serological diagnosis of cytomegalovirus infection: comparison of 8 enzyme immunoassays for the...
TRANSCRIPT

ELSEVIER Clinical and Diagnostic Virology
2 (1994) 245-259
~ Clinical and Diagnostic Virology
Serological diagnosis of cytomegalovirus infection: comparison of 8 enzyme immunoassays for the detection of
HCMV-specific IgM antibody
Bernard Weber*, Franziska Prosser, Annette Munkwitz, Hans Wilhelm Doerr
lnstitut far Meal Virologie, Zentrum der Hygiene, Universitdtskliniken Frankfurt-am-Mainz, Paul Ehrlich Strasse 40, 60596 Frankfurt-am-Main, Germany
Received 19 September 1993; accepted 21 December 1993
Abstract
Background: Recently, numerous commercial ELISA kits for the detection of HCMV- specific IgM antibodies have been developed and are available on the international market.
Objective: The aim of the present study was to compare eight different ELISAs for the early serological diagnosis of HCMV infection.
Study design: A panel of paired sera obtained from patients suffering from primary or secondary infection and potential cross-reactive serum samples positive for IgM antibodies against other herpesviruses, antinuclear antibody and rheumatoid factor were investigated with 5 indirect ELISAs (1-5) and 3 #-capture assays (ELISAs 6-8).
Results: The highest sensitivity for IgM detection was achieved by a #-capture assay (ELISA 8) and a traditional indirect ELISA (4). Their respective sensitivities were 78.0 and 76.0%. Overall, #-capture immunoassays (ELISAs 6-8) detected HCMV infection earlier than indi- rect ELISAs (1-5) and showed a higher sensitivity for antibody detection in dilution series of IgM positive serum samples. Whereas ELISAs 1, 2, 5 and 6 showed a specificity of 100%, the alternative assays were affected by a variable number of false positive results obtained by testing potential cross-reactive serum samples. Their specificities ranged from 72.0% (ELISA 8) to 96.0% (ELISA 3).
Concltrdon: The results of the present study show that recent #-capture and indirect ELISAs permit a relatively sensitive and reliable diagnosis of HCMV infection. Cross-reactive antigens and interference from antinuclear antibody may limit the specificity of commercial kits.
Key words: HCMV-specific IgM antibody; #-Capture ELISA; Indirect ELISA; Rheumatoid factor; Antinuclear antibody
* Corresponding author. Fax: (+069) 63016477.
0928-0197/94/$7.00 © 1994 Elsevier Science B.V. All fights reserved SSDI 0928-0197(93)00000-0

246 B. Weber et al./Clinical and Diagnostic Virology 2 (1994) 245-259
1. Introduction
Human cytomegalovirus (HCMV) is the most frequent cause of congenital infec- tions. HCMV also plays a major role as opportunistic pathogen in AIDS patients and organ transplant recipients. In the last 10 years considerable efforts have been made to improve the laboratory diagnosis of HCMV infection. With the shell vial culture, rapid virus isolation can be accomplished by the detection of early antigen in infected fibroblasts 24-36 h post-inoculation. More recently, quantitation of p65 antigenemia in peripheral blood leucocytes (PBL) of HCMV individuals has been shown to be an easy and rapid test for the early diagnosis of HCMV infection and correlates well with viraemia (van der Bij et al., 1988; Bein et al., 1991). Recent studies using PCR to detect HCMV DNA in clinical samples showed promising results (Boland et al., 1992; Buffone et al., 1990; Einsele et al., 1991; Fenner et al., 1991; Olive et al., 1989; Zipeto et al., 1992). Nevertheless, as a consequence of its extreme sensitivity, the predictive value of PCR for the diagnosis of HCMV disease remains controversial (Delgado et al., 1992; Weber et al., 1994). The detection of HCMV-specific antibodies is commonly achieved by enzyme immunoassays and indirect immunofluorescence. Numerous ELISA kits for the detection of HCMV IgM are available on the international market. In comparison to IFA, the ELISA technique offers the advantage of a rapid screening for HCMV infection in large collectives of samples by the use of automated pipetting robotors and so-called 'walk away systems' which automatically perform dilution, incubation and washing steps with a rapid turn around time and without any further manipulation after dispensing the sera to analyse.
Serological testing for HCMV-specific immunoglobulin classes has been markedly improved by the introduction of highly purified antigens and antibody capture techniques (Doerr et al., 1980; Schmitz el al., 1980). Unfortunately, immunocom- promised patients often fail to produce IgM antibodies to HCMV, even during symptomatic infections. Serological testing for HCMV-specific antibodies in AIDS patients detects only one-third of active infections (Weber et al., 1992a). Chiba et al. found that up to 44% of asymptomatic congenitally infected infants fail to show an IgM response (Chiba et al., 1979).
Despite its reduced sensitivity in comparison to isolation of infectious virus and direct detection of viral antigen or genome, serology will continue to play an important role for the diagnosis of HCMV infection. Differentiation of primary from secondary infection is only possible by the determination of specific IgG prior to organ transplantation. The screening of blood donors for the presence of HCMV IgG antibodies permits to identify those who may potentially transmit the virus to immunocompromised individuals who are at a particularly high risk. In asympto- matic patients, HCMV infection may be diagnosed only by serologic testing when PBL samples are not examined in sufficiently narrow time intervals to detect DNAemia and/or antigenemia (Weber et al., 1994). Serologic assays may yield a higher sensitivity for the detection of primary infection in seronegative transplant recipients than conventional virus isolation (McMahon et al., 1989). The detection

B. Weber et al./Clinical and Diagnostic Virology 2 (1994) 245-259 247
of specific IgM in the presence of a productive infection is the best way to signify active infection in immunocompetent individuals and can provide earlier diagnosis as virus isolation alone.
