sawc iss 723 - debridement - no animation for …iss+723+-+deb... · non-sequential progression...
TRANSCRIPT
Faculty
Ira M. Herman, PhD, FAPWCAProfessor and Director
Program in Cell, Molecular and Developmental BiologyCenter for Innovations in Wound Healing Research
Tufts University School of MedicineBoston, Massachusetts
Jeffrey D. Lehrman, DPM, FASPS, MAPWCAAdjunct Clinical Professor
Temple University School of Podiatric MedicinePodiatrist, Foot & Ankle Specialists of Delaware County
Springfield, Pennsylvania
Lee C. Ruotsi, MD, CWS, UHMCatholic Health System
Medical Director, Advanced Wound Healing CentersCheektowaga, New York
Disclosures
Dr. Herman: Grant/Research—Tufts University; Research—Smith & Nephew
Dr. Lehrman: Board of Directors—American Society of Podiatric Surgeons, American Professional Wound Care Association; Consultant—Endo, Smith & Nephew, Molnlycke, MTF; Speakers’ Bureau—BSN Medical, Smith & Nephew
Dr. Ruotsi: Speakers’ Bureau—Organogenesis, Smith & Nephew
Learning Objectives
• Describe the pathophysiology of chronic wounds
• Recognize the importance of aggressive wound management for chronic wounds
• Examine the role of enzymatic debridement as an adjunct to sharp debridement in progressing chronic wounds toward healing
• Recognize the impact of chronic wounds on healthcare costs and patient’s quality of life
Ira M. Herman, PhD, FAPWCAProfessor and DirectorProgram in Cell, Molecular and Developmental BiologyCenter for Innovations in Wound Healing ResearchTufts University School of MedicineBoston, [email protected]
The Chronic Wound Conundrum:Precipitating Factors and Pathophysiology
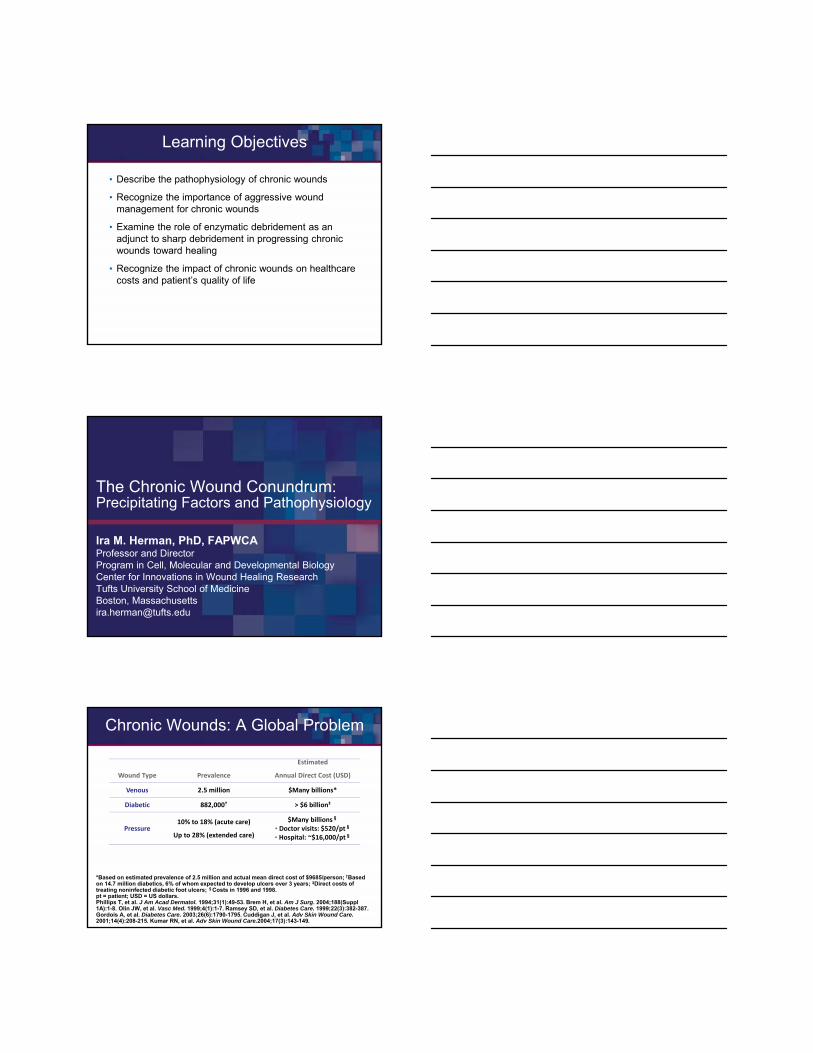
Chronic Wounds: A Global Problem
*Based on estimated prevalence of 2.5 million and actual mean direct cost of $9685/person; †Based on 14.7 million diabetics, 6% of whom expected to develop ulcers over 3 years; ‡Direct costs of treating noninfected diabetic foot ulcers; §Costs in 1996 and 1998. pt = patient; USD = US dollars.Phillips T, et al. J Am Acad Dermatol. 1994;31(1):49-53. Brem H, et al. Am J Surg. 2004;188(Suppl1A):1-8. Olin JW, et al. Vasc Med. 1999;4(1):1-7. Ramsey SD, et al. Diabetes Care. 1999;22(3):382-387. Gordois A, et al. Diabetes Care. 2003;26(6):1790-1795. Cuddigan J, et al. Adv Skin Wound Care. 2001;14(4):208-215. Kumar RN, et al. Adv Skin Wound Care.2004;17(3):143-149.
$Many billions§
• Doctor visits: $520/pt§
• Hospital: ~$16,000/pt§
10% to 18% (acute care)
Up to 28% (extended care)Pressure
> $6 billion‡882,000†Diabetic
$Many billions*2.5 millionVenous
Estimated
Annual Direct Cost (USD)PrevalenceWound Type
Regulation of Wound Healing:Dynamic and Reciprocal Signaling
u-PA = urokinase plasminogen activator; MMP = matrix metalloproteinase; t-PA = tissue plasminogen activator.Schultz GS, et al. Wound Repair Regen. 2011;19(2):134-148.
