selected readings in oral and...
TRANSCRIPT

S E L E C T E D R E A D I N G S
IN
ORAL AND
MAXILLOFACIAL SURGERY
HEMOSTATIS: A CLINICAL REVIEW OF PHYSIOLOGY,
PATHOLOGY, PHARMACOLOGY, AND
PERI-OPERATIVE MANAGEMENT
Richard P. Szumita, DDS, Paul M. Szumita, PharmD, BCPS
Volume 21, Number 3 August, 2013

SROMS VOLUME 21.32
Hemostasis: a CliniCal Review of PHysiology, PatHology, PHaRmaCology, and PeRi-oPeRative management
Richard P. Szumita, DDS and Paul M. Szumita, PharmD, BCPS
intRodUCtion
Understanding hemostasis is essential for safely managing patients in any surgical discipline. The oral and maxillofacial surgery literature has consistently reviewed the physiology, pathology, and pharmacology of hemostasis. There are multiple references in the medical and dental literature on time-tested protocols to help with decision making in the peri-operative period. With this literature support and clinical experience, oral and maxillofacial surgeons, along with input from their physician colleagues, have been proficient in safely managing patients with disorders of hemostasis.
However, the number of medications impacting upon hemostasis has increased rapidly over the last few years. These additional medications are not simply clones of medications that we have all gained clinical experience in managing but include newer classes of medications with different pharmacodynamics and varying indications for clinical use. The “time tested” clinical guidelines upon which clinicians have relied may no longer be appropriate for these newer classes of medications. In order to safely manage patients, oral and maxillofacial surgeons will need to be familiar with important steps in the hemostatic process and with how newer drugs impact hemostasis.
Another important concept is risk stratification of patients being treated with antithrombotic medications. The risk of thromboembolic complications are varied depending on the condition being treated and co-morbidities. Our literature has clearly stated that interrupting antithrombotic therapy peri-procedurally carries risk. The
medical literature has better defined the stratification of risks. Physicians can use this concept when choosing pharmacotherapy. Oral and maxillofacial surgeons can use risk stratification when discussing management strategies for anticoagulated patients.
In this paper, the physiology and pathophysiology of hemostasis will be reviewed. Included will be a review of pharmacologic agents affecting hemostasis and thrombosis. A literature-based review of the peri-operative management of patients on these medications will be provided. Also, the future of pharmacologic agents in hemostasis will be reviewed.
First, a few definitions are reviewed. Although there are slight variations in the definition of hemostasis, a clinical definition that seems apropos for the climate in which we practice is the following: Hemostasis is the physiologic system of competent blood vessels, endothelial cells, platelets, and numerous plasma proteins that act in a finely

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.33
controlled manner to preserve blood vessel integrity and prevent pathologic hemorrhage or thrombosis.1 While medical and surgical disciplines strive to prevent excessive hemorrhage and inappropriate thrombus formation, pharmacology is increasing the number of drugs available that alter hemostasis. Antithrombotic medications refer to any medications that cause an effect on the formation or maintenance of a thrombus or clot. Antithrombotic medications include anticoagulants and antiplatelet medications. Anticoagulant medications reduce the formation of fibrin from fibrinogen. Antiplatelet medications affect formation of a platelet plug.
The physiology of hemostasis is complex. This review is intended to be of sufficient depth to allow the practicing clinician a thorough understanding of the essential steps and reactions responsible for cessation of bleeding and prevention of excessive thrombus formation. A limited number of pathologic alterations in hemostasis will be reviewed in order to contrast normal physiology. A major focus of this review is to highlight pharmacologic agents that affect hemostasis, with emphasis on the expanding number and role of oral antithrombotics.
tHe PHysiology of Hemostatis
Review of the physiology of hemostasis will begin with discussion of the important contributions of blood vessels and endothelial cells, platelets, and coagulation factors. The interplay of these elements will then be highlighted in terms of a contemporary
model of hemostasis.
Primary Hemostasis
Blood Vessels and Endothelial Cells
At the time of tissue injury, immediate local tissue and vessel reaction occurs which begins the cascade of events that leads to eventual formation of a clot. Peripheral blood vessels constrict to decrease blood loss. This vasoconstriction is enhanced by ADP, ATP and 5-HT, all of which are stored in platelets. Damaged vessel endothelium releases several pro-thrombotic substances including: von Willebrand factor (vWF), tissue factor (Factor III), collagen, and plasminogen activator inhibitor-1. vWF is an important molecule in platelet adherence to the wounded site. Tissue factor initiates the coagulation reactions leading to the formation of fibrin. Collagen stimulates platelet activation and is also critical for platelet adhesion.1-4 Plasminogen activator inhibitor stops the body’s natural anticoagulant from lysing fibrin at the site of the injury. Within several minutes after injury, vessel dilation occurs, presumably signaling the onset of the healing process.
To prevent pathologic or excess clotting in vessels, the endothelium is also equipped with mechanisms opposing hemostasis. Vessels have smooth endothelial surfaces that are lined with glycocalyx, a mucopolysaccharide that repels clotting factors and platelets. In addition, the protein thrombomodulin is bound to the endothelial membrane. Thrombomudulin serves two functions. First, it binds thrombin,

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.34
neutralizing thrombin’s critical roles in promoting clotting. The thrombomodulin-thrombin complex also activates circulating protein C, which acts as an anticoagulant by inactivating factors V and VIII.3
Platelets
Two of the primary components of a “clot” are platelets and fibrin. Platelets perform three important functions in coagulation: control of thrombin generation, support of fibrin formation, and regulation of fibrin clot retraction.5 Platelets are able to anchor these functions directly at the site of tissue or vessel injury. After vessel vasoconstriction, platelets initiate the cessation of bleeding by adhering to the site of injury. Platelets then coalesce or aggregate. This “clump” of platelets is then able to focus and direct multiple biochemical reactions at the site of injury leading to the formation of fibrin.
Research continues to reveal the central roles and complex nature platelets play in hemostasis. Recent findings suggest there may be different platelet populations, with distinct surface properties, each group designed to carry out different roles in coagulation.5
Clinically, platelet evaluation is divided into platelet quantity and quality. Platelet quantity is generally easy to assess with blood sampling. Platelet quality is based on function and is divided into platelet activation, platelet adhesion, platelet aggregation, and platelet secretion. Each one of these areas can be
affected by pathology and provide varying targets for pharmacologic intervention.
Platelet Quantity
Normal platelet counts are approximately 150,000 – 400,000 per microliter.3 The estimated lifespan of a platelet is 8 to 12 days. Platelet turnover in the absence of pathology is estimated at 1.2 – 1.5 x 1011 platelets per day. The primary sites for platelet removal appear to be the spleen, liver, and bone marrow.6
Platelet Quality: Activation
Platelets circulate in a non-activated state. Upon vessel injury, platelets become activated. Collagen and thrombin are the two most powerful platelet activators. Many other substances also promote platelet activation, including thromboxane A2, 5-HT, epinephrine, and ADP. With activation, several structural and physiologic changes occur to the platelet: platelet shape change, expression of pro-inflammatory molecules, expression of platelet pro-coagulant activity, potentiation of aggregation by other prothrombotic factors (i.e. collagen), and conversion of platelet receptor GP IIb/IIIa into an active form.7,8 Platelet activation “primes” the platelet to begin its pro-hemostatic and pro-healing functions.
Platelet Quality: Adhesion

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.35
Once activated, platelets are better able adhere to the injured site in order for an effective thrombus to be formed. Platelet adhesion relies primarily on exposed collagen at the site of injury, vWF, and glycoprotein receptors in the platelet membrane. It is important to note that another substance, tissue factor (Factor III), is exposed after endothelial damage. As will be discussed shortly, tissue factor is responsible for initiating the process of thrombin and fibrin formation.
Von Willebrand factor (vWF) is a large glycoprotein that is found in in the circulation in an inactive form, in the subendothelial matrix of blood vessels, within Weibel-Palade bodies of endothelial cells, and in the α-granules of platelets.2,9 Upon endothelial damage, collagen becomes exposed and binds vWF. The glycoprotein receptor Ib/V/IX (GP Ib) in the platelet membrane then binds to vWF. Following this, additional anchoring is provided by collagen binding to other platelet receptor glycoproteins GP VI and GP Ia/IIa. Along with their adhesion roles, research is uncovering mechanisms by which the glycoprotein receptors are also involved with cell signaling.2,10
Platelet Quality: Aggregation
In the evolution of a thrombus, another essential function of platelets is to aggregate. This “clumping” together of platelets occurs between platelet membrane glycoprotein receptors (GP IIb/IIIa) and fibrinogen. Fibrinogen is the intermediary between GP IIb/IIIa receptors on adjacent platelets. GP IIb/IIIa can also bind vWF, assisting in aggregation. (Note: GP IIb/IIIa is also referred
to in the literature as αIIbβ3 integrin.)10 Platelet aggregation results in concentrating a greater number of platelets and anchoring fibrinogen at the site of injury.
Platelet Quality: Secretion
Among its attributes, the platelet is a biochemical warehouse, which is not a novel concept in our specialty.11-14 Platelet concentrates have been extensively studied and used in clinical practice. Platelets store a multitude of substances that are important in hemostasis as well as in healing. These bioactive substances are contained in α-granules, dense granules, and the cytoplasm. The stored molecules involved in hemostasis include α-granules containing vWF, Factors I (Fibrinogen), V and XI, protein S, PAI-1, HMWK. Dense granules contain serotonin, ADP, ATP and calcium. The cytoplasm contains factor XIII. These substances are secreted during the evolution of the thrombus.6
Platelet Pathologies
Defects in Platelet Quantity
Platelet quantity alterations are seen in many and varied pathologic states and can be induced by medications. (See also Selected Readings in Oral and Maxillofacial Surgery, Vol. 8, #6) In surgery, decreased numbers of platelets (thrombocytopenia) is the primary concern in perioperative management. Thrombocytopenia is caused by one of four general pathologies: decreased production, increased destruction, sequestration, or

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.36
dilution.15
decreased production is most commonly caused by marrow suppression from disease or medication or from direct infiltration of malignant cells. increased destruction of platelets can arise from immunologic or non-immunologic pathologies. Immunologic causes include viral and bacterial infections, drug-induced destruction, idiopathic thrombocytopenic purpura (ITP), and chronic autoimmune disorders. Non-immunologic causes include disseminated intravascular coagulation (DIC), thrombosis, blood vessel disorders, and hemolytic uremic syndrome.15 Platelet sequestration is caused by splenomegaly. Among its several functions, the spleen normally sequesters a physiologic number of platelets in a non-pathologic state. Increased sequestration can lead to thrombocytopenia.15 Platelet dilution can occur as a consequence of resuscitation of volume deficient patients using crystalloid fluids (i.e. normal saline, lactated ringers solution) or with colloid solutions devoid of platelets (i.e. Hespan, Hetastarch, etc.
There is debate in the surgical literature on an acceptable platelet count to perform elective surgical procedures. In a patient with a negative history and no abnormal physical findings, a platelet count of greater than or equal to 50,000 / μl has been recommended for elective minor surgical procedures.16
Levels of 100,000/μl is recommended in a patient with active bleeding or in major surgical procedures.15
Elevated number of platelets, (thrombocytosis) is due almost exclusively
to one of the following: iron deficiency, inflammation, cancer, infection, or a myeloproliferative process. Patients with increased platelet counts are not necessarily at a risk for thrombosis. Thrombocytosis from acute and chronic inflammation has not been associated with increased thrombotic risk. In addition, patients with significantly elevated platelets from a myeloproliferative disorder may actually be at risk for bleeding.17
Platelet quantity, however, does not reflect platelet function. Normal levels of platelets alone do not assure proper hemostasis. Qualitative platelet defects must also be considered.
Defects in Platelet Adhesion
von Willebrand disease (vWD) is the most common inherited bleeding disorder. von Willebrand factor (vWF) has two significant functions. First, vWF is the major molecule responsible for platelet adhesion to the subendothelium at the site of injury. Secondly, vWF serves as a binding protein for circulating factor VIII. Binding to vWF significantly increases the serum half-life of factor VIII. Two separate active (binding) sites on the large molecule convey the two separate functions. Manifestations of vWD are then either 1) “platelet-like” due to dysfunction at the platelet adhesive site of vWF or 2) resemble factor VIII deficiency (hemophilia A) due to a defect in the factor VIII binding site.
vWD has been classified into three major types: type 1, type 2, and type 3. Type 2 is further subclassified into type 2A, type 2B, type 2M, and type 2N. type i is the most

