asymmetrical hypertrophic cardiomyopathy...
TRANSCRIPT

Asymmetrical Hypertrophic CardiomyopathySimulating Mitral Stenosis
By RALPH SHABETAI, M.D., M.R.C.P., (Edin), AND SIDNEY DAVIDSON, M.D.
SUMMARYHypertrophic cardiomyopathy usually involves the left ventricle more severely than
the right, and when asymmetrical may. produce the syndrome of idiopathic subaorticstenosis. Less commonly, clinical manifestations of inflow-tract obstruction predomi-nate and produce a syndrome that may be mistaken for mitral stenosis, principallybecause of an apical diastolic rumbling murmur. The probability of this diagnosticerror and the risk of a consequent unnecessary operation can be reduced by appreci-ating the significance of the clues to left ventricular disease revealed by the electro-cardiogram and the chest roentgenogram. Furthermore, proper timing of the heartsounds differentiates the protodiastolic filling sound of cardiomyopathy from the open-
ing snap of mitral stenosis. The correct diagnosis is established following ventriculo-graphic and hemodynamic studies.
Additional Indexing Words:Mitral valvotomyCardiomyopathy with inflow-tract obstructionLeft ventriculogram
J N 1958, TEARE, with considerable diffi-dence, reported eight cases of asymmetri-
cal hypertrophy of the heart.1 Soon thereafter,a vast literature appeared stressing the impor-tance of left ventricular outflow obstruction inhypertrophic cardiomyopathy. In his descrip-tion, however, Teare included a case offishmouth distortion and narrowing of anintrinsically normal mitral valve, but did notmention outflow obstruction. His patient hadatrial fibrillation, an apical rumbling diastolic
From the Department of Medicine, Division ofCardiology, University of Kentucky Medical Center,Lexington, Kentucky.
Supported by National Institutes of Health grantsHE 05598-07, HE 05771-04, and HE 05354-12.
Dr. Davidson was a National Institutes of Healthtrainee, Department of Medicine, University ofKentucky. His present address is Peter Bent BrighamHospital, Boston, Massachusetts.
Address for reprints: Ralph Shabetai, M.D.,Division of Cardiology, Department of Medicine,University of Kentucky Medical Center, Lexington,Kentucky 40506.
Received June 7, 1971; revision accepted forpublication August 12, 1971.
Ciirculation, Volume XLV, January 1972
ElectrocardiographyEchocardiography
murmur and thrill, and a soft aortic diastolicmurmur. The chest roentgenogram showedthe heart to be of "mitral shape," but theelectrocardiogram demonstrated "left ven-tricular preponderance" and abnormal Qwaves. The patient died 1 day after mitralvalvotomy. The importance of this observationhas been obscured by the interest subsequent-ly aroused by the description of idiopathichypertrophic subaortic stenosis and the con-troversy regarding the mechanism responsiblefor outflow-tract gradients. Although