spondylosis, facet joint arthropathy and pain cme/friday/c5 1630 borowczyk.pdfand why enquire about...
TRANSCRIPT
Spondylosis, Facet Joint Arthropathy and Pain
Jim Borowczyk Department of Orthopaedics and Musculoskeletal Medicine
Christchurch School of Medicine University of Otago
Do ‘Age Related’ Changes in the Spinal Column
Cause or Contribute to Chronic Pain?
And why enquire about this?
Major insurance agencies worldwide covering work and other accident related injury often use the presence of ‘spondylosis’ and ‘facet joint arthropathy’, as seen on imaging, to decline further cover for a particular incident
This often occurs without warning in a setting in which the patient felt an inherent security in the system or process that was expected to provide for his medical rehabilitation, and protection of income while injured
Question Is this a justifiable stance? Yes or No?
GPCME South 2010 - Spondylosis and Pain 4
Questions requiring answers . . .
What is the true prevalence of spinal spondylosis and altered zygapophysial (facet joint) morphology?
What is its relation to increasing age?
How much do these changes contribute to spinal pain syndromes?
GPCME South 2010 - Spondylosis and Pain 5

Spondylosis - Definitions
GPCME South 2010 - Spondylosis and Pain
‘Spondylosis is a process whereby the morphology of the vertebral bodies change,
with the production of marginal osteophytes at the superior and inferior bodies’
‘One cardinal feature of spondylosis is said to
be the development of vertebral body osteophytes’ Bogduk, 1997 (1)
6
Spondylosis - Definition
GPCME South 2010 - Spondylosis and Pain
‘Spondylosis is a term referring to degenerative osteoarthritis of the joints
between the centra of the spinal vertebrae and or neural foraminae. In this condition
the interfacetal joints are not involved’
(Wikipedia – the online encyclopaedia)
7
Age Changes in the Spinal
Column
The ‘Wear and Tear’ of Life
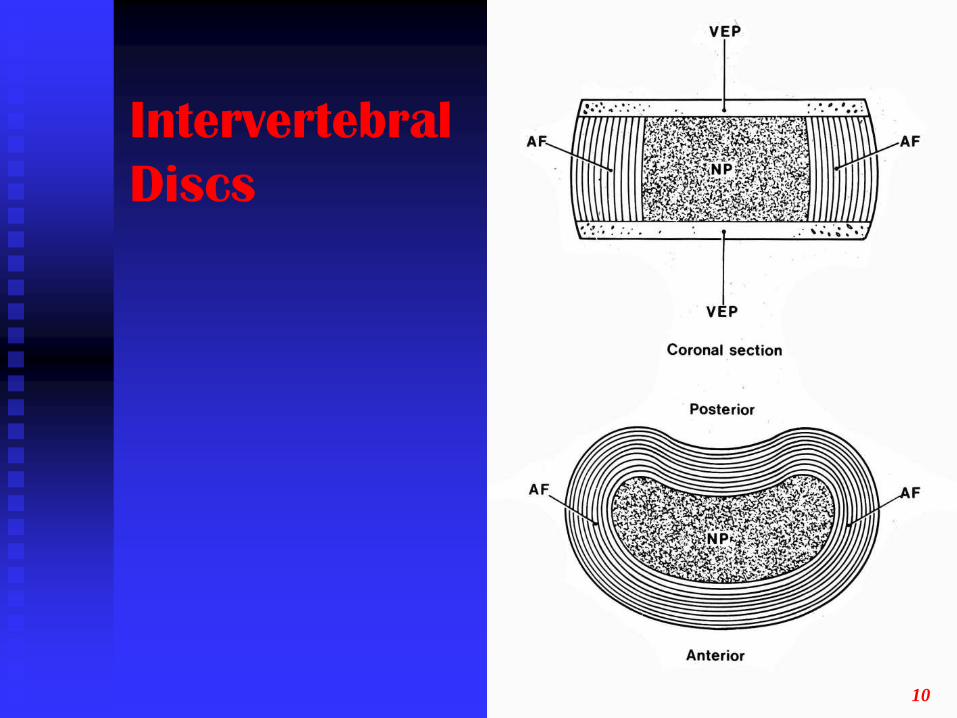
Intervertebral
Discs
10
The Ageing Disc
Reduced proteoglycan synthesis (65% by dry weight > 30% as early adulthood > age 60)
Reduction in proteoglycan size
Ratio of chondroitin/keratin drops
This decreases water binding capacity
Number of viable chondrocytes decreases with increasing evidence of necrosis
GPCME South 2010 - Spondylosis and Pain 11
The End Result . . .
The end result is that with increasing age the discs become drier with an increase in collagen density and become more fibrous and less resilient
GPCME South 2010 - Spondylosis and Pain 12

