shock occurrence and survival in 241 with implantable...
TRANSCRIPT
1880
Shock Occurrence and Survival in 241 PatientsWith Implantable Cardioverter-
Defibrillator TherapyWolfram Grimm, MD; Belinda T. Flores, RN; and Francis E. Marchlinski, MD
Background. The purpose of this study was to determine the influence of clinical characteristics on shockoccurrence and survival in 241 patients with implantable cardioverter-defibrillator (ICD) therapy.Methods and Results. Two hundred forty-one consecutive patients underwent ICD implantation between
November 1982 and November 1991 and were subsequently followed for 26±22 months (intention-to-treatanalysis). Actuarial incidence of "appropriate" shocks was 13%, 42%, and 63%, and the incidence of anyspontaneous shocks was 15%, 51%, and 76% at 1, 3, and 5 years of follow-up, respectively. Poor leftventricular function (ejection fraction 530No) was associated with an earlier occurrence of bothappropriate and any spontaneous ICD shocks (p=0.001). Appropriate and any spontaneous shocksoccurred significantly later in patients who presented with cardiac arrest and in patients in whom onlyventricular fibrillation but no uniform ventricular tachycardia was induced during preoperative pro-
grammed stimulation. In addition, amiodarone treatment at implant was associated with later occurrenceof any spontaneous shocks. Cumulative survival from all-cause mortality including perioperativemortality was 84%, 62%, and 57%, and survival from arrhythmic death was 97%, 89%o, and 83% at 1, 3, and5 years, respectively. Ejection fraction <309o was the best predictor of both total arrhythmic death(p=0.019) and total mortality (p=0.003). Antiarrhythmic therapy with class 1 agents at implant was alsoassociated with a higher total mortality during follow-up (p=0.023) but not with total arrhythmic death.Age, sex, underlying heart disease, clinical presentation, and preoperative response to programmedstimulation did not predict long-term survival. In addition, survival curves were similar for patients withand without spontaneous shocks.
Conclusions. The majority of patients receive shocks during long-term follow-up. The occurrence ofappropriate or any spontaneous shocks during follow-up is not associated with increased arrhythmic ortotal mortality consistent with effective prevention of sudden cardiac death with ICD therapy in thishigh-risk patient population. Although low ejection fraction is the strongest predictor of both shockoccurrence and mortality during follow-up, no easy algorithm can be derived from the analyzed clinicalcharacteristics to predict which patients will benefit most from ICD implantation. (Circulation1993;87:1880-1888)KEY WoRDs * implantable cardioverter-defibrillator * sudden cardiac death * ventricular
tachyarrhythmias
Since the first automatic implantable cardioverter-defibrillator (ICD) developed by MichelMirowskil was implanted on February 4, 1980,
more than 25,000 devices have been implanted world-wide. Many studies have demonstrated the efficacy ofthe WCD in preventing sudden cardiac death in patientswith life-threatening tachyarrhythmias. However, thereare only a few reports of outcome in large studypopulations with more than 200 patients.2-5 The pur-pose of this study was threefold: 1) to determine theactuarial incidence of shocks and mortality in a large
From the Clinical Electrophysiology Laboratory, CardiologyDivision, Department of Medicine, Hospital of the University ofPennsylvania, Philadelphia.
Supported in part by grants from the American Heart Associa-tion, Southeast Pennsylvania Chapter, Philadelphia, and a grantfrom the German Science Foundation (W.G.).Address for correspondence: Francis E. Marchlinski, MD, Phil-
adelphia Heart Institute, 39th and Market streets, Philadelphia,PA 19104.
Received June 15, 1992; revision accepted January 27, 1993.
cohort of ICD patients, 2) to identify clinical character-istics associated with the occurrence of appropriate andany spontaneous ICD shocks, and 3) to determineclinical variables associated with total arrhythmic andtotal mortality after ICD implantation (intention-to-treat analysis).
MethodsPatient PopulationThe study population consists of 241 consecutive
patients who underwent initial implantation of an ICDbetween November 1982 and November 1991 and atotal 112 generator replacements until the end of fol-low-up in March 1992. The clinical characteristics of the241 study patients are summarized in Table 1. Implan-tation data are provided in Table 2. All patients signedwritten informed consent before device implantation.Implantation protocols for investigational devices wereapproved by the institutional review board at the Uni-versity of Pennsylvania.
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Grimm et al Shock Occurrence and Survival With ICD Therapy 1881
TABLE 1. Clinical Characteristics of 241 Study Patients
n % Mean RangeSexWomenMen
Age (years)Ejection fraction (%)Follow-up after implant (months)Minimal follow-up in survivors
Heart diseaseCoronary artery diseaseCongestive cardiomyopathyValvular/congenital diseaseNo structural heart disease
Clinical presentationCardiac arrestSyncopeSustained VT without syncopeor cardiac arrestNonsustained VT withoutsyncope or cardiac arrest
Antiarrhythmics at first implantNoneType IAmiodaroneAmiodarone and type I
48 20193 80
60±1131±1226±22
21-8510-670-95
4
16950139
702154
169 7034 1435 15
3 1
1127450
4631212
VT, ventricular tachycardia.