Growth control:Migratory
and proliferative responses
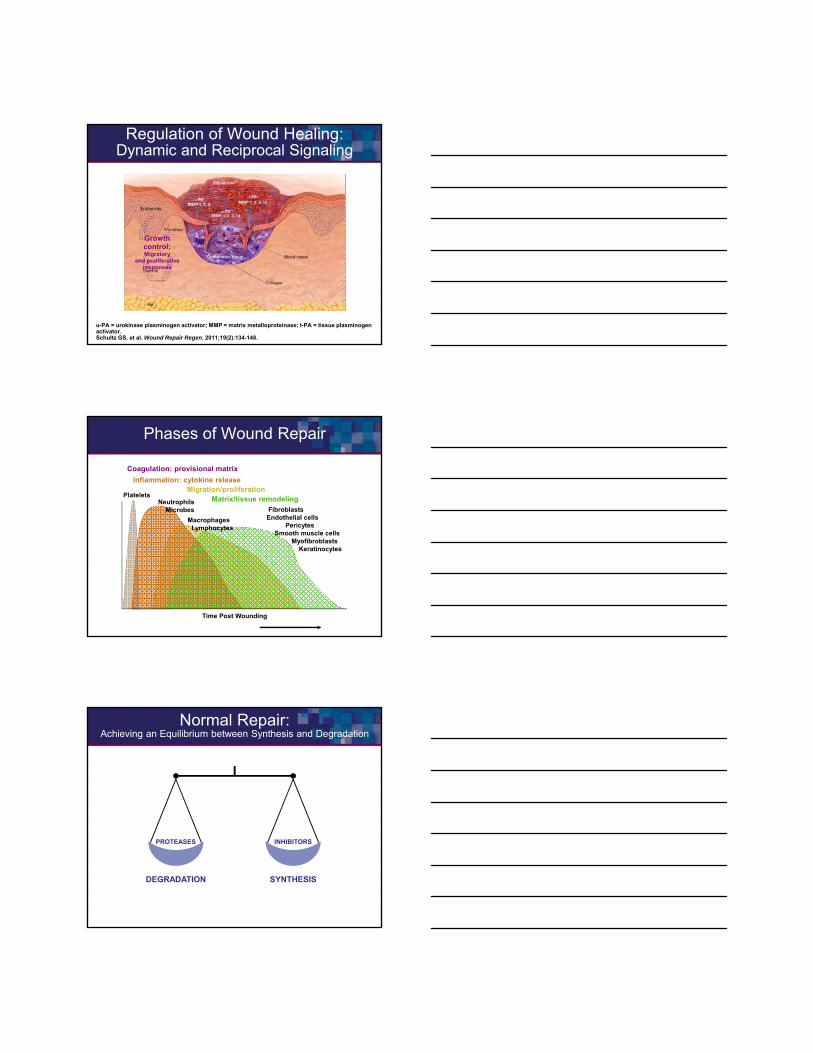
Coagulation: provisional matrix
Inflammation: cytokine releaseMigration/proliferation
Matrix/tissue remodelingPlatelets
Time Post Wounding
Fibroblasts Endothelial cells
PericytesSmooth muscle cells
MyofibroblastsKeratinocytes
MacrophagesLymphocytes
NeutrophilsMicrobes
Phases of Wound Repair
Normal Repair: Achieving an Equilibrium between Synthesis and Degradation
PROTEASES
DEGRADATION
INHIBITORS
SYNTHESIS
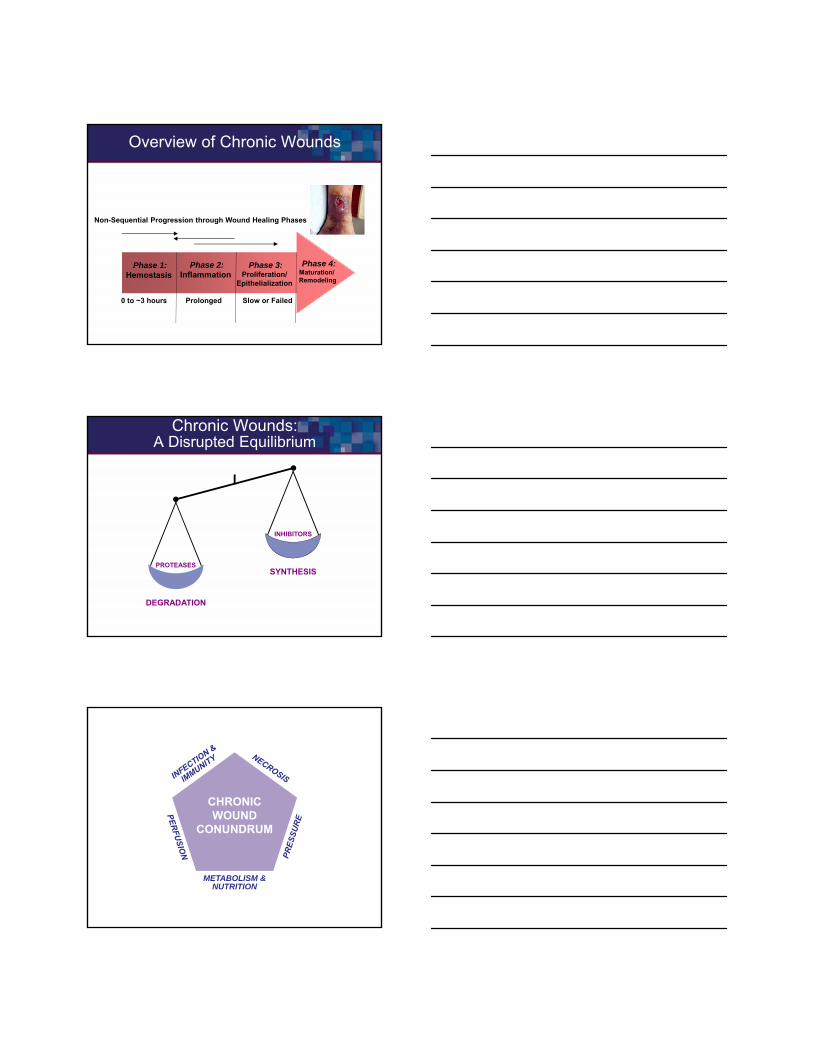
Overview of Chronic Wounds
Phase 1:Hemostasis
Phase 4:Maturation/ Remodeling
Phase 3:Proliferation/
Epithelialization
Phase 2:Inflammation
0 to ~3 hours Prolonged Slow or Failed
Non-Sequential Progression through Wound Healing Phases
PROTEASES
DEGRADATION
INHIBITORS
SYNTHESIS
Chronic Wounds:A Disrupted Equilibrium
CHRONICWOUND
CONUNDRUM
METABOLISM &NUTRITION
CHRONICWOUND
CONUNDRUM
ELEVATEDIMFLAMMATORY
MEDIATORS
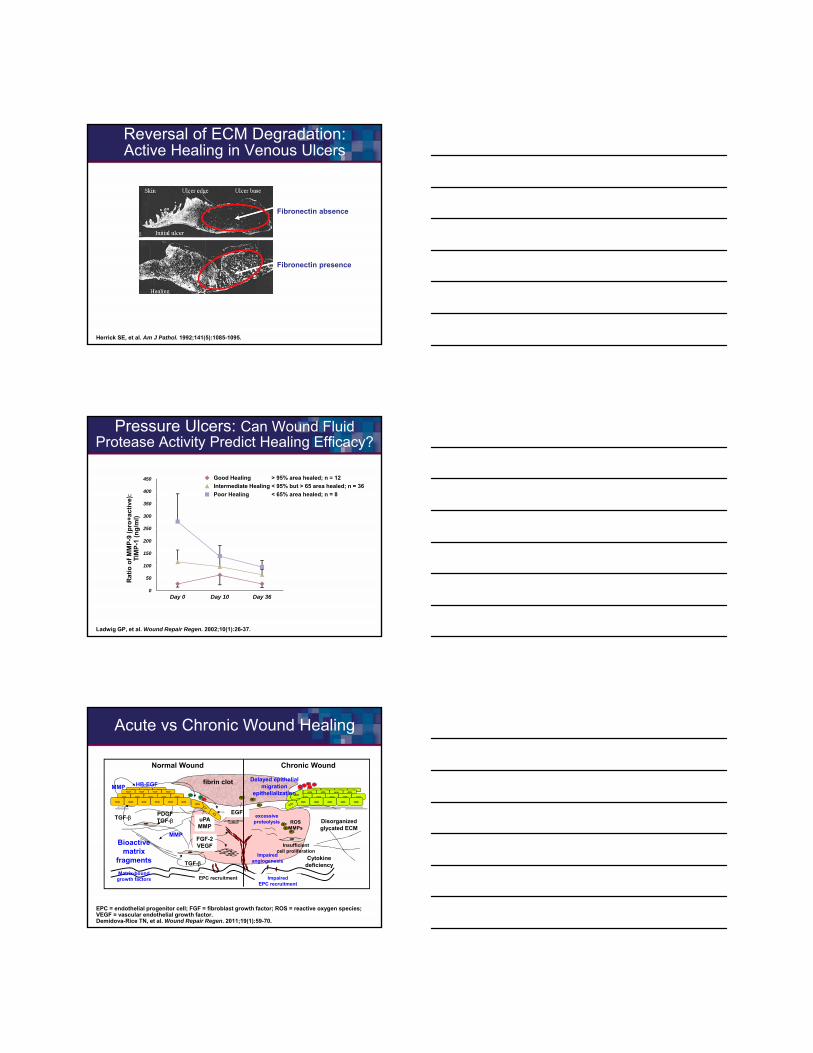
Acute vs Chronic Wound Healing
TIMP = tissue inhibitor of metalloproteinase.
Excessive inflammationMMP production
Matrix degradationCell senescence
Impairedangiogenesis
Cell proliferationApoptosis
TIMP productionMatrix
remodeling
TIME. February 23, 2004.