Goodwinand his co-workers2-5 in their earlier studiesof hypertrophic obstructive cardiomyopathystressed the importance of outflow-tractobstruction, they also alluded to inflow-tractobstruction and emphasized that diminisheddiastolic compliance of the left ventricularmyocardium is an important component of thepathophysiology of this condition. In theirlater reports6' 7these investigators reempha-sized that diastolic filling is limited by theinordinately high left ventricular diastolicpressure and by septal hypertrophy, and theystated that "we now believe that resistance to
37
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from
SHABETAI, DAVIDSON
ventricular filling consequent upon hypertro-phy and rigidity is the miiost important featureof the disease" and "'may vell be of gre.atersignificance than outflow tract gradients."Apical rumblincg and blowing diastolic mur-muirs have frequiently been reported in ob-structive cardiomyopathy with outflow-tractobstruiction,' 2,2, 6. 8 12 although Braunwaldand associatesl8 reported finldinig a diastolicmurmur in only one of 64 such patientsstudied.Echocardiograms of patients with hypertro-
phic obstructive cardiomyopathy have demon-strated that in early diastole the velocity ofposterior motion of the anterior leaflet of themitral valve is reduced in a manner compara-ble to that found in mild or moderate mitralstenosis 164-1 Analysis of the slope of descentof the left atrial V wave has furnishedadditional evidence that left ventricuilar fillingin hypertrophic obstructive cardiomyopathy isslower than normal.'7 Factors which may be
responsible for impaired left ventricular fillinginclude hypertrophy and increased wall thick-ncess per se, altered diastolic compliance of themyofibril, and impedance posed by the septumor by the anterior leaflet of the mitral valve.The purpose of this paper is to report three
cases of hypertrophic cardiomyopathy withobstruction confined to the inflow tract of theleft ventricle. We are reporting them, not asclinical curios, but because the syndrome maymimiiic mitral stenosis, vith potentially disas-trous consequences.These cases of primary myocardial disease
were characterized by exertional dyspnea, aloud apical first sound, a low-pitched apicaldiastolic mur-mur, and an initial clinicaldiagnosis of mitral stenosis. All of them werereferred to the University of Kentucky Medi-cal Center for mitral valvotomy. Since inmany centers patients with mitral stenosisundergo cardiac surgery without cardiaccatheterization, we feel that it is important to
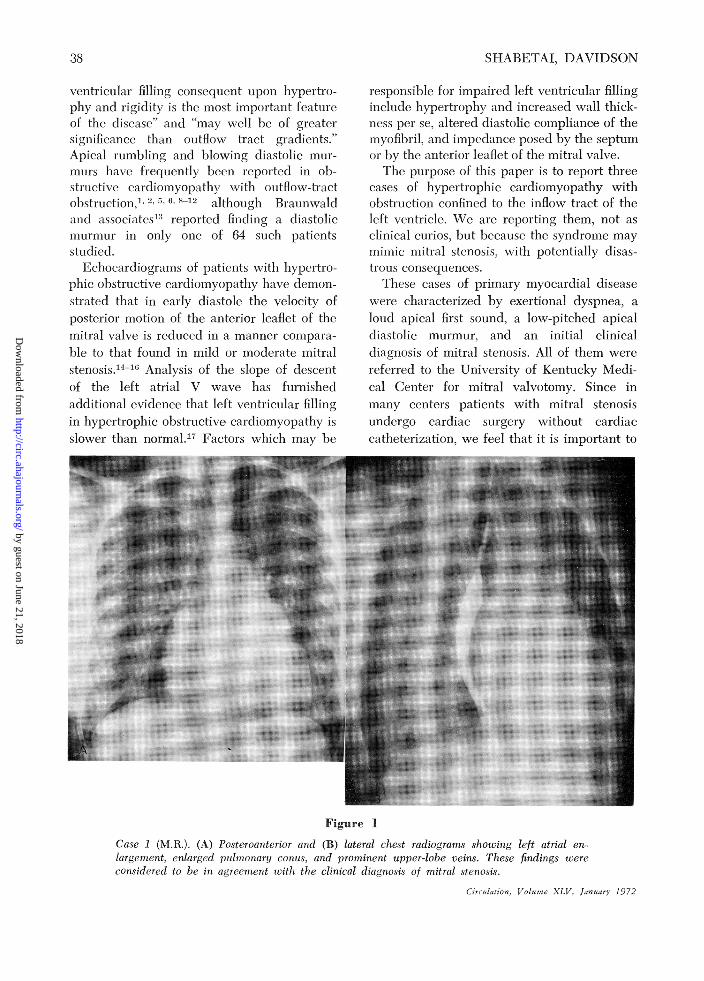
Figure 1
Case 1 (M.R.). (A) Posteroanterior and (B) lateral chest radiograms showing left atrial en-largenient, enlarged pulmonary conis, and prominient upper-lobe veins. These findings wereconsidered to be in agreement wvith the clinical diagnosis of mitral stenosis.
