sleep duration in midlife and later life in relation to cognition
TRANSCRIPT

CLINICAL INVESTIGATIONS
Sleep Duration in Midlife and Later Life in Relation toCognition
Elizabeth E. Devore, ScD,* Francine Grodstein, ScD,*† Jeanne F. Duffy, PhD,‡ Meir J. Stampfer,MD, DrPH,*†§ Charles A. Czeisler, PhD,‡ and Eva S. Schernhammer, MD, DrPH*†
OBJECTIVES: To evaluate associations between sleepduration at midlife and later life and change in sleep dura-tion over time and cognition in older women.
DESIGN: Participants reported sleep duration in 1986and 2000, and a subgroup of older participants begancognitive testing in 1995 to 2001; follow-up testing wasconducted three times, at 2-year intervals.
SETTING: Prospective Nurses’ Health Study cohort.
PARTICIPANTS: Female nurses aged 70 and older free ofstroke and depression at the initial cognitive assessment(N = 15,385).
MEASUREMENTS: Validated, telephone-based cognitivebattery to measure cognitive function; four repeated assess-ments over 6 years were averaged to estimate overall cog-nition at older ages, and trajectories of cognitive changewere evaluated over follow up.
RESULTS: Extreme sleep durations in later life were asso-ciated with worse average cognition (P < .001 for the qua-dratic term for a global score averaging all six cognitivetests). For example, women sleeping 5 h/d or less hadworse global cognition than those sleeping 7 h/d, as didwomen sleeping 9 h/d or more; differences were equivalentto nearly 2 additional years of age. Associations were simi-lar, although slightly attenuated, for sleep duration in mid-life. Women whose sleep duration changed by 2 h/d ormore over time had worse cognition than women with nochange in sleep duration (e.g., for the global score,P < .001 for the quadratic term). Sleep duration was notassociated with trajectories of cognitive function over6 years, which might be attributable to short follow-up fordetecting cognitive decline.
CONCLUSION: Extreme sleep durations at midlife andlater life and extreme changes in sleep duration over timeappear to be associated with poor cognition in olderwomen. J Am Geriatr Soc 2014.
Key words: sleep; cognition; epidemiology; cohort study
Approximately 30% of U.S. adults have usual sleepdurations outside of 7 to 8 h/d—a percentage that
increases with advancing age,1 yet growing epidemiologicalevidence suggests that shorter or longer sleep durations areassociated with higher risks of cardiovascular disease2 andtype 2 diabetes mellitus,3 both of which have been stronglylinked to cognitive impairment and Alzheimer’s disease;4
there is thus increasing interest in examining the relation-ship between sleep duration and cognitive function inolder adults. In addition to indirect effects of sleep dura-tion on cognitive health through vascular mechanisms,there might be a direct effect on the brain; experimentalstudies in mice have demonstrated that shorter sleep cancause accumulation of beta-amyloid in the brain5—a hall-mark Alzheimer’s disease pathology. Several epidemiologi-cal studies have evaluated sleep duration and cognitivefunction in later life, with varying results,6–19 but mostprevious studies have been cross-sectional, and no studieshave investigated sleep duration in midlife and later life.Thus, sleep duration was evaluated in the Nurses’ HealthStudy (NHS) at both of these time points—and change insleep duration between these two points—in relation tocognitive performance in later life.
METHODS
The NHS began in 1976, when 121,701 female nursesaged 30 to 55 returned a mailed questionnaire on healthand lifestyle. Biennial questionnaires are used to updatethis information, and follow-up is 90%. Women reportedtheir sleeping habits in 1986 (midlife) and 2000 (later life);
From the *Department of Medicine, Channing Division of NetworkMedicine, Brigham and Women’s Hospital, Harvard Medical School,†Department of Epidemiology, School of Public Health, HarvardUniversity, ‡Division of Sleep Medicine, Department of Medicine, Brighamand Women’s Hospital, and §Department of Nutrition, School of PublicHealth, Harvard University, Boston, Massachusetts.
Address correspondence to Dr. Elizabeth E. Devore, 181 LongwoodAvenue, Room 452, Boston, MA 02115.E-mail: [email protected]
DOI: 10.1111/jgs.12790
JAGS 2014
© 2014, Copyright the Authors
Journal compilation © 2014, The American Geriatrics Society 0002-8614/14/$15.00

in 1995 to 2001, a telephone-based cognitive study wasinitiated for participants aged 70 and older with no strokehistory. Of eligible women, 19,415 (92%) completed aninitial cognitive assessment, which was repeated threetimes at 2-year intervals (median time between the firstand fourth interview 6.4 years); more than 90% of thesewomen completed at least one follow-up assessment. Theinstitutional review board of Brigham and Women’s Hos-pital (Boston, MA) approved this study. Participants pro-vided implied consent by returning the questionnaires andoral consent for the cognitive study.
Population for Analysis
Of 19,415 women who completed the initial cognitiveassessment, 1,825 were excluded because they had depres-sion (potentially a strong confounding factor) before theinitial cognitive assessment; another 2,103 nursing homeresidents were excluded because an institutional environ-ment might influence sleep duration. Of 15,487 remainingparticipants, 2,435 did not report sleep duration in midlife,leaving 13,052 women for analyses of sleep duration inmidlife and cognition; 224 did not report sleep duration inlater life, which left 15,263 for analyses of sleep durationin later life and cognition. Important characteristics weresimilar between participants included in the analyticalsample and those who were excluded because they lackedsleep data (e.g., mean age 74.2 vs 74.4, mean body massindex 25.6 vs 26.1 kg/m2).