How Chronic WoundsDiffer from Acute Wounds
• Within chronic wounds, several issues can affect healing, ie, quantity and activity of inflammatory cytokines, MMPs and their inhibitors, all of which can lead to decreased levels of certain growth factors (eg, PDGF, EGF and TGF-β), when compared to acute/ normal wounds
• Bacteria and biofilms contaminating chronic wounds may be deleterious compared to those beneficial bacteria found in acute wounds
• Excessive MMPs can degrade the cytokines, eliminating the mediators of cellular processes that are critical to wound healing
EGF = epidermal growth factor ; PDGF = platelet-derived growth factor; TGF-β = transforming growth factor beta.Robbins SL, et al. Pathologic Basis of Disease. Third Edition. Philadelphia, PA: WB Saunders; 1984:1-85.
Chronic Wounds: Inflammatory Cycle
• Elevated levels of TNF (neutrophils, macrophages)
• Elevated levels of ILs (IL-1β, IL-6)
• Imbalanced protease and inhibitor profiles
– Elevated MMPs
– Decreased TIMPs
• Destruction of key survival agents (growth modulators and receptors)
• Altered microenvironment (ECM)
– Perturbation of cellular responses to injury (migration and growth)
ECM = extracellular matrix; TNF = tumor necrosis factor; IL = interleukin.Robbins SL, et al. Pathologic Basis of Disease. Third Edition. Philadelphia, PA: WB Saunders; 1984:1-85.
Bacterial Signals: Amplify Inflammation
Elevated Proteases–Decreased TIMPs
Immune Surveillance Cells:Elevated Extravasation?
Signaling through the Inflammatory Network:Role of Immune Modulators and Host Enzymes
ICAM = intercellular adhesion molecule; LFA = lymphocyte function; VLA = very late antigen; VCAM = vascular cell adhesion molecule; PMN = ploymorphonuclear neutrophils.Eming SA, et al. J Invest Dermatol. 2007;127(3):514-525.
MMP-1MMP-2MMP-3MMP-9MMP-13
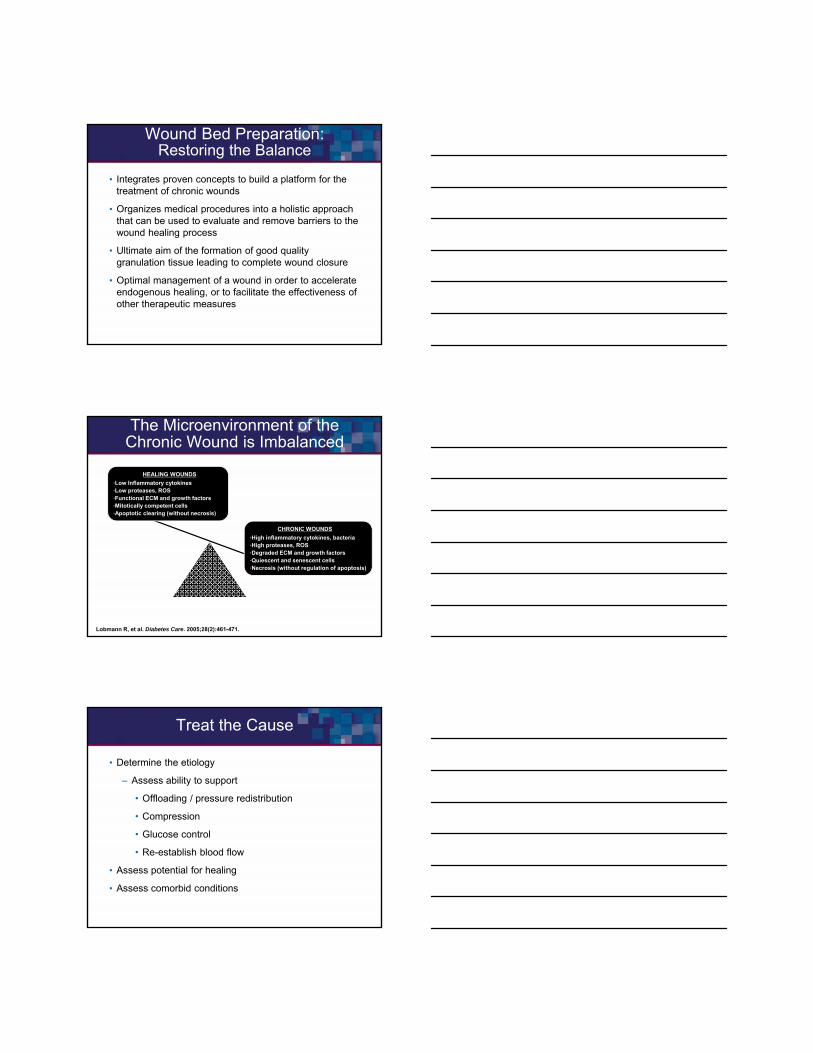
Fibronectin absence
Fibronectin presence
Reversal of ECM Degradation:Active Healing in Venous Ulcers
Herrick SE, et al. Am J Pathol. 1992;141(5):1085-1095.
Pressure Ulcers: Can Wound FluidProtease Activity Predict Healing Efficacy?
Ladwig GP, et al. Wound Repair Regen. 2002;10(1):26-37.
Ra
tio
of
MM
P-9
(p
ro+
ac
tiv
e):
TIM
P-1
(n
g/m
l)
350
450
300
250
200
150
100
0
50
Day 0 Day 10
400
Day 36
Intermediate Healing
Poor Healing
Good Healing
< 95% but > 65 area healed; n = 36
< 65% area healed; n = 8
> 95% area healed; n = 12
MMP
PDGFTGF-TGF-
MMP
TGF-
uPAMMP
EGF
HB-EGF fibrin clot
FGF-2VEGF
EPC recruitment
Bioactive matrix
fragments
Matrix-bound growth factors Impaired
EPC recruitment
excessiveproteolysis ROS
MMPsDisorganizedglycated ECM
Impaired angiogenesis
Delayed epithelial migration
epithelialization
Normal Wound Chronic Wound
Cytokine deficiency
Insufficientcell proliferation
Acute vs Chronic Wound Healing
EPC = endothelial progenitor cell; FGF = fibroblast growth factor; ROS = reactive oxygen species; VEGF = vascular endothelial growth factor.Demidova-Rice TN, et al. Wound Repair Regen. 2011;19(1):59-70.
Lee C. Ruotsi, MD, CWS, UHMCatholic Health SystemMedical Director, Advanced Wound Healing CentersCheektowaga, New York
Importance of Aggressive Wound Management for Chronic Wounds
The Importance of Aggressive Wound Bed Preparation
Triple Aim
Wound Bed Preparation: Restoring the Balance
• Integrates proven concepts to build a platform for the treatment of chronic wounds
• Organizes medical procedures into a holistic approach that can be used to evaluate and remove barriers to the wound healing process
• Ultimate aim of the formation of good quality granulation tissue leading to complete wound closure
• Optimal management of a wound in order to accelerate endogenous healing, or to facilitate the effectiveness of other therapeutic measures
Falanga V. Wounds. 2002;14(2):47-57. Enoch S, et al. Wounds. 2003;15(8):213-229.
The Microenvironment of theChronic Wound is Imbalanced
Lobmann R, et al. Diabetes Care. 2005;28(2):461-471.
HEALING WOUNDS
•Low Inflammatory cytokines•Low proteases, ROS•Functional ECM and growth factors•Mitotically competent cells•Apoptotic clearing (without necrosis)
CHRONIC WOUNDS
•High inflammatory cytokines, bacteria•High proteases, ROS•Degraded ECM and growth factors•Quiescent and senescent cells•Necrosis (without regulation of apoptosis)
Treat the Cause
• Determine the etiology
– Assess ability to support
• Offloading / pressure redistribution
• Compression
• Glucose control
• Re-establish blood flow
• Assess potential for healing
• Assess comorbid conditions
Treat the Cause
• Determine the etiology
– Assess ability to support
• Offloading / pressure redistribution
• Compression
• Glucose control
• Vascular interventions
• Nutritional support
• Assess potential for healing
• Assess comorbid conditions
TIME
• Tissue• Infection• Moist wound environment• Edge Don’t waste it…
Necrotic Tissue
• Devitalized tissue thatsupports the growth of pathological organisms
– Bacteria thrive in presence of necrotic tissue
• Perpetuates inflammatory response
• Acts as a barrier to new tissue growth
Why Debride Non-Viable Tissue?
