sciatic nerve block under fluoroscopic guidance
TRANSCRIPT
Cardiovasc Inlervent Radiol t1986} 9:59-60
Vascular anti Interventional
~" Springer-Verlag New York Inc. 1986
Sciatic Nerve Block under Fluoroscopic Guidance
W.S. Tan and D.G. Spigos Department of Radiology. t'niversit~,, of Illinois Ho~pilal. Chicago USA
Abstract. Sciatic nerve block under fluoroscopic guidance was performed in 17 patients. This anes- thetic technique along with femoral nerve block was found to be effective in patients having unilateral femoral arteriography or occlusive arteriography of their extremities. No complication was encountered in this group of patients.
Key words: Sciatic ne rve- -Anes thes ia - -F luoros - copy
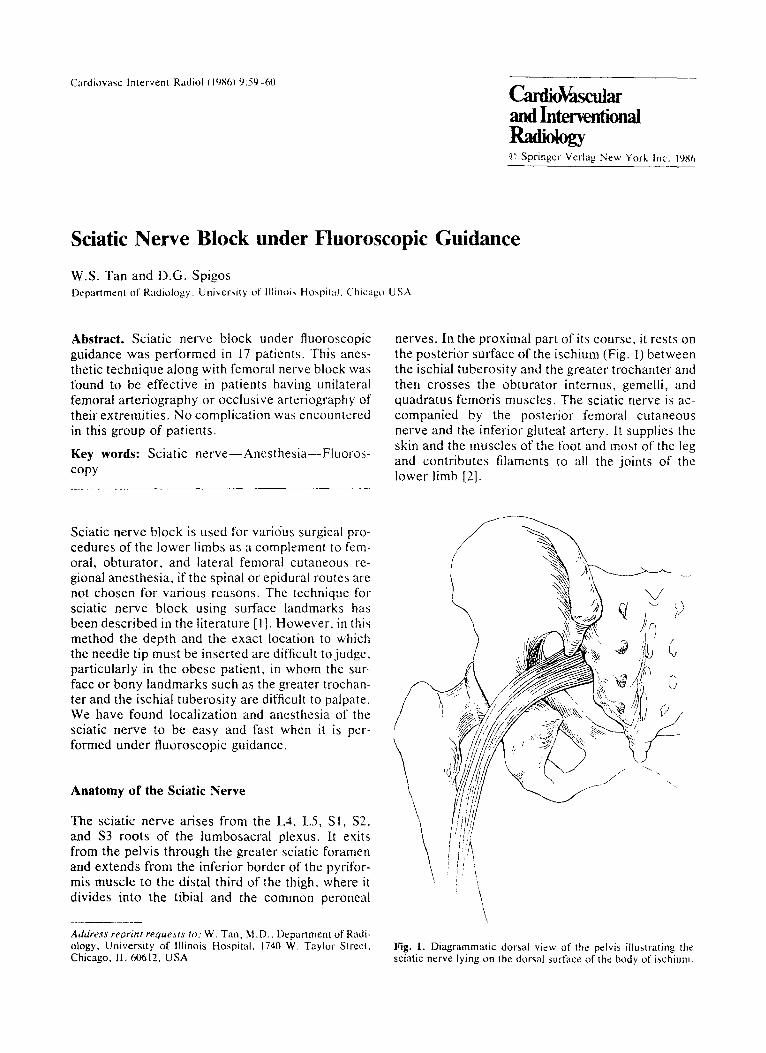
nerves. In the proximal part of its course, it rests on the posterior surface of the ischium (Fig. 1) between the ischial tuberosity and the greater trochanter and then crosses the obturator internus, gemelli, and quadratus femoris muscles. The sciatic nerve is ac- companied by the posterior femoral cutaneous nerve and the inferior gluteal artery. It supplies the skin and the muscles of the foot and most of the leg and contributes filaments to all the joints of the lower limb [2].
Sciatic nerve block is used for vario'us surgical pro- cedures of the lower limbs as a complement to fem- oral, obturator, and lateral femoral cutaneous re- gional anesthesia, if the spinal or epidural routes are not chosen for various reasons. The technique for sciatic nerve block using surface landmarks has been described in the literature [1]. However , in this method the depth and the exact location to which the needle tip must be inserted are difficult to judge, particularly in the obese patient, in whom the sur- face or bony landmarks such as the greater trochan- ter and the ischial tuberosity are difficult to palpate. We have found localization and anesthesia of the sciatic nerve to be easy and fast when it is per- formed under fluoroscopic guidance.
