scaphoid nonunions treated with 2 headless compression screws and bone grafting
TRANSCRIPT

From the Department of Orthopaedic Surgery, Duke University MedicaOrthopedic Associates, Durham, NC.
Received for publication November 8, 2013; accepted in revised form
No benefits in any form have been received or will be receiveindirectly to the subject of this article.
Corresponding author: David S. Ruch, MD, Department of OrthoUniversity Medical Center, Medical Center Boulevard, Winston-Sale-mail: [email protected].
0363-5023/14/---0001$36.00/0http://dx.doi.org/10.1016/j.jhsa.2014.02.030
SCIENTIFIC ARTICLE
Scaphoid Nonunions Treated With 2 Headless
Compression Screws and Bone Grafting
Ryan M. Garcia, MD, Fraser J. Leversedge, MD, J. Mack Aldridge, MD,Marc J. Richard, MD, David S. Ruch, MD
Purpose To evaluate union and complication rates associated with the use of 2 headlesscompression screws and bone grafting for the treatment of scaphoid nonunions.
Methods A total of 19 patients (18 male and 1 female) at an average age of 21 years weretreated with open reduction and internal fixation with 2 cannulated, headless, compressionscrews for scaphoid nonunions. Bone grafting techniques included corticocancellous autograftfrom the iliac crest in 14 patients, capsular-based vascularized distal radius graft in 3, andmedial femoral condyle free vascularized bone graft in 2. Patients were treated an average 19months after the injury. Fracture nonunions were at the waist (n ¼ 12), proximal third (n ¼ 5),or distal third (n ¼ 2) of the scaphoid. Dorsal (n ¼ 7) and volar (n ¼ 12) surgical approacheswere used.
Results All fractures had clinical and radiographic evidence of bone union at an average of 3.6months. Postoperative computed tomography scans were available in 13 patients and showedunion without evidence of screw penetration of the scaphoid cortex. No complicationsoccurred in this series, and no revision procedures have been necessary.
Conclusions Our results indicate that the use of 2 headless compression screws for the treatmentof scaphoid nonunions is safe and effective. A variety of bone grafting techniques can be usedwith this technique. The use of 2 compression screws may provide superior biomechanicalstability and ultimately improve outcomes measured with future long-term comparativestudies. (J Hand Surg Am. 2014;-:-e-. Copyright � 2014 by the American Society forSurgery of the Hand. All rights reserved.)
Type of study/level of evidence Therapeutic IV.Key words Fracture, navicular, nonunion, scaphoid, screw.
F RACTURE OF THE SCAPHOID IS A common injury,accounting for 60% of carpal fractures.1 Eightypercent of the scaphoid surface is covered by
cartilage, and 70% to 80% of the blood supply to the
l Center; and Triangle
February 25, 2014.
d related directly or
paedic Surgery, Dukeem, NC 27157-1070;
scaphoid is provided by branches of the radial arteryentering at the dorsal ridge in a predominantlyretrograde manner.2 The unique anatomy and tenuousblood supply to the scaphoid ultimately led to theintroduction of a compression screw in 1984 byHerbert and Fisher3 for the treatment of scaphoidfractures. Since then, newer generations of screwswith the same design mechanics of variable threadpitch have been developed and extensively studiedfor optimal biomechanical strength.4,5 Operative treat-ment of displaced scaphoid fractures and establishednonunions is typically performed with a single vari-able-pitch compression screw. The single screw maynot provide absolute stability, particularly with rota-tion, when considering the complex and multidirectional
� 2014 ASSH r Published by Elsevier, Inc. All rights reserved. r 1

2 SCAPHOID NONUNION AND 2 COMPRESSION SCREWS
movement of the scaphoid during wrist flexion-extension, radial-ulnar deviation, and dart-throwingmotions.6e10 Torsional stability may be furtherenhanced with the use of a derotational Kirschnerwire.11e13 Trumble et al12 advocated the use of atemporary (removed at 8 wk) derotational wire in 34patients treated for scaphoid nonunion. We suspectedthat using 2 headless compression screws wouldfurther increase the torsional stability of fracturefixation and lead to an increased union rate andimproved clinical outcomes.
