simple solutions to the complicated problem of home medication use thursday, december 18, 2008 12:00...
TRANSCRIPT

Simple Solutions to theComplicated Problem ofHome Medication Use
Thursday, December 18, 200812:00 – 1:00 p.m. EST
© American Academy of Pediatrics 2008

Moderator: Karen Frush, MD, FAAPChief Patient Safety OfficerDuke University Health SystemDurham, North Carolina

DISCLOSURESFinancial Relationships
Melissa A. Singleton, MEd, Project Manager-Consultant
has disclosed a financial relationship with an entity producing, marketing, re-selling, or distributing health
care goods or services consumed by, or used on, patients. Her husband is employed by Walgreen Co. as
a Workforce Administration Manager (technology position) for the company’s call centers. The AAP
determined that this financial relationship does not relate to the educational assignment.
None of the other involved individuals (Speaker, Moderator, Project Advisory Committee members, or Staff) has disclosed a relevant financial relationship.
Refer to full AAP Disclosure Policy & Grid available below for download.

DISCLOSURESOff-Label/Investigational Uses
Our Speaker, Kathleen E. Walsh, MD, MSc, does intend to discuss an unapproved/investigative use
of a commercial product/device in her presentation.
None of the other involved individuals (Moderator, Project Advisory Committee members, or Staff)
has disclosed plans to discuss an unapproved/investigative use of a commercial
product/device.
Refer to full AAP Disclosure Policy & Grid available below for download.

This activity was funded through an educational grant from the
Physicians’ Foundation for Health Systems Excellence.

Visit our website:http://www.aap.org/saferhealthcare
Resources: Useful strategies, valuable information links, and expert advice on reducing or eliminating medical errors affecting children.
Webinars: Register for an upcoming, live Webinar, and earn a maximum of 1.0 AMA PRA Category 1 Credit™. Or, access a full archive, including audio, from one of the past Webinar offerings. Or, download just the
Podcast or slide set from an archive.
Latest News: Links to recent articles relating to pediatric patient safety.
Email List: An e-community dedicated to pediatric patient safety issues and information exchange with other clinicians.
Parents’ Corner: Resources to help parents understand what they can do to help ensure their optimal safety in the health care that their child
receives.

CME CREDITLive Webinar Only
The American Academy of Pediatrics (AAP) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
The AAP designates this educational activity for a
maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
This activity is acceptable for up to 1.0 AAP credits. These
credits can be applied toward the AAP CME/CPD Award available to Fellows and Candidate Members of the American Academy of Pediatrics.

OTHER CREDITLive Webinar Only
This program is approved for 1.0 NAPNAP contact hours of which 1.0 contain pharmacology (Rx) content per the National Association of Pediatric Nurse Practitioners Continuing Education Guidelines.
The American Academy of Physician Assistants accepts
AMA PRA Category 1 Credit(s)TM from organizations accredited by the ACCME.
Important Note:You must have been pre-registered, and viewing the live
webinar, in order to claim CME or other credit for your participation.

LEARNING OBJECTIVESUpon completion of the webinar, participants will be
able to:
• Cite the epidemiology of home medication errors, and what questions remain unanswered.
• Recognize clinical situations where patients may be at high risk for home medication errors.
• Apply at least one strategy to reduce home medication errors in your patient population.

Speaker: Kathleen E. Walsh, MD, MScAssistant Professor of PediatricsUniversity of Massachusetts Medical SchoolWorchester, Massachusetts

Simple solutions to the Simple solutions to the complicated problem of home complicated problem of home
medication usemedication use
Kathleen E Walsh, MD, MSc
University of Massachusetts
School of Medicine

Case 1Case 1
10 mo old with anemia prescribed– Fer-gen-sol (15mg/0.6 ml) 1.2 ml orally once daily– Parents given instructions by nurse who spoke some
Spanish– No one at pharmacy spoke Spanish, bottle labeled in
English After med, child vomited, appeared ill. ED iron
level 365 mcg/dl (normal 60-180) Parent reported administering medication with a
home tablespoon (15 ml)