Anatomy of the Sciatic Nerve
The sciatic nerve arises from the L4, L5, S l, $2, and $3 roots of the lumbosacral plexus. It exits from the pelvis through the greater sciatic foramen and extends from the inferior border of the pyrifor- mis muscle to the distal third of the thigh, where it divides into the tibial and the common peroneal
Address reprint requests to.' W. Tan, M.D.. Department of Radi- ology, University of Illinois Hospital. 1740 W. Taylor Street, Chicago, IL 60612, USA
/ / /
/ f
\ Nx• I
9
I / '
\
i 5"[ /~
; \ f /
t.s
Fig. 1. Diagrammatic dorsal view of the pelvis illustrating the sciatic nerve lying on the dorsal surface of the body of ischium.

60 W.S. Tan and D.G. Spigos: Sciatic Nerve Block
Fig, 2, Spot film from a left-side sciatic block. The needle was flouroscopically guided to the dorsum of the body of ischium, which coincides with the center of flouroscopically identifiable acetabular cavity.
Materials and Methods
Sciatic nerve block was initially performed in 5 patients with pain at rest who were undergoing aortoiliofemoral arteriography. Sig- nificant alleviation of the pain on the anesthetized extremity oc- curred. Subsequently. this technique was used in 9 patients un- dergoing unilateral arteriographic studies of their extremities and in 3 patients who had occlusive arteriography of their legs. This technique is based on the tact that bony landmarks such as the greater sciatic foramen and the ischial spine can be accurately identified fluoroscopically: thus the nerve and its course can be inferred.
With the patient in the prone position, the dorsal surface of the ischium and the center of the acetabular cavity are fluoro- scopically identified (Fig. 2). The acetabular cavity projects on the body of the ischium, where the sciatic nerve lies. While the needle is advanced, the patient is questioned about the occur- rence of paresthesia. We continue advancing the needle until parestbesia is felt. Before the injection of 15 ml of 0.5% bupiva- caine HCI, the needle tip should be withdrawn a few millimeters so that the anesthetic is not injected in the subperiosteum. If the patient experiences excruciating pain during injection, i~ indi-
cares injection into the nerve, and-the needle tip should be repo- sitioned. Vollowing sciatic nerve block the patient is confined in bed until the effect of anesthesia completely wears off. because motor weakness is another effect of the block,
Discussion
Intraarterial injection of tidocaine before or during contrast medium injection has been reported to be effective to control pain [3-51. However, in a dou- ble-blind study, Eisenberg et al. pointed out its inef- fectiveness [6]. Moreover, repeated injections of contrast with lidocaine increase the danger of sys- temic toxicity. We had used epidural anesthesia with good results during the performance of aortoiliolemoral arteriograms [71. Although this method does provide complete analgesia, it has the disadvantage of additional cost and the potential of scheduling conflicts between the anesthesiology and angiography services. We have found the sci- atic nerve block to be an effective alternative to the epidural anesthesia in alleviating the pain during un- ilateral arteriography of the lower extremity. It also makes the procedure of aortoiliofemoral arteriogra- phy more comfortable in patients with pain at rest.
References
1. Lee JA, Bryce-Smith R (19761 Practical regional analge~,ia. Excerpta Medica, New York, pp 68-70
2. Gray H (1974) Gray's anatomy. Lea and Febiger, Philadel- phia, pp 997-1000
3. Gordon J J, Westcott J[, (1977) Intraarterial [idocaine: An el L fective analgesia for peripheral angiograptw. Radiology 124:43-45
4. Guthaner DF, Silverman JF~ Hayden WG. Wexler L [1977) Intraarterial lidocaine to control pain due to aortofemoral ar- teriography. A JR 128:737-739
5. Wildrich WC, Singer RJ, gobbins AH (19771 The use of in- traarterial lidoeaine to control pain due to aorlofemoral arte- riography. Radiology 124:37-41
6. Eisenberg RL, Mani RL, Hedgecock MW (1978) Pain associ- ated with peripheral angiography: Is lidocaine effective? Ra- diology 127:109-1 I1
7. Spigos DG, Akkineni S, Tan W. Espinoza G, Flanigan DP, Winnie A (1980) Epidural anesthesia: Effective analgesia in aortoiliofemoral arteriography. AIR 134:335-337