skin lesions induced by transcranial direct current stimulation (tdcs)
TRANSCRIPT

Letters to the Editor / Brain Stimulation 7 (2014) 757e769 765
Anecdotally, AC doubted his diagnosis of OCD and the relevanceof ERP at the beginning of treatment. AC’s compliance withresponse prevention and willingness to complete difficultexposures dramatically increased between the first the third weeksof treatment. For example, during the weekend after the secondweek of TMS þ ERP, AC assigned himself and completed exposuresat the top of his hierarchy. Afterward he was both proud of hisachievements and surprised at his willingness to do that whichhe considered reckless two weeks prior.
The case of AC highlights the potential of integrated TMS andERP and the need for additional research into treatments that inte-grate brain stimulation with psychotherapy, particularly fordisabling and treatment resistant forms of psychopathology suchas OCD. The present case of integrated TMS þ ERP was effectivefor all obsessive-compulsive symptom dimensions and resulted inlarge and rapid symptom reductions. This suggests that the inclu-sion of ERP with TMS may mitigate shortcomings of LF-rTMS ofthe pre-SMA for OCD and suggests that the addition of TMS mayimprove the speed of ERP. Well-controlled research will be neces-sary to establish if TMS and ERP have additive effects and to deter-mine how these interventions may synergistically augment neuralfunctioning to affect manifest symptoms.
Acknowledgments
The authors would like to thank Dr. Ron Acierno, Ph.D. for hisassistance with this case study.
The authors have no known conflicts of interest associated with this publication andthere has been no significant financial support for this work that could have influ-enced its outcome.
Thomas G. Adams Jr.*Medical University of South Carolina, USA
Ralph H. Johnson VA Medical Center, USA
University of Arkansas, USA
Bashar W. BadranMedical University of South Carolina, USA
Mark S. GeorgeMedical University of South Carolina, USA
Ralph H. Johnson VA Medical Center, USA
*Corresponding author. 67 President Street, Charleston,SC 29425, USA.
E-mail addresses: [email protected],[email protected] (T.G. Adams)
Received 30 May 2014Available online 23 July 2014
http://dx.doi.org/10.1016/j.brs.2014.06.013
References
[1] Chamberlain S, Blackwell A, Fineberg N, Robbins TW, Sahakian BJ. The neuro-psychology of obsessive compulsive disorder: the importance of failures incognitive and behavioural inhibition as candidate endophenotypic markers.Neurosci Biobehav Rev 2005;29:399e419.
[2] de Wit S, de Vries F, van den Heuvel O, et al. Presupplementary motor area hy-peractivity during response inhibition: a candidate endophenotype ofobsessive-compulsive disorder. Am J Psychiatry 2012;169:1100e8.
[3] Berlim Marcelo T, Neufeld NH, Van den Eynde F. Repetitive transcranial mag-netic stimulation (rTMS) for obsessiveecompulsive disorder (OCD): an explor-atory meta-analysis of randomized and sham-controlled trials. J Psychiatr Res2013;47:999e1006.
[4] Blom R, Figee M, Vulink N, Denys D. Update on repetitive transcranial magneticstimulation in obsessive-compulsive disorder: different targets. Curr PsychiatryRep 2011;13:289e94.
[5] Schruers K, Koning K, Luermans J, Haack MJ, Griez E. Obsessiveecompulsive dis-order: a critical review of therapeutic perspectives. Acta Psychiatr Scand 2005;111:261e71.
[6] MantovaniA, Shubeck J, Gowatsky J, SimpsonHB,GreenbergB. P 247. Incomplete-ness and harm avoidance in obsessive compulsive disorder: different response totranscranial magnetic stimulation. Clin Neurophysiol 2013;124:e182e3.
[7] Mantovani A, Simpson H, Fallon B, Rossi S, Lisanby SH. Randomized sham-controlled trial of repetitive transcranial magnetic stimulation in treatment-resistant obsessiveecompulsive disorder. Int J Neuropsychopharmacol 2010;13:217e27.