The objective of this study was to assess theclinical and radiographic union rate in a consecutiveseries of patients treated with 2 cannulated, headless,compression screws for scaphoid nonunions. We alsoaimed to analyze the complication rate associatedwith this method of fixation, including corticalpenetration of either screw. We hypothesized thatunion and complication rates after the treatment ofscaphoid nonunions using 2 headless compressionscrews would be similar to published reports using asingle, centrally placed screw.
MATERIALS AND METHODSWe retrospectively reviewed the medical records andradiographs of 19 consecutive patients with the diag-nosis of scaphoid nonunion, who underwent openreduction, debridement, bone grafting, and internalfixation with 2 cannulated, headless, compressionscrews from August 2009 to September 2012. No pa-tient presenting with a scaphoid nonunion was treatedwith a single headless compression screw during thistime. Eighteen of the patients weremen.All 19 patientswere right handed. Ten operations were performed onthe left wrist and 9 on the right. The average patient ageat the time of surgery was 21 years (SD, 5 y). Patientshad no medical comorbidities, and no patient smoked.Indications for the use of 2 headless, compressionscrews were unstable scaphoid nonunions that demon-strated a scaphoid humpback deformity with an in-creased lateral scapholunate angle, or associated boneloss indicating rotational instability. Our rationale forthe use of 2 screws was to provide multiple points offixation in a series of unstable nonunions. Institutionalreview board approval was obtained before the collec-tion of any data.
The average time to surgery from the initial injurywas 19 � 10 months (range, 2e78 mo). Injury mech-anisms included falls on outstretched hands in 8 pa-tients, sporting activities in 7, motorcycle accidents in2, and automobile accidents in 2. Five patients wereinitially treated with cast immobilization for a known
J Hand Surg Am. r V
acute scaphoid fracture, and 2 had previously under-gone open reduction and internal fixation with a singlescaphoid screw. The remaining 12 patients had notsought medical treatment after their injury. Weobserved all patients until we identified clinical andradiographic evidence of fracture union. Any intra-operative or postoperative complication including theneed for revision surgery for any reason was recorded.
Fractures occurred at the scaphoid waist in 12patients, the proximal third in 5, and the distal third in2. According to the classification of Herbert andFisher,3 there were 6 fibrous nonunions (type D1),and 13 pseudoarthroses (type D2). The classificationof each nonunion was made from radiographic im-ages and confirmed intraoperatively. We used a volarwrist approach in 12 patients and a dorsal approach in7; 4 of these had a proximal third fracture, 1 had ascaphoid waist fracture treated with a capsular-basedvascularized distal radius graft, and 2 had humpbackor dorsal intercalated segment deformities. Fourteenpatients received nonvascularized corticocancellousbone grafting from the iliac crest, 3 had a capsular-based vascularized distal radius graft,14 and 2 had avascularized medial femoral condyle free bone graft15
before placement of the 2 screws. Patients treatedwith a free vascularized bone graft had a longeraverage interval from injury to surgery (59 vs 14 mo),which resulted from a delay in referral. Three of thepatients receiving vascularized bone grafts hadproximal third fractures, and 2 had waist fractures. Atthe discretion of the surgeon, an external bone stim-ulator was used immediately postoperatively in 12patients and continued for 4 to 6 weeks. The screwswe used were Trimed (Trimed, Inc, Valencia, CA) (8patients) and combined Acutrak Mini and Acutrak 2Micro (Acumed, Beaverton, OR) (11 patients). Screwdiameters ranged from 2.3 to 3.0 mm, and screwlengths ranged from 18 to 28 mm, with an averagedifference in screw length between the 2 screws of 4mm (range, 0e8 mm). The operating surgeon deter-mined screw manufacturer and size.
All patients underwent similar postoperative man-agement. Theywere immobilized in a thumb spica castin the immediate postoperative period. After 2 weeks,this was changed to a removable thumb spica orthosisand an outpatient therapy program was started. Thetherapy program was then continued, based on patientprogress at the discretion of the operating surgeon.Patients were allowed to progress to full weightbearingafterwe observed clinical and radiographic evidence ofunion.