TABLE 2. Implantation Data in 241 Study Patients
Surgical approachMedian sternotomyLateral thoracotomySubcostal thoracotomyNonthoracotomy*
Mode of implantationICD onlyICD after CABGtICD after SERtICD after CABG+SERt
Implanted devices (first implant)CPI 1400/10/20CPI 1500/10/20CPI 1550/55/1600CPI PRXMedtronic PCDVentritex Cadence
Device or generator replacement
CPI 1400/10/20CPI 1500/10/20CPI 1550/55/1600CPI PRXMedtronic PCDVentritex Cadence
Follow-upFollow-up began at the time of first ICD implanta-
tion. End points of follow-up were 1) death from anycause including perioperative mortality, 2) heart trans-plantation (six patients), 3) last patient visit as of March1992. All patients were seen routinely every 1-3 monthsor after device discharge. One hundred ninety-onepatients were followed primarily at our hospital. Fol-low-up evaluation of the remaining 50 patients followedprimarily at other centers was completed by telephonecommunication with the patient and/or the patient'sphysician and analysis of the response to mailed ques-tionnaires completed by the patient's physician. Allspontaneous shocks and deaths during follow-up wereclassified as defined below. In 20 of the 241 patients(8%), the ICD was removed, inactivated, or not re-placed after battery depletion during follow-up for thefollowing reasons: device infection or generator skinerosion (12 patients), refusal of replacement after bat-tery depletion (five patients), end-stage heart failure(two patients), and high defibrillation threshold at at-tempted generator replacement (one patient). Of note,these 20 patients are included in the survival analysisaccording to the intention to treat.
DefinitionsPerioperative mortality was defined as death from
any cause within the first 30 days after ICD implantationor before hospital discharge. Cause of death was de-fined as previously described by Mosteller et a16: Suddendeath is defined as death occurring within 1 hour ofsymptoms in a previously medically stable patient or
ICD, implantable cardioverter-defibrillator; CABG, coronaryartery bypass grafting; SER, subendocardial resection with orwithout aneurysmectomy.
*Only Medtronic PCD devices.tPatch lead placement at the time of CABG or SER with
placement of the ICD generator in a second session a few days later.
death occurring during sleep or unwitnessed; tachyar-rhythmic/nonsudden death is defined as death associ-ated with sustained ventricular tachyarrhythmias per-sisting or recurring over a time period longer than 1hour before death; total arrhythmic death is defined assudden or tachyarrhythmic/nonsudden death; cardiacnonarrhythmic death is defined as a witnessed death ofcardiac nature other than sudden or tachyarrhythmic/nonsudden; cardiac death is defined as death that issudden, tachyarrhythmic/nonsudden, or cardiac nonar-rhythmic; noncardiac death is defined as death resultingprimarily from other causes.
Since the incidence of spontaneous shocks preceded bypresyncope or syncope clearly underestimates the occur-rence of ventricular tachycardia (VT) or ventricular fibril-lation (VF) in ICD patients and the majority of shockswere not electrocardiographically documented, analysis ofspontaneous shocks was performed for both "appropri-ate" shocks and any spontaneous shocks. Appropriateshocks were defined as previously described by Fogoros eta17 as spontaneous ICD discharges preceded by symptomsof severe light-headedness, presyncope or syncope fol-lowed by immediate relief from these symptoms, or shocksfor VT or VF as documented by Holter or telemetrymonitoring or stored electrograms by the device (Ventri-tex Cadence). The criteria for distinguishing supraventric-
No. of patients
59 (24%)127 (53%)44 (18%)11 (5%)
204 (84%)28 (12%)4 (2%)5 (2%)
45 (19%)76 (31%)49 (20%)4 (2%)19 (8%)48 (20%)
No. of models
152657329
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

1882 Circulation Vol 87, No 6 June 1993
VT, CL 226 mU, No Symptom ! Shock
1j11111 1- lLLLLII--iIllI A1 A1lRate < VT Rate Cut-Off Restored
1s. I- 1- 11 1llSR
I- 1.
Rate < VT Rate Cut-Off
FIGURE 1. Top panel: Continuous recordings (25 mm/sec) ofventricular electrograms before and after spontaneous implantablecardioverter-defibrillator (ICD) shock for rapid ventricular tachycardia (VT) with a cycle length (CL) of 220 msec. Of note, thepatient did not feel any symptoms preceding the shock. In the absence of stored electrograms by the device, this shock would nothave been classified as "appropriate." SR supraventricular rhythm. Bottom panel: Continuous recordings (25 mm/sec) ofventricular electrograms before and after spontaneous ICD shock for rapid VT degenerating into ventricular fibrillation (VF)before a 550-V shock restored a supraventricular rhythm below the rate cutoff Of note, the patient did not recall any symptomsnor did she recall having received a shock when she came for a routine follow-up visit. Importantly, this shock episode would alsonot have been classified as "appropriate" in the absence ofstored electrograms by the device, although this shock most likely savedthe patient's life at this time.
