skeletal system - jackson county faculty sites! system functions 1. ... axial – skull, vertebral...
TRANSCRIPT
SKELETAL SYSTEM FUNCTIONS 1. Support – Bones form the internal framework that supports and anchors all soft organs. 2. Protection – Bones protect soft body organs. 3. Movement – Skeletal muscles, which attach to bones by tendons, use the
bones as levers to move the body and its parts. 4. Storage – Bones serve as storehouses for minerals such as Calcium and
Phosphorus. The stored minerals are deposited and reabsorbed continuously. Mineralized bone matrix stores growth factors such as insulin-like growth factors, etc. Adipose is stored in the internal cavities of bones.
5. Blood Cell Formation – Hematopoiesis occurs within the red marrow cavities of certain bones.
6. Hormone production – Osteocalcin is a noncollagenous protein produced by osteoblast and deposited into the matrix.
CLASSIFICATION – The 206 bones are divided into two groups. Axial – skull, vertebral column, thoracic cage, sternum Appendicular – limbs and bones connecting the limbs to the pectoral girdle (scapula, clavicle)
and the pelvic girdle Bone Shapes
Long – longer than they are wide; have a shaft plus two ends
Ex. bones of limbs except wrist and ankle
Short – roughly cubed shape
Ex. wrist, ankle
A sesamoid bone forms in a tendon. (patella)
Flat – thin, flattened & usually curved
Ex. scapula, ribs, sternum, skull
Irregular – shape that doesn’t fit into other groups
Ex. vertebrae, hip
BONE MARKINGS – projections, depressions or openings Projections for muscle & ligament attachment: Tuberosity – large rounded projection Crest – narrow ridge of bone Trochanter – large, irregularly shaped process Line – narrow ridge of bone; less prominent Tubercle – small rounded projection Epicondyle – raised area on or above a condyle Spine – sharp, slender, pointed projection Process – any bony prominence Projections that help form joints: Head – bony expansion on a narrow neck
Facet – smooth, flat articular surface Condyle – rounded articular projection Ramus – arm-like bar of bone Depressions and openings allow blood vessels and nerves to pass: Meatus – canal-like passageway Sinus – cavity filled with air & mucous membrane Fossa – shallow depression or articular surface Groove – slight indention Fissure – narrow, slit-like opening Foramen – round opening through bone

Types of Osseous Tissue: Compact Bone – dense outer layer Spongy Bone (cancellous or trabecular) – honeycomb of flat pieces called trabeculae; open spaces between trabeculae are filled with red or yellow bone marrow.
GROSS ANATOMY – Skeletal Cartilages
Consist primarily of water – This high water content accounts for its resilience.
Cartilage has no nerves, no blood vessels and is surrounded by a layer of dense irregular connective tissue called perichondrium. The perichondrium resists outward expansion when the cartilage is compressed and contains blood vessels so nutrients can diffuse through the matrix into the cartilage cells.
Three types of cartilage: hyaline, elastic and fibrocartilage. Each type has chondrocytes encased in lacunae within an extracellular matrix containing ground substance and fibers.
1. Hyaline Cartilage – provide support with flexibility and resilience. Chondrocytes appear spherical, only contains collagen fibers and is the most abundant cartilage. Location: articular cartilage, costal cartilage, respiratory cartilage, and nasal cartilage.
2. Elastic Cartilage – similar to hyaline, but contains elastic fibers. Location: external ear and epiglottis.
3. Fibrocartilage – highly compressible and have great tensile strength; contains thick collagen fibers. Location: menisci of the knee and intervertebral disc
Structure of Short, Irregular and Flat Bones Consist of thin plates of periosteum-covered compact bone on the outside and endosteum covered spongy bone within. The spongy bone contains bone marrow between their trabeculae. Hyaline cartilage covers articular surfaces. It does NOT contain a shaft or epiphyses. Structure of a Long Bone Diaphysis – shaft of bone constructed of compact bone that surrounds a central medullary cavity.
The medullary cavity contains yellow marrow (fat) in adults and red marrow in infants. Yellow marrow can revert to red marrow if a person becomes very anemic and needs enhanced red blood cell production.
Epiphyses – Ends of bone with exterior compact bone and interior spongy bone.
The joint surface of each epiphysis is covered with a thin layer of articular (hyaline) cartilage which cushions the opposing bone ends during movement and absorbs stress.