Radiographic union was confirmed by computedtomography scan at the time of symptom resolution
ol. -, - 2014

SCAPHOID NONUNION AND 2 COMPRESSION SCREWS 3
(13 patients) or by serial radiographs (6 patients).With regard to fracture union, radiographs werecritically assessed for bridging trabeculation andobliteration of the prior fracture line in 3 views. Allpostoperative radiographs were reviewed first by theperforming surgeon then by a senior musculoskeletalradiologist who was blinded to the study protocol.Available computed tomography scans were alsocritically analyzed for cortical penetration of eitherscrew. Patients were assessed for complications orneed for a revision procedure, and for their return towork and level of sporting activity. Visual analogpain scores on a 10-point scale were recorded (with0 representing no pain and 10 representing the worsepossible pain) as part of each routine postoperativevisit.
Operative technique
We used a volar approach for waist and distal thirdfractures and for fractures with humpback deformity.For proximal third fractures, fractures withouthumpback deformity, and fractures for which acapsular-based distal radius vascularized bone graftwas planned, a dorsal approach was used. We openedthe nonunion site with dental picks. The fibrous tissueand necrotic bone was debrided with curets or a high-speed burr with constant irrigation. The fracturefragments were derotated and reduced using guide-wires as joysticks. The scaphoid cavity was carefullymeasured, notched, and prepared to accept the chosenbone graft. With the graft in place, the first wire forguiding a cannulated screw was inserted. The secondwire was then inserted adjacent to the first but sepa-rated in the dorsal-volar plane by a minimum distanceof the diameter of the planned screws (Fig. 1). Bothguidewires were positioned to cross perpendicular tothe fracture line. In some fracture patterns (longoblique or horizontal), it was not be possible to orientboth screws perpendicular to the fracture line withoutscrew contact. In these scenarios, we placed the firstscrew perpendicular to the fracture line. When usingthe volar approach, we typically inserted the moredorsal guidewire first, which had a lesser tendency toobstruct the placement of the second guidewire. Incircumstances in which our planned dorsal guidewireended up in a volar position, it was not repositioned,but rather, the second guidewire was simply insertedmore dorsally. The first screw was then inserted whilemaintaining the second guidewire to hold the reduc-tion of the fracture. The length of each screw was thenmeasured based on the available subchondral bone,and the longest possible screw without cortical pene-tration was chosen. Bone screws were then inserted in
J Hand Surg Am. r V
the standard fashion (Fig. 1). The final diameter andlength of screws placed from distal to proximal weresimilar to those placed proximal to distal.
RESULTSAll 19 fracture nonunions had clinical and radiographicevidence of fracture union after an average of 3.6months (range, 2e8 mo). Average time to union forpatients treated with vascularized bone grafting was 5months (range, 4e6 mo). This was noted radiograph-ically by bridging trabeculation and obliteration of thefracture line. All patients demonstrated resolution ofpreoperative pain and dysfunction. Computerized to-mography scans reviewed in 13 patients demonstratedno evidence of cortical penetration of either screw(Figs. 2, 3). Computed tomography scans and radio-graphs in all patients did not demonstrate evidence ofscrew loosening or migration, and proximal poleavascular necrosis did not occur (Figs. 2, 3).
No cases of infection or postoperative complica-tion requiring a revision procedure occurred. Allpreviously employed patients returned to their pre-injury level of work without restrictions. All patientsinterested in returning to sporting activities were ableto return to their previous level of play. The averagevisual analog pain score at the time of fracture unionfor all patients was 0.5 (range, 0e3).
DISCUSSIONThe introduction of the headless compression screw byHerbert and Fisher3 in 1984 revolutionized the treat-ment of scaphoid fractures and nonunions. High unionrates, quicker functional recovery, and low morbidityhave been reported after both open and percutaneousapproaches using a single screw.16e19 In this cohort of19 patients treated with 2 screws and bone grafting, allfracture nonunions had clinical and radiographic evi-dence of union at a mean of 4months. Our union rate iscomparable to prior reports of scaphoid nonunionstreated with fracture reduction followed by cortico-cancellous bone grafting with12,20,21 or without22,23 asingle headless compression screw. In addition, nocomplications occurred. This is similar to results re-ported by Rajagopalan et al20 and Cohen et al,21 but incontrast to the 29% complication rate reported byBushnell et al,24who challenged the complication ratesof earlier reports while detailing 5major complicationsin 24 patients.