(irc flaiion, Volaune XLV, January 1972
38
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

HYPERTROPHIC CARDIOMYOPATHY
.,.,1-- :
,I1I ' S,'
*;2W
..>* . s W.j s.. i, i :. . Jjg -r S - ---i*; ... .....
i.-- .._ -: ::, r .--:.
I
V1
-tr --i
It-A - AL- - .g -
M. R.
_.t_i_i..'' . ' D . o' ' ... 'i--- a -1t,; -.
_§ l4. 't_wF^- ---:-- - - '
S
,.7 .. .n .,w_ ¢- ) |- ..-E -- r- - ---;- - - z . ., . F t X, * g ,, . _ .. _ .@ - . .- . -4--F-- s. - ^-
:.: :,4 -! -.
._ _ X __ _, : ......... w: ^ .... t : t4 v. s . .i,
- f ^- -. ^ - .. ?.. .'.1 ;. -4 _ .i,4 - . f - -: - . - - f - - -
4__ 4-t *-8 ! ..- --*...... . i - < .. -;-^- --- r-:it 'fi -i-- t---w*_st_ _
.:;--:d ;-- :-Stf-.. iS;..'1t-:-.- t. :. ....}+.s- y - - ;t r, . -i; - ^ -e ;--[- -. . _-4^4-.+ .
;..} ,._ _* .._..,. .._i- 5
-t --- A -..- .-r t-_; .._ .. ,, ^. _ -. . .u. J:r_ ij- .s-. -t- ttt -t _E _. _._;^: ^y s->st- t + -.x, <- 1 n t;>^ .L- t -- ¢, -
W-*- i e-. ^e._ n._j _. 4 tt-; e ' f... -i^' ._ <_.. :.,*¢.. _ ,. i f; + .--- t-_LxFigure 2
Case 1 (M.R.). The P wave is wide and notched and has a wide posterior vector. The AQRSis approximately 75°. T is biphasic in V4 and V, and inverted in V6. S is of large amplitude inV -, and QRS is notched in V,. In spite of the changes suggesting left ventricular disease therecord was interpreted as compatible with the clinical diagnosis of mitral stenosis.
draw attention to this syndrome which may
simulate mitral valvular obstruction but is notamenable to operative treatment.
Report of CasesCase 1 (M.R.)
The patient, a 44-year-old woman, complainedof palpitations and mild exertional dyspnea.During the year before admission progressiveexertional dyspnea, orthopnea, nocturnal dys-pnea, and hemoptysis developed. She was
referred to a university hospital where mitralvalvotomy without prior catheterization was
recommended. The patient refused operation butcontinued to experience severe exertional incapac-ity. She was admitted to the medical center on
November 23, 1966, for mitral valvotomy.Physical findings included elevated venous
pressure and jerky arterial pulses of smallamplitude. A right parasternal lift was palpable,and the apical first heart sound was loud and was
followed by a short apical systolic murmur. Athird sound preceded a loud apical diastolicrumbling murmur. A high-pitched murmur ofsemilunar insufficiency was heard. Cardiac fluoros-copy revealed no valvular- calcification. Chestroentgenograms showed that the left atrium andboth ventricles were enlarged (fig. 1). The ECGshowed several abnormalities. The P wave was
Circulation, Volume XLV, January 1972
wide and displayed a large late posterior vector.The mean QRS axis in the frontal plane wasapproximately 75°. The QRS complexes dis-played deep S waves in leads V1 and V2 and alate rightward force. The T waves were invertedin leads V5 and V6 (fig. 2). A clinical diagnosis ofrheumatic heart disease with dominant mitralstenosis was made. Surgical intervention againwas advised and for this reason cardiac catheter-ization was performed. Cardiac catheterization(table 1) revealed no diastolic pressure differencebetween the left atrium and the left ventricle.The ventricular septum and the posterior papil-lary muscle were greatly hypertrophied. Leftatrial injection through a transseptal catheterdemonstrated poor opacification of the appen-dage, wide patency of the mitral valve, andasymmetrical hypertrophy of the left ventricle(fig. 3A). The aortogram revealed minimal aorticinsufficiency. The left ventricular diastolic pres-sure was elevated and the cardiac output wasreduced. Left ventricular systolic pressure wasequal to that in the ascending aorta.
