treatment of obstructive hypertrophic cardiomyopathy symptoms
TRANSCRIPT

1
Treatment of Obstructive Hypertrophic Cardiomyopathy Symptoms and
Gradient Resistant to First-Line Therapy with Beta-Blockade or Verapamil
Sherrid et al: Obstructive HCM Resistant to First-Line Therapy
Mark V. Sherrid, MD; Aneesha Shetty, MD, MPH; Glenda Winson, RN;
Bette Kim, MD; Dan Musat, MD*; Carlos L. Alviar, MD; Peter Homel, PhD;
Sandhya K. Balaram, MD; Daniel G. Swistel, MD
Hypertrophic Cardiomyopathy Program, St. Luke’s-Roosevelt Hospital Center, Columbia
University, College of Physicians & Surgeons, New York, NY
*Current address: Valley Health Care System, Ridgewood, NJ
Correspondence to Mark V. Sherrid, MD 1000 10th Avenue New York, NY 10019 Phone: 212 523 7370Fax: 212 523 7765Email: [email protected]
DOI: 10.1161/CIRCHEARTFAILURE.112.000122
Journal Subject Codes: Heart failure:[11] Other heart failure, Treatment:[118] Cardiovascular pharmacology, Cardiovascular (CV) surgery:[39] CV surgery: other
lllllllt t t t t t t HoHoHoHoHoHoHospspspspspspspitititititititalalalalalalal CCCCCCCenenenenenenenttttttt
N YYYYYYY kkkkkkk NYNYNYNNYNYNniversity, College of Physicians & Surgeons, New York, NY
C
D
niversityyyyy,,,,, College of Physicians & Surgeons, ,,,, New York, NY
Curururrrrent adddddreessss: VaVaVaVaVallllll eyyyyy HHeeealtlthh CaCCareeeee SSSSSysyy teemmm, RRidddddggeggg wowowowowoodododdd, NJNNNN
DD
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

2
Abstract
Background—There is controversy about preferred methods to relieve obstruction in hypertrophic
cardiomyopathy (HCM) patients still symptomatic after beta-blockade or verapamil.
Methods and Results—Of 737 patients prospectively registered at our institution, 299 (41%) required
further therapy for obstruction for limiting symptoms, rest gradient 61+45, provoked gradient 115+49
mmHg, followed 4.8 years. Disopyramide was added in 221 (74%) and pharmacologic control of
symptoms was achieved in 141 (64%). Overall, 138 (46%) patients had surgical relief of obstruction
(91% myectomy), and 6 (2%) alcohol septal ablation. At follow-up resting gradients in the 299
patients had decreased from 61+44 to 10+25 mmHg, p<0.0001; NYHA class decreased from 2.7+0.7
to 1.8+0.5, p<0.0001. Kaplan-Meier survival at 10 years in the 299 advanced-care patients was 88%
and did not differ from non-obstructed patients (p=0.28). Only one patient had sudden death, a low
annual rate of 0.06%/year. KM survival at 10 years in the advanced-care patients did not differ from
that expected in a matched cohort of the US population (p=0.90).
Conclusions—Patients with obstruction and symptoms resistant to initial pharmacologic therapy with
beta-blockade or verapamil may realize meaningful symptom relief and low mortality through stepped
management, adding disopyramide in appropriately selected patients, and when needed, by surgical
myectomy.
Key Words: hypertrophic cardiomyopathy, surgery, pharmacologic treatment
NYHA class dddddddeeceeeee
99 adadadaddadadvavavavavavavancncncncncncncededededededed-c-c-cccccara
o u
% s
ooooom mmmm non-obobobobobstsstststrurururuucccccteteteteted d d d papapapapatititititienenenee tsssss (((p=p 00.288888).)))) OOOOOnlnnlnlnlyyyy ononononone papapapapatititititienenenene t t t t t hahahahahad d d dd su
%/yyyyyeaeaeaeaear.r.r. KKKKKM MMMM sususususurvvrvvvivivivalalalaal aaaaat tttt 100000 yyyyyeaeaeaeaearsrsrsss ininininn ttttthehehehehe aaaaadvdvdvdvdvanananananceceeeed-d-ddd-cacacacacarerererere pppppatatatatatieeieeentntntnn s
atatatchchchededed cccohohohorororttt ofofof ttthehehe UUUSSS popopop pupupulalalatititiononon ((((p=p=p=pp 000.909090).).).
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

3
Left ventricular outflow tract (LVOT) obstruction at rest or after physiologic provocation occurs in
approximately 2/3 of patients with HCM, usually from systolic mitral-septal apposition1 and is
associated with adverse outcomes2. In symptomatic obstructed patients pharmacologic therapy is
the first-line approach. Using recommendations from the previous two decades we selected
treatment paths for patients with obstruction resistant to first-line pharmacotherapy with beta-
blockade or verapamil, based on their cardiac pathology, risk stratification for sudden death, and
symptoms3-7. There have been case series describing the response of obstructed patients to
treatments such as disopyramide, surgery, alcohol ablation, or dual chamber (DDD) pacing with
short AV delay3,7-10. However, given the heterogeneous presentation and anatomy of obstructive
HCM, and the wide age range of presentation from youth to old age, a “one size fits all” approach
cannot be applicable or practical6,11.
Methods
St. Luke’s-Roosevelt Hospital Center (SLR) has offered organized consultation services for
referred HCM patients since 1985; we have maintained a prospective registry of evaluated
patients. The current report includes all patients initially evaluated from 1985 to June 30, 2011.
The diagnosis of HCM was confirmed by demonstrating a hypertrophied (> 15 mm) non-dilated
LV in the absence of a cause of hypertrophy sufficient to cause that observed.
For each patient heart failure symptoms were assessed based on NYHA classification and
the Minnesota Living with Heart Failure Questionnaire (MLHF QOL). All patients signed
informed consent approved by the IRB of SLR for use of their clinical data for research purposes
and for annual questionnaire or scripted telephone follow-up. If patients could not be reached,
their survival was determined by interrogation of the social security death index.
tion and anatooooooommmmmmm
age, a a aaa a “o“ooooonenenenenenene sssssssizizizizizizizee
ee oooorr rrr practitititt cacacacacal6,11.
MeMeththododsss
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

4
Echocardiography: Echocardiograms with standard imaging planes were performed at initial
evaluation and last follow-up. Continuous wave Doppler was used to measure LVOT gradient
from the apical 5 and 3 chamber views to record maximum velocity parallel to the systolic
LVOT flow. Care was taken to separate LVOT signal from that of mitral regurgitation (MR).
Gradient was measured during 3 Valsalva maneuvers and after standing. The simplified
Bernoulli equation was used to calculate gradient. After 1994 capable patients underwent
treadmill testing with Bruce protocol and had gradients acquired after exercise1.
Echocardiographic maximal LV wall thickness was measured from parasternal long axis and
short axis views3. Since 2004 cardiac magnetic resonance imaging was performed in patients
with ambiguous or suboptimal echocardiograms3. The length of the anterior mitral valve leaflet
was measured on the echocardiographic apical three chamber view in diastole from the tip of the
anterior leaflet to the insertion of the non-coronary aortic cusp12,13.
Stepped treatment
After year 2000 all patients were stratified for sudden death (SCD) risk4. Patients who were
deemed to be at increased risk for SCD because of prior sustained ventricular tachycardia or
resuscitated ventricular fibrillation, massive thickening >30 mm, sudden death in first degree
relative, unexplained syncope, or non-sustained ventricular tachycardia in patients < 30 years old
were counseled about the benefits and risks of the implanted defibrillator (ICD) and, given
consent, were implanted3,4. ICD follow-ups were obtained either at our own clinic or through
questionnaires and scripted phone calls. The nature of ICD interventions were confirmed by
analysis of stored electrograms in all cases by a SLR attending electrophysiologist.
Based on their treatment path patients were divided into 3 groups.
ng was performememmmmm
the anananananananteteteteteteteririririririiororororororor mmmmmmmiiiiititi r
e echocardiographic apical three chamber view in diastole o
e
e eeceee hocaaaardrdrdrddioioioi grgrgrgrgrapapapapaphihihihihic c ccc apapapapapiciciciccalalaal ttttthrhh eeee chahahahahambmbmbmbm ererereer vvvvieieieieiew ww ininininin dddddiaiiaiiastststststololololole eeee frff o
e inininininsesesesesertrtrtrttiiiiiononononon ooooof ff thththththe eee nonononoon-n--n--cccoc rororororonananananaryryryryr aaaaaororororrtititititic cccc cucucucucuspspspspsp12,12,12,12,2,1333.
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