Ascertainment of Sleep Duration
Women reported their usual hours of sleep in a 24-hourperiod on the 1986 and 2000 questionnaires; response cat-egories were 5 or less, 6, 7, 8, 9, 10, and 11 or morehours. In a validation study, 260 NHS participants com-pleted a sleep diary over 6 days; a single questionnaire-based report of sleep duration correlated highly with sleepduration recorded in these diaries (q = 0.79).20
Ascertainment of Cognitive Function
The Telephone Interview of Cognitive Status (TICS), atelephone version of the Mini-Mental State Examination,was initially administered; these tests are highly correlated(q = 0.97).21 After establishing high participation rates,five additional tests were added: East Boston Memory Testimmediate and delayed recall, category fluency, delayedrecall of the TICS 10-word list, and digit span back-ward.22–24 In a validation study, a telephone-basedcognitive battery performed as well as detailed, 1-hour, in-person interviews conducted by a neuropsychologist in 61women aged 70 and older (q = 0.81 comparing the twoassessment modes).25 Interinterviewer reliability was highacross 10 interviewers each scoring the same cognitiveinterview (q > 0.95 for each cognitive test).
Three primary outcomes were selected a priori: twomeasures of general cognition (a global score averaging allsix cognitive tests and the TICS score) and a verbal mem-ory score (averaging immediate and delayed recall fromthe East Boston Memory Test and TICS 10-word list).Verbal memory is the strongest predictor of Alzheimer’s
disease.26 Because the six cognitive tests are scaled differ-ently, z-scores were used to create composite measures bycalculating the difference between each participant’s scoreand the mean score for the study population divided bythe population standard deviation, relevant z-scores werethen averaged to calculate the global and verbal scores.Individual cognitive test scores were considered as second-ary outcomes.
Statistical Analysis
Two approaches to modeling the repeated measures ofcognitive function were used. First, sleep duration in mid-life (measured in 1986, when women were aged 56–66),sleep duration in later life (measured in 2000, whenwomen were aged 70–80), and change in sleep duration(between midlife and later life) were evaluated in relationto “average” cognitive performance, which was calculatedby averaging all four repeated cognitive assessments.Because these assessments were ascertained over a shortperiod (6 years), this outcome provides the most statisti-cally stable estimate of the women’s overall cognitive sta-tus in later life. For these analyses, multivariable-adjustedlinear regression were used to estimate mean differences inaverage cognition for each of the categories of sleep dura-tion (≤5, 6, 7, 8, ≥9 h/d); the reference category was7 hours of sleep per day. Second, the associations betweensleep duration and change in sleep duration and cognitivedecline were examined over 6 years of follow up. Nonlin-earity in cognitive trajectories was found because of“learning effects,” primarily between the first and secondinterviews. (That is, there was an average increase in cog-nitive scores between the first and second assessmentsbecause of participants’ familiarity with the tests, followedby an average decline in scores at the third and fourthinterviews.) Thus, test scores at the first and second cogni-tive assessments were averaged to obtain a “robust base-line” score (as described previously27); this method yieldedlinear cognitive trajectories over time. Multivariable-adjusted mixed linear regression was then used to estimaterates of cognitive decline for the same exposure categoriesdescribed above. Specifically, repeated-measures modelingwith random intercepts and slopes, which permits descrip-tion of individual cognitive trajectories over time and pro-vides explicit tests of association between sleep durationand rates of cognitive decline, were used; 95% confidenceintervals (CIs) were calculated for all effect estimates, anda quadratic term was used to test for inverted, U-shapedassociations. The partial F-test was used to evaluate therelative contribution of sleep duration in midlife versuslater life in predicting cognitive performance.28
Many possible confounding factors were considered,including age, education (registered nursing degree, bache-lor’s degree, graduate degree), shift work history (never,1–9, 10–19, ≥20 years), smoking status (never, past, cur-rent), alcohol intake (none, 1–14, ≥15 g/d), physical activ-ity (in quintiles of metabolic equivalent h/wk), body massindex (<22, 22–24, 25–29, ≥30 kg/m2), history of highblood pressure (yes, no), Medical Outcomes Study 36-itemShort-Form Survey mental health score (≤52 points (poormental health), >52 points (normal mental health)), livingalone (yes, no), and tranquilizer use (yes, no).
2 DEVORE ET AL. 2014 JAGS

Several secondary analyses were conducted. First, theanalyses of change in sleep duration and cognitive functionwere stratified according to midlife sleep duration toexamine whether associations were strongest in womenwho initially reported “normal” sleep duration (7 h/d).Second, women who reported a history of shift work wereexcluded because shift work might have strongly influ-enced sleep duration and perhaps cognitive function, soshift work history might be a substantial confounding fac-tor. Third, secondary analyses of sleep duration in laterlife and cognition were conducted, excluding women inthe bottom 10% of the cognitive score distribution. Theseanalyses were intended to address concern about the cross-sectional nature of the analyses focused on sleep in laterlife; specifically, because individuals with greater cognitiveimpairments are more likely to have sleep disturbances, itis possible that any observed associations might reflect theinfluence of pathological processes in the brain on sleepduration in these individuals (reverse causation). There-fore, women with the worst cognitive scores (bottom 10%of the score distribution) were excluded to evaluatewhether associations remained after removing thesewomen from the analyses.
