sciatica - ard.bmj.com · sciatica an anatomical and mechanical study of the lumbosacral region by...
TRANSCRIPT

SCIATICAAN ANATOMICAL AND MECHANICAL STUDY OF THE LUMBOSACRAL REGION
BY
NORMAN CAPENERPrincess Elizabeth Orthopaedic Hospital, Exeter
Great interest is being shown in sciatica at thepresent time. It is a common disturbance of obscureetiology. Its association with rheumatism andtrauma renders it a severe economic problem, in waras in peace. An advance in the understanding ofsome forms of sciatica has been made in the recogni-tion of the important part played by intervertebraldisc lesions (Alajouanine and Petit-Dutaillis. 1930;Mixter and Barr, 1934; Peet and Echols, 1934). Acertain amount of clinical research is being con-ducted upon special groups of cases. It is probablethat other and more extensive investigations will beembarked upon as soon as circumstances permit.Therefore I have felt that the time is appropriate forthe publication of certain researches into the anato-mical and mechanical background of the problem.*Very little originality is claimed for the greater partof the work. Material (both clinical and radio-logical) has been studied and is here presented in thehope that it may prove a guide for investigators.Written as it is from the orthopaedic point of view, itis natural that the mechanical factors should bestressed rather than the pathological. I have triedto avoid glaring excursions into theoretic considera-tions, but it is impossible to avoid them altogether.
The Normal Lumbar CurveThe lumbar hollow is a human characteristic
which babies acquire in the first year of life (Fig. 1).It is dependent upon extension of the thighs, which
* Based on a Hunterian Lecture, " The Lumbo-sacral Joint: a Dis-cussion upon Spondylolisthesis, Scoliosis, and Sciatica," RoyalCollege of Surgeons; Jan. 22, 1941.
before birth have been held flexed upon the abdo-men. After birth some " fixed " flexion of the hipsremains. Extension force applied to these joints insmall babies is communicated to the lumbar spineand a lordotic concavity is developed. Willis (1932)has suggested that the deleterious effects of suchforce upon the lumbar spine are aggravated incivilized people by " the efficient bathing, diapering,and swaddling attentions of the modern nurse."Certainly lordosis and protuberant abdomen arenormal features in infants who are learning to walk;the relation of this in some children to lack of hipextension is to be remembered. Later, as true exten-sion of the hip-joints occurs, there is shortening ofthe ham-string muscles, the influence of which, bytilting the pelvis backwards, is to reduce the lumbarlordosis. Any circumstance which unduly in-creases ham-string tension will restore the prenataltype of lumbar convexity backwards (Fig. 1, D).This is by no means an unusual circumstance, for itis to be found in any person who chooses to situpright with his knees extended; or, with the kneesextended, to pick up something from the ground.As we shall see later, the latter position is fraughtwith danger for those prone to sciatica, and theformer is one all too frequently indulged in by thosewho spend too much time in bed. It is more than ofpassing interest that while the prenatal condition ofthe foetal lumbar spine is one of backward con-vexity, so, as Lambrinudi (1934) observed, is that ofits mother's; which is not lordotic as so commonlythought. The condition of the gravid woman's
AFutL4enuTtat SpLIn Utero
FIG. 1. The Lumbosacral Paradox. Vulnerability in infancy by deviation from prenatal curvature-i.e. by extensionforce. Vulnerability in adult life by return to prenatal type of curvature-i.e. by flexion force.
D 29
on January 5, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.4.2.29 on 1 D
ecember 1944. D
ownloaded from

ANNALS OF THE RHEUMATIC DISEASES
lumbar spine -from the sixth month onwards isfavourable for the development of sciatica.
