre for Kidney Research; 455
2014. p. 1. 456 26. Australian and New Zealand Society of Nephrology. ANZSN Renal Supportive Care Guidelines 457
2013. Nephrology 2013; 18: 54. 458 27. McCombie SP, Thyer I, Corcoran NM, et al. The conservative management of renal trauma: a 459
literature review and practical clinical guideline from Australia and New Zealand. BJU Int 460 2014; 114 Suppl 1: 13-21. 461
462

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 18
Appendices 463
Appendix 1: Resources 464
Recommended texts for nephrology
Renal Drug Database
Discretionary texts (at least one would be available in most nephrology departments)
Morlidge, Clare; Ashley, Caroline (2008) Introduction to Renal Therapeutics. Pharmaceutical Press
London. Available as eBook via EBSCOhost for SHPA members
American College of Physicians (2007) Drug Prescribing in Renal Failure. 5th Edition. ISBN:978-1-
930513-76-1
Seyffart G (2011) Seyffart’s Directory of Drug Dosage in Kidney Disease . Dustri-Verlag.
Useful journals specific to nephrology
American Journal of Nephrology
American Journal of Kidney Diseases
Kidney
Kidney Diseases
Kidney International
Kidney Research and Clinical Practice
BMC Nephrology
Case Reports in Nephrology
Clinical Nephrology
Current Opinion in Nephrology & Hypertension
European Medical Journal: Nephrology
International Journal of Nephrology
Journal of Nephrology
Journal of Pediatric Nephrology
Journal of the American Society of Nephrology (JASN)
Kidney International
Nature Reviews Nephrology (formerly Nature Clinical Practice Nephrology)
Nephrology
Nephrology, dialysis, transplantation
Seminars in Nephrology
American Journal of Transplantation
Peritoneal Dialysis International
Transplantation
Clinical Guidelines
• KHA-CARI Guidelines e.g. KHA-CARI Chronic Kidney Disease Guidelines, KHA-CARI Dialysis
Guidelines, KHA-CARI Transplantation Guidelines
• KDIGO Guidelines e.g. Acute Kidney Injury (AKI), Anemia in CKD, Blood Pressure in CKD,
CKD Evaluation and Management
• ANZSN Renal Supportive Care Guidelines 2013 26
• Conservative Management of Renal Trauma 2014 27
Useful websites

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 19
Kidney Health Australia Patient information, GP practice guide,
professional information
National Kidney Foundation US based health organisation focussed on kidney
disease. Publishes resources for health
professionals and patients.
ANZData Statistics relating to the outcomes of treatment
for end stage renal failure
Global Kidney Health Atlas Global report on kidney disease in all countries
BC Renal Agency Multidisciplinary collective, focused on improving
care for the kidney community in British
Columbia
Think Kidneys UK program dedicated to raising awareness
about kidney disease. Includes resources for
health professionals and patients.
Conservative Kidney Management (CKM) Care A resource for patients and healthcare
professionals with a focus on quality of life,
symptom management, and living well without
dialysis.
Societies
International Society of Nephrology
Renal Society of Australasia
UK Renal Pharmacist Group
Useful Apps
eGFR Calculators National Kidney Foundation
Transplant Hero
CKD Go KHA
My Kidneys My Health – KHA
465
466

DRAFT prepared 18.04.2019. Property of The Society of Hospital Pharmacists Australia 20
Appendix 2: Common Abbreviations in Nephrology 467
Abbreviation Description
AKI Acute Kidney Injury
ANCA Anti-neutrophil cytoplasmic antibody
APD Automated Peritoneal Dialysis
AVF Arteriovenous Fistula
CARI Caring for Australians with Renal Impairment
CKD Chronic Kidney Disease
CKD -MBD Mineral Bone Disorder
CrCl Creatinine Clearance
CVVH Continuous Veno-Venous Hemofiltration
CVVHDF Continuous Veno-Venous Hemodiafiltration
eGFR Estimated Glomerular Filtration Rate
ESRD End Stage Renal Disease
HD Haemodialysis
HHD Home Haemodialysis
HUS Haemolytic Uraemic Syndrome
KDIGO Kidney Disease Improving Global Outcomes
KHA Kidney Health Australia
MDRD Modification of Diet in Renal Disease
MDT Multidisciplinary Team
NKF KDOQI The National Kidney Foundation Kidney Disease
Outcomes Quality Initiative (KDOQI)
PD Peritoneal dialysis
RRT Renal Replacement Therapy
TMA Thrombotic Microangiopathy
468