session 5. case diagnosis - sclerosing adenosis with lobular neoplasia. no invasion in images...
TRANSCRIPT

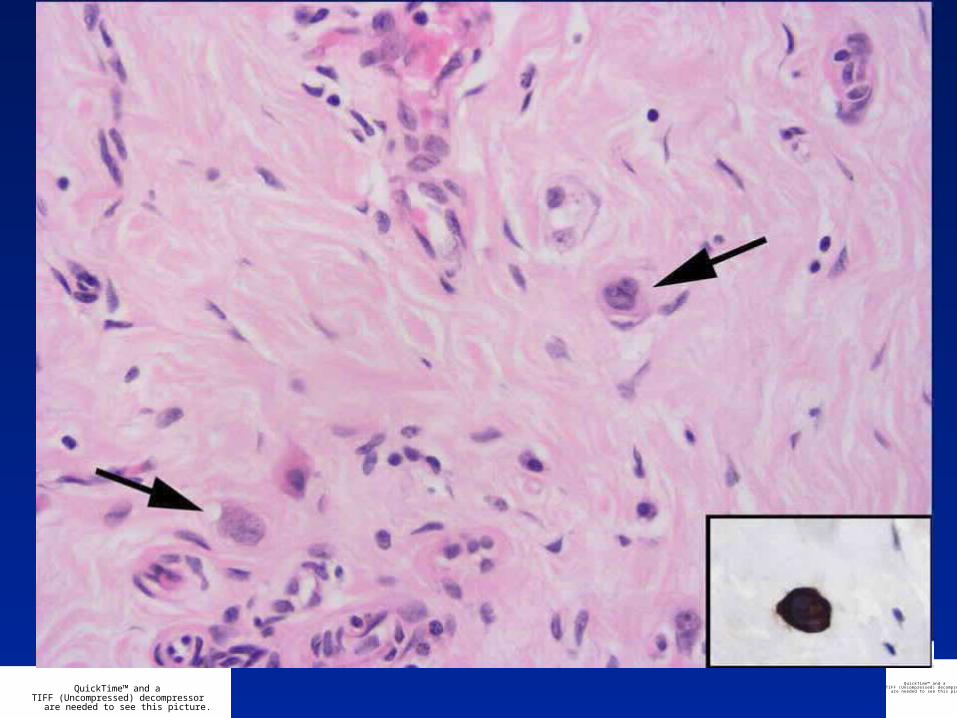
Session 5
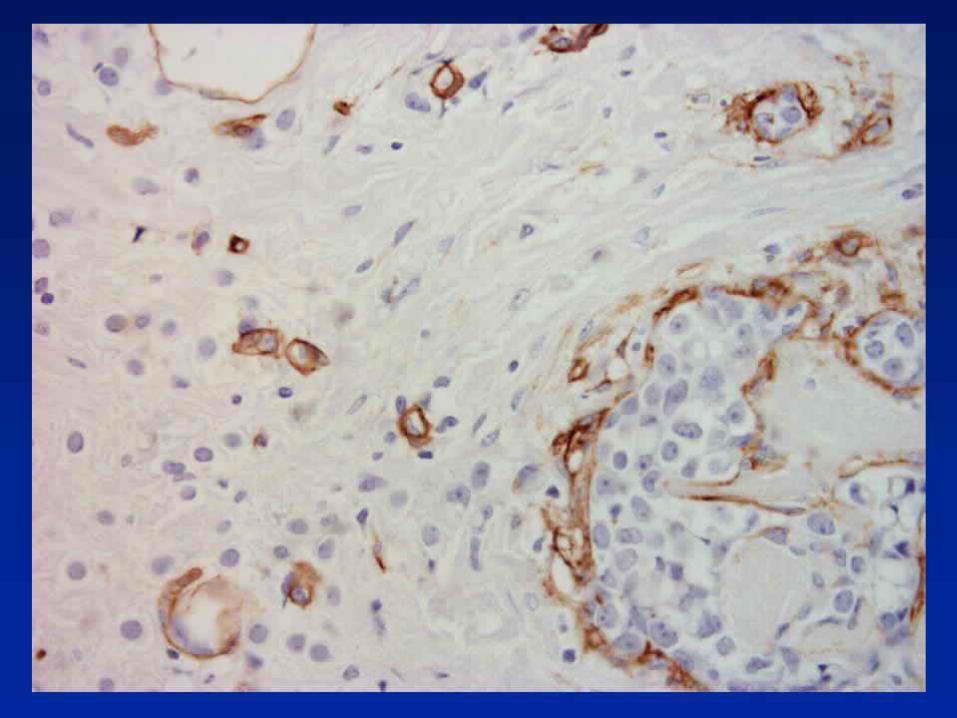
Case

