some chronic non-tuberculous pulmonary conditions
TRANSCRIPT
T H E IRISH J O U R N A L MEDICAL SCIENCE THE OFFICIAL JOURNAL OF THE ROYAL ACADEMY OF MEDICINE IN I R E L A N D
OF
SIXTH SEaIES. No. 142. OCTOB~a% 1937.
SOME CHRONIC NON-TUBERCULOUS PULMONARY CONDITIONS.*
By G. T. O'B~I~,r
I N this paper are presented some of the clinical and radiological features of a group of patients suffering from non-tuberculous diseases of the lungs; not that such features are rar~ and
interesting, but with a view to considering what the incidence of such conditions may be. Three groups of cases are presented: (~) the bronchiectatic, (b) the indeterminate, and (c) the neoplastic.
I n a certain number of these patients the physical signs and general examination could lead to only one diagnosis, namely, pu lmonary tuberculosis; and I hope to point out th rough the medium of the following notes the necessity for auxiliary aids to diagnosis in cases of pulmonary disease simulating tuberculosis where the B. tuberculosis is repeatedly absent from the sputum, in " mir ror tests " of expired air, and in ,contents of gastric lavage.
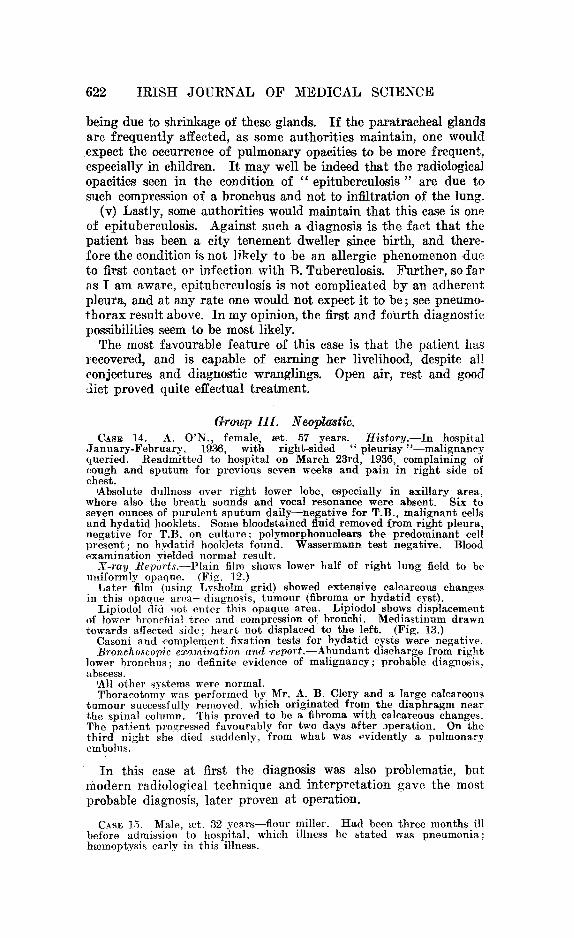
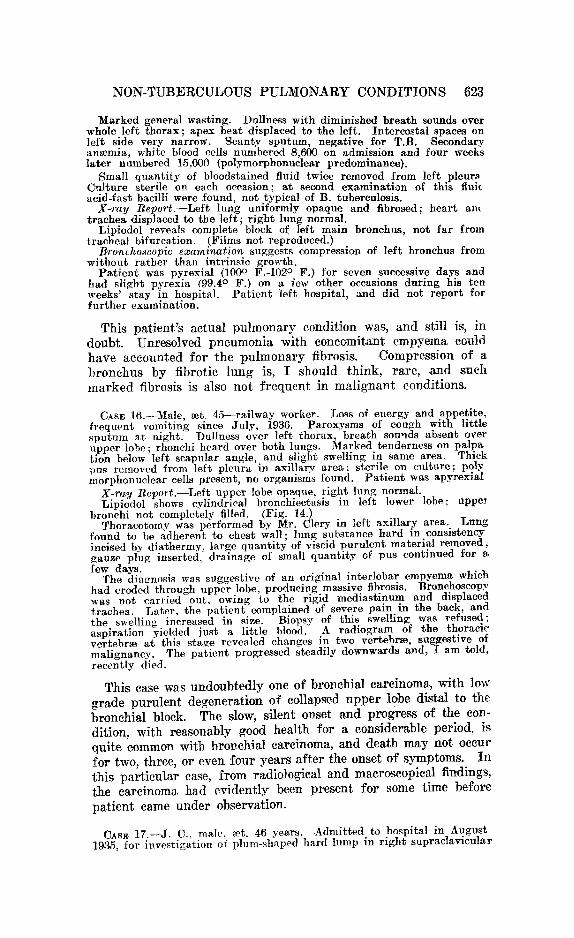
Grau.p I. B~'onchiectati~. Case 1. R. E., female, mr. 19 years. History of cough and sputum for
nine years. Sputum never found to contain T.B. No hmmoptysis. Marked clubbing of fingers. Treated in a sanatorium for nine months. 'Antral infection suspected.
X-ray Report (a#er lipiodol iniection).~Saccular bronchiectasis in right upper and middle lobes. Note position of main right lower bronchi within cardiac shadow. (Figs. I and 2.)
