shalom college formcollege.shalomchristianschools.com/wp-content/uploads/2014/01/...nihort/sonso...
TRANSCRIPT

SHALOM CHRISTIAN COLLEGESHALOM CHRISTIAN COLLEGEGRACELAND,NIHORT/SONSO ROAD,OFF IDI-ISHIN ESTATE,IBADAN, OYO STATE,NIGERIA.
Tel: 080832181970802324410208034447808
E-mail: [email protected]@shalomchristianschools.com
Website: www.shalomchristianschools.com
STUDENTSTUDENTAPPLICATION FORMAPPLICATION FORM
SURNAME FIRST NAME OTHER NAMES
NAME OF STUDENT
GRADE/CLASS AND YEAR OF APPLICATION
DATE OF BIRTH
GRADE/CLASS YEAR
DAY MONTH YEAR
PHOTOGRAPH OF STUDENT
Accession No.:
Family Code:
Notes:
Admission Secretary
Documentation to be enclosed:
<2x ID Photographs
<A certified copy of Parents’/Guardian’s ID Documents
<A certified copy of Child’s Birth Certificate
<Previous Reports, if applicable
<Registration Fee paid
<Staff (Shalom Christian Schools)
<Sibling(s) at Shalom Christian N/P School
<Sibling(s) at Shalom Christian College
<Foreign Student (copy of Entry Visa/Study Permit)
<Missionary Kid
FOR ADMIN PURPOSES ONLY:
MEDICAL BACKGROUND INFORMATION
_____________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
_________________________________Family Doctor Dr. Tel:
Family Dentist Dr. Tel:
Eye Test Date: Hearing Test Date:
Additional Information:
The College undertakes to contact the parent/s or guardian in the event of any emergency. However, in the event of an emergency, I/We give my/our consent to the College taking whatever steps may be deemed necessary for my/our child/ward:
Print Name: Print Name:
Signature: Signature:
Are all fees paid up at the previous school? Yes No
ACCOUNTS: PLEASE TICK APPLICABLE BOX) Post E-mail Both
EMAIL ADDRESS, FOR ACCOUNT PURPOSES:
POSTAL FOR ACCOUNTS: (IF DIFFERENT FROM POSTAL) ____________________________________
_____________________________________________________________________________________
REGISTRATION FEE – Payment of ? ________________, has been made. I understand that this Registration
Fee is non-refundable whether or not my application to have my child/ward accepted at Shalom Christian College (SCC) is successful.
ADMISSION FEE – On offer of admission, an admission fee will be paid, which guarantees a place for your child/ward in the College. All fees however, must be paid on or before the first day of the term.
Dated at ________________________________ this _________ day of ____________________, 20______
Signed: ____________________________________________________________(PARENT / GUARDIAN / OTHER) WHOSE LIABILITY IN TERMS HEREOF SHALL BE JOINED AND SEVERAL.
This application is accepted on behalf of the College _____________________________________________
Designation _______________________________ Signature/Date _____________________________
ACCOUNTS
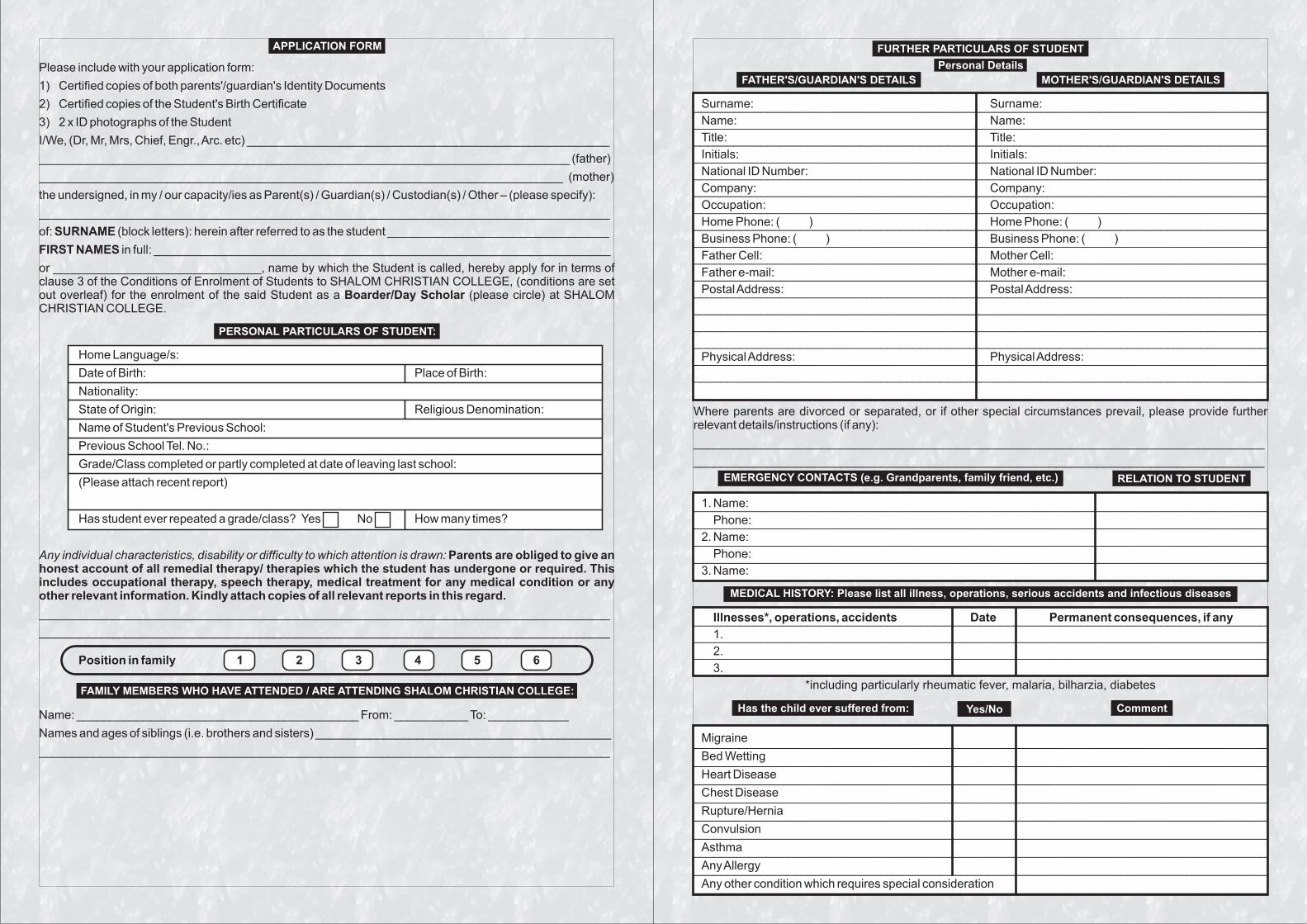
APPLICATION FORM
PERSONAL PARTICULARS OF STUDENT:
FAMILY MEMBERS WHO HAVE ATTENDED / ARE ATTENDING SHALOM CHRISTIAN COLLEGE:
_____________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
_________________________________
_____________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
_________________________________
_____________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
_________________________________
FURTHER PARTICULARS OF STUDENT
Personal Details
FATHER'S/GUARDIAN'S DETAILS MOTHER'S/GUARDIAN'S DETAILSPlease include with your application form:
1) Certified copies of both parents'/guardian's Identity Documents
2) Certified copies of the Student's Birth Certificate
3) 2 x ID photographs of the Student
