seetharam opthalmology - cdn.ymaws.com · 2/16/2015 1 ophthalmology cases from a primary care...
TRANSCRIPT

2/16/2015
1
Ophthalmology Cases from a Primary Care Perspective
Shabari Seetharam, M.D.
Arizona Retina and Vitreous Consultants
Eye Anatomy
Retinal Anatomy
• http://www.images.missionforvisionusa.org/anatomy/uploaded_images/NORMALcopy‐737523‐792494.jpg

2/16/2015
2
Gross Anatomy
Definitions
• Slit Lamp
• Fundus
– Posterior Pole
–Midperiphery
– Periphery
• Anterior Segment

2/16/2015
3
Presbyopia
The Eye Exam
Dermatochalasis

2/16/2015
4
Styes
Other Anterior Abnormalities
Dry Eye

2/16/2015
5
Dilated Eye Exams
Cataracts
PSC cataract

2/16/2015
6
Cortical Cataract
Floaters
Posterior Vitreous Degeneration

2/16/2015
7
Floaters
Case 1
• 33 yo female c/o blurred vision right eye
• When she looks at faces they are blurred.
• PMHx: G2P2
• Meds: None
• POHx: None
• Cannot pinpoint onset, maybe past week
• Progressive decline
• C/o pain, exacerbated with eye movement
Case 1
• Vision
– 20/40 OD
– 20/25 OS
• IOP
– 20
– 19
• Pupil Exam
– 43 OU, +right APDExample of Central Scotoma

2/16/2015
8

2/16/2015
9
Fundus Exam
The next step in management?
• A. Begin IV antibiotics for likely orbital abscess
• B. Obtain Fluorescein Angiogram to evaluate for retinal vasculitis
• C. Order an MRI to evaluate for inflammatory lesions
• D. Observe with close follow‐up as this is likely a retinal migraine
• E. Begin IV steroids for inflammatory disorder

2/16/2015
10
Diagnosis
• Answer: E; Diagnosis—Retrobulbar Optic Neuritis– Truly a clinical diagnosis– C is also correct, expect to see optic nerve enhancement and evaluate for MS
• Etiology– Manifestation of Multiple Sclerosis– Idiopathic– Viral papillitis usually anterior optic neuritis (see inflammation on fundus
exam)• VZV, EBV, HSV
– Infectious cause unusual in adults– Granulomatous inflammation (Sarcoid)
• Treatment: IV steroids followed by oral taper– NOT ORAL—increased risk of recurrence– Optic Neuritis is self limited
Summary
• Classic Presentation of Optic Neuritis
– Female pt in childbearing years with subacute vision loss. Central scotoma.
• RELATIVE Afferent Pupillary Defect
• Blurred vision—probe for specific defects
Eye Pain
• Pain Associated with Corneal injury
– Sharp or Stabbing
– c/o foreign body sensation.
– Associated with Tearing*
– Better with eye closure
– Can be worse with blinking
–Worse with reading/sustained activities
– Occasionally c/o Light Sensitivity

2/16/2015
11
Eye Pain
• Pain associated with high intraocular pressure
–Headache/Deep throbbing pain
–Acute Angle Closure Glaucoma (ER setting)
• Pain associated with Uveitis
–Headache/Deep throbbing pain
– Sensitivity to Light as Iris Constricts
Eye pain
• Eye Pain in optic neuritis worsened with eye movements.
• After intraocular surgery, worry about endophthalmitis.
• Referred pain to the eye.
Cellulitis—Preseptal or Postseptal?

2/16/2015
12
Orbital Septum
Orbital Signs
• Proptosis
• Chemosis
• Ophthalmoplegia
• Decreased visual acuity/color vision
• Pupillary abnormalities
• ex
Case 2
• 48 yo female. PMHx: Hypertension. Meds: Hydrochlorothiazide 25mg.
• POHx: Myopia since age 16. Wears soft contact lenses.
• Family history: +eye surgery in father, unsure what surgery.
• Noticing flashing arcs of light x3 days in the left eye. Yesterday woke up with floaters
• Pt thinks it is a little blurry for her to read with the left eye. No visual field defect.

2/16/2015
13
Case 2
• Exam
– 20/20; 20/30
– Pupils 53 OU, no APD
– IOP 15, 17
• Anterior Segment ‐‐ Normal
• Posterior Segment
– Vitreous +pigmented cell
– Dot hemorrhage in the periphery
• http://www.djo.harvard.edu/files/7288_1173.jpg

2/16/2015
14
• http://www.mvretina.com/presentation/images/tear.jpg
Posterior Vitreous Detachment
• http://www.retinacarecenternj.com/images/p‐pvd_diagram_100.jpg

2/16/2015
15
• http://coloradoretina.com/wp‐content/uploads/2008/10/tear.jpg
• http://www.nethradhama.org/images/retinal_tear_2.jpg