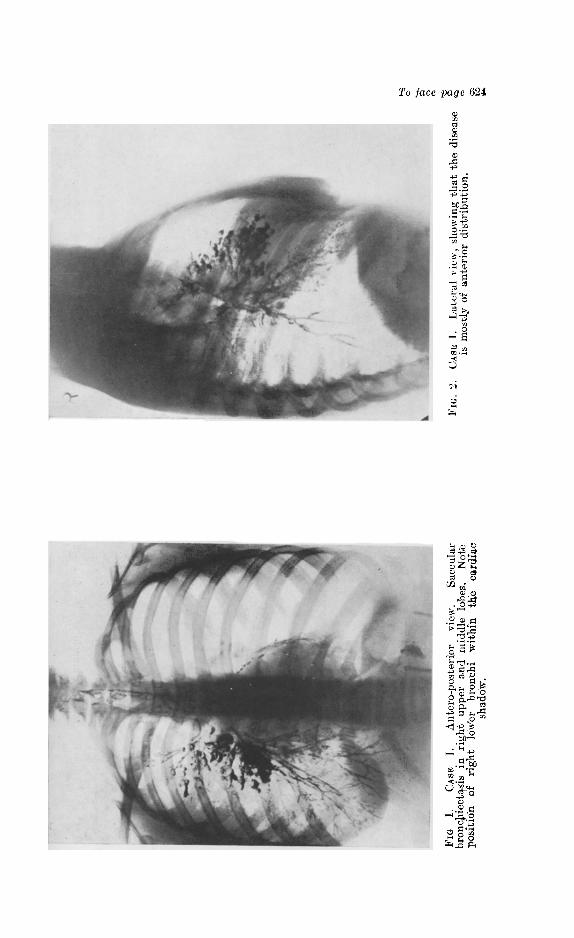
CASE 2. M. B., female, mr. 35 years. History of ethmoidal infection for four years. Increasing cough and sputum, latter persistently negative for T.B. H~emoptysis twice. Ethmoidal cells and antra show active infection at present.
X-ray Report.--Lipiodol demonstrates saccular bronchiectasis in right upper lobe and cylindrical type in middle lobe. Note tortuous bronchi. (Fig 3.)
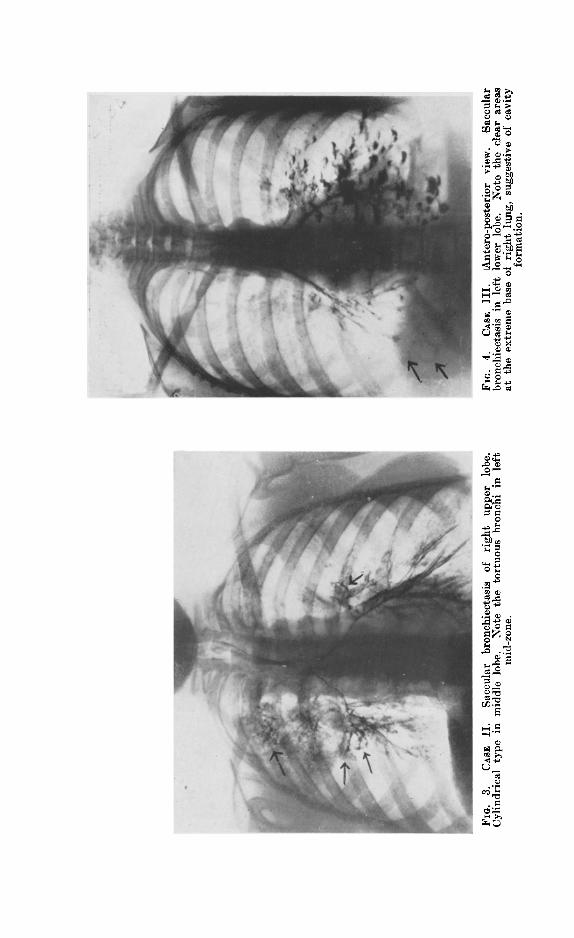
CAss 3. M. S., female, mr. 25 years. History of cough with sputum for over two years; sputum negative for T.B. H~emoptysis on several occasions. No previous illness. Family history good. Auscultation revealed coarse breath sounds over left base, and sub-crepitan~ rales over both lower lobes posteriorly; vocal resonance increased over left lower lobe. Cardio-vascular system normal. Antra and sinuses normal.
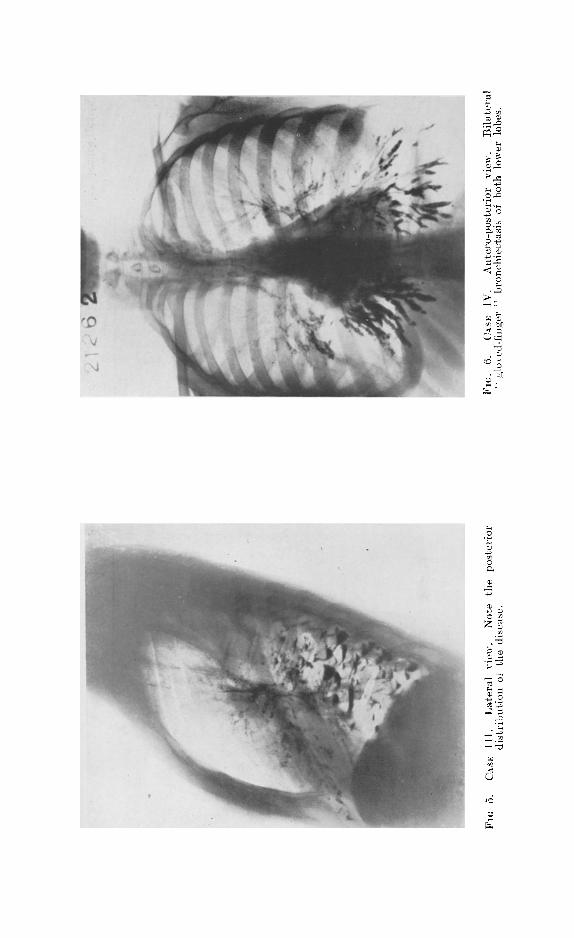
Plain x-ray film demonstrates shadows over left base suggestive of bronchiectasis. Lipiodol shows saccular bronchiectasis of left lower lobe (see Fig. 4), localised posteriorly (see Fig. 5.)
From the negative history of previous illness and absence of air sinus infection this case is probably of congenital origin. Postural drainago and bronehoscopic lavage have yielded a fairly good palliative result in this instance; lobectomy is contra-indicated owing to physical and sligh$
Communication made to the Section of Medicine, January 8th, 1937.
618 I R I S H J O U R N A L O F M E D I C A L S C I E N C E
radiological evidence of similar disease at extreme right base (note clear areas in A.P. view on right side).