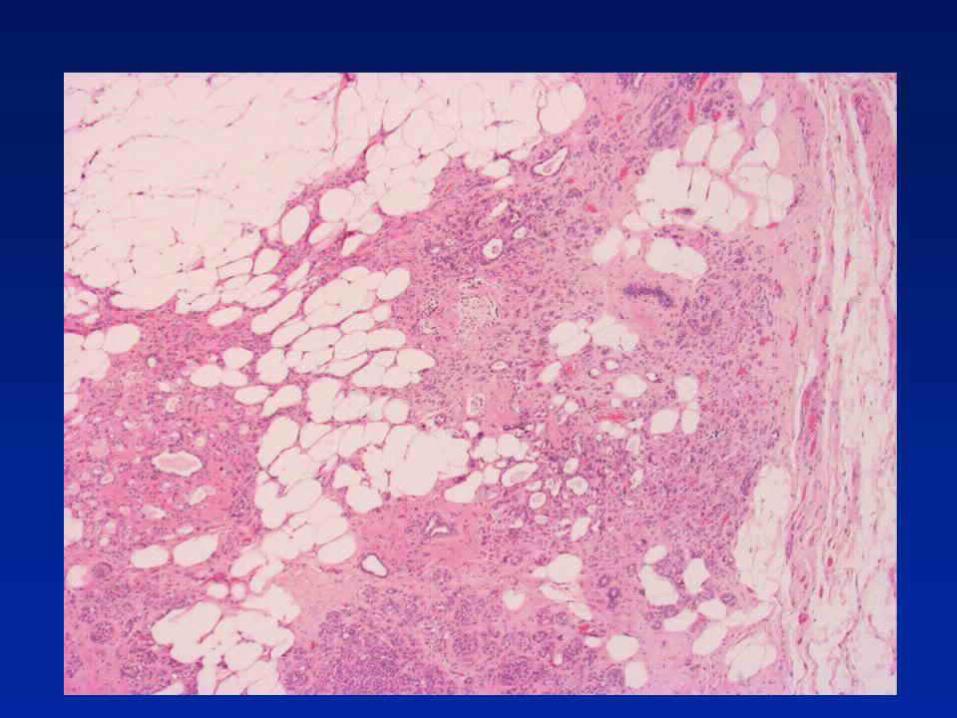










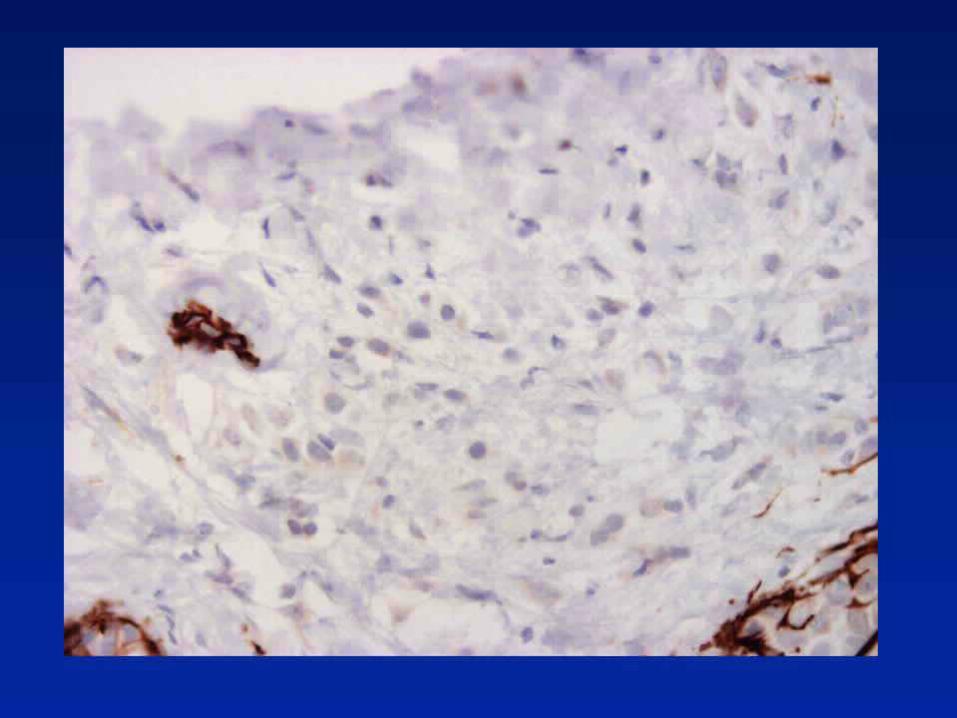
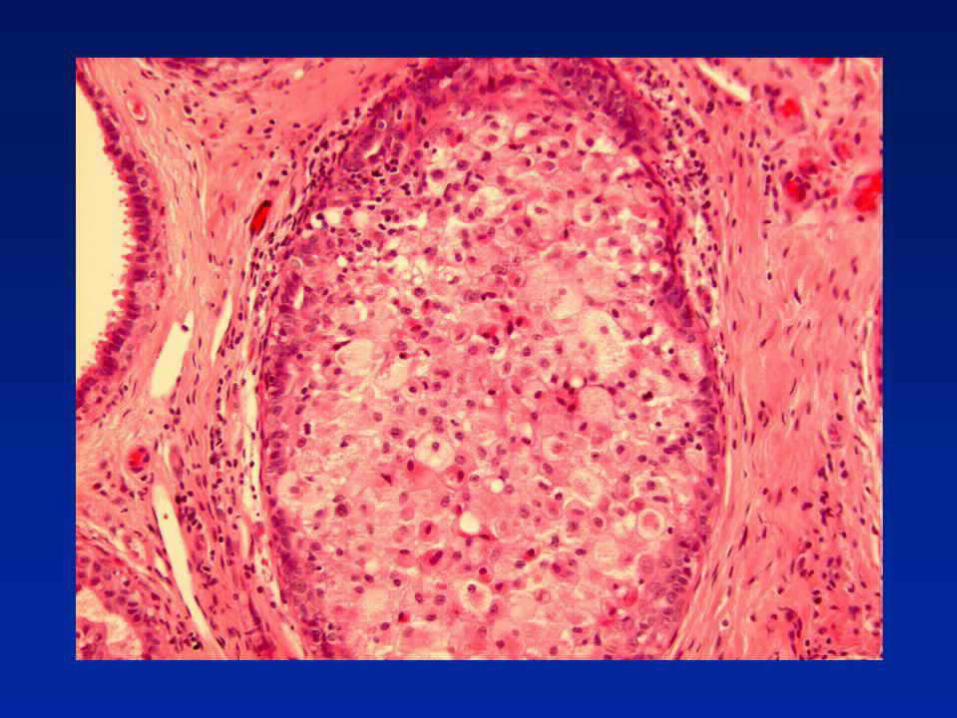