MRI
Imaging
Normal
Sagittal
T2
GPCME South 2010 - Spondylosis and Pain 13
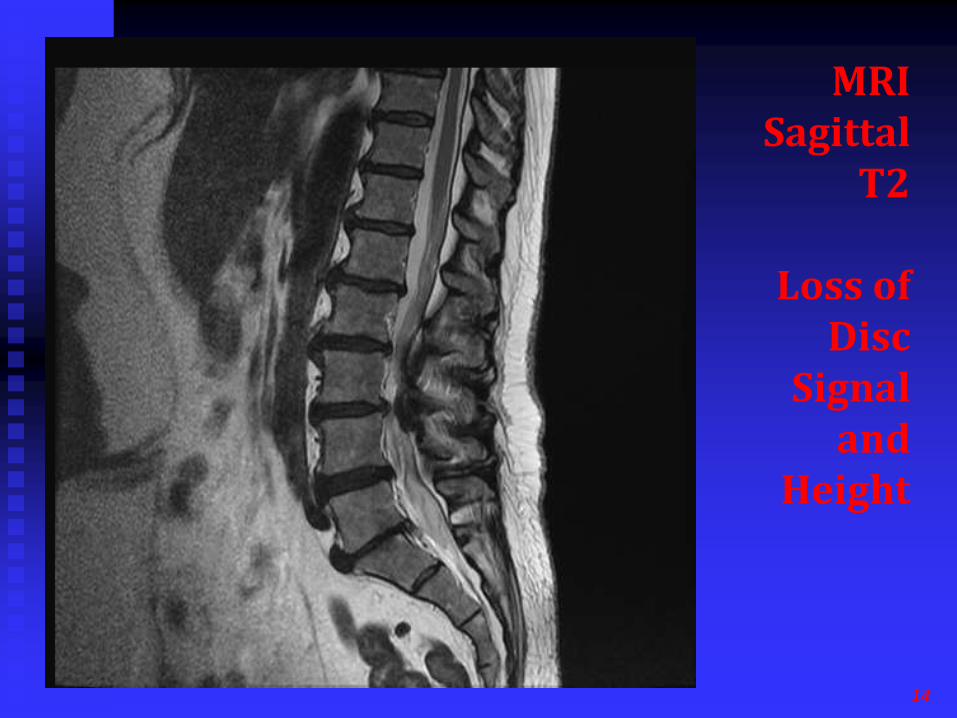
MRI Sagittal
T2
Loss of Disc
Signal and
Height
14
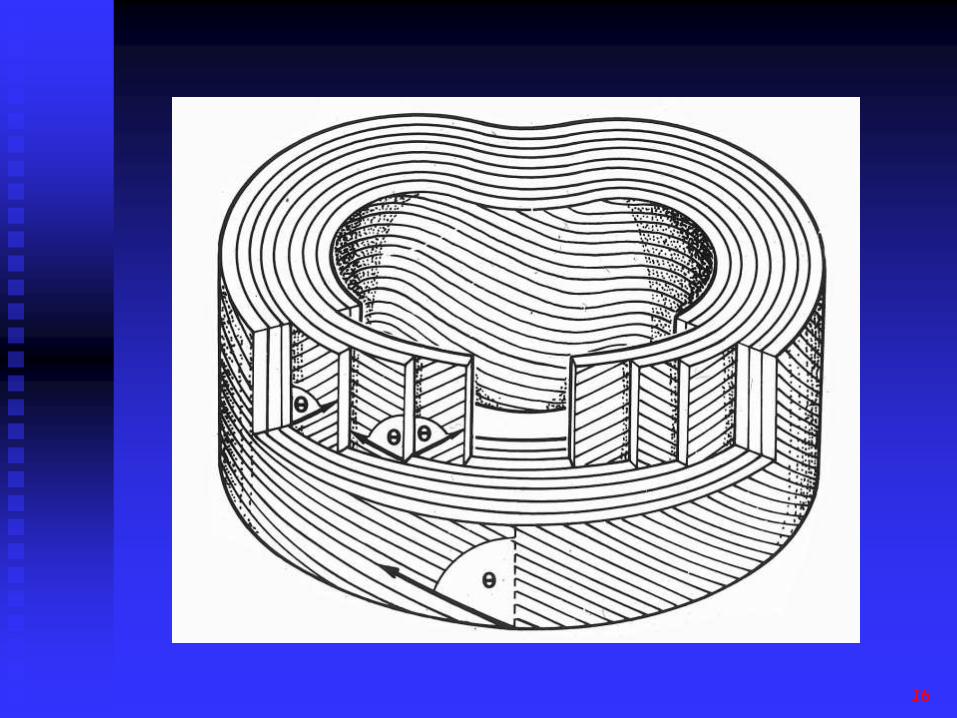
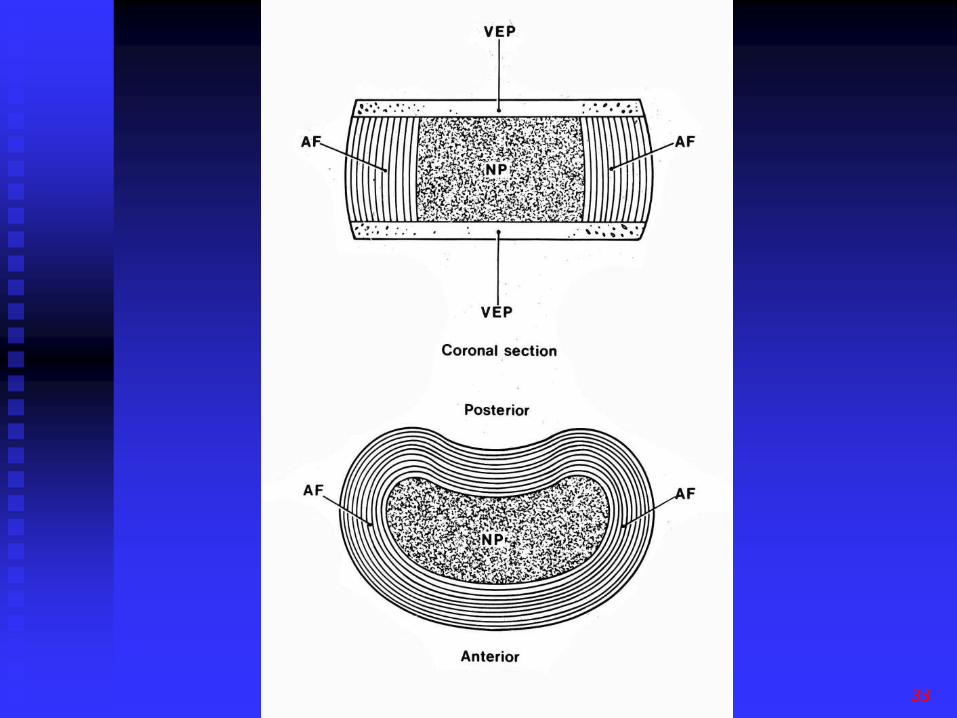
Anulus fibrosis
As the nucleus dries more load is borne by the anulus
The lamellae of the anulus become thickened and fibrillated
Cracks cavities and fissures may develop in the anulus
Intervertebral disc height and diameter tend to increase with age
GPCME South 2010 - Spondylosis and Pain 15
16