In the present study, different commercially available ELISAs for the detection of HCMV-specific IgM were evaluated for the rapid serological diagnosis of primary or secondary HCMV infection. To assess the specificity, potentially cross-reactive samples were investigated with each assay.
2. Material and methods
ELISA assays Eight different commercially available ELISAs for the detection of HCMV-specific
IgM antibodies were investigated. ELISAs 1-4 (Enzygnost-Cytomegalie, Behringwerke, Marburg, Germany; Enzygnost Anti-CMV-IgM, Behringwerke; CMV-IgM, Radim, Italy; CMV IgM ELISA, Gull, Salt Lake City, USA) are manually performed traditional indirect assays in which microtiter plate wells are coated with purified HCMV antigen. The automated ELISA 5 (IMx CMV IgM, Abbott, Delkenheim, Germany) is based on indirect microparticle enzyme immuno- assay (MEIA) technology. ELISAs 6-8 (CAPTIA CMV-M, Mercia, England; CMV- IgM-ELA, Medac, Hamburg, Germany; ETI-Cytok-M reverse, Sorin Biomedica, Saluggia, Italy) are manually performed/~-capture assays.
Serum samples were pretreated by rheumatoid factor absorbent prior to testing with ELISA 1, 2 and 5. All serologic tests were performed according to the manufac- turer's recommendations. The respective test specific quality controls were consid- ered. Sensitivity and specificity of the assays were determined by commonly used methods (Griner et al., 1981).
HCMV-DNA-polymerase chain reaction (PCR), shell vial culture and p65 antigen detection
HCMV DNA amplification and quantitative p65 antigen detection from peripheral blood leukocytes (PBL) and rapid virius isolation from urine were performed as described elsewhere (Bein et al., 1991; Schacherer et al., 1988; Weber et al., 1994). PCR, p65 antigen detection and virus isolation served as reference tests for the evaluation of the different ELISA kits. An ELISA result was considered as true positive when rapid virus isolation from urine and/or antigen detection and /or DNA amplification from PBLs were positive in one or more clinical samples obtained from a patient with or without clinical symptoms attributable to HCMV infection. A true negative ELISA result was considered when virus isolation, DNA and p65 antigen detection were negative in clinical specimens obtained from asymptomatic patients or patients suffering from diseases not attributable to HCMV infection.
Serum samples Each test was evaluated with a panel of 72 to 85 serum samples obtained from
patients hospitalized at the University Clinics of Frankfurt during the time interval

248 B. Weber et al./Clinical and Diagnostic Virology2 (1994)245-259
Table 1 Evaluation of 8 commercial kits for the detection of H C M V IgM in serum samples f rom patients with active H C M V infection
Patient, age in Clinical Date of years, transplant, manifestations sampling date o f transpl., attributable to serostatus H C M V infection recipient/donor
Results o f virus isol. (IPS), H C M V p65-antigen detection and IgG D N A amplification (PCR) titer
PCR p65-Ag. IPS
S. J, 54 elevated ALT 13.01.92 320 RTR(3 .12 .91) (13.01.92) 14.01.92 + 160 R - / D + 23.01.92 + 320
10.02.92 640 20.02.92 320 16.03.92 160 21.03.92 160
B. Y., 23 H C M V infection
during pregnancy
25.01.93 - 160 28.01.93 320 29.01.93 160 04.02.93 160 11.02.93 +1 - 160 18.02.93 320 09.03.93 320
W. H., 45 leukopenia, 22.02.93 + - 640 LTR (8.02.93) thrombocytopenia, 08.03.93 + + 640 R + / D + fever >39°C 22.03.93 + + 1280
(5.03.90-30.03.93) 29.03.93 + - 2560 elevated ALT 05.04.93 + - 1280 (23.03-26.03.93) 21.04.93 + - 1280
S. H., 37 leukopenia, 21.08.92 - - - 2560 RTR (20.07.92) thrombocytopenia, 24.08.92 + + 2560 R - / D + fever >39°C 26.08.92 - + 2560
elevated ALT 28.08.92 - + 2560 (21.08-7.09.93) 02.09.92 + + 1280
07.09.92 1280 14.12.92 1280
from May 1992 to April 1993. All investigated serum samples were screened for the presence of HCMV-specific IgG and IgM antibodies by ELISA 1. Serum samples were selected on the basis of the clinical data and results of laboratory investigations (virus isolation, pp65-antigen detection, PCR and serology).