Six months later, the patient was readmittedwith axillary vein thrombosis and pulmonaryembolism. In the ensuing months pulmonaryembolism recurred frequently and progressivecardiac failure developed. The apical systolicmurmur became louder and longer suggestingthat mitral incompetence had worsened. The
,4 ..
- IIf:|: ..a .s
, l.-- ,1-aY_R..
V i_4
4 3
aVL
Vs
aLVi
V6
39
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

SHABETAI, DAVIDSON
Table 1
Sumunary of Data oni Cardiac Catheterization
C'ase 1 (A1.11.)7 9/9i68
Case 3 (S.M.)6/6/69
Pr.esstniie (mi3 Hg)PCPA10\lH ALVLAAoiit a
Cardiac otutptl
ll:1Exercise
Left veiitriculogranLV septunm thiukIJV papillary mulltiles
thickilitral incompetence
20
47 15-47/4
412:) 7
1'I128
3.08I_.6
Yes
Yes
3- 1
67/ 1
67 5.)
6
104 '20
.104 /61)
Yes
Yes+ ++++ +++ ++++
2.5
1.50/22
6.0
7.2
Nes
Yes
1129/1129 51)
140/ 11
140/90
20
40/ 1940/11
13.5 21
185; /9(0
6.6
Yes
YesYes0} H--V++++ -+++
Abbreviat.ions: PC pu.lmoiiary (apillalir; PA
LV anid LA = left ventricle anid attrium.ptulriionlary Rrteiyt.i aidi HA ilight ventricle anid atriim;
Figure 3
Case 1 (M.R.). Left ventriculograrn, October 10, 1968. (A) Anterior posterior projectioni. (B)Lateral projection. (A) The lowcer arrow points to the hypertrophic interventiciclar septuim,aind the upper arr.ows point to the unusuially clear mitial "`wash in" which is a fturther signof septal hypertrophy. (B) The arrow poinits to diastolic coning of the outflow area causedby the hypertrophic rigid septum.
Circulation, Volume XLV, JanuarY 1972
11 28A66('ase 2 (P.P.)
10/ 2 /65 4/24J67
40
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

HYPERTROPHIC CARDIOMYOPATHYm 07 03 43- 7-1068
..p
ANT -a-
41
)4 88 66 - 8-29-69 SM 07 37 94 -5-29-69*AN T.f ~~~~~~ANT-
A'~~~~. -.SG-
Figure 4
Echocardiograms front left to right: case 1 (M.R.), case 2 (P.P.), anid case 3 (S.M.). (A) (M.R.)Closure is rapid and characteristic of severe mitral incompetence. (MVE =mitral valve echo,SE = septal echo.) (B) (P.P.) Slowing of the diastolic movement toward closure. The septalecho is not represented. (C) (S.M.) Early diastolic closure is slowed and the leaflet remains inthe mid openi position through the latter two thirds of diastole.
cardiac signs were otherwise unchanged. Echo-cardiography showed rapid and extensive motionof the anterior leaflet of the mitral valve (fig. 4A)inconsistent with mitral stenosis, but compatiblewith mitral incompetence.
Cardiac catheterization was repeated on July 9,1968 (table 1). The changes that had taken placein 20 months were due to the development ofsevere mitral incompetence, as documented byleft ventriculography, echocardiography, and theappearance of tall V waves with rapid Y descentin the pulmonary wedge tracing.
Isoproterenol infusion (4 jug/min) did niotprovoke a systolic pressure difference between thecavity of the left ventricle and the aorta.
Case 2 (P.P.)