17
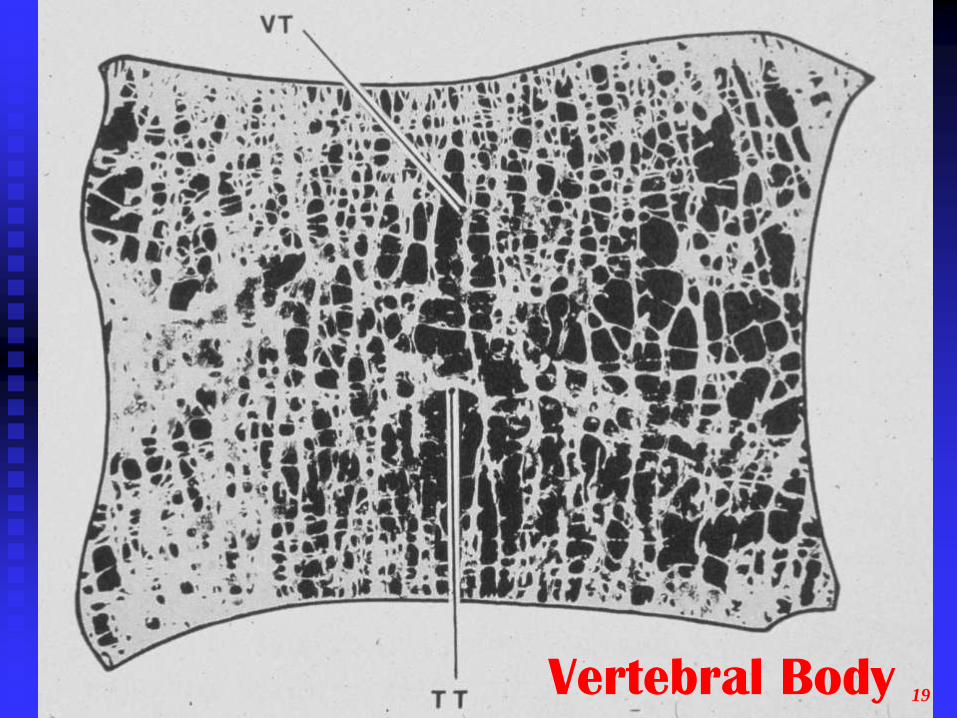
Vertebral Body
Bone density decreases with age
There is a relative loss of horizontal trabeculae
This reduces the load bearing capacity of the vertical trabeculae and, greater load is borne by the cortical bone of the vertebra
Cortical bone is more prone to failing under deformation than trabecular bone so that the vertebral body is more liable to deformation
Osteophytes occur at the bony margins
GPCME South 2010 - Spondylosis and Pain 18
GPCME South 2010 - Spondylosis and Pain Vertebral Body 19
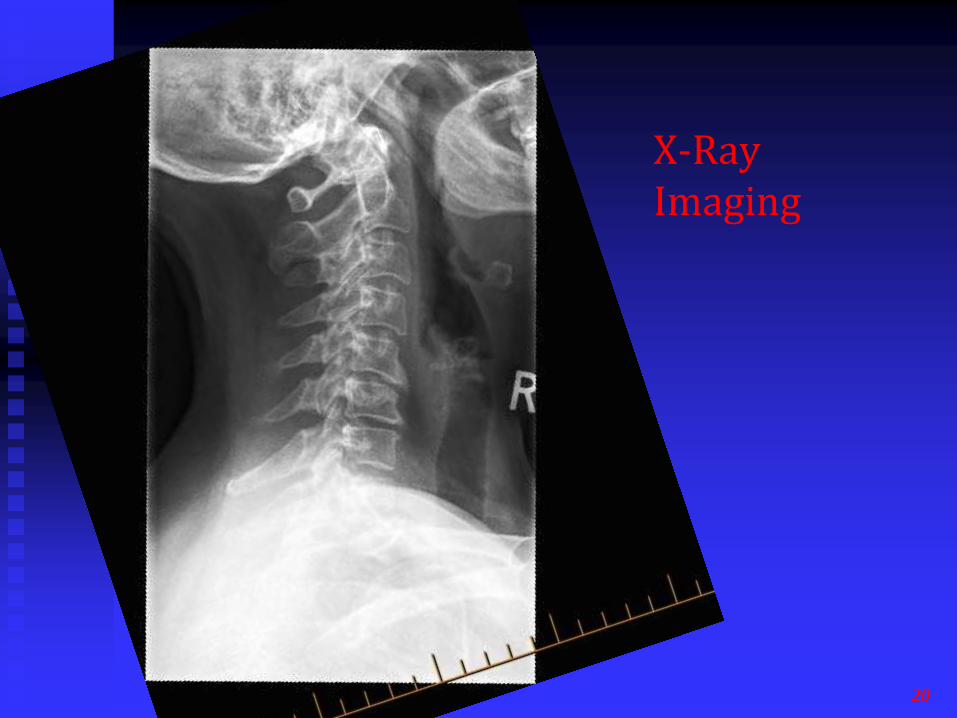
X-Ray Imaging
20
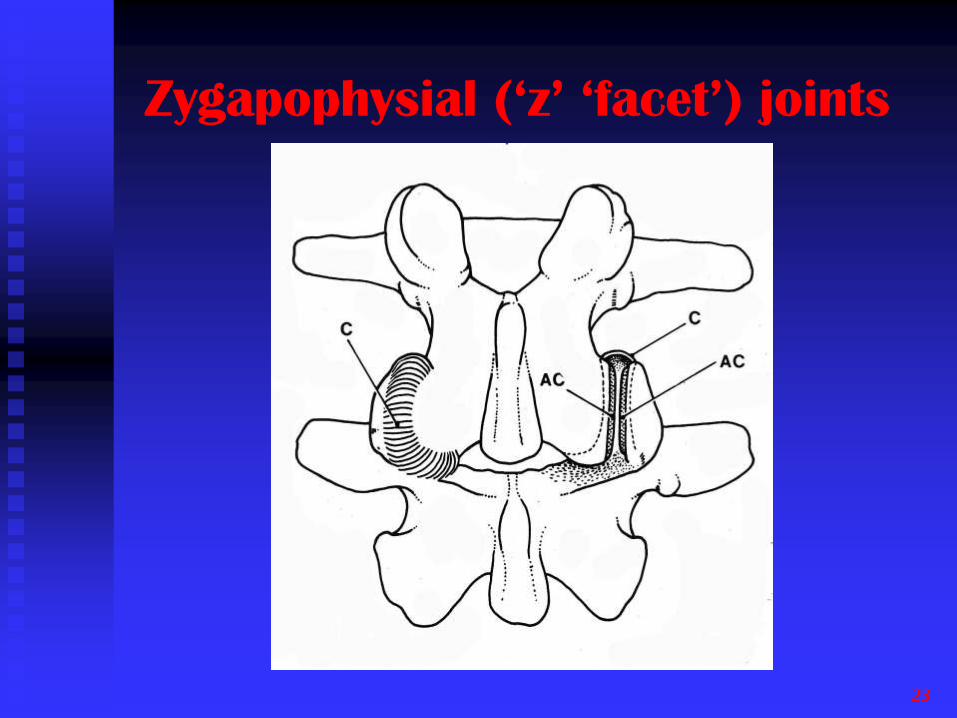
Zygapophysial (‘z’ ‘facet’) joints
23
‘Z’ Joint Arthropathy
The subchondral bone gradually increase in thickness with age
Cartilage fibrillation occurs from repeated stresses of daily living with erosion and focal thinning of the cartilage
Osteophytes develop at the attachment sites of the joint capsule and the ligamentum flavum hypertrophies
There may be excess intra-articular fluid
GPCME South 2010 - Spondylosis and Pain 24