ular tachycardia and VT by stored electrograms usingelectrogram morphology, rate, and RR interval variabilityhave been described previously.8 Of note, 67 of the 241study patients (28%) received one or more shocks for VTor VF documented by surface Holter or telemetry moni-toring or stored electrograms by the device during follow-up. According to the definition above, these shocks areappropriate shocks despite the frequent absence of severesymptoms preceding the shocks for electrocardiographi-cally documented VT (Figure 1). Any shocks were definedas any spontaneous ICD shocks other than electrocardio-graphically documented shocks for a non-VT rhythm orshocks in an asymptomatic patient with documented ICDgenerator or lead malfunction in whom the shock wasmost likely preceded by a non-VT rhythm, e.g., leadadapter breakage, magnet misdirection.9
Statistical MethodsData were analyzed for appropriate shocks versus no
appropriate shocks, for any shocks versus no shocks, fortotal arrhythmic death versus no arrhythmic death, andfor total death versus survival in relation to the follow-ing clinical variables: age, sex, ejection fraction, under-lying heart disease, clinical presentation of the arrhyth-mia, result of programmed stimulation before ICDimplant, coronary artery bypass grafting or subendocar-dial resection preceding ICD implantation, and antiar-rhythmic drug treatment at implant. For the continu-
ous-variable ejection fraction, subgroups were formedfor patients with an ejection fraction <30% and .30%as suggested by the study of Kim and colleagues,10 whofound a significantly increased risk for total arrhythmicand total mortality in patients with an ejection fraction<30%. For the continuous variable, age subgroups wereformed arbitrarily at 70 years since no previous studysuggested a particular cutoff for age as a predictor forspontaneous shocks, total arrhythmic, and total mortal-ity. All analysis was performed according to the inten-tion-to-treat principle unless specified otherwise. Val-ues are expressed as mean±SD. Survival curves wereplotted using the Kaplan-Meier method. Univariatecomparison between survival curves was performedusing the log-rank method for all variables listed above.A value ofp<0.05 was considered significant. Variablesdemonstrating sufficient association with the dependentvariable (occurrence of appropriate shocks, any shocks,arrhythmic death, and total mortality, respectively) atp<0.15 were then included in a multivariate stepwiseCox proportional hazards analysis requiring p<0.05 forvariable entry and p>0.10 for variable removal.11'12
ResultsIncidence ofAppropriate and Any SpontaneousICD Shocks
During 24±20 months of follow-up with active ICD,135 of 241 patients (56%) received a spontaneous ICD
-A- AL- A- a A- A- A A- L L A- 1 ._ ._ .^ ._ ._ ._ ._ ._ - 1 ._ ._ ._ .. .^ . . . A. I- a- a- a- a-
iii UT j ilfilii.7.-
V~ 7
I'1.I I 1. I-
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from
Grimm et al Shock Occurrence and Survival With ICD Therapy 1883
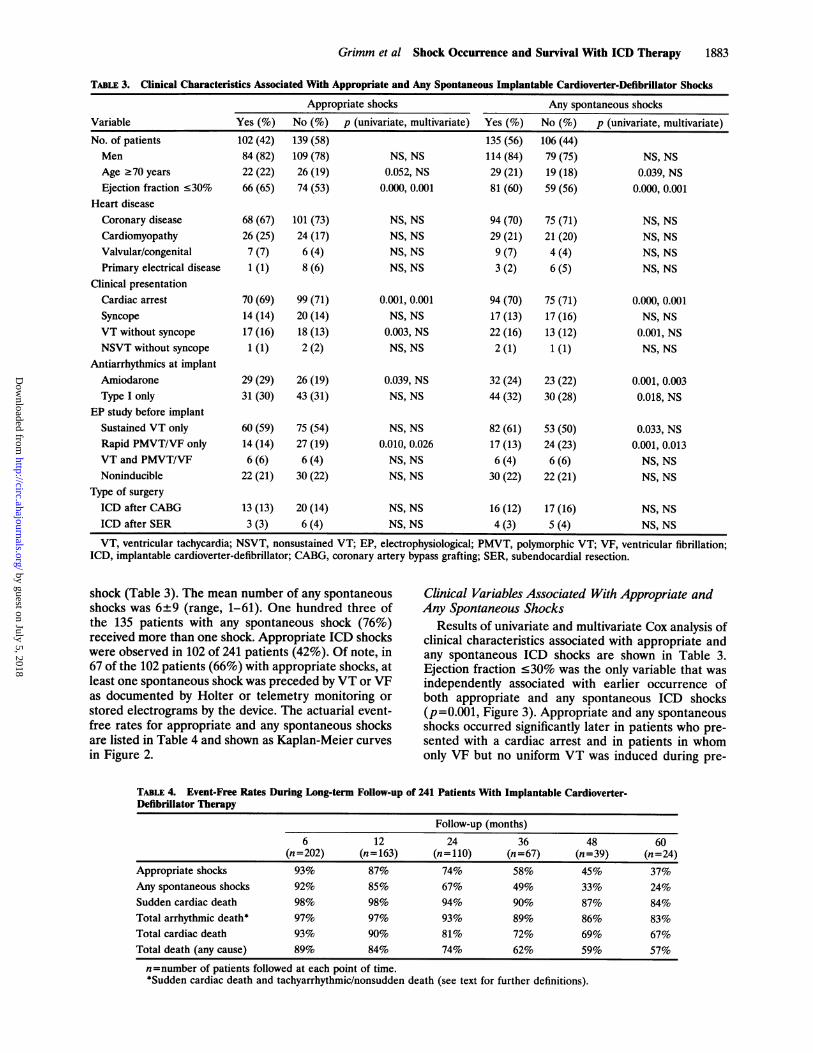
TABLE 3. Clinical Characteristics Associated With Appropriate and Any Spontaneous Implantable Cardioverter-Defibrillator Shocks
Appropriate shocks Any spontaneous shocksVariable Yes (%) No (%) p (univariate, multivariate) Yes (%) No (%) p (univariate, multivariate)No. of patients 102 (42) 139 (58) 135 (56) 106 (44)Men 84 (82) 109 (78) NS, NS 114 (84) 79 (75) NS, NSAge .70 years 22 (22) 26 (19) 0.052, NS 29 (21) 19 (18) 0.039, NSEjection fraction s30% 66 (65) 74 (53) 0.000, 0.001 81 (60) 59 (56) 0.000, 0.001
Heart diseaseCoronary disease 68 (67) 101 (73) NS, NS 94 (70) 75 (71) NS, NSCardiomyopathy 26 (25) 24 (17) NS, NS 29 (21) 21 (20) NS, NSValvular/congenital 7 (7) 6 (4) NS, NS 9 (7) 4 (4) NS, NSPrimary electrical disease 1 (1) 8 (6) NS, NS 3 (2) 6 (5) NS, NS
Clinical presentationCardiac arrest 70 (69) 99 (71) 0.001, 0.001 94 (70) 75 (71) 0.000, 0.001Syncope 14 (14) 20 (14) NS, NS 17 (13) 17 (16) NS, NSVT without syncope 17 (16) 18 (13) 0.003, NS 22 (16) 13 (12) 0.001, NSNSVT without syncope 1 (1) 2 (2) NS, NS 2 (1) 1 (1) NS, NS
Antiarrhythmics at implantAmiodarone 29 (29) 26 (19) 0.039, NS 32 (24) 23 (22) 0.001, 0.003Type I only 31 (30) 43 (31) NS, NS 44 (32) 30 (28) 0.018, NS
EP study before implantSustained VT only 60(59) 75 (54) NS, NS 82 (61) 53 (50) 0.033, NSRapid PMVT/VF only 14 (14) 27 (19) 0.010, 0.026 17 (13) 24 (23) 0.001, 0.013VT and PMVT/VF 6(6) 6(4) NS, NS 6 (4) 6(6) NS, NSNoninducible 22 (21) 30 (22) NS, NS 30 (22) 22 (21) NS, NS
Type of surgeryICD after CABG 13 (13) 20 (14) NS, NS 16 (12) 17 (16) NS, NSICD after SER 3 (3) 6 (4) NS, NS 4 (3) 5 (4) NS, NS
VT, ventricular tachycardia; NSVT, nonsustained VT; EP, electrophysiological; PMVT, polymorphic VT; VF, ventricular fibrillation;ICD, implantable cardioverter-defibrillator; CABG, coronary artery bypass grafting; SER, subendocardial resection.