Lumbar Spine as a UnitThe Question of Rotation.-Much of anatomical
description in textbooks is directed to the varyingfeatures of individual segments, their shape, attach-ments and articulation. Too little attention, how-ever, is paid to the spine as a whole, or to its regionsas units of the whole. The spine is a concatenationand behaves like a chain. Movement of one seg-ment involves movement of the whole. The perio-dicity of scoliosis, which so closely resembles a phaseof vibration in a monochord, has its counterpart inthe twists and curves of unstable pillars and towers.This is too big a subject to go into here, but if we dorealize the obvious idea of the chain, it will be mucheasier to understand the question of whether rotationmovements occur in the lumbar spine. Manywriters still quote old textbook descriptions denyingit, and J. E. Frazer still repeats that the articularfacets of the lumbar vertebrae are so placed as toprevent rotation, which is only considered as beingaround a vertical axis situated in the centre of thevertebral bodies (Fig. 4). If, however, we disregardthe segmental idea, there is no reason at all why theaxis of rotation should not be found anywhere, evenin mid-air. Certainly, from a mechanical view-point, one would expect it to lie on the concave sideof the normal curve (as it does in the thoracicregion). To everyone familiar with the problems ofscoliosis it is obvious that a considerable degree ofrotation does occur in the lumbar region. If theaxis for this movement is regarded as being posteriorto the spinal canal, then it is quite easy to see howthe arrangement of the lumbar articular facts readilypermits it. The range need be less than eight degreesbetween each segment to permit a total of forty-fivedegrees between the chest and the pelvis, which isprobably as much as a normally supple personrequires, and is more than he could produce in thethoracic region, which, relatively, has far less rota-tion because of the need for protection of its viscera.Owing to the more coronal arrangement of thelumbo-sacral facets it is probable that a larger degreeof rotation is possible here than in the rest of thelumbar region. There can be no doubt about thismatter of rotation for another reason-because it isa physical necessity in any lateral flexion. Bendingsideways any structure like the lumbar spine, whichhas a pre-existing forward convexity, must be accom-panied by torsion of the whole region (or rotationbetween individual segments).The posterior neural arches and spinous pro-
cesses are of gteater mechanical importance thanhas generally been realized. Under the heading of" weight transmission " I shall have more to say, buthere one should remark on an interesting pheno-menon in the movement of hyper-extension: notonly does weight tend to be transferred to thearticular and spinous processes, but individualvertebrae tend to slide backwards on the one below.It is more readily detected in the upper lumbar
region, and was well shown in the extreme exampleof lumbar hyperextension in a contorsionist whoseradiograph was described by Lockhart and repro-duced in the last edition of Cunningham's Textbookof Anatomy. I have demonstrated the same point inradiographs of normal spines (Fig. 2), and (Capener,1932) in a remarkable case of spinal tuberculosis
FIG. 2. Two views of the same spine in standingposition. In the original films the distance betweenthe same points marked X in extension and o inflexion were 5i in. and 71 in. respectively.
associated with spondylolisthesis (Fig. 5). In theupper lumbar spine it may become a fixed conditionand is then known as retrospondylolisthesis; beingoften due to post-traumatic degeneration of theintervertebral disc, or osteoarthritis.
Fourth Lumbar VertebraThe importance of this vertebra in the present
discussion is that it is the " spear head of attack " bysuperimposed body weight upon the mechanicalweaknesses of the fifth lumbar vertebra. It is oftenthe last vertebra of completely lumbar type. Fromthe intervertebral disc beneath it there occursposterior herniation with almost equal frequency asfrom the lumbo-sacral disc. In the past, prominencehas been given to the various forms of true con-genital anomaly of the fifth lumbar vertebra, such ascomplete or partial sacralization. Generally, atten-tion has been paid to the aberrant masses which pro-ject laterally from one or other transverse processand articulate more or less completely with thelateral mass of the sacrum. Probably osteo-arthritic changes can occur at these additional joints,but what tends to be overlooked is the consequentaltered mechanical conditions in the joints betweenthe fourth and fifth lumbar vertebrae. With thegreater fixation of the fifth, the stresses to which thefourth is exposed without doubt explain such a cir-cumstance as the greater liability then for the fourthto show spondylolytic changes, and of its inter-vertebral disc to suffer from trauma.