MRI Imaging
Normal
Axial
25

26
GPCME South 2010 - Spondylosis and Pain
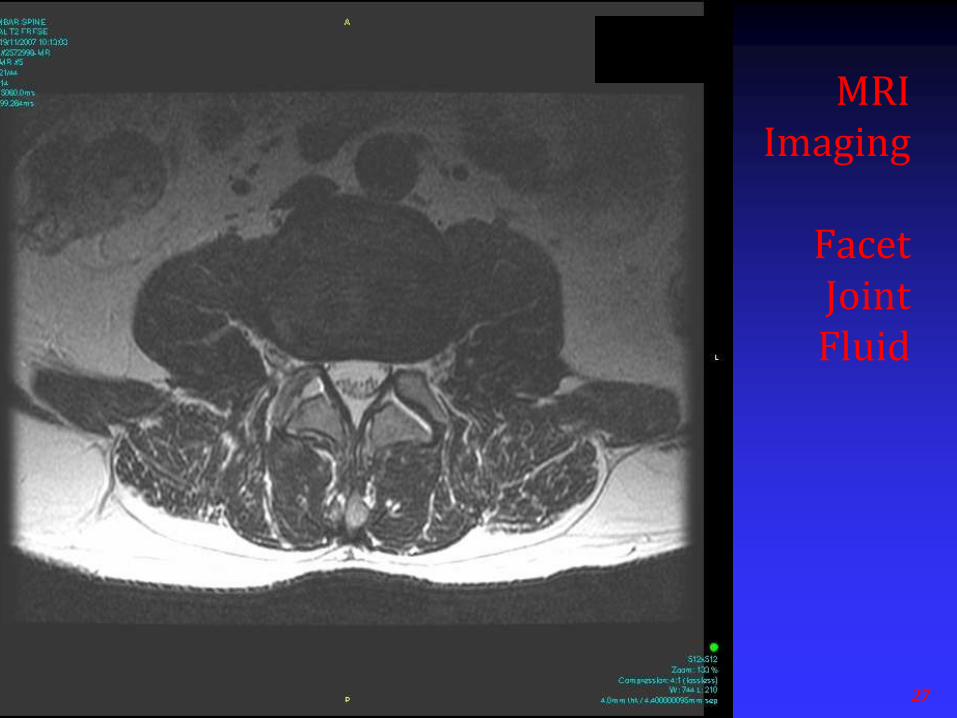
MRI Imaging
Facet Joint Fluid
27

So What Are the Real
Causes of
Spinal Pain?
What Does Cause Spinal Pain?
Any tissue in the spinal column, with the exception of an intact nucleus pulposus may cause pain
These tissues include: Intervertebral discs – nucleus and anulus
Facet joints
Vertebral bodies
Muscle, ligament and tendon
Nerves and dorsal root ganglia
GPCME South 2010 - Spondylosis and Pain 30
3 main sources are . . .
Discs up to 40% Schwarzer, 1995 (2)
Facet joints 15 – 40% Schwarzer, 1994 (3)
In a study of 438 patients with presumed facet joint pain: Cervical – 39%
Thoracic – 34%
Lumbar – 27% Manchukonda,2007 (4)
Lumbar facets 33 – 42% Manchikanti, 2008 (5)
And for low back, the SIJ (15%) Schwarzer 1995 (6)
GPCME South 2010 - Spondylosis and Pain 31
Discogenic Pain
Spondylosis per se is not a cause
The pathogenesis of discogenic pain is internal disc disruption
This is a process that is first initiated by microfracture of the endplates
GPCME South 2010 - Spondylosis and Pain 32
33

Vertebral end-plates
Each end-plate is a layer of cartilage 1 mm thick. In infancy the vertebral end-plate is part of the growth plate of the vertebral body
By age 20 the end-plate is gradually sealed of from the vertebral body
With age the end-plate becomes thinner with increasing cell death
GPCME South 2010 - Spondylosis and Pain 34

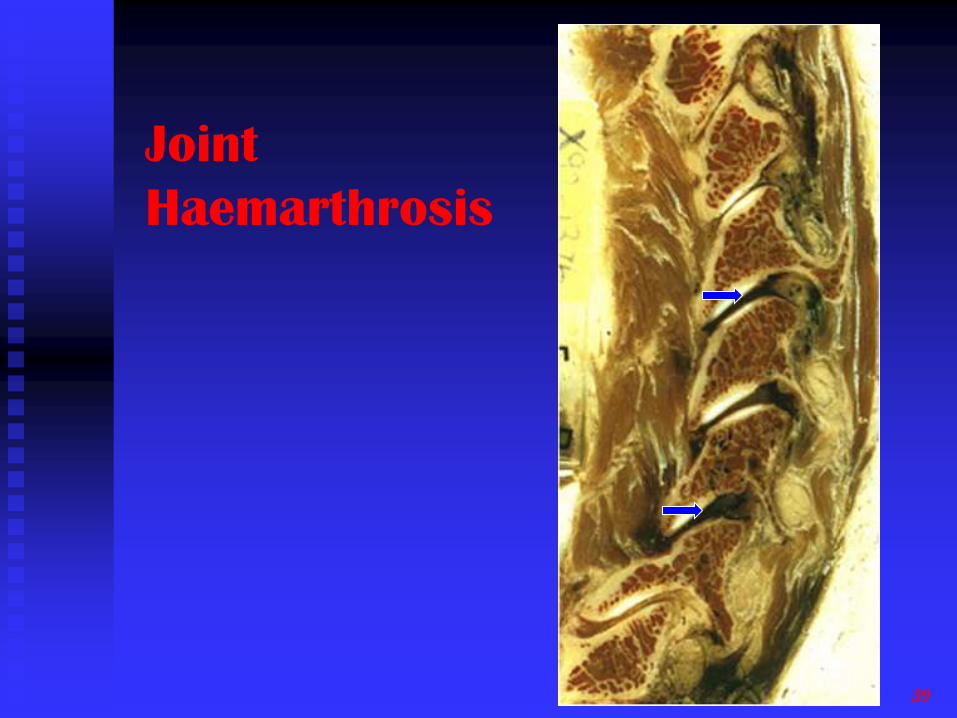
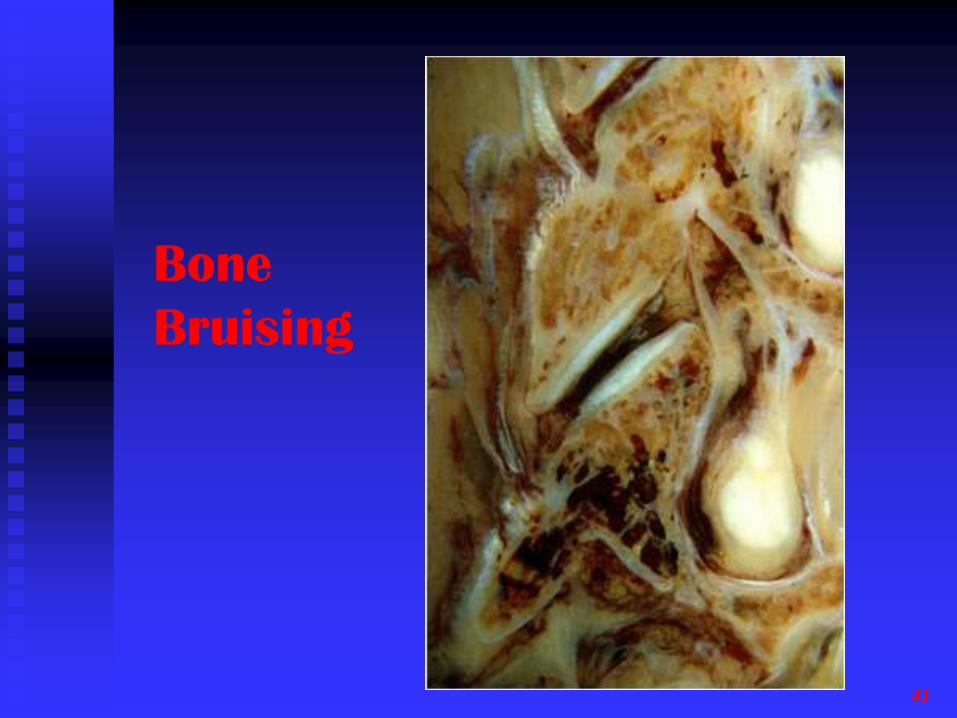
Facet Joint Pain
When facet joints are injured (MVA) the non radiological pathology includes:
Joint capsule stretching and tearing
Gouging , tears, splits and partial loss of the articular cartilage
Damage to the surface layers of the underlying subchondral bone – infraction
Small undisplaced fractures of facet tips
GPCME South 2010 - Spondylosis and Pain 38
39
Joint
Haemarthrosis
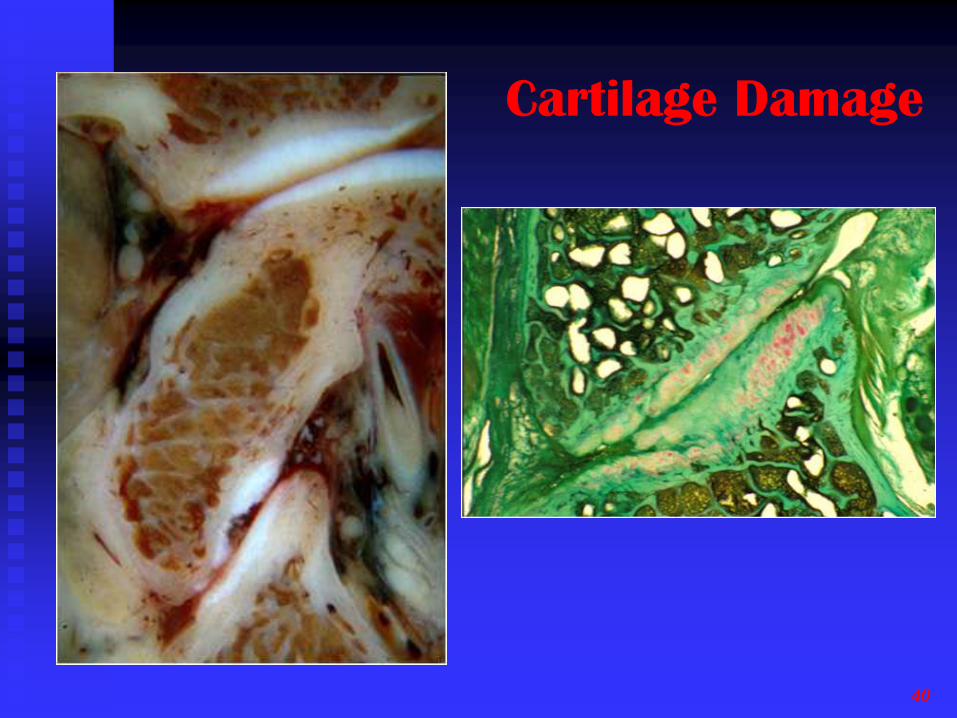
Cartilage Damage
40
41
Bone
Bruising

