schenider first rank symptoms
TRANSCRIPT

SCHENIDER FIRST RANK SYMPTOMS
BY DR.WASIMUNDER GUIDANCE OF
DR.SANJAY.JAIN.
• Kurt Schneider was a German psychiatrist known largely for his writing on the diagnosis and understanding of schizophrenia, as well as personality disorders then known as psychopathic personalities.
• Schneider was born in Crailsheim, Kingdom of Württemberg, and trained in medicine in Berlin and Tübingen. He was drafted for and completed military service in World War I and later obtained a postgraduate qualification in psychiatry.
• In 1931 he became director of the German Psychiatric Research Institute in Munich, which was previously founded by Emil Kraepelin.
• Disgusted by the developing tide of psychiatric eugenics championed by the Nazi Party, Schneider left the institute, but did serve as a doctor for the german armed forces during World War II.
• After the war, academics who hadn't taken part in the Nazi eugenics policies were appointed to serve in, and rebuild Germany's medical institutions and Schneider was given the post of Dean of the Medical School at Heidelberg University. Schneider kept this post until his retirement in 1955.

INTRODUCTION
• Schneider accepted Kraepelin’s system of classificationand distinguished between “abnormal personalities”,“abnormal reactions”, “organic psychosis”, “schizophrenia andcyclothymia”.• He had taken a group of psychotic patients, excludedthose with clear organic psychosis, reactive psychosis,obvious cyclothymia, and then performed a statistical analysisof the symptom of the remaining psychotic patients, whowere presumed to have schizophrenia.• In those patients he termed the most frequently foundsymptoms as ‘First Rank Symptoms [FRS]’(Schneider 1959).• As per Schneider, FRS is mostly found in schizophrenia(Crichton, 1996).

EVOLUTION OF CONCEPT
• Morel, in 1852 reported a series of cases of severe intellectual deterioration starting in adolescence and he called this illness demence precoce.
• In 1874, Kahlbaum drew attention to a mental illness in which stupor occurred in the absence of disease of nervous system, he called this illness tension insanity or catatonia.
• In 1893, Kraepelin brought together the syndromes of demence precoce, hebephrenia, catatonia, and dementia paranoides in the 4th edition of his textbook and called this group of illness ‘psychological degeneration process’. In 1899, he used the term dementia praecox to designate this group of illnesses because intellectual deterioration was a common feature and the illness usually occurred in young people (Hamilton,1984).
• Bleuler coined the term schizophrenia in 1911.
• According to him, the disease is characterized by a specific type of alteration of thinking, feeling, and relation to external world, which appears nowhere else in this particular fashion. He said that certain symptoms of schizophrenia are present at all times and in every case. Here he is referring to the so-called basic symptoms. Accessory symptoms on the other had may also occur in other illnesses (Bleuler, 1950). The basic symptoms were characterized by the four A’s
• Ambivalence
• Autism
• Affect disturbances
• Association disturbances

• Schneider wrote that the presence of delusional perception excludes a reactive experience and always indicates a true psychosis, which in practical terms is a schizophrenic illness. If the symptom is present in a non-organic psychosis, then we call that psychosis as schizophrenia as opposed to cyclothymic psychosis or reactive psychosis in abnormal personality (Hamilton, 1984).
EVOLUTION OF THE CONCEPT OF FRS• Schneider reported that the presence of FRS always signifies
schizophrenia but first rank symptoms need not always be present in schizophrenia. The search for pathognomic symptoms among positive phenomena is the hallmark of Schneider’s clinical psychopathology (Monti, 1996).
• However Schneider had given few statistics to demonstrate, not how he arrived at his choice of FRS but how the use of FRS led to clear cut diagnosis in most cases (Schneider, 1980).
• In FRS, the use of the term ‘symptoms’ is somewhat idiosyncratic (Boyle, 1990). Patients do not complain it as a symptom of illness (Crichton, 1996). FRS is referred to a more or less characteristic but invariably detectable feature of a purely psychopathological ‘state course complex’ (Schneider, 1980).
• According to some authors (Huber, 1994), Schneider’s personal prestige also contributed to the success of his concept of FRS. In 1931, Schneider became Director of German Research Institute for Psychiatry in Munich founded by Kraepelin and led the honorary professorship at the University of Munich 1934 onward (Huber 1994).

CONCEPTS AND DEFINITION
• FRS deals with mainly delusions and hallucinations. Firstrank symptoms were regarded as primary symptoms.Schneider said, “From the standpoint of psychopathology,primary symptoms are final and irreducible” (Sims, 1991).
• According to Jasper (1968) “If we try to get some closerunderstanding of these primary experiences of delusion,we soon find we cannot really appreciate these quite alienmodes of experience. They remain largelyincomprehensible, unreal and beyond our understanding.

