san joaquin county office of … joaquin county office of emergency services annex d – emergency...
TRANSCRIPT

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page i of 48
SAN JOAQUIN COUNTY OFFICE OF EMERGENCY SERVICES
ANNEX D – EMERGENCY MEDICAL SERVICES MANUAL 4 – MEDICAL SURGE CAPACITY PLAN
Annex of San Joaquin County Multi-Hazard Functional Plan
September 2005
*Note: This manual is part of Annex D of San Joaquin County Multi-Hazard Functional Plan, and should be use in conjunction with other manuals and annexes. It is not a stand alone plan.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 2 of 48
FORWARD
In recent years, concern over the possibility of a biological terrorist attack within the United States has become a national priority. The events of September 11, 2001 resulted in an increased focus on the need to plan for and when possible mitigate potential public health emergencies across the nation. In response to the real threat of a biological, nuclear, incendiary, chemical, or explosive (BNICE) terrorist attack, President George W. Bush established the Homeland Security Department. Since the inception of the Homeland Security Department, millions of dollars have been dedicated to enhancing prevention, preparation, and response to bioterrorism. In 2002, a cooperative agreement between the Health Resources Administration (HRSA) and the United States Department of Health and Human Services (USDHS) was formed to upgrade preparedness of the nation’s hospitals and collaborating entities in order to ensure that our nation’s healthcare providers are able to effectively respond to a bioterrorism emergency. Funding to support the program was provided in the form of grants to individual states. Grant objectives included completion of needs assessments by medical systems and building of infrastructure for planning and implementation of integrated activities in health care systems before and during a disaster. San Joaquin County has taken steps to fulfill objectives related to disaster and bioterrorism preparedness. The HRSA Planning Committee was formed in 2003 to begin the steps of evaluating the capacity of county hospitals to respond to a major biological incident. In 2005, the HRSA Planning Committee joined the county Bioterrorism Preparedness Advisory Committee (BPAC) to consolidate resources and facilitate collaboration of all participating agencies. This combined committee meets monthly to plan and discuss San Joaquin County (SJC) emergency planning and response initiatives. Membership of this committee includes local representatives from all seven acute care hospitals, local healthcare clinics, SJC Emergency Medical Services (EMS), Public Health, the Coroner’s office, Agriculture, Public Works, Office of Emergency Services, fire, law, mental health, community health, and education. It is through the collaborative efforts of the HRSA Planning Committee and BPAC that the Annex D, Manual 4, Medical Surge Capacity Plan was developed.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 3 of 48
TABLE OF CONTENTS SECTION PAGE SECTION 1: INTRODUCTION........................................................................................ 5
1.1 PURPOSE ........................................................................................................... 5 1.2 ASSUMPTIONS..................................................................................................... 5 1.3 SCOPE OF PLAN .................................................................................................. 5 1.4 DEFINITIONS ....................................................................................................... 6
SECTION 2: MASS CASUALTY INCIDENTS ................................................................ 9 2.1 DESCRIPTION...................................................................................................... 9 2.2 LEVELS OF RESPONSE ......................................................................................... 9
2.2.1 Local Response............................................................................................. 9 2.2.1.1 Activation.......................................................................................... 9 2.2.1.2 Notification ....................................................................................... 9 2.2.1.3 Triage ............................................................................................. 10 2.2.1.3.1 Hospital Triage ................................................................ 10 2.2.1.4 Transport........................................................................................ 10 2.2.2 Regional Response ..................................................................................... 11 2.2.3 State Response........................................................................................... 11 2.2.4 Federal Response ....................................................................................... 12 2.2.4.1 Federal Agencies............................................................................ 12 2.2.4.2 NDMS............................................................................................. 12
SECTION 3: HOSPITAL BED SURGE CAPACITY...................................................... 13 3.1 ACUTE CARE FACILITIES...................................................................................... 13
3.1.1 Base Hospitals ............................................................................................ 13 3.1.2 Receiving Hospitals..................................................................................... 13