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.37
common form of the disease accounting for approximately 80% of all cases. This type is caused by a decrease in vWF, vWF function, and factor VIII. Manifestation of the disease usually occurs in childhood with significant ecchymoses without trauma, epistaxis, and other mucosal bleeding. However, not all patients have symptoms. Mild type 1 vWD may first manifest after dental extractions, especially third molar extractions.
type 2 vWD represents a group of disorders where qualitative defects are noted in vWF. Type 2A is the result of molecular structural defects in the platelet binding sites. Clinically, platelet adhesion is affected. A structural defect at the platelet binding site is also seen in type 2B vWD. However, this defect results in increased spontaneous binding to platelets in circulation. The vWF-platelet complex is then cleared from the circulation by the reticuloendothelial system.
Type 2M forms of the disease are caused by a qualitative defect in the vWF without structural abnormalities. Type 2N is caused by decreased ability to bind factor VIII. In type 3, also called severe vWD, significant deficiencies are noted in vWF, vWF activity, and factor VIII levels.17
Another clinical disorder of platelet adhesion is Bernard-Soulier disease, which is caused by a defect in the platelet membrane glycoprotein Ib /V/IX complex.18 Defects in this platelet receptor lead to decreased platelet adhesion at the site of injury and pathologic hemorrhage.
Defects in Platelet Aggregation
Glanzmann thrombasthenia (GT) is characterized by either a quantitative or qualitative defect in the platelet membrane receptor GPIIb/IIIa. As reviewed above, this receptor is intimately involved with platelet aggregation. It is an inherited autosomal recessive disorder. Clinical bleeding is usually restricted to homozygotes and presents as purpura, epistaxis, gingival bleeding, and menorrhagia.18,19
Defects in Platelet Secretion
Platelet storage pool disease and a number of syndromes have been identified where the secretory components of platelets, the α- and δ-granules, are abnormal.
Storage pool disease (SPD) represents a group of disorders with deficiencies in platelet granules or their components. There are three groups of SPD: deficiencies in α-granules (known as α-SPD or gray platelet syndrome), abnormality of dense granules (δ-SPD), or abnormalities in both α- and δ-granules (αδ-SPD). These diseases are rare and have variable clinical bleeding risks.19
The following syndromes have been associated with defects in platelet secretion: Quebec platelet syndrome, Hermansky-Pudlak syndrome, Chediak-Higashi syndrome, Griscelli syndrome, Paris-Trousseau (Jacobsen) syndrome, and arthrogryposis-renal dysfunction-cholestasis syndrome. As with storage pool disease, these syndromes are rare and clinical bleeding is variable.19
secondary Hemostasis

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.38
With formation of the platelet plug, the next goal of hemostasis is the conversion of fibrinogen to fibrin. This is often referred to as secondary hemostasis. The formation of fibrin involves a number of enzymatic conversions of protein factors and cells on which these reactions occur and are directed.
The Factors
Factor I, fibrinogen, is a large protein manufactured in the liver and circulates in plasma.20 Fibrinogen serves two critical functions. Platelet aggregation occurs when fibrinogen binds to adjacent platelet membrane GPIIb/IIIa receptors. Fibrinogen is also the precursor to fibrin. Fibrin forms when thrombin catalyzes proteolysis of fibrinogen.
Factor II, prothrombin, is synthesized in the liver and is one of four factors (II, VII, IX, X) that contains carboxylated glutamic acid residues needed for function. These residues require vitamin K for synthesis. The activated form of Factor II is thrombin. Thrombin has many important functions including: catalyzing the conversion of fibrinogen to fibrin, activating factors V, VIII, XI, and XIII, and activating platelets.1,21,22
Factor III is commonly referred to as tissue factor (TF). TF is unique in that it is a membrane protein found within subendothelial cells of blood vessels and cells of perivascular tissue (i.e., fibroblasts).4,21,23
Upon vessel disruption or injury TF becomes exposed and initiates coagulation.
Factors IV, V and VIII are cofactors. Without these cofactors, several of the
proteolytic factor activations would not occur. Specifically, factor IV (which is calcium) is required as a cofactor in the activation of factors II, IX, X, XI. Factor V is a cofactor with calcium to convert factor II (prothrombin) to thrombin. Factor VIII is also known as antihemophilic factor. Decreases in factor VIII levels are associated with classic hemophilia (hemophilia A). Factor VIII circulates in plasma bound to vWF. It is converted to an active form by thrombin and then serves as a cofactor with calcium for the activation of factor X.20,21,24
Factor IX is also known as Christmas factor and deficiencies are responsible for hemophilia B or Christmas disease.20 Factor XIII is the fibrin stabilizing factor. The fibrin monomers formed by proteolysis of fibrinogen are initially held together by weak noncovalent bonding. Factor XIII, after activation by thrombin, converts the fibrin linkages to strong covalent bonds and creates the fibrin mesh by cross-linking adjacent fibrin molecules.20
Cascade Model of Coagulation
Our understanding of coagulation has been evolving over the last century and continues to evolve through present day. A major contribution to our understanding of hemostasis occurred in 1964 when the cascade model of the enzymatic reactions resulting in fibrin formation was introduced.25 Since then, studies have further defined where and when these reactions occur in vivo. This updated model is often referred to as the cell-based model of coagulation.5,21,26-28
For completeness, the biochemical

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.39
table 1: sUmmaRy of faCtoRsfactor synonym site of synthesis
I Fibrinogen LiverII Prothrombin LiverIII Tissue Factor Membrane protein in perivascu-
lar tissuesIV CalciumV Proaccelerin Liver, Megakaryocytes
VII Prothrombin Conversion Factor LiverVIII Antihemophilic Factor LiverIX Christmas Factor LiverX Stuart-Prower Factor LiverXI Plasma Thromboplastin Antecedent LiverXII Hageman Factor LiverXIII Fibrin Stabilizing Factor Liver, Megakaryocytes
Adopted from Hall: Textbook of Medical Physiology3______________________________________________________________________________
Figure 1: Biochemical Model of Coagulation
cascade will be reviewed first, followed by a discussion of the cell-based model. Reviewing both emphasizes that the enzymatic reactions occur not in a cascading fashion but in conjunction with specific cell surface receptors that localize and direct the enzymatic conversions. In addition, when we discuss pharmacotherapeutics, the cascade model (Fig. 1, on P. 8) will be used because it provides an effective backdrop to illustrate where medications exert their effect. However, the reader is again cautioned to relate the enzymatic reactions in terms of the cell-based model.
Common Pathway

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.310
Within the common pathway, three factors undergo proteolysis culminating in the conversion of fibrinogen to fibrin. Factor X becomes activated by products from the extrinsic and intrinsic pathways. Activated factor X (Xa) catalyzes the conversion of factor II (prothrombin) to thrombin. Thrombin then catalyzes the conversion of fibrinogen to fibrin.1,3
The Extrinsic / Initiator / Tissue Factor Pathway
The extrinsic pathway is also referred to as the initiator pathway and tissue factor pathway. Factors III (tissue factor) and VII comprise the extrinsic pathway. Tissue factor (TF) represents membrane bound receptors in perivascular tissue. At the site of injury, tissue factor is exposed and then binds circulating factor VII and catalyzes its conversion to activated factor VII (VIIa). Factor VIIa then catalyzes the conversion of factor X to activated factor X in the common pathway. As will be discussed shortly, Factor VIIa also activates factor IX.20,21,28
The Intrinsic / Propagator Pathway
The intrinsic pathway is also referred to as the propagator pathway. The factors that constitute the intrinsic pathway include: factors IX, XI, XII. Factor XII is listed as the first reaction in the pathway. Factor XII is a protein that circulates in plasma. It is activated by contact with collagen in an injured vessel. Activated factor XII (XIIa) catalyzes the activation of factor XI. High molecular weight kininogen (HMWK) acts as a cofactor in this conversion and
prekallikrein accelerates the reaction. Factor XIa then catalyzes the activation of factor IX (Christmas factor), and Factor IXa then activates factor X in the common pathway.20
Cell-Based Model of Hemostasis
The cascade model of coagulation, introduced in 1964, has had a significant impact on our understanding of how fibrin is formed. However, researchers and clinicians had known for years this model alone could not readily explain situations encountered clinically. For instance, deficiencies in factor XII do not result in pathologic hemorrhage, whereas deficiencies in factors VIII and IX are consistently linked to pathologic hemorrhage in hemophilia A and B, respectively.21
It had also become obvious to researchers that membrane phospholipids were essential for in vivo thrombin and fibrin formation. Accumulation of data led researchers to develop surface-dependent and cell-dependent models of hemostasis that have now become a modern theory of in vivo hemostasis known as the cell-based model of hemostasis.21,24,25,27,28 (Fig. 2, on P. 10) Cell-based hemostasis links the above described enzymatic activation of factors with specific cells accumulating at the site of vascular injury.
The process of coagulation begins when tissue factor (FIII) is exposed to blood at the site of injury. As discussed above, tissue factor is a transmembrane protein found in certain perivascular cells. Tissue factor functions as a receptor and cofactor for FVII. Factor VII circulates in the blood and if a disruption of the vessel wall is encountered,

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.311
Figure 2: Cell-Based Model of Hemostasis. a. Ini-tiation: Upon injury and vessel disruption, collagen, vWF, and Tissue Factor (TF) become exposed. Factor VII binds to, and is activated by, TF. TF then activates factors IX and X. Factor Xa generates local thrombin. Factor IXa will diffuse to platelet membranes of the forming platelet plug; b. Amplification: Local throm-bin generated by the TF/VIIa complex helps to acti-vate platelets for platelet adhesion and aggregation, further activates factor IX, and activates factors V and VIII; C. Propagation: Activated factors Va, VIIIa, and IXa become platelet membrane bound with calcium (factor IV) and are then responsible for the formation of large quantities of factor Xa and thrombin, leading to the conversion of fibrinogen to fibrin at the site of injury.27
___________________________________
a
b
C
FVII will adhere to the TF in the membranes of exposed cells (e.g., fibroblasts, etc). Once bound to TF, FVII becomes activated to FVIIa. The TF/FVIIa cell membrane bound complex then activates factor X and factor IX. Factor Xa reacts with cofactor Va to produce
___________________________________
a small amount of thrombin at the TF/FVIIa complex. This thrombin activates platelets and activates factors V, VIII, and XI. These reactions are restricted to the TF bearing cells because FXa is immediately inactivated by the natural anticoagulants antithrombin (AT) and tissue factor pathway inhibitor (TFPI).
The other factor activated by the TF/FVIIa complex, FIXa, is not inactivated by TFPI and only slowly by AT, and, therefore, can diffuse to the surface of the activated platelets that are adhering to the injury site and aggregating by mechanisms previously discussed. Factor IXa binds to platelet receptors. Activated platelets also bind factors Va, VIIIa, and XIa. The platelet bound activated factors Va, VIIIa, IXa, and XIa then further activate plasma FX, leading to a significant amount of thrombin production on the platelet surface. This thrombin is the catalyst for converting fibrinogen to fibrin and for activating factor XIII, which will stabilize the clot.21,25
The cell-based model is divided into

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.312
three overlapping processes: initiation, amplification, and propagation. initiation (Fig. 2A) is when exposed cell membrane tissue factor binds FVII, and the TF/VIIa cell bound complex activates factor X, leading to a small amount of thrombin production. Amplification (Fig. 2B) is when the thrombin produced during initiation activates platelets and factors V, VIII, XI. These activations set in motion propagation (Fig. 2C) , the procoagulant response that will lead to an explosion of thrombin production at the platelet membrane surface.21
tHRombUs
The summation of cellular and enzymatic coagulation processes is the formation of the thrombus or clot immediately at the site of disruption of blood vessel integrity. The thrombus thus contains platelets and fibrin. The platelets were anchored to the wound by glycoprotein receptor binding to exposed vWF and collagen at the injury, and the platelets were aggregated by membrane glycoprotein receptor binding of fibrinogen.
Formation of a physiologic thrombus at a wound site is essential for any surgical discipline and for preservation of life. However, formation of a pathologic thrombus away from the site of a vessel disruption can lead to morbidity and death. To avoid this, medicine and the medical subspecialties along with pharmacologists have been designing antithrombotic strategies for the treatment, maintenance, and prevention of pathologic thrombus formation in coronary artery infarctions, thromboembolic strokes, deep vein thromboses that can lead to pulmonary embolism, and other areas that can lead to
vessel infarction and loss of organ function. It is at this juncture that medicine and surgery collide—each with a different perspective but with the same goal of safely guiding our shared patients through surgical procedures by avoiding excessive and possibly life-threatening hemorrhage from the surgical site while also avoiding pathologic and possibly life-threatening thrombus formation remote from the site of surgery.
For antithrombotic medications that have been in clinical use for decades the literature is replete with recommendations for the peri-operative management of patients, and practicing surgeons have acquired significant clinical experience.29-49 The challenge surgical disciplines face today is the increasing number of antithrombotic medications, most particularly oral, available for clinical use.
For a number of years, aspirin and clopidogrel have been the mainstay of antiplatelet therapy, and warfarin was the only oral anticoagulant for nearly six decades. However, since 2009, five additional oral antithrombotic medications have been approved by the FDA and introduced into clinical practice: the antiplatelet medications prasugrel (Effient®) (2009)50 and ticagrelor (Brilinta®) (2011)51 and the anticoagulant medications dabigatran (Pradaxa®) (2010)52, rivaroxaban (Xarelto®) (2011)51, apixaban (Eliquis®) (2012)53 – with others likely to follow. It may be some time before proven clinical guidelines are published on, and surgeons have acquired significant clinical experience in, the peri-operative management of patients on these newer antithrombotics. In the meantime, for clinicians to make sound clinical decisions, an understanding of