This 32-year-old woman was referred onOctober 25, 1965, for mitral valvotomy. Completeleft bundle-branch block was discovered in aroutine ECG made in October 1964. She was welluntil March 1965 when she began to experienceexertionial dyspnea.On examination, the venous pressure was
Ci culation, Vo/ume XLV, January 1972
normal but showed a dominant a wave. The bloodpressure was 120/70 mm Hg and the heart ratewas 76/min. The apex beat was in themidelavicular line, and a left parasternal lift waspalpable. The intensity of the first heart sound atthe apex was increased, and the second heartsound was paradoxically split. A third heartsound and an apical diastolic rumbling murmurwith loud presystolic accentuation were auscul-tated at the apex. Roentgenographic studiesrevealed slight cardiomegaly and left atrialenlargement. The ECG showed complete leftbundle-branch block.
Cardiac catheterization was carried out onOctober 27, 1965 (table 1). The left ventricularend-diastolic pressure was elevated, and thedegree of pulmonary hypertension was commen-surate. The opacified left ventricle showedlhypertrophy of the septu-m and an anter ior,tonguelike prlOtrlusion. The right ventriculardiastolic pressure was abnormal and displayed theconfiguration of an early diastolic dip followed bya high plateau. There was practically nodifference between the pulmonary wedge and left
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

42 ~~~~~~~~~~~SHABETAL,DAVIDSON
ventricular pressures at end-diastole, but thisdifference averaged from 10 to 5 mm Hg duringthe first half of diastole.
Clinical reevaluation was undertaken onSeptember 17, 1969. She reported an episode ofpulmonary embolism. Upon recovery, she wasleading a moderately active and asymptomaticlife. The only change on clinical, electrocardio-graphic, and roentgenographic examination of theheart was an increase in the apical systolicmurmur. The echocardiogram (fig. 4B) showedan ample range of motion of the anterior leaflet ofthe mitral valve, but some slowing of itsmovement toward closure.
Case 3 (S.M.)This 48-year-old woman was admnitted in
February 1967 for treatment and evaluation ofaphasia and fight hemiparesis of 8-days' duration.The blood pressure was 110/70 and the pulse
rate was 120/mmn and irregular. The apex beatwas normally located, but she had a leftventricular heave. The apical first heart sound
7 1- +
r..
1, t-np <14z
js
ruSttt ,
... F...
.
Figure 5
Case 3 (S.M.). The loud third heart sound and theshort apical diastolic murmur (MDM) which werinterpreted as evidence for mitral stenosis are illus-trated. Note atrial fibrillation. The record was madeshortly after admission to the hospital for treatment ofan acute cerebrovascular accident.
was abnormally loud, and she had a third heartsound and a soft rumbling apical diastolicmurmur (fig. 5). The chest roentgenogramshowed moderate cardiac enlargement andprominence of the left atrial appendage. TheEGG recorded atrial fibrillation and small Qwaves in leads II, III, aVF, V5,, and VC, Nineweeks later, she underwent cardiac catheteriza-tion (table 1). At the beginning of diastole therewas a pulmonary wedge to left ventriculardiastolic pressure gradient of 10 mm Hg.However, the gradient diminished during diasto-le, such that in a long cardiac cycle the pressureswere equal from middiastole onward. A diagnosisof mitral stenosis was made, but operation wasnot advised because the obstruction was judgedto be mild and the EGG suggested coronaryartery disease.
After discharge, exertional symptoms increasedto the point that she was no longer able toaccomnplish her household duties. This led to areview of her left ventriculogram and ECGs and arevised diagnosis of primary myocardial disease.The vectorcardiogram suggested left ventricularhypertrophy. The echocardiogram (fig. 4C) wasabnormal in that the slope of closure of theanterior leaflet of the mitral valve was interrupt-ed by a long plateau.
Cardiac catheterization was repeated 20months after the first study. The pulmonary arteryand pulmonary capillary pressures had increased,the mitral insufficiency had worsened, and thecardiac output had diminished. The differencebetween pulmonary wedge and left ventricularend-diastolic pressure remained zero followinglong R-R inter-vals. The left ventriculogramdisclosed triangulation of the outflow tract typicalof septal hypertrophy. This appearance was verysimilar to that of the earlier study, but mitralincompetence had greatly increased. No evidenceof outflow-tract obstruction was elicited byinfusion of 4 gg/min of isoproterenol.