Intervertebral DiscsFrom a study of recent literature, it is obvious
that these structures are of considerable significancein any discussion of sciatica. The best work uponthe normal and morbid anatomy is that by Schmorl,made readily available to English readers by Beadle
30
on January 5, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.4.2.29 on 1 D
ecember 1944. D
ownloaded from
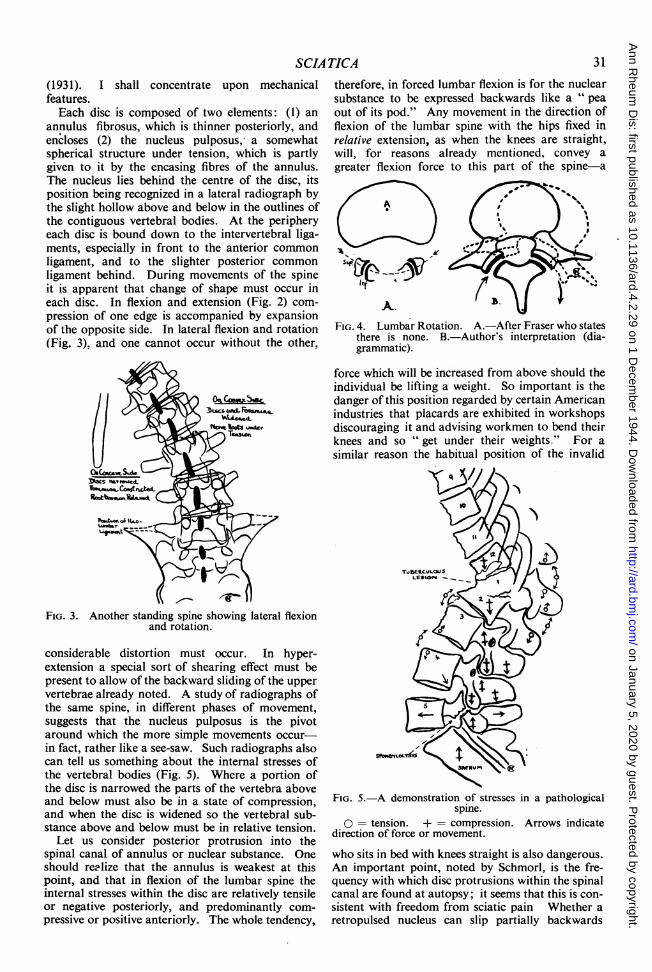
therefore, in forced lumbar flexion is for the nuclearsubstance to be expressed backwards like a " peaout of its pod." Any movement in the direction offlexion of the lumbar spine with the hips fixed inrelative extension, as when the knees are straight,will, for reasons already mentioned, convey agreater flexion force to this part of the spine-a
FIG. 4. Lumbar Rotation. A.-After Fraser who statesthere is none. B.-Author's interpretation (dia-grammatic).
force which will be increased from above should theindividual be lifting a weight. So important is thedanger of this position regarded by certain Americanindustries that placards are exhibited in workshopsdiscouraging it and advising workmen to bend theirknees and so " get under their weights." For asimilar reason the habitual position of the invalid
C 4 IN/N
(1931). I shall concentrate upon mechanicalfeatures.Each disc is composed of two elements: (1) an
annulus fibrosus, which is thinner posteriorly, andencloses (2) the nucleus pulposus, a somewhatspherical structure under tension, which is partlygiven to it by the encasing fibres of the annulus.The nucleus lies behind the centre of the disc, itsposition being recognized in a lateral radiograph bythe slight hollow above and below in the outlines ofthe contiguous vertebral bodies. At the peripheryeach disc is bound down to the intervertebral liga-ments, especially in front to the anterior commonligament, and to the slighter posterior commonligament behind. During movements of the spineit is apparent that change of shape must occur ineach disc. In flexion and extension (Fig. 2) com-pression of one edge is accompanied by expansionof the opposite side. In lateral flexion and rotation(Fig. 3). and one cannot occur without the other,
FIG. 3. Another standing spine showing lateral flexionand rotation.
considerable distortion must occur. In hyper-extension a special sort of shearing effect must bepresent to allow of the backward sliding of the uppervertebrae already noted. A study of radiographs ofthe same spine, in different phases of movement,suggests that the nucleus pulposus is the pivotaround which the more simple movements occur-in fact, rather like a see-saw. Such radiographs alsocan tell us something about the internal stresses ofthe vertebral bodies (Fig. 5). Where a portion ofthe disc is narrowed the parts of the vertebra aboveand below must also be in a state of compression,and when the disc is widened so the vertebral sub-stance above and below must be in relative tension.
Let us consider posterior protrusion into thespinal canal of annulus or nuclear substance. Oneshould realize that the annulus is weakest at thispoint, and that in flexion of the lumbar spine theinternal stresses within the disc are relatively tensileor negative posteriorly, and predominantly com-pressive or positive anteriorly. The whole tendency,
FIG. 5.-A demonstration of stresses in a pathologicalspine.