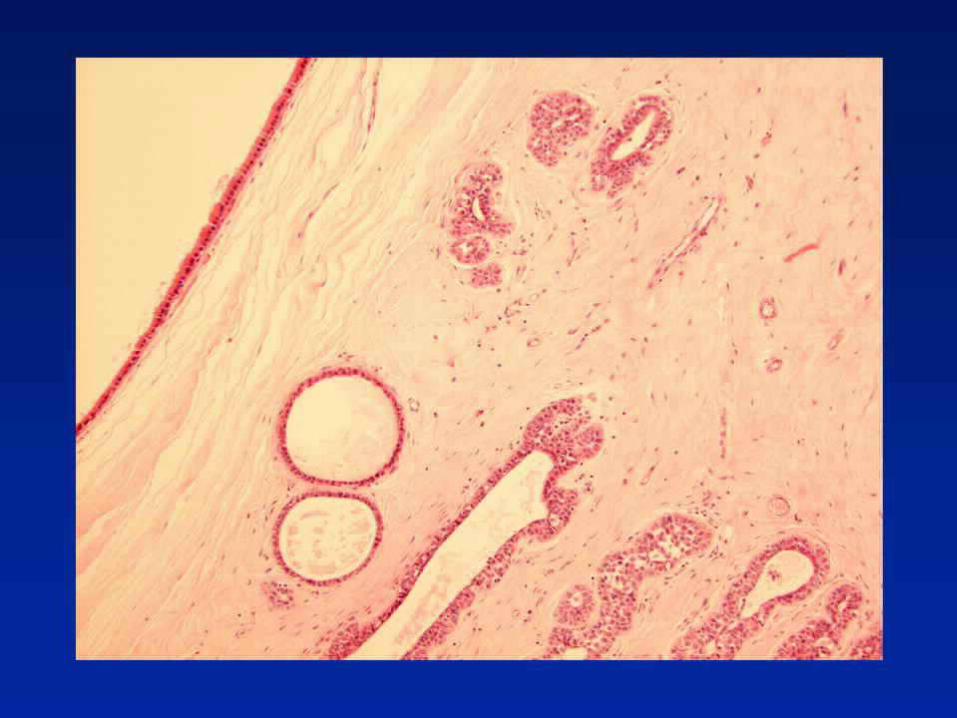
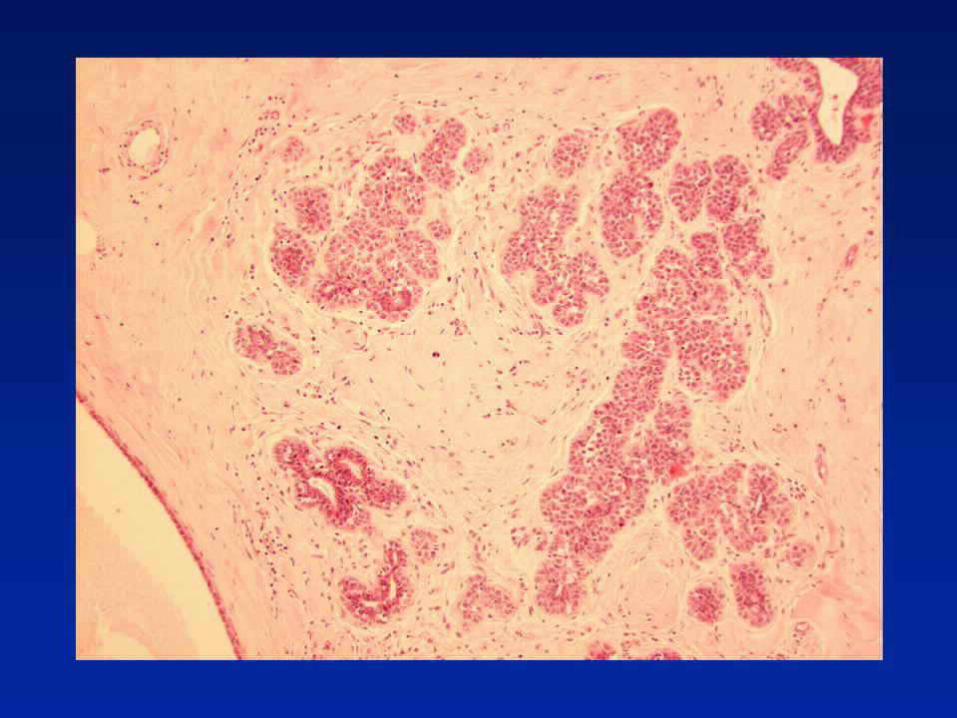
Diagnosis - Sclerosing adenosis with
lobular neoplasia.
No invasion in images provided.