[8] Oliveira Gomes P, Brasil-Neto J, Allam N, Rodrigues de Souza E. A randomized,double-blind trial of repetitive transcranial magnetic stimulation in obsessive-compulsive disorder with three-month follow-up. J Neuropsychiatry Clin Neu-rosci 2012;24:437e43.
[9] Foa E, Liebowitz M, Tu X, et al. Randomized, placebo-controlled trial of expo-sure and ritual prevention, clomipramine, and their combination in the treat-ment of obsessive-compulsive disorder. Am J Psychiatry 2005;162:151e61.
Skin Lesions Induced byTranscranial DirectCurrent Stimulation(tDCS)
For several years, at the Institute Guttmann NeurorehabilitationHospital (Barcelona, Spain), we have been applying Transcranialdirect current stimulation (tDCS) for the management of Neuro-pathic pain after spinal cord injury. TDCS has been established asuseful therapeutic option for patients with neuropathic pain [1].Several recent studies demonstrate its efficacy, good toleranceand minimal side effects [2,3]. Our accumulated experience spansto having treated more than 100 patients, using always the samestandardized protocols. Direct current is delivered with a battery-driven, constant current stimulator (NeuroConn, Ilmenau, Ger-many) and two surface sponge electrode pads (7 � 5 cm, 35 cm2)soaked with a saline solution (0.9% NaCl; 308 mosm/l). The anodeis placed over C3 or C4 (EEG 10/20 system) aiming to target the mo-tor cortex, and the cathode over the contralateral supraorbital area[4,5]. The electrodes were fastened into position by using two rub-ber polyester headbands (70 cm � 3 cm). For patients with asym-metric pain, the anode is placed contralateral to the afflicted bodypart, while for patients with symmetric pain, the anode is placedover the dominant hemisphere. A constant current of 2 mA inten-sity is applied in daily sessions of 20 min (Current was ramped-up for 15 s until it reached 2 mA; and finally the device wasturned-off with a ramp-down of 15 s) during a period of 2 weeks(from Monday to Friday; total of 10 treatment sessions). Aftereach session and patient, the material was replaced and cleanedwith soap and water.
Here we report on three cases of skin burns during this tDCStreatment. All three affected patients were men with little hair ontheir scalp. The three were stimulated with the same parametersgetting values of impedance of 3e4.5 kU. Their skin’s surface wasnot cleaned with alcohol because the impedance levels werecorrect. All reported a usual tingling and itching sensation underthe electrodes, but none experienced significant discomfort orpain. Following our standard operating procedures, constant elec-trode’s moistness, electrode position and impedance levels werecontrolled and stable during stimulation sessions.
All patients showed a mild redness of the skin under the centralpart of the electrodes after the tDCS session but it disappeared afterfew minutes without discomfort. However, in all three instances,the skin lesions occurred under the cathode (supraorbital region)

Letters to the Editor / Brain Stimulation 7 (2014) 757e769766
at the end of the sessions. By separating the electrodes from theskin they presented small skin lesions, which resembled red burns,with small blisters (Fig. 1). The extension of the lesions ranged from2 to 3 mm up to 1.5 cm. Lesions appeared after the second stimula-tion session in one patient, while for the other two, they appearedbetween the eighth and tenth sessions. None of the patients had askin lesion before the start, skin disease or a history of any patho-logical skin disorder.
Stimulation sessions were interrupted when the skin lesionsappeared and postponed for a week until the lesions disappeared(lesions healed without any scars). Once stimulation sessionswith new electrodes were restarted, none of the subjects notedpain or discomfort, and lesions did not reappear.
To our knowledge, these side effects have only been reportedtwice previously [6,7]. In one instance the skin lesion was underthe cathode, while in the second reported case the lesionwas underthe anode, but in both cases the lesions occurred in the supraorbitalregion. In both published instances the investigators had used tapwater tomoisten the electrodes. Tapwater can containmetallic par-ticles which can be iontophoretically transferred into the skin andcause heating. However, in our patients the burns occurred despitethe use of saline solution.