We recognize a number of limitations. Ours was aretrospective study of a nonrandomized patient pop-ulation; thus, selection bias may have been an influ-encing factor. Our patient population was also small,
ol. -, - 2014

FIGURE 1: A, B Intraoperative fluoroscopy image demonstrating guidewire pin placement before to insertion of 2 screws. Central axisscrew placement is not desired when 2 screws are planned. The guidewires should be separated at a minimum distance as the diameter ofthe planned screw. Separation of the screws is mainly in the dorsal-volar plane. C, D Anteroposterior and lateral image after finalinsertion of 2 screws.
4 SCAPHOID NONUNION AND 2 COMPRESSION SCREWS
which may have led to small-sample bias. Bonegrafting techniques were not randomized and weredetermined by the operating surgeon. Although avariety of bone grafting techniques were used, allwere compatible with using 2 screws dependent onthe screw sizes chosen. Even with the various bonegrafts in place, the smallest diameter screws availablewere successfully positioned adjacent to each other inall patients. Clinical and radiographic follow-up waslimited to the short- and mid-term. The wide range ofunion times may be explained by patient return forfollow-up. Two outlying patients treated with non-vascularized bone grafting returned to clinic 6 and 8months after their initial 2- or 3-week postoperativevisit. Our goal was to ensure comparable union andcomplication rates of this technique with respect to
J Hand Surg Am. r V
published series using single compression screws.We recognize that long-term follow-up and func-tional outcome scores are still needed. Computedtomography scans were not obtained in all patients, atthe discretion of the operating surgeon. Therefore, wecannot definitively conclude that cortical penetrationdid not occur in the patients receiving only radio-graphs. Finally, magnetic resonance imaging was notroutinely obtained to evaluate for proximal polevascular insufficiency.
Biomechanical studies have extensively investi-gated bending strength and resistance in scaphoidfracture constructs for flexion-extension stability, butless often for torsional stability.5,25e30 We believe thattorsional resistance in fracture stabilization is impor-tant when considering the complex, multidirectional
ol. -, - 2014
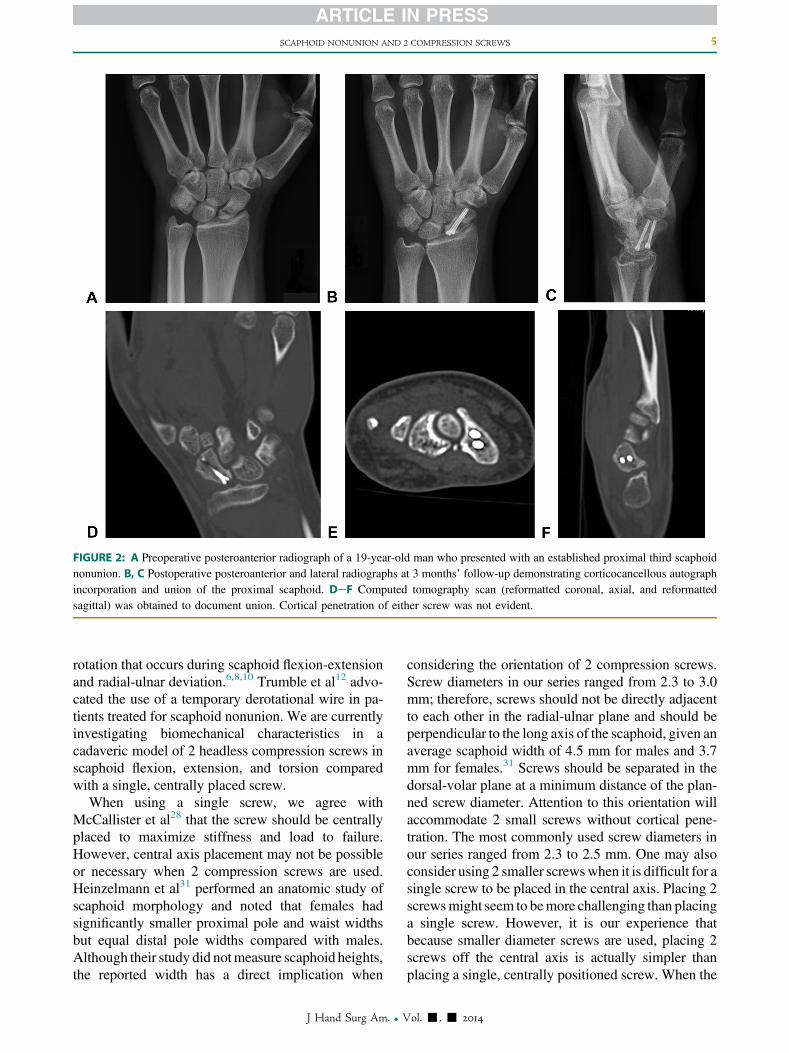
FIGURE 2: A Preoperative posteroanterior radiograph of a 19-year-old man who presented with an established proximal third scaphoidnonunion. B, C Postoperative posteroanterior and lateral radiographs at 3 months’ follow-up demonstrating corticocancellous autographincorporation and union of the proximal scaphoid. DeF Computed tomography scan (reformatted coronal, axial, and reformattedsagittal) was obtained to document union. Cortical penetration of either screw was not evident.