Fracture
Facet Joint
Tip
42

However . . .
Whilst these tissues are frequently the cause of spinal pain, there is no reason to suspect that there is any particular relationship to spondylosis and altered facet joint anatomy changes that occur with age
For example, in patients with whiplash, particularly in younger patients, imaging commonly shows no abnormality
GPCME South 2010 - Spondylosis and Pain 43
Prevalence of Spondylosis
GPCME South 2010 - Spondylosis and Pain 45
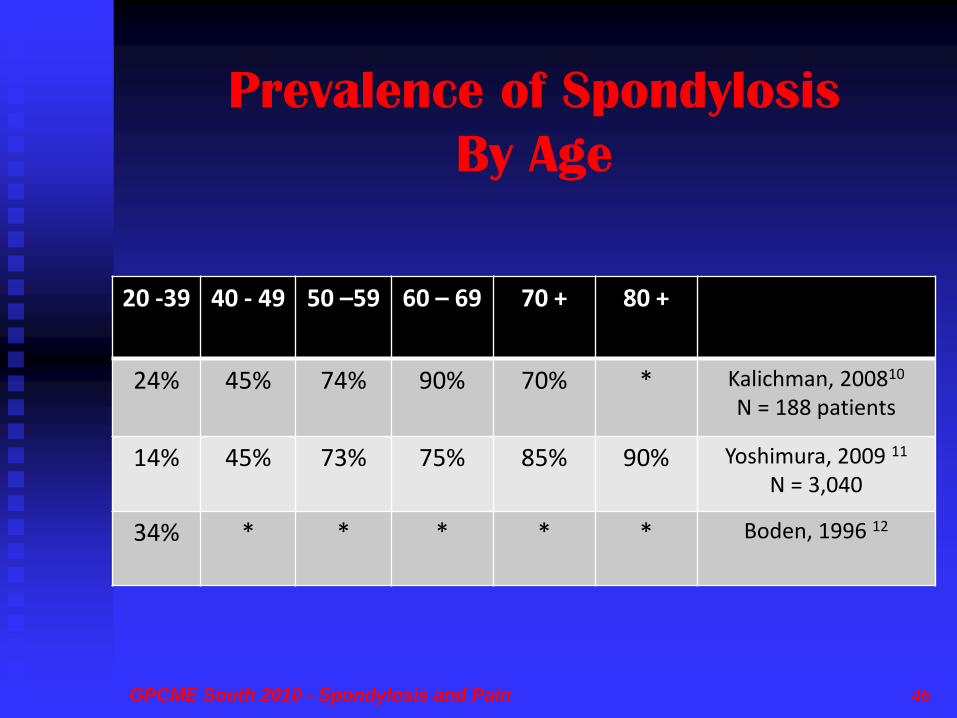
Prevalence of Spondylosis
By Age
20 -39 40 - 49 50 –59 60 – 69 70 + 80 +
24% 45% 74% 90% 70% * Kalichman, 200810
N = 188 patients
14% 45% 73% 75% 85% 90% Yoshimura, 2009 11
N = 3,040
34% * * * * * Boden, 1996 12
GPCME South 2010 - Spondylosis and Pain 46
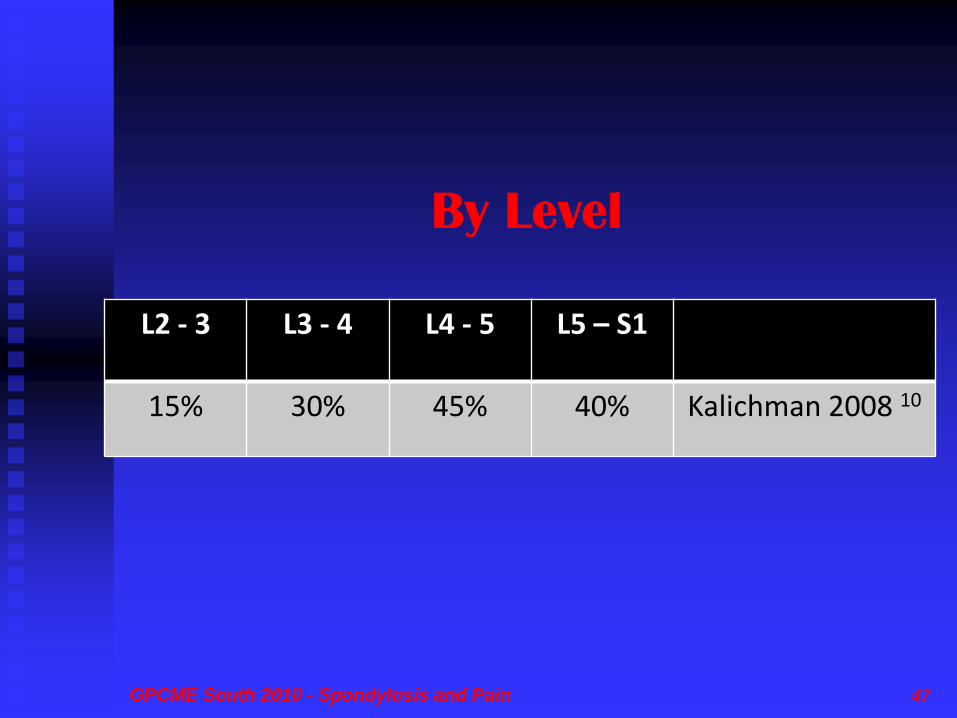
By Level
L2 - 3 L3 - 4 L4 - 5 L5 – S1
15% 30% 45% 40% Kalichman 2008 10
GPCME South 2010 - Spondylosis and Pain 47
And, as we get older . . .
Two hundred twenty-three subjects who underwent MRI 10 years ago, underwent another MRI, neurologic examination, and questionnaire survey regarding symptoms related to cervical spine and life style. Progression of degeneration of cervical spine on MRI was frequently observed during 10-year period. No factor related to progression of degeneration of cervical spine was identified except for age.
(Okada, E., et al., Aging of the cervical spine in healthy volunteers: a 10-year longitudinal magnetic resonance imaging study. Spine, 2009. 34(7): p. 706-12. 27)
GPCME South 2010 - Spondylosis and Pain 48