Update - Risk with LISN
Meta-analysis 9 studies of 228 patients
15% ipsilateral, 9% contralateral carcinoma
Ipsilateral 3x more likely than contralateral
• A “model of premalignancy for ALH intermediate between a local precursor and a generalised risk for both breasts”
Page DL. Lancet. 2003;361:125-9

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Is there a sub-group of pre-invasive LCIS? LCIS with Microinvasion
6 LCIS with microinvasion described
Nemoto T et al. J Surg Oncol 1998; 67; 41-46

Case 19










Diagnosis - Fibrocystic change with
papillomas and florid usual epithelial hyperplasia

Case 32













Diagnosis - Fibrocystic change with
atypical lobular hyperplasia and flat high grade DCIS

Case 54






Diagnosis - Radial scar with florid usual
epithelial hyperplasia

• Central fibro-elastosis with entrapped tubular structures
• Usual epithelial hyperplasia
• Helpful features – retraction around tubular structures – often seen in radial scars
• Lack of fibroblastic stromal reaction (commonly, but not invariably seen (!) in tubular carcinoma)
• Confirm presence of myoepithelial cells and exclude diagnosis of tubular carcinoma (e.g. with smooth muscle myosin or smooth muscle actin or p63)
• In the epithelial proliferation look for (a) mixed population, (b) streaming and (c) slit-like peripheral spaces
Radial Scar