O = tension. + = compression. Arrows indicatedirection of force or movement.
who sits in bed with knees straight is also dangerous.An important point, noted by Schmorl, is the fre-quency with which disc protrusions within the spinalcanal are found at autopsy; it seems that this is con-sistent with freedom from sciatic pain Whether aretropulsed nucleus can slip partially backwards
SCIA TICA 31
on January 5, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.4.2.29 on 1 D
ecember 1944. D
ownloaded from

ANNALS OF THE RHEUMATIC DISEASESagain is open to doubt. It certainly would seem un-likely that it could return completely. The idea ofspontaneous reduction is attractive to the surgeonwho at operation finds nothing when lipiodol radio-graphy has been clearly positive. In such circum-stances it should be recognized that the influence ofweight-bearing is removed and that in recumbencythere is a natural tendency for the intervertebral discsto resume a normal shape. It would be interestingto know if the amount of retropulsion is a variablephenomenon in any particular case.
The Meninges and Intervertebral ForaminaIn the spinal canal the meningeal tube is separated
from its bony and ligamentous surroundings by anappreciable layer of extradural fatty areolar tissuewhich permits easy movement. The amount of thismovement requires further attention, for it is sur-prising to most people.
If one compares lateral radiographs of the lumbarspine in full flexion with those of the same spine inhyperextension, the disparity in length is remarkable.In the illustrations (Fig. 2) showing this, measure-ments were taken between the two same points inthe canal, and the elongation in full flexion is foundto be at least one-third of the shorter length in hyper-extension. Obviously, in flexion the meninges andcauda equina are under telative tension. It is thesame position of danger for intervertebral discs andnuclei, so that the retropulsive tendencies of themare met by nerve tissues on the stretch. Conversely,in hyperextension relaxed meninges and nerves gowith closed-up posterior disc spaces. While dis-cussing the effect of lumbar movement and postureupon the intraspinal soft tissues one should mentionchanges occurring within the intervertebral fora-mina. First of all, there is interest in the feature towhich attention was drawn by Danforth and Wilson(1925). Throughout the lumbar series these fora-mina become progressively smaller from abovedownwards to the lumbo-sacral interspace. This,which transmits the largest nerve root of them all,has the smallest available space. We must realizethat each foramen also contains meningeal bloodvessels and a prolongation of dura which eventuallymerges with the perineural sheath. Furthermore,each nerve root, which has emerged at an angle from
beneath the pedicle above. has a variable degree ofprolongation of arachnoid with cerebro-spinal fluid(Capener, 1937) (Fig. 6). This extension of thetheca, particularly on the lower lumbat nerve roots,is generally not appreciated.
In full flexion of the lumbar spine the foraminaaie enlarged to their maximum, in hyperextensionthey are smallest (Fig. 2). The vulnerability of struc-tures within them is greatest in hyperextension,which is the reverse to the dangers to structureswithin the spinal canal. In these altered relationswe have, I believe, some explanation for the con-flicting signs that many patients present. Thediagram shows this graphically (Chart 1). In some
MeningeB and Chorda
Foramoina
Intervertebral DiacPosteriorAnterior
Flexion
Extension
loexion
Tension
Niae open
WNidenedNarrowed
Extension
Relaxed
Constricted
NarrowedWidened
5it-.ple Graph to explain why in certain types of Sciaticano satisfactory relief In given by change of position Inthe dlrection of flexion or extension. In these lateralflexion (Scollosts) is necessary.
Che rt
patients relief from pain is given by hyperextension;in others, by flexion. In the former, relief may bedue to relaxation of the cauda equina and meningealtension or of nerve-root kink; while in flexionrelief may result because there is greater room forthe foraminal contents. On the contrary, flexion
FIG. 6. Relation of nerve roots, pedicles and intervertebral foramina. A and B.-Autopsy specimen in whichtheca has been filled with lipiodol. C.-Radiograph taken in course of investigation of a case of nuclearretropulsion.