5
Group 1: Obstructed, beta-blocker or verapamil. These patients had LVOT obstruction >30 mm
Hg, either at rest or after physiologic provocation and symptoms could be managed with beta-
blocker or verapamil, or they were asymptomatic and required no pharmacologic therapy. In all
obstructed patients vasodilator medications for hypertension or renal disease were stopped3.
Group 2: Obstructed, advanced-care: These obstructed patients required advanced-care because
they had both limiting symptoms and had rest or provoked gradients >50 mm Hg despite
treatment with beta-blockade, verapamil, or both. Group 3: Patients without obstruction at rest or
after provocation.
The treatment paths for the 299 obstructed, advanced-care patients are shown in Figure 1.
1) The largest group of these obstructed, advanced-care patients were started on
disopyramide. Time-release disopyramide 250 mg 2x/day was added to either beta-blocker or
verapamil. If patient weight was <100 pounds, or for mild degree of renal failure (creatinine 1.3-
2.0) initial dose was decreased to 200 mg 2x/day. Disopyramide was initiated during a 3 day
hospitalization under continuous ECG monitoring7,14. Additionally during hospitalization, daily
ECGs were performed to assess the expected QTc prolongation. In patients with an inadequate
echocardiographic response (resting LVOT gradient > 40 mm Hg after 2 days) the dose of
disopyramide was titrated up to 600 mg/day and beta-blockade was optimized to a resting heart
rate of 50-60 bpm.
After hospital discharge patients were seen after 3 weeks and then every 4 months in follow-
up for drug titration and 12 lead ECG monitoring. Follow-up visits were at our center in 85% of
patients; the remaining patients saw their local cardiologists. Regular disopyramide dosing was
continued unless QTc exceeded 525 msec in patients with initial normal QRS duration, or 550-
560 msec in patients with initial intraventricular conduction delay14. Patients who experienced
patients are shohohohohohooww
nts wwwwwwwererererererereeeeee stststststststararararararartetetetetetetedd
e
t e
u
-r-rr-rreeelee ease dddddisisisisisopopopopopyryryryryramamammamididididideeeee 252525252 0 mgmmmm 2x22 /dddddayayayayay wwwwwasassaa aaaaadddddd eddddd ttttto oo o o eiieieieithththththererererer bbbbbe
t weweweweweigigigigighththththt wwwwasasasasas <<<<<1010101100 000 popopopp uuunuu dsdsdsdsds, ororororor fofofofoforr rrr mimimimimildldldldld dddddegegegegegrerererereee ofoffofof rrrrrenenenenenaaaal ll fafafaaaililllururururure
dededecrcrcreaeaeaseseseddd tototo 222000000 mmmg g g gg 2x2x2x/d/d/dayayay. DDDisisisopopopppyryryryy amamamididideee wawawasss inininitititiaiaiateteteddd dududu
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
6
improvement in their limiting symptoms were continued on pharmacologic therapy. To mitigate
vagolytic side effects of dry mouth or constipation, sustained-release pyridostigmine, a
cholinesterase inhibitor, was administered as needed in doses of 90-180 mg, 2x/day. This allows
continuation of adequate disopyramide dosing15. Patients who had no symptom improvement, or
who experienced drug side effects were referred for surgical septal myectomy, unless they had
significant medical co-morbidity or refused surgery3.
2) Selected patients were referred for surgical septal myectomy without an intervening
disopyramide trial. These patients had SAM, mitral-septal contact but also had either: a)
significant coexisting conditions that required combined surgical repair. b) Selected patients who
had the combination of anterior mitral leaflet length > 33 mm plus resting gradients > 85 mm Hg
were also referred to surgery without disopyramide trial because of our experience that such
patients have a mechanical problem that does not respond to pharmacotherapy13. c) patients with
symptomatic prostatism (hesitancy, dribbling) were referred for surgery as disopyramide is
contraindicated in this setting. Depending on patient choice, surgery was performed at SLR in
80% of patients while the remaining 20% had their operations at other North American centers16.
Operative technique and results of the resect-plicate-release (RPR) modification of the standard
Morrow myectomy as performed at SLR have been described previously10. Individual
components of the operation are extended myectomy, horizontal plication of the anterior mitral
leaflet and release of the papillary muscles. Components are selectively applied, as necessary,
depending on scrutiny of the pre-operative echocardiogram, intraoperative transesophageal
echocardiography and direct surgical inspection.
3) DDD pacing with short AV delay and complete ventricular capture was applied sparingly
and selectively in specific conditions3.
repair. b) Sellllececeeeee
us reeeeeeeststststststiiiiiiingngngngngngng gggggggrararararararadidididididd e
o
h .
t p
o suuuuurgery yyy wwwwwitii hohohohohoutututuu dddddisisisisisopopopopopyryryryy ammmmmidii eee ttriaaaaalllll bebebebebecacacacacaususususeeeee ofo oooooururururur eeeeexpxpxpxpxperererererieieieieien
hannnnnicicicicicalalala ppppprororoooblblblbb ememememem thhhhhatatatatat dddddoeeeeesss ss nononononott ttt rererereespspspss ononononond dddd tototototo ppppphahahahaharmrmrmrmrmacacacacacotototototheheheheherararararapypypyypy1131 .
tititismsmsm (((hehehesisisitatatancncncy,y,y,y dddririribbbbbblililingngngg))) wewewererere rrrefefeferererrerereddd fofoforrr sususurgrgrggererery y y yy asasas dddisisisopopop
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
7
Dyslipidemia was treated with appropriate pharmacologic therapy, usually a statin17.
Statistical Methods
Normally distributed data are described as mean ± SD and categorical data as frequency
(percent). Baseline characteristics were compared by ANOVA. In patients who first received
disopyramide and then septal reduction therapy, gradients after disopyramide are reported both
before the intervention, and after the intervention. Changes in gradient and symptoms were
compared using paired t-tests. Cox proportional hazards test was used to compare survival in the
3 treatment groups. Survival rate for the obstructed advanced-care group was compared with
survival rate published by the CDC for the general US population in 2005, matched for age of
diagnosis, gender, and race18. A Microsoft Excel 2007 program (Microsoft Inc. Redmond WA)
developed by Finkelstein19 for calculating a one sample log rank test was used to test for a
difference. SAS 9.1 (SAS, Inc. Cary, NC) was used for all other analyses.
Results
Patients and treatment paths: Of the 737 patients in the registry, 14 patients who received
surgical myectomy before our initial evaluation were excluded from survival analysis. The whole
group of registry patients, n=723 were followed for median 4.5 years (IQR=2.2-7.6). In groups 1,
2 and 3 the follow-ups were 3.9 years (IQR=1.9-6.4), 4.8 years (IQR=2.6-8.1), and 4.9 years
IQR=(2.1-8.1) respectively. Characteristics of the 723 patients in the 3 treatment groups are
shown in Table 1. There were 299 obstructed advanced-care patients (group 2) who had
gradients and symptoms unresponsive to beta-blockade or verapamil requiring further treatment.
The interquartile age range was wide, 45.8-68.2 years. They had been treated before initial
evaluation with beta-blockade (235) or verapamil (64) or both (38). Compared to the other 2
n in 2005, matattttttchcccccc
(Miicrcrcrcrcrcrcrosososososososofofofofofofoft t t t t t t InInInInInInInc.cccccc
llsssssteteteetein19 fofofofofor r r rr caaaaalclclclclculululululatatatatatinininining g g g g a aa aa onononnneeeee saaampmppplelelelele lllllogogogogog rrrranannannk k kkk teststststst wwwwwasasasasas uuuuusesesesesed dddd t
(SSSSSASASASASAS,,, InInInInInc.cc CCCCCarararaaryyy,yy NNNNNC)C)C)C)C) wwwasasasasas uuuuusesesess d dddd fofofofoforrr rr alalalalallll ll otototototheheheheher rrrr anananananalalalalalysysysysyseseeee .
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