CAs~ 4. E. M., female, rot. 18 years. History.--Treated as pulmonary tuberculosis in a sanatorium for several months; sputum repeatedly nega- tive. Sub-crepitant rales over both mid-zones and lower lobes; distant cavernous breathing in same areas. No h~emoptysis. Sinuses normal. Measles and pertussis when a child. Clubbed fingers. General condition poor.
X-ray Report.--Lipiodol demonstrates bilateral " glove f inge r" or combination of fusiform and cylindrical bronchiectasis. (Figs. 6 and 7.)
Disease in this instance probably originated after measles or pertussis. Pat ient attended hospital for only a short period of treatment.
CASE 5. R. C., female, rot. 17 years. History.--Ten months in a sanatorium. Copious sputum, always negative for T.B. No h~emoptysis. Bilateral nasal obstruction. Marked kyphosis and " pigeon chest." No previous illness. Sinuses and antra normal.
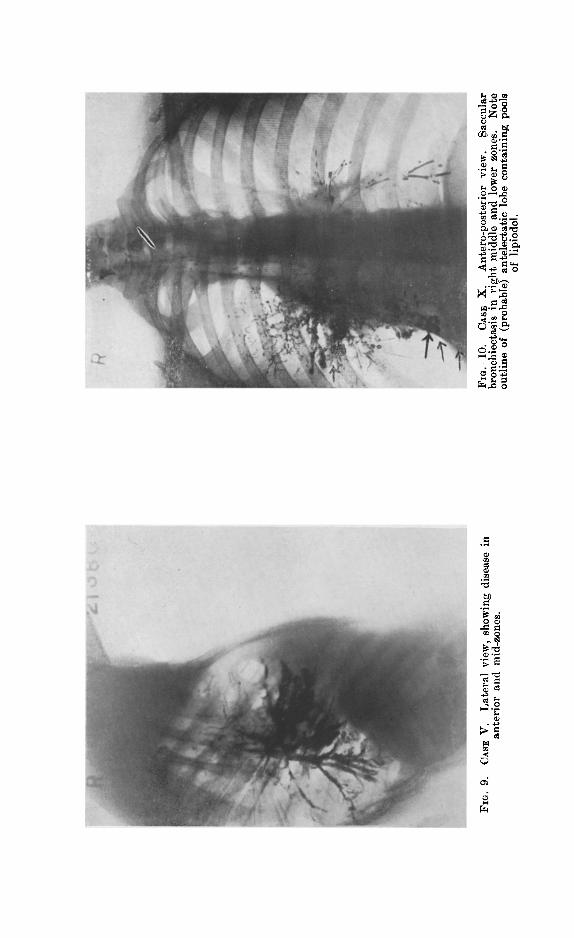
X-ray Report.--Lipiodol shows bilateral saccular bronchiectasis with very large sacs, possibly congenital. (Figs. 8 and 9.)
This case is most probably one of congenital origin. Open-air t reat- ment with postural drainage has yielded a quite satisfactory result in this instance.
CASE 6. G. F., female, mr. 36 years. History.--Cough since a child. Pneumonia (left side) five years ago. Pleural thickening over left lower lobe; fine bubbling rales after coughing and deep respiration. Air sinuses normal. Copious sputum, repeatedly negative for T.B.
X-ray Report.--Saccular bronchiectasis of left lower lobe shown by lipiodol; these shadows are completely obscured in ordinary films by the cardiac shadow. (Fihns not reproduced.)
This may possibly be an instance of congenital bronchiectasis (cough since a child) aggravated by lobar pneumonia. ~A suitable case for lobect~)my, as disease was unilateral, age and general condition were suitable for operation, but surgical t reatment was refused by patient.
CAs~ 7. J . B., male, ~et. 25 years. Admitted to hospital as a case of chronic nasal sinusitis; both antra contained mucopus and were treated by lavage, eventually clearing up completely. Cough and sputum, lat ter negative for T.B. ; patient had previously been treated as a tuberculous patient in a sanatorium.
X-ray Report.--Lipiodol shows slight bronchiectasis in right base, bronchiectatic cavities in cardio-phrenic angle. Many large bronchiectatic cavities in left base ; appearances quite typical. Bronchiectasis suggested by ordinary film. (Films not re.produced.)
Treated palliatively by autogenous vaccine and postural, drainage; did not remain under observation sufficiently long enough to judge results.
CAs~ 8. R. M., female, eet. 24 years. History of cough, sputum and hmmoptysis. Treated as tuberculous in a sanatorium; sputum repeatedly negative for T.B.
X-ray t~eport.--Lipiodol shows fusiform and cylindrical bronchiectasis of r ight upper, middle and lower lobes. Sinuses normal. Films not repro- duced.
Previous history of " bad " measles, latter the probable origin of the pulmonary disease. Open-air treatment, together with a creosote mixture, have proved of definite palliative value.
CASE 9. M. B., male, ~et. 14 years. Good health whilst living in the country, but cough, sputum and hmmoptysis when living in the city.
Physical examination yielded evidence suggestive of pulmonary tuber- culosis; sputum negative for T.B.
X-ray Beport.--Plain film shows no evidence of tuberculosis, but shadows over left lower lobe are suggestive of bronchiectasis. Lipiodo! shows cylindrical or " glove finger i' bronchiectasis of left lower lobe. Both antra radiologically opaque.
Antra found to contain pus; lavage of antra carried out, later radical drainage operation performed. Progress since operation, good.
CAs~ 10. J. K.. male, ~et. 28 years. Apparently in good health up to December, 1936, When he developed epigastric pain of r days' dura- t ion; this was followed by cough and sputum (2 ozs. daily), the latter bearing a bad taste and odour. Lost 16 lbs. in weight over a period of nine weeks.
Previous illnesses-=influenza in 1926. Sub-crepitant rales over r ight mid- and lower genes, distant cavernous breathing in right axillary area.