32
on January 5, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.4.2.29 on 1 D
ecember 1944. D
ownloaded from

beyond the confines of the intervertebral foramen.This, of course, need not be the explanation of thecommonly observed remark of patients that sciaticpain is increased by sneezing or coughing. Thebombardment of an oedematous nerve root by asudden wave of increased intrathecal pressure issufficient to account for it. Compression of thejugular veins will act in the same way: for example,with the patient sitting comfortably and the knee ofthe affected side extended to a point just short ofthat necessary to cause sharp sciatic pain, compressthe jugulars-with intraspinal lesions the patientwill probably expetience sharp pain in the affectedsciatic distribution. Even more significant is itwhen the test is carried out on the unaffected leg andpain is produced on the affected side. In such testsit must be remembered that straight leg raising(Laseague's test) necessarily causes elimination ofthe normal lumbar curve and produces all that goeswith lumbar flexion. Laseague's test on the un-affected limb, if it gives pain on the affected side, ismuch more significant than when performed on theaffected side alone. It does then indicate that painis being produced by spinal movement, and not bystretching the affected sciatic nerve trunk.
The LigamentsTwo ligamentous structures in this region call for
particular comment. The first is the ligamentumflavum, which has come into prominence recentlybecause of the more frequent operations for sciatica.This " yellow " ligament is an interesting structurebecause, in a histological sense, it is composed ofalmost pure elastic tissue fibres and because a con-dition of " hypertrophy " has been described. Itbridges the gap between each neural arch posteriorly;it thus completes the protection of the intraspinaltissues, and because of its density and elasticity actslike the flexible sheath to a motor brake-rod orcarburettor control. At operation it is not infre-quently found to be thickened, and appears to con-strict the deeper tissues. Dockerty and Love (1940)have shown, however, that, rather than hyper-trophy, the condition is the result of degeneration,and the thickening is due to invasion and replace-ment of elastic tissue by fibrous tissues. Probablyit is secondary to local irritative changes-e.g. osteo-arthritis or nuclear retropulsion. It is a convenientcondition on which to pin a diagnosis when laminec-tomy is otherwise negative; but we deceive our-selves if we think that this is the real cause of thepatient's trouble.The ilio-lumbar ligaments provide an important
means of anchoring the fifth lumbar vertebra. Thisvertebra has potentialities for considerable rotation,and is exposed to an amount of shearing stress notfound elsewhere in the spine. Extending from thetransverse processes (which are placed relativelymore anteriorly) these ligaments (Fig. 3) areattached, at each side, to the crest of the ilium; arewell placed for the control of rotation, and togetherprovide a sling restraining forward movement of thelast lumbar vertebra. That this is so is shown
may increase disc and nuclear retropulsion, while byhyperextension one may aggravate pain by con-stricting foraminal contents. Lateral flexion willhave a similar effect on the concave side, and rota-tion will increase nerve-root tension on one side.The constriction of intervertebral foraminal con-tents is, of course, of more significance should thenerve root be oedematous, or if the size of the fora-men is further reduced by lateral disc protrusion,osteoarthritic outgrowth, and so forth. Here itshould be noted that herniation of disc substanceinto a foramen is not seen in opaque myelography.Some of the most distressing forms of sciatica arein individuals who get relief by no alteration inposition, and in whom every movement is agonizing.It will readily be appreciated from the above dis-cussion how movement giving relief from oneelement of the painful condition is vitiated by theaggravation of something else. Nevertheless,posture does sometimes produce the most astonish-ing relief. When dealing with muscular functionlater on I shall have more to say on this; but hereone should remark upon the fact that hyperextensionoccasionally is very helpful. It suggests that a nerveroot, caught upon the summit of a bulging inter-vertebral disc, may be dislodged into the neighbour-ing valley by the backward sliding tendency of theupper vertebra, at a time when the chorda equinaand meningeal tension is eased. Sudden jerks maydo the same thing.A phenomenon which illustrates the complexities
of spinal mechanics is the peculiar scoliotic dis-placement of the trunk which is almost invariablyassociated with sciatica. Most frequently such dis-placement is to the opposite side (contralateral) andprobably is to be interpreted as an attempt to relieveintervertebral compression; when the curvature istowards the same side (ipsi- or homo- lateral) it isprobably nerve-root tension which the body is tryingto avoid. Another element of deformity usuallypresent is elimination of lordosis; such flattening ofthe lumbar hollow may be so severe as to constitutea lumbar kyphos. These deformities which arefixed by muscle spasm are comparable to the ham-string spasm which fixes a deranged knee in flexion.A rarer anomaly is an alternating type of sciaticscoliosis (ischiatica alternans) in which the patientmay vary the side of his displacement, sometimesvoluntarily; at one moment ipsilateral, anothertime contralateral; but never can he hold the spinestraight. Closer analysis of such a case reveals thatthe curves are not mirror images of each other.In one case reported by the writer (Capener, 1933)it was found that ipsilateral scoliosis had its apex ata higher level in the lumbar spine than the contra-lateral curvature.