• To remove dead, devitalized, contaminated tissue or foreign material, senescent cells
• To reduce microbes, toxins, and other substances that inhibit healing
• To provide a clinician the ability to assess the depth of wound and the condition of surrounding tissue
• To remove the physical barrier to healing and reduce bacterial growth
• To adequately prepare for advanced agents, CTPs
• Recommended in all guidelines
CTP = cellular tissue-based product.Weir D, et al. Wound debridement. In: Krasner DL, et al. (Eds.). Chronic Wound Care: A Clinical Source Book for Healthcare Professionals. Fourth Edition. Malvern, PA: HMP Communications; 2007:343-355.
Types of Debridement
Weir D, et al. Wound debridement. In: Krasner DL, et al. (Eds.). Chronic Wound Care: A Clinical Source Book for Healthcare Professionals. Fourth Edition. Malvern, PA: HMP Communications; 2007:343-355.
Strategy
Strategy Description Examples
Surgical (Excisional/Sharp)
Removal by surgical instrumentScalpel, scissors, hydrosurgery,
lasers, curettes,
Mechanical
Removal of necrotic tissue by mechanical means
Wet to dry dressings, hydrotherapy, ultrasound,
abrasion
BiosurgicalSterile larvae selectively digest
necrotic tissue and bacteria
Sterile blowfly or housefly larvae
AutolyticUses the body’s own enzymes to dissolve necrotic tissue; assisted with moisture-retentive dressings
Moisture retentive dressings
EnzymaticTopical application of enzymes
to liquefy necrotic tissueCollagenase
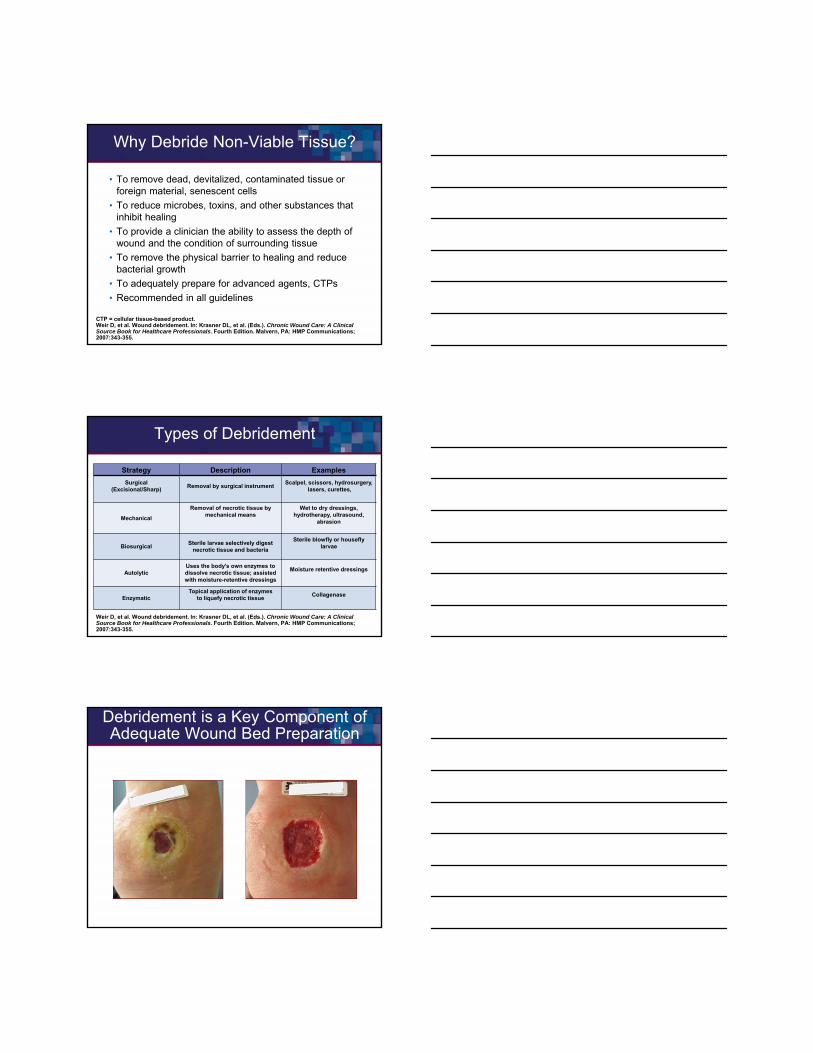
Debridement is a Key Component of Adequate Wound Bed Preparation
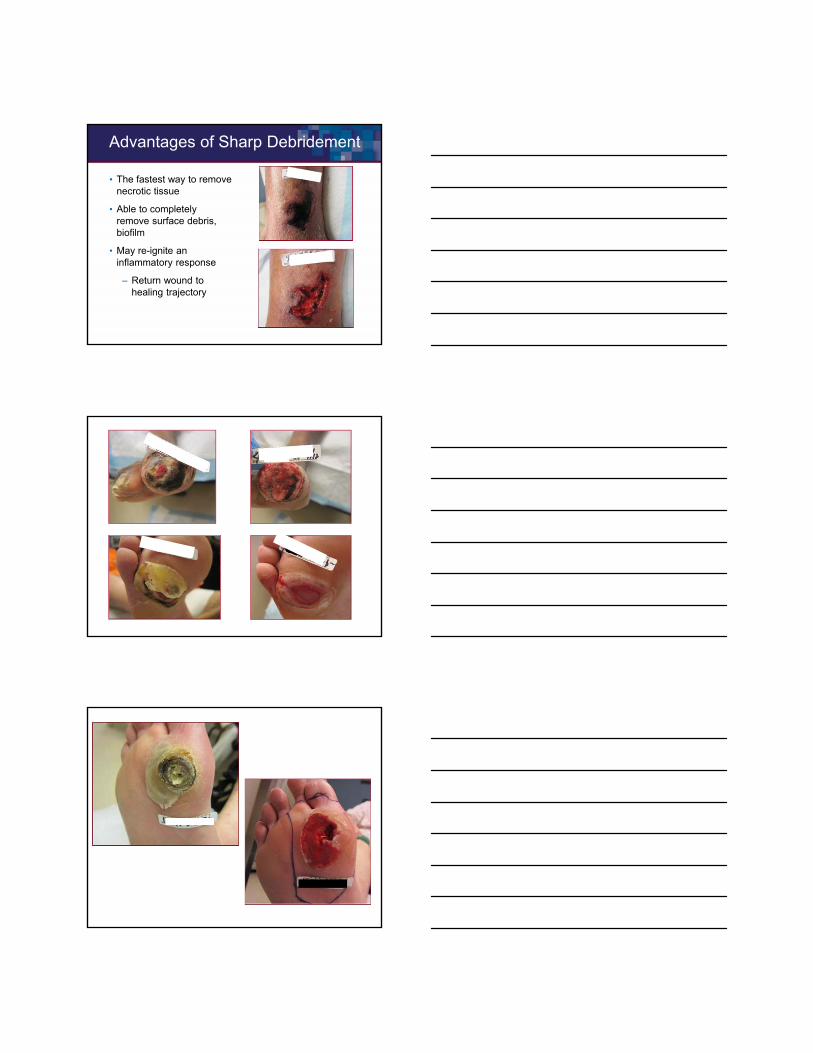
Advantages of Sharp Debridement
• The fastest way to remove necrotic tissue
• Able to completely remove surface debris, biofilm
• May re-ignite an inflammatory response
– Return wound to healing trajectory
Adjunctive Debridement with Collagenase
• Daily debridement adjunct to weekly or bi-weekly sharp debridement
• Exogenously applied agent works directly on devitalized tissue or indirectly by dissolving collagen anchoring devitalized tissue to wound bed
• Little to no effect on healthy collagen or tissue
• Easily applied by patient or caregivers
• Collagenase is the only enzymatic debriding agent approved by the FDA
Collagenase
• Collagenase belongs to a family of MMPs
– Naturally occurring enzymes produced by in response to bacteria, debris, and are produced by activated inflammatory cells and certain wound cells
• Exogenous collagenase is a derived from fermentation by clostridium histolyticum
– Complex biologic that requires a year-long manufacturing process in a sterile environment
– Digests collagen in the necrotic wound environment
– Targets only devitalized collagen
Sibbald GR, et al. Ostomy Wound Manage. 2000;46(11):14-35. Falanga V. Wound Repair Regen. 2000;8(5):347-352.