2/16/2015
16
Management of Retinal Detachment
• In Office:
– Very early and peripheral detachments can be lasered
– Pneumatic Retinopexy
• In the OR:
– Pars Plana Vitrectomy
– Scleral Buckle
Pars Plana Vitrectomy (PPV)

2/16/2015
17
Scleral Buckle
Case 3
• 68 yo male with intermittent loss of vision in the right eye. He has had 2 episodes in the past 2 weeks. The top half of vision looked like “snow on the TV.” Lasted about 2 minutes each time.
• PMHx: Lung Cancer s/p RLL lobectomy. Hypertension. Hyperlipidemia. Meds: Lipitor, Diovan. FHx: Diabetes.
• POHx: Cataract Surgery OU 5 years ago.
Amaurosis Fugax
• Intermittent loss of visual field
• Can be total or partial
• Vision returns to normal between episodes
• Conventionally Unilateral **
• Painless– If there is headache or pain consider Giant Cell Arteritis• Jaw Claudication/Scalp Tenderness/ Wt loss/Weakness
– Pain may also be sign of carotid dissection

2/16/2015
18
Amaurosis Fugax
Amaurosis Fugax
• http://www.nature.com/eye/journal/v20/n9/images/6702113f2.jpg

2/16/2015
19
Differential of Amaurosis Fugax
• Carotid Stenosis
• Cardiac Emboli
• Giant Cell Arteritis
• Vasospasm (Retinal Migraine)
• Gaze Evoked (orbital mass)
Work‐Up for Amaurosis Fugax
• Carotid Dopplers*
• Transthoracic Echocardiogram
• Blood Pressure
• Lab work for vascular risk factors: CBC with differential, hyperglycemia, hyperlipidemia
– ESR/CRP when GCA suspected
• Imaging if concern for orbital mass or carotid dissection.
Differential of Transient Binocular Vision Loss
• Posterior Circulation TIA– Vertebrobasilar artery insufficiency
• Vertebral artery dissection
• Migraine
• Papilledema (Increased Intracranial Pressure)

2/16/2015
20
Case 4
• 32 yo female c/o mild blurring of the left eye when reading. For the past few months.
• PMHx: Rheumatoid Arthritis x 5 years. Medications: On Plaquenil 200mg PO BID; Prednisone 5mg PO daily. FHx: Glaucoma.
• POHx: Needed antibiotics for a “scratch on her eye” 1 year ago.
Case 4
• Exam– 20/20; 20/25
– Pupils 53 OU, no APD
– IOP 15, 17
• Anterior Segment– L/L—nl
– C/S—w/q
– K—clear
– AC –D/Q
Which of these Cataracts is caused by Prednisone?
• Posterior Subcapsular • Nuclear Sclerotic

2/16/2015
21
Plaquenil Toxicity
• Early signs show‐‐ RPE mottling, speckling of retina.
• Later sign is frank atrophy
• Would expect bilateral maculopathy, but can be asymmetric in the early stages
• Mechanism not completely understood– Affects photoreceptor metabolism
– Medication binds to melanin in RPE

2/16/2015
22
• http://webeye.ophth.uiowa.edu/eyeforum/cases‐i/case139/Slide2.jpg
Advanced Maculopathy
Plaquenil Toxicity
• Recommend Baseline exam
– If abnormalities on baseline, consider other med.
• Q1 year after*
• Toxicity not reversible, and may even progress after cessation (build up in RPE)
• Increased Dosage (>6.5mg/kg/day; >1000g cumulative dose)
– Renal disease, Liver Disease, >60 yo

2/16/2015
23
Medication with Ocular Side Effects
• Plaquenil ‐‐Maculopathy
• Prednisone –subcapsular cataracts– Central serous retinopathy
• Tamsulosin– Intraoperative Floppy Iris Syndrome
• Ethambutol –Optic neuropathy
• Sildenafil –Dyschromatopsia
• Bisphosponates ‐‐ Uveitis
• Sulfa Medications (Topamax)– Choroidal Effusion
Case 5
• 43 yo male, type I diabetic, hypothyroid– Complains of mobile spider web/cloud in vision.
• Is this likely due to:A) Macular Edema from Hypothyroidism
B) Tear film instability from Diabetes
C) Macular Edema from Diabetes
D) Neovascularization from Diabetes
E) Cataract from a combination of thyroid disease and diabetes

2/16/2015
24
Diabetic Macular Edema (DME)

2/16/2015
25
DME in Cross‐Section
Diabetic Care
• Diabetes Control and Complications Trial
– Lowering a1c by 1% reduces risk of ocular complications by ~35%
• Rosiglitazone may* increase DME
• Hemodialysis can help decrease DME
• Control other vascular risk factors
– Blood Pressure/Lipids/Sleep Apnea/Sickle Cell/Anemia/CHF/Renal Disease
Hypertensive Retinopathy