Red marrow is found within trabecular cavities of spongy bone. In adults, red marrow is only found in head of femur and humerus, trabeculae of flat bones and some irregular bones.
Between the diaphysis and each epiphysis of adult long bones is an epiphyseal line, a remnant of the epiphyseal plate. The epiphyseal plate is a disc of hyaline cartilage that grows during childhood to lengthen bone.
Periosteum – double-layered membrane covering entire bone except articular cartilage.
Outer fibrous layer is dense irregular connective tissue.
Inner osteogenic layer composed of osteoclast (bone destroying cells) and osteoblast (bone forming cells).
The periosteum is richly supplied with nerve fibers, blood, and lymphatic vessels, which enter the diaphysis via a nutrient foramina.
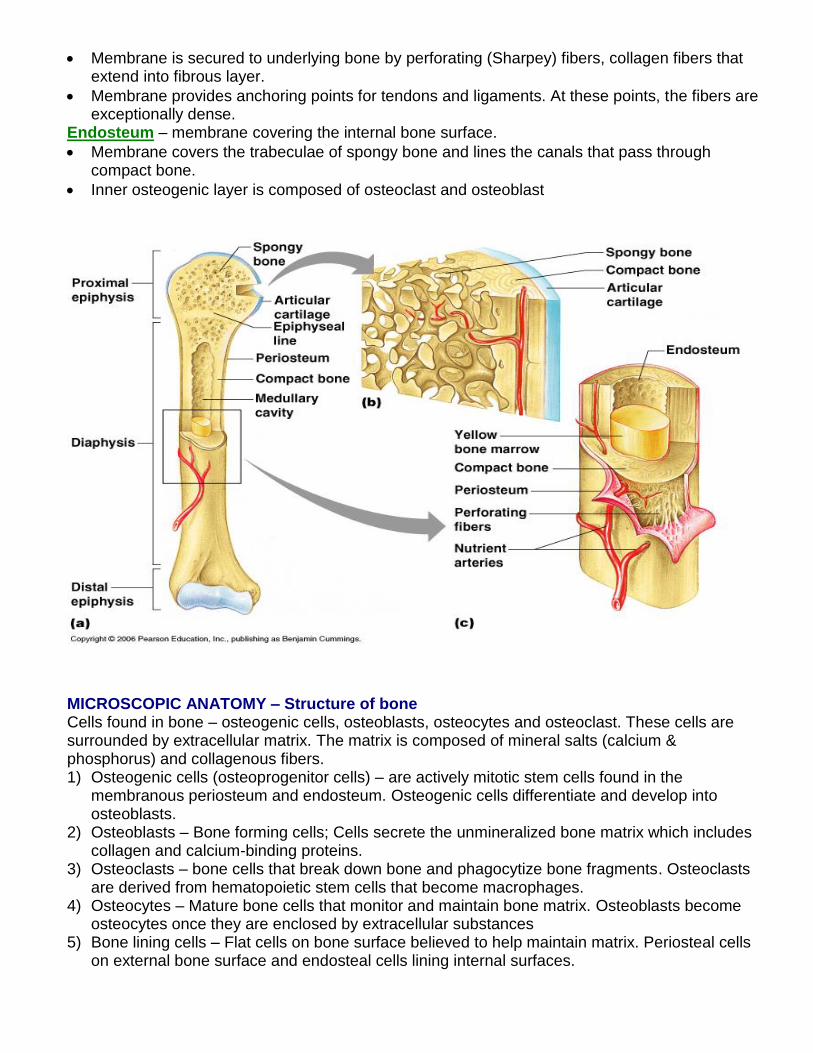
Membrane is secured to underlying bone by perforating (Sharpey) fibers, collagen fibers that extend into fibrous layer.
Membrane provides anchoring points for tendons and ligaments. At these points, the fibers are exceptionally dense.
Endosteum – membrane covering the internal bone surface.
Membrane covers the trabeculae of spongy bone and lines the canals that pass through compact bone.
Inner osteogenic layer is composed of osteoclast and osteoblast
MICROSCOPIC ANATOMY – Structure of bone Cells found in bone – osteogenic cells, osteoblasts, osteocytes and osteoclast. These cells are surrounded by extracellular matrix. The matrix is composed of mineral salts (calcium & phosphorus) and collagenous fibers. 1) Osteogenic cells (osteoprogenitor cells) – are actively mitotic stem cells found in the
membranous periosteum and endosteum. Osteogenic cells differentiate and develop into osteoblasts.