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.313
the pharmacology of the antithrombotics and their clinical indications is important.
antiplatelet medications
Antithrombotic medications are divided into antiplatelet and anticoagulant medications. Antiplatelet medications have their primary clinical effect on platelet function and primary hemostasis, i.e. the platelet plug. Antiplatelet medication can be subdivided into types by their actions listed in Table 2 (on P. 13).
Glycoprotein IIb/IIIa Inhibitors
The medications of this group are abciximab (ReoPro®), eptifibitide (Integrilin®), and tirofiban (Aggrastat®). Glycoprotein IIb/IIIa inhibitors are administered intravenously in the hospital setting for treatment of acute myocardial infarction and in patients undergoing percutaneous coronary interventions. These medications inhibit the level of platelet membrane glycoprotein IIb/IIIa, decreasing platelet aggregation.54
Cyclooxygenase (COX) Inhibitors
COX inhibitors have several useful clinical functions. Surgeons are undoubtedly well versed in and utilize their anti-inflammatory and analgesic properties. Their antiplatelet properties are also well understood. COX inhibitors exert their effect by altering the function of the cyclo-oxygenase enzyme found in the platelet membrane. Within the developing thrombus, phospholipids comprising the platelet membranes are released. (Fig.
Figure 3: Schematic of cyclooxygenase enzyme’s role in hemostasis___________________________________
3) Phospholipase enzymes cleave these molecules resulting in phosphates and lipid chains. The lipids are degraded to arachidonate which is converted to prostaglandin by cyclo-oxygenase enzymes. Prostaglandin G2 is then further catabolized to prostaglandins and thromboxane A2. Thromboxane A2 is a powerful stimulant for platelet aggregation and vasoconstriction.6
When COX is antagonized, less prostaglandins and thromboxane are produced resulting in the clinical effects of analgesia, decreased inflammation, and platelet inhibition via decreased aggregation. The primary difference between aspirin and all of the other non-steroidal anti-inflammatory medications is that aspirin irreversibly antagonizes COX while all of the others reversibly bind this enzyme. Hence, aspirin is the only medication in its class to be an effective agent in the management and prevention of thromboembolism.54
Adenosine Diphosphate Inhibitors

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.314
table 2: antiPlatelet mediCations: oRal and PaRenteRalgeneric name Proprietary name action Route
Abciximab ReoPro Glycoprotein IIb/IIIa Inhibitor
IV
Eptifibatide Integrilin Glycoprotein IIb/IIa Inhibitor
IV
Tirofiban Aggrastat Glycoprotein IIb/IIIa Inhibitor
IV
Acetylsalicylic acid Aspirin COX Inhibition OralClopidogrel Plavix® ADP Receptor Inhibi-
tionOral
Prasugrel Effient® ADP Receptor Antag-onist
Oral
Ticagrelor Brilinta® ADP Receptor Antag-onist
Oral
Cilostazol Pletal Phosphodiesterase In-hibitor
Oral
Dipyridimole Persantine Adenosine Reuptake Inhibitor
Oral
Acetylsalicylic acid + dipyridimole
Aggrenox® See Above Oral
Adapted form: Tarascon Pocket Pharmacopoeia, Jones & Bartlett Publishing and USBMIS, Inc.2013______________________________________________________________________________
This class of drug has become a staple in antiplatelet therapy. (Table 3, on P. 14) Adenosine diphosphate (ADP) inhibitors include the thienopyridines and ticagrelor (Brilinta®). Thienopyridines include: ticlodipine, clopidogrel, and prasugrel (Effient®).55 Although ticagrelor’s chemical classification is a cyclopentyltriazolopyrimidine,56 its mechanism of action is similar to the thienopyridines, it is classified with them clinically as ADP inhibitors.57
Platelet membranes contain two receptors involved with platelet activation and aggregation, receptors P2Y1 and P2Y12.
Both receptors are activated by ADP. When these receptors bind ADP, platelets become activated. Blocking one of the receptors is sufficient to block platelet activation. In addition, ADP inhibition deactivates the platelet receptor GP IIb/IIIa decreasing platelet aggregation.54,58,59
Ticlodipine was the first in this class to be developed. However, because it has been associated with life-threatening blood dyscrasias and a high rate of TTP, its use has been limited.54
Dual antiplatelet therapy, combining clopidogrel (Plavix®) with aspirin, has

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.315
proven efficacious in lowering the risk of coronary artery stent thrombosis and thrombotic complications of acute coronary syndromes.60 Recently, two additional adenosine diphosphate inhibitors have been released: prasugrel (Effient®) (approved in July, 2009) and ticagrelor (Brilinta®) (approved in July, 2011).50,51
Although clopidogrel (Plavix®), Prasugrel (Effient®), and Ticagrelor (Brilinta®) are in the same pharmacologic class, there are several important differences among these drugs. Clopidogrel (Plavix®) and Prasugrel (Effient®) are both prodrugs, requiring biotransformation in the liver to become active. Clopidogrel (Plavix®) additionally requires a specific liver cytochrome (CYP 2C19) for biotransformation. It is estimated that 30% of the population has decreased function of this cytochrome (25% in Caucasians, 30% in African-Americans, and 50% in Asians).61
In those patients, less active metabolite is available, decreasing efficacy.62
However, it should be that noted some evidence exists refuting the clinical importance of the defective cytochrome.63 Prasugrel (Effient®) does not require this cytochrome for biotransformation and,
therefore, has less variation in efficacy. Clopidogrel (Plavix®) and Prasugrel (Effient®) irreversibly inhibit platelets, while ticagrelor (Brilinta®) reversibly inhibits platelet function.64
Like clopidogrel (Plavix®) and prasugrel (Effient®), ticagrelor (Brilinta®) partially blocks the platelet membrane receptor adenosine diphosphate. Unlike clopidogrel (Plavix®) and prasugrel (Effient®), ticagrelor (Brilinta®) is the active form of the drug not requiring biotransformation for clinical efficacy, and platelet inhibition is reversible.65 However, evidence suggests ticagrelor is a more potent platelet inhibitor than clopidogrel, and even though ticagrelor is reversible, after discontinuation, it takes approximately 24 to 48 hours for platelet inhibition to return to levels equivalent with maintenance levels of clopidogrel.66
Phosphodiesterase inhibitor
Cilostazol has antiplatelet effects along with vasodilatory properties and antiproliferative effects (after endothelial injury). Studies have demonstrated its effectiveness in treating symptoms of intermittent claudication, preventing thrombotic events in patients with peripheral
table 3: CHaRaCteRsitCs of adenosine diPHosPHate inHibitoRsclopidogrel prasugrel ticagrelor
Partially blocks platelet ADP P2Y12 receptor
Partially blocks platelet ADP P2Y12 receptor
Partially blocks platelet ADP P2Y12 receptor
Prodrug Prodrug Active formRequires CYP450 2C19 for biotransformation
Does not require CYP450 2C19 for biotransformation
N/A
Irreversible platelet inhibition Irreversible platelet inhibition Reversible platelet inhibition
______________________________________________________________________________

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.316
arterial disease, and preventing stent restenosis.55
Adenosine Reuptake Inhibitors
Dipyridamole is a vasodilator with minimal antithrombotic activity.54 Studies showed efficacy when combined with aspirin in preventing vascular events in patients with a history of TIA or stroke. However, no benefit was found in patients with coronary artery disease, peripheral arterial disease, or other high-risk patients.55
anticoagulant medications
Prior to discussing anticoagulant medications, a brief review of the body’s natural anticoagulants will help in the understanding of pharmacologic anticoagulants. Endogenous anticoagulants serve primarily to prevent excessive and pathologic thrombin and fibrin formation away from the site of injury. The body has three natural anticoagulant systems: Antithrombin (AT), Tissue factor pathway inhibitor, and Protein C / Protein S.
antithrombin (AT), also referred to as antithrombin III (ATIII), is a protein made in the liver that inhibits all coagulation factors except for factor VIIa. It has a primary affinity for neutralizing factors IIa and Xa. AT forms a complex with the activated factors causing inhibition of factor activity.1
tissue factor pathway inhibitor (TFPI) first binds to factor Xa. This complex then binds to TF-VIIa forming a quaternary complex inhibiting VIIa.1
Proteins C and s are manufactured in the liver. Protein C, which circulates in blood, is activated by the endothelial bound thrombomodulin-thrombin complex. Protein C, in the presence of its cofactor protein S, inactivates factors V and VIII.
Anticoagulant medications decrease the formation, growth, and embolization of thrombi and are effective in the prevention and treatment of thromboembolic disease.67
The anticoagulation medications are listed in Table 4 (on P. 16).
Brief History
The history of anticoagulant medications can be arbitrarily divided based on route of administration: parenteral versus oral. The first anticoagulant medication was heparin which was released in the 1940’s. Heparin is for parenteral use only.
Warfarin, the first oral anticoagulant, was released in 1954.The history of the development of warfarin began in 1939, when dicumarol was isolated as the cause of a hemorrhagic disorder noted in cattle. From dicumarol, a number of congeners were synthesized, including warfarin. These substances were first thought too toxic for use in medicine and instead were employed as effective rat poisons. In the early 1950’s, human clinical trials began after their safety in humans had been documented. This led to a published report from the American Heart Association in 1954 showing favorable results when dicumarol was used in patients with myocardial infarction.69,70
Not until 1993 was another class of