N O N - T U B E R C U L O U S P U L M O N A R Y C O N D I T I O N S 619
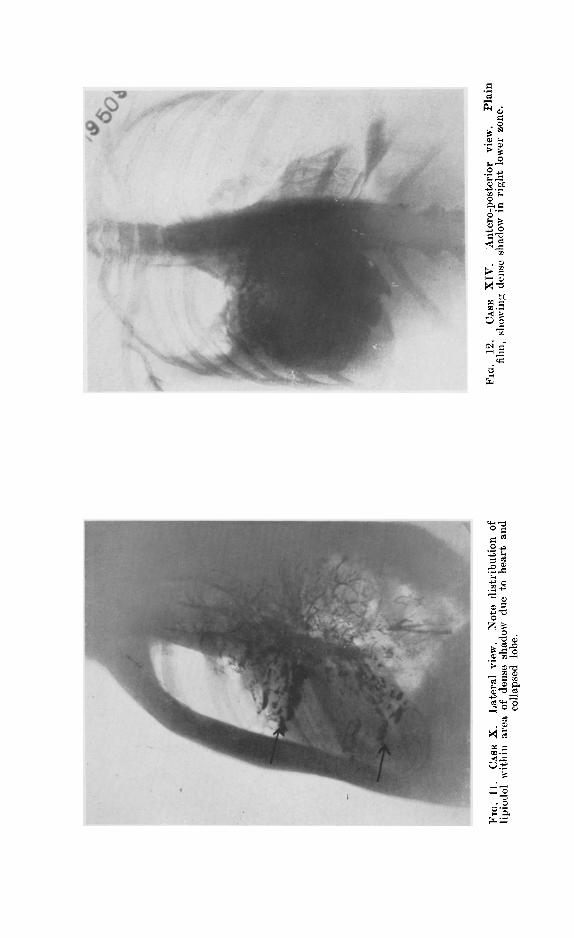
X-ray t~eport.--Lipiodol demonstrates saccular bronchiectasis in right mid-zone; heart and trachea displaced to the right, outline of atelectatie lobe containing pools of lipiodol can be seen behind and extending below cardiac shadow. Note s t raight line appearance of atelectatic lobe. (Figs. 10 and 11.)
The bronchiectasis in this case is probably due to the atelectatie lobe and fibrosis brought about by the latter. Pa t ien t ' s general progress up to time of his last examination (March, 1937) was good. He has not returned for examination since. No special t reatment employed.
A s the fo rego ing cases have al l been col lected d u r i n g the p a s t twe lve months , t h e y have no t y e t been f u l l y i n v e s t i g a t e d as to the c o m p a r a t i v e va lue of v a r i o u s me thods of t r e a t m e n t . The m a j o r i t y o f these cases p r e sen t b i l a t e r a l disease, t h u s p r e c l u d i n g lobec tomy as t he me thod of choice. The e q u i p m e n t of a creosote c ha mbe r fo r the t r e a t m e n t of these cond i t ions is to be cons ide red when accom- m o d a t i o n fo r each a t the ]~ichmond H o s p i t a l becomes avMlable. ( D u k e F i n g a a r d i n h a l a t i o n t h e r a p y is also to be considered. )
The associa t ion of s inus i t i s and ant ra] in fec t ion in f o u r cases of the smal l ser ies quo ted is of in teres t . The absence of j u v e n i l e eases in th i s g roup is also no tewor thy , f o r in t h e E n g l i s h a n d A m e r i c a n l i t e r a t u r e t h e r e is f r e q u e n t r e f e r e n c e to b r o n c h i e c t a s i s o c c u r r i n g in chi ldren . The i m p o r t a n c e of i nve s t i ga t i on b y means of l i p i o d o l is, I t h i n k , w e l l d e m o n s t r a t e d b y these cases. I n p l a i n x - r a y f i lms an upper lobe bronchie~tavis c a ~ o t be differentiated f r o ~ pulmonary tuberculosis.
The a p p a r a t u s a n d m e t h o d o f i n t r o d u c t i o n of l i p i o d o l t h a t I e m p l o y m a y be b r ie f ly d e s c r i b e d here.
Special 20 e.c. lipiodol syringe (Mayer and Phelps) with " screw-on " c~unula; to the end of la t ter is attached a No. 10 rubber catheter, lubricated with glycerine; one or other nostril is an~esthetised by installa- t ion of a few drops of ]0 per cent. cocaine solution; the tonsils, fauces and posterior pharyngeal wall are also swabbed with this solution; the tongue is drawn forward and a few drops of cocaine solution sprayed over the epiglottis on to the vocal cords. XVhen anaesthesia is thought to be complete, the catheter is introduced through the nose and pushed gently backwards until i t reaches the rima glottidis; the pat ient is asked breathe deeply during this stage, and traction on the tongue often facili- tates the correct direction of the catheter. Float ing on the surface of the lipiodol in the syringe is 1 c.c. of 10 per cent. cocaine solution. At the first indication of the entry of the catheter into the trachea, this cocaine is injected in order to anmsthetise the tracheal and bronchial mucous membrane. Cough, slight respiratory embarrassment and inabili ty properly to pronounce the let ter " E " are indications tha t the catheter ]Jas entered the glottis. To fill the r ight lower bronchus the lipiedol is injected with the pat ient s i t t ing upr ight ; to demonstrate the r ight mid- zone and eparterial bronchus the pat ient is lying on the r ight side while the lipiodol is injected. To demonstrate the left lower bronchus the pat ient lies on the left side during injection of lipiodol, and to fill the left upper bronchus, the pat ient ' s head and shoulders are lowered whilst still on the left side, the pat ient being also rotated slightly face- wards; the left upper bronchus is the most difficult to demonstrate.