8
groups the obstructed advanced-care patients were older, more frequently had rest obstruction,
had greater maximal wall thickness, were more symptomatic, and more frequently had atrial
fibrillation (AF) and coronary disease (CAD). The treatment paths for the advanced-care group
are shown in Figure 1.
Change in gradient depending on the treatment selected is shown in Table 2 and in the Figure
in the supplemental online material. In the whole patient group (n=299) resting gradient
decreased from 61 +44 to 10 +23 mm Hg (p<0.0001). Table 3 shows the change in symptoms by
final therapy selected. Symptom management was an iterative process. Patients who did not
respond to disopyramide were offered septal reduction. There was improvement in NYHA
classification and MLHF QOL after the final treatment selected in all patient groups.
Disopyramide was administered to 221 patients, mean daily dose 501 ±30 mg, followed for
5.1 +3.8 years. This dose was higher than that used in the multicenter registry of obstructive
HCM patients reported in 2005 (432 +181 mg, p< 0.0001) 7. To mitigate the vagolytic effects of
disopyramide 117 (53%) patients received pyridostigmine timespan, at least temporarily. The
221 patients who were begun on disopyramide might otherwise have been candidates for septal
reduction; but, 141 (64%) were successfully continued on therapy and followed 4.5 +3.6 years
with a favorable response without need for septal reduction. In the whole group of 221 patients
in whom it was used, disopyramide lowered resting gradients, from 63 +45 to 25 +32 mmHg
(p<0.0001). In the 141 patients (64%) successfully managed with pharmacologic therapy
including disopyramide, without need for septal reduction, the average resting gradient was 18
mmHg at final evaluation demonstrating long-term gradient reduction; additionally, symptoms
improved as shown in Table 3. In contrast, in the 80 patients (36%) who eventually required
septal reduction, the final gradients achieved with pharmacologic treatment were lower than
as improvemenennnnnntt
n alall l lllll papapapapapapatititititiitienenenenenenent t t t t tt grgrgrgrgrgg o
w m
f
t g
wawawawawas admimimimm nininininistststststerererererededededed tttto o ooo 222222222211111 papapaaatititit ennntss, mmmmmeaeaeaeaean n n n n dadadadd ililillly y y y y dooooosesesesese 55555010101101 ±±±±±3030303030 m
dddosososososee eee wawawawawasss hihihihihighghghhherereree thahahahahannnn n ththtthatatatatat uuuuusesesesesed dddd ininininin ttttthehehehehe mmmmmululululultititititicececececentntnnn ererererer rrrrregeeee isisisisstrtrtrtrt y yyyy ofofofoo
teteteddd ininin 222000000555 (4(4(4( 323232 +++181818111 mgmgmg, p<p<p< 000 00.00000001)1)1) 77777. ToToTo mmmitititigigiggatatateee thththeee vavavaggg
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

9
initial values (p<0.0001), but were inadequate to control symptoms, and averaged 40 mmHg,
higher than in the patients who could be managed without septal reduction therapy (p<0.0001)
Table 2.
Septal reduction: In 63 obstructed HCM patients surgical myectomy was judged to be the best
treatment without a disopyramide trial. Table 4 shows the characteristics of these patients. The
balance of the septal reduction patients, n=80, were those who received disopyramide but failed
to respond adequately or had drug side effects and who then underwent septal reduction (75
surgical, and 5 alcohol ablation). The 138 patients who underwent surgery were followed for 5.5
±3.6 years; 125 (91%) patients had surgical septal myectomy, and 13 (9%) had mitral valve
replacement for calcific disease. In this series only 6 (2%) patients received ablation, 3 because
of severe medical co-morbidities and 3 because of patient choice. As expected, gradient
reduction was most complete in the surgical group, gradient at follow-up 3 +9 mmHg and
symptoms improved in parallel as shown in Table 3.
Survival: Survival follow-up was complete in 718 (99.3%) patients; 5 (0.7%) patients were
lost to follow-up (only 1 in the advanced-care group). Survival comparison between the 3 HCM
groups, graphed in Figure 2, showed no difference in survival between the 3 groups; 10 year
survival was 87% in group 1, 88% in group 2, and 85% in group 3 (p=0.28).
Deaths in the obstructed advanced-care group: Of the 299 patients there were 25 deaths over
the 5.6 years of follow-up. Fifteen deaths were judged to be non-cardiac, while 10 deaths were
from cardiovascular cause including 4 patients who died after cerebrovascular accidents (mean
age 81, 3 with AF). In the obstructed advanced-care group there was only one sudden death, in a
77 female heavy smoker who died suddenly 7 years after beginning disopyramide. Annual rate
of sudden death was very low 0.06% /year in the whole advanced-care group. There were no in-
d 13 (9%) had d d d d d d mm
ts reeeeeeececececececeeivivivivivivi ededededededed aaaaaaablblblblblblblata
o g
c m
d
o-m-m-m-m-morbididddd titititiieseeee aaaaandndndndnd 3333 bbbbbecececececauauauaa seeeee oof pappatiiiiienenenenent t t tt chhchchhoioioio cecececece. AssAsAsAs eeeeexpxpxpxpxpecececececteteteteted,d,d,d,d, g
comomomommplplplplp etetetetete ininininin ttthehehehehe sururrrrgigigiicccacc l gggggrororororoupupupupu , grgrgrgg adadadadadieieieieientntntntnt aaaaat ttt fofofofofolllllllll owwwww-u-u-u-u-uppp pp 33333 +9+9+9+9+9 mmmmm
d dd ininin ppparararalalallllelelel aaasss shshshowowownnn ininin TTTababablelele 333.
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