A total of 50 subsequent serum samples obtained from 6 organ transplant recipi- ents, 1 pregnant woman and 1 leukemia patient suffering from active primary or recurrent HCMV infection were investigated (Table 1 ). In all these patients, HCMV infection was documented by virus isolation and/or p65 antigen detection and/or PCR. Furthermore 5 of the 8 patients presented clinical symptoms potentially

B. Weber et al./Clinical and Diagnostic Virology 2 (1994) 245-259 249
(Table I continued)
Results o f HCMV IgM-specific serologic tests
ELISA 1 ELISA 2 ELISA 3 ELISA 4 ELISA 5 ELISA 6 ELISA 7 ELISA 8
- -t- + + + + + +
+ + + + + + + + § + + + + + + + + + + + + + + + + + + + + + + + - + + + + + + +
_ _ + - + - _ _
§ + + + + + + + +_ + + + + + + + - + + + + + + +
___ + + + + + + + - + + + + + + +
- + + + + + + +
. . . . . + - +
. . . . . - . [ - _ _ - -
_ _ _ + - - _ _ +
_ _ + + + - - + +
- - + + + + ___ + +
. . . . . . . . 4 -
-- ___ - - + + + + +
PCR, HCMV-DNA.amplification from PBLs by 'nested'-PCR; p65-Ag, quantitative p65-antigen detection from PBLs; IPS, 24 h virus isolation from clinical samples (urine and BAL) by immune peroxydase staining o f infected fibroblasts; tHCMV-DNA amplification from amniotic fluid in the 35th week of pregnancy; RTR, renal transplant recipient; LTR, liver transplant recipient; R/D, recipient/donor HCMV IgG serostatus; §, unspecific result.
attributable to HCMV infection. Patient BY was suffering from HCMV infection during pregnancy demonstrated by amplification of HCMV DNA from the amniotic fluid and viruria of the newborn presenting signs of generalized infection.
To further assess the sensitivity of the different ELISAs, five dilution series of IgM-positive sera were investigated (Table 2).

250 R Weber et al./ClinicalandDiagnostic Virology2 (1994) 245-259
(Table l continued)
Patient, age in years, transplant, date of transpl., serostatus recipient/donor
Clinical Date of Results of rapid virus HCMV manifestations sampling isolation (IPS) and DNA IgG attributable to amplification (PCR) titer HCMV infection
IPS PCR
S. C., 12
P. M., 26 RTR (10.09.90) R-/D+
P. W., 61 RTR (4.11.91)
R-/D+
V. P., 30 RTR (10.12.91) R - / D +
ALL 21.20.91 +BAL 320 interstitial 09.03.92 320
pneumonifis, (21.10.91) 10.03.92 320
asymptomafic 31.12.91 +urine 320 22.02.92 1280 11.05.92 - 640 18.05.92 - 640 25.05.92 - 640 14.05.92 + urine - 640
thrombocytopenia, 10.12.91 +urine 2560 leucopenia 21.01.92 2560
(10.12.91) 28.01.92 2560 10.03.92 2560 17.03.92 2560 24.03.92 10240 10.04.92 10240
asymptomafic 15.01.92 +urine 320 22.01.92 1280 25.02.92 1280 02.03.92 2560 24.03.92 1280 31.03.92 1280 07.04.92 1280
For the determination of specificity, a panel of potentially cross-reactive sera was tested (Table 3). All the serum samples were obtained from patients suffering from diseases not attributable to HCMV infection. Virus isolation from dilferent clinical specimens of these individuals was negative. Twenty-two serum samples were drawn from patients undergoing active infections with herpes simplex virus (HSV), Epstein- Barr virus (EBV) and varicella zoster virus (VZV) (Table 3). A variable number of serum samples with antinuclear antibodies and/or rheumatoid factor were eval- uated in the different ELISA assays (Table 4).
All serum samples were stored at -20°C before testing. Serum samples were diluted in the respective test buffers according to the manufacturer's recommenda-

R Weber et al./Clinical and Diagnostic Virology 2 (1994) 245-259 251
(Table 1 continued)
Results of HCMV IgM-speciflc serologic tests
ELISA 1 ELISA 2 ELISA 3 ELISA 4 ELISA 5 ELISA 6 ELISA 7 ELISA 8
+ + + + + + + +
+ + + + + + + + - - + + + + + + +
+ + + + + + + + + + + + + + + +
+ +_ + + + + + + - - + + + + + + +
- - + + + + + + +
+_ + + + + + + +
- - + + + + + + +
+ + + + + + + +
+ + + + + + + +
+ + + + + + + + + + + + + + + +
+ + + + + + + + + + + + + + + +
D R . a f t . . . . .
_ _ + - _ _ + -
+ + + + + -k + + - - + + + + + + +
+ + + + + + + + - - + + + + + + +
+ + + + + + + +
Table 2 Titration of HCMV IgM-positive serum samples with 6 different ELISAs
Sample Titer number
ELISA 1 ELISA 2 ELISA 3 ELISA4 ELISA 5 ELISA 6 ELISA 7 ELISA 8
1 92/30795 80 80 80 <40 80 160 640 160 2 92/30822 160 320 320 80 320 320 640 1280 3 92/33538 80 1280 640 80 1280 1280 > 1280 > 1280 4 92/33549 80 320 320 40 320 320 > 1280 > 1280 5 92/33314 80 640 640 160 320 160 > 1280 640

Ta
ble
3
Co
mp
ari
son
o
f 8
dif
fere
nt
EL
ISA
s fo
r th
e d
ete
cti
on
o
f H
CM
V
IgM
in
po
ten
tia
lly
cro
ss-r
ea
cti
ve
a
nd
in
terf
eri
ng
se
rum
sa
mp
les
po
siti
ve
fo
r Ig
M
to
oth
er
he
rpe
svir
use
s, r
he
um
ato
id
fac
tor
an
d
an
ti n
uc
lea
r a
nti
bo
dy
Sa
mp
le
Cli
nic
al
Tit
er
nu
mb
er
ma
nif
est
ati
on
s
HSV
- E
BV
- V
ZV
- Ig
M
EA
- Ig
M
IgM
Re
sult
s o
f se
rolo
gic
al
test
s (O
.D.
va
lue
s)
EL
ISA
1
EL
ISA
2
EL
ISA
3
EL
ISA
4
EL
ISA
5
EL
ISA
6
EL
ISA
7
EL
ISA
8
21
36
2
1/4
0
..