shock (Table 3). The mean number of any spontaneousshocks was 6±9 (range, 1-61). One hundred three ofthe 135 patients with any spontaneous shock (76%)received more than one shock. Appropriate ICD shockswere observed in 102 of 241 patients (42%). Of note, in67 of the 102 patients (66%) with appropriate shocks, atleast one spontaneous shock was preceded by VT or VF
as documented by Holter or telemetry monitoring orstored electrograms by the device. The actuarial event-free rates for appropriate and any spontaneous shocksare listed in Table 4 and shown as Kaplan-Meier curvesin Figure 2.
Clinical Variables Associated With Appropriate andAny Spontaneous Shocks
Results of univariate and multivariate Cox analysis ofclinical characteristics associated with appropriate andany spontaneous ICD shocks are shown in Table 3.Ejection fraction <30% was the only variable that was
independently associated with earlier occurrence ofboth appropriate and any spontaneous ICD shocks(p=0.001, Figure 3). Appropriate and any spontaneousshocks occurred significantly later in patients who pre-sented with a cardiac arrest and in patients in whomonly VF but no uniform VT was induced during pre-
TABLE 4. Event-Free Rates During Long-term Follow-up of 241 Patients With Implantable Cardioverter-Defibrillator Therapy
Appropriate shocksAny spontaneous shocksSudden cardiac deathTotal arrhythmic death*Total cardiac deathTotal death (any cause)
6 126(n=202)93%92%98%97%93%89%
12(n= 163)87%85%98%97%90%84%
Follow-up (months)24 36
(n=110) (n=674% 58%67% 49994% 90993% 89981% 72974% 62%
57)Y0
0
0
0
0
0
48(n=39)45%33%87%86%69%59%
6060
(n=24)37%24%84%83%67%57%
n=number of patients followed at each point of time.*Sudden cardiac death and tachyarrhythmic/nonsudden death (see text for further definitions).
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from
1884 Circulation Vol 87, No 6 June 1993
1.0
CD 0.80
I= 0.6
a° 0.4U.O 0.20( nfl
0 1 2 3 4 5
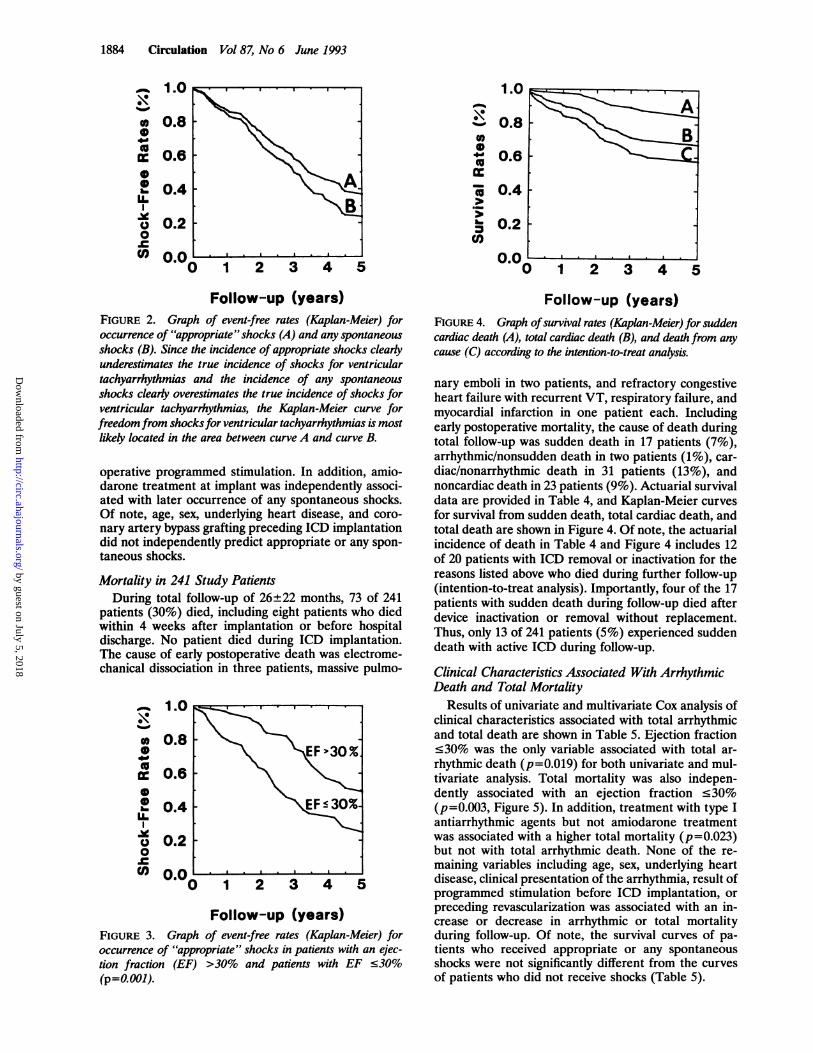
Follow-up (years)FIGURE 2. Graph of event-free rates (Kaplan-Meier) foroccurrence of "appropriate" shocks (A) and any spontaneousshocks (B). Since the incidence of appropriate shocks clearlyunderestimates the true incidence of shocks for ventriculartachyarrhythmias and the incidence of any spontaneousshocks clearly overestimates the true incidence of shocks forventricular tachyarrhythmias, the Kaplan-Meier curve forfreedomfrom shocksfor ventricular tachyarrhythmias is mostlikely located in the area between curve A and curve B.
operative programmed stimulation. In addition, amio-darone treatment at implant was independently associ-ated with later occurrence of any spontaneous shocks.Of note, age, sex, underlying heart disease, and coro-nary artery bypass grafting preceding ICD implantationdid not independently predict appropriate or any spon-taneous shocks.