Analyses were performed using SAS version 6.0 (SASInstitute, Inc., Cary, NC).
RESULTS
Table 1 shows participant characteristics in midlife accord-ing to category of sleep duration in midlife. Few meaning-ful differences in these characteristics were observed,although women with shorter and longer sleep durationshad somewhat lower physical activity levels than womenwith 7 hours of sleep per day. Table 2 shows participantcharacteristics in later life according to category of sleepduration in later life. Few substantial differences werefound, although women with shorter and longer sleepdurations had higher body mass indexes and lower physi-cal activity levels than women who reported 7 hours ofsleep per day. Women with the shortest sleep durationwere also more likely to live alone than other women inthe study.
In general, models adjusted for age and educationyielded results similar to those of models adjusted formultiple potential confounding factors. Here, results arepresented from fully adjusted models only.
When the association between sleep duration in mid-life and cognition was examined, an inverted U-shapedassociation was observed for the global score and the TICSscore (P = .002 and P < .001 for the quadratic terms,respectively; Figure 1). For example, women reporting5 hours or fewer of sleep per day had average globalscores that were lower by 0.04 standard units than thosewith 7 hours of sleep per day (mean score �0.06 standardunits, 95% CI = �0.12 to 0.00 standard units vs �0.02standard units, 95% CI = �0.06 to 0.02 standard units),whereas women with 9 hours or more of sleep had aver-age scores that were 0.07 standard units lower than thosesleeping 7 h/d (mean score �0.09 standard units, 95%CI = �0.15 to �0.04 standard units vs �0.02 standardunits, 95% CI = �0.06 to 0.02 standard units). Associa-tions were observed for all individual cognitive tests,except for those contributing to verbal memory score. Sim-ilar associations, but slightly stronger, were found for sleepduration in older age and average cognition for all threeprimary outcomes (P < .001 for the quadratic term for theglobal, verbal, and TICS scores; Figure 2). For example,women who slept 5 h/d or less had average global scoresthat were 0.06 standard units lower than women sleeping7 h/d (mean score �0.07 standard units, 95% CI = �0.11to �0.02 standard units vs �0.01 standard units, 95%CI = �0.04 to 0.02 standard units); in addition, womensleeping 9 h/d or more had worse global scores by 0.10standard units than women with 7 hours of sleep per day(mean score �0.11 standard units, 95% CI = �0.15 to�0.06 standard units vs �0.01 standard units, 95%CI = �0.04 to 0.02 standard units). These associationswere evident for all six of the cognitive tests. When sleepduration in mid- and later life were included in the samemodel, sleep duration in later life contributed significantinformation to the model (F4,∞ = 6.09 > 2.37, P < .001),but sleep duration in midlife did not (F4,∞ = 1.33 < 2.37,P = .30); thus, sleep duration in later life was morestrongly associated with cognitive performance in later life
Table 1. Characteristics of Study Participants According to Category of Sleep Duration in Midlife (Reported in1986)
Characteristic
≤5 h/d,
n = 577
6 h/d,
n = 3,302
7 h/d,
n = 5,432
8 h/d,
n = 3,356
≥9 h/d,
n = 626
Age, mean 60.9 61.0 61.0 61.2 61.5Master’s or doctoral degree, % 7 7 7 6 5Never smoker, % 48 47 48 49 45Alcohol intake none, % 39 37 34 37 35Body mass index, kg/m2, mean 25.4 25.3 25.0 25.4 25.6Physical activity, metabolic equivalent h/wk, median(interquartile range)a
6.6 (2.3–18.3) 7.9 (2.9–20.0) 8.8 (3.2–20.2) 7.9 (2.9–20.2) 7.7 (2.7–17.2)
History of high blood pressure, % 34 34 32 34 36Poor Medical Outcomes Study 36-item Short-Form Surveymental health score, %
7 4 4 4 5
Living alone, % 20 20 17 15 16Use of tranquilizers, % 4 2 2 2 4
These numbers reflect nonmissing values.aA metabolic equivalent hour is equal to the amount of energy expended while sitting quietly for 1 hour.
JAGS 2014 SLEEP DURATION AND COGNITION 3

than sleep duration in midlife. Each year of age in thecohort was associated with a decrease of 0.05 standardunits on the global score; thus, the observed mean scoredifferences of 0.04 to 0.10 standard units between extremecategories of sleep duration and 7 hours of sleep per daywere equivalent to 1–2 years of cognitive aging.
