st catherine’s hospice primary thromboprophylaxis in advanced disease mj johnson
TRANSCRIPT

ST CATHERINE’SHOSPICE
Primary thromboprophylaxis in
advanced diseaseMJ Johnson
(The Mail on Sunday, 17/12/2000) 2

3

(The Sunday Telegraph, 28/1/2001)4

5
Daily Mail3/2/01
6

7
Background
• VTE : important cause of death in cancer patients • Potentially preventable with appropriate risk assessment
and prophylaxis• Therefore a healthcare priority for many countries• Some (e.g. UK) using financial incentives and targets to
drive implementation • International guidelines:
Farge D, Debourdeau P, Beckers M, Baglin C, Bauersachs RM, Brenner B, et al. International clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. J Thromb Haemost 2013 Jan;11(1):56-70.
What about palliative care?• Clinical relevance and research focus very recent in
palliative care• Moderate to high risk of VTE
– Advanced/active disease– Received ++ therapies (chemo/surgery)– Poorly mobile
• Secondary prevention is much more accepted• Still divided opinion about primary prevention
– Agreement not for those imminently dying
• But – hospice care now not just for the imminently dying
Things have changed• Hospice is no longer “the Death House”• But
– Only 7% SPC units have TP guidelines (Noble 2007)
– Not perceived as “a big problem” by clinicians– Outcome measures in studies not appropriate– Studies don’t include our patients– “A big PE is a nice way to go” (Noble 2008)
• However, difficult to keep being an ostrich…
10

11
Why prevent VTE in palliative care patients?
• High risk – Up to 50% in hospice in patients
• VTE confers a poor prognosis• Cause symptoms
– Attributable and non attributable• Challenging to treat
– Bleeding– Recurrent thrombosis– Six months of LMWH
(Noble et al Lancet Oncology 2008)

Current state of play
12
• Majority of palliative care patients admitted through medical take…
• …will be receiving PTP by default
• Some admitted to the hospice……
• ….won’t get PTP when they could benefit
Hospice VTE risk assessment project
• The utility of risk assessment tools in patients with advanced disease, and prediction of symptomatic VTE is unknown.
• Investigation: i)what is the relationship between risk of VTE and development of symptoms and, ii)what is the utility of risk assessment tools for these patients?
Method
• Retrospective consecutive admission case-note data from seven UK hospices
• Data collected during an evaluation of a VTE risk assessment protocol – Pan Birmingham Cancer Network palliative-modified
Thromboembolic Risk Factors (THRIFT) Consensus Group criteria,
– presence/absence of a temporary elevated risk (TER) of VTE.
• Symptoms/signs during admission consistent with possible VTE were documented.
Analysis plan• An exploration of the association of THRIFT, TER with
– prescription of PTP,– development of symptoms
• An estimation of the utility of THRIFT and TER in predicting symptomatic VTE during their hospice admission: – sensitivity, specificity, – predictive value (PPV and NPV), – likelihood ratios (LR(+/-)) – odds ratios
• Tests were 2-sided using a significance level of 5%, odds ratios and accuracy measures such as sensitivity are presented with 95% confidence intervals.