2/16/2015
26
Trauma
Conjunctivitis
• Allergic Conjunctivitis– Itching
– Antihistamines
– Steroids
• Viral looks like allergic but without itch
• Bacterial
2/16/2015
27
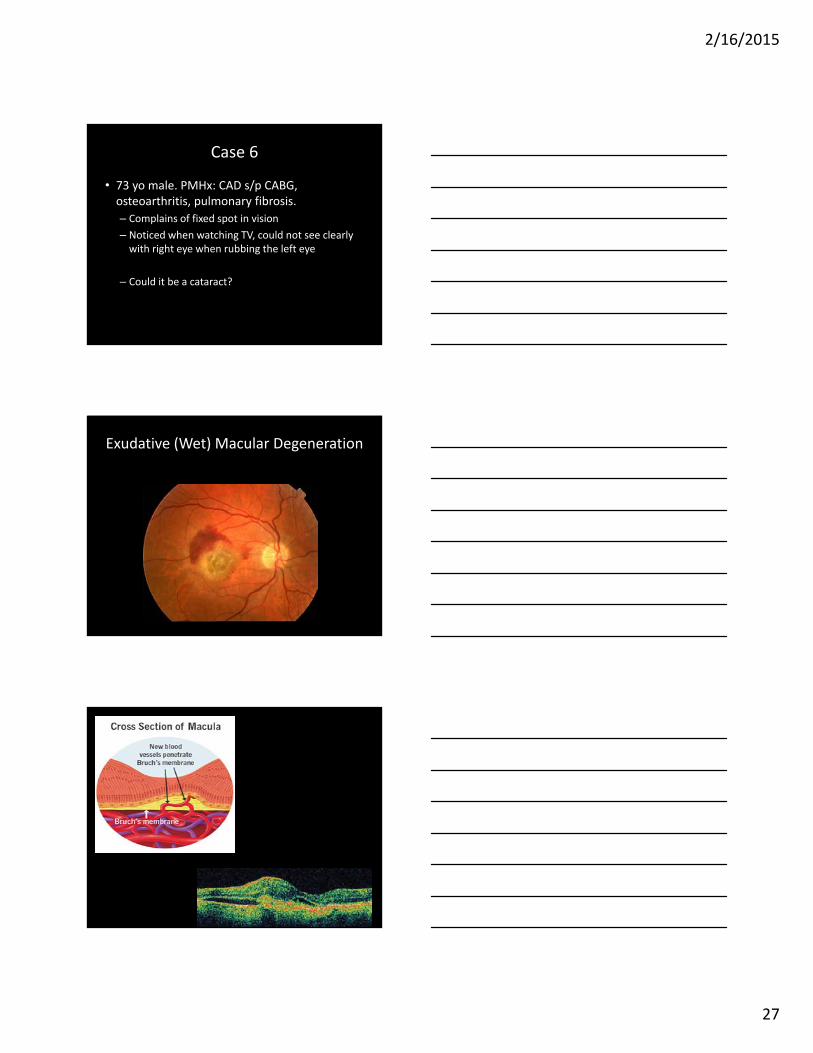
Case 6
• 73 yo male. PMHx: CAD s/p CABG, osteoarthritis, pulmonary fibrosis.
– Complains of fixed spot in vision
– Noticed when watching TV, could not see clearly with right eye when rubbing the left eye
– Could it be a cataract? .
Exudative (Wet) Macular Degeneration

2/16/2015
28
Treatment for Exudative AMD
Intravitreal Injections
• Often Monthly
• Avastin (Bevacizumab)
• Lucentis (Ranibizumab)
• Eylea (Aflibercept)
Treatment for Wet AMD
• Injectable medications

2/16/2015
29
Dry AMD
Early Intermediate
Dry AMD

2/16/2015
30
Complement Cascade
MAC Attack

2/16/2015
31
Glaucoma
• What is it?
– A slowly progressive optic neuropathy
– Usually, but not always, associated with high eye pressure
– Normal eye pressure is between 10‐21 mmHg
Glaucoma
• “Patients with glaucoma should check with their doctor before starting this medication.”
• Anticholinergic component to many drugs
• Can lead to relative pupillary block

2/16/2015
32
• http://i1.ytimg.com/vi/leMexvs9HVU/hqdefault.jpg
Using a direct ophthalmoscope
• Have the patient look over your shoulder– Prevents Miosis– Moves optic nerve closer to your view
• Use a small light if pt is undilated
• If your prescription is 0, you still may need to dial in a ‐2
• Pivot the light
Dilation
• Tropicamide 0.5% or 1%– Anticholinergic– Dilation and Cylcoplegia
• Phenylephrine 2.5%– Sympathomimetic– Dilation without Cycloplegia
• Risk of Angle Closure Glaucoma 1/20,000

2/16/2015
33
View through a Direct Scope
Slit Lamp

2/16/2015
34
AAO recommendations
Thank you
Papilledema