OutlineOutline
BackgroundHome medication errorsUnanswered questions and
next steps

Take home pointsTake home points
Even home medication errors are a systems problem
There are several simple solutions to help prevent errors in the homes of your patients now
Outpatient quality improvement just getting started

BackgroundBackground
44,000 to 98,000 patients die a year from medical errors
21st Century Healthcare System –Safety–Effectiveness–Patient-centeredness–Timeliness–Efficiency–Equity

DefinitionsDefinitions
Medication error: error in drug ordering, dispensing, administering, or monitoring
Adverse drug event: injury that results from medication use

Adverse drug events and Adverse drug events and medication errorsmedication errors
Error without adverse
event
Adverse event
without error
Error with
adverse event
Medication errors Adverse drug events

Swiss cheese modelSwiss cheese model
Reduce human error
1. Person-centered
2. Systems-centered
Reason, J. BMJ 2000; 320(7237): 768-70.

Swiss cheese model Swiss cheese model
Patient receives overdose
No interpreterLabel in English
Pharmacy
No interpreter,Did not give syringe
MD
Parent
Wrong measurementinstrument

Outpatient medication pathwayOutpatient medication pathway
Patient
Monitoring
Ordering Dispensing Administering

What’s different about What’s different about the home?the home?
Vast majority of US medications taken at home Liquid medications
– Much more complex to calculate– Reconstituted from powder– Measurement devices
Cutting or crushing pills Vomiting or spitting medicines Day care or school administration of medications Risks of over-the-counter medicines Many children live in poverty

The solutionThe solution
“Every system is perfectly designed to achieve exactly the results it achieves”
-Don Berwick

OutlineOutline
BackgroundHome medication errorsUnanswered questions and
next steps

Methods in existing literatureMethods in existing literature
Medical record reviewParent interviewBring meds to clinic to reviewDemonstration of the dose in clinicHome visit

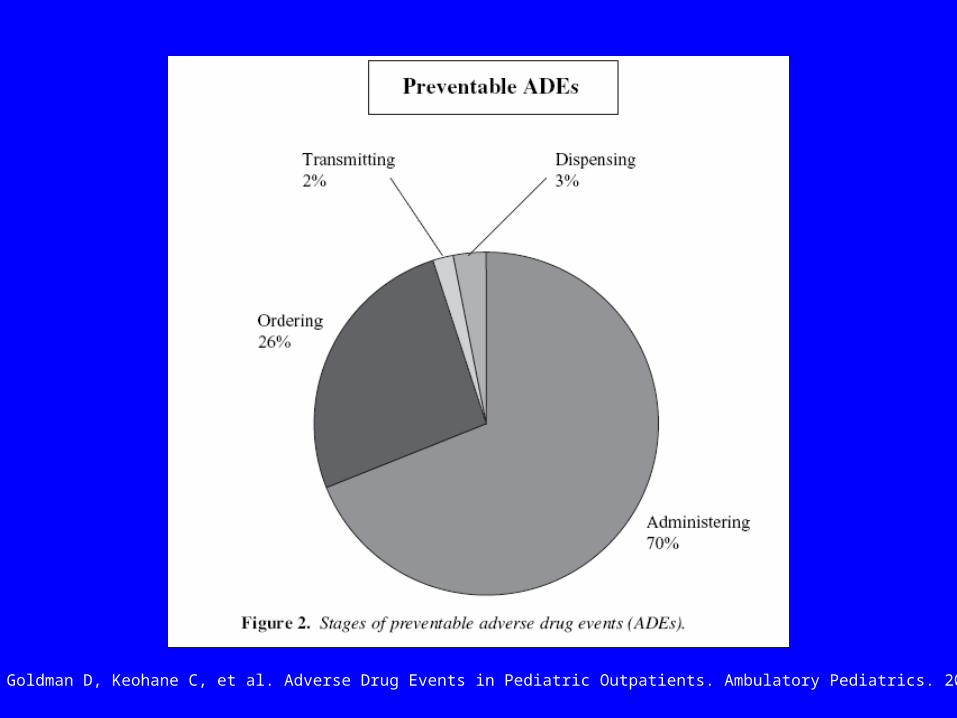
Outpatient pediatric adverse Outpatient pediatric adverse drug eventsdrug events
Prospective cohort study of 1,788 patients who had medications prescribed at 6 Boston practices
Medical record review and parent survey 3% had a preventable ADE (injury due to an error)
– E.g.: 9 yo with strep prescribed amoxicillin. Parent did not fill the prescription and child returned with persistent symptoms
13% had a nonpreventable ADE– E.g.: 2 yo given cold medicine developed anaphylaxis
Kaushal R, Goldman D, Keohane C, et al. Adverse Drug Events in Pediatric Outpatients. Ambulatory Pediatrics. 2007;7:383-9.
Kaushal R, Goldman D, Keohane C, et al. Adverse Drug Events in Pediatric Outpatients. Ambulatory Pediatrics. 2007;7:383-9.