I have often wondered whether herniation of thearachnoid farther into an intervertebral foramenoccurs; possibly through local defect in its cover-ings or from frequent sudden rises of intrathecalcerebrospinal pressure. In one case of sciatica(Fig. 6, C), radiographed with lipiodol, I did find anunusually long prolongation around a nerve root
33SCIA TICA
on January 5, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.4.2.29 on 1 D
ecember 1944. D
ownloaded from

ANNALS OF THE RHEUMATIC DISEASES
decisively by some patients with spondylolisthesis,where the ligaments become calcified, as so oftenhappens when ligamentous bands are exposed tolong-standing tension of a pathological degree(e.g. the interspinous ligaments in tuberculouskyphosis). It requires little stretch of the imagina-tion to envisage lesser degrees of ligamentous fibrosisas the result of trauma, such as, for example, occurselsewhere in occupational lesions. It is worth noting,in passing, that from this ligament arises some ofthe fibres of the quadratus lumborum muscle.
Weight TransmissionSo far I have discussed the vulnerability of the
lumbo-sacral region mainly from the aspect ofdynamics. There are, however, questions of staticswhich are no less important. Let us start first withthe lumbo-sacral angle, which has been variouslydescribed by different authors. Most frequently itis used to denote the angle formed between theanterior surfaces of the last lumbar and first sacralbodies. Considered in terms of statics, the angledescribed by Whitman is more significant. Accord-ing to him the lumbo-sacral angle is that between theupper surface of the sacrum and the horizontal. Itmatters little whether this angle is measured thus orin relation to the vertical. To avoid confusion Iwill use the term " lumbo-sacral inclination," whichfrom a mechanical viewpoint is the angle to thehorizontal of a plane midway through the lumbo-sacral intervertebral disc. There is no record thatlumbo-sacral angles have ever been measured inliving erect human beings: one suspects thatmeasurements have been done on cadavers or inrecumbency both fallacious. I have radiographedthe lumbo-sacral ilclinataioni in a number of standingindividuals and have found the angle to be about25-30 degrees (Fig. 7B). In the habitual lordoticperson the angle is greater; in an individual withshort hamstrings it is less. The angle is of coursevery variable according to posture. When the spineis hyperextended, or when the individual sits withknees extended, the inclination becomes almost
horizontal; as it also does with Goldthwaite's back-flattening exercise. When standing with the spineand hips flexed, the lumbo-sacral intervertebralplane tilts forward to the vertical and beyond. Inthe joint between the fourth and fifth lumbar verte-bra the plane of the intervertebral disc, except inlordotic people, is almost horizontal. The import-ance of the lumbo-sacral inclination is in the shearingstress exerted upon the intervertebral disc, and theconsequent tendency for the whole lumbar spine toslide forwards off the sacrum. That this sliding does,to a certain degree, occur is seen in cases of spondv-lolisthesis, a condition which is far commonet thanis usually thought. Mathematically, it can be shownthat for an angle of 30 degrees the shearing forceamounts to 43 per cent. of the superincumbent weight.The lumbo-sacral inclination lies a little above thecentre of gravity in a standing person; therefore itcan be estimated that if he weighs 140 lb. the shearingforce will amount to about 27 lb.; which is muchsmaller than one would have thought (Fig. 7 B).Obviously in carrying weights the force will increaseproportionately.
In an intact last lumbar vertebra the interlockingof its lower articular facets with those of the sacrumclearly counterbalance shear. The ilio-lumbar liga-ments play a part, as does also the intervertebraldisc. I am going into this in more detail because Ibelieve that in the human machine and its dis-abilities not enough attention is directed to theinternal stressing of its materials in this region asimportant as anywhere. Of particular importanceis the nucleus pulposus which though composed ofsoft tissues expands when released from its cover-ings; thus constituted it is clearly compressible. Ifin a lumbo-sacral skeleton one places a steel ball ofthe same size and in the same position as the nucleuspulposus, but embed it in rubber instead of theannulus, and then erect the specimen in a positioncomparable to that of erect posture with a super-imposed weight, interesting information can beobtained. Briefly the ball sets up reactionary forces(Newton's Law) the effect of which is to " push "
A BFIG. 7. A.-The mechanics of nuclear retropulsion. B. The mechanics of spondvlolisthesis (the nucleus
pulposus exerts reactionary force to shear).