..
n
.d.
- -
-
24
42
5
dis
sem
ina
ted
1
/80
.
..
..
..
.
zo
ste
r
26
02
1
1/1
60
.
..
.
n.d
. -
- -
26
07
7
1/1
60
.
..
.
n.d
. -
- -
28
19
1
AL
L
1/4
0
- -
- n
.d.
- -
-
30
11
7
1/4
0
..
..
..
..
30
80
5
1/4
0
..
..
..
.
+ (
0.4
03
)
20
09
4
HIV
se
rop
osi
tiv
e
1/1
60
.
..
..
..
.
20
70
4
1/3
20
-
- +
(0.4
67
) +
(1.1
35
) n
.d.
- -
-
20
72
6
1/1
60
.
..
..
..
.
20
84
1
intr
ac
ere
bra
l 1
/16
0
..
..
..
spa
ce
-oc
cu
py
ing
lesi
on
20
89
2
1/1
60
.
..
.
n.d
. -
- -
18
06
3
va
gin
al
zo
ste
r 1
/40
-
- -
+(0
.67
8)
- -
- +
(0.1
87
)
24
32
5
1/3
20
.
..
..
..
.
27
81
7
po
st z
ost
er
1/3
20
-
- +
(0.4
50
) +
(0.8
96
) .
..
.
rad
ieu
liti
s
zo
ste
r
28
35
7
zo
ste
r 1
/40
.
..
..
..
.
28
62
7
C6
zo
ste
r 1
/80
-
- -
+ (
0.8
01
) .
..
.
rad
icu
liti
s
20
02
7
AID
S
1/4
0
..
..
..
..
20
05
2
AL
L
1/4
0
..
..
n
.d.
- -
-
20
21
2
HIV
se
rop
osi
tiv
e
1/8
0
..
..
n
.d.
- -
+(0
.42
5)
g~
~o
Ka

(Tab
le 3
con
tinue
d)
3769
4 H
IV s
erop
osit
ive
3769
6 H
IV s
erop
osit
ive
1/80
.
..
..
..
1/80
-
- -
+(0.
605)
-
- +(
0.58
8)
+(o
.185
) +
(0.2
08)
Sam
ple
ANA
num
ber
RF
R
esul
ts o
f se
rolo
gica
l te
sts
(O.D
. va
lues
)
EL
ISA
1
EL
ISA
2
EL
ISA
3
EL
ISA
4
EL
ISA
5
EL
ISA
6
EL
ISA
7
EL
ISA
8
3188
2 1/
80
1/32
0 .
..
..
..
3522
5 1/
80
1/32
0 .
..
..
.
+(0.
545)
18
213
1/40
00
..
..
..
_+
(0.
274)
1814
5 I/
I000
-
- n.
d.
n.d.
-
- n.
d.
3506
1 1/
40
1/32
0 -
- n.
d.
n.d.
-
- n.
d.
3555
3 1/
80
- -
n.d.
n.
d.
- -
n.d.
2593
4 1/
80
- -
n.d.
n.
d.
- -
n.d.
35
381
1/40
1/
640
- -
n.d.
n.
d.
- -
n.d.
+(0
.172
)
+(0
.221
) n.
d.
hAL
n.
d,
n.d.
n.
d.
t~
AN
A,
anti
nucl
ear
anti
body
; R
F,
rheu
mat
oid
fact
or;
n.d.
, n
ot
dete
rmin
ed.