3.2 SURGE CAPACITY BED PROJECTIONS ................................................................. 14 3.2.1 Flexible Bed Licensure ................................................................................ 14
3.3 PATIENT CARE CATEGORIES .............................................................................. 15 3.4 SURGE RECOMMENDATIONS............................................................................... 16 3.5 HOSPITAL SURGE CAPACITY GUIDANCE .............................................................. 16 3.5.1 REGULATORY INFORMATION ............................................................................ 16 3.6 SPECIALTY SERVICES ........................................................................................ 17
3.6.1 Hazardous Materials Incidents .................................................................... 17 3.7 ISOLATION CAPABILITIES ................................................................................... 17
3.7.1 Isolation Beds.............................................................................................. 17 3.7.2 Specialty Equipment (Ventilators and PPE) ................................................ 18
3.8 ALTERNATIVE CARE SITES................................................................................... 18 3.8.1 Casualty Collection Points........................................................................... 18 3.8.2 Surge Capacity Tents.................................................................................. 18
SECTION 4: SURGE CAPACITY STAFFING .............................................................. 19 4.1 STAFFING GUIDELINES........................................................................................ 19

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 4 of 48
4.1.1 STANDARDS ................................................................................................. 19 4.1.1.1 NURSE - PATIENT STAFFING RATIOS ................................................... 19 4.1.2 STAFFING PATTERNS ..................................................................................... 20 4.2 MUTUAL AID....................................................................................................... 20 4.3 ALTERNATIVE LEVELS OF CARE............................................................................ 20
4.3.1 Goals ........................................................................................................... 20 SECTION 5: LOCAL RESOURCES ............................................................................. 21
5.1 AMERICAN RED CROSS...................................................................................... 21 5.2 COMMUNITY CLINICS .......................................................................................... 21 5.3 SAN JOAQUIN COUNTY PUBLIC HEALTH ................................................................. 21 5.4 SAN JOAQUIN COUNTY OFFICE OF EMERGENCY SERVICES ...................................... 21 5.5 SKILLED NURSING FACILITIES .............................................................................. 22 5.6 STOCKTON FIRE DEPARTMENT............................................................................. 22
5.6.1 MMRS Plan and Resources ....................................................................... 22 SECTION 6: APPENDICES.......................................................................................... 23
6.1 APPENDIX A ACUTE CARE HOSPITAL AND SNF PARTNERSHIPS .......................... 24 6.2 APPENDIX B NOTIFICATION ALGORITHM FOR LARGE SCALE MCIS ....................... 26 6.3 APPENDIX C SJC ACUTE CARE SURGE CAPACITY HOSPITAL BED SUMMARY....... 27 6.4 APPENDIX D TITLE 22, SECTION 70741 ............................................................ 28 6.5 APPENDIX E TERTIARY HOSPITAL REFERENCE GUIDE........................................ 29 6.6 APPENDIX F SAMPLE MUTUAL AID MEMORANDUM OF UNDERSTANDING .............. 31 6.7 APPENDIX G SJC ACUTE CARE HOSPITAL CHEMICAL AGENT SUMMARY .............. 34 6.8 APPENDIX H SJC ACUTE CARE HOSPITAL BIOLOGICAL RESPONSE SUMMARY....... 35 6.9 APPENDIX I SJC MMRS DESIGNATED CCPS................................................... 36 6.10 APPENDIX J SJGH SURGE CAPACITY TENT DEPLOYMENT PROCEDURES............. 38 6.11 APPENDIX K SJGH SURGE CAPACITY TENT SET UP PROCEDURES...................... 38
SECTION 7: REFERENCES......................................................................................... 46

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 5 of 48
SECTION 1 INTRODUCTION
1.1 Purpose The purpose of this manual is to outline actions to be taken by San Joaquin County Emergency Medical Services, prehospital providers, and acute care hospitals/clinics in conjunction with local, state, and federal governmental agencies and cooperating private or volunteer organizations to effectively:
Plan for a large scale medical emergency requiring a significant increase in hospital admissions and emergency services. Identify potential resources available to augment healthcare
services during a public health emergency. Respond to public health emergencies of all types and all sizes,
from small to large-scale catastrophic disasters by maximizing hospital bed capacity and optimizing efficiency of available resources.
1.2 Assumptions The planning committee has developed some basic assumptions to guide the development of this Medical Surge Capacity Plan:
A significant, large scale event will overwhelm the local hospital and EMS system.
Hospitals should be prepared to stand alone for at least 48-72 hours until mutual aid resources arrive.
It is likely that hospital resources will need to be redirected to care for the most seriously ill and critically injured patients.