2) Osteoblasts – Bone forming cells; Cells secrete the unmineralized bone matrix which includes collagen and calcium-binding proteins.
3) Osteoclasts – bone cells that break down bone and phagocytize bone fragments. Osteoclasts are derived from hematopoietic stem cells that become macrophages.
4) Osteocytes – Mature bone cells that monitor and maintain bone matrix. Osteoblasts become osteocytes once they are enclosed by extracellular substances
5) Bone lining cells – Flat cells on bone surface believed to help maintain matrix. Periosteal cells on external bone surface and endosteal cells lining internal surfaces.
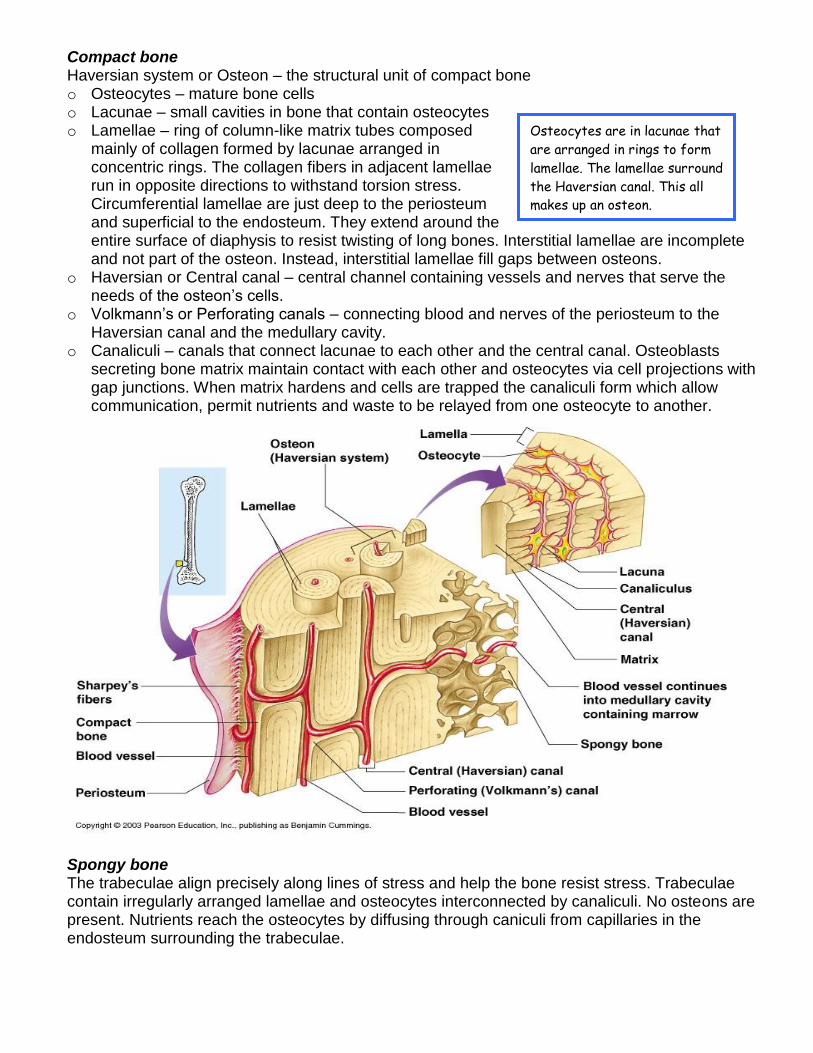
Compact bone Haversian system or Osteon – the structural unit of compact bone o Osteocytes – mature bone cells o Lacunae – small cavities in bone that contain osteocytes o Lamellae – ring of column-like matrix tubes composed
mainly of collagen formed by lacunae arranged in concentric rings. The collagen fibers in adjacent lamellae run in opposite directions to withstand torsion stress. Circumferential lamellae are just deep to the periosteum and superficial to the endosteum. They extend around the entire surface of diaphysis to resist twisting of long bones. Interstitial lamellae are incomplete and not part of the osteon. Instead, interstitial lamellae fill gaps between osteons.
o Haversian or Central canal – central channel containing vessels and nerves that serve the needs of the osteon’s cells.
o Volkmann’s or Perforating canals – connecting blood and nerves of the periosteum to the Haversian canal and the medullary cavity.
o Canaliculi – canals that connect lacunae to each other and the central canal. Osteoblasts secreting bone matrix maintain contact with each other and osteocytes via cell projections with gap junctions. When matrix hardens and cells are trapped the canaliculi form which allow communication, permit nutrients and waste to be relayed from one osteocyte to another.