Outpatient oncology errorsOutpatient oncology errors
Retrospective review of medical records 4 oncology clinics in Georgia, New
Mexico, California, and New England117 pediatric visits with 913 medications
– 18% had a medication error1,259 adult patient visits with 10,995
medications – 7% had a medication error
Walsh KE, Dodd KS, Seetharaman K, et al., Medication Errors among Adults and Children with Cancer in the Outpatient Setting.
Journal of Clinical Oncology. (in press).

Outpatient oncology errorsOutpatient oncology errors
Order36%
Dispense
56%Administration
Monitoring Other

Outpatient oncology errorsOutpatient oncology errors
77% of pediatric errors were in medications used at home– E.g.: child with ALL and abscess is given
incorrect frequency of antibiotic at home, abscess does not improve and requires surgical drainage
7% of adult errors were in medications used at home

Chemotherapy administration Chemotherapy administration errorserrors
Prospective observational study in an outpatient oncology clinic
Parents asked to bring in the child’s chemotherapy and demonstrate how they would measure and administer the dose– 30% did not bring in some of the chemotherapy
17 errors in 69 patients with 172 medications– 12 administration and 5 prescribing
Taylor JA., Winter L, Geyer LJ, et al., Oral outpatient chemotherapy medication errors in children with acute lymphoblastic leukemia. Cancer, 2006. 107(6): p. 1400-6.

Antipyretic dosing by Antipyretic dosing by parent reportparent report
Li S, Lathcer B, Crain E. Acetaminophen and ibuprofen dosing by parents. Pediatric Emergency Care 2000;16:394-7.

Chronic acetaminophen overdoseChronic acetaminophen overdose47 cases of hepatotoxicity after
multiple overdoses of acetaminophen1
– 20 survived, including 4 liver transplants
– 3 causes: Parent ran out of pediatric meds and used adult meds, misread label, fever was high so gave more medicine
Henretig FM, Selbst SM, Forrest C, et al. Repeated acetaminophen overdosing. Clin Pediatr. 1989 Nov;28(11):525-8.

Acetaminophen dosing Acetaminophen dosing intervention: Color syringesintervention: Color syringes
Color chart, material to help identify their child’s color, syringe with colored lines
Compared with conventional methods, less errors with color syringes
Average deviation from correct dose 26% for conventional vs. 1.7% for color syringes
Frush KS, Luo X, Hutchinson P, Higgins JN. Evaluation of a method to reduce over-the-counter medication dosing error. Arch Pediatr Adolesc Med. 2004 Jul;158(7):620-4.

Dispensing cup: simple Dispensing cup: simple solution or complex problemsolution or complex problem
34 calls to poison control centers with dispensing cup errors
3 types:1. Confusing teaspoon and tablespoon on the
cup2. Assumption that the dispensing cup was the
unit of measure3. Assumption that the full dispensing cup was
the actual dose Litovitz T. Implication of dispensing cups in dosing errors and pediatric poisonings: a report from the American Association of
Poison Control Centers. The Annals of pharmacotherapy 1992; Jul-Aug;26(7-8):917-8.