The standard of care delivered by acute care and prehospital care providers may need to be adapted to the existing situation and may require altered levels of care, including austere care in the most serious of situations.
Various facilities, clinics, organizations, and groups will be needed to support and supplement hospital services during a local disaster (CNA Corporation, 2004).
1.3 Scope of Plan
It is not the intent of this manual to attempt to deal with those events that happen on a daily basis, which do not cause widespread problems and are handled routinely by the healthcare community. This manual will, however, attempt to deal with those occurrences that create a local public health emergency, which creates needs and causes suffering to citizens that cannot be alleviated without the cooperative response of county

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 6 of 48
healthcare service providers and local, state, and/or federal governmental agencies, prehospital first responders, and private/volunteer agencies.
1.4 Definitions
A. Austere Medical Care: Austere care is the level of medical care, modified from the expected standard of care that is provided when hospital resources, medical supplies and medical personnel are limited or unavailable for an extended response period.
B. Bioterrorism: Terrorism using a biological source as a weapon. C. Disaster Control Facility (DCF): Pre-determined hospital which will serve as first point of contact in disaster.
D. Disaster Medical Assistance Team (DMAT): National Disaster Medical System (NDMS), through the U. S. Public Health Service, has developed Disaster Medical Assistance Teams (DMAT's). These teams are made up of medical and ancillary personnel to provide medical care to areas where local EMS and medical systems are overwhelmed due to natural or man-made disasters.
E. Disaster (“Major”): As defined in the Stafford Act, a “major disaster” is any natural catastrophe (including any hurricane, tornado, storm, high water, wind-driven water, tidal wave, tsunami, earthquake, volcanic eruption, landslide, mudslide, snowstorm, or which in the determination of the President causes damage of sufficient severity and magnitude to warrant major disaster assistance under this Act to supplement the efforts and available resources of States, local governments, and disaster relief organizations in alleviating the damage, loss, hardship, or suffering caused thereby. F. Emergency Operations Centers (EOC): The EOC is used in varying ways at all levels of government and within private industry to provide coordination, direction, control or support during emergencies.
G. Hospital Incident Command System (HEICS): Incident Command
structure for use by health care facilities, based on an organizational chart which clearly defines a chain of command and Job Action Sheets which assist hospital management in focusing on critical issues affecting a facility during a crisis.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 7 of 48
H. First Responder: Refers to individuals who in the early stages of an incident are responsible for the protection and preservation of life, property, evidence, and the environment, including emergency response providers as defined in Section 2 of the Homeland Security Act of 2002 (6 U.S.C. 101). It includes emergency management, public health, clinical care, public works, and other skilled support personnel (e.g., equipment operators) that provide immediate support services during prevention, response, and recovery operations. I. Incident: An actual or impending hazard impact, either human caused or by natural phenomena, that requires action by emergency personnel to prevent or minimize loss of life or damage to property and/or natural resources.
J. Incident Command System (ICS): A command and organizational system for use by emergency response agencies to manage large or complex emergencies. This system is intended to ensure that command is established and essential staff and operational functions for multi-agency coordination and support are completed. K. Mass Casualty Incident (MCI): Incident involving multiple patients that exceeds the capabilities of local resources.
L. Mitigation: Activities designed to reduce or eliminate risks to persons or property or to lessen the actual or potential effects or consequences of a hazard. M. Mutual Aid Region: A "mutual aid region" is a subdivision of the state emergency services organization, established to facilitate the coordination of mutual aid and other emergency operations within an area of the state consisting of two or more county operational areas. N. Operational Area: Intermediate level of the state emergency services organization, consisting of a county an all political subdivisions within the county. O. Preparedness: The range of deliberate, critical tasks and activities necessary to build, sustain, and improve the capability to protect against, respond to, and recover from hazard impacts. P. Region IV: California mutual aid region including: Stanislaus, San Joaquin, El Dorado, Sacramento, Yolo, Calaveras, Tuolumne, Placer, Amador, Nevada, and Alpine counties.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 8 of 48
Q. Region IV Disaster Medical/Health Coordinator (RDMHC): State appointed coordinator that is responsible for regional area resource management and mutual aid requests. R. Resources: All personnel and major items of equipment, supplies, and facilities available, or potentially available, for assignment to incident or event tasks on which status is maintained.