34
on January 5, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.4.2.29 on 1 D
ecember 1944. D
ownloaded from

that in forward flexion it is possible for the muscleto act as a flexor. Normally spinal flexion rarelyneeds any flexor muscles; it is a gravity aided actionwhich chiefly requires extensor muscles to control it.One can, without greatly stretching the imagination,appreciate circumstances in which, the " trigger "
having gone off with the lumbar spine flexed, thequadratus lumborum is caught by explosive musclespasm in a flexion phase. Should the spine also betwisted at the same time, it is possible for thequadratus on one side to be fixed in flexor spasmwhile the opposice is in extension. This is somewhathypothetical, but I believe that in some such disorderis to be found one of the explanations of what, tosome patients with an acute attack of lumbago, is analmost catastrophic disturbance. These musclesmust. therefore, for coordinated action require anice adjustment of control. Under conditions offatigue or strain, physical or mental, this regulationmay more readily break down. Is it too fanciful toregard minor degrees of such disturbance in othermuscles as well, by causing atrophy, fibrosis, andadhesions, to be the same thing as much of thefibrositis about which we hear in sciatica?
It is worth considering the phases of muscularactivity which have to be coordinated; thus can thecomplexity of the spinal problem be more fullyappreciated. These are:
A. Simple Shortening Contraction.-The " normal'"anatomical action, e.g. of the biceps in flexing theelbow or the gluteals in extending the pelvis on thefemur.
B. Maintained Contraction (static).-As when thequadriceps is tensed without movement of the knee.
C. Lengthening Relaxation.-As when the tricepselongates to permit the biceps to flex the elbow.
D. Lengthening Contraction.-The converse to A andseen when a weight in the hand is lowered by exten-sion of the elbow. This is the " paradoxical "
action of the biceps. It is the same action that thespinal extensors have in controlling flexion of thespine and in the quadriceps particularly in walkingdown hill.
E. Maintained Relaxation.-The static condition ofcomplete relaxation.
F. Shortening Relaxation.-The converse to C, aswhen the triceps shortens during the paradoxicalaction of the biceps in controlling elbow extensionagainst gravity. Similarly in the spinal flexorswhen the extensors are in action against flexion ofthe spine.
SummaryThe lumbar spine presents many features in ana-
tomy and mechanics the appreciation of whichshould help in the elucidation of the clinical pro-blems of sciatica. It remains to state that in clinicalinvestigations more note should be taken of suchfactors.The history should have regard for details of
trauma, particularly of the more slowly operativeor static types. The habitual postures of occupation
the last lumbar vertebra backwards and upwards-in other words the ball tends to prevent it from slid-ing forwards. In the body, however, as the nucleusis a compressible structure its influence mechanicallyis even greater than the ball, because under weightit exposes a larger surface for the opposition ofshearing force. In spondylolisthesis, where there islack of continuity in the posterior neural archbetween the upper and lower articular facets, theinfluence of restraint by both the ilio-lumbar liga-ments and by the nucleus pulposus is probably muchgreater. Spondylolisthesis in its earlier state, thatis spondylolysis, is probably present in about 5 percent. of people, a frequency that adds point todiscussions of lumbo-sacral vulnerability.