Discussion
The history was no.t helpful in diagnosis.Exertional dyspnea, orthopnea, palpitations,and peripheral edema are identical to those ofrheumatic mitral valvular stenosis. Likewise, ahistory of pulmonary or cerebral embolizationand of atrial fibrillation is a nonspecificindication of heart disease.The clinical examination yielded findings
that were deceptive and led, in all threepatients, to the erroneous diagnosis of mitralstenosis. In all, the apical first heart sound was
abnormally loud, and in all a delayed apicalCirculation, Volume XLV, January 1972
42
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

HYPERTROPHIC CARDIOMYOPATHY
diastolic murmur with a low-pitched rumblingquality was heard. The murmur was indis-tinguishable from that of mitral stenosis.Under the circumstances, the third heartsound was mistaken for the opening snap ofmitral stenosis, an error that would have beenavoided had simultaneous apex cardiogramsbeen obtained.12 An apical systolic murmur,which is common even in "pure" mitralstenosis,18 is the rule in mixed mitral valvelesions, and therefore is not helpful indistinguishing primary myocardial diseasefrom rheumatic mitral valve disease. A leftventricular heave without evidence of mitralincompetence, aortic valve disease, or hyper-tension is an anomalous finding in a patientwith the auscultatory findings of mitralstenosis and should strongly suggest thediagnosis of primary myocardial disease.
All three of our patients showed un-equivocal roentgenographic evidence of leftatrial enlargement. Pulmonary venous con-gestions with prominence of the upper-lobevasculature was indistinguishable from thatseen in patients with mitral stenosis. All hadstraightening of the left heart border, but incase 1 (M.R.) the films also suggested leftventricular enlargement, a finding whichshould have led to clinical distrust of thediagnosis of pure or dominant mitral stenosis.Calcification of the mitral valve was absent inall the patients. Conventional radiologic studyof this syndrome yields results that superficial-ly suggest mitral stenosis, but more thoroughscrutiny discloses abnormalities which impli-cate left ventricular enlargement.Electrocardiography
The ECG can be helpful in differentiatinginflow-tract obstruction from mitral stenosis;however, the ECGs recorded from case 1(M.R.) showed atrial fibrillation or P mitraland a frontal plane QRS axis of 750 and wereconsidered to be consistent with mitral steno-sis. However, the deep S waves in the rightprecordial leads and the T inversions in theleft precordial leads should certainly havearoused suspicion of left ventricular hypertro-phy. The ECGs in the other two cases weremore helpful. That in case 2 (P.P.) registeredCirculation, Volume XLV, January 1972
complete left bundle-branch block, an extra-ordinarily rare finding in mitral stenosis but acommon one in myocardial disease and leftventricular hypertrophy. In case 3 (S.M.), Qwaves in leads reflecting the inferior andlateral aspect of the myocardium were usefulin establishing the diagnosis of primarymyocardial disease. This finding and thevectorcardiogram, which showed signs of leftventricular hypertrophy, would not be ex-pected in ordinary mitral stenosis. Thus, whilesome features consistent with mitral stenosismay be seen on the electrocardiogram, thetracing may be expected to reveal in additionevidence of left ventricular hypertrophy andmyocardial abnormality.
Echocardiography
Echocardiography was helpful in excludingsignificant mitral stenosis but was disappoint-ing in that, so far, it has not yielded a patterndiagnostic of inflow-tract obstructive cardio-myopathy. Excursion of the anterior leaflet ofthe mitral valve was normal or supranormal inall the cases. and this observation establishedthat the valves were pliable. In S.M. and P.P.the rate of mitral valve closure was slowerthan normal. In these cases it is probable thatimpedance to left ventricular filling caused byreduced diastolic compliance of the leftventricle or extrinsic distortion of the valve asin Teare's' case was the cause of slow closureof the anterior leaflet of the mitral valve. Fur-ther experience with echocardiography in hy-pertrophic cardiomyopathy without outflow-tract obstruction may clarify this problem.