Case 44







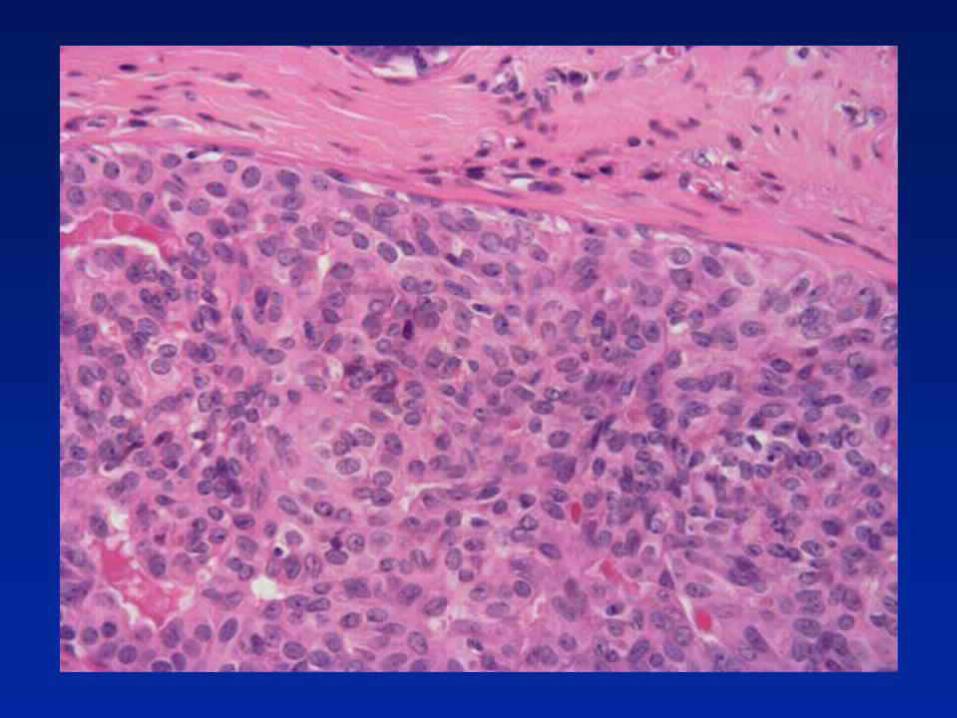
Diagnosis - High grade DCIS with comedo-
type necrosis and cancerisation of lobules.
No invasion or microinvasion.

MicroinvasionMicroinvasion• DCIS with a focus of invasion less than 1mm in
max. dimension• More than one focus, if each less than 1mm
Individual deposits may vary in size from a few islands to 1 mm diameter
• In the non-specialised, interlobular or inter-ductal connective tissue - neoplastic islands definitely within interlobular fibrous or adipose tissue
Excludes:Ultrastructural or immunocytochemical evidence of
breached or discontinuous basement membrane"Cancerisation of lobules"
Microinvasion
Observations
• Associated with high-grade comedo DCIS more than other types
• Increasing risk of axillary node involvement with increasing duct space involvement (>50 ducts)

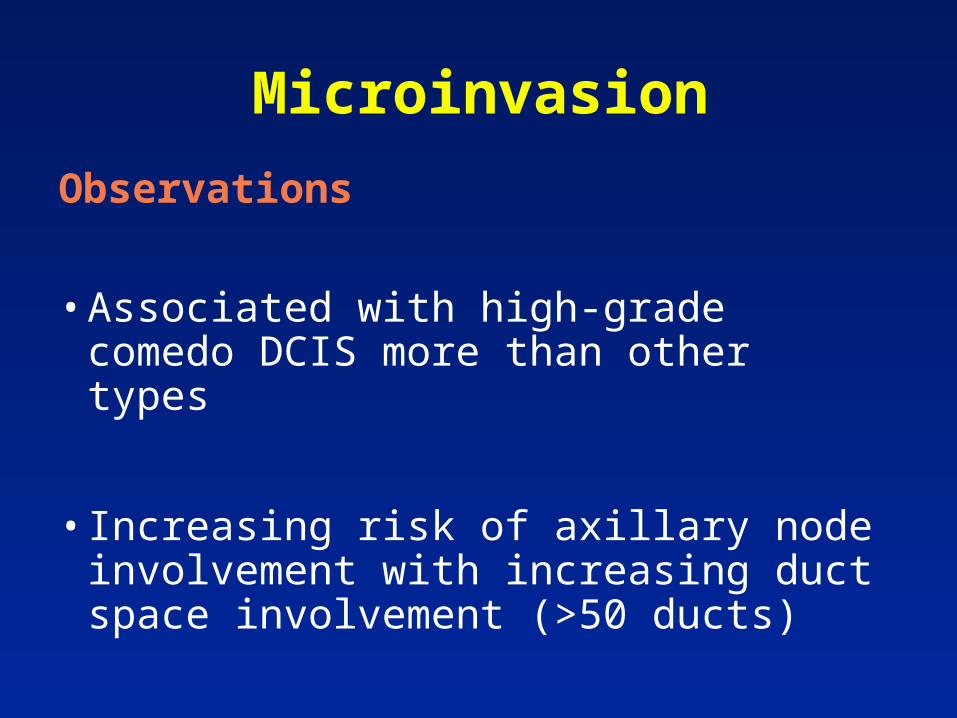
Microinvasion
Problems of interpretation
• Duct boundary poorly defined
• Periductal fibrosis
• Indistinct basement membrane zone
• Tangential cutting of involved duct/lobule