Spongy bone The trabeculae align precisely along lines of stress and help the bone resist stress. Trabeculae contain irregularly arranged lamellae and osteocytes interconnected by canaliculi. No osteons are present. Nutrients reach the osteocytes by diffusing through caniculi from capillaries in the endosteum surrounding the trabeculae.
Osteocytes are in lacunae that
are arranged in rings to form
lamellae. The lamellae surround
the Haversian canal. This all
makes up an osteon.
Chemical Composition of Bone:
Organic Components – include bone cells and osteoid (1/3 of matrix) secreted by osteoblasts. Osteoid contains ground substances (proteoglycans and glycoproteins) and collagen fibers that are produced and secreted by osteoblast. Organic components contribute to structure, provides tensile strength and flexibility. This resilience comes from the presence of sacrificial bonds in or between collagen molecules that break easily on impact to dissipate energy and prevent fractures. In the absence of additional trauma, bonds reform.
Inorganic Components – mostly hydroxyapatites or mineral salts (65% of bone mass); Calcium phosphates present in form of tiny, tightly packed crystals in and around the collagen fibers in the matrix. The crystals are responsible for hardness and resistance to compression.
Healthy bone is ½ as strong as steel in resisting compression and fully as strong as steel in resisting tension. Bones last long after death due to the salts.
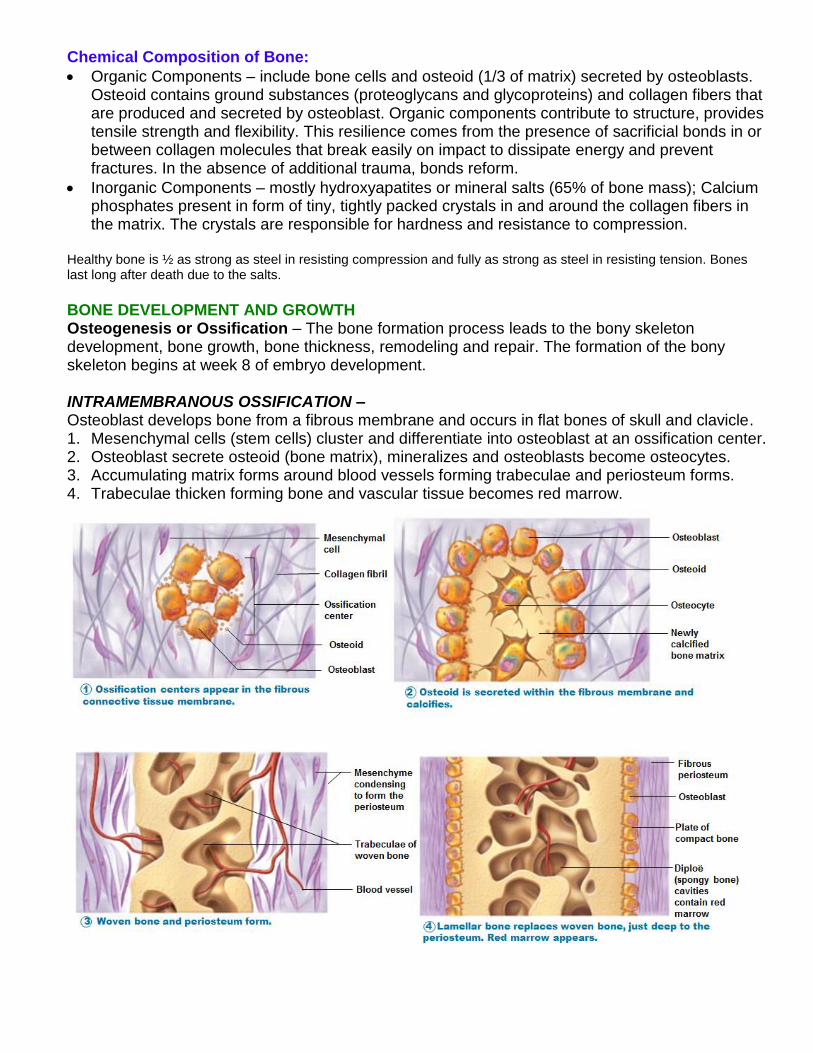
BONE DEVELOPMENT AND GROWTH Osteogenesis or Ossification – The bone formation process leads to the bony skeleton development, bone growth, bone thickness, remodeling and repair. The formation of the bony skeleton begins at week 8 of embryo development. INTRAMEMBRANOUS OSSIFICATION – Osteoblast develops bone from a fibrous membrane and occurs in flat bones of skull and clavicle. 1. Mesenchymal cells (stem cells) cluster and differentiate into osteoblast at an ossification center. 2. Osteoblast secrete osteoid (bone matrix), mineralizes and osteoblasts become osteocytes. 3. Accumulating matrix forms around blood vessels forming trabeculae and periosteum forms. 4. Trabeculae thicken forming bone and vascular tissue becomes red marrow.