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.317
_____________________________________________________________________________
table 4: antiCoagUlation mediCations: oRal and PaRenteRalgeneric name Proprietary
nameClassification Route
Heparin Unfractionated Heparin IV / SubcutaneousDalteparin Fragmin® Low Molecular Weight Heparin
(LMWH)Subcutaneous
Enoxaparin Lovenox® Low Molecular Weight Heparin (LMWH)
Subcutaneous
Warfarin Coumadin®, Jantoven®
Vitamin K Antagonist Oral
Fondaparinux Arixtra® Factor Xa Inhibitor SubcutaneousRivaroxaban Xarelto® Factor Xa Inhibitor OralApixaban Eliquis® Factor Xa Inhibitor OralArgatroban Argatroban Direct Thrombin Inhibitor IVBivalirudin Angiomax® Direct Thrombin Inhibitor IVDesirudin Iprivask® Direct Thrombin Inhibitor SubcutaneousDabigatran Pradaxa® Direct Thrombin Inhibitor Oral
anticoagulant was available for clinical use when low molecular weight heparin (LMWH), enoxaparin, a parenteral agent, was introduced into clinical practice. Following LMWH, two additional classes of parenteral anticoagulants were released. In 1998, the first parenteral direct thrombin inhibitor was introduced, followed in 2001 by the first parenteral factor Xa inhibitor.
It was not until 2010 that an oral anticoagulant other than warfarin became available in clinical practice when the direct thrombin inhibitor, dabigatran, was approved.52 This was followed the next year by the release of the oral factor Xa inhibitor, rivaroxiban.
Vitamin K Antagonists (warfarin)
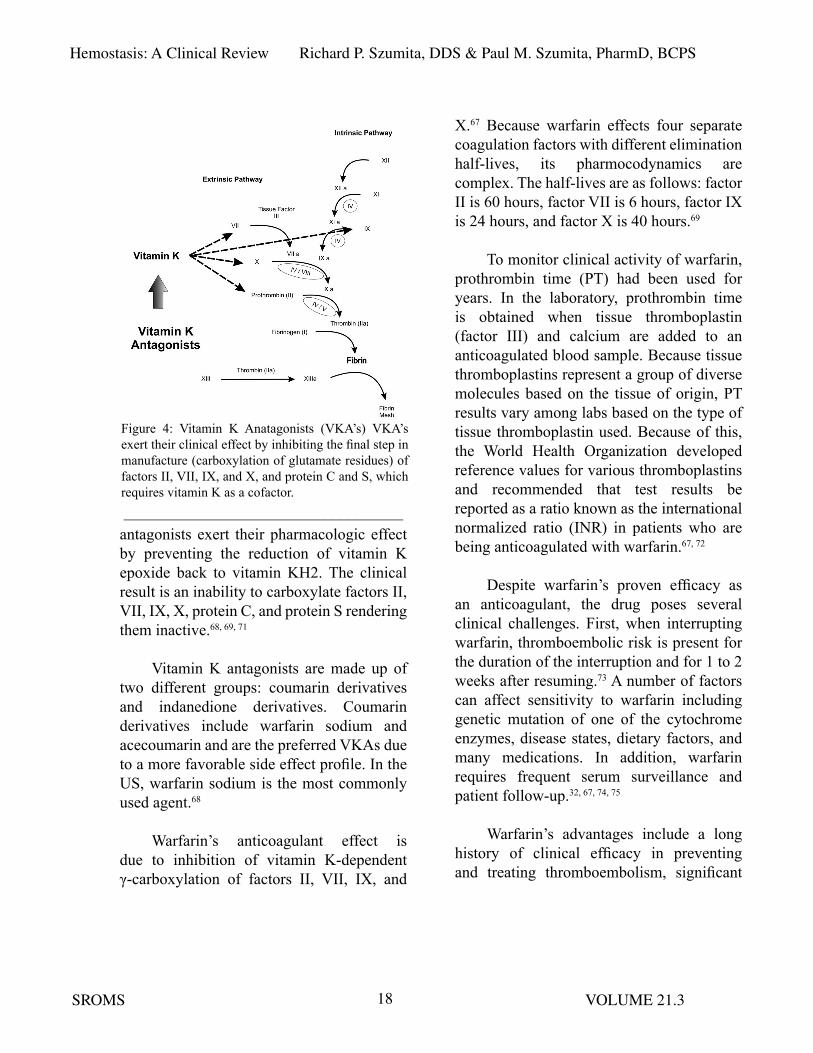
Vitamin K is required for proper synthesis of a number of proteins related to hemostasis (i.e., factors II, VII, IX, X, protein C, and protein S.) (Fig. 4, on P. 17) These proteins are synthesized by ribosomes in hepatocytes and immediately after formation contain glutamate residues. To complete synthesis and make the factors biologically active, vitamin K is needed to convert the glutamate residues to γ-carboxyglutamate. Without this conversion, the factors remain biologically inactive.68, 69
Vitamin K cycles between reduced and oxidized forms. The reduced form (vitamin KH2) acts as the coenzyme for carboxylase. The oxidation of vitamin KH2 to vitamin K epoxide (vitamin KO) provides the energy required for the γ-carboxylation. Vitamin K
Adapted from: Tarascon Pocket Pharmacopoeia, Jones & Bartlett Publishing and USBMIS, Inc.2013.
Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.318
antagonists exert their pharmacologic effect by preventing the reduction of vitamin K epoxide back to vitamin KH2. The clinical result is an inability to carboxylate factors II, VII, IX, X, protein C, and protein S rendering them inactive.68, 69, 71
Vitamin K antagonists are made up of two different groups: coumarin derivatives and indanedione derivatives. Coumarin derivatives include warfarin sodium and acecoumarin and are the preferred VKAs due to a more favorable side effect profile. In the US, warfarin sodium is the most commonly used agent.68
Warfarin’s anticoagulant effect is due to inhibition of vitamin K-dependent γ-carboxylation of factors II, VII, IX, and
X.67 Because warfarin effects four separate coagulation factors with different elimination half-lives, its pharmocodynamics are complex. The half-lives are as follows: factor II is 60 hours, factor VII is 6 hours, factor IX is 24 hours, and factor X is 40 hours.69
To monitor clinical activity of warfarin, prothrombin time (PT) had been used for years. In the laboratory, prothrombin time is obtained when tissue thromboplastin (factor III) and calcium are added to an anticoagulated blood sample. Because tissue thromboplastins represent a group of diverse molecules based on the tissue of origin, PT results vary among labs based on the type of tissue thromboplastin used. Because of this, the World Health Organization developed reference values for various thromboplastins and recommended that test results be reported as a ratio known as the international normalized ratio (INR) in patients who are being anticoagulated with warfarin.67, 72
Despite warfarin’s proven efficacy as an anticoagulant, the drug poses several clinical challenges. First, when interrupting warfarin, thromboembolic risk is present for the duration of the interruption and for 1 to 2 weeks after resuming.73 A number of factors can affect sensitivity to warfarin including genetic mutation of one of the cytochrome enzymes, disease states, dietary factors, and many medications. In addition, warfarin requires frequent serum surveillance and patient follow-up.32, 67, 74, 75
Warfarin’s advantages include a long history of clinical efficacy in preventing and treating thromboembolism, significant
Figure 4: Vitamin K Anatagonists (VKA’s) VKA’s exert their clinical effect by inhibiting the final step in manufacture (carboxylation of glutamate residues) of factors II, VII, IX, and X, and protein C and S, which requires vitamin K as a cofactor. ___________________________________
Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.319
volume of clinical data available to help guide the perioperative management of patients, and accumulation of clinical experience from years of use. Despite complex pharmacodynamics and a narrow therapeutic window with respect to international normalized ratio (INR), vitamin K antagonists have proven efficacious over a wide variety of thrombotic disorders.68
Heparin
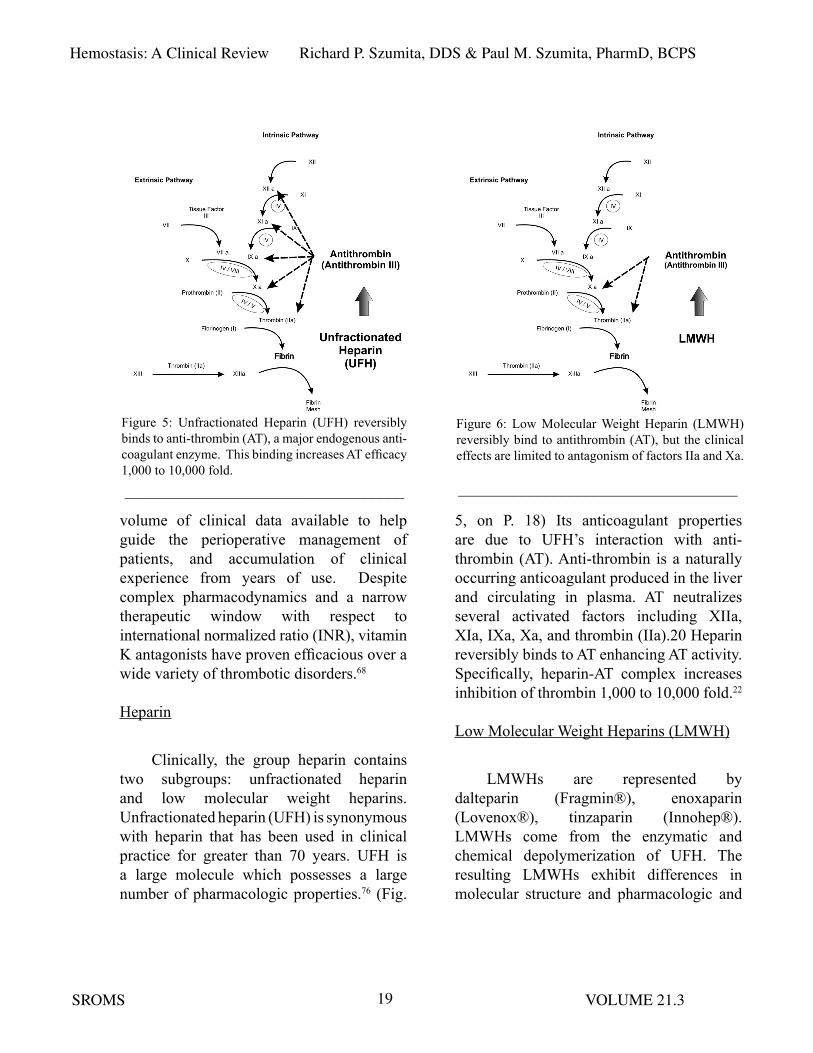
Clinically, the group heparin contains two subgroups: unfractionated heparin and low molecular weight heparins. Unfractionated heparin (UFH) is synonymous with heparin that has been used in clinical practice for greater than 70 years. UFH is a large molecule which possesses a large number of pharmacologic properties.76 (Fig.
5, on P. 18) Its anticoagulant properties are due to UFH’s interaction with anti-thrombin (AT). Anti-thrombin is a naturally occurring anticoagulant produced in the liver and circulating in plasma. AT neutralizes several activated factors including XIIa, XIa, IXa, Xa, and thrombin (IIa).20 Heparin reversibly binds to AT enhancing AT activity. Specifically, heparin-AT complex increases inhibition of thrombin 1,000 to 10,000 fold.22
Low Molecular Weight Heparins (LMWH)
LMWHs are represented by dalteparin (Fragmin®), enoxaparin (Lovenox®), tinzaparin (Innohep®). LMWHs come from the enzymatic and chemical depolymerization of UFH. The resulting LMWHs exhibit differences in molecular structure and pharmacologic and
Figure 5: Unfractionated Heparin (UFH) reversibly binds to anti-thrombin (AT), a major endogenous anti-coagulant enzyme. This binding increases AT efficacy 1,000 to 10,000 fold. ___________________________________
Figure 6: Low Molecular Weight Heparin (LMWH) reversibly bind to antithrombin (AT), but the clinical effects are limited to antagonism of factors IIa and Xa.
___________________________________

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.320
functional properties. Therefore, each of the LMWHs available in clinical practice are developed for a given indication and cannot be used interchangeably.76 However, as a group, LMWHs demonstrate the same pharmacologic activity by inactivating Xa and thrombin. (Fig. 6) LMWHs have been utilized as bridging agents when warfarin is interrupted because they can be administered by subcutaneous injection in an outpatient setting.
Factor Xa Inhibitors
There are two major classes of Xa inhibitors, indirect and direct. Indirect factor Xa inhibitors bind to antithrombin (AT), in a way similar to heparin and LMWH, and inhibit factor Xa via this complex. (Fig. 7 on P. 19)
The molecular structure of indirect factor Xa inhibitors contains the first five monomeric sugars of heparin and LMWH’s. Because of this five-sugar chain, these Xa inhibitors are also referred to as pentasaccharide factor Xa inhibitors. 76-79
Direct factor Xa inhibitors directly bind to FXa, reversibly and competitively blocking its effect. However, they are not structurally similar to heparin and do not have a pentasaccharide structure. Unlike heparin and LMWH, factor Xa inhibitors have no effect on thrombin.77-84
Fondaparinux (Arixtra®) is the only available indirect Xa inhibitor currently on the US market. Fondaparinux has been on the marketavailable since 2001, and is available only as a subcutaneous injection (i.e., similar to LMWH). It is indicated for the prophylaxis of deep vein thrombosis (VTE) in patients undergoing hip fracture surgery, hip replacement surgery, knee replacement surgery or abdominal surgery. Fondaparinux is also indicated for the treatment of acute deep vein thrombosis and acute pulmonary embolism when administered in conjunction with warfarin sodium.79, 85-88
Rivaroxaban (Xarelto®) and apixaban (Eliquis®) are the only currently available direct Xa inhibitors on the US market. Both of these medications recently were approved for use in the US and are both only available in an oral formulation. 89, 90
Rivaroxaban and Apixaban have FDA labeled indications to reduce the risk of stroke and systemic embolism in patients with non-valvular atrial fibrillation. Rivaroxaban has
Figure 7: Factor Xa Inhibitors Indirect factor Xa inhibitors reversibly bind to antithrombin (AT), which then antagonizes factor Xa. Direct factor Xa inhibi-tors do not require interaction with AT. Their clinical effect is with direct, reversible binding to factor Xa.___________________________________

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.321
the additional indication of prophylaxis of deep vein thrombosis (DVT), which may lead to pulmonary embolism (PE) in patients undergoing knee or hip replacement surgery. They are both being investigated for the management of VTE treatment. 80, 91-99
There are several advantages of the new oral direct Xa inhibitors including an alternative to warfarin for the prevention of arterial thrombus due to non-valvular atrial fibrillation, a fixed dosage, less potential for pharmacogenetic variability compared to warfarin, predicable pharmacodynamics and kinetics that do not require monitoring with an anticoagulation laboratory test. 100
Their disadvantages include limited clinical experience, no direct reversal agent if a patient has a life threatening bleed,
unknown clinical consequences if a few doses are missed (due to their relatively short duration of action), and no clear laboratory test to measure the amount of anticoagulation. Abrupt discontinuation, even for a short period of time, may lead to thrombosis, which is particularly important when interruptions of anticoagulants are considered preoperatively. The prescriber of the anticoagulant should be consulted when any regimen interruption is being considered. 48, 78, 101-106
Direct Thrombin Inhibitors (DTI)
Direct thrombin inhibitors (DTI) directly inhibit thrombin (factor IIa) preventing the conversion from fibrinogen to fibrin. (Fig. 8) Several DTIs have been on the market for years in an IV form, bivalirudin, argatroban, and lepirudin (recently taken off the US market). These IV DTIs are used to treat prevent and treat thrombosis secondary to heparin-induced thrombocytopenia and in the acute management of acute coronary syndrome (ACS) undergoing percutaneous coronary intervention (PCI) in the hospital setting as an alternative to IIB/IIIA inhibitors and heparin.107-112
Dabigatran (Pradaxa®), approved by the FDA in July, 2010, was the first non-warfarin oral anticoagulant on the US market. Dabigatran is an orally available DTI with the FDA labeled indication for prevention of stroke in patients with non-valvular atrial fibrillation. The FDA has a specific recommendation against the use of dabigatran in patients with mechanical heart valves. Dabigatran It is also being studied in VTE treatment and VTE prevention in
Figure 8: Direct Thrombin Inhibitors (DTI’s) DTI’s reversibly bind to and antagonize thrombin (factor IIa).
___________________________________