Schneider formulated what he considered to be pathognomic of first rank symptoms of
schizophrenia (Schneider, 1959).
1.Audible thoughts (voices speaking out his thoughts aloud).2.Voices arguing (Referring to the patient in 3rd person)3.Voices commenting on one’s actions.4.Thought withdrawal5.Thought insertion6.Thought broadcasting7.Made volition.8.Made affect9.Made impulse10.Somatic passivity (experiencing externally controlled body changes)11.Delusional perception (a real percept elaborated in a delusional way)
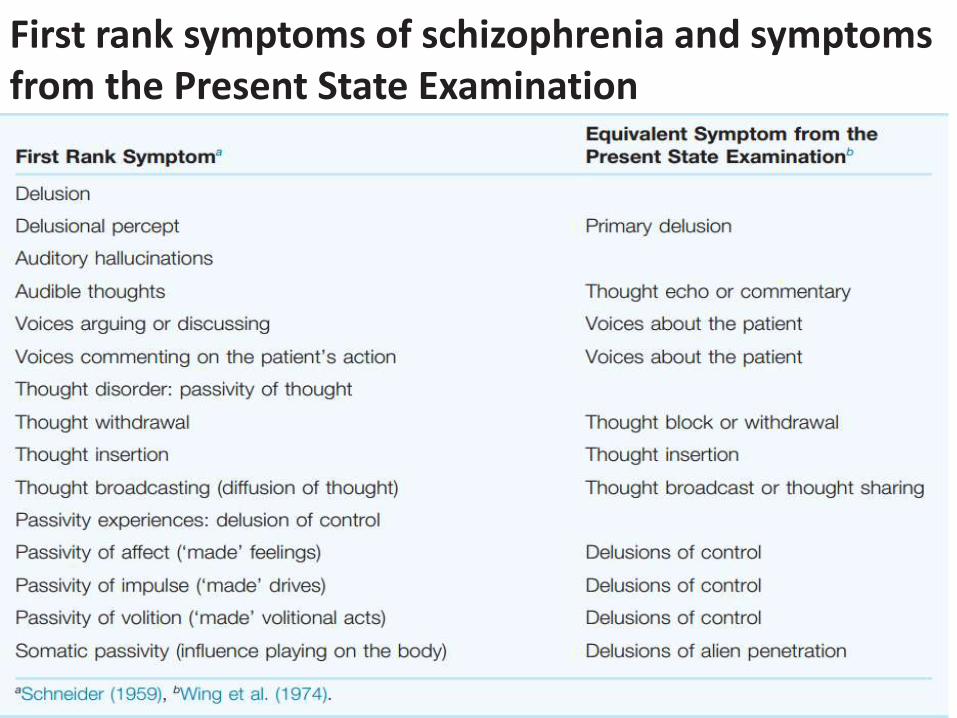
First rank symptoms of schizophrenia and symptoms from the Present State Examination

1.Audible thoughts - is the patient’s experience of hearing his own thoughts said out loud. The patient may hear people repeating his thoughts out loud just after he has thought them, answering his thoughts, talking about them having said them audibly or saying aloud what he is about to think so that his thoughts repeat the voices.
A 35-year-old painter heard a quiet voice with ‘an Oxford accent’, which he attributed to the BBC. The volume was slightly lower than that of normal conversation and could be heard equally well with either ear. He could locate its source at the right mastoid process. The voice would say, ‘I can’t stand that man, the way he holds his hand he looks like a poof’…..
He immediately experienced whatever the voice wassaying as his own thoughts, to the exclusion of all otherthoughts. When he read the newspaper the voice wouldspeak aloud whatever his eyes fell on. He had not time to think of what he was reading before it was uttered aloud.(Mellor, 1970: 16)
2.Voices arguing - Voices heard arguing with each other implies two or more hallucinatory voices quarrelling or discussing with each other. The patient usually features in the third person in the content of these arguing voices.
A 24-year-old male patient reported hearing voices coming from the nurse’s office. One voice, deep in pitch and roughly spoken, repeatedly said, ‘G.T. is a bloody paradox’, andanother, higher in pitch, said, ‘He is that, he should be locked up.’ A female voice occasionally interrupted, saying ‘He is not, he is a lovely man.’ (Mellor, 1970: 16)
3.Voices commenting - Hallucinatory voices giving a running commentary on the patient’s activities occur and are of first rank. The time sequence of the commentary may be such that it takes place just before, during or after the patient’s activities. The patient does not know that his particular perception is unique, that other people do not share his perceptual experience. The abnormal thing about voices commenting is that they should be experienced as perceptions and as coming from outside the self.
A 41-year-old housewife heard a voice coming from the house across the road… The voice went on incessantly in a flat monotone describing everything she was doing, with an admixture of critical comments. ‘She is peeling potatoes, got hold of the peeler, she does not want that potato, she isputting it back, because she thinks it has a knobble like a penis, she has a dirty mind, she is peeling potatoes, now she is washing them.’ (Mellor, 1970: 16)