ENDOCHONRAL OSSIFICATION Hyaline cartilage is gradually replaced by bone. Process begins at primary ossification center in center of shaft – the perichondrium covering the hyaline cartilage is infiltrated with blood vessels, converting it to vascularized periosteum. Underlying mesenchyme cells change to osteoblasts and bone collar forms around diaphysis. Central cartilage in diaphysis calcifies then develops cavities. Periosteal bud invades cavities formation of spongy bone. Diaphysis elongates, medullary cavity forms and epiphyses ossify. Hyaline cartilage remains only in the epiphyseal plates and articular cartilages. Interstitial Growth – increase in length at the epiphyseal plate. The epiphyseal plate maintains a constant thickness – the rate of cartilage growth on one side of the plate is balanced by bone replacement on the other side. 1. Chondrocytes in the lacunae divide and secrete new matrix, expanding the cartilage from
within. The cartilage on the diaphysis side of plate are rapidly dividing, pushing the epiphysis away from the diaphysis lengthening.
2. Older chondrocytes and their lacunae enlarge, the matrix calcifies and chondrocytes die. Chondrocytes deteriorate and leave long spicules of calcified cartilage. Spicules are eroded by osteoclasts and osteoblast cover area with new bone. Once the osteoblast is enclosed in matrix, it becomes an osteocyte.
3. Bones increase in length as these cartilage cells continue to reproduce and ossify. As long as growth is occurring, the plate remains between the diaphysis and epiphysis.
4. This process continues until the cartilage growth slows and finally stops. The epiphyseal plate completely ossifies and only a thin epiphyseal line remains. The bones can no longer grow in length.
Growth hormones produced by the pituitary gland promote general bone growth and stimulates the epiphyseal plate. Thyroid hormones modulate the activity of growth hormone to ensure proper bone proportions. At puberty, sex hormones are released to increase osteoblast activity and stimulate bone growth. These hormones contribute to a spurt of growth during puberty. Later the sex hormones induce epiphyseal plate closure.
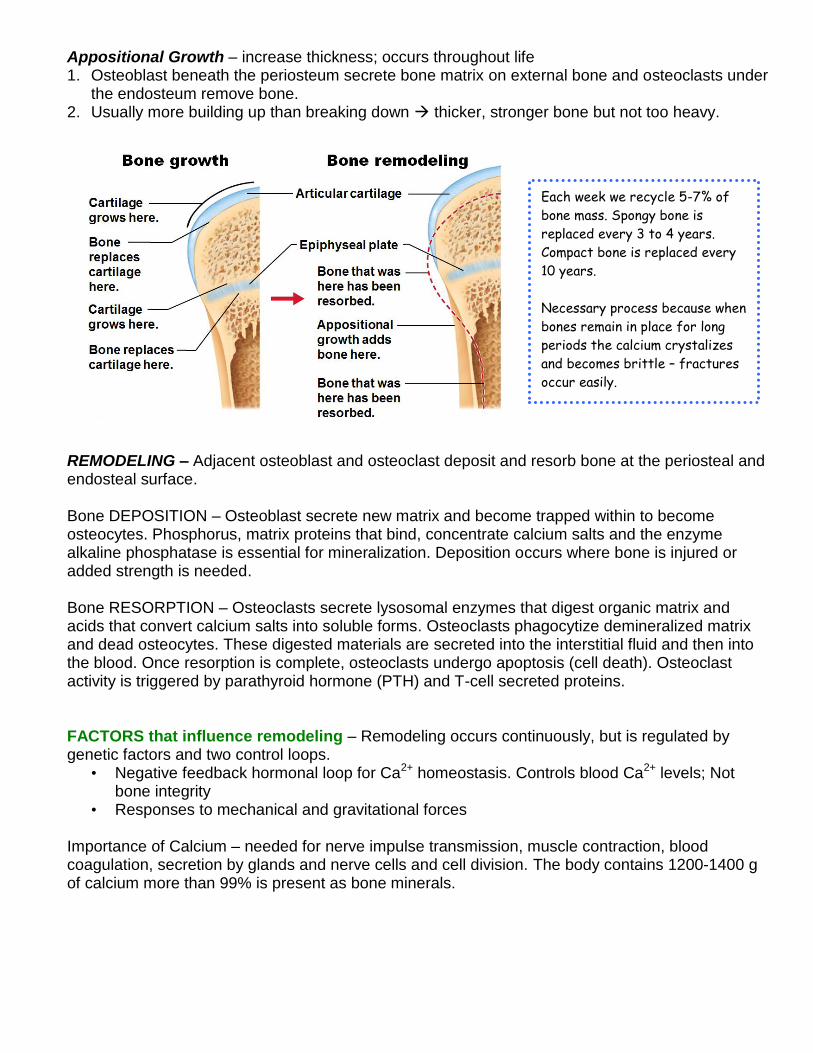
Appositional Growth – increase thickness; occurs throughout life 1. Osteoblast beneath the periosteum secrete bone matrix on external bone and osteoclasts under
the endosteum remove bone. 2. Usually more building up than breaking down thicker, stronger bone but not too heavy.