10
hospital deaths in our surgical patients, and long-term survival was 95% at 10 years. In the 221
disopyramide-treated patients the annual rate of sudden death was 0.1% /year.
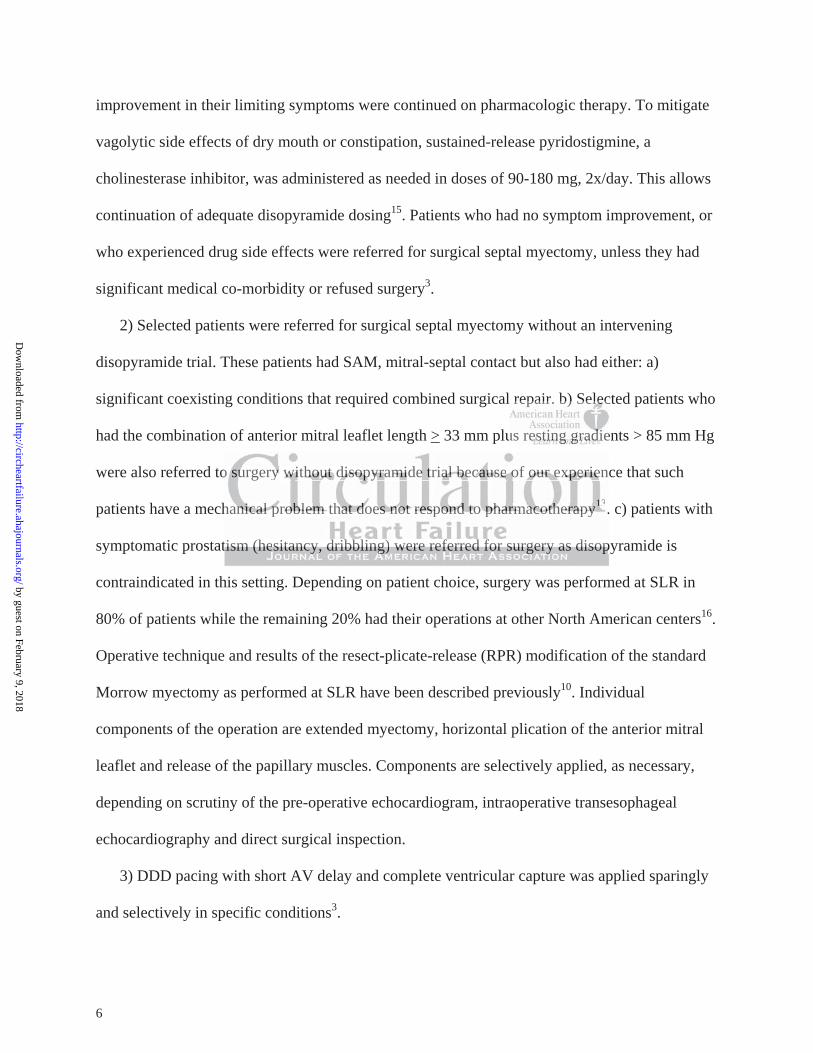
Comparison with age-matched US survival: There were 25 deaths observed in the
advanced-care group while 24 were expected based on the general population. As shown in
Figure 3 the observed rate of survival for the 299 obstructed advanced-care patients did not differ
from the expected survival in the general United States population, p = 0.90.
Device therapy: In the obstructed advanced-care group 56 (19%) patients had ICD
implanted at SLR for primary prevention, and 3 for secondary prevention. ICD patients were
followed up 6.1 +3.5 years. There were appropriate discharges in 3 (5%) patients implanted for
primary prevention. These discharges occurred in 2 patients at 2 months and 5 years after
surgery, respectively, and in one patient 2 years after disopyramide. Two patients implanted for
secondary prevention (both with mid-LV obstruction and an apical akinetic chamber also had
appropriate discharges).
Lethal, and potentially lethal arrhythmias: In the whole advanced-care group events
included sudden death (1 pt), successfully resuscitated ventricular tachycardia (1 pt), post-
operative prolonged non-sustained ventricular tachycardia (1 pt) and appropriate ICD discharge
in primary prevention patients (3 pts). The combined annual rate of lethal and potentially lethal
arrhythmic events was 0.4% /year.
Of the patients with ICD 38 patients were also DDD paced with short AV delay for gradient
reduction. An additional 19 patients had DDD pacemaker inserted specifically for gradient
reduction, but without an ICD. Thus, overall, 57 (19%) of the obstructed advanced-care patients
were DDD paced for gradient in combination with pharmacologic therapy and were followed for
6.3 ± 3.9 years. Only ten (18%) of these patients required surgical myectomy for control of
n 3 (5%) patieentntntnntnn s
monnnnnnnththththththhsssssss ananananananand d d d d dd 5555555 yeyyyy
y t
m
g
y,y,y, aaaaand in nnn onononononeeeee papapapapatitittit enenenenent t ttt 2 2 2 22 yeyeyeyeyearararrrs s sss afaaa teerr dididididisososososopypypypypyraraarramimimimimidedd . TwTwTwTwTwooooo papapapapatititititieneneneent
n (((((boboboboboththththh wwwwitititii hh hhh mimimimimid-dd LVLVLVLVLV ooooobsbsbssstrtrtrtrtrucucucucuctititit ononononon aaaaandndndndnd aaaaan nnnn apapapapapicicicccalalaala aaaaakikikikikinenenenen tiitiiic cc chchchhhamamaama
gggeseses))).
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

11
gradient and symptoms. At follow-up in the paced patients there had been 8 deaths, 4 non-
cardiac and 4 cardiovascular deaths.
Complications in the 299 obstructed-advanced care patients are shown in Table 5.
Discussion
A relatively common clinical dilemma that confronts physicians caring for obstructive HCM
patients is how to manage patients whose symptoms and gradients are resistant to first-line therapy
with beta-blockade or verapamil. These patients represent a subset of HCM patients who often are
referred for advanced care3,16. In this study we applied a stepped approach to this widely
heterogeneous group, in whom therapy was individually tailored for sudden death prevention and
for symptom relief. We found that such an approach can result in a meaningful improvement in
functional status, very low sudden death mortality, and overall mortality that did not differ from
that expected in a matched cohort of the general U.S. population. Additional major observations
from this experience are 1) patients whose symptoms and gradients can be successfully controlled
by disopyramide and beta-blockade have a low mortality, and a very low sudden death mortality.
A similar disopyramide/beta blockade experience has recently been reported by Ball and
colleagues11. In their report, patients who responded to conservative pharmacologic therapy with
symptom relief had an 87% HCM-related survival at 10 years. In their report >150 patients
achieved symptom relief with disopyramide but without septal reduction. In the present report a
similar number achieved symptom relief without septal reduction and together, this experience
numbers nearly 300 patients with excellent survival. In both reports patients who responded to
pharmacotherapy were maintained on their successful regimens, and those who did not were
referred for septal reduction. 2) In the present study, carefully selected patients preferentially
d approach to thththththththi
for sususususususuddddddddddddddenenenenenenen dddddddeaeaeaeeee t
W m
r d
j
WeWeWeWeWe foundndndnnd tttthahahahahat t tt sususususuchchchchch aaaaan n nn n apapapaa prprprprprooach hh caaaaan n n nn rererereresususususultltltl iiiiin n nn n a mememememeanananananinininningfgfgfgfgfululululul im
ry lololololow wwww sususssuddddddddddenenenenen dddddeaeaeaaththththth mmmmmorrrrrtatatatatalililililitttttyyy,yy aaaaandndndndnd oooooveveveveverararararallllllllll mmmmmororooro tatatatatalililililitytytytyty tthahahahahat t didididididdd
atatatchchchededed cccohohohorororttt ofofof ttthehehe ggggeneneneeerararalll UUU.SSS. pppopopopppulululatatatioioionnn. AAAdddddditititioioionananalll mamamajjj
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