Collagenase
• Continuously removes necrotic tissue from the wound while allowing normal granulation to proceed
• Selectively attacks and cleaves collagen strands anchoring cellular debris
• Enables it to work from the “bottom up”
Motley TA, et al. Wounds. 2014;26(3):57-64.
Debridement with and without Adjunctive Clostridial Collagenase Ointment
• Objective– Provide descriptive outcomes data regarding
chronic diabetic foot ulcers treated with 6 weeks of serial sharp debridement with or without adjunctive CCO debridement
• Endpoints– Primary
• Percent change in ulcer area from baseline at end of the treatment period (Week 6) and after an additional 6 weeks of follow-up (Week 12)
– Secondary• Wound appearance at Week 6 and Week 12
using a standardized wound assessment toolCCO = Clostridium collagenase ointment.Motley TA, et al. Wounds. 2014;26(3):57-64.
Debridement with and without Adjunctive Clostridial Collagenase Ointment (cont’d)
• Aim was to generate rather than not test a hypothesis based on sample size (N = 55)
• Objective decision making relative to sharp debridement
– Bates-Jensen Wound Assessment Score
• Edges
• Undermining
• Necrotic tissue type and amount
• Exudate type and amount
• Periwound skin color
• Granulation tissue
Motley TA, et al. Wounds. 2014;26(3):57-64.
Debridement with and without Adjunctive Clostridial Collagenase Ointment: Results
• Wound appearance scores improved in both treatment groups
• On average, ulcers receiving serial sharp debridement decreased in size more rapidly with the addition of CCO
– The CCO group demonstrated a 68% decrease in ulcer area from baseline at Week 6 (P < .001) vs 36% in the control group (P = NS)