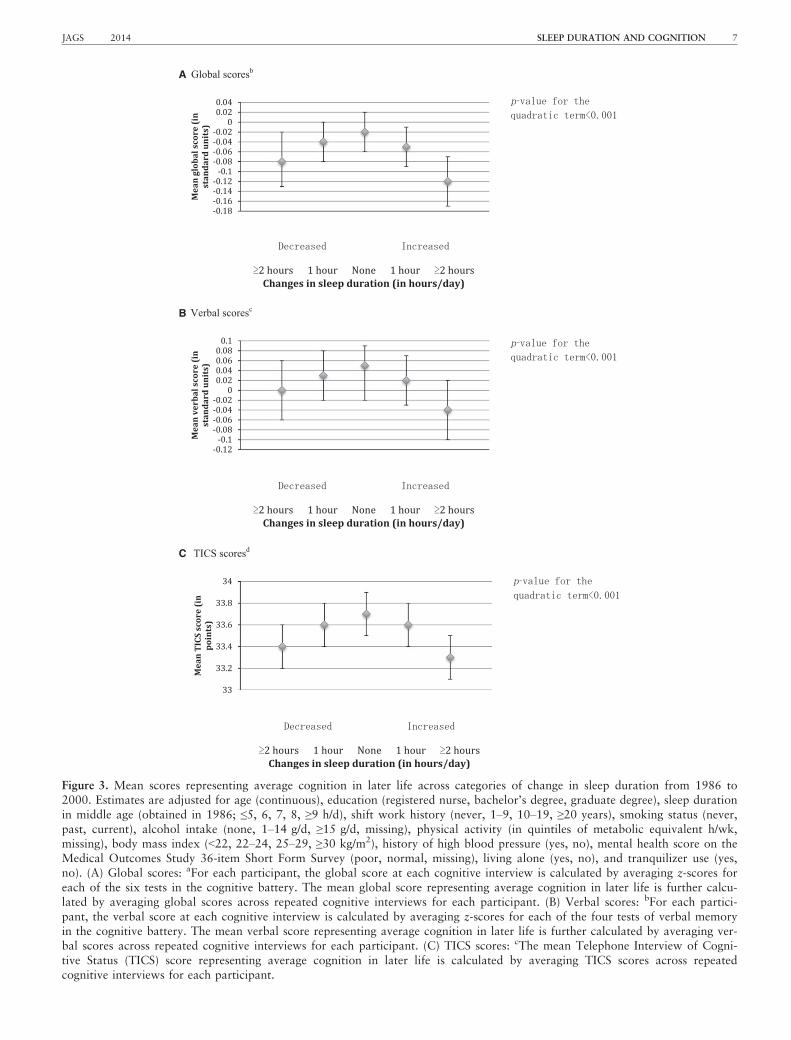
In the analysis of change in sleep duration (frommiddle to older age) and average cognition, an invertedU-shaped association was also observed for all three cogni-tive outcomes (P < .001 for the quadratic terms for theglobal, verbal, and TICS scores; Figure 3). For example,the mean global score was 0.06 standard units lower forwomen who reported changes in sleep duration thatincreased or decreased by 2 hours or more over time (13%of the cohort) than for women reporting no changes insleep duration (42% of the cohort; e.g., mean score �0.08standard units, 95% CI = �0.13 to �0.02 standard unitsand �0.12 standard units, 95% CI = �0.17 to �0.07standard units vs �0.02 standard units, 95% CI = �0.06,0.02 standard units). Associations were consistent for allindividual cognitive tests, and the magnitude of theseeffects was approximately equivalent to 1 to 2 years ofcognitive aging.
When cognitive trajectories in later life were analyzed(change in cognitive performance over the four assess-ments), there were no associations between sleep durationin midlife, sleep duration in later life, or change in sleepduration from midlife to later life and cognitive decline.
In secondary analyses, associations between extremesleep duration and worse cognitive function were strongestin women who reported normal sleep duration in midlife(7 h/d; e.g., mean global score = �0.14 standard units,95% CI = �0.24 to �0.03 standard units vs �0.01 stan-dard units, 95% CI = �0.07 to 0.05 standard units forwomen with ≥2-hour decreases in sleep per day vs nochange in sleep duration, and mean global score = �0.14standard units, 95% CI = �0.22 to �0.05 standard unitsvs �0.01 standard units, 95% CI = �0.07, 0.05 standardunits for women with ≥2 hour increases in sleep/day, com-pared with those with no changes in sleep duration).Analyses excluding women with a history of shift work
did not change the results materially, nor did analyses thatexcluded women in the bottom 10% of the score distribu-tion in analyses of sleep duration in older age.
DISCUSSION
The current study found that, shorter and longer sleepduration in women in mid- and later life were associatedwith worse average cognition in later life than normalsleep duration (7 h/d), with sleep duration in later lifebeing more strongly associated with cognition than sleepduration in midlife. Changes in sleep duration of 2 h/d ormore between middle and older age were also related tolower cognitive performance in later life. In general, hav-ing shorter or longer sleep duration was cognitivelyequivalent to aging 1 to 2 years. No associations wereobserved between sleep duration or change in sleep dura-tion and rate of cognitive decline over time, which mightbe due to relatively short follow-up, so average cognitivefunction may be a better measure of cognitive status inthis cohort.