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.322
orthopedic surgery patients.70, 78, 94, 113-119
Similar to the oral factor Xa inhibitors, oral DTIs have several advantages over warfarin, including a fixed dosage, no need for routine laboratory monitoring, limited drug-drug interactions, less potential for pharmacogenetic variability compared to warfarin, potentially more cost-effective than warfarin, and a relatively short half life.92, 100,
113, 120, 121
Disadvantages of dabigatran (also similar to the Factor Xa inhibitors) are limited clinical experience, no direct reversal agent if patient has a life threatening bleed, unknown clinical consequences if a few doses are missed (due to its relative short duration of action), no clear laboratory test to determine the level of anticoagulation, and it has a relatively high incidence of gastrointestinal upset. The prescriber of the anticoagulant should be consulted when any regimen interruption is being considered.78, 84,
101, 103, 122, 123
fibrinolysis
Once a clot is formed, it will need to be cleared after hemostasis has been achieved in order to restore vessel integrity and allow tissue healing. The body’s natural fibrinolytic enzyme is plasmin. Plasmin is a proteolytic enzyme that degrades fibrin as well as the procoagulant factors fibrinogen (I), prothrombin (II), and factors V, VIII, XII.3 Plasmin is formed upon activation of plasminogen. Plasminogen circulates in blood and becomes trapped within the developing
thrombus. Activation of plasminogen then occurs primarily via tissue plasminogen activator (tPA). tPA is produced in, and released from, endothelial cells and is mainly responsible for the lysing of clots in vessels.
A second endogenous activator is urinary plasminogen activator, uPA, which is often referred to as urokinase. Urokinase (uPA) is produced by the kidney and was originally found in the urine but later noted in plasma and other cell types.124
Regulation of fibrinolysis is primarily through α2-antiplasmin, circulating in blood, and plasminogen activator inhibitor-1 (PAI-1) released from endothelial cells.124 Plasminogen activator inhibitor-2 (PAI-2) also exists but is a less potent inhibitor of fibrinolysis. It is generally not circulating in blood except in pregnancy and in association with certain neoplasms.125
Pharmacologic manipulations of the fibrinolytic system are used clinically. Fibrinolytic agents digest and dissolve arterial and venous thrombi and emboli. Fibrinolytic agents are administered intravenously and have been used in the treatment of thromboembolic strokes, myocardial infarction, and other acute thrombo-occlusive disease.126 Current advanced cardiac life support (ACLS) guidelines include the administration of fibrinolytic therapy for patients who meet the inclusion criteria and are suffering from a thromboembolic stroke or diagnosed with a posterior wall MI.127 Examples of these “clot busting” drugs include: rtPA (recombinant form of tissue plasminogen activator), streptokinase,

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.323
reteplase, and tenecteplase.
Pharmacologic agents to antagonize fibrinolysis are also available. Tranexamic acid (Cyklokapron®) and ε-aminocaproic acid (EACA, Amicar®) are antifibrinolytic agents that have been employed in oral and maxillofacial surgery as adjuncts in treating patients with bleeding disorders or in procedures with significant blood loss.128-131 Both drugs competitively inhibit plasminogen binding sites, decreasing plasmin formation and fibrinolysis.
Antifibrinolytics are not effective in obtaining initial hemostasis. However, they stabilize the formed clot by preventing clot lysis once hemostasis has been achieved. These agents have proven particularly effective as adjunctive treatments in maintaining hemostasis of the oral and nasal mucosa in patients with congenital coagulation disorders.132 Aminocaproic acid can be administered parenterally and orally. Tranexamic acid is administered intravenously or topically as an oral rinse.
toPiCal agents foR Hemostasis
In managing patients with disorders of hemostasis, the use of local therapies is common. Local therapies have been discussed extensively in the literature. A recent thorough review was provided by Aldridge and Cunningham and readers are encouraged to review this source.133 A synopsis of local therapies is reviewed here.
Careful surgical planning and execution should be considered as effective local
deterrents to surgical site bleeding and should include prevention of excessive soft tissue trauma, removal of hyperemic inflammatory tissue, control of obvious bony bleeding prior to wound closure, careful suturing, and application of surgical site pressure. Aside from the standard practice of wound packing with gauze, surgical site pressure can also be achieved with dentures and surgically created stents, when indicated.
Adjuncts to surgical manipulation include socket and wound packing agents. Oxidized regenerated cellulose (Surgicel®, Oxycel®), gelatin sponge (Gelfoam®), and collagen-based products (microfibrillar collagen and collagen-based matrices) have all been used with success in oral and maxillofacial surgery. These agents are able to activate coagulation locally. In addition, topical thrombin, used either alone or in combination with a gelatin sponge, has proven effective. However, adding thrombin to oxidized regenerated cellulose or microfibrillar collagen is not recommended as the low pH of these products inactivates thrombin.133
Tranexamic acid has been shown to be efficacious as a topical agent and mouth rinse in patients undergoing dental extractions.131,
134, 135 In orthognathic surgery, however, topical use of tranexamic acid in irrigation fluid did not show reduced blood loss in one study, although pre-operative intravenous administration use did reduce intra-operative blood loss in another study.35,136 Tranexamic acid is approximately 6 to 10 times more potent than ε-aminocaproic acid (EACA). This difference may account for discrepancies

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.324
table 5: antitHRombotiC mediCations: oRalgeneric name Proprietary name action
antiplatelet medicationsAcetylsalicylic acid Aspirin COX InhibitionClopidogrel Plavix® ADP Receptor InhibitionPrasugrel Effient® ADP Receptor AntagonistTicagrelor Brilinta® ADP Receptor AntagonistCilostazol Pletal Phosphodiesterase InhibitorDipyridimole Persantine Adenosine Reuptake InhibitorAcetylsalicylic acid + dipyridimole
Aggrenox® See Above
anticoagulant medicationsWarfarin, Coumadin®,
Jantoven®Vitamin K Antagonist
Rivaroxaban Xarelto® Factor Xa InhibitorApixaban Eliquis® Factor Xa InhibitorDabigatran Pradaxa® Direct Thrombin Inhibitor
Adapted form: Tarascon Pocket Pharmacopoeia, Jones & Bartlett Publishing and USBMIS, Inc. 2013_____________________________________________________________________________in the clinical efficacy of tranexamic acid versus EACA as a mouth rinse. In one report, EACA use as a topical agent was questioned due to lack of data supporting its efficacy.133 In another report, although limited data was noted, a modest benefit was said to justify its use in cases where tranexamic acid is unavailable.135 Neither product is manufactured as a mouth rinse. However, each can be compounded into a topical form upon request.
Fibrin sealants, whether autogenous, an allograft, or commercial product, have multiple clinical uses, including local control of bleeding.137 Tissue glue, n-butyl-2-cyanoacrylate, has been successfully used topically as a surgical wound dressing and control of bleeding.29 Other topical dressings
have been employed with efficacy including freeze-dried chitosan wound dressing.39
PatHologiC tHRombosis
Although pathologic thromboses represent a very diverse spectrum of diseases and clinical manifestations, a brief review of a few pertinent clinical concepts are reviewed.
arterial thromboemolism (ate) versus venous thromboembolism (vte)
Thrombosis is the leading cause of morbidity and mortality in the Western world.138 However, not all thromboses are alike. Arterial thromboemolism (ATE) is responsible for myocardial infarction and stroke. ATE’s are often termed “white clots”

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.325
because they are platelet-rich and fibrin-poor. They usually form at the site of vascular injury and disturbed (i.e., elevated sheer stress) blood flow. The treatment and prevention of ATE’s is generally antiplatelet therapy. Anticoagulants are sometimes employed because thrombin is present.
In venous thromboembolism (VTE), the thrombi are composed primarily of red cells trapped within fibrin mesh. These thrombi are fibrin-rich and platelet-poor and are referred to as “red clots.” They generally tend to occur under conditions of reduced blood flow (i.e., stasis) and activated coagulation proteins. Treatment and prevention of VTE’s are with anticoagulants. VTE’s include deep venous thrombosis (DVT), pulmonary embolism (PE), and emboli from atrial fibrillation.138,139
Coronary artery stents
Special considerations are taken in patients with endovascular coronary artery stents. Percutaneous coronary interventions (PCI) have become the most frequently performed therapeutic procedures in medicine. PCI has evolved from balloon angioplasty, to placement of bare metal stents (BMS), to placement of drug-eluting stents (DES). Balloon angioplasty was complicated by early vessel closure and restenosis. This led to the development and use of bare metal stents designed to maintain patency of the coronary artery lumen. BMS’s were found to cause intimal hyperplasia and restenosis in approximately one third of patients. To combat this, drug-eluting stents were designed to release antiproliferative agents in order to decrease intimal hyperplasia, decreasing restenosis.140 Currently, coronary
stents are used in the vast majority of PCI’s due to increased success rates and decreased arterial restenosis.141
However, with the use of coronary stents, there is risk of stent thrombosis. Bare metal stents require approximately 4 to 6 weeks to re-endothelialize, while drug-eluting stents require approximately 12 months. Antiplatelet therapy, especially dual antiplatelet therapy, has been successful in preventing stent thrombosis. Discontinuing antiplatelet therapy prior to reendothelialization is extremely risky.141
Risk of stroke in atrial fibrillation
Atrial fibrillation is associated with a risk of ischemic stroke. However, the risk of stroke varies across different groups of patients with atrial fibrillation. Treatment recommendations for prevention of stroke range from no treatment in low risk patients to indefinite anticoagulation in higher risk patients.142 Stroke risk is not solely due to the presence of atrial fibrillation but also from associated cardiovascular diseases such as hypertension, coronary artery disease, congestive heart failure, diabetes, and others.143 Several risk stratification schemes have been reported in the literature to guide the physician in recommending treatment. One scheme is the CHADS2 score. CHADS2 refers to: (C) recent congestive heart failure, (H) hypertension, (A) age, (D) diabetes mellitus, (S) history of stroke, and (S) history of TIA. A CHADS2 score of 0 carries a 1.9% risk of stroke, whereas a score of 6 carries an 18.2% risk. Treatment recommendations for patients with atrial fibrillation are based on multiple individual factors including risk

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.326
stratification analysis.144
Risk of thrombosis when antithrombotics are interrupted/discontinued
Consideration of risk versus benefit is a mainstay in dental and medical practice. The risk/benefit balance to consider when performing oral surgical procedures on patients being treated with antithrombotic therapy are:
• First, consider the risk of surgical site bleeding versus the benefit of protecting the patient from a pathologic thrombus/embolus if antithrombotic treatment is maintained.
• Second, evaluate the risk of a pathologic thrombus/embolus versus the benefit of decreased risk of surgical site bleeding if antithrombotic treatment is interrupted.
The general consensus in the literature is that the risk of a thrombus/embolus when interrupting warfarin, aspirin, or aspirin with clopidogrel (Plavix®) therapy is low but the consequences are devastating. Likewise, when warfarin, aspirin, or aspirin with clopidogrel therapy is maintained at therapeutic levels for minor oral surgical procedures, there is a risk of surgical site hemorrhage; however, the consequences are minor because any bleeding is almost always controllable with local measures.38,40,44,145-151
Therefore, when patients are being managed with aspirin or aspirin with clopidogrel and minor oral surgical procedures are planned, the literature
supports maintaining these antiplatelet medications and utilizing local measures to assure hemostasis. Furthermore, in patients being managed with warfarin for whom minor oral surgical procedures are planned, it would seem prudent to maintain warfarin (if INR < 3.5) and utilize local measures to aid in achieving hemostasis.31,33,36,38,40,43-45,49,133,152
Despite the guidance provided by the literature, questions remain. The primary question is: how do the newer antithrombotics compare to the established agents? Excellent reviews of the newer agents are being published, but it will be some time before data is accumulated on the impact these medications have on clinical practice.48,101 Evidence-based conclusions and recommendations from studies on established antithrombotic medications should not be blindly extrapolated to include the newer agents.
As an example, studies on the affect dual antiplatelet therapy has on post-operative bleeding have primarily been with aspirin and clopidogrel (Plavix®). Despite having a similar mechanism of action, it should not be assumed that substituting the newer platelet inhibitors (e.g., prasugrel (Effient®) or ticagrelor (Brilinta®)) for clopidogrel (Plavix®) will yield similar results.
Moreover, the newer oral anticoagulants cannot be compared with warfarin. Their mechanisms of action are different and their clinical effects on post-operative bleeding should not be assumed to parallel those of warfarin.
CliniCal ReCommendations