Simple solution: syringe Simple solution: syringe with line markedwith line marked
1. Prescription and verbal instructions
2. Prescription with syringe and demonstration
3. Prescription, syringe with a line marked, and demonstration
1. 37% correct – 32%-147% dose
2. 83% correct– 20%-152% dose
3. 100% correct
McMahon SR, Rimsza ME, Bay RC. Pediatrics 1997; 100(3 Pt 1): 330-3.

McMahon SR, Rimsza ME, Bay RC. Pediatrics 1997; 100(3 Pt 1): 330-3.

1970 Home visit study1970 Home visit study
104 visits to parents recruited from a private pediatric practice using home medications
Observation of medication administration, measurement of the home teaspoon, interview
Only 1/3 of teaspoons measure 4.5-5.5 ml 4 parents misunderstood dosing instructions 15 parents were non compliant with instructions
Arnhold, RG, Adebonojo FO, Callas ER, et al., Patients and prescriptions comprehension and compliance with medical instructions in a suburban pediatric practice. Clinical Pediatrics, 1970. 9(11): p. 648-651.

Cold medicineCold medicine

Cold medicine toxicityCold medicine toxicity10 infant overdose deaths; 8 accidental.
Several cold meds involvedGunn: 1) overdose in 3 yo with VP shunt;
2) healthy 3 yo with poor LV function; 3) repeated overdoses in a healthy 9 mo old with an at home arrest
1965-1990: >100 cases of phenylpropanolamine toxicity, including several intracranial hemorrhage

Cold medicine effectivenessCold medicine effectiveness1. RCT: 0.5 to 5 year olds: brompheniramine + PPA +
phenylephrine vs. placebo vs. nothing No change in symptom scores
2. RCT: 1.5 to 12 years: codeine vs. placebo vs. dextromethorphan
No change in symptom scores
3. Review of trials 1950-1991 2 studies with preschoolers showed no effect. 2 with 6 and older showed some symptom improvement
4. RCT: 6 mo to 5 years; brompheniramine + PPA vs. placebo No change in symptoms, significantly more sleep

Cold medicine solutionCold medicine solution

Summary of the literatureSummary of the literature
Rates and types of errors vary by study method and target population
Only one study in home where all medicines, including over-the-counter medicines, and administration tools can be reviewed
Parent errors appear to be common Parents may be unaware of many errors they make

OutlineOutline
BackgroundHome medication errorsUnanswered questions and
next steps

Description of the problemDescription of the problem
Methods needed to describe the range and types of home medication errors to target interventions
Define high risk populations, if any– Many medications– Particular disease groups– SES, other demographic variables– Low health literacy
One solution may be home visit studies

Patient-centered Patient-centered communicationcommunication
1/3 of parents can not accurately repeat back medication use instructions
Patients who skip doses, stop taking medications, and experience side effects do not tell the doctor
Primary care residency programs reassessing physician training, pilot testing new methods
One solution: Need to refocus our outpatient time and infrastructure to ensure effective communication about home care

Patient activationPatient activation AAP parents guide to children’s
medications “Ask your doctor to wash his/her
hands” One solution is email One practice that used email had
1.2 emails per MD per day. 6% were urgent, and it was 57% faster for MD than phone
Rosen P, Kwoh CK “Patient-Physician email: An opportunity to transform pediatric health care delivery. Pediatrics 2007; 120 (4): 701-706.

Systems to support home careSystems to support home care
Pill boxesCalendarsWeb based systemsTelephone based systemsSupport for organization and
complianceReal time problem solving

Take home pointsTake home points
Even home medication errors are a systems problem
There are several simple solutions to help prevent errors in the homes of your patients now
Outpatient quality improvement just getting started

Thanks!!Thanks!!Jerry Gurwitz Linda Sagor
Bob Klugman Chris Stille
Kathy Mazor Doug Roblin
Naheed Usmani, Peter Newburger,
Chris Kaucher,Hellen Mullen
Katie Dodd and Kevin Chysna
Terry Field
Marianne Felice

QUESTION & ANSWER SESSION
Click on the Q&A button to submit your questions.