Palm et al. [6] applied tDCS at the same intensity as in our pro-tocol (2 mA) but Frank et al. [7] used lower intensities (1.5 mA).Frank et al. [7] found skin lesions located in the area where thewire connects with the electrode (forehead), but in our patientswe were careful to prevent contact with the wire or the connectorwith the skin.
Current density must not exceed 14.29mA/cm2 to prevent tissuedamage [5]. In our patients current densities were approximately0.057 mA/cm2 (2 mA/35 cm2), which is far below safety thresholds.Despite having a good electrode contact with the skin, a homoge-nous electrode pressure could not be guaranteed because themaximum pressure of the band was centered in the middle of thesponge. In spite of these conditions, we did not observe any effectof considerable heat under surface electrodes, such as redness orsweating. We conclude that the electrodes were not dried outbecause we kept on moisturizing them whenever they seemed tostart drying out (controlled from the impedance values).
In addition to stimulation intensity, several other factors canaffect current density, e.g. sponge shape, solution salinity, skin con-ditions, electrode shape, location, placement and electrode subjec-tion. Several studies simulate the current flow density across theskin in different models [8,9].
Figure 1. Cathodal skin lesion after tDCS.
Considering our experience and the two previously publishedcases it seems that the properties of the skin may be the key factorfor the risk of burns. However, it is also important to rememberelectrode characteristics: the shape of the electrodes can determinethe potential risk for higher current densities at the edges, and thematerial integrity of the electrodes which can be lost over time canaffect isotropic conductivity.
Based on the above, tDCS electrodes may need to be replacedperiodically and round electrodes may offer some advantagesover square or rectangular electrodes. Rectangular electrodes areknown to cause moderately higher peak concentration of current,comparing to round electrodes, at least at the rectangular electrodecorners [10]. Measures to reduce the risk of skin lesions shouldinclude a more homogenous subjection of the electrodes thinkingof using caps to make it safer and more effective.
Neus Rodríguez*Eloy Opisso
Institute Guttmann Neurorehabilitation Hospital(University Institute attached to the Universitat Autònoma de
Barcelona (UAB)), Department of Research and Innovation,Camí de can ruti, s/n. 08916 Badalona, Spain
Álvaro Pascual-LeoneInstitut Guttmann Neurorehabilitation Hospital
(University Institute attached to the Universitat Autònoma deBarcelona (UAB))
Berenson-Allen Centre for Noninvasive Brain Stimulation,Department of Neurology, Beth Israel Deaconess Medical Centre
and Harvard Medical School, 330 Brookline Avenue,KS-158 Boston, MA 02215, USA
Maria Dolors SolerInstitut Guttmann Neurorehabilitation Hospital
(University Institute attached to the Universitat Autònoma deBarcelona (UAB)), Department of Clinical Psychology,
Camí de can ruti, s/n. 08916 Badalona, Spain
*Corresponding author. Tel.: þ34 93 497 77 00x2254.E-mail address: [email protected] (N. Rodríguez)
Received 25 March 2014Available online 27 July 2014
http://dx.doi.org/10.1016/j.brs.2014.06.005
References
[1] Fregni F, Boggio PS, Lima MC, et al. A sham-controlled, phase II trial of trans-cranial direct current stimulation for the treatment of central pain in trau-matic spinal cord injury. Pain 2006;122:197e209.
[2] Soler MD, Kumru H, Pelayo R, et al. Effectiveness of transcranial direct currentstimulation and visual illusion on neuropathic pain in spinal cord injury. Brain2010;33:2565e77.
[3] Kumru H, Soler MD, Vidal J, et al. The effects of transcranial direct currentstimulation with visual illusion in neuropathic pain due to spinal cord injury:an evoked potentials and quantitative thermal testing study. Eur J Pain 2013;17(1):55e66.
[4] Nitsche MA, Paulus W. Sustained excitability elevations induced by transcra-nial DC motor cortex stimulation in humans. Neurology 2001;57:1899e901.