Microinvasion
Tips
• Outside organoid structures
• Involves non-specialised stroma
• Host lymphocytic response
• No myoepithelial component

Microinvasion
Key points
• Restrictive definition
• Rare
• Axillary node involvement low
• Prognosis very good

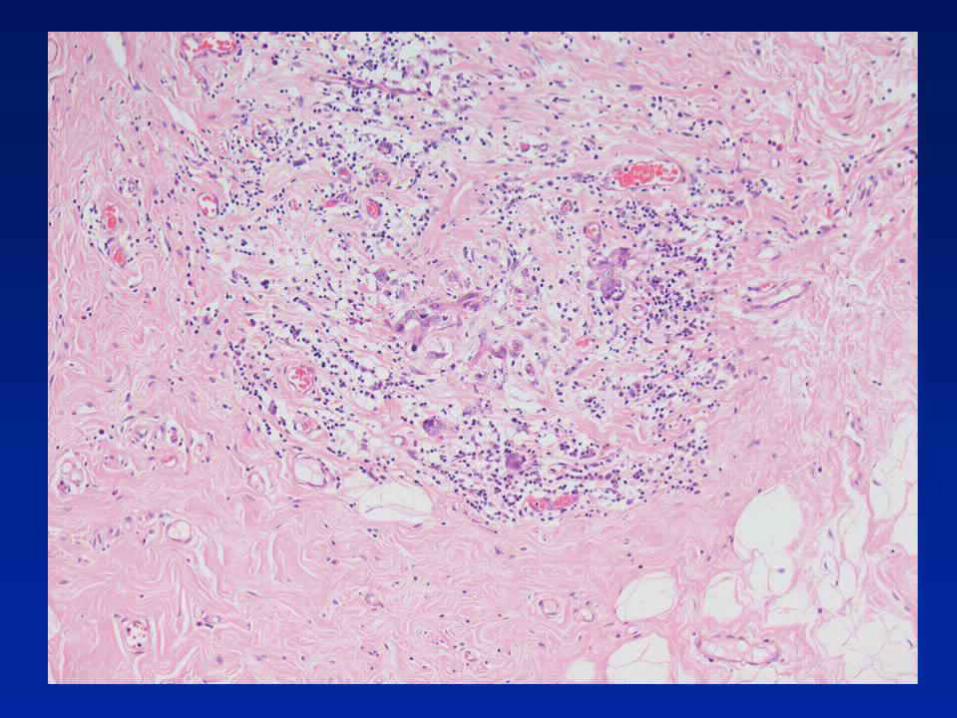



Case 11a








Diagnosis -Medullary-like carcinoma

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
CASE ?
• 36 year old patient
• Mastectomy and ALND post chemotherapy
• 5 months previously had core from 41mm mobile hypoechoic mobile mass in RUOQ