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.327
Clinical management of patients with hematologic pathology requires thorough patient evaluation, careful surgical planning, understanding the pathophysiology of the patient’s hematologic disorder, and discussion and coordination of peri-operative medical interventions with the patient’s hematologist. Clinical management of patients with underlying medical disease requiring pharmacologic antithrombotic intervention also requires a thorough patient evaluation, careful surgical planning, understanding the pathophysiology of the patient’s thrombotic risk, understanding the pharmacology of their antithrombotic therapy, assessment of surgical bleeding risk, and discussion of peri-operative antithrombotic treatment strategies with the patient’s treating physician, when appropriate. In both scenarios, it is also important to execute the planned surgery with precision and utilize local hemostatic adjuncts when appropriate.
Because of the complexity and variability of the disease states and medication effects encountered in clinical practice, there is no doubt that individualizing treatment for every patient is important.45,153 However, published guidelines can provide valuable assistance to the oral and maxillofacial surgeon when devising treatment strategies and discussing peri-operative care with our colleagues. The following guidelines have been pulled from referenced sources that highlight general principles of peri-operative management strategies for patients on antithrombotic medications.
The American College of Chest Physicians has published evidence-based
clinical practice guidelines in the journal Chest.103 Brief summaries of pertinent recommendations from this publication are listed below. The reader is also strongly encouraged to review the source paper for a complete listing of recommendations and for detailed explanations.
1. In patients who are receiving acetylsalicylic acid (ASA) for the secondary prevention of cardiovascular disease and are having minor dental or dermatologic procedures or cataract surgery, we suggest continuing ASA around the time of the procedure instead of stopping ASA 7 to 10 days before the procedure.
2. In patients with a coronary stent who are receiving dual antiplatelet therapy and require surgery, we recommend deferring surgery for at least 6 weeks after placement of a bare-metal stent and for at least 6 months after placement of a drug-eluting stent instead of undertaking surgery within these time periods.
3. In patients who require surgery within 6 weeks of placement of a bare-metal stent or within 6 months of placement of a drug-eluting stent, we suggest continuing dual antiplatelet therapy around the time of surgery instead of stopping dual antiplatelet therapy 7 to 10 days before surgery.
4. In patients who require a minor dental procedure, we suggest continuing vitamin K antagonists (VKAs) with coadministration of an oral prohemostatic agent or stopping

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.328
VKAs 2 to 3 days before the procedure instead of alternative strategies.
5. In patients who require temporary interruption (i.e., for major oral surgery) of a VKA before surgery, we recommend stopping VKAs approximately 5 days before surgery instead of stopping VKAs a shorter time before surgery.
6. In patients who require temporary interruption of a VKA before surgery, we recommend resuming VKAs approximately 12 to 24 h after surgery (evening of or next morning) and when there is adequate hemostasis instead of later resumption of VKAs.
7. In patients with a mechanical heart valve, atrial fibrillation, or VTE at high risk for thromboembolism, we suggest bridging anticoagulation instead of no bridging during interruption of VKA therapy.
8. In patients with a mechanical heart valve, atrial fibrillation, or VTE at low risk for thromboembolism, we suggest no bridging instead of bridging anticoagulation during interruption of VKA therapy.
In the clinical guidelines published in Chest, the newer oral anticoagulants (factor Xa inhibitors and direct thrombin inhibitor) have not yet been included. However, guidelines for the peri-operative management of the oral direct thrombin inhibitor, dabigatran, have been published by van Ryn, et al,116 and can be summarized as follows:
• In patients with standard surgical bleeding risks and normal renal
function, discontinuing dabigatran for 24 hours prior to surgery is recommended.
• For patients with high surgical bleeding risks and normal renal function, discontinuing dabigatran for 2-4 days is recommended.
• In patients with declining renal function, the times of cessation prior to surgery are increased.
Future recommendations will no doubt include expanded data on peri-operative oral anticoagulant use and alterations in bridging strategies. Additionally, the effect of various antiplatelet regimens on surgical bleeding risk will be better defined.
ConClUsions
Bleeding risks in oral and maxillofacial surgery are many and varied. Bleeding can occur from a local derangement of hemostasis, injury to a vessel too large for spontaneous hemostasis, inherited or acquired pathologies of hemostasis, and pharmacologic alteration of thrombin formation. Local surgical site interventions will lead to bleeding cessation of local disturbances and may control the others. Vessel control at the surgical site, or proximally when necessary, will afford control of hemorrhage of large-vessel bleeding when local management is ineffective. Along with surgical site interventions, systemic therapies will often be required in pathologies of hemostasis (i.e. vWD, hemophilias, cirrhosis, severe thrombocytopenia, etc.). In pharmacologic alterations of hemostasis, the goal of the prescriber is to balance the prevention of pathologic thrombosis while maintaining physiologic hemostasis.

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.329
Unfortunately, this “balance” varies among patients and among surgical procedures making it difficult to create a “cookbook” approach to peri-operative management. The complexity of the topic is further highlighted when one considers the diversity of procedures performed. With dental extractions alone, there is considerable variation in surgical manipulation and bleeding risk, ranging from single tooth extractions to multiple deep impactions, where even “routine” dental extractions are known to challenge the hemostatic mechanisms.17 With intraoral surgery and other superficial procedures, advantages include the ability to monitor post-operative bleeding and to gain immediate access for surgical site interventions. However, these local interventions may be insufficient to control bleeding when physiologic hemostasis has been significantly altered. So, in patients on antithrombotic therapy, the clinical “balances” which should be considered are:
1) the bleeding risks associated with the proposed surgical procedures,
2) the thrombotic risks associated with the systemic disease, and
3) the likelihood the prescribed antithrombotic medications (whether therapeutic or hyper-therapeutic) causes
sufficient disruption of physiologic hemostasis to render surgical site interventions ineffective.
It is our responsibility as the treating surgeon to evaluate these parameters in order to provide our patients with minimal surgical complications without exposing them to unnecessary and possibly dangerous periods of antithrombotic interruption. To complicate matters, this must also be accomplished in a clinical environment where the numbers and types of antithrombotic medications are rapidly expanding, the population is aging, and multiple medical conditions exist which rely on antithrombotics for treatment and prevention of thromboembolic complications.
Understanding the pathophysiology of conditions for which patients are treated with antithrombotic medications, knowing the pharmacology and impact these medications have on hemostasis, and stratifying procedural bleeding risks should help the oral and maxillofacial surgeon individualize peri-operative management strategies to complete surgical treatment safely and effectively. This knowledge should also guide the oral and maxillofacial surgeon when discussing peri-operative care with their patients’ treating physicians, when appropriate.
Richard P. szumita, DDS received his dental degree at Case Western Reserve University School of Dentistry. Post-graduate training included a general practice residency at the VAMC Cleveland, Ohio, and oral and maxillofacial surgery residency at the VAMC, East Orange, New Jersey. Currently, Rick is Associate Chairman, Department of Dentistry and Associate Program Director for oral and maxillofacial surgery residency

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.330
REFERENCES
1. Macik BG: Hemostasis. IN: Moylan JA (ed.) Surgical Critical Care St. Louis: Mosby-Year Book, Inc.; 1994, pp. 697-718.
2. Nuyttens BP, Thijs T, Deckmyn H, et al: Platelet adhesion to collagen. Thromb Res Jan 127 (Suppl 2): S26, 2011.
3. Guyton AC and Hall JE: Textbook of Medical Physiology 11th ed. Philadelphia: Elsevier Inc. 2006.
4. Mackman N: The many faces of tissue factor. J Thromb Haemost 7 (Suppl 1): 136, 2009.
5. Heemskerk JW, Mattheij NJ and Cosemans JM: Platelet-based coagulation: different populations, different functions. J Thromb Haemost 11:2, 2013.
6. Calverly DCT and Christiane D: Platelet structure and function in hemostasis and Thrombosis. IN: Greer JP, Foerster J, Rodgers GM, et al. (eds.) Wintrobe’s Clinical Hematology Vol 1 Philadelphia: Lippincott Williams & Wilkins; 2009.
7. Angiolillo DJ, Capodanno D and Goto S: Platelet thrombin receptor antagonism and atherothrombosis. Eur Heart J 31: 17, 2010.
8. Davi G and Patrono C: Platelet activation and atherothrombosis. N Engl J Med 357: 2482, 2007.
9. Wagner DD and Ginsburg D: Structure, biology, and genetics of von Willebrand Factor. IN: Hoffman R, Benz EJ Jr, Shattil SJ, et al, (eds.) Hematology Basic Principles and Practice. 2nd ed. New York: Churchill Livingstone Inc; 1995 pp. 1717-1725.
10. Nieswandt B, Pleines I and Bender M: Platelet adhesion and activation mechanisms in arterial thrombosis and ischaemic stroke. J Thromb Haemost 9 (Suppl 1): 92, 2011.
11. Marx RE: Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg 62: 489, 2004.
12. Marx RE, Carlson ER, Eichstaedt RM, et al: Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 85: 638, 1998.
13. Freymiller EG and Aghaloo TL: Platelet-rich plasma: ready or not? J Oral Maxillofac Surg 62: 484, 2004.
14. Slapnicka J, Fassmann A, Strasak L, et al: Effects of activated and nonactivated platelet-rich plasma on proliferation of human osteoblasts in vitro. J Oral Maxillofac Surg 66: 297, 2008.
15. Henderson JM, Bergman S, Salama A, et al: Management of the oral and maxillofacial surgery patient with thrombocytopenia. J Oral Maxillofac Surg 59: 421, 2001.
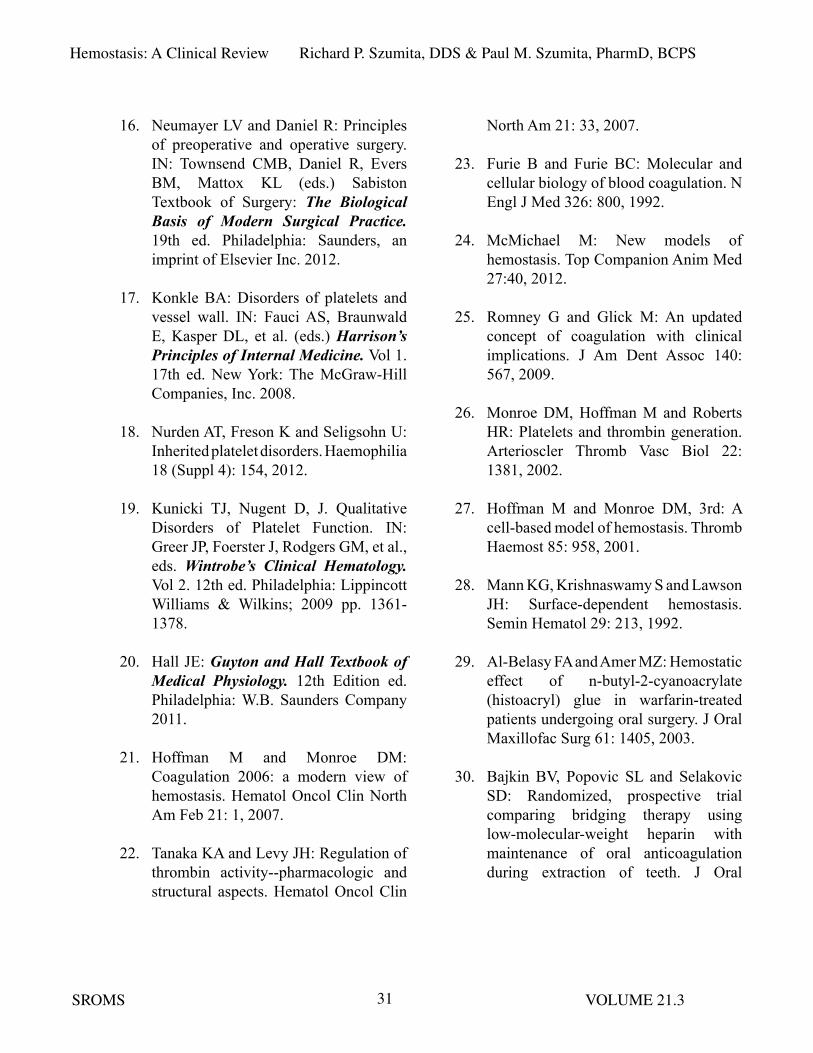
Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.331
16. Neumayer LV and Daniel R: Principles of preoperative and operative surgery. IN: Townsend CMB, Daniel R, Evers BM, Mattox KL (eds.) Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 19th ed. Philadelphia: Saunders, an imprint of Elsevier Inc. 2012.
17. Konkle BA: Disorders of platelets and vessel wall. IN: Fauci AS, Braunwald E, Kasper DL, et al. (eds.) Harrison’s Principles of Internal Medicine. Vol 1. 17th ed. New York: The McGraw-Hill Companies, Inc. 2008.
18. Nurden AT, Freson K and Seligsohn U: Inherited platelet disorders. Haemophilia 18 (Suppl 4): 154, 2012.
19. Kunicki TJ, Nugent D, J. Qualitative Disorders of Platelet Function. IN: Greer JP, Foerster J, Rodgers GM, et al., eds. Wintrobe’s Clinical Hematology. Vol 2. 12th ed. Philadelphia: Lippincott Williams & Wilkins; 2009 pp. 1361-1378.
20. Hall JE: Guyton and Hall Textbook of Medical Physiology. 12th Edition ed. Philadelphia: W.B. Saunders Company 2011.
21. Hoffman M and Monroe DM: Coagulation 2006: a modern view of hemostasis. Hematol Oncol Clin North Am Feb 21: 1, 2007.
22. Tanaka KA and Levy JH: Regulation of thrombin activity--pharmacologic and structural aspects. Hematol Oncol Clin
North Am 21: 33, 2007.
23. Furie B and Furie BC: Molecular and cellular biology of blood coagulation. N Engl J Med 326: 800, 1992.
24. McMichael M: New models of hemostasis. Top Companion Anim Med 27:40, 2012.
25. Romney G and Glick M: An updated concept of coagulation with clinical implications. J Am Dent Assoc 140: 567, 2009.
26. Monroe DM, Hoffman M and Roberts HR: Platelets and thrombin generation. Arterioscler Thromb Vasc Biol 22: 1381, 2002.
27. Hoffman M and Monroe DM, 3rd: A cell-based model of hemostasis. Thromb Haemost 85: 958, 2001.
28. Mann KG, Krishnaswamy S and Lawson JH: Surface-dependent hemostasis. Semin Hematol 29: 213, 1992.
29. Al-Belasy FA and Amer MZ: Hemostatic effect of n-butyl-2-cyanoacrylate (histoacryl) glue in warfarin-treated patients undergoing oral surgery. J Oral Maxillofac Surg 61: 1405, 2003.
30. Bajkin BV, Popovic SL and Selakovic SD: Randomized, prospective trial comparing bridging therapy using low-molecular-weight heparin with maintenance of oral anticoagulation during extraction of teeth. J Oral