SCAPHOID NONUNION AND 2 COMPRESSION SCREWS 5
rotation that occurs during scaphoid flexion-extensionand radial-ulnar deviation.6,8,10 Trumble et al12 advo-cated the use of a temporary derotational wire in pa-tients treated for scaphoid nonunion. We are currentlyinvestigating biomechanical characteristics in acadaveric model of 2 headless compression screws inscaphoid flexion, extension, and torsion comparedwith a single, centrally placed screw.
When using a single screw, we agree withMcCallister et al28 that the screw should be centrallyplaced to maximize stiffness and load to failure.However, central axis placement may not be possibleor necessary when 2 compression screws are used.Heinzelmann et al31 performed an anatomic study ofscaphoid morphology and noted that females hadsignificantly smaller proximal pole and waist widthsbut equal distal pole widths compared with males.Although their study did notmeasure scaphoid heights,the reported width has a direct implication when
J Hand Surg Am. r V
considering the orientation of 2 compression screws.Screw diameters in our series ranged from 2.3 to 3.0mm; therefore, screws should not be directly adjacentto each other in the radial-ulnar plane and should beperpendicular to the long axis of the scaphoid, given anaverage scaphoid width of 4.5 mm for males and 3.7mm for females.31 Screws should be separated in thedorsal-volar plane at a minimum distance of the plan-ned screw diameter. Attention to this orientation willaccommodate 2 small screws without cortical pene-tration. The most commonly used screw diameters inour series ranged from 2.3 to 2.5 mm. One may alsoconsider using 2 smaller screwswhen it is difficult for asingle screw to be placed in the central axis. Placing 2screwsmight seem to bemore challenging than placinga single screw. However, it is our experience thatbecause smaller diameter screws are used, placing 2screws off the central axis is actually simpler thanplacing a single, centrally positioned screw. When the
ol. -, - 2014
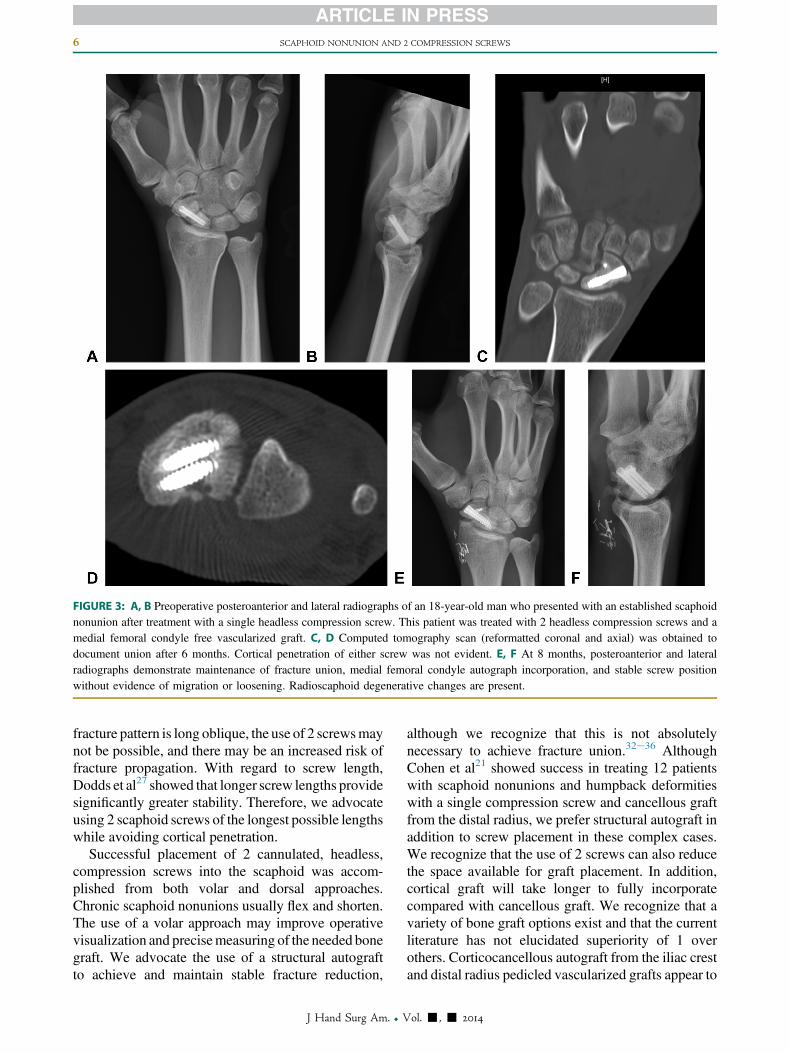
FIGURE 3: A, B Preoperative posteroanterior and lateral radiographs of an 18-year-old man who presented with an established scaphoidnonunion after treatment with a single headless compression screw. This patient was treated with 2 headless compression screws and amedial femoral condyle free vascularized graft. C, D Computed tomography scan (reformatted coronal and axial) was obtained todocument union after 6 months. Cortical penetration of either screw was not evident. E, F At 8 months, posteroanterior and lateralradiographs demonstrate maintenance of fracture union, medial femoral condyle autograph incorporation, and stable screw positionwithout evidence of migration or loosening. Radioscaphoid degenerative changes are present.