Lumbo-sacral MusculatureIn 1934, before we heard much about the lesions of
the intervertebral discs, I stated that I befleved that 75per cent. of the disturbance of lumbo-sacral sciaticawas of a physiological nature-meaning musclespasm. This may be an exaggeration; neverthelessI still believe it is near to the truth. The wrenchedligament, the retropulsed intervertebral nucleus, thestretched nerve root, whatever the inner lesion, ismerely the trigger released; the explosion is in themuscular system. It may be large or small. Whatwe later have to contend with is the atrophy and thedissociation of coordination in the muscles. Suchatrophy, so obvious in the thigh muscles after de-rangement of the knee, is not so apparent in spinallesions.A simple picture of the posterior spinal muscula-
ture can be obtained if we regard it as comprising acontinuous mass arising mainly from the sacrumand ilium on each side and passing upwards towardsthe neck, where it becomes more specialized.Throughout its course its deeper surface receivesreinforcements from the bony structures upon whichit lies. The superficial part of the mass splits intothree perpendicular bundles attached respectively tothe rib angles, the transverse and spinous processes.The deeper part of the muscle comprises shortermuscle units which have a more oblique courseaccording to depth, but in the main they pass fromtransverse processes below, upwards and inwards tothe spinous processes one or more vertebrae above,the more superficial passing over five or morevertebrae. The anterior spinal muscles are theabdominal muscles. The lateral spinal musclescomprise the extensions of the abdominal musclesinto the loin, together with the psoas and a musclewhich is often overlooked-namely, the quadratuslumborum. This arises from the iliac crest and ilio-lumbar ligament and passes upwards to be attachedto the tips of the lumbar transverse processes and tothe lowest rib. It is described as being a lateralflexor of the spine and a weak extensor. As a lateralflexor it is necessarily affected by the rotation (ortorsion) that always accompanies side bending. Thequadratus lumborum lies very close to the axis ofbackward and forward movement-so close, in fact,
SCIA TICA 35
on January 5, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.4.2.29 on 1 D
ecember 1944. D
ownloaded from

ANNALS OF THE RHEUMATIC DISEASESshould be inquired into as well as the postureassumed during any isolated incident which hasprecipitated an acute sciatic attack. Such aninquiry may be found just as important as the well-recognized details of the mechanics of knee-cartilageinjuries. Additional information should be soughtabout those postures which either aggravate orrelieve symptoms-matters which will be availablefor corroboration during the physical examination.During the latter more attention than is usual shouldbe paid to the influences of spinal movement uponthe intraspinal and intervertebral tissues and to thechanges in intrathecal pressure. Finally, we shouldmake a closer study of the muscular control of thelumbar region.
In this paper I have presented information and afew theories about the mechanics of the lumbo-sacral region. Amongst the points I have discussedfrom a new angle are the rotation of the lumbarspine, the movements of the meninges and nerveroots, the mechanics of the nucleus pulposus, weighttransmission and matters relating to the " internalstresses of materials," and the action of the quad-ratus lumborum muscles. In the course of the paperit has been necessary to touch on some very element-ary facts, but the whole is given as a guide to theinvestigation and elucidation of the problems ofsciatica for clinical workers.
The researches upon which this is a brief report startedin the departments of anatomy, radiology, and ortho-paedics at the University of Michigan and have been con-tinued during the past twelve years in the orthopaedichospitals of Devon. It owes much to the inspiration ofthe late Dr. P. M. Hickey, Professor of Roentgenologyat the University of Michigan and to Sir Arthur Keith.To Professor F. H. Newman of the Department ofPhysics, University College of the South West, Exeter, Iam most grateful for his guidance upon the mechanicalproblems involved. For the radiological studies uponnormal spines in standing and other postures, I amindebted to the patience of various past and presentmembers of my Staff in the Princess Elizabeth Ortho-paedic Hospital, Exeter.
REFERENCESAlajouanine, I., and Petit-Dutaillis, D. (1930). Presse Med., 38, 1657,
1749.Beadle, 0. A. (1931). M. R. C., Special Report No. 161.Capener, N. (1932). Brit. J. Surg., 19, 374.
(1933), Proc. roy. Soc. Med., 26, 29.(1934). J. Chart. Soc. Mass. Med. Gym., Special Congress No.(1937). Proc. roy. Soc. Med., 30, 54.
Cunningham (1937). Textbook of Anatomy. Seventh Edition.Plate XVII, p. 328.
Danforth, M. S., and Wilson, P. D. (1925). J. Bone and Joint Surg.,7, 109.Dockerty, M. B., and Love, J. G. (1940). Proc. Mayo Clin., 15, 161.Frazer, J. E. (1933). The Anatomy cf the Human Skeleton.Lambrinudi, C. (1934). J. Bone and Joint Surg., 17, 239.Mixter, W. J., and Barr, J. S. (1934). New England J. Med., 211, 210.Peet, M. M., and Echols, D. H. (1934). Arch. Neurol. and Psych.,
32, 924.Willis, J. A. (1932). J. Bone and Joint Surg., 14, 267.
36
on January 5, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.4.2.29 on 1 D
ecember 1944. D
ownloaded from