• This was designed as a descriptive study; further work underway
Motley TA, et al. Wounds. 2014;26(3):57-64.
Precautions
• The optimal pH range of collagenase is 6 to 8
• Adversely affected by certain detergents, and heavy metal ions such as mercury and silver which are used in some antiseptics
• Soaks containing metal ions or acidic solutions should be avoided because of the metal ion and low pH
• A slight transient erythema has been noted occasionally in the surrounding tissue, particularly when CCO was not confined to the wound. Therefore, the ointment should be applied carefully within the area of the wound
www.santyl.com/content/pdf/SANTYL_Package_Insert-2013.pdf. Accessed February 28, 2017.
With that said…
• Thoroughly flush with saline if agents are used
• Awareness of compatibility with cleansers and antimicrobial dressings/agents helpful
Jovanovic A, et al. Wounds. 2012;24(9):242-253.

Case Study 1
• 24-year-old male spent a morning pouring a cement sidewalk in sneakers with no protection from the wet cement and lime contained therein. These are lime-related chemical burns with associated eschar.
Day 1
5d post
exposure
Day 10
Case Study 2
• 44-year-old male with leukocytoclastic vasculitis and hospitalized after several weeks of ineffective treatment
• Biopsy done in hospital and seen in Wound Center 5 days later
• Thick, broad-based hard black eschars were cross-hatched on Day 1
• Concomitant systemic steroids and CCO
Day 1 Day 12
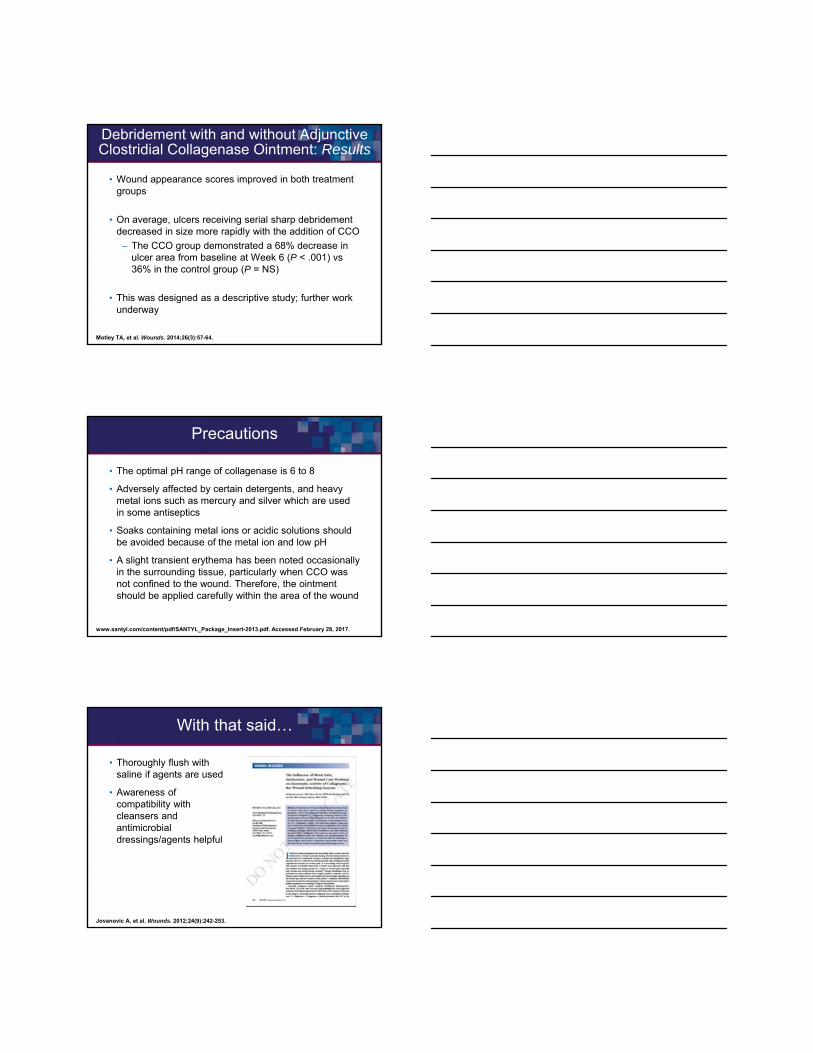
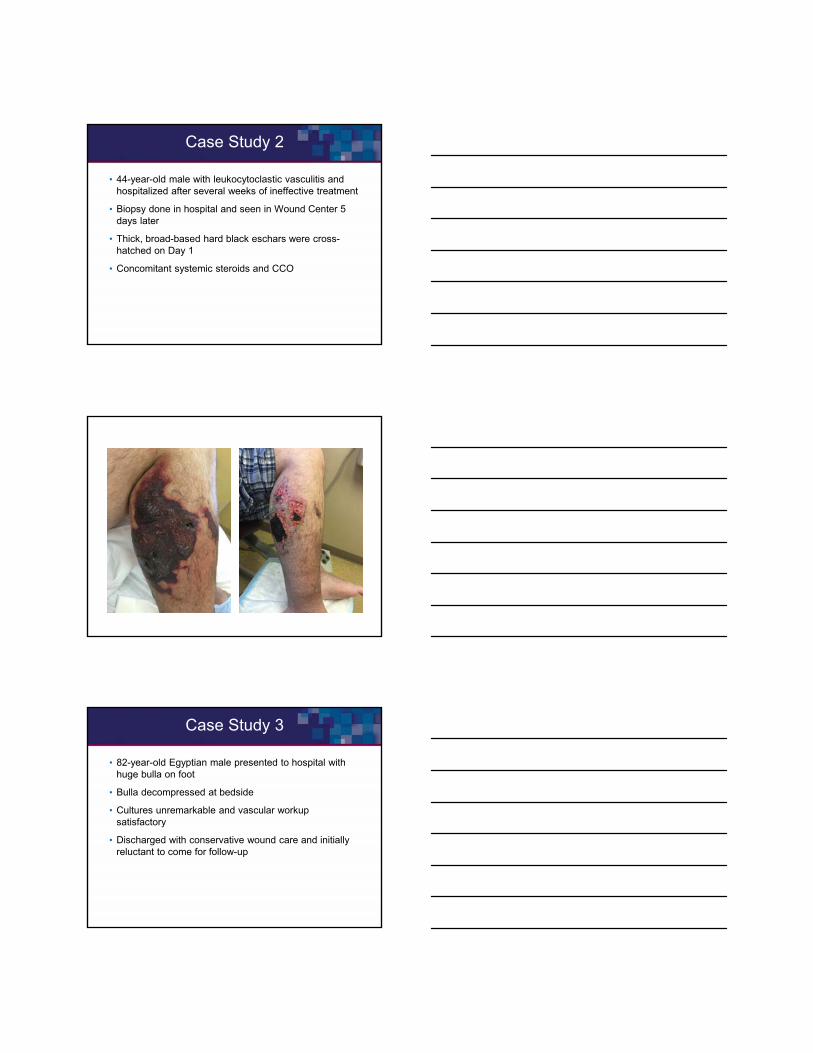
Case Study 3
• 82-year-old Egyptian male presented to hospital with huge bulla on foot
