sphenopalatine artery control instructional course - … course ... – sphenopalatine ......
TRANSCRIPT

Sphenopalatine Artery ControlSphenopalatine Artery ControlInstructional CourseInstructional Course
Mr Maged AbdelkaderMr Maged AbdelkaderMSc MD FRCS(Edin.,Glas.,Irel.) FRCS(ORLMSc MD FRCS(Edin.,Glas.,Irel.) FRCS(ORL--HNS)EdinHNS)Edin
Consultant ENT Head&Neck surgeonConsultant ENT Head&Neck surgeonBasildon &Thurrock University HospitalsBasildon &Thurrock University HospitalsAssociate Teaching Hospitals, University Associate Teaching Hospitals, University
College LondonCollege LondonUKUK
TopicsTopics�� IntroductionIntroduction�� AnatomyAnatomy�� IndicationsIndications�� InstrumentsInstruments�� Technique and pitfallsTechnique and pitfalls�� ResultsResults�� ConclusionsConclusions

Epistaxis treatment cascadeEpistaxis treatment cascade
�� SPA not yet 1SPA not yet 1stst lineline�� Direct therapy is Direct therapy is
bestbest�� Nasal packing Nasal packing –– ifif
direct treatment failsdirect treatment fails�� Ligation or Ligation or
embolisation if embolisation if packing failspacking fails
Epistaxis treatment cascadeEpistaxis treatment cascade
�� SPA not yet 1SPA not yet 1stst lineline�� Direct therapy is Direct therapy is
bestbest

IntroductionIntroduction
�� Around 20% of nose bleeds are posteriorAround 20% of nose bleeds are posterior(Schaitkin, 1987)(Schaitkin, 1987)
�� Posterior epistaxis poses a challenge. Posterior epistaxis poses a challenge. (O(O’’Flynn and Shadaba, 2000)Flynn and Shadaba, 2000)
�� Failure rates of AP packing varies widely from Failure rates of AP packing varies widely from 0% to 52% (Pollice PA, 1997. Cannon CR, 0% to 52% (Pollice PA, 1997. Cannon CR, 1993)1993)
IntroductionIntroduction
�� Transnasal endoscopic sphenopalatine artery Transnasal endoscopic sphenopalatine artery (SPA) ligation has become a popular (SPA) ligation has become a popular techniquetechnique
�� Published data suggest cessation of epistaxis Published data suggest cessation of epistaxis in 90in 90--100% of patients100% of patients
�� Individual study sample sizes are small, Individual study sample sizes are small, continuing audit of surgical outcome is continuing audit of surgical outcome is required to validate these early results required to validate these early results (Kumar(Kumar et alet al, 2003), 2003)

AnatomyAnatomy
AimAim
�� Review applied anatomy for SPA Review applied anatomy for SPA ligationligation
�� Consider immediate anatomical Consider immediate anatomical relationsrelations

Ligation HierarchyLigation Hierarchy�� Ligate as close to bleed as possibleLigate as close to bleed as possible
–– SphenopalatineSphenopalatine
–– Internal MaxillaryInternal Maxillary ? Anterior ethmoidal? Anterior ethmoidal
–– External CarotidExternal Carotid
Internal maxillary arteryInternal maxillary artery


Sphenopalatine artery Sphenopalatine artery anatomyanatomy

Endoscopic anatomyEndoscopic anatomy
Target: sphenopalatine Target: sphenopalatine foramenforamen