[5] Nitsche MA, Liebetanz D, Lang N, Tergau F, Paulus W. Safety criteria for trans-cranial direct current stimulation (tDCS) in humans. Clin Neurophysiol 2003;114(11):2220e2.
[6] Palm U, Keeser D, Schiller C, et al. Skin lesions after treatment with transcra-nial direct current stimulation. Brain Stimul 2008;1:386e7.
[7] Frank E, Wilfurth S, Landgrebe M, et al. Anodal skin lesions after treatmentwith transcranial direct current stimulation. Brain Stimul 2010;3:58e9.
Letters to the Editor / Brain Stimulation 7 (2014) 757e769 767
[8] Miranda PC, Faria P, Hallett M. What does the ratio of injected current to elec-trode area tell us about current density in the brain during tDCS? Clin Neuro-physiol 2009;120(6):1183e7.
[9] Kronberg G, Bikson M. Electrode assembly design for transcranial direct cur-rent stimulation: a FEM modeling study. Conf Proc IEEE Eng Med Biol Soc2012;2012:891e5.
[10] Minhas P, Datta A, Bikson M. Cutaneous perception during tDCS: role of elec-trode shape and sponge salinity. Clin Neurophysiol 2011;122(4):637e8.
Transcranial DirectCurrent Stimulation(TDCS) ImprovedCognitive Outcomes in aCancer Survivor WithChemotherapy-inducedCognitive Difficulties
Chemotherapeutic drugs for cancer treatment are cytotoxic andmay cause unintended damage to neuronal networks in the CNSand lead to deleterious adverse effects on cognitive function. Thechemotherapy-related cognitive decline may range from subtlecognitive difficulties to profound cognitive impairment and maylast years after cessation of the chemotherapy [1,2]. To date, thereare no proven interventions that may ameliorate this condition.
Cognitive processes are to a large degree mediated by the fron-tal/prefrontal cortex and related structures, such as the hippocam-pus and amygdala, involving dopaminergic and serotoninergicneural circuits. Notably, a non-invasive neuromodulatory method,Transcranial Direct Current Stimulation (tDCS), delivered over thearea of the prefrontal cortex (DLPFC) has been shown to increasecognitive performance in healthy subjects, as well as in patientswith neurodegenerative diseases, such as Alzheimer’s or Parkin-son’s Diseases [3e5]. The primary mechanism of tDCS is a sub-threshold modulation of neuronal resting membrane potentialwhich induces a polarity-dependent modification of N-Methyl-D-
A
C
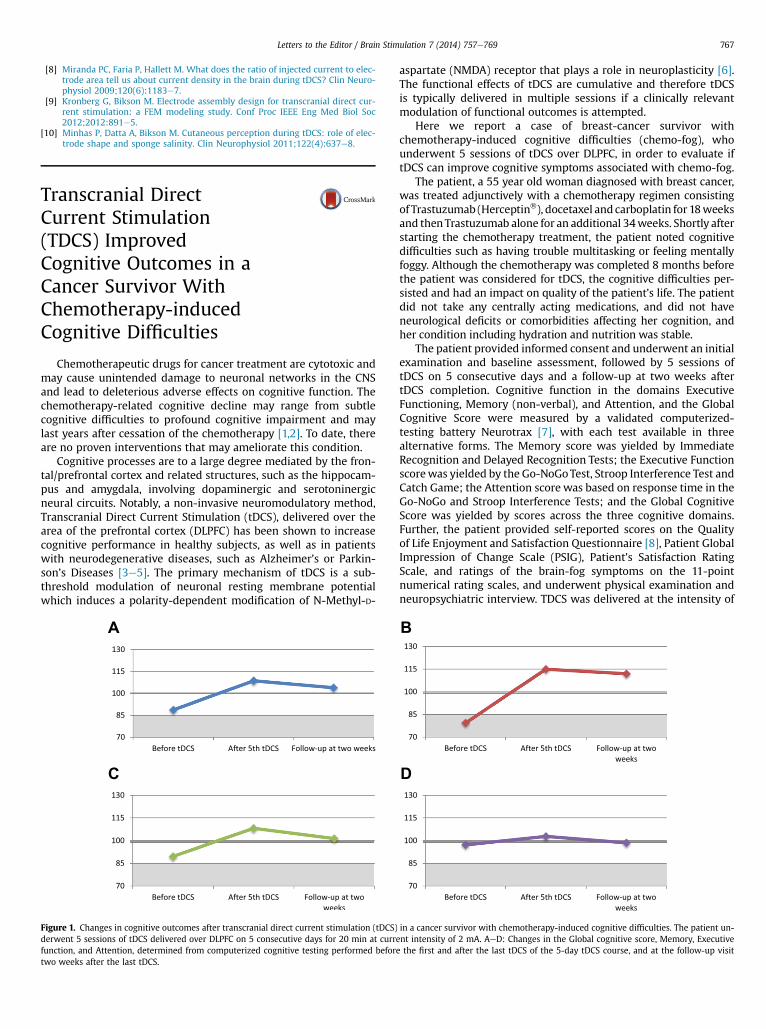
Figure 1. Changes in cognitive outcomes after transcranial direct current stimulation (tDCS)derwent 5 sessions of tDCS delivered over DLPFC on 5 consecutive days for 20 min at currfunction, and Attention, determined from computerized cognitive testing performed befortwo weeks after the last tDCS.