W i t h a l i t t l e exper ience t h i s m e t h o d is eas i ly c a r r i e d ou t a n d has t he a d v a n t a g e t h a t a n y one side o r s ing le lobe m a y be d e m o n s t r a t e d a t wi l l w i t h o u t f i l l ing the comple t e b ronch ia l t r ee a n d alveoli . The i n j e c t i o n shou ld be c a r r i e d ou t in an a n n e x e of t h e x - r a y room, a n d r a d i o g r a m s t aken or f luoroscopic s c reen ing c a r r i e d ou t as soon

620 I R I S H J O U R N A L OF M E D I C A L S C I E N C E
as possible af ter injection. A li t t le t ime should in tervene between injection and rad iography as i t allows for a more accurate demon- s t rat ion of the bronchioles (which may be affected in moniform bronchiectasis) by the lipiodol, as it takes a l i t t le t ime for the heavy oil to displace the residual air in the bronchioles.
Dur ing the injection and rad iography the pa t ien t is exhorted to re f ra in f rom coughing ( f requent ly difficult for the patient), and deep breathing through the open mouth apparen t ly helps to alleviate the tendency to cough; thorough local an~esthetisation is the best prophylactic. When radiography is completed the pat ient ~s placed in postures favour ing drainage of .the bronchus or bronchi containing lipiodol, and coughing is encouraged. I n this way much of the lipiodol is expectorated. I have seen bu t slight iodism in three pat ients following injections of lipiodol; slight coeainism is not uncommon and is t r ea t ed by enforced exercise, br isk walk ing about ; la ter a cup of s t rong coffee is given to the pat ient to drink.
Group II. Indeterminate. CAs~ 11. P. G., male, ~et. 51 years. Histary.--Peritonsillar abscess in
May, 1936, cough with aching pain in right side of. thorax developed in June, 1938. Copious yellow sputum, especially when lying on right side. Sputum negative for T.B. No hmmoptysis.
Dullness in right axilla, bronchial breathing and moist rales in same a r e a .
X-ray tteport.--Plain film shows consolidation of right middle lobe with cavity near upper margin. Lipiodol shows a wedge-shaped area clear o[ lipiodol; bronchi proximal to this area are completely filled and are of cylindrical bronchiectatie contour; obstruction of peripheral branches. (~'ilms not reproduced.)
This was a case of pu lmonary abscess, which responded perfectly to postural drainage. Recent physical and radiological examina- tions revealed the pa t ien t to be normal save for some fibrosis (radiological) in r ight mid zone.
CAs~ 12. G. A., female, mr. 24 years. History.--In February, 1935, developed lump on forehead, with frontal hea~laches which persisted for six months; during this period patient had a brisk h~moptysis, and also complained of pains in left side of thorax, worse at night.
Previous illnesses--mumps and whooping cough. Patient had previous to 1935 been treated in a sanatorium as tuberculous; a left phrenic evulsion had been performed.
Dullness over lower two-thirds of. left side of chest; diminished breath sounds over left base, few rhonchi and distant mucous rales over same area. Other systems normal, save for bilateral keratitis. ,Sputum nega- tive for B. tuberculosis. Wassermann test, full positive (+3).
X-ray tteport.--Skull normal. Chest, dense shadow in lower left chest, probably not fluid; diaphragm elevated. Lipiodol shows a large cavity in .centre of dense area, which communicated with a tm~uous bronchus.
The differential diagnosis of the actual na tu re of the pulmonary condition in this case is problematic. The condition may have originally been an atelectatic lobe, congenital or otherwise, in which bronchiectasis developed. A previous pu lmonary abscess could have given rise to fibrosis of the lobe with resul tant dilatation of the bronchus. Last ly, a gummatous infi l t rat ion of the lef t lower bronchus may ha~e caused collapse of the lower lobe with subse-
NON-TUBERCULOUS PULMONARY CONDITIONS 621
quent fibrosis, but such is not the usual course and distribution of pulmonary syphilis.
This patient has had two courses of antisyphilitic treatment, with no change in the Wassermann reaction. Some general improve- ment has taken place, but, as expected, without effect on the pulmonary condition.
CAs~ 13. M. O'R., fema!e, eet. 17 years. History.--Pain in right shoulder for four weeks; cough with little sputum. Vague history of either epistaxis or h~emoptysis in November, 1935; treated as pulmonary tuberculosis in a city hospital in November, 1935.
At first examination (30/4/36) dullness with pure tubular breathing, bronchophony and pectoriloquy over right upper lobe; patient was pyrexial at this time, and was admitted to hospital as a case of pneumonic pulmonary phthisis. Sputum was scanty, and on five examinations was each time negative for T.B., the predominating organism being the pneumococcus.
During four months in hospital the patient displayed pyrexia twice for two and three days respectively; her weight increased from 6 st. 13 lbs. to 7st. 6 lbs. Physical signs gradually cleared up with the exception of the supraclavicular and suprascapular areas, where tubular breathing is still present; adventitious sounds were absent throughout. Wasser- mann test was negative. Blood count and hmmoglobin content normal; sedimentation rate of red blood ceils normal. Mantoux test, as expected, was positive, but not grossly so as might occur if tile condition present w(,;'e an acute tuberculous one.
Patient returned to work in December, 1936, and has remained in good health since.
X-ray t~eports.--30/4/36. Consolidation or atelectasis of right upper lobe; lower right zone and left lung normal.
S/5/36. Lipiodol failed to penetrate opaque area; peripheral bronchi filled. Lateral view showed opacity against posterior wall of chest, anterior area clear.
As a diagnostic measure artificial pneumothorax was induced on the right side. X-ray examination (22/5/36) showed collapse of mid and lower lobes, with the upper lobe adherent.
3/12/36. Partial resolution of opaque area.
There are many possibilities as to the diagnosis of this patient 's pulmonary opacity. The sudden and single attack of epistaxis or h~emoptysis (?) in November, 1936, suggests the possible inhalation of a radio-translucent foreign body into the eparterial bronchus, i.e., blood, with subsequent clotting and resultant collapse of lobe. The subsequent gradual partial absorption of the opacity rather favours this view.
(ii) Unresolved, ambulatory pneumonia is another suggested diagnosis. In such a condition, purulent complications would be liable to occur, and whether they did arise or not one would expect much more fibrosis of the affected lobe over such a period of time as this case has been under observation.