S. State: Any State of the United States, the District of Columbia, the Commonwealth of Puerto Rico, the Virgin Islands, Guam, American Samoa, the Commonwealth of the Northern Mariana Islands, and any possession of the United States. T. Surge: To rise suddenly to an excessive or abnormal value. U. Surge Capability: The ability to manage patients requiring unusual or very specialized medical evaluation and care. Requirements span the range of specialized medical and health services, and include patient problems that require special intervention to protect medical providers, other patients, and the integrity of the medical care facility. V. Surge Capacity: The ability to expand care capabilities in response to prolonged demand. “Surge capacity encompasses potential patient beds; available space, in which patients may be triaged, managed, vaccinated, decontaminated, or simply located; available personnel of all types; necessary medications, supplies and equipment; and even the legal capacity to deliver health care under situations which exceed authorized capacity” (JCAHO, 2003). W. Terrorism: Any premeditated, unlawful act dangerous to human life or public welfare that is intended to intimidate or coerce civilian populations or governments.
X. Weapons of Mass Destruction (WMD): Per Title 18 of the United States Code, Part I, Chapter 113B, Section 2332 (A) any destructive device as defined in section 921 of this title; (B) any weapon that is designed or intended to cause death or serious bodily injury through the release, dissemination, or impact of toxic or poisonous chemicals, or their precursors; (C) any weapon involving a disease organism; or (D) any weapon that is designed to release radiation or radioactivity at a level dangerous to human life.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 9 of 48
SECTION 2 MASS CASUALTY INCIDENTS
2.1 Description
Mass casualty incidents (MCI) are events that involve multiple patients that require care that is likely to exceed the capabilities of local resources. This plan is not intended for use with routine MCIs involving less than 50 patients. Annex D, Manual 1 of the San Joaquin County Multi Hazard Plan describes the response organizations, personnel, equipment, resources, and procedures for field operations that are designed to be used in San Joaquin County during such events. The intent of this plan is to provide guidelines for first receivers in the event of a MCI with >50 victims requiring acute hospital care.
2.2 Levels of Response 2.2.1 Local Response During the initial phase of local response to a large scale MCI, pandemic illness or terrorist attack, all emergency and in-patient services will be provided at our seven local hospitals. All seven hospitals have the ability to provide general acute care medical services for victims of a WMD/NBC incident. Local resources are available to augment acute care hospitals surge capacity and capabilities during a large scale multiple casualty incident. These resources can be requested through the DCF during a disaster or large scale medical incident. Resources include but are not limited to:
Pharmaceutical and medical supply caches and trailers TVI Surge Capacity Tents, cots and generators Large volume portable decontamination systems
2.2.1.1 Activation Per MCI procedures outlined in Manual 1, the county Disaster Control Facility will be activated to appropriately distribute victims. 2.2.1.2 Notification Notification of hospitals during a large scale MCI is outlined in Manual 1 of this Annex. Incidents that exceed the capabilities of local resources may require mutual aid assistance from regional, state, and federal emergency response agencies. See Appendix B for an overview of local, regional, and state/federal notification steps.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 10 of 48
2.2.1.3 Triage Large scale medical incidents will be triaged according to
county field standard operating procedures. Patients will be triaged utilizing the Simple Triage and Rapid Treatment (START) triage approach. In sufficiently large mass casualty incidents, this triage approach may need to be coupled with a system of secondary triage termed, "Secondary Assessment of Victim Endpoint" (SAVE) (Benson, Koenig, Schultz, 1996). START Triage standards are outlined in Manual 1 of this Annex. 2.2.1.3.1 Hospital Triage Due to the large quantities of patients that can be expected to self report to the hospital, it is recommended that acute care hospitals and clinics establish on site triage areas located away from the Emergency Department. Triage should be conducted according to hospital policies; however, it is recommended that hospitals utilize the START triage approach to determine who will receive priority medical care. Hospitals may need to turn away minor patients with recommendations to seek medical attention later. According to Garan, Lucow, & Miller (2005), as long as hospitals ensure that everyone who presents is being seen and attended to equally, without any consideration of or discrimination based on financial considerations, compliance with EMTALA regulations during a large scale disaster should not be an issue. Note: It cannot be emphasized enough that security issues and facility lock down procedures must be addressed early to control the influx of patients into the seven local acute care hospitals.