t,,o
",o
254 B. Weber et al./Clinical and Diagnostic Virology 2 (1994) 245-259
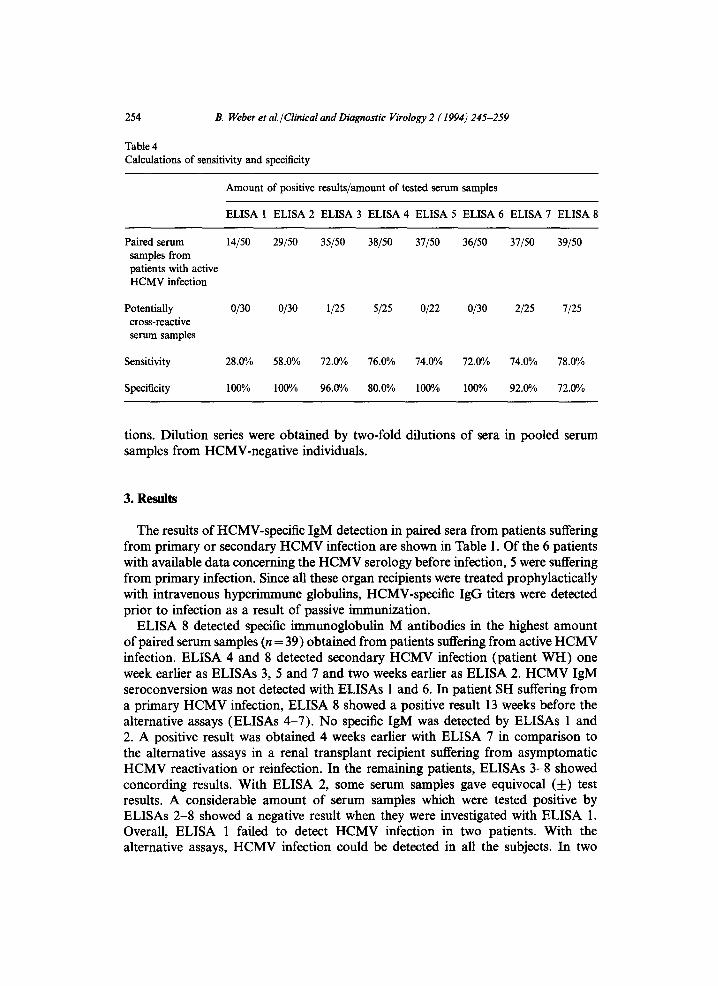
Table 4 Calculations of sensitivity and specificity
Amount of positive results/amount of tested serum samples
ELISA 1 ELISA 2 ELISA 3 ELISA 4 ELISA 5 ELISA 6 ELISA 7 ELISA 8
Paired serum samples from patients with active HCMV infection
Potentially cross-reactive serum samples
14/50 29/50 35/50 38/50 37/50 36/50 37/50 39/50
0/30 0/30 1/25 5/25 0/22 0/30 2/25 7/25
Sensitivity 28.00/0 58.0% 72.00/0 76.0% 74.0% 72.00/0 74.0o/0 78.0°/0
Specificity 100% 1000/o 96.00/0 80.0% 100% 100% 92.00/0 72.0%
tions. Dilution series were obtained by two-fold dilutions of sera in pooled serum samples from HCMV-negative individuals.
3. R ~
The results of HCMV-specific IgM detection in paired sera from patients suffering from primary or secondary HCMV infection are shown in Table 1. Of the 6 patients with available data concerning the HCMV serology before infection, 5 were suffering from primary infection. Since all these organ recipients were treated prophylactically with intravenous hyperimmune globulins, HCMV-specific IgG titers were detected prior to infection as a result of passive immunization.
ELISA 8 detected specific immunoglobulin M antibodies in the highest amount of paired serum samples (n = 39) obtained from patients suffering from active HCMV infection. ELISA 4 and 8 detected secondary HCMV infection (patient WH) one week earlier as ELISAs 3, 5 and 7 and two weeks earlier as ELISA 2. HCMV IgM seroconversion was not detected with ELISAs 1 and 6. In patient SH suffering from a primary HCMV infection, ELISA 8 showed a positive result 13 weeks before the alternative assays (ELISAs 4-7). No specific IgM was detected by ELISAs 1 and 2. A positive result was obtained 4 weeks earlier with ELISA 7 in comparison to the alternative assays in a renal transplant recipient suffering from asymptomatic HCMV reactivation or reinfection. In the remaining patients, ELISAs 3-8 showed concording results. With ELISA 2, some serum samples gave equivocal (_) test results. A considerable amount of serum samples which were tested positive by ELISAs 2-8 showed a negative result when they were investigated with ELISA 1. Overall, ELISA 1 failed to detect HCMV infection in two patients. With the alternative assays, HCMV infection could be detected in all the subjects. In two

R Weber et al./Clinical and Diagnostic Virology 2 (1994) 245-259 255
renal transplant recipients (WH and SH), from whom results of DNA amplification and p65 antigen detection from sequential PBL samples were available, there were considerable delays between the first positive DNAemia or antigenemia result and IgM detection.
Table 2 shows the results obtained by testing 5 dilution series of HCMV-IgM- positive serum samples with 5 different indirect ELISAs and 3 #-capture assays. The #-capture ELISAs showed a higher sensitivity for HCMV IgM detection than the conventional assays based on antigen-coated wells.
A high rate of false positive results were obtained with ELISA 4 (n=6) and ELISA 8 (n=7) when potentially cross-reactive sera obtained from individuals suffering from diseases not attributable to HCMV infection were investigated (Table 3). In contrast, ELISAs 1, 2, 5 and 6 were not influenced by the presence of IgM antibodies to other herpesviruses, rheumatoid factor or antinuclear antibodies. With ELISA 3, only false positive result was observed by testing a serum sample from a HIV-infected patient suffering from an active EBV infection.
Sensitivity and specificity ELISAs 3 and 8 detected specific IgM in the highest amount of serum samples
obtained from patients suffering from active HCMV infection; their respective sensi- tivities were 78.0 and 76.0% (Table 4). The lowest values for sensitivity were observed with ELISA 1 (28.0%) and ELISA 2 (58.0%). The other assays showed sensitivity values greater than 70%. A specificity of 100% was achieved with ELISAs 1, 2, 5 and 6. Since a high number of serum samples were tested false positive with ELISAs 8 and 4, the values for specificity were only 72.0% and 80.0% respectively.