results• Total population: N=1164• 45 (4%) prescription of PTP on admission; (68
came on PTP; 13 of these continued; 32 new prescription)
• “Clinically relevant population” : N = 528 (45%)– The population who would have been eligible to have
PTP with LMWH– Excludes
• Contraindication to anticoagulation (bleeding, dying, thrombocytopenic) N= 496
• Already on therapeutic anticoagulation N = 139
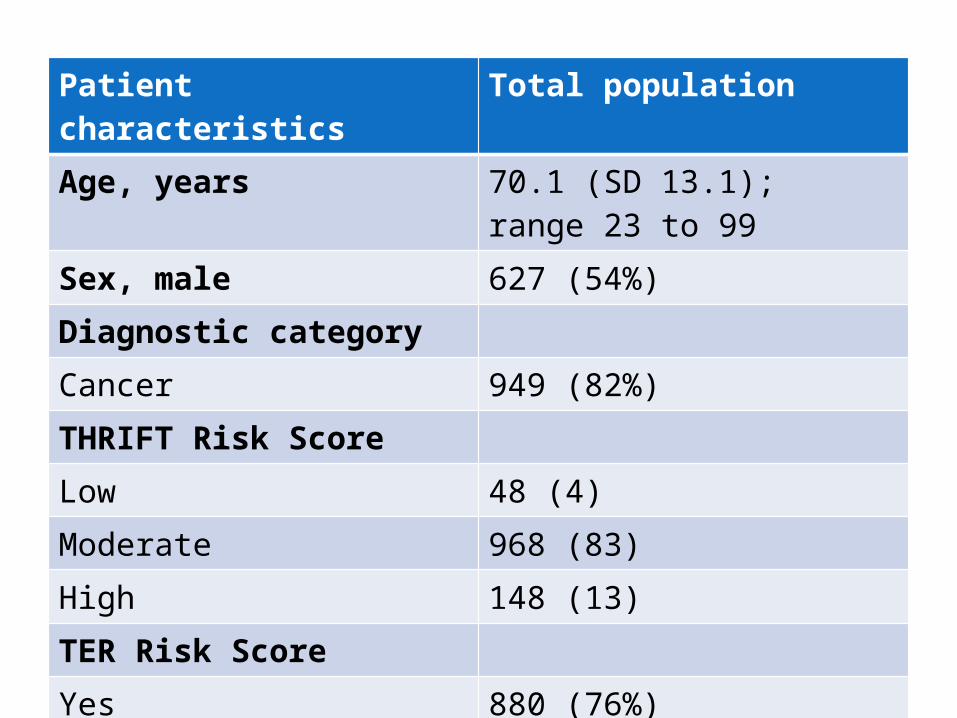
Patient characteristics Total populationAge, years 70.1 (SD 13.1); range 23 to 99 Sex, male 627 (54%)Diagnostic categoryCancer 949 (82%)THRIFT Risk Score Low 48 (4)Moderate 968 (83)High 148 (13)TER Risk ScoreYes 880 (76%)No 279 (24%)missing 5 (0%)
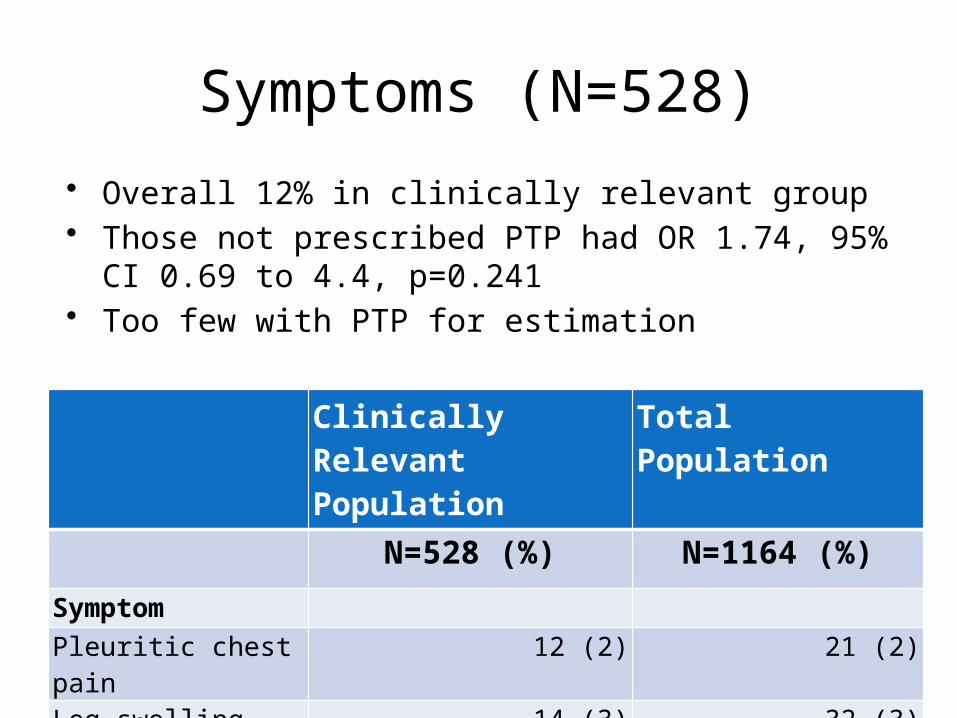
Symptoms (N=528)
Clinically Relevant Population
Total Population
N=528 (%) N=1164 (%)
Symptom
Pleuritic chest pain 12 (2) 21 (2)
Leg swelling 14 (3) 32 (3)Breathlessness 47 (9) 99 (9)
• Overall 12% in clinically relevant group• Those not prescribed PTP had OR 1.74, 95% CI 0.69 to
4.4, p=0.241• Too few with PTP for estimation
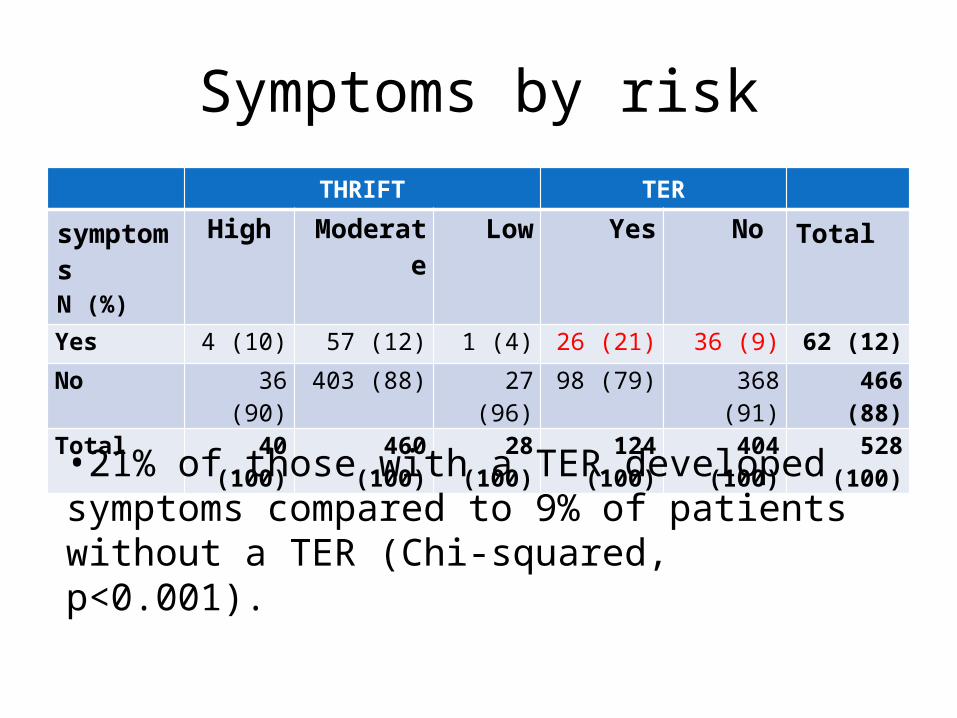
Symptoms by riskTHRIFT TER
symptomsN (%)
High Moderate Low Yes No Total
Yes 4 (10) 57 (12) 1 (4) 26 (21) 36 (9) 62 (12)
No 36 (90) 403 (88) 27 (96) 98 (79) 368 (91) 466 (88)
Total 40 (100) 460 (100) 28 (100) 124 (100) 404 (100) 528 (100)