(iii) The possibility of tumour, extrinsic or intrinsic, involving the eparterial bronchus was also considered. As the progress of the pat ient was satisfactory, and the nature of the condition i~1 doubt, bronchoscopic examination was not carried out. The subse- quent course was against diagnosis of tumour, benign or malignant.
(iv) Extrinsic pressure on the eparterial bronchus by enlarged para t racheal glands (? tuberculosis) is also a possible diagnosis; the subsequent relief of compression with re-expansion of the lobe
622 I R I S H J O U R N A L OF M E D I C A L S C I E N C E
being due to shrinkage os these glands. I f the paratracheal gland~ are f requent ly affected, as some authorities maintain, one would expect the occurrence of pulmonary opacities to be more frequent, especially in children. I t may well be indeed that the radiological opacities seen in the condition of " epituberculosis " are due to such compression of a bronchus and not to infiltration of the lung.
(v) Lastly, some authorities would maintain that this case is one of epituberculosis. Against such a diagnosis is the fact tha t the pat ient has been a city tenement dweller since birth, and there- fore the condition is not likely to be an allergic phenomenon due to first contact or infection with B. Tuberculosis. Fur ther , so fa r as I am aware, epitube~culosis is not complicated by an adherent pleura, and at any rate one would not expect it to be; see pneum~ thorax result above. In m y opinion, the first and four th diagnostic possibilities seem to be most likely.
The most favourable feature of this case is that the patient has recovered, and is capable of earning her livelihood, despite al! conjectures and diagnostic wranglings. Open air, rest and goo~ diet proved quite effectual treatment.
Ga'awp I lL Neopla'st~c. C~s~ 14. A. O'N., female, mr. 57 years. History.--In hospital
January-February, 1~6, with right-sided " pleurisy "--malignancy queried. Readmitted to hospital on March 23rd, 1936, complaining of cough and sputum for previous seven weeks and pain in right side of chest.
~Absolute dullness over right lower lobe, especially in axillary area, where also the breath sounds and vocal resonance were absent. Six to seven ounces of purulent sputum daily--negative for T.B., malignant cells and hydatid hooklets. Some bloodstained fluid removed f.rom right pleura, negative for T.B. on culture: polymorphonuclears the predominant cell present; no hydatid hooklets found. Wassermann test negative. Blood examination yielded normal result.
X-ray Repo.rts.--Plain film shows lower half of right lung field to be uniformly opaque. (Fig. 12.)
Later film (using Lysbolm grid) showed extensive calcareous changes in this opaque area--diagnosis, tumour (fibroma or hydatid cyst).
Lipiodol did not enter this opaque area. Lipiodol shows displacement of lower bronchial tree ,and compression of bronchi. Mediastinum drawn towards affected side: heart not displaced to the left. (Fig. 13.)
Casoni and .complement fixation tests for hydatid cysts were negative. Bronchoscopic examination and report.--Abundant discharge from right
lower bronchus; no definite evidence of malignancy; probable diagnosis, abscess.
'All other systems were normal. Thoracotomy was performed by Mr. A. B. Clery and a large calcareous
tumour successfully removed, which originated from the diaphragm near the spinal column. This proved to be a fibroma with calcareous changes. The patient progressed favourably for two days after )peration. On the third night she died suddenly, from what was evidently a pulmonary embolus.
I n this case at first the diagnosis was also problematic, but modern radiological technique and interpretat ion gave the most probable diagnosis, later proven at operation.
CASE ]5. Male, rot. 32 years--flour miller. Had been three months ill before admission to hosp'ital, which illness he stated was pneumonia; hmmoptysis early in this illness.
N O N - T U B E R C U L O U S P U L M O N A R Y C O N D I T I O N S 623
Marked general wasting. Dullness with diminished breath sounds over whole left thorax; apex beat displaced to the left. Intercostal spaces on left side very narrow. Scanty sputum, negative for T.B. Secondary anaemia, white blood cells numbered 8,600 on admission and four weeks later numbered 15,900 (polymorphonuclear predominance).
Small quanti ty of bloodstained fluid twice removed from left pleura Culture sterile on each occasion; at second examination of this fluit acid-fast bacilli were found, not typical of B. tuberculosis.
X-ray Report.--Left lung uniformly opaque and fibrosed; heart am trachea displaced to the left ; r ight lung normal.
Lipiodol reveals complete block of left main bronchus, not far from tracheal bifurcation. (Films not reproduced.)
Bronchoscopic examination suggests compression of left bronchus from without rather than intrinsic growth.
Pa t i en t was pyrexial (100 ~ F.-102 ~ F.) for seven successive days and had slight pyrexia (99.4 ~ F.) on a few other occasions during his ten weeks' stay in hospital. Pa t i en t left hospital, and did not report for fur ther examination.
Th is p a t i e n t ' s a c tua l p u l m o n a r y condi t ion was, a n d s t i l l is, in doub t . Unreso lved p n e u m o n i a w i th concomi tan t e m p y e m a could h a v e a c c o u n t e d f o r t h e p u l m o n a r y f ibrosis . C o m p r e s s i o n of a b r o n c h u s b y f ib ro t ic l u n g is, I shou ld t h i n k , r a r e , a n d such m a r k e d f ibros is is also n o t f r e q u e n t in m a l i g n a n t cond i t ions .
CAsE 16.--Male, eet. 45--rai lway worker. Loss of energy and appeti te , frequent vomiting since July, 1936. Paroxysms of cough with l i t t le sputum at night. Dullness over left thorax, breath sounds absent over upper lobe; rhonchi heard over both lungs. Marked tenderness on palpa tion below left scapular angle, and slight swelling in same area. Thick ])us removed from left pleura in axillarv area; sterile on culture; polv morphonuclear cells present, no organisms found. Pa t i en t was apyrexial
X-ray Report.--Left upper lobe opaque, r ight lung normal. Lipiodol shows cylindrical bronchiectasis in left lower lobe; uppe.,
bronchi not completely filled. (Fig. 14.) Thoracotomy was performed by Mr. Clery in left axil lary area. Lung
found to he adherent to chest wall; lung substance hard in consistency incised by diathermy, large quanti ty of viscid purulent material removed, gauze plug inserted, drainage of small quant i ty of pus continued for a few days.