REMODELING – Adjacent osteoblast and osteoclast deposit and resorb bone at the periosteal and endosteal surface. Bone DEPOSITION – Osteoblast secrete new matrix and become trapped within to become osteocytes. Phosphorus, matrix proteins that bind, concentrate calcium salts and the enzyme alkaline phosphatase is essential for mineralization. Deposition occurs where bone is injured or added strength is needed. Bone RESORPTION – Osteoclasts secrete lysosomal enzymes that digest organic matrix and acids that convert calcium salts into soluble forms. Osteoclasts phagocytize demineralized matrix and dead osteocytes. These digested materials are secreted into the interstitial fluid and then into the blood. Once resorption is complete, osteoclasts undergo apoptosis (cell death). Osteoclast activity is triggered by parathyroid hormone (PTH) and T-cell secreted proteins. FACTORS that influence remodeling – Remodeling occurs continuously, but is regulated by genetic factors and two control loops.
• Negative feedback hormonal loop for Ca2+ homeostasis. Controls blood Ca2+ levels; Not bone integrity
• Responses to mechanical and gravitational forces Importance of Calcium – needed for nerve impulse transmission, muscle contraction, blood coagulation, secretion by glands and nerve cells and cell division. The body contains 1200-1400 g of calcium more than 99% is present as bone minerals.
Each week we recycle 5-7% of
bone mass. Spongy bone is
replaced every 3 to 4 years.
Compact bone is replaced every
10 years.
Necessary process because when
bones remain in place for long
periods the calcium crystalizes
and becomes brittle – fractures
occur easily.

Hormonal Mechanisms Rising blood Ca levels trigger the thyroid gland
to release the hormone, calcitonin. Calcitonin accelerates Ca absorption and inhibits osteoclast.
Falling blood Ca levels signal the parathyroid glands to release the hormone, parathyroid hormone (PTH). PTH signals osteoclasts to break down bone and release Ca into bloodstream.
These hormonal controls act not to preserve the skeleton’s strength or well-being, but rather to maintain blood calcium homeostasis. Minute changes in blood calcium can be dangerous – cause severe neuromuscular problems. Hypercalcemia – sustained high blood calcium
levels can lead to deposits of calcium salts in blood vessels and kidneys.
Leptin – A hormone released by adipose tissue plays a
role in bone density regulation. It inhibits osteoblast in animals.