Mortality in 241 Study PatientsDuring total follow-up of 26±22 months, 73 of 241
patients (30%) died, including eight patients who diedwithin 4 weeks after implantation or before hospitaldischarge. No patient died during ICD implantation.The cause of early postoperative death was electrome-chanical dissociation in three patients, massive pulmo-
1.0
. 0.8ID
cc 0.6
2 0.4U.
Y 0.20
(" nf0
Follow-up (years)FIGURE 3. Graph of event-free rates (Kaplan-Meier) foroccurrence of "appropriate" shocks in patients with an ejec-tion fraction (EF) >30% and patients with EF .30%(p=O.001).
1.0
0X(U
tocc
cc
r)
Follow-up (years)FIGURE 4. Graph ofsurvival rates (Kaplan-Meier) for suddencardiac death (A), total cardiac death (B), and death from anycause (C) according to the intention-to-treat analysis.
nary emboli in two patients, and refractory congestiveheart failure with recurrent VT, respiratory failure, andmyocardial infarction in one patient each. Includingearly postoperative mortality, the cause of death duringtotal follow-up was sudden death in 17 patients (7%),arrhythmic/nonsudden death in two patients (1%), car-diac/nonarrhythmic death in 31 patients (13%), andnoncardiac death in 23 patients (9%). Actuarial survivaldata are provided in Table 4, and Kaplan-Meier curvesfor survival from sudden death, total cardiac death, andtotal death are shown in Figure 4. Of note, the actuarialincidence of death in Table 4 and Figure 4 includes 12of 20 patients with ICD removal or inactivation for thereasons listed above who died during further follow-up(intention-to-treat analysis). Importantly, four of the 17patients with sudden death during follow-up died afterdevice inactivation or removal without replacement.Thus, only 13 of 241 patients (5%) experienced suddendeath with active ICD during follow-up.
Clinical Characteristics Associated With ArrhythmicDeath and Total Mortality
Results of univariate and multivariate Cox analysis ofclinical characteristics associated with total arrhythmicand total death are shown in Table 5. Ejection fraction<30% was the only variable associated with total ar-rhythmic death (p=0.019) for both univariate and mul-tivariate analysis. Total mortality was also indepen-dently associated with an ejection fraction <30%(p=0.003, Figure 5). In addition, treatment with type Iantiarrhythmic agents but not amiodarone treatmentwas associated with a higher total mortality (p=0.023)but not with total arrhythmic death. None of the re-maining variables including age, sex, underlying heartdisease, clinical presentation of the arrhythmia, result ofprogrammed stimulation before ICD implantation, orpreceding revascularization was associated with an in-crease or decrease in arrhythmic or total mortalityduring follow-up. Of note, the survival curves of pa-tients who received appropriate or any spontaneousshocks were not significantly different from the curvesof patients who did not receive shocks (Table 5).
-
L
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Grimm et al Shock Occurrence and Survival With ICD Therapy
TABLE 5. Clinical Characteristics Associated With Arrhythmic Death and Total Mortality in Patients With ImplantableCardioverter-Defibrillator Therapy
Arrhythmic death Total death
Variable Yes (%) No (%) p (univariate, multivariate) Yes (%) No (%) p (univariate, multivariate)No. of patients 19 (8) 222 (92) 73 (30) 168 (70)Men 14 (74) 179 (81) NS, NS 59 (81) 134 (80) NS, NSAge .70 years 4 (21) 44 (20) NS, NS 15 (21) 33 (20) NS, NSEjection fraction <30% 14 (74) 126 (57) 0.019, 0.019 49 (67) 91 (54) 0.002, 0.003
Shocks during follow-upAppropriate shocks 12 (63) 90 (41) NS, NS 39 (53) 63 (38) NS, NSAny shocks 13 (68) 122 (55) NS, NS 47 (64) 88 (52) NS, NS
Heart diseaseCoronary disease 14 (74) 155 (70) NS, NS 51 (70) 118 (70) NS, NSCardiomyopathy 5 (26) 45 (20) NS, NS 16 (22) 34 (20) NS, NSValvular/congenital ... 13 (6) NS, NS 5 (7) 8 (5) NS, NSPrimary electrical disease ... 9 (4) NS, NS 1(1) 8 (5) NS, NS
Clinical presentationCardiac arrest 14 (74) 155 (70) NS, NS 55 (75) 114 (68) NS, NSSyncope 3 (16) 31 (14) NS, NS 7 (10) 27 (16) NS, NSVT without syncope 2 (10) 33 (15) NS, NS 10 (14) 25 (15) NS, NSNSVT without syncope ... 3 (1) NS, NS 1(1) 2 (1) NS, NS
Antiarrhythmics at implantAmiodarone 8 (42) 47 (21) NS, NS 23 (31) 32 (19) NS, NSType I only 7 (37) 67 (30) NS, NS 29 (40) 45 (27) 0.028, 0.023
EP study before implantSustained VT only 10 (53) 125 (56) NS,NS 45 (62) 90(54) NS, NSRapid PMVT/VF only 4 (21) 37 (17) NS, NS 8 (11) 33 (20) 0.051, NSVT and PMVT/VF 2 (10) 10 (5) NS, NS 6 (8) 6 (4) NS, NSNoninducible 3 (16) 49 (22) NS, NS 14 (19) 38 (23) NS, NS
Type of surgeryICD after CABG 2 (11) 31 (14) NS,NS 9(12) 24 (14) NS,NSICD after SER ... 9 (4) NS, NS 1(1) 8 (5) NS, NS
VT, ventricular tachycardia, NSVT, nonsustained VT; EP, electrophysiological; PMVT, polymorphic VT; VF, ventricular fibrillation;ICD, implantable cardioverter-defibrillator; CABG, coronary artery bypass grafting; SER, subendocardial resection.