The diagnosis was suggestive of an original interlobar empyema which had eroded through upper lobe, producing massive fibrosis. Bronchoscopy was not .carr ied-out , -owing t o the rigid mediastinum and displaced trachea. Later, the pat ient complained of severe pain in the back, and the swelling increased in size. Biopsy of this swellin~ was refused; aspiration yielded just a l i t t le blood. A radiogram of the thoracic vertebrm at this sta~e revealed changes in two vertenrm sugges~lve or malignancy. The pat ient progressed steadily downwards and, I am told, recently died.
Th is case was u n d o u b t e d l y one of b ronch ia l ca rc inoma, wi th low g r a d e p u r u l e n t d e g e n e r a t i o n of col lapsed u p p e r lobe d i s t a l to the b ronch i a l block. The slow, s i l en t onset a n d p r o g r e s s of the con- d i t ion , w i th r ea sonab ly good hea l t h fo r a cons ide rab le per iod , is q u i t e common wi th b r o n c h i a l ca rc inoma, and d e a t h m a y no t occur fo r two, three , or even f o u r y e a r s a f t e r the onset o f symptoms . I n th i s p a r t i c u l a r case, f r om rad io log ica l a n d mac roscop ica l f indings, the c a r c i n o m a had e v i d e n t l y been p r e sen t fo r some t ime be fore p a t i e n t came u n d e r observa t ion .
Chs~ 17.--J. c . , male, ~et. 46 years. Admitted to hospital in August 1935, for investigation of plum-shaped hard lump in r ight supraclavicular
To ]ace page 624
~2
~.~ J
bf~,---~
~J
S~
~ o ~
0
o.~
o
~ o
~ 2
rT

~ c~
C~
o~
c~
~ ~
c~
c~
0
~ ~.~ ~,~-~.~ ~'~=
�9
~ 0
~.~ o
~Q
c~
o ~ ~
,~.~
c~
~ ~

, ' o o o
;.~ .
o r ~
~ ' ~
~ ~ . ~
o ~
~o~
r n ~
o ~
~ �9 0
o ~ 0

624 I R I S H J O U R N A L O F M E D I C A L S C I E N C E
area. Complained of slight breathlessness at night, and pain in right shoulder. Pneumonia three years previously.
Lump in neck was removed for histological examination and reported to be secondary carcinoma of bronchogenie type.
Dullness over right upper lobe, with diminished breath sounds, venous arborisation on thorax and abdomen.
X-ray Report.--Consolidation of right upper lobe, possibly collapsing lobe.
Lipiodol--did nob fill over consolidated area; smaller bronchi partially and irregularly filled. Right diaphragm elevated 2 ins. ; paralysis of phrenic nerve (?).
Diagnosis--Bronchial neoplasm. An attempt to induce artificial pneumothorax (as a further possible aid
to diagnosis and to facilitate lobectemy, if the latter were contem- plated) failed, owing to adhesion of right upper lobe to chest wall. Pat ient treated by deep x-ray ~herapy at City of Dublin Skin and Cancer Hos- pital ; condition became rapidly worse and treatment was stopped; patient died a week later.
The p r a c t i c a l l y comple te absenee of r e s p i r a t o r y s y m p t o m s d u r i n g the ea r l i e r stages of th is ease, before the secondary g l and appeared, robbed the pa t i en t of possible benefits of ea r ly t r ea tmen t , whether opera t ive or radio- therapeut ic .
CAss 18. J. O'R., male, ~et. 58 years. Complaining of cough, sputum and slight h~emoptysis. Family history good. Previous illnesses, influenza 18 years ago, enteric fever 19 years ago. Cough worse at night ; loss of weight; appetite good; no dyspnoea.
Subresonance in left axitla; pleural rub over left lower and mid-zones. Blood-pressure 138/70. Wassermann test negative. Sputum negative
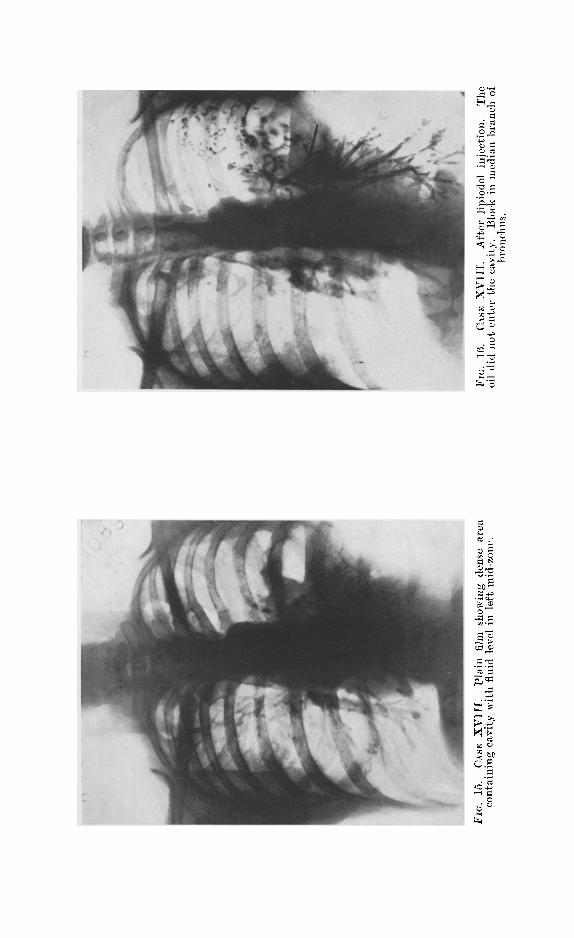
for T.B.; mitotic cells on repeated examinations. Electrocardiogram showed evidence of myocardial disease. X-ray Report.--Lipiodol showed block of bronchus in left mid-zone,
with a massive shadow distal to block, central cavity with fluid level which did not fill with lipiodol, deformity of median bronchus. (Figs. 15 and 16.)