•21% of those with a TER developed symptoms compared to 9% of patients without a TER (Chi-squared, p<0.001).
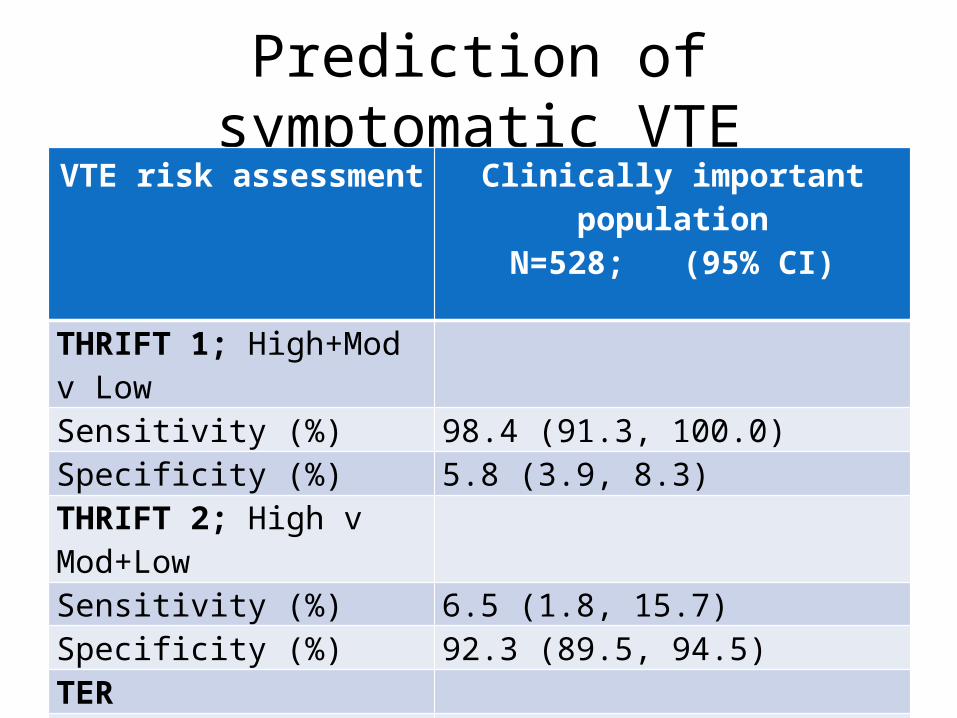
Prediction of symptomatic VTEVTE risk assessment Clinically important
populationN=528; (95% CI)
THRIFT 1; High+Mod v Low Sensitivity (%) 98.4 (91.3, 100.0)Specificity (%) 5.8 (3.9, 8.3)THRIFT 2; High v Mod+LowSensitivity (%) 6.5 (1.8, 15.7)Specificity (%) 92.3 (89.5, 94.5)TERSensitivity (%) 41.9 (29.5, 55.2)Specificity (%) 79.0 (75.0, 82.6)
Limitations
• Symptoms not routinely investigated with imaging - proxy measure
• Number caused by confirmed VTE events not known• Severity not systematically documented
– But significant enough to the patient and doctor to document in the clinical record.
• Retrospective chart review– symptoms were not systematically sought for, graded or
documented – Therefore likely to be an underestimate.
Conclusions 1: Does risk matter?
• Most patients admitted to these hospices were at moderate to high risk of developing VTE during their stay.
• Does this matter?
• There is a highly significant association between
TER and “proxy” symptoms in those who could have PTP

Conclusions 2: what should we do about it?
• Use TER rather than THRIFT for hospice patients on admission
• But…• Unknown whether PTP improves outcome • Unknown what effect symptoms have on QoL
• Therefore consider PTP in those at risk and discuss with patient