4. Discussion
The results of the present study show that there are great differences in sensitivity for HCMV IgM detection between commercially available ELISAs. With the most sensitive tests, about 22-28% of paired serum samples obtained from patients suffer- ing from active HCMV infection were tested HCMV IgM-negative. ELISA 1, which uses alkaline phosphatase labelled anti-IgM as conjugate, failed to detect HCMV infection in two patients, only 28.0% of the serum samples drawn from patients with active HCMV infection were tested positive for HCMV-specilic IgM. The recently introduced ELISA 2, which is commercialised by the same manufacturer shows a markedly improved sensitivity in comparison to ELISA 1. These findings confirm previous observations showing that ELISA 1 yields a poor sensitivity for the detec- tion of HCMV-specific IgM (Steinmann and Bischoff, 1991; Weber et al., 1992a, 1992b, 1992c). Recent indirect and #-capture assays are more adequate for rapid diagnosis of HCMV infection in immunocompromised individuals. However, the results of serologic testing on paired serum samples from renal transplant recipients with active infection show that there may be a long delay between DNA or antigen detection and HCMV-specific IgM response. Adequate monitoring of HCMV infec- tion in high risk individuals can therefore only be performed by using a combination

256 B. Weber et al./Clinical and Diagnostic Virology 2 (1994) 245-259
of virus isolation from clinical samples (BAL, induced sputum, urine,...), p65 antigen detection and/or DNA amplification from PBL and serology.
A major problem is the definition of a 'golden standard' for the evaluation of the sensitivity and specificity of HCMV IgM assays. Virus may be isolated from urine during asymptomatic infection and on the oposite documented infection may not be accompanied by viruria or antigenemia (Weber et al., 1994). Due to the high sensitivity of the PCR, HCMV DNA can occasionally be amplified from PBL of asymptomatic HCMV-seropositive and even seronegative individuals (Weber et al., 1994; Taylor-Wiedemarm et al., 1993). In 6 of 8 patients, active HCMV infection was diagnosed since they presented clinical symptoms potentially attributable to HCMV infection and had a positive result in at least two different laboratory methods. In two asymptomatic patients with viruria, definitive evidence of active HCMV infection was obtained by the detection of specific IgM with 8 different ELISAs. The usefulness of the Western blot as a reference method for the detection of HCMV-specific IgM antibodies is limited by the fact that a recently established immunoblot showed reactivities with HCMV-specific proteins in serum samples drawn from asymptomatic seropositive individuals (Braun et al., 1993).
By the titration of serum dilutions, #-capture assays showed a higher sensitivity than the traditional indirect ELISAs. Although they cannot mimic early HCMV- specific IgM seroconversion specimens, dilution series represent an objective criterion for the assessment of sensitivity. For ELISA 8, the highest sensitivity as measured by serial dilutions correlated with the highest sensitivity measured by seroconversion performance.
Concerning the specificity of HCMV IgM antibody detection, considerable differ- ences were observed between the different immunoassays. ELISA 8 showed the highest amount of false positive results. That high sensitivity is not necessarily associated with a poor specificity is shown by ELISAs 3, 5, 6 and 7. While ELISAs 5 and 6 showed a specificity of 100%, the two other assays generated only 1 respectively 2 false positive results.
Previous studies on IgM-capture ELISA have shown that false-positive reactions may be seen in sera, which are Paul-Bunnell positive, or contain antinuclear antibod- ies (Nielsen et al., 1987). Reactivity in sera against cellular antigens in the HCMV conjugate may occur (Chou et al., 1987; Nielsen et al., 1987; Rasmussen et al., 1982). As shown by the results in Table 3, two/~-capture assays showed false positive reactions with antinuclear antibody and rheumatoid factor positive serum samples. Since IgM-capture ELISAs are not influenced by rheumatoid factor, antinuclear antibodies must be the cause of the false positive results.
Furthermore, indirect ELISAs may be influenced by factors such as competition by high levels of IgG and interference from rheumatoid factors (Doerr et al., 1987). Pretreatment of serum samples with anti-human IgG eliminates efficiently this source of false positive reactions (Table 3). However, the persistence of interfering reactivity may limit the specificity of assays (Joassin et al., 1986).
Cross-reactions with other herpesviruses occur frequently with commercially avail- able kits (Doerr and Albert, 1990). ELISAs 3, 4, 7 and 8 reacted with a variable amount of serum samples with IgM antibodies to HSV, EBV-early antigen

R Weber et al./Clinical and Diagnostic Virology 2 (1994) 245-259 257
(EBV-EA) and VZV. This problem is very likely due to cross-reacting antigens and host cell proteins in the viral envelope which is derived from the Golgl vesicles (Severi et al., 1988). Perhaps, the next generation of ELISA kits, using a combination of different well characterized and highly specific recombinant or synthetic antigens, will overcome these cross-reactivities. However, the overall sensitivity of IgM detec- tion using single peptides is still under 85% (Landini et al., 1989).
A serum sample obtained from a HIV-positive individual was tested positive in three of eight ELISAs. Since the patient presented no evidence for active HCMV infection (repeated negative results of virus isolation) and 2 of the 3 ELISAs generated a relatively high number of false positive results with potentially cross- reactive samples, the results obtained with ELISAs 4, 7 and 8 were considered as false positives.
Numerous attempts have been made to improve the serologic diagnosis of HCMV infection in immunocompromised patients by the determination of specific immuno- globulins other than IgG or IgM (Nielsen et al., 1988, Van Loon et al., 1985; Doerr et al., 1987, Weber et al., 1993a). The detection HCMV-specific IgA increases the efficiency of serologic diagnosis of active infection in organ transplant recipients and AIDS patients suffering from primary or secondary HCMV infection (Braun et al., 1993; Engelhard et al., 1991; Sarov et al., 1981; Weber et al., 1992a).