To the knowledge of the authors, this is the firststudy to examine the association between sleep durationin mid- and later life and cognitive performance in olderadults. The findings are consistent with some, but not all,epidemiological studies in which sleep duration and cogni-tion have been measured in later life. Most studies havebeen modest in size and cross-sectional, and findings havebeen mixed but tend to suggest that shorter7,8,19 andlonger10–12 sleep durations or both14–16 are associatedwith worse cognitive function. The largest of these studiesis a cross-sectional investigation of 28,670 older Chineseadults that found that shorter and longer sleep durationwas associated with worse scores on a delayed wordrecall test (multivariable-adjusted P-trend < .001 for cate-gories of sleep duration from 3 to 4 to 7 h/d; P-trend < .001 for categories of sleep duration from 7 to≥10 h/d).16 In contrast, one prospective study (N = 1,664)was less clear, finding that short sleep duration was asso-ciated with greater risk of cognitive impairment in men(odds ratio (OR) = 2.91, 95% CI = 1.24–6.82, ≤5 vs
Table 2. Characteristics of Study Participants According to Category of Sleep Duration in Later Life (Reported in2000)
Characteristic
≤5 h/d,
n = 920
6 h/d,
n = 3,484
7 h/d,
n = 5,379
8 h/d,
n = 4,257
≥9 h/d,
n = 1,223
Age, mean 74.3 74.3 74.1 74.2 74.5Master’s or doctoral degree, % 4 5 6 6 8Never smoker, % 47 46 48 47 45Alcohol intake none, % 55 49 47 49 52Body mass index, kg/m2, mean 26.0 25.5 25.3 25.8 26.3Physical activity, metabolic equivalent h/wk, median(interquartile range)a
7.9 (2.3–20.2) 9.9 (3.4–22.5) 10.9 (3.7–22.9) 10.2 (3.2–22.2) 7.6 (2.1–18.5)
History of high blood pressure, % 60 55 52 55 60Poor Medical Outcomes Study 36-item Short-Form Surveymental health score, %
8 4 2 2 4
Living alone, % 37 36 32 29 28Use of tranquilizers, % 8 5 4 4 6
These numbers reflect nonmissing values.aA metabolic equivalent hour is equal to the amount of energy expended while sitting quietly for 1 hour.
4 DEVORE ET AL. 2014 JAGS

5–9 hours of sleep/night), but long sleep duration wasassociated with greater risk of cognitive impairment inwomen (OR = 2.10, 95% CI = 1.10–4.00, ≥9 vs 5–9 hours of sleep/night).18
In addition, two previous studies reported on changein sleep duration over time and cognition in olderadults.13,15 In the German Heidelberg longitudinal study
(n = 409), participants whose sleep duration increasedfrom 7 to 8 to more than 8 hours of sleep per night over10 years had greater odds of cognitive impairment at theend of follow-up than those with no change in sleep dura-tion.13 The Whitehall study (N = 1,457) found a similarassociation with cognitive function for individuals withincreased sleep duration versus no change in sleep duration
A
B
C
Figure 1. Mean scores representing average cognition in later life according to category of sleep duration in midlife (reported in1986). Estimates are adjusted for age (continuous), education (registered nurse, bachelor’s degree, graduate degree), shift workhistory (never, 1–9, 10–19, ≥20 years), smoking status (never, past, current), alcohol intake (none, 1–14 g/d, ≥15 g/d, missing),physical activity (quintiles of metabolic equivalent h/wk, missing), body mass index (<22, 22–24, 25–29, ≥30 kg/m2), history ofhigh blood pressure (yes, no), mental health score on the Medical Outcomes Study 36-item Short Form Survey (poor, normal,missing), living alone (yes, no), and tranquilizer use (yes, no). (A) Global scores: afor each participant, the global score at eachcognitive interview is calculated by averaging z-scores for each of the six tests in the cognitive battery. The mean global scorerepresenting average cognition in later life is further calculated by averaging global scores across repeated cognitive interviewsfor each participant. (B) Verbal scores: bfor each participant, the verbal score at each cognitive interview is calculated by averag-ing z-scores for each of the four tests of verbal memory in the cognitive battery. The mean verbal score representing average cog-nition in later life is further calculated by averaging verbal scores across repeated cognitive interviews for each participant. (C)TICS scores: cthe mean Telephone Interview of Cognitive Status (TICS) score representing average cognition in later life is calcu-lated by averaging TICS scores across repeated cognitive interviews for each participant.
JAGS 2014 SLEEP DURATION AND COGNITION 5

over 5 years, although individuals with decreased sleepduration appeared to have worse cognitive function aswell.15 Both studies are consistent with the findings of thecurrent study in that greater changes in sleep duration overtime were related to worse cognition; thus, existing dataon this association generally support the current results,although evidence remains somewhat limited.
Several lines of evidence suggest biological linksbetween sleep duration and cognition. First, experimentalstudies involving mice have demonstrated that sleep depri-vation can lead to accumulation of amyloid beta in thebrain—a hallmark pathology of Alzheimer’s disease.5 Thesefindings indicate that sleep duration may have direct effectson the brain, although human studies have shown that sleep
A
B
C
Figure 2. Mean scores representing average cognition in later life according to category of sleep duration in later life (reported in2000). Estimates are adjusted for age (continuous), education (registered nurse, bachelor’s degree, graduate degree), shift workhistory (never, 1–9, 10–19, ≥20 years), smoking status (never, past, current), alcohol intake (none, 1–14 g/d, ≥15 g/d, missing),physical activity (quintiles of metabolic equivalent h/wk, missing), body mass index (<22, 22–24, 25–29, ≥30 kg/m2), history ofhigh blood pressure (yes, no), mental health score on the Medical Outcomes Study 36-item Short Form Survey (poor, normal,missing), living alone (yes, no), and tranquilizer use (yes, no). (A) Global scores: afor each participant, the global score at eachcognitive interview is calculated by averaging z-scores for each of the six tests in the cognitive battery. The mean global scorerepresenting average cognition in later life is further calculated by averaging global scores across repeated cognitive interviewsfor each participant. (B) Verbal scores: bfor each participant, the verbal score at each cognitive interview is calculated by averag-ing z-scores for each of the four tests of verbal memory in the cognitive battery. The mean verbal score representing average cog-nition in later life is further calculated by averaging verbal scores across repeated cognitive interviews for each participant. (C)TICS scores: cthe mean Telephone Interview of Cognitive Status (TICS) score representing average cognition in later life is calcu-lated by averaging TICS scores across repeated cognitive interviews for each participant.