Time From First ICD Discharge to DeathThirty-nine of 102 patients (38%) who received ap-
propriate shocks during follow-up died during further
1.0 . . . . . . .
0.8
0.6
X 0.4
0.2
0.0 . . . . . . . .0 1 2 3 4 5
Follow-up (years)FIGURE 5. Graph of survival rates (Kaplan-Meier) for totaldeath in patients with an ejection fraction (EF) >30% andpatients with an ejection fraction .30% (p=0.003).
follow-up. Mean survival after the first appropriateshock for the 39 patients who died until the end of totalfollow-up was 12±13 months (range, 0-63 months).Mean survival after the first appropriate ICD shockuntil the end of total follow-up for all 102 patients whoreceived appropriate shocks was 20±21 months (range,0-94 months).
Forty-seven of 135 patients (35%) who received anyspontaneous shocks during follow-up died during fur-ther follow-up. Mean survival after the first shock forthe 47 patients who received any spontaneous shocksand died later during follow-up was 13±13 months(range, 0-63 months). Mean survival after the firstspontaneous ICD shock for all 135 patients who re-ceived any shock was 21±20 months until the end offollow-up (range, 0-94 months).
DiscussionPrevention of sudden cardiac death with ICD therapy
has already been well documented.2-5,7,13-23 The presentstudy of 241 consecutive patients who underwent ICDimplantation for life-threatening ventricular tachyar-rhythmias confirms the efficacy of ICD therapy insudden cardiac death prevention by the following ob-
1885
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

1886 Circulation Vol 87, No 6 June 1993
servations: 1) the actuarial 5-year incidence of appro-priate shocks in 63% of patients and of any spontaneousshocks in 76% of patients, 2) the time from the firstappropriate or any spontaneous shock to death with amean of 12 months or 13 months, respectively, with nodifference in total arrhythmic and total survival forpatients with and without spontaneous shocks, and 3)the low incidence of sudden cardiac death during fol-low-up in 13 of 241 patients (5%) with active ICD(follow-up, 24+20 months) and 17 of 241 patients (7%)during total follow-up of 26±22 months according to theintention-to-treat analysis. The multivariate analysis ofclinical characteristics associated with spontaneousshocks, total arrhythmic death, and total mortality mayhave important implications for future clinical trials.
Incidence of Spontaneous ShocksThe incidence of appropriate shocks defined as
shocks preceded by presyncope or syncope clearly un-derestimates the true incidence of shocks for ventriculartachyarrhythmias (Figure 1). Conversely, the incidenceof any spontaneous ICD shocks, excluding shocks fordocumented non-VT rhythm or device malfunction,clearly overestimates the true incidence of shocks forVT or VF. Therefore, both appropriate and any spon-taneous shocks were analyzed in this study. Using thisapproach, the true incidence of shocks for ventriculartachyarrhythmia recurrence is most likely in the areabetween the two Kaplan-Meier curves for freedom ofappropriate and any spontaneous shocks (Figure 2). Ofnote, the actuarial 5-year incidence of appropriateshocks in 63% of patients in our study is very similar tothe findings of other investigators ranging from 62% inthe study from Gross and colleagues24 to 69% in thereport of Fogoros et a12 and Tchou et al.25
Effect of Ejection Fraction on Shock Occurrenceand Survival
Poor left ventricular function (ejection fraction <30%)was the only clinical variable in our study that was inde-pendently associated with all four dependent variables,i.e., earlier occurrence of appropriate and any spontane-ous shocks (Figure 3) and higher total arrhythmic andtotal mortality (Table 5). However, the predictive value ofpreserved left ventricular function at implant for remain-ing shock free during follow-up is low, since 51% ofpatients with an ejection fraction >30% are estimated toreceive appropriate shocks during 5-year follow-up (Fig-ure 3). These findings are similar to the results of Levineand colleagues,3 who found an ejection fraction <25%predictive for earlier ICD discharge and shorter survivalafter ICD discharge. Our results also confirm the findingof Kim and colleagues10 that an ejection fraction <30% isassociated with a higher total arrhythmic and total mor-tality after ICD implant. In our study, patients who diedduring the early postoperative period after ICD implan-tation (3%) tended to have a lower ejection fraction of27±11% as compared with 31±12% in patients whosurvived the early postoperative period. However, thedifference in ejection fraction was not significant becauseof the small number of patients who died early postoper-atively in our study. Similar to our results, a recentmulticenter study reported by Mosteller and colleagues6revealed a significant, inverse correlation between perino-
tion; patients who died perioperatively had a mean ejec-tion fraction of 26% versus 34% in survivors of ICDimplantation.
Effect ofAntiarrhythmic Drug Treatment at the TimeofICD Implantation
Treatment with amiodarone at implantation was in-dependently associated with later occurrence of anyspontaneous shocks, but there was no significant differ-ence in the occurrence of appropriate shocks in patientswith and without amiodarone at implantation (Table 3).This finding may merely reflect differences in patientselection for amiodarone therapy at implantation thatwere not accounted for by the clinical variables listed inTable 3, such as frequency and hemodynamic toleranceof the clinical VT and intolerance or failure of otherantiarrhythmic agents. Treatment with class 1 antiar-rhythmic drugs at implantation was associated with a
higher total mortality but not with sudden death or totalarrhythmic death (Table 5). Of note, the lack of in-creased sudden death or total arrhythmic death rate inpatients with class 1 agents at implantation excludes acausal relation between the increased total mortalityand potential proarrhythmic effects of class 1 agents.Differences in patient characteristics other than thevariables listed in Table 5 may also account for thehigher nonarrhythmic mortality of patients with class 1agents at implantation. Furthermore, treatment withspecific antiarrhythmic drugs at the time of ICD implan-tation by no means represents a stable clinical variableduring long-term follow-up. Antiarrhythmic drug treat-ment was discontinued, started, or altered in many
patients according to the clinical judgment of the pa-
tients' physician for the following reasons: 1) side effectsduring follow-up, 2) frequency of documented or sus-pected recurrences of ventricular tachyarrhythmias, 3)control of supraventricular tachyarrhythmias during fol-low-up, and 4) patient's compliance.