In conclusion, the results of the present study show that recent/z-capture and indirect ELISAs permit a relatively sensitive and reliable diagnosis of HCMV infec- tion. However, since in immunocompromised patients, the production of specific immune globulins may be delayed, rapid virus isolation, antigen detection or ampli- fication of viral genome sequences are more adequate for early diagnosis of HCMV infection in these individuals.
Acknowledgements
We thank U. Kauk, G. Schulz, G. Metz, V. Brehm, R. Middletown and M. Kolb for their excellent technical assistance.
References
Bcin, G., Bitsch, A., Hoyer, J. and Kirchner H (1991) The detection of human cytomegalovirus immediate early antigen in peripheral blood leucocytes. J. Immunol. Methods 137, 175-178.
Boland, G.J., Weger, R.A., Tflanus, M.G.J., Ververs, C., Bosboom-Kalsbeek, K. and De Gast, G.C. (1992) Detection of cytomegalovirus (CMV) in granulocytes by polymerase chain reaction compared with the antigen test. J. Clin. Microbiol. 30, 1763-1767.
Braun,W, Weber, B., Moell, U., Hamann, A. and Doerr, H.W. (1993) Comparison of specific immunoglobulin A and M patterns in human cytomegalovirus infection studied by a modified Western blot method. J. Virol. Methods 43, 65-76.
Buffone, (i.J., Hine, E. and Demmler, G.J, (1990) Detection of mRNA from the immediate early gene of human cytomegalovirus in infected cells by in vitro amplification. Molec. Cell Probes 4, 143-151.

258 B. Weber et al./Clinical and Diagnostic Virology 2 (1994) 245-259
Chiba, S., Kamada, M., Hanazono, H., Motokawa, T., Nakao, T. and Komori A. (1979) IgG antibody against early antigen in subclinical congenital cytomegalovirus infection. Lancet i, 496.
Chou, S., Kim, D.Y., Scott, K.M. and Scwell D.L. (1987) Immunoglobuha M to cytomegalovirus in primary and reactivation infections in renal transplant recipients. J. Clin. Microbiol. 25, 52-55.
Delgado, R., Lumbreras, C., Alba,C., Pedraza, M.A., Otero, J.R., Gomez, R., Moreno, E., Noriega, A.R. and Paya, C.V. (1992) Low predictive value of polymerase chain reaction for diagnosis of cytomegaiovirus disease in fiver transplant recipients. J. Clin. Microbiol. 30, 1876-1878.
Doerr, H.W. and Albert, S. (1990) New developments in CMV antibody screening. Biotest Bull. 4, 125-130.
Doerr, H.W., Fretschner, R. and Geisen, H.P. (1980) Virus-specific IgM proof with routine serologic methods. Zbl. Bakt. Hyg., I. Abt. Orig. A 246, 158-166.
Doerr, H.W., Rentschler, M. and Scheitter, G. (1987) Serologic detection of active infections with human herpes viruses (CMV, EBV, HSV, VZV): diagnostic potential of IgA class and IgG subclass- specific antibodies. Infection 15, 93-98.
Einsele, H., Ehninger, G., Steidie, M., Valibracht, A., Mtlller, M., Schmidt, H., Saul, J.G., Waller, H.D. and MliUer, C.A. (1991) Polymerase chain reaction to evaluate antiviral therapy for cytomegalovirus disease. Lancet 338, 1170-1172.
Engelhard, D., Weinberg, M., Or, R., Shaked, O., Naparstek, E., Halkin, H., Slavin, S., and Sarov, I. (1991) Immunoglobnlins A, G, and M to cytomegalovirus during recurrent infection in recipients of allogenic bone marrow transplantation. J. Infect. Dis. 163, 628-630.
Fenner, T.E., Garweg, J., Hufert, F.T., Boehnke, M. and Schmitz, H. (1991) Diagnosis of human cytomegalovirus-induced retinitis in human immunodeficiency virus type 1-infected subjects by using polymerase chain reaction. J. Clin. Microbiol. 29, 2621-2622.
Griner, P., Mayeski, R., Mushlin, A. and Greenland, P. (1981) Selection and interpretation of diagnostic tests and procedures. Ann. Intern. Med. 94, 557-600.
Joassin, L. and Reginster, M. (1986) Elimination of nonspecific cytomegalovirus immunogiobulin M activities in the enzyme-finked immunosorbent assay by using anti-human immunoglobulin G. J. Clin. Microbiol. 23, 576-581.
Landini, M.P., Lazzarotto, T., Ripalti, A., Guan, M.X. and LaPlaca, M. (1989) Antibody response to recombinant lambda gtll fusion proteins in cytomegalovirus infection. J. Clin. Microbiol. 27, 2324-2327.
McMahon, C.A., Dock, N.L., Lentz, E.B., Forbes, B.A., Reinitz, E.R. and Lambcrson, H.V. Jr. (1989) Detection of cytomegalovirus-specific IgM in renal transplant recipients. J. Clin. Lab. Anal. 3, 350-354.
Nielsen, C., Hansen, M.K., Andersen, H.K., Gerstoft, J. and Vestergaard, B.F. (1987) An enzyme labelled nuclear antigen immunoassay for detection of cytomegalovirus IgM antibodies in human serum: specific and non-specific reactions. J. Med. Virol. 22, 67-76.