4.Thought withdrawal- In thought withdrawal, it is believed by the patient that his thoughts are in some way being taken out of his mind; he has some feeling of loss resulting from this process. It may be coupled with other thought passivity experiences.
A 22-year-old woman said, ‘I am thinking about my mother, and suddenly my thoughts are sucked out of my mind by a phrenological vacuum extractor, and there is nothing in my mind, it is empty.’ (Mellor, 1970: 16)

5.Thought insertion- experiences thoughts that do not have the feeling of familiarity, of being his own, but he feels that they have been put in his mind, without his volition, from outside himself.
A 29-year-old housewife said, ‘I look out of the window and I think the garden looks nice and the grass looks cool, but the thoughts of Eamonn Andrews come into my mind. There are no other thoughts there, only his ….He treats my mind like a screen and flashes his thoughts onto it like you flash a picture.’ (Mellor, 1970: 17)

6.Thought broadcasting-the patient experiences his thoughts withdrawn from his mind and then, in some way, made public and projected over a wide area. The explanation he gives for how this can occur will, as usual for the content of a delusion, depend on his background culture and predominant interests.
A 21-year-old student said, ‘As I think, my thoughts leave my head on a type of mental ticker-tape. Everyone around has only to pass the tape through their mind and they know my thoughts.’ (Mellor, 1970: 17)
7.Made volition-passivity of volition the patient feels that it is not his will that carried out the action.
A 29-year-old shorthand typist described her actions as follows, ‘when I reach my hand for the comb it is my hand and arm which move, and my fingers pick up the pen, but I don’t control them… I sit there wanting them to move, and they are quite independent, what they do is nothing to do with me … Iam just a puppet who is manipulated by cosmic strings. When the strings are pulled my body moves and I can’t prevent it.’(Mellor, 1970: 17)
8.Made affect-Passivity of emotion occurs when the affect that the patient experiences does not seem to him to be his own. He believes that he has been made to feel it.
A 23-year-old female patient reported, ‘I cry, tears roll down my cheeks and I look unhappy, but inside I have a cold anger because they are using me in this way, and it is not me who is unhappy, but they are projecting unhappiness onto my brain. They project upon me laughter, for no reason, and you have no idea how terrible it is to laugh and look happy and know it is not your, but their reaction.’(Mellor, 1970: 17)
9.Made impulse-the patient experiences a drive, which he feels is alien, to carry out some motor activity. The impulse may be experienced without the subject carrying out the behaviour. The action is admitted to be the patient’s own, but he feels that the impulse that precipitated him into doing it was not his own.
A 26-year-old engineer emptied the contents of a urine bottle over the ward dinner trolley. He said, ‘The sudden impulse came over me and I must do it. It was not my feeling, it came into me from the X-ray department, that was why I was sent there for implants yesterday. It was nothing to do with me,they wanted it done. So I picked up the bottle and poured it in. It seemed all I could do.’ (Mellor, 1970: 17)

10.Somatic passivity – Somatic passivity is the belief that outside influences are playing on the body. It is not the same as haptic hallucination, but it is a delusional belief that the body is being influenced from outside the self. May occur in association with various somatic hallucinations.
The event is experienced as alien by the patient in that it is not experienced by the patient as his own but inserted into the self from outside.
A 38-year-old man had jumped from a bedroom window, injuring his right knee which was very painful. He described his physical experience as, ‘The sun-rays are directed by US army satellites in an intense beam which I can feel entering the centre of my knee and then radiating outwards causingthe pain.’ (Mellor, 1970: 16)
The terms disorders of passivity made experiences delusions of control disorders of personal activity Are in practice synonymous and interchangeable.
Passivity experiences are those events in the realm of sensation, feeling, drive and volition that are experienced as made or influenced by others.
They have been well described as delusions of control, because the patient’s experience of the event being made to occur takes the form of delusion.
11.Delusional perception - The only type of delusion that is regarded as of first rank is a delusional perception.A normal perception delusionally interpreted and regarded as being highly significant to the patient.
A woman said, ‘every night blood is being injected out of my arms [sic]’. When asked for her evidence, she explained that she had little brown spots on her arms and therefore knew that she was being injected. The interviewer looked at the spots on her arms, rolled up his sleeve and showed her spots identical in appearance on his own arm. He said that they had been on his arm as long as he could remember and were called ‘freckles’. She agreed that both sets of spots looked similar and accepted his explanation of his own spots, but she still insisted that her freckles proved that she was being injected in her sleep.
As per Schneider, there were less important criteria for the diagnosis of schizophrenia other than FRS and he termed them as second rank symptoms. Those are:
Other hallucinations Delusional notionsPerplexityDepressed or elated mood,Experiences of flattened feelings.
Other abnormal modes of expression eg., disorder of speech and other motor manifestations were known as third rank symptoms.

THANK YOU