6 SCAPHOID NONUNION AND 2 COMPRESSION SCREWS
fracture pattern is long oblique, the use of 2 screwsmaynot be possible, and there may be an increased risk offracture propagation. With regard to screw length,Dodds et al27 showed that longer screw lengths providesignificantly greater stability. Therefore, we advocateusing 2 scaphoid screws of the longest possible lengthswhile avoiding cortical penetration.
Successful placement of 2 cannulated, headless,compression screws into the scaphoid was accom-plished from both volar and dorsal approaches.Chronic scaphoid nonunions usually flex and shorten.The use of a volar approach may improve operativevisualization and precisemeasuring of the needed bonegraft. We advocate the use of a structural autograftto achieve and maintain stable fracture reduction,
J Hand Surg Am. r V
although we recognize that this is not absolutelynecessary to achieve fracture union.32e36 AlthoughCohen et al21 showed success in treating 12 patientswith scaphoid nonunions and humpback deformitieswith a single compression screw and cancellous graftfrom the distal radius, we prefer structural autograft inaddition to screw placement in these complex cases.We recognize that the use of 2 screws can also reducethe space available for graft placement. In addition,cortical graft will take longer to fully incorporatecompared with cancellous graft. We recognize that avariety of bone graft options exist and that the currentliterature has not elucidated superiority of 1 overothers. Corticocancellous autograft from the iliac crestand distal radius pedicled vascularized grafts appear to
ol. -, - 2014

SCAPHOID NONUNION AND 2 COMPRESSION SCREWS 7
have equivalent union rates and clinical success.37,38
Jones et al39 reported on a small series of scaphoidnonunions treated with a medial femoral condyle freegraft and showed improved union rates and shortenedtime to union compared with a pedicled distal radiusgraft. They later reported promising results in patientswith avascular necrosis and carpal collapse using asimilar technique.40 With the numbers available in ourpresented series, we cannot determine the best bonegraft technique. Regardless of which structural bonegraft technique is chosen, bone healing is required at 2interfaces that may benefit from improved torsionalstability provided by 4 points offixationwhen 2 screwsare used.