Cardiac Catheterization
Hemodynamic studies were helpful, butinterpretation was not always straightforward.The data in case 1 (M.R.) provided unequiv-ocal es ,dence against mitral stenosis becauseleft atriai and left ventricular diastolic pres-sures equiAibrated perfectly at rest and duringexercise. The cardiac output was diminishedand the left ventricular end-diastolic pressurewas elevated. These data were compatiblewith myocardial disease and incompatiblewith mitral stenosis but failed to disclose the
43
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

SHABETAI, DAVIDSON
reasoins for the clinical simulation of mitralstenosis.The pressure data from cases 2 and 3 (PP.
and S.M.) demonistrated a gradient of 2 to 3mm Hg across the mitral valve confined toearly diastole. Such small pressure differences,although sometimes found in mild mitralstenosis, especially in association with lowcardiac output, are not uncommon for patientswvithout mitral stenosis. In case 2 (P.P.) theleft ventricular end-diastolic pressure was
conspicuously increased. Diminution of car-
diac output and elevation of left ventriculardiastolic pressure were not documiented untilthe second cardiac catheterization in the thirdcase (S.XI.). The left atrial or pulmonary'Wedge pressure tracinigs showed large Vxvaves at the time of the second catheteriza-tion in both the patients in whom thisprocedure was repeated. Evidence for outflow-tract obstruction was not disclosed in any ofthe cases by postextrasystolic beats, exercise,
or isoproterenol infusion.Left ventriculography xxvas of crucial im-
portance. In all three patients the opacifiedleft ventricle appeared grossly abnormal. Themyocardium was thick and showed muchhypertrophy of the septum and a ragged,concave diaphragmatic surface. \Mitral incom-petence was demonstrated by reflux of con-
trast medium into an enlarged left atrium inall three patients. In both patients wvhounderwent second hemodynamic studies 18and 20 months after their first catheterizations.mitral incompetence had substantially in-creased.As in all types of primary myocardial
disease, the etiology is obscure. None of thepatients had evidence of preceding myocar-
ditis, but iral studies vere not undertaken.These cases of asymmetrical left ventricularhypertrophy with inflowv-tract obstruction lackthe clinical ventriculographic and hemody-namic indicators of outfloxv-tract obstructionand cannot be considered to be cases ofidiopathic subaortic stenosis.
Clinical CourseThe clinical course suggests that the natural
history is one of rapid deterioration, xvith
atrial fibrillation, thromboembolic complica-tions, progressive mitral incompetence, andrapidly advancing cardiac failure. The clinicalfeatures changed dramatically in the last 3vears of I.R.'s life. In that spaln, the signis ofmitral stenosis gaxve w.7ay to those of a mixedmitral valve lesioni. Atrial fibrillation, axillarxvine thrombosis, pulmoinary emboli, anidiintractable cardiac failure followed relentlesslyupon each other. In the 2 y.ears that haveelapsed since \ve first examined P-P., she hassustained pulmonary emboli and episodicheart failure. When we first encountered S.M.,she displayed the findings of mitral stenosis.Txx o years later she had signs of mitralincompetence. Her subsequent course h-asbeen that of progressive cardiac failure.
Conclusions
The mechanisms for the loud apical firstheart sound and diastolic rumbling mnurmurremain in doubt. The P-R interval was notabbreviated in ainy instance. In individualcases the mechanisms differ. Thus, in S.M. andPP.. echocardiography and small mitral dia-stolic pressure gradients were compatible xvitbmitral valve distortion, but in M.R. evidencefor mitral restriction was absent.The prognosis is poor and the specific
dangers are pulmonary or cerebral embolism,atrial fibrillation, progressive mitral incompe-tence, and cardiac failure. The diagnosisdepends upon recognizing that apical diastolicrumbling murmurs are not necessarily diag-lnostic of mitral stenosis or left-to-right shunt.They may be audible in left ventriculardysfunction. The ECG may offer xvaluablepointers to left ventricular disease, and theechocardiogram excludes severe mitral steno-sis. The apex cardiogram is valuable in distini-guishing early protodiastolic gallop soundsfrom late opening snaps. Careful roentgeno-graphic ex aluation will frequently discloseevidence of left ventricular disease incompati-ble with the diagnosis of predominant mitralsten osis. Hemodynamic studies exclude severemitral stenosis and provide functional andstructural proof of left x-entricular disease.