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.332
Maxillofac Surg 67: 990, 2009.
31. Beirne OR: Evidence to continue oral anticoagulant therapy for ambulatory oral surgery. J Oral Maxillofac Surg 63: 540, 2005.
32. Brooks AS: Delayed complications of tooth extraction in patients taking warfarin, antibiotics, and other medications. J Oral Maxillofac Surg 69: 977, 2011.
33. Ferrieri GB, Castiglioni S, Carmagnola D, et al: Oral surgery in patients on anticoagulant treatment without therapy interruption. J Oral Maxillofac Surg 65: 1149, 2007.
34. Hong CH, Napenas JJ, Brennan MT, et al: Frequency of bleeding following invasive dental procedures in patients on low-molecular-weight heparin therapy. J Oral Maxillofac Surg 68: 975, 2010.
35. Kaewpradub P, Apipan B and Rummasak D: Does tranexamic acid in an irrigating fluid reduce intraoperative blood loss in orthognathic surgery? A double-blind, randomized clinical trial. J Oral Maxillofac Surg 69: e186, 2011.
36. Karsli ED, Erdogan O, Esen E, et al: Comparison of the effects of warfarin and heparin on bleeding caused by dental extraction: a clinical study. J Oral Maxillofac Surg 69: 2500, 2011.
37. Krishnan B, Shenoy NA and Alexander
M: Exodontia and antiplatelet therapy. J Oral Maxillofac Surg 66: 2063, 2008.
38. Madan GA, Madan SG, Madan G, et al: Minor oral surgery without stopping daily low-dose aspirin therapy: a study of 51 patients. J Oral Maxillofac Surg 63: 1262, 2005.
39. Malmquist JP, Clemens SC, Oien HJ, et al: Hemostasis of oral surgery wounds with the HemCon Dental Dressing. J Oral Maxillofac Surg 66: 1177, 2008.
40. Medeiros FB, de Andrade AC, Angelis GA, et al: Bleeding evaluation during single tooth extraction in patients with coronary artery disease and acetylsalicylic acid therapy suspension: a prospective, double-blinded, and randomized study. J Oral Maxillofac Surg 69: 2949, 2011.
41. Morimoto Y, Niwa H, Hanatani A, et al: Hemostatic management during oral surgery in patients with a left-ventricular assist system undergoing high-level anticoagulant therapy: efficacy of low molecular weight heparin. J Oral Maxillofac Surg 66: 568, 2008.
42. Morimoto Y, Niwa H and Minematsu K: Risk factors affecting hemorrhage after tooth extraction in patients undergoing continuous infusion with unfractionated heparin. J Oral Maxillofac Surg 70: 521, 2012.
43. Morimoto Y, Niwa H and Minematsu K: Hemostatic management of tooth extractions in patients on

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.333
oral antithrombotic therapy. J Oral Maxillofac Surg 66: 51, 2008.
44. Partridge CG, Campbell JH and Alvarado F: The effect of platelet-altering medications on bleeding from minor oral surgery procedures. J Oral Maxillofac Surg 66: 93, 2008.
45. Todd DW: Evidence to support an individualized approach to modification of oral anticoagulant therapy for ambulatory oral surgery. J Oral Maxillofac Surg 63: 536, 2005.
46. Todd DW and Roman A: Outpatient use of low-molecular weight heparin in an anticoagulated patient requiring oral surgery: case report. J Oral Maxillofac Surg 59: 1090, 2001.
47. Ward BB and Smith MH: Dentoalveolar procedures for the anticoagulated patient: literature recommendations versus current practice. J Oral Maxillofac Surg 65: 1454, 2007.
48. Firriolo FJ and Hupp WS: Beyond warfarin: the new generation of oral anticoagulants and their implications for the management of dental patients. Oral Surg Oral Med Oral Pathol Oral Radiol 113: 431, 2012.
49. Hong C, Napenas JJ, Brennan M, et al: Risk of postoperative bleeding after dental procedures in patients on warfarin: a retrospective study. Oral
Surg Oral Med Oral Pathol Oral Radiol 114: 464, 2012.
50. FDA. FDA News Release. 2009; http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm171497.htm.
51. FDA. FDA News Release. 2011; http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm263964.htm.
52. FDA. FDA News Release. 2010; http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm230241.htm.
53. FDA. FDA News Release. 2012; http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm333634.htm.
54. Majerus PW and Tollefsen DM: Blood coagulation and anticoagulant, thrombolytic, and antiplatelet drugs. IN: Brunton LL, Lazo JS and Parker KL (eds.) Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 11th ed. New York: The McGraw-Hill Companies, Inc.; 2006, pp. 1467-1488.
55. Eikelboom JW, Hirsh J, Spencer FA, et al: Antiplatelet drugs: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141(2 Suppl):e89S, 2012.
56. Capodanno D, Dharmashankar K and Angiolillo DJ: Mechanism of action and clinical development of ticagrelor,

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.334
a novel platelet ADP P2Y12 receptor antagonist. Expert Rev Cardiovasc Ther 8: 151, 2010.
57. Ferraris VA, Saha SP, Oestreich JH, et al: 2012 update to the Society of Thoracic Surgeons guideline on use of antiplatelet drugs in patients having cardiac and noncardiac operations. Ann Thorac Surg 94: 1761, 2012.
58. Sullivan J and Amarshi N: Dual antiplatelet therapy with clopidogrel and aspirin. Am J Health Syst Pharm 65: 1134, 2008.
59. Riley AB, Tafreshi MJ and Haber SL: Prasugrel: a novel antiplatelet agent. Am J Health Syst Pharm 65: 1019, 2008.
60. Wiviott SD, Braunwald E, McCabe CH, et al: Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 357: 2001, 2007.
61. Momary KM, Dorsch MP and Bates ER: Genetic causes of clopidogrel nonresponsiveness: which ones really count? Pharmacotherapy 30: 265, 2010.
62. Sorich MJ, Vitry A, Ward MB, et al: Prasugrel vs. clopidogrel for cytochrome P450 2C19-genotyped subgroups: integration of the TRITON-TIMI 38 trial data. J Thromb Haemost 8: 1678, 2010.
63. Pare G, Mehta SR, Yusuf S, et al: Effects of CYP2C19 genotype on outcomes of clopidogrel treatment. N Engl J Med
363: 1704, 2010.
64. Bhatt DL: Prasugrel in clinical practice. N Engl J Med 361: 940, 2009.
65. Teng R, Maya J and Butler K: Evaluation of the pharmacokinetics and pharmacodynamics of ticagrelor co-administered with aspirin in healthy volunteers. Platelets Dec 18 [Epub ahead of print] Early Online: 1, 2012.
66. Ferraris VA, Bernard AC and Hyde B: The impact of antiplatelet drugs on trauma outcomes. J Trauma Acute Care Surg 73: 492, 2012.
67. Da Silva MS and Sobel M: Anticoagulants: to bleed or not to bleed, that is the question. Semin Vasc Surg 15: 256, 2002.
68. Pineo GF and Hull RD: Vitamin K antagonists and direct thrombin inhibitors: present and future. Hematol Oncol Clin North Am 19: 69, 2005.
69. O’Reilly RA: Anticoagulant, antithrombotic, and thrombolytic drugs. IN: Gilman AGG, Louis S, Rall TW, et al. (eds.) Goodman and Gilman’s The Pharmacological Basis of Therapeutics. Seventh Edition ed. New York: MacMillan Publishing Company; 1985 pp. 1338-1362.
70. Gums JG: Place of dabigatran in contemporary pharmacotherapy.

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.335
Pharmacotherapy 31: 335, 2011.
71. Furie B and Furie BC: Molecular basis of vitamin K-dependent gamma-carboxylation. Blood 75: 1753, 1990.
72. Beirne OR and Koehler JR: Surgical management of patients on warfarin sodium. J Oral Maxillofac Surg 54: 1115, 1996.
73. Ansell J, Hirsh J, Poller L, et al: The pharmacology and management of the vitamin K antagonists: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 126(3 Suppl): 204S, 2004.
74. Schulman S: Clinical practice. Care of patients receiving long-term anticoagulant therapy. N Engl J Med 349: 675, 2003.
75. Eikelboom JW and Hankey GJ: The beginning of the end of warfarin? Med J Aust 180: 549, 2004.
76. Bick RL, Frenkel EP, Walenga J, et al: Unfractionated heparin, low molecular weight heparins, and pentasaccharide: basic mechanism of actions, pharmacology, and clinical use. Hematol Oncol Clin North Am 19: 1, 2005.
77. Nutescu E, Rhoades R, Bailey C, et al: Apixaban: a novel oral inhibitor of factor Xa. Am J Health Syst Pharm 69: 1113, 2012.
78. Miyares MA and Davis K: Newer oral anticoagulants: a review of laboratory monitoring options and reversal agents in the hemorrhagic patient. Am J Health Syst Pharm 69: 1473, 2012.
79. Decousus H, Prandoni P, Mismetti P, et al: Fondaparinux for the treatment of superficial-vein thrombosis in the legs. N Engl J Med 363: 1222, 2010.
80. Abrams PJ and Emerson CR: Rivaroxaban: a novel, oral, direct factor Xa inhibitor. Pharmacotherapy 29: 167, 2009.
81. Agnelli G, Buller HR, Cohen A, et al: Apixaban for extended treatment of venous thromboembolism. N Engl J Med 368: 699, 2013.
82. Hellwig T and Gulseth M: New oral therapies for the prevention and treatment of venous thromboembolism. Am J Health Syst Pharm 70: 113, 2013.
83. Cohen AT, Spiro TE, Buller HR, et al: Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N Engl J Med 368: 513, 2013.
84. Shamoun FE, Martin EN and Money SR: The novel anticoagulants: The surgeons’ prospective. Surgery 153: 303, 2013.
85. Baroletti S, Labreche M, Niles M, et al: Prescription of fondaparinux in hospitalised patients. Thromb Haemost. 101: 1091, 2009.
86. Buller HR, Davidson BL, Decousus H,

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.336
et al: Subcutaneous fondaparinux versus intravenous unfractionated heparin in the initial treatment of pulmonary embolism. N Engl J Med 349: 1695, 2003.
87. Turpie AG: Fondaparinux: a Factor Xa inhibitor for antithrombotic therapy. Expert Opinion on Pharmacotherapy. 5: 1373, 2004.
88. Turpie AG: The safety of fondaparinux for the prevention and treatment of venous thromboembolism. Expert Opinion on Drug Safety. 4: 707, 2005.
89. Hylek EM: Therapeutic potential of oral factor Xa inhibitors. N Engl J Med 363: 2559, 2010.
90. Bauersachs R, Berkowitz SD, Brenner B, et al: Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 363: 2499, 2010.
91. Buller HR, Prins MH, Lensin AW, et al: Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 366: 1287, 2012.
92. Wittkowsky AK: Novel oral anticoagulants and their role in clinical practice. Pharmacotherapy. 31: 1175, 2011.
93. Patel MR, Mahaffey KW, Garg J, et al: Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 365: 883, 2011.
94. Mega JL: A new era for anticoagulation
in atrial fibrillation. N Engl J Med 365: 1052, 2011.
95. Granger CB, Alexander JH, McMurray JJ, et al: Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 365: 981, 2011.
96. Goldhaber SZ, Leizorovicz A, Kakkar AK, et al: Apixaban versus enoxaparin for thromboprophylaxis in medically ill patients. N Engl J Med 365: 2167, 2011.
97. Connolly SJ, Eikelboom J, Joyner C, et al: Apixaban in patients with atrial fibrillation. N Engl J Med 364: 806, 2011.
98. Lassen MR, Gallus A, Raskob GE, et al: Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N Engl J Med 363: 2487, 2010.
99. Lassen MR, Raskob GE, Gallus A, et al: Apixaban or enoxaparin for thromboprophylaxis after knee replacement. N Engl J Med 361: 594, 2009.
100. Cavallari LH, Shin J and Perera MA: Role of pharmacogenomics in the management of traditional and novel oral anticoagulants. Pharmacotherapy 31: 1192, 2011.
101. Little JW: New oral anticoagulants: will they replace warfarin? Oral Surg Oral Med Oral Pathol Oral Radiol 113: 575, 2012.
102. Patel MR, Hellkamp AS, Lokhnygina