• Bulla decompressed at bedside
• Cultures unremarkable and vascular workup satisfactory
• Discharged with conservative wound care and initially reluctant to come for follow-up
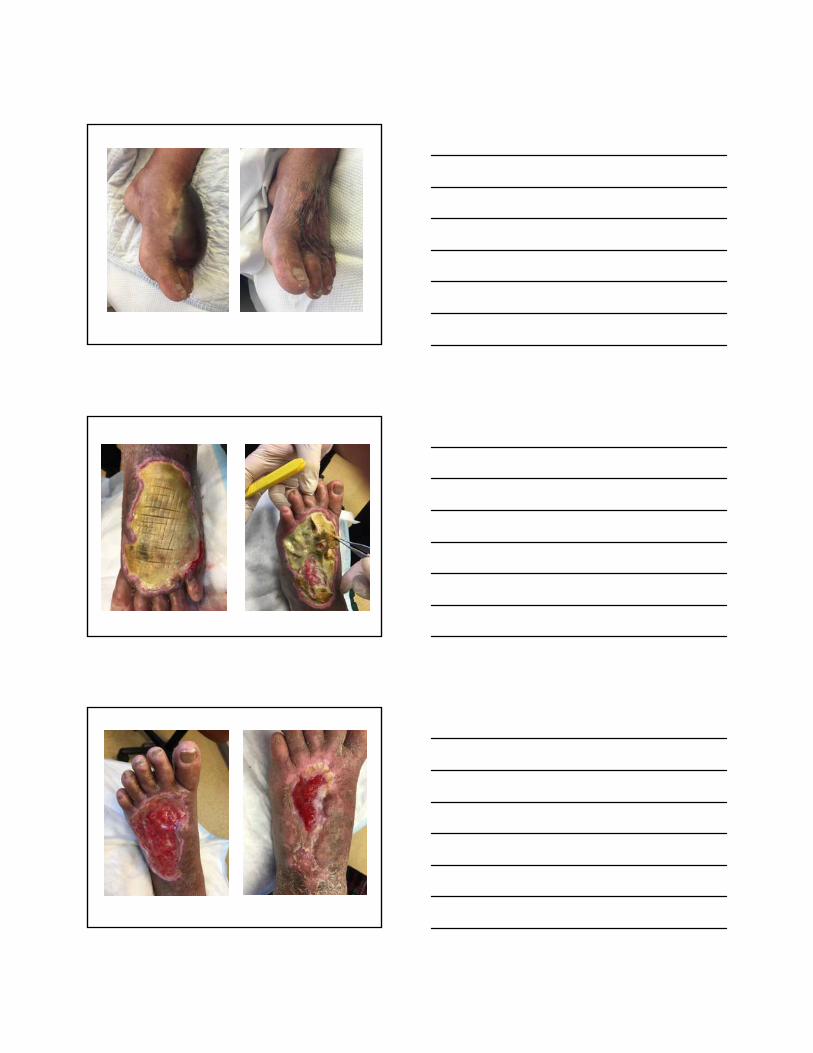
Hospital
Day 1
Day 14 Day 28
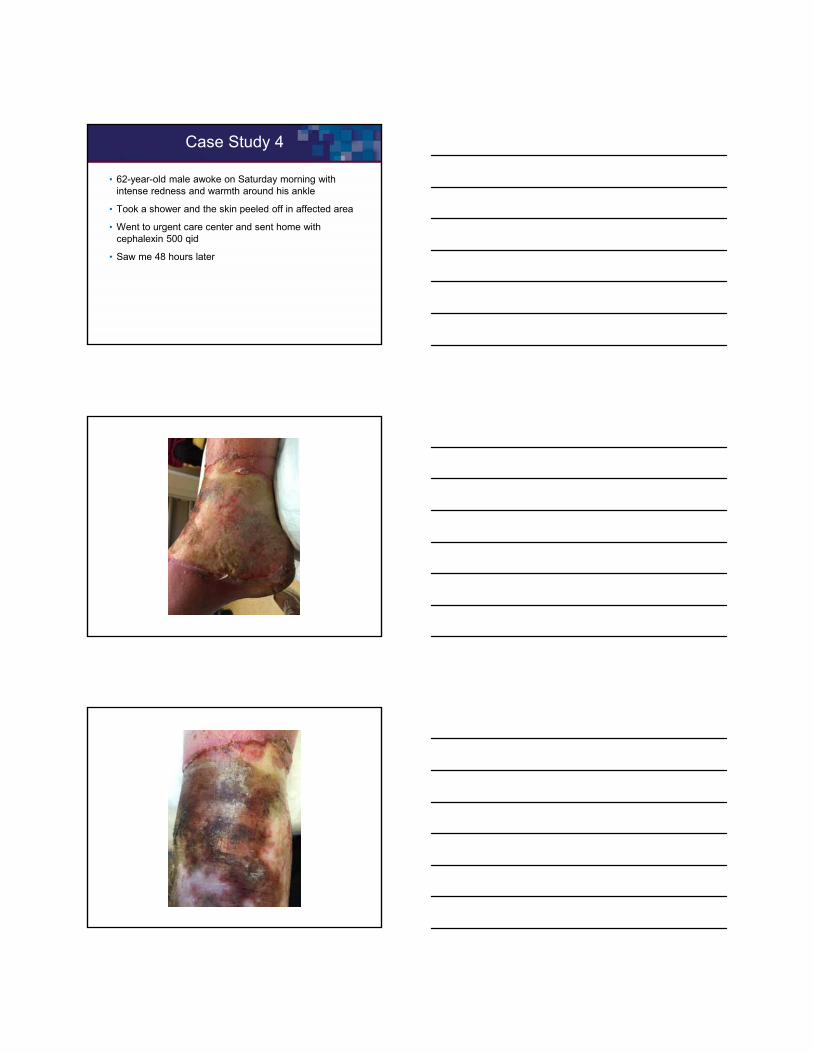
Case Study 4
• 62-year-old male awoke on Saturday morning with intense redness and warmth around his ankle
• Took a shower and the skin peeled off in affected area
• Went to urgent care center and sent home with cephalexin 500 qid
• Saw me 48 hours later
Day 1
Day 1 - Crosshatched
Day 14
Day 28
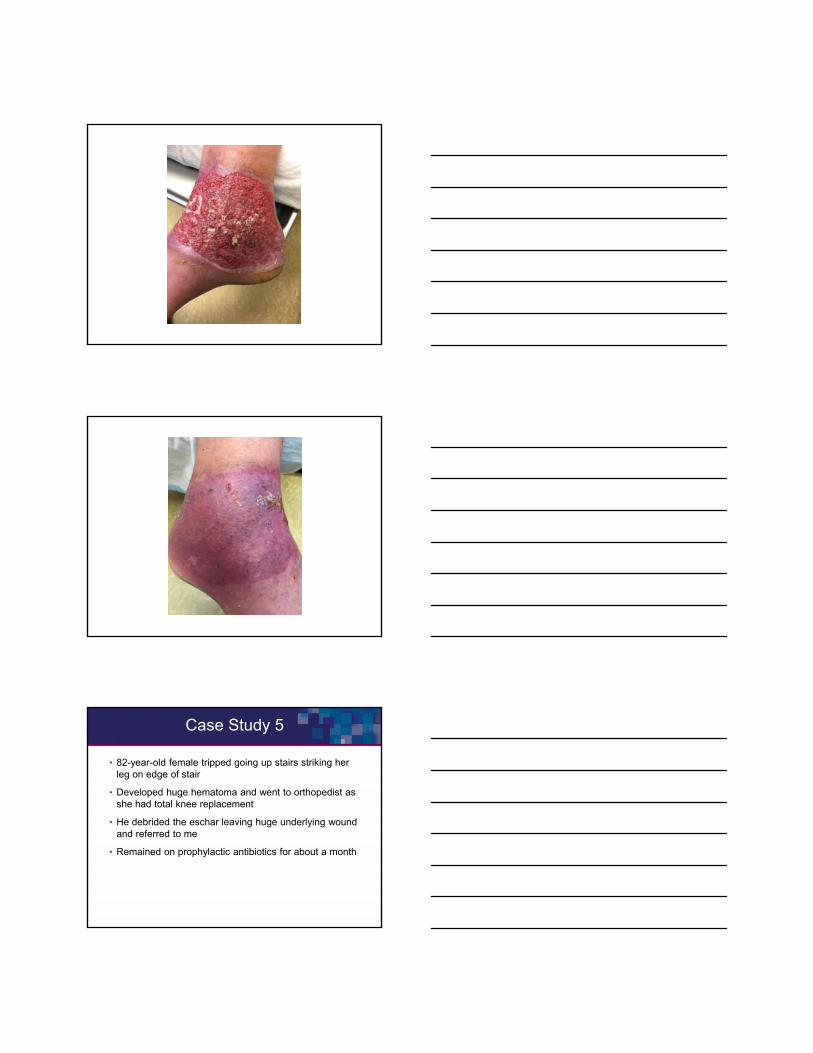
Case Study 5
• 82-year-old female tripped going up stairs striking her leg on edge of stair
• Developed huge hematoma and went to orthopedist as she had total knee replacement
• He debrided the eschar leaving huge underlying wound and referred to me
• Remained on prophylactic antibiotics for about a month
Day 1
Day 30
Day 60
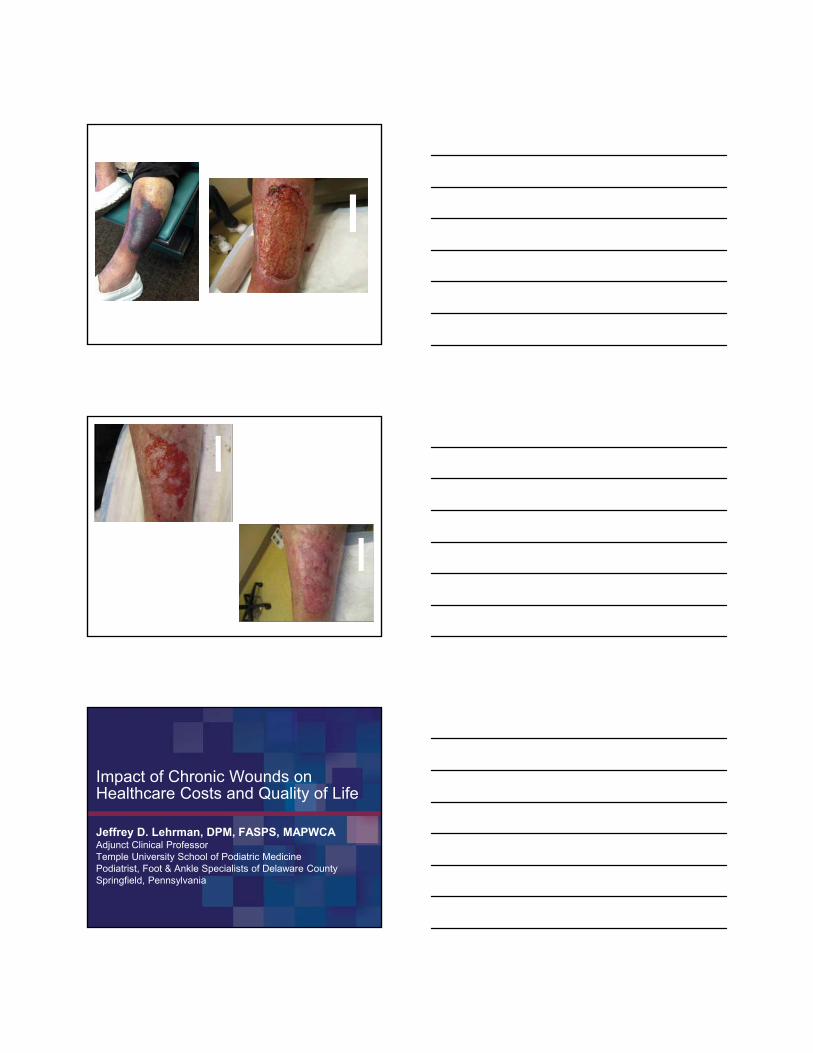
Jeffrey D. Lehrman, DPM, FASPS, MAPWCAAdjunct Clinical ProfessorTemple University School of Podiatric MedicinePodiatrist, Foot & Ankle Specialists of Delaware CountySpringfield, Pennsylvania
Impact of Chronic Wounds on Healthcare Costs and Quality of Life
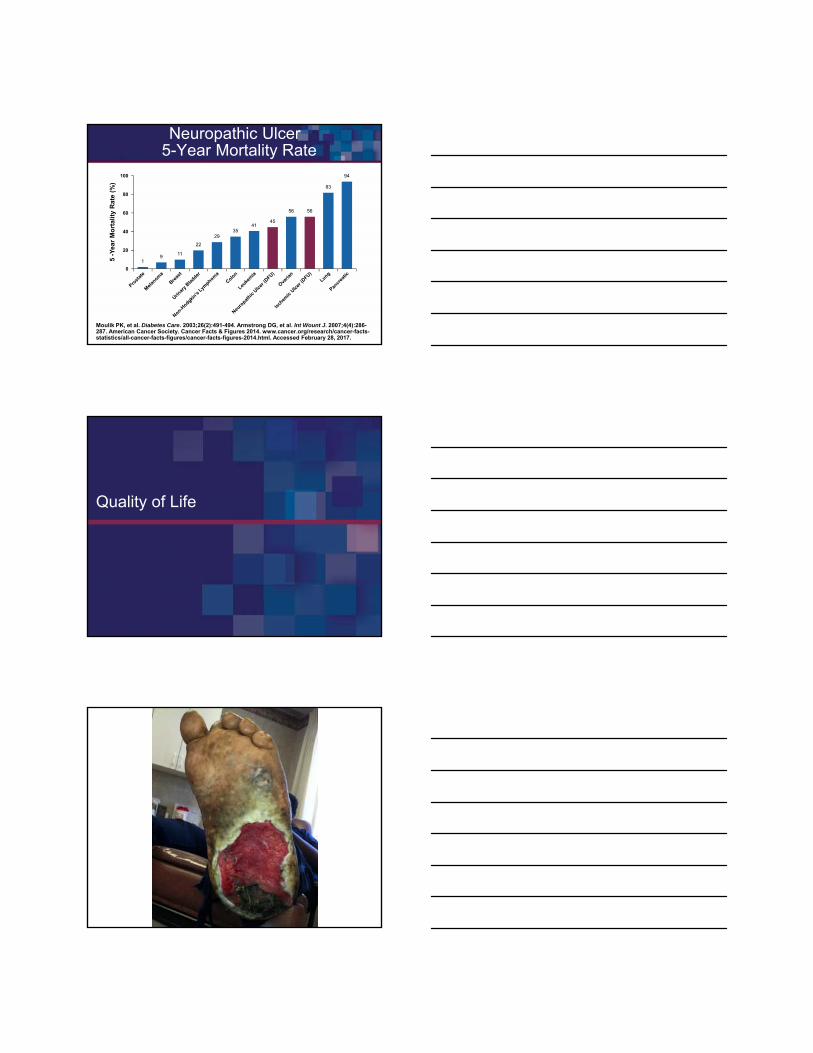
1
56
45
911
22
2935
41
56
83
94
Neuropathic Ulcer5-Year Mortality Rate
Moulik PK, et al. Diabetes Care. 2003;26(2):491-494. Armstrong DG, et al. Int Wount J. 2007;4(4):286-287. American Cancer Society. Cancer Facts & Figures 2014. www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2014.html. Accessed February 28, 2017.