Relations to neighbouring Relations to neighbouring structuresstructures

Basic outline -matchbox ethmoid cavityAnterior relations

Posterior relations
II
VbVidian

Branches of the SPABranches of the SPA
Branches of the SPABranches of the SPA

Posterior septal branch

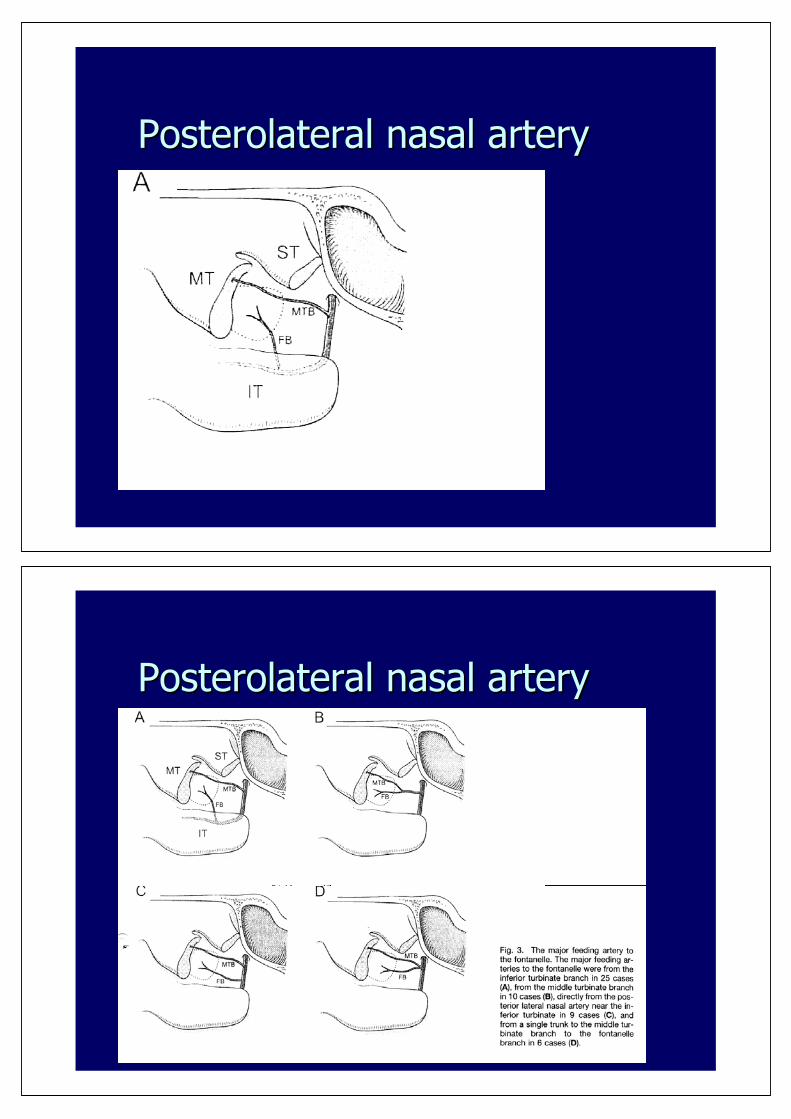
Posterolateral nasal arteryPosterolateral nasal artery
Posterolateral nasal arteryPosterolateral nasal artery

InstrumentationInstrumentation


Technique and pitfallsTechnique and pitfalls

Endoscopic SPA ligationEndoscopic SPA ligation
�� 3 techniques3 techniques
–– Via a middle meatal antrostomyVia a middle meatal antrostomy
–– Direct via middle meatusDirect via middle meatus
–– Combined antroscopic approach Combined antroscopic approach --
The MMA approachThe MMA approach
�� InfundibulotomyInfundibulotomy�� MMAMMA�� Resect fontanelleResect fontanelle�� Create tunnelsCreate tunnels

Accessory nasal artery 10%Accessory nasal artery 10%
Middle meatal approachMiddle meatal approach
�� Good if meatus wideGood if meatus wide�� May miss branchesMay miss branches�� Avoids antrosotmyAvoids antrosotmy

Combined MMA & antroscopic Combined MMA & antroscopic approachapproach
�� Time consumingTime consuming�� Access to main trunkAccess to main trunk�� BiBi-- manualmanual
techniquetechnique–– AntroscopeAntroscope–– Ipisilateral nasal Ipisilateral nasal
airwayairway -- instrumentsinstruments
Combined antroscopic approachCombined antroscopic approach

Combined antroscopic approachCombined antroscopic approach
Combined antroscopic approachCombined antroscopic approach

Combined antroscopic approachCombined antroscopic approach
Technical Pitfalls of MMA Technical Pitfalls of MMA approachapproach
�� CurvatureCurvature

Technical PitfallsTechnical Pitfalls
�� CurvatureCurvature�� Arterial traumaArterial trauma

Technical PitfallsTechnical Pitfalls
�� CurvatureCurvature�� Arterial traumaArterial trauma�� Failed superior Failed superior
tunneltunnel�� Failure to check for Failure to check for
22ndnd branchbranch
What should we have done?
Creating the superior tunnel

ResultsResults
Prospective AuditProspective AuditTo assess the following outcome measures of To assess the following outcome measures of
transnasal endoscopic SPA ligation:transnasal endoscopic SPA ligation:
1.1. Immediate postoperative cessation of Immediate postoperative cessation of
epistaxisepistaxis
2.2. Assess early and late recurrenceAssess early and late recurrence
3.3. Morbidity and mortality Morbidity and mortality