Bronchoscop~c examination strongly suggested carcinoma of bronchus; owing to restlessness of patient, material for biopsy could not be obtained.
Pat ient received a full course of deep x-ray therapy from Dr. F. O. Pilkington at City of Dublin Skin and Cancer Hospi tal Result so far very satisfactory.
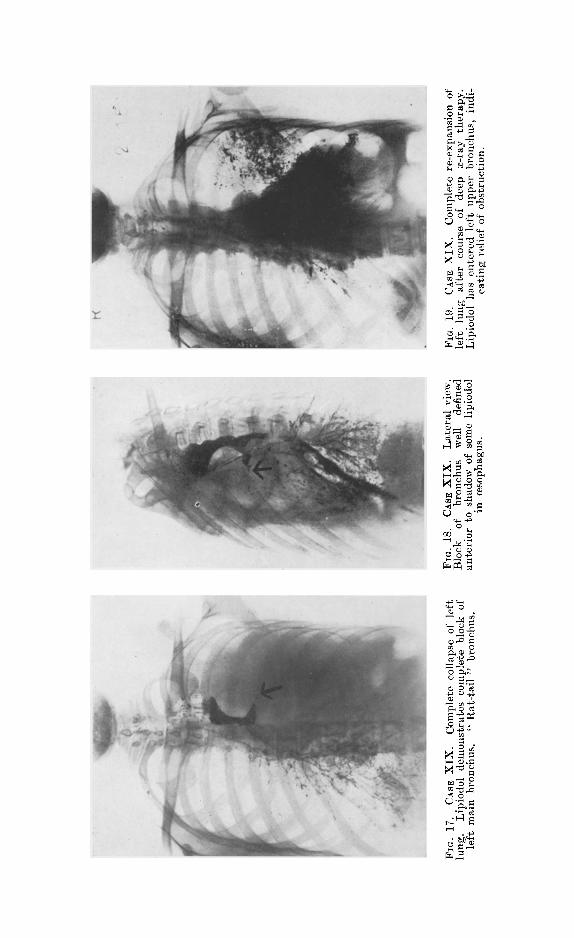
CAs~ 19. M. E., female, ~et. 51 years. !Admitted in March, 1936, with vomit ing and cough after meals. Six months previous to admission developed pain in lef~ axillary region; for two months prior to admission had slight recurrent attacks of h~emoptysis. Loss of weight.
Dullness over left thorax; bronchial and broncho-vesicular breathing over corresponding area.
X-ray Report.--Preliminary film showed complete opacity of left side suggesting a total collapse of lung, for there was no displacement of the heart towards the opposite side. A barium emulsion demonstrated a con- striction of the oesophagus at level of 7th dorsal vertebra with a displace- merit towards the left side. Though the oesophagus was constricted the emulsion passed through fairly well, showing a normal stomach and duodenum. (Figs. 17, 18, t9.)
Lipiodol injection demonstrated a block of the ]eft main bronchus, the constriction tapering to a fine point.
Diagnosis: Carcinoma of left bronchus; the constriction of the oesophagus being presumably due to extrinsic pressure factors t,ond not to an intrinsic growth.
Bronchoscopic exami~ation revealed a carcinoma of bronchus, which was confirmed by biopsy.
Deep x-ray therapy was administered by Dr. O. Chance with resultant complete re-expansion of left lung. Unfortunately, six weeks later multiple metastases appeared, involving the skin end spine, with a fatal termination two months later.
NON-TUBERCULOUS P U L ~ O N A R u C O N D I T I O N S 625
This is another case i l lus t ra t ing the insidious onset of bronchial carcinoma, with symptoms not relat ive to the r e sp i r a to ry system.
CASE 20. Male, mr. 43 years, referred to Dr. Stafford Johnson in 1934, with complaint of dyspnoea and slight recurrent h~emoptysis. Indurated discrete glands were present on the left side of the neck and biopsy demonstrated secondary bronchogenic carcinoma. Physical examination revealed diminished resonance and air entry over the left lower lobe. Lipiodol examination not satisfactory. Deep x-ray therapy produced ill-effect.
Lobectomy was successfully performed by Mr. J. H. Coolican in April, ]934. Patient lived for nine months, in a reasonably good state of health, and died at home from unascertained cause.
The second group of cases is impor tan t as a demonstrat ion of different ia l diagnosis in pu lmonary opacities, and again i l lustrates the invaluable aid of in t ra t rachea l lipiodoh
As an ind ica t ion of the necess i ty fo r de t a i l ed examina t ion in r e s p i r a t o r y disease, i t may be ment ioned t h a t an even l a rge r series of non-tuberculous cases as quoted above were diagnosed by these means, but were not included in this communication to avoid duplicat ion.
I t would not be just if iable to evaluate the re la t ive meri ts of opera t ive and deep x - r ay t h e r a p y in b ronch ia l carc inoma f rom the smal l number of eases considered.
In conclusion I wish to thank my medical and surgical colleagues at the Richmond Hospital and the City of Dublin Skin and Cancer Hospital for their help and for suggestions in the management of these cases. In particular I wish to thank Dr. T. G. Hardman for his painstaking inter- pretation of the films. I should also like to thank Mr. Murphy, our radiographer, for the keen interest he has shown in the radiography of these cases. Their work illustrates how essential is expert radiological technique in this particular branch of modern medicine. To Dr. J. Duffy, of the Dublin City Tuberculosis Dispensary, I am indebted for having referred several of these patients for special investigation.
LABORATORY TECHNICIANS' ASSOCIATION, I.F.S.
Etnployers requiring skilled laboratory technicians are requested to notify the Hon. Sec., Mr. W. Kampff, School of Pathology, Trinity College, Dublin.