12
underwent surgical myectomy3,4. There were no in-hospital deaths in our 138 surgical patients, and
survival at 10 years was 95% with no late sudden deaths.
Stepped management: In our therapy we were guided by additional maxims: 1) all patients
regardless of obstruction and category had formal risk stratification for sudden death; in patients
with high risk implanted defibrillators were placed; 2) patients with concomitant cardiac pathology
like severe CAD, moderate aortic valve disease, or MR from intrinsic mitral abnormalities more
than SAM, had surgery sooner in their course17; 3) We have observed that patients who fail to
respond to disopyramide have a combination of adverse physiologic and anatomic features: both
very high resting gradients and long anterior mitral leaflets as described above. Patients with this
combination (~15% of considered individuals) have a mechanical problem; in recent years we
have referred patients with this combination directly to surgery if they fail beta-blockade
/verapamil, without an intervening disopyramide trial, particularly if they are less than 45 years of
age13,14. 4) patients otherwise were treated by adding disopyramide to their pharmacologic
regimen, usually with beta-blockade5-7,11,14. 5) For elderly or frail patients resistant to
disopyramide DDD pacing with short AV delay was preferred. Disopyramide was continued
because of the previously reported positive synergy between DDD pacing and disopyramide20.
Survival: Overall, mortality in our advanced-care obstructed patients was low; survival did not
differ from the expected mortality observed an age, gender and race matched cohort of the United
States population. Kaplan-Meier survival at 10 years was 88%. These results are similar to that
previously reported when surgical therapy was employed for resistant cases8. Mortality has
previously been reported higher in obstructive HCM patients than in patients without obstruction2.
In sharp contrast, we observed no difference in mortality between our advanced-care obstructed
patients and our non-obstructed patients, Figure 2. There was only one sudden death in the 299
scribed abovee....... PP
al prroboboboboboboblelelelelelelem;m;m;m;m;m;m; iiiiiiin n n n n n n rer
t b
o m
tsssss wwwwwith thththththisisisiss comomomomombibibibibinananananatititititiononononon ddddiiirererrr ctc lyly to o ooo sususususurgrgrgrgrgererereery yy ififififif theheheehey yyyy fafafafafailllll bbbbbeteteteteta-aaaa b
annnnn iiiiintntntnn erererrervevevvevenininininingngnggg ddddisopopopoo yryryryry ammmmmididididideeeee trrtrrtriaiaiaiaial,ll pppppararararartititititicucucuuulalaalalarlrrlrr yy yyy ififififif ttttthehehehehey ararararare ee lelelelelesss
otototheheherwrwrwisisiseee wewewererere tttrerereatatatededed bbby y y y adadaddididingngngg dddisisisopopoppyryryryy amamamididideee tototo tttheheheiririr ppphahaharmrmrm
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

13
patients in the obstructed advanced-care group, a very low annual incidence of 0.06% / year. The
combined annual rate of sudden death, resuscitated ventricular tachycardia and appropriate ICD
discharge in primary prevention patients was low, 0.4% /year. We posit that these low rates of
mortality, sudden death, and potentially fatal arrhythmias occurred because of the stepped
treatment herein described that yielded a mean final resting gradient of 10 mmHg21.
There are few randomized trials of treatments in HCM22. In their absence, below are comments
pertinent to our choices for therapy.
Disopyramide: Introduced by investigators from Toronto, disopyramide is often administered
to patients whose next option would be septal reduction therapy should pharmacologic therapy
fail3, 5-7,11,14. We found a 60% reduction in resting gradient in the 221 patients initiated on
disopyramide and a corresponding improvement in symptoms. Of the patients begun on
disopyramide who might otherwise have been candidates for septal reduction, 141 nearly two
thirds continue on pharmacologic therapy 4.5 years without need for septal reduction.
Disopyramide’s particular efficacy in obstructive HCM is due to its marked negative inotropic
effect compared to other agents23,24, and that it has no vasodilator effect25. In direct head-to-head
comparisons of its effect on gradient, it is more potent than verapamil or beta-blockade24. It is
usually given in combination with beta-blockade to blunt the exercise-related rise in gradient, for
synergistic negative inotropic effect, and to provide AV delay should AF occur. Despite its type I
antiarrhythmic effects, proarrhythmia with disopyramide is very rare in patients with HCM; we
found a very low rate of sudden death mortality, 0.1% /year. This low sudden death incidence may
most likely be attributed to gradient lowering, though we cannot exclude a beneficial intracellular
metabolic effect. Nevertheless, we continue the surveillance described above in our disopyramide-
should pharmamaaaaaaccccccc
2211 pppppppatatatatatata ieieieieieeientntntntntntnts s s s sss ininininininini
e
m 4
h c
cccccororororo respononononndidididd ngngngngng iiiiimpmpmpmpmprororororovevevevevememmmm ntntnnn in ssympmpmpmpmptototototomsmsmsmms.. OfOfOfOO thehehehehe pppppataaaa ieieieeientntntntnts ssss bebbbb
miggiggghththththt oooothththththerererrrwiwiwiww sesesesese hhhavavavavveee bebbbb enenenenen cacacacacandndndndndididdddatatatatateseseseses fffffororororor sssssepepepepeptatatatatal rererereredudududuductcttttioioiooon,nn 111114
hahaharmrmrmacacacololologogoggicicic tttheheherararapypypypyp 444 55.5 yeyeyey arararsss wiwiwithththouououttt neneneededed fffororor sssepepepptatatalll rereredududuccc
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

14
treated patients3,7. We did not observe any organ toxicity from disopyramide, no renal, hepatic,
hematologic or central nervous system adverse effects. This makes it suitable for long-term use.
We administered a higher dose disopyramide in the present cohort than in the multicenter
registry of 2005 (501 vs. 432 mg/day)7 because there is a prominent dose-response relationship
with disopyramide, with more effective gradient reduction at higher dose14. Pyridostigmine
controlled-release (Mestinon timespan) administered with disopyramide attenuates side effects
such as dry mouth and constipation and we offer it, as needed, to all patients15. Half of our patients
received pyridostigmine timespan at least temporarily . The safety of the combination in
obstructive HCM is shown in the present study.
Though disopyramide is a mainstay of pharmacologic therapy at UK and Canadian programs
with national scope6,11 it has seen less use in the US. For example, it had been prescribed in 11% of
patients before surgical myectomy in one study8 and in 11% of patients before ablation in
another26. The current experience is unique in the US as 74% of patients received disopyramide, at
higher dose than previously, and pyridostigmine sustained release was used to control vagolytic
side effects.
Surgical septal myectomy: A third of our patients failed their trial of disopyramide/beta-
blockade, or had adverse side effects, and required septal reduction. Surgical septal myectomy is
the “gold standard” treatment for such patients and has been performed for 40 years3,16. In recent
years because of improved understanding about the cause of mitral-septal contact, appreciation of
the role of the mitral valve and the papillary muscles, and because of improved surgical technique,
excellent outcomes are now reported with in-hospital mortalities <1% and excellent long term
survival3,8,10,27,28. In the 80% of patients operated at SLR we applied a patient-tailored
individualized modification of the classic Morrow myectomy that we have termed the Resect-
py atatttttt UUUUUUUK K K K K K K aaaaaaandndndndndndnd CCCCCCCa
6 r
i b
e e
6,111111111 it has sss seseseseseenenenene lllllesesesesessssss usususususeeeee ininininin tttheheheee UUS.SS. FFororororor eeeeexaxaxaxaxammmmplplplplple,eeee it t t t hahahahahad dddd bebebebebeenenenenen ppppprmmm
icalalalalal mmmmmyeyeyeyeyectctcttomomomomomy yyyy ininini ooooonennenen stuuuuudydydydydy88888 aaaaandndndndnd iiin nnnn 1111111111%%% %% ofofofofof pppppatatatata ieeeeentntntntntsssss bebebebebefofofooorerereee aaaaab
eeentntnt eeexpxpxperererieieiencncnceee isisis uuunininiquququq eee ininin ttthehehe UUUSSS asasas 7774%4%4% ooofff papapap tititieeentntntsss rererecececeiviviveee
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