20
100
0
5 -
Ye
ar
Mo
rta
lity
Ra
te (
%)
40
60
80
Quality of Life
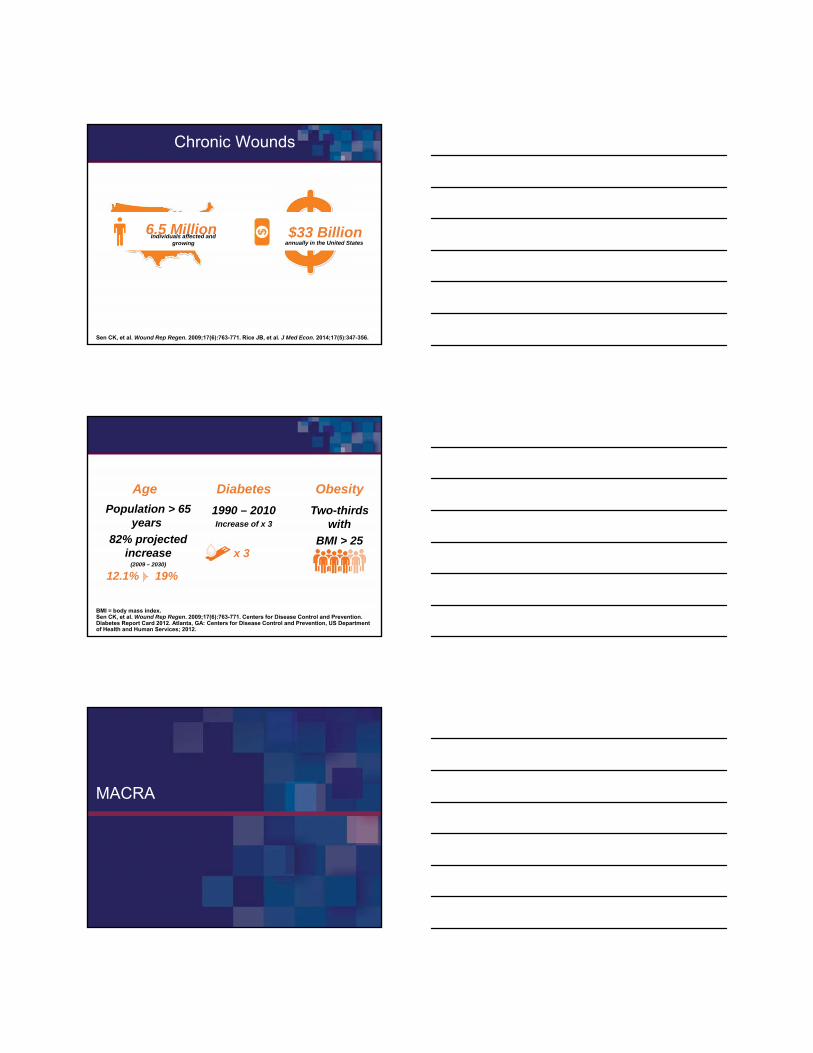
Chronic Wounds
Sen CK, et al. Wound Rep Regen. 2009;17(6):763-771. Rice JB, et al. J Med Econ. 2014;17(5):347-356.
6.5 MillionIndividuals affected and
growing annually in the United States
Estimated at
$33 Billion
BMI = body mass index.Sen CK, et al. Wound Rep Regen. 2009;17(6):763-771. Centers for Disease Control and Prevention. Diabetes Report Card 2012. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2012.
Age
Population > 65 years
82% projected increase
(2009 – 2030)
Diabetes
1990 – 2010Increase of x 3
Obesity
Two-thirds with
BMI > 25
12.1% 19%
x 3
MACRA
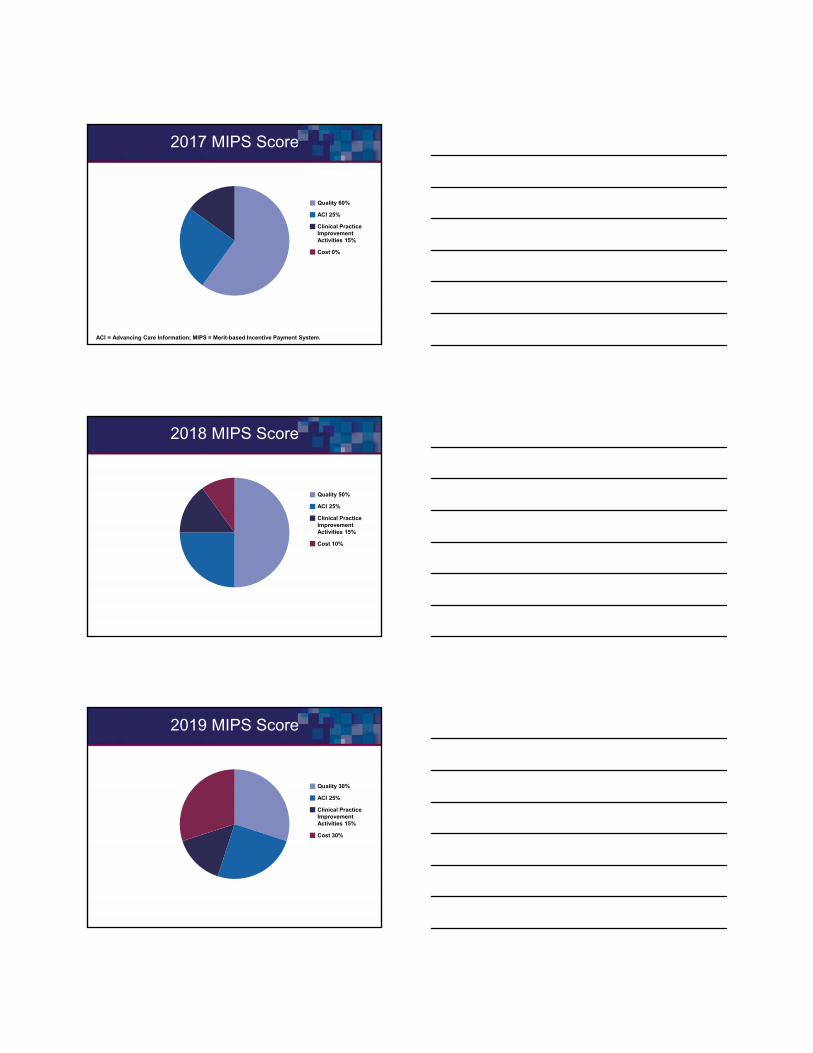
2017 MIPS Score
ACI = Advancing Care Information; MIPS = Merit-based Incentive Payment System.
Sales
Quality 60%
ACI 25%
Clinical PracticeImprovementActivities 15%
Cost 0%
2018 MIPS Score
Sales
Quality 50%
ACI 25%
Clinical PracticeImprovementActivities 15%
Cost 10%
2019 MIPS Score
Sales
Quality 30%
ACI 25%
Clinical PracticeImprovementActivities 15%
Cost 30%
Triple Aim
Comparative Effectiveness of Clostridial Collagenase Ointmentto Medicinal Honey for Treatment of Pressure Ulcers
Gilligan AM, et al. Advances in Wound Care. 2017;[Epub ahead of print].
Clostridial Collagenase Ointment vs Honey
• 517 CCO Treated Pressure Ulcers
• Matched to Honey Treated Pressure Ulcers
• CCO group: 38% more likely to achieve 100% granulation at 1 year
• CCO group: 47% more likely to epithelialize at 1 year
Gilligan AM, et al. Advances in Wound Care. 2017;[Epub ahead of print].
Clostridial Collagenase Ointment vs Honey
• CCO group:
– Fewer office visits
– Fewer debridements
– Less likely to require NPWT
NPWT = negative pressure wound therapy.Gilligan AM, et al. Advances in Wound Care. 2017;[Epub ahead of print].
Summary
• Pathophysiology
• Aggressive Management!
• Enzymatic Debridement + Sharp Debridement
• Quality of Life
• Healthcare Costs
Q & A