6 DEVORE ET AL. 2014 JAGS
A
B
C
Figure 3. Mean scores representing average cognition in later life across categories of change in sleep duration from 1986 to2000. Estimates are adjusted for age (continuous), education (registered nurse, bachelor’s degree, graduate degree), sleep durationin middle age (obtained in 1986; ≤5, 6, 7, 8, ≥9 h/d), shift work history (never, 1–9, 10–19, ≥20 years), smoking status (never,past, current), alcohol intake (none, 1–14 g/d, ≥15 g/d, missing), physical activity (in quintiles of metabolic equivalent h/wk,missing), body mass index (<22, 22–24, 25–29, ≥30 kg/m2), history of high blood pressure (yes, no), mental health score on theMedical Outcomes Study 36-item Short Form Survey (poor, normal, missing), living alone (yes, no), and tranquilizer use (yes,no). (A) Global scores: aFor each participant, the global score at each cognitive interview is calculated by averaging z-scores foreach of the six tests in the cognitive battery. The mean global score representing average cognition in later life is further calcu-lated by averaging global scores across repeated cognitive interviews for each participant. (B) Verbal scores: bFor each partici-pant, the verbal score at each cognitive interview is calculated by averaging z-scores for each of the four tests of verbal memoryin the cognitive battery. The mean verbal score representing average cognition in later life is further calculated by averaging ver-bal scores across repeated cognitive interviews for each participant. (C) TICS scores: cThe mean Telephone Interview of Cogni-tive Status (TICS) score representing average cognition in later life is calculated by averaging TICS scores across repeatedcognitive interviews for each participant.
JAGS 2014 SLEEP DURATION AND COGNITION 7

deprivation also has adverse effects on cardiometabolic fac-tors (e.g., increasing blood pressure and insulin resis-tance),29,30 and cardiovascular and metabolic health havebeen associated with cognitive health in older adults.4 Thus,there is the potential for direct and indirect effects of sleepduration to influence cognitive status in later life. Anotherpossibility is that self-reported sleep duration might be amarker of sleep quality, as a study that found that partici-pants self-reporting extreme sleep durations also had themost objectively measured sleep fragmentation suggested.This study reported that, although extreme sleep durationand greater sleep fragmentation were each associated withpoor cognitive function in separate models, only sleep frag-mentation remained significantly associated with cognitionin models simultaneously adjusted for both variables. Thus,in the only large-scale epidemiological study that has evalu-ated these measures simultaneously, poor sleep qualityappears to explain much of the association between subjec-tive sleep duration and cognitive function.14 Moreover, arecent clinical study found that it is likely that poor sleepquality is a contributing factor to cognitive impairment inlater life.31 Alternatively, extreme sleep duration andextreme changes in sleep duration over time could be mark-ers of underlying circadian disruption, which have increas-ingly been related to cognitive decrements. For example,several studies have found that job-related circadian disrup-tions are associated with poorer short-term cognitive func-tion32–34 and possibly structural brain atrophy,33 andemerging investigations of objectively measured circadianrhythms have observed relationships between disturbedrhythms and cognitive impairment in older adults.35–37
These studies support the biological plausibility of the find-ings of the current study, although it is likely that the rela-tionship between sleep duration and cognition is complexand may be bidirectional.
Several limitations of this study should be considered.First, this is an observational study, and therefore the possi-bility cannot be excluded that residual confoundingexplains the observed associations. A wide variety of possi-ble confounding factors was controlled for, which did notchange the effect estimates substantially, suggesting thatresidual confounding by measured factors is less likely toexplain the findings, although unmeasured factors relatedto health status could still explain the results. For example,sleep-disordered breathing was not measured in this cohort,and this condition might influence sleep duration and riskof cognitive impairment.38 The prevalence of sleep-disor-dered breathing is relatively low in women and even lowerin younger women,39 suggesting that lack of adjustment forthis variable probably had a limited effect. This might havecaused associations between sleep duration and cognition,particularly those involving sleep duration in later life, tobe slightly underestimated because sleep-disordered breath-ing is somewhat more prevalent in later life. Second, partic-ipants self reported sleep duration, which probably led tosome random misclassification, although a previous valida-tion study found that these participants self-reported usualsleep duration well compared with sleep durations derivedfrom sleep diaries.20 In addition, several other studies in theNHS have reported that sleep duration is associated withmortality,20 coronary heart disease,40 and type 2 diabetesmellitus,41 providing reassurance that the measurement of
sleep duration used in the current study contains importantinformation for predicting health outcomes in this cohort.Third, although the analyses of sleep duration in midlifeand cognition were prospective (the exposure was measuredbefore outcome assessment), the evaluation of sleep dura-tion in later life and cognition could be subject to reversecausation bias if underlying cognitive health influencedsleep duration in these older women, but the results did notchange when women with the worst cognitive scores inlater life (women most likely to have underlying brainpathology that could affect sleep) were excluded, indicatingthat reverse causation is not likely to be completely respon-sible for observed associations. Finally, the period overwhich cognitive decline was measured was short (6 years),and no associations were observed between sleep durationand cognitive decline over 6 years, which stands in contrastto the associations observed between sleep duration andaverage cognitive status in later life; thus, follow-up mayhave been too short to capture the amount of decline neces-sary to detect significant associations. As noted above, aver-age cognitive status may provide a better reflection ofwomen’s later-life cognition in this cohort.