Nielsen, L.N., Sorensen, I. and Andersen, H.K. (1988) Kinetics of specific lmmunoglobufins M, E, A, and G in congenital primary, and secondary cytomegalovirus infection studied by antibody-capture enzyme-linked immunosorbent assay. J. Clin. Microbiol. 26, 654-661.
0live, D.M., Simsek, M. and A1-Mnfti, S. (1989) Polymerase chain reaction assay for the detection of human cytomegalovirus. J. Clin. Microbiol. 27, 1238-1242.
Rasmussen, L., Kelsall, D., Nelson, R., Carney, W., Hirsch, M., Winston, D., Preiksaltis, J. and Merigan. T.C. (1982) Virus-specific IgG and IgM antibodies in normal and immunocompromised subjects infected with cytomegalovirus. J. Infect. Dis. 145, 191-199.
Sarov, I., Siqueira-Linhares, M., Chardonnet, Y., Levy, E., Aymard, M., Bosshard, S., Nord, E. and Revillard, J.P. (1981) Detection of specific IgA antibodies in serum of kidney transplant patients with receurent cytomegalovirus infection. Intervirology 15, 228-234.
Schacherer, Ch., Braun, W., and Doerr, H.W. (1988) Detection of cytomegalovirus in bronchial lavage and urine using a monoclonal antibody to an HCMV early nuclear protein. Infection 16, 288-292.
Schmitz, H., Deimling, U. and Flehming, B. (1980) Detection of IgM antibodies to cytomegalovirus (CMV) using an enzyme-labelled antigen (ELA). J. Gen. Virol. 50, 59-68.
Severi, B., Landini, M.P., and Govoni, E. (1988) Human cytomegalovirus morphogenesis: An ultrastrnctural study of the late cytoplasmatic phases. Arch. Virol. 98, 51-64.

R Weberetal./ClinicalandDiagnostic Virology2 (1994) 245-259 259
Steinmann, J. and Bisehoff, J. (1991) Vergleich serologiseher Methoden zum Nachweis einer Cytomegalievirus-Infektion. Lab. Med. 15, 585-589.
Taylor-Wiedeman, J., Hayhurst, G.P., Sissons, J.G.P. and Sinclair J.H. (1993) Polymorphonuclear cells are not sites of persistence of human cytomegalovirus in healthy individuals. J. Gen. Virol. 74, 265-268.
Van Loon, A.M., Van der Logt, J.T.M., Heessen, F.W.A. and Van der Ven, J. (1985) Quantitation of immunoglobulin E antibody to cytomegalovirus by antibody capture enzyme-linked immunosorbent assay. J. Clin. Microbiol. 21,558-561.
Van der Bij, W., Torensma, R., Van Son, W.J., Anema, J,, Schirm, J., Tegzess, A.M. and The, T.H. (1988) Rapid immunodiagnosis of active CMV infection by monoclonal antibody staining of blood leucocytes. J. Med. Virol. 25, 179-188.
Weber, B., Hamann, A., Ritt, B., Rabenau, H. and Doerr, H.W. (1992a) Comparison of shell vial culture and serology for the diagnosis of human cytomegalovirus infection in neonates and immunocompromised subjects. Clin. Investig. 70, 503-507.
Weber, B., Stemmler, A., Ernst, W., Scheuermann, E,. H., Braun, W. and Doerr, H.W. (1993a) Improvement of serological diagnosis of human cytomegalovirus (HCMV) infection in renal transplant recipients by testing for specific immunoglobulin E by ELISA. Infection 21, 158-163.
Weber, B., Opp, M., Born, H.J., Langenbeck, U. and Doerr, H.W. (1992b) Laboratory diagnosis of congenital human cytomegalovirus infection using PCR and shell vial culture: a case report. Infection, 20, 155-157.
Weber, B., Klinghardt, U., Lux, A., Rabenan, H., Braun, W. and H.W. Doerr. (1993b) The detection of neutralizing antibodies against human cytomegalovirus is not influenced by strain heterogenicity. J. Med. Virol. 40, 28-34.
Weber, B., Braun, W., Tyralla, B., and Doerr, H.W. (1992c) Human cytomegalovirus (HCMV) specific IgE in primary HCMV infection. Clin. Investig. 70, 497-502.
Weber, B., Braun, W., Cinatl, J. Jr. and Doerr, H.W. (1993c) Humoral immune response to human cytomegalovirus infection: Diagnostic potential of immunoglobulin class and IgG subclass antibody response to HCMV early and late antigens. Clin. Investig. 71,270-276.
Weber, B., Nestler, U., Ernst, W., Rabenan, H., Braner, J., Birkenbach, A., Scbeuermann, E.H., Schoeppe, W. and Doerr, H.W. (1994). Low correlation of human cytomegalovirus DNA amplification by potymerase chain reaction with cytomegalovirus disease in organ transplant recipients. J. Med. Virol. in press.
Zipeto, D., Revello, M.G., Silini, E., Parea, M., PercivaUe, E., Zavattoni, M., Milanesi, G. and Gerna, G. (1992) Development and clinical significance of a diagnostic assay based on the polymerase chain reaction for detection of human cytomegalovirus DNA in blood samples from immunocompromised patients. J. Clin. Microbiol. 30, 527-530.