15
Plicate-Release operation. The surgical techniques of the RPR repair grew out of prior surgical
innovations27 and its results have been reported previously10. A unique aspect of this surgical
cohort is the application of horizontal anterior mitral leaflet plication in selected patients with long,
redundant slack mitral anterior leaflets. Within the advanced-care group a subgroup analysis of
survival between aggressive-pharmacologic and surgical patients would not be a valid comparison
because of selection bias: the pharmacologic group included more patients with advanced age and
severe comorbidities.
Alcohol septal ablation: The myectomy vs. alcohol ablation controversy cannot be resolved
by a prospective randomized trial3,22,26. ten Cate found late sudden death and appropriate ICD
discharge in 14% of ablation patients after 5.4 years, substantially higher than in their surgically-
treated patients29. From the prospective data in the current study, we can at least conclude that
excellent overall resuIts can be obtained by a strategy that reserves alcohol ablation for patients in
whom surgical myectomy is contraindicated, or when informed patients are reluctant to undergo
surgery.
DDD pacing with short AV delay, though not a primary therapeutic option for young patients
with obstructive HCM30 has a limited positive role in selected patients such as the elderly or those
already implanted with an ICD3. There is a synergistic beneficial effect for gradient reduction
when DDD pacing is used with disopyramide20.
Treatment of obstructive HCM has evolved over the 26 years encompassed in this study.
Comparing the first with the second half of the time period under consideration, the annual number
of surgical myectomies performed for resistant symptoms nearly tripled, the number of ICD
implants more than doubled, and DDD pacing for gradient reduction declined, to the benefit of our
most severely affected patients.
en death and apapapapapapappp
y hiighghghghghghgherererererere ttttttthahahahahahahan n n n n n n iiiininii
r
u i
c c
romomomomom the pppprororororospspspspspececececectititititiveveveveve dddddatatatata a aa aa ininiin ttttthehh cururrererererennnnnt t tt t stststststudududu y,y,y,y,y, we e ee cacacacacan nnnn atatatatat llllleaeaeaeaeastsss
uItItItItItsss ss cacacacac n nnnn bebebebebe ooooobtbbtbb aiaiaiaa neeeeedd ddd bybybybyby aaaaa ssssstrtrtrtrtratatataa egegegegegy yyyy thththththatatatatat rrrrreseseseseserererere veveveveves sss alalalalalcococococohohohohohol ll ababababablalaaaatitt
ccctototomymymy iiisss cococontntntrararaininindididicacacateteted,d,d,, ooorrr whwhwhenenen iiinfnfnfororormememeddd papapap tititienenentststs aaarerere rrrelelelucucuc
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

16
Conclusion: Patients with obstruction and symptoms unresponsive to initial pharmacologic therapy
with beta-blockade or verapamil may realize meaningful symptom relief and low mortality through
stepped management by adding disopyramide in appropriately chosen patients, and when needed, by
surgical septal myectomy.
DisclosuresNone.
References
1. Maron MS, Olivotto I, Zenovich AG, Link MS, Pandian NG, Kuvin JT, Nistri S, Cecchi F, Udelson JE, Maron BJ. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation. 2006;114:2232-2239.
2. Maron MS, Olivotto I, Betocchi S, Casey SA, Lesser JR, Losi MA, Cecchi F, Maron BJ. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med. 2003;348:295-303.
3. Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE, Towbin JA, Udelson JE, Yancy CW. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: Circulation. 2011;124:2761-2796.
4. Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, Shah PM, Spencer WH, 3rd, Spirito P, Ten Cate FJ, Wigle ED. ACC/ESC clinical expert consensus document on hypertrophic cardiomyopathy. J Am Coll Cardiol. 2003;42:1687-1713.
5. Wigle ED, Rakowski H, Kimball BP, Williams WG. Hypertrophic cardiomyopathy. Clinical spectrum and treatment. Circulation. 1995;92:1680-1692.
6. Elliott PM, Gimeno JR, Thaman R, Shah J, Ward D, Dickie S, Tome Esteban MT, McKenna WJ. Historical trends in reported survival rates in patients with hypertrophic cardiomyopathy. Heart. 2006;92:785-791.
7. Sherrid MV, Barac I, McKenna WJ, Elliott PM, Dickie S, Chojnowska L, Casey S, Maron BJ. Multicenter study of the efficacy and safety of disopyramide in obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2005;45:1251-1258.
8. Ommen SR, Maron BJ, Olivotto I, Maron MS, Cecchi F, Betocchi S, Gersh BJ, Ackerman MJ, McCully RB, Dearani JA, Schaff HV, Danielson GK, Tajik AJ, Nishimura RA. Long-term effects of surgical septal myectomy on survival in patients with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2005;46:470-476.
9. Sorajja P, Ommen SR, Holmes DR, Jr., Dearani JA, Rihal CS, Gersh BJ, Lennon RJ, Nishimura RA. Survival after alcohol septal ablation for obstructive hypertrophic cardiomyopathy. Circulation. 2012;126:2374-2380.
NGNGNGNGNGNGNG,,, , , , , KuKuKuKuKuKuKuvivivivivivivin n n n n n n JTJTJTJTJTJTJT, , , NNNNNNNis prrrrrrredededededededomomomomomomominininininininananananananantlt
l fl bs i Ci l ion. 2006;114:2232-223O cta
M un a
guideline for the diagnosis and treatment of hypertrophic ca
larrrrr oooooutututututflflflflflowowowowow tttttract obstruction. CiCiCiCiircrrcr ulation. 20000006;6666 114:2232-223OOOOOliiiiivotto III, BBBBBetetetetetocococococchchchchchi iiii S,S,S,S,S, CCCCCasasaseyeyeee SAAA, LeLeLeLeLessssssssssererererer JJJJR,R,RR,R LLLLLosososososi iiii MAMAMAMAMA, CeCeCeCeCecccccct vvvvveeenee tricularaar outuutflowowowww traaaaactctt obsbstrucuuctiiiiiononononon ooon ccclinnnicaalaaa outttcocococc mme innn athyhyhyhyhy. N NNNN EnEnEnEEnglgllgll JJJJJ MMMMMeddddd. 2020202020033333;3;3;3;334848484848:2:2:2:29595959595 3-33330303030303. aron BJ, Bonow RRRRO,O,O,O,O, DDDDDeaeaeaeaeararararr nin JJAAAAA,, ,, FiFFFF fefer rrr MAMAMAMAMA,,,,, Link MS, Naidu
n nn SRSRSR, RaRaRaakokokokowswswswskikikiki HHHH, , , SeSeSeSeS ididididmamamaman n n n CECECECE, ,,, ToToToT wbwbwbwwbinininnn JJJJJA,A,A,A,, UUUUdedededelslslslssonononon JJJEEE, YYYaaagguiuidedelilinene fforor tthehe ddiaiagngnososisis aandnd ttrereatatmementnt ooff hyhypepertrtrorophphicic ccaa
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