aspartate (NMDA) receptor that plays a role in neuroplasticity [6].The functional effects of tDCS are cumulative and therefore tDCSis typically delivered in multiple sessions if a clinically relevantmodulation of functional outcomes is attempted.
Here we report a case of breast-cancer survivor withchemotherapy-induced cognitive difficulties (chemo-fog), whounderwent 5 sessions of tDCS over DLPFC, in order to evaluate iftDCS can improve cognitive symptoms associated with chemo-fog.
The patient, a 55 year old woman diagnosed with breast cancer,was treated adjunctively with a chemotherapy regimen consistingof Trastuzumab (Herceptin�), docetaxel andcarboplatin for 18weeksand thenTrastuzumab alone for an additional 34weeks. Shortly afterstarting the chemotherapy treatment, the patient noted cognitivedifficulties such as having trouble multitasking or feeling mentallyfoggy. Although the chemotherapy was completed 8 months beforethe patient was considered for tDCS, the cognitive difficulties per-sisted and had an impact on quality of the patient’s life. The patientdid not take any centrally acting medications, and did not haveneurological deficits or comorbidities affecting her cognition, andher condition including hydration and nutrition was stable.
The patient provided informed consent and underwent an initialexamination and baseline assessment, followed by 5 sessions oftDCS on 5 consecutive days and a follow-up at two weeks aftertDCS completion. Cognitive function in the domains ExecutiveFunctioning, Memory (non-verbal), and Attention, and the GlobalCognitive Score were measured by a validated computerized-testing battery Neurotrax [7], with each test available in threealternative forms. The Memory score was yielded by ImmediateRecognition and Delayed Recognition Tests; the Executive Functionscorewas yielded by the Go-NoGoTest, Stroop Interference Test andCatch Game; the Attention score was based on response time in theGo-NoGo and Stroop Interference Tests; and the Global CognitiveScore was yielded by scores across the three cognitive domains.Further, the patient provided self-reported scores on the Qualityof Life Enjoyment and Satisfaction Questionnaire [8], Patient GlobalImpression of Change Scale (PSIG), Patient’s Satisfaction RatingScale, and ratings of the brain-fog symptoms on the 11-pointnumerical rating scales, and underwent physical examination andneuropsychiatric interview. TDCS was delivered at the intensity of
B
D
in a cancer survivor with chemotherapy-induced cognitive difficulties. The patient un-ent intensity of 2 mA. AeD: Changes in the Global cognitive score, Memory, Executivee the first and after the last tDCS of the 5-day tDCS course, and at the follow-up visit