A large, multicenter trial directly comparing theclinical outcomes of patients treated with either 1 or 2headless compression screws remains necessary.
REFERENCES
1. Hove LM. Epidemiology of scaphoid fractures in Bergen, Norway.Scand J Plast Reconstr Surg Hand Surg. 1999;33(4):423e426.
2. Gelberman RH, Menon J. The vascularity of the scaphoid bone.J Hand Surg Am. 1980;5(5):508e513.
3. Herbert TJ, Fisher WE. Management of the fractured scaphoid usinga new bone screw. J Bone Joint Surg Br. 1984;66(1):114e123.
4. Beadel GP, Ferreira L, Johnson JA, et al. Interfragmentarycompression across a simulated scaphoid fracture—analysis of 3screws. J Hand Surg Am. 2004;29(2):273e278.
5. Newport ML, Williams CD, Bradley WD. Mechanical strength ofscaphoid fixation. J Hand Surg Br. 1996;21(1):99e102.
6. Crisco JJ, Coburn JC, Moore DC, et al. In vivo radiocarpal kine-matics and the dart thrower’s motion. J Bone Joint Surg Am.2005;87(12):2729e2740.
7. Kobayashi M, Berger RA, Nagy L, et al. Normal kinematics of carpalbones: a three-dimensional analysis of carpal bone motion relative tothe radius. J Biomech. 1997;30(8):787e793.
8. Moojen TM, Snel JG, Ritt MJ, et al. Scaphoid kinematics in vivo.J Hand Surg Am. 2002;27(6):1003e1010.
9. Wolfe SW, Neu C, Crisco JJ. In vivo scaphoid, lunate, and capitatekinematics in flexion and in extension. J Hand Surg Am. 2000;25(5):860e869.
10. Short WH, Werner FW, Fortino MD, et al. Analysis of the kinematicsof the scaphoid and lunate in the intact wrist joint. Hand Clin.1997;13(1):93e108.
11. Adams BD, Blair WF, Reagan DS, et al. Technical factors related toHerbert screw fixation. J Hand Surg Am. 1988;13(6):893e899.
12. Trumble TE, Clarke T, Kreder HJ. Non-union of the scaphoid:treatment with cannulated screws compared with treatment withHerbert screws. J Bone Joint Surg Am. 1996;78(12):1829e1837.
13. Manske PR, McCarthy JA, Strecker WB. Use of the Herbert bonescrew for scaphoid nonunions. Orthopedics. 1988;11(12):1653e1661.
14. Sotereanos DG, Darlis NA, Dailiana ZH, et al. A capsular-basedvascularized distal radius graft for proximal pole scaphoid pseu-darthrosis. J Hand Surg Am. 2006;31(4):580e587.
15. Jones DB Jr, Burger H, Bishop AT, et al. Treatment of scaphoidwaist nonunions with an avascular proximal pole and carpal collapse:surgical technique. J Bone Joint Surg Am. 2009;91(suppl 2):169e183.
16. Fowler JR, Ilyas AM. Headless compression screw fixation ofscaphoid fractures. Hand Clin. 2010;26(3):351e361, vi.
J Hand Surg Am. r V
17. Slade JF III, Gillon T. Retrospective review of 234 scaphoid fracturesand nonunions treated with arthroscopy for union and complications.Scand J Surg. 2008;97(4):280e289.
18. Ring D, Jupiter JB, Herndon JH. Acute fractures of the scaphoid.J Am Acad Orthop Surg. 2000;8(4):225e231.
19. Rettig ME, Raskin KB. Retrograde compression screw fixation ofacute proximal pole scaphoid fractures. J Hand Surg Am. 1999;24(6):1206e1210.
20. Rajagopalan BM, Squire DS, Samuels LO. Results of Herbert-screwfixation with bone-grafting for the treatment of nonunion of thescaphoid. J Bone Joint Surg Am. 1999;81(1):48e52.