I/We, (Dr, Mr, Mrs, Chief, Engr., Arc. etc) ______________________________________________________
_______________________________________________________________________________ (father)
______________________________________________________________________________ (mother)
the undersigned, in my / our capacity/ies as Parent(s) / Guardian(s) / Custodian(s) / Other – (please specify):
_____________________________________________________________________________________
of: SURNAME (block letters): herein after referred to as the student _________________________________
FIRST NAMES in full: ____________________________________________________________________
or _______________________________, name by which the Student is called, hereby apply for in terms of clause 3 of the Conditions of Enrolment of Students to SHALOM CHRISTIAN COLLEGE, (conditions are set out overleaf) for the enrolment of the said Student as a Boarder/Day Scholar (please circle) at SHALOM CHRISTIAN COLLEGE.
Home Language/s:
Date of Birth: Place of Birth:
Nationality:
State of Origin: Religious Denomination:
Name of Student's Previous School:
Previous School Tel. No.:
Grade/Class completed or partly completed at date of leaving last school:
(Please attach recent report)
Has student ever repeated a grade/class? Yes No How many times?
Any individual characteristics, disability or difficulty to which attention is drawn: Parents are obliged to give an honest account of all remedial therapy/ therapies which the student has undergone or required. This includes occupational therapy, speech therapy, medical treatment for any medical condition or any other relevant information. Kindly attach copies of all relevant reports in this regard.
_____________________________________________________________________________________
_____________________________________________________________________________________
Position in family 1 2 3 4 5 6
Name: __________________________________________ From: ___________ To: ____________
Names and ages of siblings (i.e. brothers and sisters) ____________________________________________
_____________________________________________________________________________________
Has the child ever suffered from: Yes/No Comment
MEDICAL HISTORY: Please list all illness, operations, serious accidents and infectious diseases
EMERGENCY CONTACTS (e.g. Grandparents, family friend, etc.) RELATION TO STUDENT
Surname:
Name: Name:
Title: Title:
Initials: Initials:
National ID Number: National ID Number:
Company: Company:
Occupation: Occupation:
Home Phone: ( ) Home Phone: ( )
Business Phone: ( ) Business Phone: ( )
Father Cell: Mother Cell:
Father e-mail: Mother e-mail:
Postal Address: Postal Address:
Physical Address: Physical Address:
Where parents are divorced or separated, or if other special circumstances prevail, please provide further relevant details/instructions (if any):
_____________________________________________________________________________________
_____________________________________________________________________________________
1. Name:
Phone:
2. Name:
Phone:
3. Name:
Illnesses*, operations, accidents Date Permanent consequences, if any
1.
2.
3.
*including particularly rheumatic fever, malaria, bilharzia, diabetes
Migraine
Bed Wetting
Heart Disease
Chest Disease
Rupture/Hernia
Convulsion
Asthma
Any Allergy
Any other condition which requires special consideration
Surname:_____________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
_________________________________