So Does Spondylosis
and Arthropathy cause
Spinal Pain?
The Medical Literature
For the Affirmative
Class IV evidence . . .
‘Low back pain is responsive to therapies that are effective for osteoarthritis in other locations. Osteoarthritis of the lumbar spine does cause low back pain’. Patients who do not have osteoarthritis of the facet joints on magnetic resonance scan do not have back pain’ (Borenstein 2004 13)
‘When mechanical factors are prominent, the condition is often referred to as “cervical spondylosis,” although the term is often applied to all non-specific neck pain. Mechanical and degenerative factors are more likely to be present in chronic neck pain.’ (Binder 2007 14)
GPCME South 2010 - Spondylosis and Pain 50

For the Negative
For the Negative . . .
Studies have highlighted the fact that a simple relationship of structural abnormalities to low back pain is impossible because similar alterations can be found in symptomatic as well as in asymptomatic individuals (Boos, 1998 19)
GPCME South 2010 - Spondylosis and Pain 52
Since the 1960’s . . .
The relationship between degenerative changes seen on imaging and back pain has been questioned . . .
Lawrence 1966 (15)
Biering-Sorensen, 1985 (16)
Frymoyer 1984 (17)
GPCME South 2010 - Spondylosis and Pain 53
As for imaging . . .
With normal X-ray the documented reliability of reporting for facet joint disease is poor, with kappa scores ranging from 0.2 to 0.3 (Coste 1991)
Although some diagnoses related to low back pain were quite consistently evaluated, the substantial disagreement on many findings should alert clinicians and radiologists against overestimating the validity and usefulness of the examinations (Espeland 1998 28)
GPCME South 2010 - Spondylosis and Pain 54
There is a weak correlation between back pain and spondylosis on plain films. The data have poor sensitivity, poor specificity, and only generate likelihood ratios (LR) of a little over 1 (Bogduk 2002 18)
Plain X-ray lacks validity, and with some exception, generates Likelihood Ratios seldom better than 1.5 (Bogduk 200218)
GPCME South 2010 - Spondylosis and Pain 55
van Tulder, M.W., et al., Spinal radiographic findings and nonspecific low back pain. A systematic review of observational studies. Spine, 1997. 22(4): p. 427-34. 25
Degeneration, defined by the presence of disc space narrowing, osteophytes, and sclerosis, turned out to be associated with nonspecific low back pain with odds ratios ranging from 1.2 to 3.3.
There is no firm evidence for the presence or absence of a causal relationship between radiographic findings and nonspecific low back pain.
GPCME South 2010 - Spondylosis and Pain 56

MRI . . .
Two decades following their description, the significance of Modic vertebral endplate and marrow changes remains a matter of debate. These changes are closely related to the normal degenerative process affecting the lumbar spine, and their prevalence increases with age. (Rahme, 2008 24)
MRI has been recognized as a modality of choice in the evaluation of the spine. Morphological abnormalities demonstrated by MR imaging do not always reflect low back pain (Fukuda, 2001 7)
GPCME South 2010 - Spondylosis and Pain 57
And . . .
Low back pain is a common but poorly understood entity. Features of degeneration depend on which component of the motion segment is predominantly affected, and include disk space narrowing, vacuum phenomenon, disk desiccation, vertebral osteophyte formation, disk herniation, and facet arthrosis, but these features do not necessarily have any relationship to symptoms (Miller, 2004 20)
GPCME South 2010 - Spondylosis and Pain 58
And . . .
Degenerative changes of the spinal column have long been and continue to be confused with the presence of spinal distress and pain (Anderrson 1998 22)
Degenerative disorders in the spine are normal, age-related phenomena and largely asymptomatic in most cases (Roh, 2005 21)
GPCME South 2010 - Spondylosis and Pain 59
And this is telling . . .
Degenerative spinal pathology is often implicated as the primary reason for chronic low back pain in older adults. Despite evidence that spinal pathology may be ubiquitous in older adults regardless of pain status, radiography continues to be heavily used in the diagnostic process (Hicks 2004 23)
Radiographic severity of disc and facet disease was not associated with pain severity among those with
chronic low back pain (Hicks 2004 23)
GPCME South 2010 - Spondylosis and Pain 60
Influence of occupation
An MRI study was performed in female subjects aged 45 to 62 years with persistent LBP and in age-matched controls. Subjects (n = 109) were selected from nursing and administrative professions
These findings give evidence that in subjects performing non-heavy work, patterns of lumbar disc degeneration are not associated with the job type and characteristic physical loadings (Schenk et al, Spine, 2006 26)
GPCME South 2010 - Spondylosis and Pain 61

Imaging Reporting

Roland, M. and M. van Tulder, Should radiologists change the way they report plain radiography of the spine? Lancet, 1998. 352(9123): p. 229-30. (31)
‘Radiologists must take some responsibility for the way their reports are used and interpreted. At present reports of plain radiographs are relayed in a manner that is unintentionally damaging to patients because they promote beliefs and patterns of behaviour that contravene current guidelines on the management of back pain.
Radiologists should use epidemiological information to convey precise and useful information, to reduce potential harm, and to educate their users’
GPCME South 2010 - Spondylosis and Pain 63

And should spondylosis be
reported at all?
The labeling of disease can be beneficial in terms of defining appropriate treatment such as in coronary artery disease. However, sometimes it may be detrimental such as when x-rays are used to diagnose lumbar spondylosis
(Bedson 2004 30)
GPCME South 2010 - Spondylosis and Pain 64
Illustrative Case 1
Mrs G
Age 79
GPCME South 2010 - Spondylosis and Pain 65
Mrs G’s History . . .
Mrs G tripped over a kerb, whilst running to catch a plane in the airport in the semi darkness
She fell heavily striking her head and breaking a rib
The rib healed, but six weeks later she still had significant left sub-occipital neck pain and headache VAS 70-90/100 with marked restriction of movement
GPCME South 2010 - Spondylosis and Pain 66