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Core Biopsy• B5, invasive carcinoma of provisional (core)
grade 3 (333) and no special type
• ER = 6/8
• PGR = 0/8
• HER2 = negative (score 0)
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
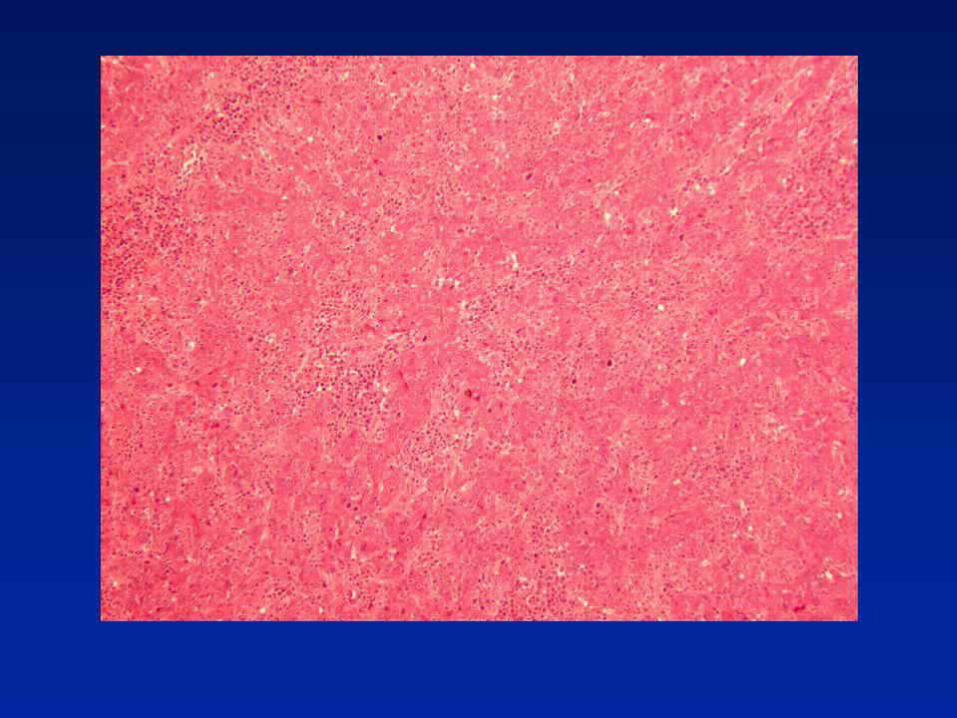
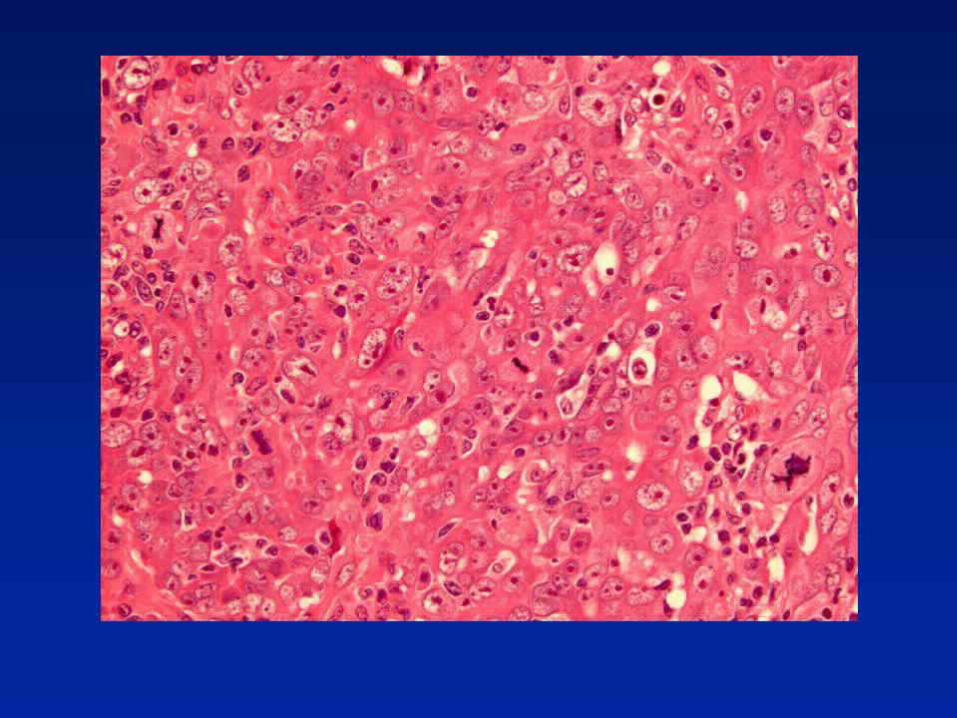
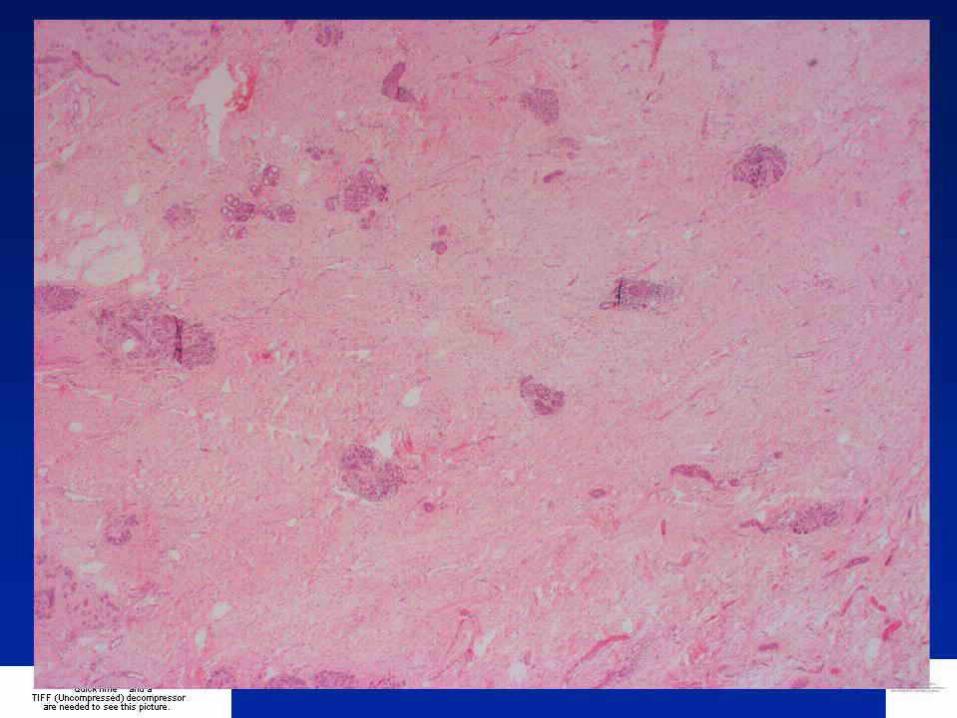
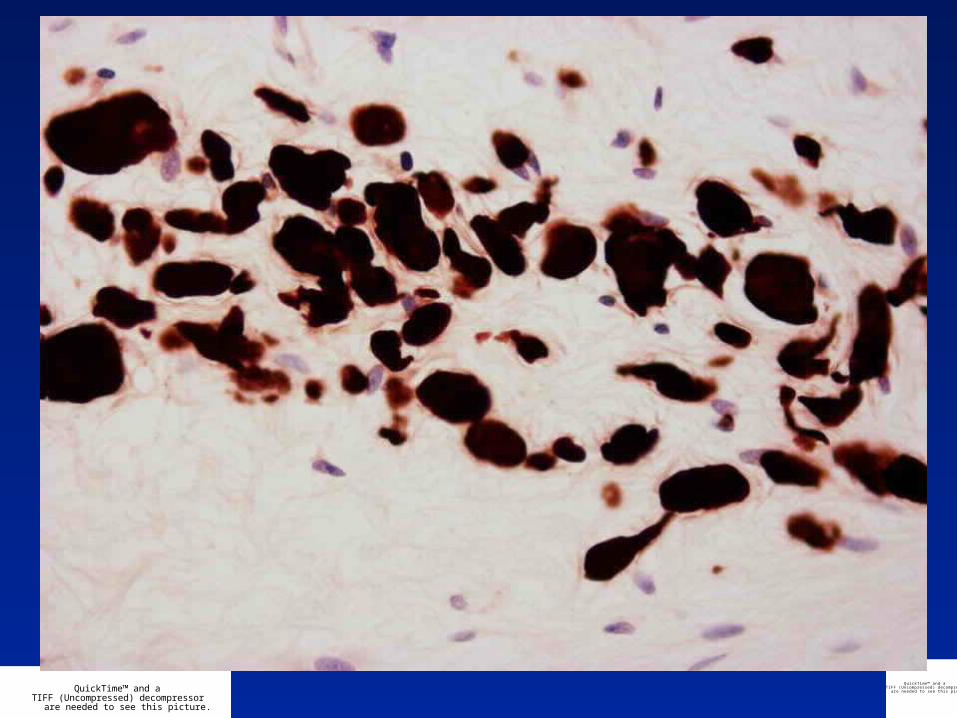
Diagnosis
Residual carcinoma cells mimicking histiocytes
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
• Central fibrotic scarring usually seen
• Patchy chronic inflammation within and around fibrosis
• Oedema or mucinous or myxoid changes to stroma or even areas of necrosis
• Cancer cells may mimic histiocytes, and vice versa, but collections of macrophages may also be present
• Cytokeratin IHC invaluable
Post-Chemotherapy Changes

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Grade 1 Some alteration to individual cells but no overall reduction in numbers compared to pre-treatment core
Grade 2 Mild loss of invasive cells, still high cellularityGrade 3 Considerable reduction, up to 90% lossGrade 4 Marked reduction - only small clusters of
widely dispersed cells detectedGrade 5 No invasive carcinoma, in situ carcinoma or
tumour stroma may still be noted
Bonadonna G et al. J Natl Cancer Inst. 1990 3;82:1539-45Smith IC et al. J Clin Oncol 2002;20:1456-66
Response to Chemotherapy

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Response to Chemotherapy
1. Disappearance of all tumour
2. Presence of in situ carcinoma but no residual invasive tumour & no metastatic carcinoma found in the lymph nodes
3. Invasive carcinoma present with stromal changes, such as sclerosis or fibrosis
4. Few modifications of appearance of tumour
Chevallier B et al. Am J Clin Oncol 1993;16:223–228