Exercise – mechanical and gravitational forces: o Exercise stimulates the piezoelectric effect – a physical connection between exercise and bone
maintenance that stimulates the formation of osteoblasts. Exercise provided a healthy stress on bones and stimulates the production of calcitonin by the thyroid gland. Bone growth and remodeling responds to the forces or demands placed upon it through gravity or pull of muscle.
o Removal of mechanical stress through lack of exercise induces removal of mineral salts and collagen.
o Bones reflect stresses they encounter - long bones thickest midway along diaphysis where bending stresses greatest
o Bones stressed when weight bears on them or muscles pull on them – usually off center so tends to bend bones and bending compresses on one side; stretches on other.
o Wolff’s Law – bones grow or remodel in response to demands placed on it. Explains: handedness results in thicker stronger bone of that upper limb, curved bones thickets where most likely to buckle, trabeculae form trusses along lines of stress, large projections occur where heavy and active muscles attach, bones of fetus and bedridden featureless
Hormonal controls determine whether and when remodeling occurs to changing blood calcium levels. Mechanical stress determines where remodeling occurs.
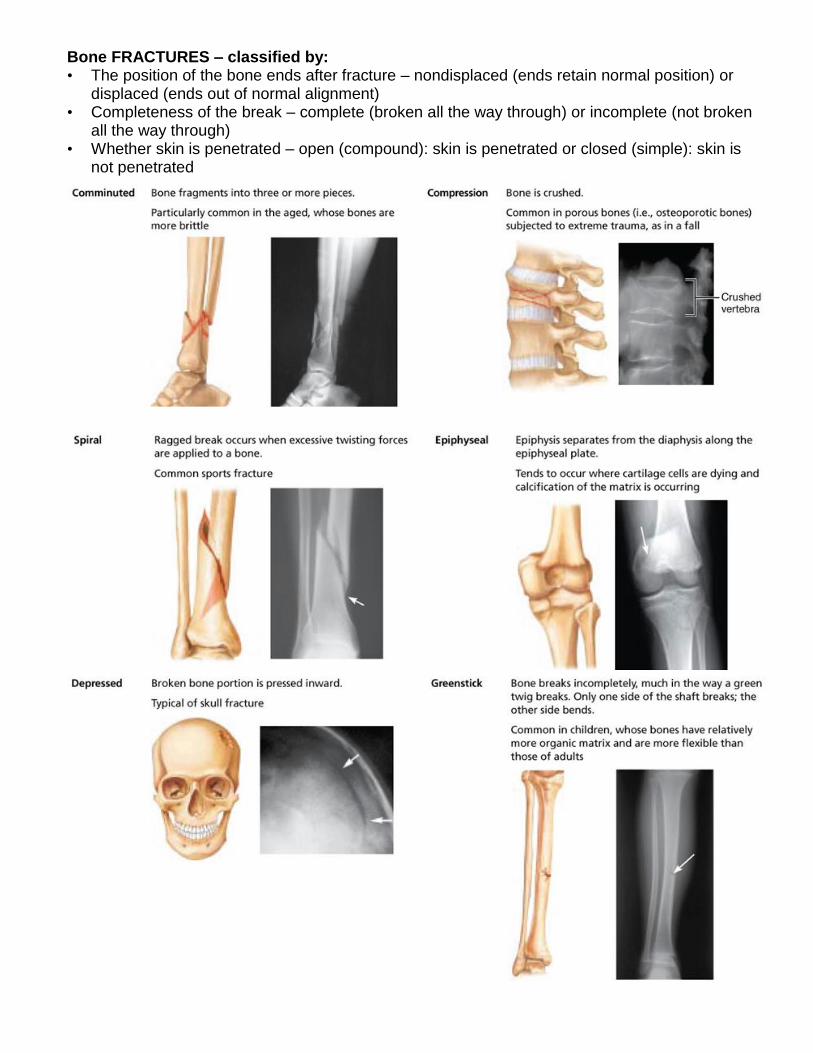
Bone FRACTURES – classified by: • The position of the bone ends after fracture – nondisplaced (ends retain normal position) or
displaced (ends out of normal alignment) • Completeness of the break – complete (broken all the way through) or incomplete (not broken
all the way through) • Whether skin is penetrated – open (compound): skin is penetrated or closed (simple): skin is
not penetrated
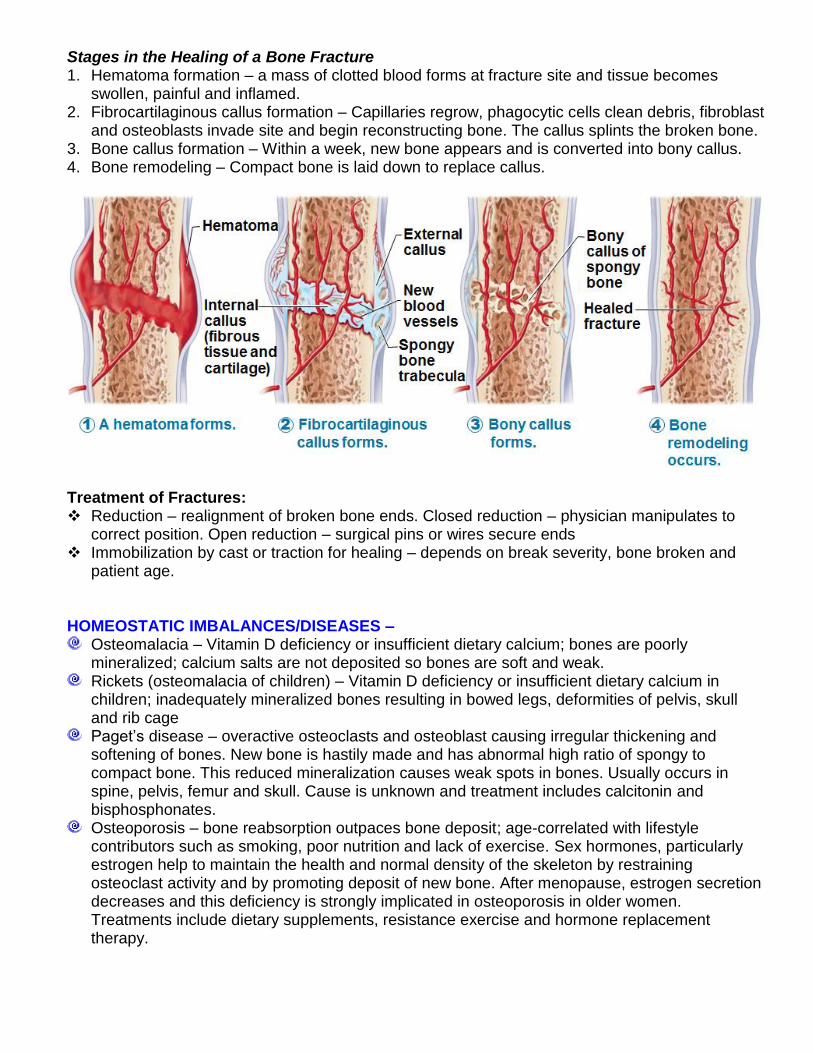
Stages in the Healing of a Bone Fracture 1. Hematoma formation – a mass of clotted blood forms at fracture site and tissue becomes