68
CT Imaging
Loss of Disc
Space
C1-2 Facet
Arthropathy
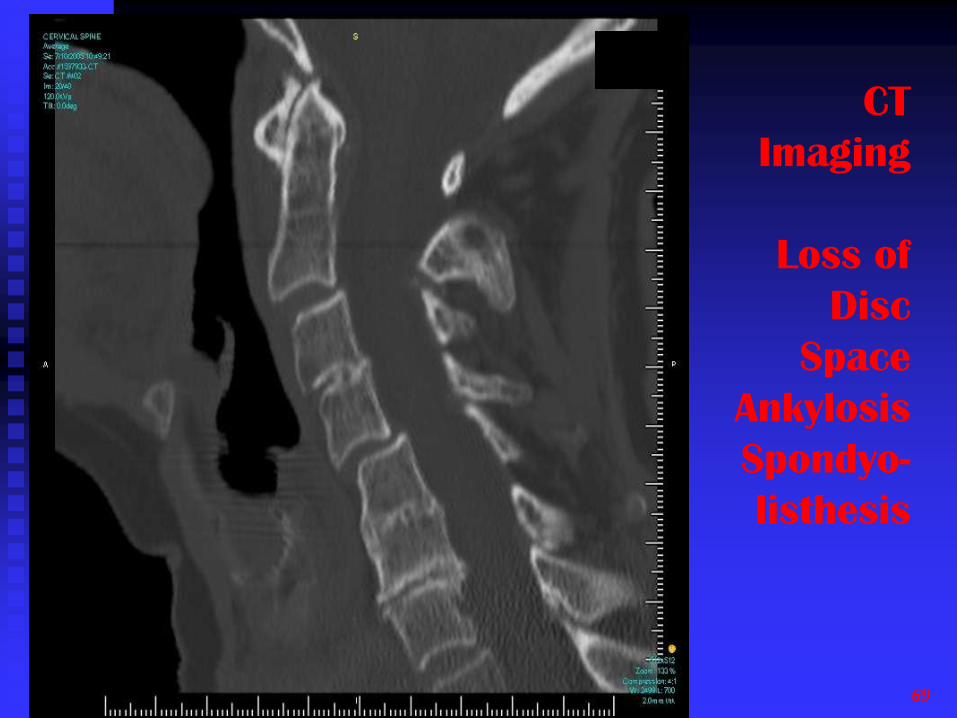
CT
Imaging
Loss of
Disc
Space
Ankylosis
Spondyo-
listhesis
GPCME South 2010 - Spondylosis and Pain 69
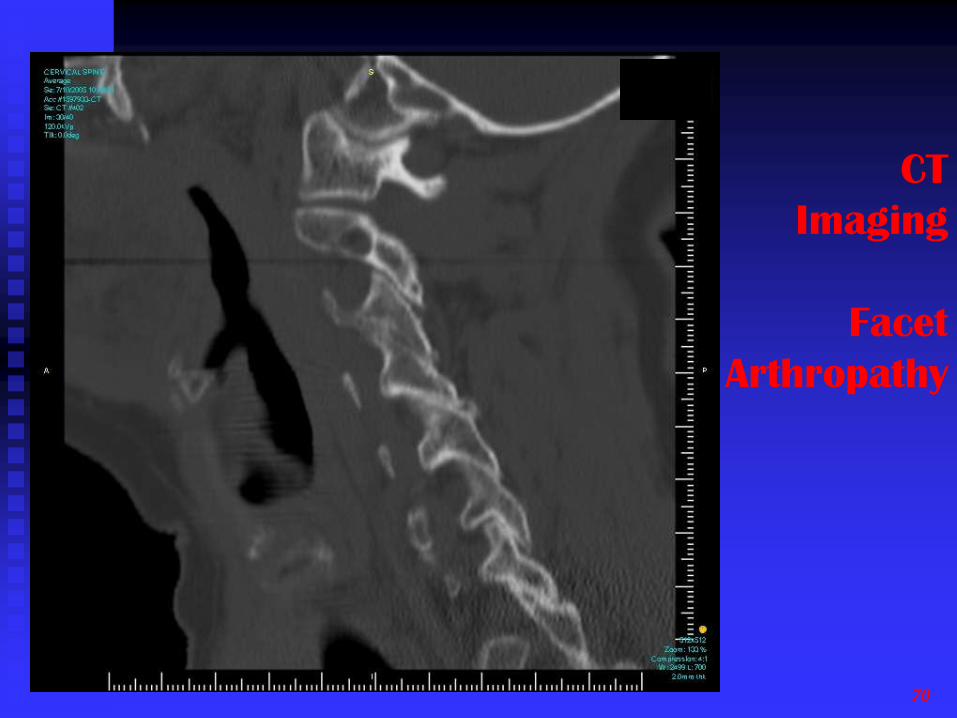
CT
Imaging
Facet
Arthropathy
70
71
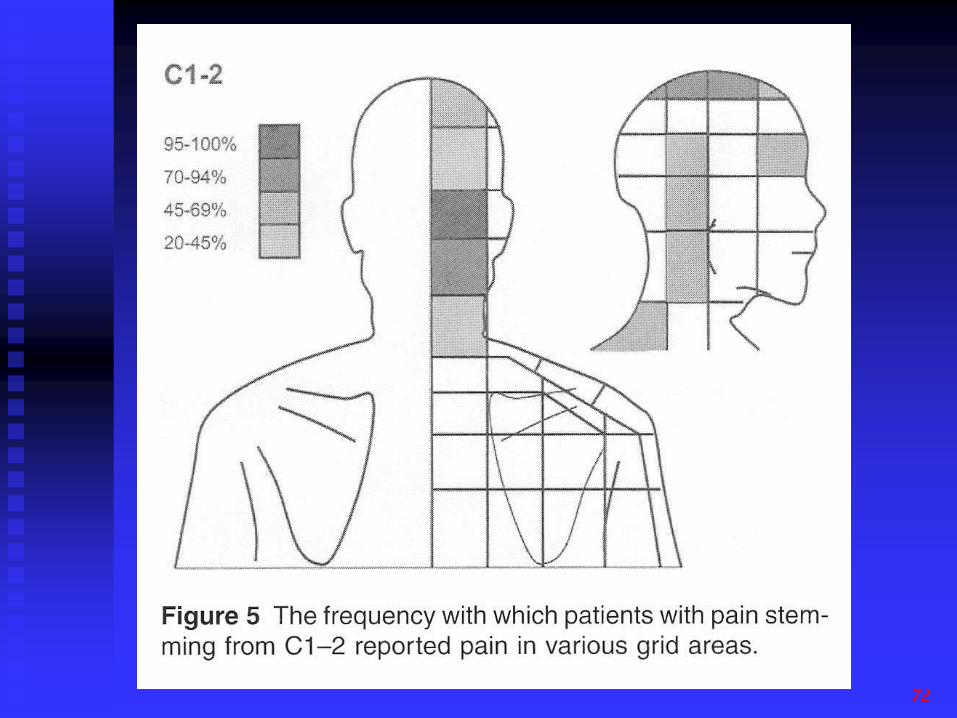
72

73
Left
C1-2
Facet
Injection
Illustrative Case 2
Mr ‘C’
Age 39
GPCME South 2010 - Spondylosis and Pain 74
Mr C’s History . . .
39 year old truck driver
Helping to lift 200kg sheet of metal
Slipped, twisted and developed ALBP
Previously fit and healthy, an active sportsman, 9 months later he cannot work or play sport
Was assessed by an orthopaedic specialist on behalf of ACC who organised an MRI scan
GPCME South 2010 - Spondylosis and Pain 75