17
10. Balaram SK, Tyrie L, Sherrid MV, Afthinos J, Hillel Z, Winson G, Swistel DG. Resection-plication-release for hypertrophic cardiomyopathy: Clinical and echocardiographic follow-up. Ann Thorac Surg. 2008;86:1539-1544.
11. Ball W, Ivanov J, Rakowski H, Wigle ED, Linghorne M, Ralph-Edwards A, Williams WG, Schwartz L, Guttman A, Woo A. Long-term survival in patients with resting obstructive hypertrophic cardiomyopathy comparison of conservative versus invasive treatment. J Am Coll Cardiol. 2011;58:2313-2321.
12. Alhaj E, Kim B, Cantales D, Uretsky S, Chaudhry FA, Sherrid MV. Symptomatic exercise-induced left ventricular outflow tract obstruction without left ventricular hypertrophy. J Am Soc Echocardiogr 2013;26:556-565.
13. Musat D, Joshi R, Obeleniene R, Bangalore S, Winson G, Castaneda V, Musat C, Chaudhry FA, Sherrid MV. Impact of acute response of obstructive hypertrophic cardiomyopathy to oral disopyramide and correlates of response. J Am Coll Cardiol. 2008;51:A61 Abstract.
14. Sherrid MV, Arabadjian M. A primer of disopyramide treatment of obstructive hypertrophic cardiomyopathy. Prog Cardiovasc Dis. 2012;54:483-492.
15. Teichman SL, Ferrick A, Kim SG, Matos JA, Waspe LE, Fisher JD. Disopyramide-pyridostigmine interaction: Selective reversal of anticholinergic symptoms with preservation of antiarrhythmic effect. J Am Coll Cardiol. 1987;10:633-641.
16. Maron BJ. Hypertrophic cardiomyopathy centers. Am J Cardiol. 2009;104:1158-1159. 17. Sorajja P, Ommen SR, Nishimura RA, Gersh BJ, Berger PB, Tajik AJ. Adverse
prognosis of patients with hypertrophic cardiomyopathy who have epicardial coronary artery disease. Circulation. 2003;108:2342-2348.
18. Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: Final data for 2005. Natl Vital Stat Rep. 2008;56:1-120.
19. Finkelstein DM, Muzikansky A, Schoenfeld DA. Comparing survival of a sample to that of a standard population. J Natl Cancer Inst. 2003;95:1434-1439.
20. Minami Y, Kajimoto K, Kawana M, Hagiwara N, Sherrid MV. Synergistic effect of dual chamber pacing and disopyramide in obstructive hypertrophic cardiomyopathy. Int J Cardiol. 2010;141:195-197.
21. McLeod CJ, Ommen SR, Ackerman MJ, Weivoda PL, Shen WK, Dearani JA, Schaff HV, Tajik AJ, Gersh BJ. Surgical septal myectomy decreases the risk for appropriate implantable cardioverter defibrillator discharge in obstructive hypertrophic cardiomyopathy. Eur Heart J. 2007;28:2583-2588.
22. Olivotto I, Ommen SR, Maron MS, Cecchi F, Maron BJ. Surgical myectomy versus alcohol septal ablation for obstructive hypertrophic cardiomyopathy. Will there ever be a randomized trial? J Am Coll Cardiol. 2007;50:831-834.
23. Sherrid MV, Pearle G, Gunsburg DZ. Mechanism of benefit of negative inotropes in obstructive hypertrophic cardiomyopathy. Circulation. 1998;97:41-47.
24. Kajimoto K, Imai T, Minami Y, Kasanuki H. Comparison of acute reduction in left ventricular outflow tract pressure gradient in obstructive hypertrophic cardiomyopathy by disopyramide versus pilsicainide versus cibenzoline. Am J Cardiol. 2010;106:1307-1312.
25. Epstein SE, Rosing DR. Verapamil: Its potential for causing serious complications in patients with hypertrophic cardiomyopathy. Circulation. 1981;64:437-441.
26. Nagueh SF, Groves BM, Schwartz L, Smith KM, Wang A, Bach RG, Nielsen C, Leya F, Buergler JM, Rowe SK, Woo A, Maldonado YM, Spencer WH, 3rd. Alcohol septal
Fisher JD. Disisisisisisisooininininininnererererererergigigigigigigicc c ccc c sysysysysysysympmpmpmpmpmpmptototototototommmmmmm1987878787777;1;1;1;1;1;1;10:0:0:0:0:0::636363636363633-3-3-3-3-3-3-66664666
Hypertrophic cardiomyopathy centers. Am J Cardiol. 2009;10mmen SR, Nishimura R Gersh BJ, Berger PB, Ta k AJ. Af re
a6DM Muzikansky A Schoenfeld DA Comparing survival of
Hypepepepepertrtrtrtrtrororororophpppp icicicicic cardiomyopathy cececeecentnnnn ers. Am J CaCCCC rdiol. 2009;10mmmmmmmmmmen SR,R,R,RR NNNNNisisisisishihihihihimumumumumurarararara RRRRRA,AAAA GGGGGere shssh BBBBBJ,J,J,JJ BBBBBererererergegegeg r r r rr PBPPBPBP ,, ,, TaTaTaTaTajijijjijik k k kk AJAJAJAJAJ. Af pppppaataaa ients wwwitth hhypppeeere troppppphihiic cacardddiiomymymymymyopopopo aathhhy wwhohohohoho havavvavve eepiccaaare. CiCiCiCiCircrcrcrcr ulululululatatatttioioiooon.nnnn 222220000003;3;3;3;3 10101010108:8:8:8::23232323234242424242-2-2-2223434343434888.88 oyert DL, Xu J, MuMuMuMuMurprprprprphyhyhyhyhy SSSSSL.LLL DDDDeaeaeaaaththththths:ss:s FFFFFinininnalalalalal dddddata for 2005. Na666:1:1:1-1-1-1202020. DMDM MuMuziziziiikakakakk nsnskykykykk AAAA SSSSchchchhhoeoenfnfnfffelelelllddddd DADADADAD CoCoCoCC mpmpararinininii gg susurvrvivivivalalal oofff
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

18
ablation for the treatment of hypertrophic obstructive cardiomyopathy. A multicenter North American registry. J Am Coll Cardiol. 2011;58:2322-2328.
27. Sherrid MV, Chaudhry FA, Swistel DG. Obstructive hypertrophic cardiomyopathy: Echocardiography, pathophysiology, and the continuing evolution of surgery for obstruction. Ann Thorac Surg. 2003;75:620-632.
28. Iacovoni A, Spirito P, Simon C, Iascone M, Di Dedda G, De Filippo P, Pentiricci S, Boni L, Senni M, Gavazzi A, Ferrazzi P. A contemporary European experience with surgical septal myectomy in hypertrophic cardiomyopathy. Eur Heart Journ. 2012;33:2080-2087.
29. ten Cate FJ, Soliman OI, Michels M, Theuns DA, de Jong PL, Geleijnse ML, Serruys PW. Long-term outcome of alcohol septal ablation in patients with obstructive hypertrophic cardiomyopathy: A word of caution. Circ Heart Fail. 2010;3:362-369
30. Maron BJ, Nishimura RA, McKenna WJ, Rakowski H, Josephson ME, Kieval RS, assessment of permanent dual-chamber pacing as a treatment for drug-refractory symptomatic patients with obstructive hypertrophic cardiomyopathy a randomized, double-blind, crossover study (M-PATHY). Circulation. 1999;99:2927-33.
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

19
Table 1. Baseline characteristics of 723 patients with HCM
Variable All HCM n=723 Group1, Obstructed Beta Blocker or Verapamil n=210
Group 2, Obstructed advanced care n=299
Group 3, Non-obstructed n=214
p value
Age 53.8 ±17 54.1 ±18 56.7 ±15 48.4 ±17 <0.001
Gender (%m) 57 65 51 59 0.003 Rest LVOT Gradient mmHg 33 ±42 26 ±31 61 ±45 1 ±4 <0.001 %Obstructed at rest 41 38 71 0 <0.001 Provoked gradient mmHg 74 ±64 89 ±41 115 ±49 2.5 ±10 <0.001 %Obstructed at rest or after provocation 68 100 100 0 <0.001
NYHA class 2.3 ±0.8 2.1 ±0.9 2.7 ±0.7 1.7 ±0.8 <0.001
MLHF QOL 27 ±24 22 ±23 37 ±23 19 ±21 <0.001
MWT (mm) 22 ±6 20.8 ±6 22.7 ±6 22.4 ±7 0.02
Syncope (%) 26 21 28 28 0.16 FH SCD first degree relative (%) 16 21 14 22 0.10
NSVT (%) 26 21 31 26 0.28
BB (%) 66 64 76 55 <0.001
CCB (%) 22 26 21 18 0.14
FH of HCM (%) 39 36 35 48 0.005
AF (%) 19 12 24 19 0.002
CAD (%) 10 8 15 5 <0.001
EF (%) 64.6 ±13 63.5 ±16 66.5 ±9 63.3 ±13 0.33
BB=beta blocker; EF=ejection fraction; FH=family history; MWT= Maximal LV wall thickness; NSVT= non-sustained ventricular tachycardia
0
±0.8 2.1 ±0.9 2.7 ±0.7 1.7 ±0.8
±24 22 ±23 37 ±23 19 ±21
±
21 28 28
±0.0.000.8 888 8 2.1 ±0.9 2.77. ±0.7 1.7 ±0.8
±222224 4 4 44 22222 ±2323232323 3777 ±2222233333 1919191919 ±211111
±6 20.888 ±±±±±6666 2222222.7.7.777 ±±±±±6 6666 22.4 ±7
222221111 2828282828 2222288888
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