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.337
Y, et al: Outcomes of discontinuing rivaroxaban compared with warfarin in patients with nonvalvular atrial fibrillation: Analysis from the ROCKET AF Trial (Rivaroxaban once-daily, oral, direct factor Xa inhibition compared with Vitamin K antagonism for prevention of stroke and embolism trial in atrial fibrillation). J Amer College Cardiol 61: 651, 2013.
103. Douketis JD, Spyropoulos AC, Spencer FA, et al: Perioperative management of antithrombotic therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141(2 Suppl): e326S, 2012.
104. Garwood CL, Gortney JS and Corbett TL: Is there a role for fondaparinux in perioperative bridging? Am J Health Syst Pharm 68: 36, 2011.
105. Samama MM: Which test to measure the anticoagulant effect of rivaroxaban? The anti-xa assay. J Thromb Haemost: 11: 579, 2013.
106. Tripodi A: Which test to measure the anticoagulant effect of rivaroxaban: The prothrombin time test. JThromb Haemost 11: 576, 2013.
107. Schaden E and Kozek-Langenecker SA: Direct thrombin inhibitors:
pharmacology and application in intensive care medicine. Intensive Care Med 36: 1127, 2010.
108. Saugel B, Phillip V, Moessmer G, et al: Argatroban therapy for heparin-induced thrombocytopenia in ICU patients with multiple organ dysfunction syndrome: a retrospective study. Crit Care 14: R90, 2010.
109. Shantsila E, Lip GY and Chong BH: Heparin-induced thrombocytopenia. A contemporary clinical approach to diagnosis and management. Chest 135: 1651, 2009.
110. Hirsh J, Bauer KA, Donati MB, et al: Parenteral anticoagulants: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 133(6 Suppl): 141S, 2008.
111. Kiser TH, Burch JC, Klem PM, et al: Safety, efficacy, and dosing requirements of bivalirudin in patients with heparin-induced thrombocytopenia. Pharmacotherapy 28: 1115, 2008.
112. Dyke CM, Smedira NG, Koster A, et al: A comparison of bivalirudin to heparin with protamine reversal in patients undergoing cardiac surgery with cardiopulmonary bypass: the EVOLUTION-ON study. J Thorac Cardiovasc Surg 131: 533, 2006.

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.338
113. Mahan CE and Fanikos J: New antithrombotics: the impact on global health care. Thromb Res 127: 518, 2011.
114. Gulseth MP, Wittkowsky AK, Fanikos J, et al: Dabigatran etexilate in clinical practice: confronting challenges to improve safety and effectiveness. Pharmacotherapy 31: 1232, 2011.
115. Wallentin L, Yusuf S, Ezekowitz MD, et al: Efficacy and safety of dabigatran compared with warfarin at different levels of international normalised ratio control for stroke prevention in atrial fibrillation: an analysis of the RE-LY trial. Lancet 376: 975, 2010.
116. van Ryn J, Stangier J, Haertter S, et al: Dabigatran etexilate–a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity. Thromb Haemost 103: 1116, 2010.
117. Friedman RJ, Dahl OE, Rosencher N, et al: Dabigatran versus enoxaparin for prevention of venous thromboembolism after hip or knee arthroplasty: a pooled analysis of three trials. Thromb Res 126: 175, 2010.
118. Baetz BE and Spinler SA: Dabigatran etexilate: an oral direct thrombin inhibitor for prophylaxis and treatment of thromboembolic diseases. Pharmacotherapy 28: 1354, 2008.
119. Van de Werf F, Brueckmann M, Connolly SJ, et al: A comparison of dabigatran etexilate with warfarin in patients with mechanical heart valves: The randomized, phase II study to evaluate the safety and pharmacokinetics of oral dabigatran etexilate in patients after heart valve replacement (RE-ALIGN). American Heart J 163: 931, 2012.
120. Atay JK, Fiumara K, Piazza G, et al: Hospital budget implications of substituting dabigatran for warfarin in an anticoagulation service. Clin Appl Thromb Hemost 18: 181, 2012.
121. Pink J, Lane S, Pirmohamed M, et al: Dabigatran etexilate versus warfarin in management of non-valvular atrial fibrillation in UK context: quantitative benefit-harm and economic analyses. BMJ 343: d6333, 2011.
122. Breik O, Tadros R and Devitt P: Thrombin inhibitors: surgical considerations and pharmacology. ANZ J Surg 83: 215, 2013.
123. Dumkow LE, Voss JR, Peters M, et al: Reversal of dabigatran-induced bleeding with a prothrombin complex concentrate and fresh frozen plasma. Am J Health Syst Pharm 69: 1646, 2012.
124. Takada A, Takada Y and Urano T: The physiological aspects of fibrinolysis. Thromb Res 76: 1, 1994.
125. Shetty S and Idell S: Plasminogen activator and plasmin. IN: Laurent GJ and Shapiro SD, (eds.) Encyclopedia

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.339
of Respiratory Medicine. Oxford: Academic Press; 2006, pp. 205-210.
126. Bell WR. Fibrinolytic therapy: indications and management. IN: Hoffman R, Benz JEJ, Shattil SJ, et al. (eds.) Hematology Basic Principles and Practice. 2nd ed. New York: Churchill and Livingstone Inc.; 1995, pp. 1814-1829.
127. Aehlert B. ACLS Study Guide. 4th ed. St. Louis: Mosby, an imprint of Elsevier Inc.; 2012.
128. Bajkin BV, Rajic NV and Vujkov SB. Dental extraction in a hemophilia patient without factor replacement therapy: a case report. J Oral Maxillofac Surg 70: 2276, 2012.
129. Ramstrom G, Sindet-Pedersen S, Hall G, et al: Prevention of postsurgical bleeding in oral surgery using tranexamic acid without dose modification of oral anticoagulants. J Oral Maxillofac Surg 51: 1211, 1993.
130. Song G, Yang P, Hu J, et al: The effect of tranexamic acid on blood loss in orthognathic surgery: a meta-analysis of randomized controlled trials. Oral Surg Oral Med Oral Pathol Oral Radiol 115: 595, 2013.
131. Carter G, Goss A, Lloyd J, et al: Tranexamic acid mouthwash versus autologous fibrin glue in patients taking
warfarin undergoing dental extractions: a randomized prospective clinical study. J Oral Maxillofac Surg 61: 1432, 2003.
132. Gill JC: Transfusion principles for congenital coagulation disorders. IN: Hoffman R, Benz JEJ, Shattil SJ, et al. (eds.) Hematology Basic Principles and Practice. 2nd ed. New York: Churchill Livingstone Inc.; 1995, pp. 2029-2038.
133. Aldridge E and Cunningham LL, Jr. Current thoughts on treatment of patients receiving anticoagulation therapy. J Oral Maxillofac Surg 68: 2879, 2010.
134. Sindet-Pedersen S, Ramstrom G, Bernvil S, et al: Hemostatic effect of tranexamic acid mouthwash in anticoagulant-treated patients undergoing oral surgery. N Engl J Med 320: 840, 1989.
135. Patatanian E and Fugate SE: Hemostatic mouthwashes in anticoagulated patients undergoing dental extraction. Ann Pharmacother 40: 2205, 2006.
136. Choi WS, Irwin MG and Samman N: The effect of tranexamic acid on blood loss during orthognathic surgery: a randomized controlled trial. J Oral Maxillofac Surg 67: 125, 2009.
137. Fattahi T, Mohan M and Caldwell GT: Clinical applications of fibrin sealants. J Oral Maxillofac Surg 62: 218, 2004.
138. Mackman N and Becker RC: DVT: a new era in anticoagulant therapy. Arterioscler Thromb Vasc Biol 30: 369, 2010.

Hemostasis: A Clinical Review Richard P. Szumita, DDS & Paul M. Szumita, PharmD, BCPS
SROMS VOLUME 21.340
139. Schafer AI: Antiplatelet therapy. Am J Med 101: 199, 1996.
140. Stefanini GG and Holmes DR, Jr: Drug-eluting coronary-artery stents. N Engl J Med 368: 254, 2013.
141. Vaclavik J and Taborsky M: Antiplatelet therapy in the perioperative period. Eur J Intern Med 22: 26, 2011.
142. You J, Singer DE, Howard PA, et al: Antithrombotic therapy for atrial fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141: e531S, 2012.
143. Choudhury A, Chung I, Blann A, et al: Platelet adhesion in atrial fibrillation. Thromb Res 120: 623, 2007.
144. Lip GY and Boos CJ: Antithrombotic treatment in atrial fibrillation. Heart 92: 155, 2006.
145. Bajkin BV, Bajkin IA and Petrovic BB: The effects of combined oral anticoagulant-aspirin therapy in patients undergoing tooth extractions: a prospective study. J Am Dent Assoc 143: 771, 2012.
146. Campbell JH, Alvarado F and Murray RA: Anticoagulation and minor oral surgery: should the anticoagulation regimen be altered? J Oral Maxillofac Surg 58: 131, 2000.
147. Ardekian L, Gaspar R, Peled M, et
al: Does low-dose aspirin therapy complicate oral surgical procedures? J Am Dent Assoc 131: 331, 2000.
148. Wahl MJ: Bleed or die? A bloody simple decision. Oral Surg Oral Med Oral Pathol Oral Radiol 113: 147; author reply 150, 2012.
149. Wahl MJ: Dental surgery in anticoagulated patients. Arch Intern Med 158: 1610, 1998.
150. Ezekowitz MD: Anticoagulation interruptus: not without risk. Circulation 110: 1518, 2004.
151. Aframian DJ, Lalla RV and Peterson DE: Management of dental patients taking common hemostasis-altering medications. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 103(Suppl:S45): e41, 2007.
152. Napenas JJ, Oost FC, Degroot A, et al: Review of postoperative bleeding risk in dental patients on antiplatelet therapy. Oral Surg Oral Med Oral Pathol Oral Radiol 115: 491, 2013.
153. Assael LA: Hemostasis is a shared responsibility. J Oral Maxillofac Surg 61: 1377, 2003.
Related aRtiCles in SELECTED READINGS IN ORAL AND MAXILLOFACIAL SURGERY

SELECTED READINGSIN
ORAL ANDMAXILLOFACIAL SURGERY
PUBLISHER SELECTED READINGS IN ORAL AND MAXILLOFACIAL SURGERY c/o Elizabeth Muscatell 5323 Harry Hines Blvd., M/C 9109 Dallas, TX 75390-9109 PHONE: 214/648-3554 FAX: 214/648-2918 Email to: [email protected] WEB PAGE: http://www.selectedreadingsoms.com
STAFF
DOUGLAS P. SINN, D.D.S. FELICE S. O’RYAN, D.D.S. EDITOR-IN-CHIEF CO-FOUNDING EDITOR CO-FOUNDING EDITOR
JAMES E. BERTZ, D.D.S., M.D. THOMAS W. BRAUN, D.M.D., Ph.D. ASSOCIATE EDITOR ASSOCIATE EDITOR
G. E. GHALI, D.D.S., M.D. EDWARD ELLIS, III, D.D.S., M.S. ASSOCIATE EDITOR ASSOCIATE EDITOR
JOHN P. W. KELLY, D.M.D., M.D. GAYLORD S. THROCKMORTON, Ph.D. ASSOCIATE EDITOR MEDICAL EDITOR
THOMAS P. WILLIAMS, D.D.S. ELIZABETH MUSCATELL ASSOCIATE EDITOR ADMINISTRATIVE COORDINATOR
SUBSCRIPTIONS Order Online at www.selectedreadingsoms.com Order Online at www.selectedreadingsoms.com Digital Subscription 2013 $160; Resident Digital Subscription $99* Digital Subscriptions include online access to the current volume (Vol. 21) and Volumes 10 -20, with access to full text and PDF issues. PAYABLE TO “SELECTED READINGS IN ORAL AND MAXILLOFACIAL SURGERY PAYMENTS IN U.S. FUNDS ONLY. NOTIFY 30 DAYS IN ADVANCE OF ADDRESS CORRECTION.
*To receive the resident rate, please include a letter of resident status from your residency director or appropriate individual on program letterhead (email to [email protected]).
Selected Readings in Oral and Maxillofacial Surgery is partially supported by Biomet Microfixation (Walter Lorenz Surgical), Jacksonville, Florida
ISSN #1044-7032