76

Summary

Bogduk 1997 (1)
Traditionally certain changes in the intervertebral discs and zygapophysial joints have been described as features of a disease
With respect to the intervertebral discs, the term used is ‘spondylosis’
With respect to the zygapophysial (or facet) joints the terms used are ‘osteoarthrosis’, or ‘degenerative joint disease’
GPCME South 2010 - Spondylosis and Pain 78
Spondylosis and spinal osteoarthrosis are irregularly, if ever, in themselves associated with symptoms and disability
Osteoarthrosis or altered morphology of the z joints is not a disease, but an expression of the morphological changes resulting as a natural consequence of the stresses applied to the zygapophysial joints during life.
GPCME South 2010 - Spondylosis and Pain 79
Conclusion
Patients with spondylosis and osteoarthrosis may present with pain, but there are a greater number of others of the same age with spondylosis who do not have pain, and many with pain who have no changes at all
The presence of these findings on imaging should be interpreted with great caution, and should never be relied upon to establish a tissue-specific diagnosis for spinal pain.
GPCME South 2010 - Spondylosis and Pain 80
References
1. Bogduk, N., Age Changes in the Lumbar Spine, in Clinical Anatomy of the Lumbar Spine and Sacrum. 1997,
Churchill Livingstone: Edinburgh, London, New York, Philadelphia, Sydney, Toronto. p. 171-176.
2. Schwarzer, A.C., Aprill, C. N., Derby, R., Fortin, J., Kine, G., Bogduk, N., The prevalence and clinical features of internal disc disruption in patients with chronic low back pain. Spine., 1995. 20(17): p. 1878-83.
3. Schwarzer, A.C., et al., Pain from the lumbar zygapophysial joints: a test of two models. Journal of Spinal Disorders., 1994. 7(4): p. 331-6.
4. Manchukonda, R., et al., Facet joint pain in chronic spinal pain: an evaluation of prevalence and false-positive rate of diagnostic blocks. Journal of Spinal Disorders & Techniques, 2007. 20(7): p. 539-45.
5. Manchikanti, L., et al., Age-related prevalence of facet-joint involvement in chronic neck and low back pain. Pain Physician, 2008. 11(1): p. 67-75.
6. Schwarzer, A.C., C.N. Aprill, and N. Bogduk, The sacroiliac joint in chronic low back pain. Spine., 1995. 20(1): p. 31-7.
7. Fukuda, K. and G. Kawakami, Proper use of MR imaging for evaluation of low back pain (radiologist' view). Seminars in Musculoskeletal Radiology, 2001. 5(2): p. 133-6.
8. Kalichman, L. and D.J. Hunter, Lumbar facet joint osteoarthritis: a review. Seminars in Arthritis & Rheumatism, 2007. 37(2): p. 69-80.
9. Cavanaugh, J.M., et al., Pain generation in lumbar and cervical facet joints. Journal of Bone & Joint Surgery - American Volume, 2006. 88 Suppl 2: p. 63-7.
10. Kalichman, L., et al., Facet joint osteoarthritis and low back pain in the community-based population. Spine, 2008. 33(23): p. 2560-5.
GPCME South 2010 - Spondylosis and Pain 82
11. Yoshimura, N., et al., Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: the research on osteoarthritis/osteoporosis against disability study. Journal of Bone & Mineral Metabolism, 2009. 27(5): p. 620-8.
12. Boden, S.D., The use of radiographic imaging studies in the evaluation of patients who have degenerative disorders of the lumbar spine. Journal of Bone & Joint Surgery - American Volume, 1996. 78(1): p. 114-24.
13. Borenstein, D., Does osteoarthritis of the lumbar spine cause chronic low back pain? Current Pain & Headache Reports, 2004. 8(6): p. 512-7.
14. Binder, A.I., Cervical spondylosis and neck pain. BMJ, 2007. 334(7592): p. 527-31.
15. Lawrence, J., J. Bremner, and F. Bier, Osteoarthrosis: prevalence in the poulation and relationship between symptons and X-ray changes. Ann Rheum Dis, 1966. 25: p. 1-24.
16. Biering-Sorensen, F., The relation of spinal X-ray to low back pain and physical activity among 60-year old men and women. Spine, 1985. 10: p. 445-451.
17. Frymoyer, J., Spine radiographs in patients with low back pain. J Bone Joint Surg, 1984. 66A: p. 1048-1055.
18. Bogduk, N. and B. McGuirk, Imaging. Spondylosis, in Medical Management of Acute and Chronic Low Back Pain. An Evidence-Based Approach. 2002, Elsevier: Amsterdam. p. 50.
19. Boos, N. and J. Hodler, What help and what confusion can imaging provide? Baillieres Clinical Rheumatology, 1998. 12(1): p. 115-39.
20. Miller, T.T., Imaging of disk disease and degenerative spondylosis of the lumbar spine. Seminars in Ultrasound, CT & MR, 2004. 25(6): p. 506-22.
GPCME South 2010 - Spondylosis and Pain 83
21. Roh, J.S., et al., Degenerative disorders of the lumbar and cervical spine. Orthopedic Clinics of North America, 2005. 36(3): p. 255-62.
22. Andersson, G.B., What are the age-related changes in the spine? Baillieres Clinical Rheumatology, 1998. 12(1): p. 161-73.
23. Hicks, G.E., N. Morone, and D.K. Weiner, Degenerative lumbar disc and facet disease in older adults: prevalence and clinical correlates. Spine, 2009. 34(12): p. 1301-6.
24. Rahme, R. and R. Moussa, The modic vertebral endplate and marrow changes: pathologic significance and relation to low back pain and segmental instability of the lumbar spine. Ajnr: American Journal of Neuroradiology, 2008. 29(5): p. 838-42.
25. van Tulder, M.W., et al., Spinal radiographic findings and nonspecific low back pain. A systematic review of observational studies. Spine, 1997. 22(4): p. 427-34.
26. Schenk, P., et al., Magnetic resonance imaging of the lumbar spine: findings in female subjects from administrative and nursing professions. Spine, 2006. 31(23): p. 2701-6.
27. Okada, E., et al., Aging of the cervical spine in healthy volunteers: a 10-year longitudinal magnetic resonance imaging study. Spine, 2009. 34(7): p. 706-12.
28. Espeland, A., et al., Observer variation in plain radiography of the lumbosacral spine. British Journal of Radiology, 1998. 71(844): p. 366-75.
29. Beattie, P.F. and S.P. Meyers, Magnetic resonance imaging in low back pain: general principles and clinical issues. Physical Therapy, 1998. 78(7): p. 738-53.
30. Bedson, J., R. McCarney, and P. Croft, Labelling chronic illness in primary care: a good or a bad thing? British Journal of General Practice, 2004. 54(509): p. 932-8.
31. Roland, M. and M. van Tulder, Should radiologists change the way they report plain radiography of the spine? Lancet, 1998. 352(9123): p. 229-30.
GPCME South 2010 - Spondylosis and Pain 84