20
Table 2. Gradient reduction after treatment in 299 patients with advanced-care for obstructive HCM
Treatment Initial resting gradient mmHg
Gradient at follow-upmmHg
Interim gradient after disopyramide but before septal reduction n=80 p value
All obstructed pts receiving advanced care, n=299 61 ±44 10 ±23 <0.0001
Disopyramide, all pts n=221 63 ±45 25 ±32* <0.0001
Disopyramide without septal reduction n= 141† 59 ±46 18 ±31 <0.0001
Septal reduction after disopyramide=80§ 69 ±41 7 ±17** 40 ±27‡
‡< 0.0001 **<0.0001
All surgical pts n=138 65 ±42 3 ±9# <0.0001
*Gradient reported here includes that measured before intervention in 80 patients who had subsequent septal reduction. †43 (30%) patients had DDD pacing for gradient as well20.§surgery in 75 and septal reduction in 5. **final gradient after septal reduction in 80 patients who first received disopyramide. ‡interim gradient after disopyramide but before septal reduction, lower compared with their initial gradients, but higher than the final gradients in the 141 patients who could be managed without septal reduction, both p< 0.0001. #less than final gradient in 221 patients treated with disopyramide (p<0.0001), and less than final gradient in 141 patients treated with disopyramide but without septal reduction (p<0.0001)
27‡
8
r h
aptal reduction in 5
88888 65 ±4±4±4±4±422 33333 ±9± ###
re ininininclclclclcludududududes tthhhahh t t measurred bbbbbefeffefefooore iiii tnterventntntntntiioiii n nn iiniii 8880 0000 paaatititititientst whohhhh hhhhh
add DDDDDDDDD pppppacacacining g g g foforrr grgrgrgg adadieientntnt aaasss wewewellll20.pptatall rereduductctioiioii nn iininii 555
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

21
Table 3. Improvement in symptoms in the obstructed, advanced-care group
Treatment NYHA Initial Evaluation
NYHA Last Visit p value
MLHF QOL Score Init Evaluation
MLHF QOL Last Visit p value
All patients n=299 2.7 ±0.7 1.8 ±.5 <0.0001 37 ±23 27 ±23 <0.0001
All surgical patients n=138 2.7 ±0.7 1.7 ±.5 <0.0001 39 ±23 27 ±22 <0.0001
All disopyramide-treated pts without septal reduction n=141
2.7 ±0.6 1.9 ±.5 <0.0001 40 ±23 27 ±23 <0.0001
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

22
Table 4. Characteristics of 63 patients with LVOT obstruction due to SAM,mitral-septal contact referred directly for surgery without a trial of disopyramide
* including 5 patients with syncope and 1 with cardiogenic shock. MVR=mitral valve replacement; RVOT=right ventricular outflow tract
Characteristics # of patients
Concomitant cardiac surgery (n=23)
Coronary bypass 9
MVR to relieve MR due to intrinsic abnormality more than SAM, i.e., calcified leaflet 7
Aortic valve replacement for moderate aortic valve disease 4
Aortic root replacement for aortic aneurysm 1
RVOT myectomy for RV outflow obstruction 1
ICD lead extraction 1
Unfavorable anatomy thought not likely to respond to any pharmacologic therapy; long anterior mitral leaflet and high resting gradient * 20
Contraindications (n=11)
Symptomatic prostatism 6
Amiodarone therapy for AF 5
Patient choice 7
Psychosocial 2
ttheheheheheheherararararararapypypypypypypy; ; ; ; ; ; ; lololololololongngngngngngng 22
)
s 6
f 5
7
)
sm m m mm 6
for AF 5
7
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

23
Table 5. Complications of therapy in 299 patients in the obstructed, advanced-care group
Class of therapy, number of patients treated
Complication Number of patients
Outcome
Surgical,n=138
Large ventricular septal defect and early post-op heart failure
1 Required reoperation for complete closure, NYHA I outcome
Post-operative stroke 1 Disability
Post-operative TIA 1 Complete resolution
Large Pericardial Effusion 4 (3%) Pericardial windows with complete resolution
Post-operative respiratory failure in patients with pulmonary disease
2 Prolonged ICU course
Heart block 7 (5%) Permanent pacer
Wound infection 2 Resolved with drainage and antibiotics
Disopyramide, n=221
Torsade de pointes in female, age 82 with 96 mmHg resting gradient who developed diarrhea-induced hypokalemia.
1 ICD discharge terminated arrhythmia which completely subsided after K+ repletion. Disopyramide resumed
Heart block (age 88) 1 Permanent pacemaker
Urinary hesitancy (age 53) Urinary retention (age 88)
11
Discontinued diso
Device Therapy ICD, n=59; DDD pacemaker n=24
Tamponade 2 Pericardial window with complete resolution
Inappropriate shockInappropriate ATP
12 (20%) 1
Specifically targeted responses
ICD infection 1 System extraction
PrPrPrPrPrPrProlololololololononononononongegegegegegegeddddddd
h
ws
Torsadddde eeee dedededede pppppoioioioiointntntntn eseseseses iiiin nnn fefefefefemamamamamalelelelele, agagagagageeeee 8282828282 1111 ICICICICICDDDDD disch
HeHeHeHeHeararararartttt blblblblblooocoo kkkkk 7 (5(5(55(5%))))) Permanen
WoWoWoWoWoununununu d dddd inininininfefefeffectctctcc ioioiooionn nnn 222 22 ReReRRR sososososolvlvlvlvededededed wantibiotics
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

24
Figure Legends
Figure 1. Treatment paths in 299 obstructed advanced-care patients. ASA=alcohol septal ablation; Ant.
Leaf=anterior leaflet of mitral valve; DDD paced=AV sequential paced with short AV delay; Diso =
diso; verap = verapamil; *43 (30%) of the 141 patients who were successfully treated with
disopyramide were DDD paced as well.
Figure 2. Kaplan Meier plot comparing survival in 3 groups of HCM patients. Survival in the
obstructed advanced-care patients did not differ from non-obstructed patients.
Figure 3. Kaplan Meier plot comparing observed survival in the obstructed advanced-care group
(n=299, solid line) versus the expected survival based on 2005 US survival matched for age, sex
and race (dashed line).
US survival maaaaaaatctcttttt
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

Homel, Sandhya K. Balaram and Daniel G. SwistelMark V. Sherrid, Aneesha Shetty, Glenda Winson, Bette Kim, Dan Musat, Carlos L. Alviar, Peter
First-Line Therapy with Beta-Blockade or VerapamilTreatment of Obstructive Hypertrophic Cardiomyopathy Symptoms and Gradient Resistant to
Print ISSN: 1941-3289. Online ISSN: 1941-3297 Copyright © 2013 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation: Heart Failure published online May 23, 2013;Circ Heart Fail.
http://circheartfailure.ahajournals.org/content/early/2013/05/23/CIRCHEARTFAILURE.112.000122World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circheartfailure.ahajournals.org/content/suppl/2013/05/23/CIRCHEARTFAILURE.112.000122.DC1Data Supplement (unedited) at:
http://circheartfailure.ahajournals.org//subscriptions/
is online at: Circulation: Heart Failure Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information about thisEditorial Office. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation: Heart Failure Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on February 9, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

Supplemental Material

Figure Legend
Echocardiographic resting LVOT gradients in 299 patients in the obstructed advanced-care
group at initial evaluation and at last measurement after treatment. In the patients who received a
disopyramide trial, but then required septal reduction, interim gradients obtained just before the
invasive intervention are shown as well.