21. Cohen MS, Jupiter JB, Fallahi K, et al. Scaphoid waist nonunion withhumpback deformity treated without structural bone graft. J HandSurg Am. 2013;38(4):701e705.
22. Green DP. The effect of avascular necrosis on Russe bone graftingfor scaphoid nonunion. J Hand Surg Am. 1985;10(5):597e605.
23. Russe O. Fracture of the carpal navicular: diagnosis, non-operative treat-ment, and operative treatment. J Bone Joint Surg Am. 1960;42:759e768.
24. Bushnell BD, McWilliams AD, Messer TM. Complications in dorsalpercutaneous cannulated screw fixation of nondisplaced scaphoidwaist fractures. J Hand Surg Am. 2007;32(6):827e833.
25. Rankin G, Kuschner SH, Orlando C, et al. A biomechanical evalu-ation of a cannulated compressive screw for use in fractures of thescaphoid. J Hand Surg Am. 1991;16(6):1002e1010.
26. Takase K, Yamamoto K. Mechanical strength and optimal site ofplacement of a threaded bone screw assessed on the basis of thescrew breakage for non-union of the scaphoid: a biomechanicalstudy. Hand Surg. 2005;10(2e3):225e230.
27. Dodds SD, Panjabi MM, Slade JF III. Screw fixation of scaphoidfractures: a biomechanical assessment of screw length and screwaugmentation. J Hand Surg Am. 2006;31(3):405e413.
28. McCallister WV, Knight J, Kaliappan R, et al. Central placement ofthe screw in simulated fractures of the scaphoid waist: a biome-chanical study. J Bone Joint Surg Am. 2003;85(1):72e77.
29. Toby EB, Butler TE, McCormack TJ, et al. A comparison of fixationscrews for the scaphoid during application of cyclical bending loads.J Bone Joint Surg Am. 1997;79(8):1190e1197.
30. Carter FM Jr, Zimmerman MC, DiPaola DM, et al. Biomechanicalcomparison of fixation devices in experimental scaphoid osteotomies.J Hand Surg Am. 1991;16(5):907e912.
31. Heinzelmann AD, Archer G, Bindra RR. Anthropometry of the hu-man scaphoid. J Hand Surg Am. 2007;32(7):1005e1008.
32. Stark HH, Rickard TA, Zemel NP, et al. Treatment of ununitedfractures of the scaphoid by iliac bone grafts and Kirschner-wirefixation. J Bone Joint Surg Am. 1988;70(7):982e991.
33. Bindra R, Bednar M, Light T. Volar wedge grafting for scaphoidnonunion with collapse. J Hand Surg Am. 2008;33(6):974e979.
34. Daly K, Gill P, Magnussen PA, et al. Established nonunion of thescaphoid treated by volar wedge grafting and Herbert screw fixation.J Bone Joint Surg Br. 1996;78(4):530e534.
35. FernandezDL.Anterior bone grafting and conventional lag screwfixationto treat scaphoid nonunions. J Hand Surg Am. 1990;15(1):140e147.
36. Fernandez DL. A technique for anterior wedge-shaped grafts forscaphoid nonunions with carpal instability. J Hand Surg Am.1984;9(5):733e737.
37. Christodoulou L, Chamberlain ST. Internal fixation of scaphoid frac-tures with an AO mini-fragment lag screw, using temporary interoper-ative AO mini external fixation. J Hand Surg Br. 1999;24(6):676e678.
38. Tambe AD, Cutler L, Murali SR, et al. In scaphoid non-union, doesthe source of graft affect outcome? Iliac crest versus distal end ofradius bone graft. J Hand Surg Br. 2006;31(1):47e51.
39. Jones DB Jr, Burger H, Bishop AT, et al. Treatment of scaphoidwaist nonunions with an avascular proximal pole and carpal collapse:a comparison of two vascularized bone grafts. J Bone Joint Surg Am.2008;90(12):2616e2625.
40. Jones DB Jr, Moran SL, Bishop AT, et al. Free-vascularized medialfemoral condyle bone transfer in the treatment of scaphoid non-unions. Plast Reconstr Surg. 2010;125(4):1176e1184.
ol. -, - 2014