Effect of the Clinical Presentation and Result ofProgrammed Stimulation Before ICD ImplantationOf note, both appropriate and any spontaneous
shocks occurred significantly later in patients who pre-
sented with a cardiac arrest before ICD implantationthan in patients who presented with syncope or VTwithout syncope. In addition, appropriate and any spon-taneous shocks occurred significantly later in patientswho had only rapid polymorphic VT or VF inducedbefore ICD implantation. Both findings may be due todifferences in the electrophysiological substrate in pa-tients with cardiac arrest and only inducible polymor-phic VT or VF as compared with patients with inducibleuniform VT presenting with VT with or without synco-pe.26 Similar to the results of Levine and colleagues3 andVeltri et al,27 clinical presentation and result of pro-grammed stimulation before ICD implantation in ourstudy did not influence survival in patients with ICDtherapy.
Other VariablesSimilar to the results of Levine and colleagues3 and
Reiter et al,28 we found no difference in shock occur-rence or survival curves among patients with coronaryartery disease, nonischemic cardiomyopathy, valvular or
perative mortality (3%) and left ventricular ejection frac- congenital heart disease, and primary electrical disease,
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Grimm et al Shock Occurrence and Survival With ICD Therapy
although the latter group was too small for subgroupanalysis. However, Gross and colleagues24 and Zilo eta129 found a higher incidence of shocks in patients withcoronary disease. This difference may in part be due todifferences in patient population as well as the lack ofmultivariate analysis in both studies. Similar to theresults of Levine and coworkers3 and Meyerburg et al,'4age and sex of patients in our study were not indepen-dently associated with shock occurrence or survivalafter ICD implantation (Tables 3 and 5). In contrast tothe finding of Levine and colleagues3 that coronarybypass surgery at the time of ICD implantation wasassociated with later occurrence of appropriate ICDshocks, we did not find differences in shock occurrencein patients with and without coronary bypass surgerypreceding ICD implantation. This difference may alsobe due to differences in patient population in bothstudies. All patients who underwent coronary bypasssurgery preceding ICD implantation in our study had aremote myocardial infarction generating the "anatomicsubstrate" for arrhythmia recurrence, which is unlikelyto be altered by revascularization.30 Coronary arterybypass grafting, however, may reduce the role of isch-emia for triggering tachyarrhythmias in these patients toa level comparable to patients with a remote myocardialinfarction who did not need revascularization, resultingin a similar incidence of shocks during follow-up in bothgroups in our study.
Limitations of the StudyThis study was retrospective and uncontrolled. Simi-
lar to all previously published follow-up studies of largepatient populations with ICD therapy, electrocardio-graphic documentation of the rhythm preceding spon-taneous ICD shocks was not available in the majority ofcases. Shock analysis was, therefore, performed forappropriate and any spontaneous shocks as discussedabove. Of note, 67 of 135 patients in our study (50%)who received any spontaneous shocks during follow-uphad VT or VF preceding one or more spontaneousshocks documented by Holter or telemetry monitoringor stored electrograms by the device.
ConclusionsThe majority of patients receive shocks during long-
term follow-up after ICD implantation. The occurrenceof appropriate or any spontaneous shocks during fol-low-up is not associated with increased arrhythmic ortotal mortality consistent with effective prevention ofsudden cardiac death with ICD therapy in this high-riskpatient population. Although low ejection fraction is thestrongest predictor of both shock occurrence and mor-tality during follow-up, no easy algorithm can be de-rived from the analyzed clinical characteristics to pre-dict which patients will benefit most from ICDimplantation. The results of this study warrant furtherinvestigation and may have important implications forfuture prospective studies with ICD therapy.