In conclusion, extreme sleep duration, including sleephabits in midlife, was associated with worse cognition inlater life. More extreme changes in sleep duration frommiddle to older age were related to worse cognitive func-tion as well. If future research supports these findings, clin-ical interventions based on sleep therapy should beexamined for the prevention of cognitive impairment.Future research is necessary to better understand the mech-anisms by which sleep duration might be associated withcognitive function, including measurement of objectivesleep assessments in middle-aged and older individuals.
ACKNOWLEDGMENTS
A preliminary version of these data was presented, in part,during an oral presentation at the Alzheimer’s AssociationInternational Conference, July 14 to 19, 2012, Vancouver,Canada.
Conflict of Interest: The editor in chief has reviewedthe conflict of interest checklist provided by the authorsand has determined that the authors have no financial orany other kind of personal conflicts with this paper.
The Nurses’ Health Study is funded by Grant P01CA87969 from the National Institutes of Health.
Author Contributions: Devore: conception and design,analysis and interpretation of data, drafting the article andrevising it for important intellectual content. Grodstein:conception and design, acquisition and interpretation ofdata, revising the article for important intellectual content.Duffy: interpretation of data, revising the article forimportant intellectual content. Stampfer: conception anddesign; acquisition, analysis, and interpretation of data;revising the article for important intellectual content.Czeisler, Schernhammer: conception and design, analysisand interpretation of data, revising the article for impor-tant intellectual content. All authors have given finalapproval of the version of this article to be published.
Sponsor’s Role: The sponsor played no role in thedesign, methods, subject recruitment, data collection,analysis, and preparation of this article.
8 DEVORE ET AL. 2014 JAGS

REFERENCES
1. Schoenborn CA, Adams PE. Health behaviors of adults: United States,
2005–2007. Vital Health Stat 2010;10:1–132.2. Cappuccio FP, Cooper D, D’Elia L et al. Sleep duration predicts cardiovas-
cular outcomes: A systematic review and meta-analysis of prospective stud-
ies. Eur Heart J 2011;32:1484–1492.3. Cappuccio FP, D’Elia L, Strazzullo P et al. Quantity and quality of sleep
and incidence of type 2 diabetes: A systematic review and meta-analysis.
Diabetes Care 2010;33:414–420.4. Gorelick PB, Scuteri A, Black SE et al. Vascular contributions to cognitive
impairment and dementia: A statement for healthcare professionals from
the American Heart Association/American Stroke Association. Stroke
2011;42:2672–2713.5. Kang JE, Lim MM, Bateman RJ et al. Amyloid-beta dynamics are regulated
by orexin and the sleep-wake cycle. Science 2009;326:1005–1007.6. Foley DJ, Masaki K, White L et al. Sleep-disordered breathing and cognitive
impairment in elderly Japanese-American men. Sleep 2003;26:596–599.7. Ohayon MM, Vecchierini MF. Normative sleep data, cognitive function
and daily living activities in older adults in the community. Sleep
2005;28:981–989.8. Tworoger SS, Lee S, Schernhammer ES et al. The association of self-
reported sleep duration, difficulty sleeping, and snoring with cognitive func-
tion in older women. Alzheimer Dis Assoc Disord 2006;20:41–48.9. Blackwell T, Yaffe K, Ancoli-Israel S et al. Poor sleep is associated with
impaired cognitive function in older women: The Study of Osteoporotic
Fractures. J Gerontol A Biol Sci Med Sci 2006;61A:405–410.10. Schmutte T, Harris S, Levin R et al. The relation between cognitive func-
tioning and self-reported sleep complaints in nondemented older adults:
Results from the Bronx Aging Study. Behav Sleep Med 2007;5:39–56.11. Faubel R, Lopez-Garcia E, Guallar-Castillon P et al. Usual sleep duration
and cognitive function in older adults in Spain. J Sleep Res 2009;18:
427–435.12. Kronholm E, Sallinen M, Suutama T et al. Self-reported sleep duration and
cognitive functioning in the general population. J Sleep Res 2009;18:
436–446.13. Loerbroks A, Debling D, Amelang M et al. Nocturnal sleep duration and
cognitive impairment in a population-based study of older adults. Int J Ge-
riatr Psychiatry 2010;25:100–109.14. Blackwell T, Yaffe K, Ancoli-Israel S et al. Association of sleep characteris-
tics and cognition in older community-dwelling men: The MrOS sleep
study. Sleep 2011;34:1347–1356.15. Ferrie JE, Shipley MJ, Akbaraly TN et al. Change in sleep duration and
cognitive function: Findings from the Whitehall II Study. Sleep
2011;34:565–573.16. Xu L, Jiang CQ, Lam TH et al. Short or long sleep duration is associated
with memory impairment in older Chinese: The Guangzhou Biobank
Cohort Study. Sleep 2011;34:575–580.17. Auyeung TW, Lee JS, Leung J et al. Cognitive deficit is associated with
phase advance of sleep-wake rhythm, daily napping, and prolonged sleep
duration-a cross-sectional study in 2,947 community-dwelling older adults.