MethodsMethods
�� Prospective audit of patients who underwent Prospective audit of patients who underwent
transnasal endoscopic SPA ligationtransnasal endoscopic SPA ligation
�� Patients were treated in one of three centres Patients were treated in one of three centres
between April 2003 and April 2006between April 2003 and April 2006
�� 46 patients 46 patients ((minimum 9 months follow up minimum 9 months follow up
only includedonly included))
PatientsPatientsn= 46 , 34 male, 10 femalen= 46 , 34 male, 10 female
Mean Range
Age (years) 68.5 37-100
Follow up (months) 15.8 9-24
Pre-operative stay (days) 2.3 1-4
Post-operative stay (days) 1.5 1-4

TechniqueTechnique
Method % in total sample
% in patients with recurrence
Clips only 33 16.6
Diathermy only 12.5 50.4
Both 54.5 33
ResultsResultsRecurrence of epistaxisRecurrence of epistaxis No. of No. of
patientspatientsTime of Time of
recurrencerecurrence
Immediate post operative period Immediate post operative period (24 hours)(24 hours)
00 --
During inpatient stayDuring inpatient stay 22 --MAMAligationligation--conservativeconservative
3 & 7 days3 & 7 days
Post discharge Post discharge -- requiring medical attentionrequiring medical attention 11 --angiographyangiography
5 days 5 days
Post discharge Post discharge -- not requiring medical attentionnot requiring medical attention 22 4 & 10 4 & 10 monthsmonths

M & MM & M
�� Morbidity: NoneMorbidity: None
�� Mortality: (2 patients)Mortality: (2 patients)
Patient 1: ARDSPatient 1: ARDSPatient 2: 100 years old, HFPatient 2: 100 years old, HF
LiteratureLiteraturepatientspatients arteriesarteries f/up in f/up in
monthmonthSuccessSuccess%%
complicaticomplicationsons
RoweRowe--Jones,Jones,19981998
1010 1111 99 100100 nonenone
OO’’FlynnFlynn etetalal, 2000, 2000
1212 1414 99 100100 nonenone
Voegels,Voegels,20012001
1111 1212 -- 100100 nonenone
RamRam et alet al,,20002000
66 66 -- 9292 nonenone
SnydermanSnydermanet al, et al, 19921992
3838 3838 1010 9292 Crusting (34%), Crusting (34%), palatal numbness palatal numbness (13%)(13%)
AbdelkaderAbdelkaderet alet al, 2007, 2007
4343 4545 Up to 24 Up to 24 (mean(mean15.3)15.3)
(93.4%)(93.4%) nonenone

ConclusionsConclusions�� Both post operative and longBoth post operative and long--term success rates for term success rates for
the procedure are lower than previously published the procedure are lower than previously published datadata
�� Recurrence of epistaxis requiring active intervention Recurrence of epistaxis requiring active intervention occurred within one month of the procedure in all of occurred within one month of the procedure in all of the cases where the procedure failedthe cases where the procedure failed
�� No incidence of failure in the long term found (after No incidence of failure in the long term found (after 12 month)12 month)
ConclusionsConclusions
�� Endoscopic intranasal clipping of the SpA Endoscopic intranasal clipping of the SpA is a reliable procedure in controlling is a reliable procedure in controlling posterior epistaxis but has a consistent posterior epistaxis but has a consistent failure rate ~ 10%failure rate ~ 10%
�� Failures occur within a month of ligationFailures occur within a month of ligation

My NCBI [Sign In][Register]All DatabasesPubMedNucleotideProteinGenomeStructureOMIMPMCJournalsBooks Search for Limits
Preview/IndexHistoryClipboardDetails
Display ShowAll: 1
Review: 0
Endoscopic control of the sphenopalatine artery for epistaxis: long-term results.Abdelkader M,Leong SC,White PS.
Department of Otolaryngology, University of Dundee, Ninewells Hospital and Medical School, Dundee, Scotland, UK.The aim of this study was to prospectively evaluate post-operative cessation of bleeding and late recurrence of epistaxis in a cohort of patients treated by endoscopic ligation of the sphenopalatine artery. Participants comprised patients undergoing sphenopalatine artery ligation for posterior epistaxis at three east Scotland hospitals. Main outcome measures were recurrence of epistaxis in the immediate post-operative period and at long-term follow up (minimum nine months). Forty-three patients (30 men and 13 women) underwent 45 procedures; two patients underwent bilateral ligation. Two patients suffered recurrence as in-patients. Two patients experienced subsequent epistaxis requiring medical treatment. Two further patients suffered minor late epistaxis not requiring treatment. Success in preventing significant recurrence was 93 per cent. All recurrences requiring intervention occurred within one month of surgery. None of the patients in this series reported nasal complications. We found sphenopalatine artery ligation to be an effective means of achieving long-term control of posterior epistaxis.PMID: 17201991 [PubMed - as supplied by publisher]