References1. Mirowski M, Reid PR, Mower MM, Watkins L, Gott VL, Schauble
JF, Lanzer A, Heilman MS, Kolenik SA, Fischell RF, WeisfeldtML: Termination of malignant ventricular tachyarrhythmias withan implanted automatic defibrillator in human beings. N Engl JMed 1980;303:322-324
2. Fogoros RN, Elson JJ, Bonnert CA: Survival of patients who havereceived appropriate shocks from their implantable defibrillators.PACE 1991;14:1842-1845
3. Levine JH, Mellits ED, Baumgardner RA, Veltri EP, Mower M,Grunwald L, Guarnieri T, Aarons D, Griffith LSC: Predictors offirst discharge and subsequent survival in patients with automaticimplantable cardioverter-defibrillators. Circulation 1991;84:558-566
4. Winkle RA, Mead RH, Ruder MA, Gaudiani VA, Smith NA,Buch WS, Schmidt P, Shipman T: Long-term outcome with theautomatic implantable cardioverter-defibrillator. JAm Coil Cardiol1989;13:1353-1361
5. Winkle RA, Mead RH, Ruder MA, Smith NA, Ellis TL, ShipmanTC, Schmidt P, Buch WS, Gaudiani VA: Ten-year experience withimplantable defibrillators. (abstract) Circulation 1991;84(suppl II):II-426
6. Mosteller RD, Lehmann MH, Thomas AC, Jackson K: Operativemortality with implantation of the automatic cardioverter-defibrillator. Am J Cardiol 1991;68:1340-1345
7. Fogoros RN, Elson JJ, Bonnet CA: Actuarial incidence and pat-tern of occurrence of shocks following implantation of the auto-matic implantable cardioverter defibrillator. PACE 1989;12:1465-1473
8. Hook BG, Marchlinski FE: Value of ventricular electrogramrecordings in the diagnosis of arrhythmias precipitating electricaldevice shock therapy. JAm Coll Cardiol 1991;17:985-990
9. Grimm W, Flores BF, Marchlinski FE: ECG-documented unnec-essary spontaneous shocks in 206 patients with implantable car-dioverter defibrillator. (abstract) JAm Coll Cardiol 1992;19:287A
10. Kim SG, Fisher JD, Choue CW, Gross J, Roth J, Ferric KJ,Brodman R, Furman S: Influence of left ventricular function onoutcome of patients treated with implantable defibrillators. Circu-lation 1992;85:1304-1310
11. Cox DR, Oakes D: Analysis of Survival Data. New York, Chapp-man and Hall, 1984
12. Lee ET: Statistical Methods for Survival Data Analysis. Wadsworth,Belmont, Calif, 1980
13. Newman D, Sauve MJ, Herre J, Langberg JJ, Lee MA, Titus C,Franklin J, Scheinman MM, Griffin JC: Survival after implantationof the cardioverter defibrillator. Am J Cardiol 1992;69:899-903
14. Myerburg RJ, Luceri RM, Thurer R, Cooper DK, Zaman L,Interian A, Fernandez P, Cox M, Glicksman F, Castellanos A:Time to first shock and clinical outcome in patients receiving anautomatic implantable cardioverter-defibrillator. JAm Coll Cardiol1989;14:508-514
15. Kelly PA, Cannom DS, Garan H, Mirbal GS, Harthorne W, Hur-vitz RJ, Vlahakes GJ, Jacobs ML, Ilvento JP, Buckley MJ, RuskinJN: The automatic implantable cardioverter-defibrillator: Efficacy,complications and survival in patients with malignant ventriculararrhythmias. JAm Coil Cardiol 1988;11:1278-1286
16. Thomas AC, Moser SA, Smutka ML, Wilson PA: Implantabledefibrillation: Eight years clinical experience. PACE 1988;11:2053-2058
17. Fogoros RN, Elson JJ, Bonnet CA, Fiedler SB, Burkholder JA:Efficacy of the automatic implantable cardioverter-defibrillator inprolonging survival in patients with severe underlying cardiac dis-ease. JAm Coll Cardiol 1990;16:381-386
18. Gross J, Zilo P, Ferrick K, Fisher JD, Furman S: Sudden deathmortality in implantable cardioverter defibrillator patients. PACE1991;14:250-254
19. Axtell K, Tchou P, Akthar M: Survival in patients with depressedleft ventricular function treated by implantable cardioverterdefibrillator. PACE 1991;14:291-296
20. Echt DS, Armstrong K, Schmidt P, Oyer PE, Stinson EB, WinkleRA: Clinical experience, complications, and survival in 70 patientswith the automatic implantable cardioverter/defibrillator. Circula-tion 1985;71:289-296
21. Edel TB, Maloney JD, Moore S, McGiunn WP, Gohn D, WilliamsD, Wilkoff BL, McCarthy P, Morant VA, Pearce G, Simmons TW,Trohman R, Firstenberg M, Castle LW: Six-year clinical experi-ence with the automatic implantable cardioverter defibrillator.PACE 1991;14:1850-1854
22. Tchou P. Axtell K, Keim S, Anderson AJ, Troup P. Jazayeri M,Avitall B, Akhtar M: Does reception of appropriate shocks fromthe implantable cardioverter defibrillator affect survival? PACE1991;14:1929-1934
23. Klein H, Trappe HJ: Implantable cardioverter defibrillator ther-apy: Indications and decision making in patients with coronaryartery disease. PACE 1992;15:610-615
1887
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

1888 Circulation Vol 87, No 6 June 1993
24. Gross J, Song SL, Buckingham T, Furman S, Bilitch RegistryGroup: Influence of clinical characteristics and shock occurrenceon ICD patient outcome: A multicenter report. PACE 1991;14:1881-1886
25. Tchou P, Axtell K, Anderson AJ, Keim S, Sra J, Troup P, JazayeriM, Avitall B, Akthar M: When is it safe not to replace an implant-able cardioverter defibrillator generator? PACE 1991;14:1875-1880
26. Josephson ME: Recurrent ventricular tachycardia, in Clinical Car-diac Electrophysiology, ed 2. Malvern, Lea & Febiger, 1992, pp417-615
27. Veltri EP, Mower MM, Mirowski M, Juanteguy J, Watkins L,Levine JH, Guarnieri T, Reid PR, Griffith LSC: Follow-up of
patients with ventricular tachyarrhythmia treated with the auto-matic implantable cardioverter defibrillator: Programmed elec-trical stimulation results do not predict clinical outcome.J Electrophysiology 1989;3:467-476
28. Reiter MJ, Fain ES, Senelli KM, Cadence Investigators: Determi-nants of recurrent ventricular arrhythmias in patients with implant-able pacemaker/defibrillators. (abstract) Circulation 1991;84(supplII):II-426
29. Zilo P, Gross JN, Benedek M, Fisher JD, Furman S: Occurrence ofICD shocks and patient survival. PACE 1991;14:273-279
30. Josephson ME: Myocardial infarction: Special considerations, inClinical Cardiac Electrophysiology, ed 2. Malvern, Lea & Febiger,1992, pp 616-629
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

W Grimm, B T Flores and F E Marchlinskitherapy.
Shock occurrence and survival in 241 patients with implantable cardioverter-defibrillator
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1993 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.87.6.1880
1993;87:1880-1888Circulation.
http://circ.ahajournals.org/content/87/6/1880World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 5, 2018http://circ.ahajournals.org/
Dow
nloaded from