Age (Dordr) 2013;35:479–486.18. Potvin O, Lorrain D, Forget H et al. Sleep quality and 1-year incident cog-
nitive impairment in community-dwelling older adults. Sleep 2012;35:
491–499.19. Keage HA, Banks S, Yang KL et al. What sleep characteristics predict
cognitive decline in the elderly? Sleep Med 2012;13:886–892.20. Patel SR, Ayas NT, Malhotra MR et al. A prospective study of sleep
duration and mortality risk in women. Sleep 2004;27:440–444.
21. Brandt J, Spencer M, Folstein M. The telephone interview of cognitive sta-
tus. Neuropsychol Behav Neurol 1988;1:111–117.22. Baddeley AD, Bressi S, Della Sala S et al. The decline of working memory
in Alzheimer’s disease. A longitudinal study. Brain 1991;114(Pt 6):
2521–2542.23. Monsch AU, Bondi MW, Butters N et al. Comparisons of verbal fluency
tasks in the detection of dementia of the Alzheimer type. Arch Neurol
1992;49:1253–1258.24. Albert M, Smith LA, Scherr PA et al. Use of brief cognitive tests to identify
individuals in the community with clinically diagnosed Alzheimer’s disease.
Int J Neurosci 1991;57:167–178.25. Evans DA, Grodstein F, Loewenstein D et al. Reducing case ascertainment
costs in U.S. population studies of Alzheimer’s disease, dementia, and cog-
nitive impairment-Part 2. Alzheimers Dement 2011;7:110–123.26. Locascio JJ, Growdon JH, Corkin S. Cognitive test performance in detect-
ing, staging, and tracking Alzheimer’s disease. Arch Neurol 1995;52:
1087–1099.27. Devore EE, Kang JH, Stampfer MJ et al. The association of antioxidants
and cognition in the Nurses’ Health Study. Am J Epidemiol 2012;177:
33–41.28. Rosner B. Fundamentals of Biostatistics, 5th Ed. Pacific Grove, CA: Dux-
bury, 2000.
29. Knutson KL. Sleep duration and cardiometabolic risk: A review of the epi-
demiologic evidence. Best Practice Res Clin Endocrinol Metab 2010;24:
731–743.30. Buxton OM, Cain SW, O’Connor SP et al. Adverse metabolic conse-
quences in humans of prolonged sleep restriction combined with circadian
disruption. Sci Transl Med 2012;4:129–143.31. Mander BA, Rao V, Lu B et al. Prefrontal atrophy, disrupted NREM slow
waves and impaired hippocampal-dependent memory in aging. Nat Neuro-
sci 2013;16:357–364.32. Cho K, Ennaceur A, Cole JC et al. Chronic jet lag produces cognitive defi-
cits. J Neurosci 2000;20:RC66.
33. Cho K. Chronic ‘jet lag’ produces temporal lobe atrophy and spatial cogni-
tive deficits. Nat Neurosci 2001;4:567–568.34. Machi MS, Staum M, Callaway CW et al. The relationship between shift
work, sleep, and cognition in career emergency physicians. Acad Emerg
Med 2012;19:85–91.35. Cochrane A, Robertson IH, Coogan AN. Association between circadian
rhythms, sleep and cognitive impairment in healthy older adults: An acti-
graphic study. J Neural Transm 2012;119:1233–1239.36. Oosterman JM, van Someren EJ, Vogels RL et al. Fragmentation of the
rest-activity rhythm correlates with age-related cognitive deficits. J Sleep
Res 2009;18:129–135.37. Tranah GJ, Blackwell T, Stone KL et al. Circadian activity rhythms and
risk of incident dementia and mild cognitive impairment in older women.
Ann Neurol 2011;70:722–732.38. Yaffe K, Laffan AM, Harrison SL et al. Sleep-disordered breathing,
hypoxia, and risk of mild cognitive impairment and dementia in older
women. JAMA 2011;306:613–619.39. Peppard PE, Young T, Barnet JH et al. Increased prevalence of sleep-disor-
dered breathing in adults. Am J Epidemiol 2013;177:1006–1014.40. Ayas NT, White DP, Manson JE et al. A prospective study of sleep dura-
tion and coronary heart disease in women. Arch Intern Med
2003;163:205–209.41. Ayas NT, White DP, Al-Delaimy WK et al. A prospective study of self-
reported sleep duration and incident diabetes in women. Diabetes Care
2003;26:380–384.
JAGS 2014 SLEEP DURATION AND COGNITION 9