Ci,ul it on,VI oluione LI J xl 97
44
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

HYPERTROPHIC CARDIOMYOPATHY
References1. TEARE D: Asymmetrical hypertrophy of the heart
in young adults. Brit Heart J 20: 1, 19582. COHEN J, EFFAT H, GOODWIN JF, OAKLEY CM,
STEINER RE: Hypertrophic obstructive cardi-omyopathy. Brit Heart J 26: 16, 1964
3. GOODWIN JF, GoPDON H, HOLLMAN A, BISHOPMB: Clinical aspects of cardiomyopathy. BritMed J 1: 69, 1961
4. GOODWIN JF: Cardiac function in primarymyocardial disorders. Brit Mled J 1: 1527,1964
5. GOODWIN JF, HOLLMAN, A, CLELAND WVP,TEARE D: Obstructive cardiomyopathy simulat-ing aortic stenosis. Brit Heart J 22: 403,1960
6. GOODWIN JF: Obstructive cardiomyopathy. Car-diologia 52: 69, 1968
7. GOODWIN JF: Congestive and hypertrophiccardiomyopathies. Lancet 1: 731, 1967
8. HANSEN PF, DAVIDSEN HG, FABRICUS J:Subvalvular aortic stenosis of muscular type.Acta Med Scand 171: 6, 743, 1962
9. BRACHFIELD N, GORLIN R: Functional subaorticstenosis. Ann Intern Med 54: 1, 1961
10. PARE1 JAP, FRASER RG, PIROZYNSKI WJ, SHANKSJA, STABINGTON D: Hereditary cardiovasculardysplasia. Amer J Med 31: 37, 1961
11. MEERSCHWA-M: Hypertrophic Obstructive Cardi-omyopathy. Baltimore, Williams & WilkinsCo., 1969
12. Case Records of the Massachusetts GeneralHospital. New Eng J Med Sept. 4, 1969
13. BRAUNWALD E, LANIBREW CT, ROCKOFF SD,Ross J JR, MORRow AG: Idiopathic hypertro-phic subaortic stenosis: I. A description of thedisease based upon an analysis of 64 patients.Circulation 30 (suppl IV): IV-3, 1964
14. Popp RL, HARRISON DC: Ultrasound in thediagnosis and evaluation of therapy of idi-opathic subaortic stenosis. Circulation 40: 905,1969
15. SHAH PM, GRAMXIAK R, KRAMER DH: Ultra-sound localization of left ventricular outflowobstruction in hypertrophic obstructive cardi-omyopathy. Circulation 40: 3, 1969
16. MIOREYRA E, KLEIN JJ, SHINIADA H, SEGAL BL:Idiopathic hypertrophic subaortic stenosis di-agnosed by reflected ultrasound. Amer J Cardiol23: 32, 1969
17. STEWARD S, 'MASON DT, BRAUNWALD E: Im-paired rate of left ventricular filling inidiopathic hypertrophic subaortic stenosis andvalvular aortic stenosis. Circutlation 37: 8,1968
18. SURAWICz B, MERCER C, CHLEBUS H, REEVES JT,SPENCER FC: The role of the phonocardiogramin the evaluation of the severity of mitralstenosis and the detection of associated valvelesions. Circulation 34: 798, 1966
Circulation, Volume XLV, January 1972
45
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

RALPH SHABETAI and SIDNEY DAVIDSONAsymmetrical Hypertrophic Cardiomyopathy Simulating Mitral Stenosis
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1972 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.45.1.371972;45:37-45Circulation.
http://circ.ahajournals.org/content/45/1/37located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from