swollen, painful and inflamed. 2. Fibrocartilaginous callus formation – Capillaries regrow, phagocytic cells clean debris, fibroblast
and osteoblasts invade site and begin reconstructing bone. The callus splints the broken bone. 3. Bone callus formation – Within a week, new bone appears and is converted into bony callus. 4. Bone remodeling – Compact bone is laid down to replace callus.
Treatment of Fractures: Reduction – realignment of broken bone ends. Closed reduction – physician manipulates to
correct position. Open reduction – surgical pins or wires secure ends Immobilization by cast or traction for healing – depends on break severity, bone broken and
patient age. HOMEOSTATIC IMBALANCES/DISEASES –
Osteomalacia – Vitamin D deficiency or insufficient dietary calcium; bones are poorly mineralized; calcium salts are not deposited so bones are soft and weak.
Rickets (osteomalacia of children) – Vitamin D deficiency or insufficient dietary calcium in children; inadequately mineralized bones resulting in bowed legs, deformities of pelvis, skull and rib cage
Paget’s disease – overactive osteoclasts and osteoblast causing irregular thickening and softening of bones. New bone is hastily made and has abnormal high ratio of spongy to compact bone. This reduced mineralization causes weak spots in bones. Usually occurs in spine, pelvis, femur and skull. Cause is unknown and treatment includes calcitonin and bisphosphonates.
Osteoporosis – bone reabsorption outpaces bone deposit; age-correlated with lifestyle contributors such as smoking, poor nutrition and lack of exercise. Sex hormones, particularly estrogen help to maintain the health and normal density of the skeleton by restraining osteoclast activity and by promoting deposit of new bone. After menopause, estrogen secretion decreases and this deficiency is strongly implicated in osteoporosis in older women. Treatments include dietary supplements, resistance exercise and hormone replacement therapy.