2.2.1.4 Transport Patients classified as “Immediate” will receive first priority for transport to acute care facilities. All patients transported to receiving hospitals must be screened for exposure and/or contamination from biological, chemical, and/or radiological substances. All efforts will be made to decontaminate patients prior to transport to acute care hospitals. Report will be given to the receiving hospital staff prior to entry into the facility regarding the level of field decontamination provided on scene and/or suspicion of NBC agent exposure or infection. Acute care hospitals should establish external triage sites to receive patients prior to allowing entry into the

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 11 of 48
facility to ensure proper placement of possibly contagious or contaminated patients.
2.2.2 Regional Response If the number of victims exceeds the capability of local resources, the Medical/Health Mutual Aid System will be activated. The Medical/Health Operational Area Coordinator (MHOAC), activated through Stockton Fire Dispatch, is responsible for arranging all medical and health resources necessary to mitigate the situation. Procedures for this are outlined in the Region IV MCI Plan (Stockton Fire Department, 2003). Local hospitals seeking regional mutual aid assistance should communicate such requests through the DCF. 2.2.3 State Response Medical assistance from the State government can be requested if Regional Mutual Aid resources are not adequate to augment medical resources during a large scale incident. State Government agencies include:
Governor’s Office of Emergency Services (OES) The Governor's Office of Emergency Services (OES) is responsible for the overall coordination of the state’s disaster response. OES is responsible for initiating the state response to disasters, including alerting and activating state agencies with response responsibilities. It provides approval for expenditures for acquisition of resources and requests for federal assistance. OES operates the State Operations Center (SOC) in Sacramento.
Emergency Medical Services Authority (EMSA) The EMSA coordinates the state's medical response to major disasters. The Director of EMSA is the State Disaster Medical Coordinator (SDMC) and serves as a member of the Governor's Emergency Operations Executive Council.
State Department of Health Services
The DHS is responsible for the state public health and environmental health response to a disaster. DHS also supports the state medical response by establishing and operating the Joint DHS/EMSA Emergency Operations Center (JEOC). DHS also directs the deployment of resources to protect the public and environmental health, and performs licensing inspections of hospitals, nursing homes, and clinics.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 12 of 48
State Department of Health Services The DHS is responsible for the state public health and environmental health response to a disaster. DHS also supports the state medical response by establishing and operating the Joint DHS/EMSA Emergency Operations Center (JEOC). DHS also directs the deployment of resources to protect the public and environmental health, and performs licensing inspections of hospitals, nursing homes, and clinics. 2.2.4 Federal Response Federal government assistance can be requested by the state if the demand for medical resources exceeds the capabilities of the lower levels of government. Under the coordination of the Federal Emergency Management Agency (FEMA), federal agencies will provide resources to support state and local emergency response efforts at the request of and in coordination with state response officials. Federal agencies may, under their own authority, provide disaster assistance prior to a presidential declaration. 2.2.4.1 Federal Agencies Federal agencies and organizations with responsibilities for the support of the states’ medical response are the United States Public Health Service (USPHS), Department of Veterans Affairs (VA), Department of Defense (DOD), and Department of Transportation (DOT). 2.2.4.2 National Disaster Medical System (NDMS) In 1983, Congress created the National Disaster Medical System (NDMS) to improve the federal government’s ability to respond to medical disasters. Through a coordinated effort, the NDMS:
• Provides Disaster Medical Assistance Teams (DMATS), Disaster Mortuary Teams (DMORT) and Disaster Veterinary Assistance Teams (VMATS) to support patient care, coroner, and animal response operations within the disaster area.
• Assists communities to develop the capability to receive evacuated casualties
• Coordinates the evacuation of casualties to sources of medical care outside the state.
Disaster support team assistance can be requested through FEMA.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 13 of 48
SECTION 3
HOSPITAL BED SURGE CAPACITY 3.1 Acute Care Facilities There are a total of seven acute care hospitals in San Joaquin County. The combined licensed acute care capacity in San Joaquin County is 1064 beds. The following is a list of local acute care hospitals. 3.1.1 Base Hospitals
There are two designated base hospitals in San Joaquin County. San Joaquin County General Hospital also serves as the county Disaster Control Facility. Dameron Hospital 525 W. Acacia Street Stockton, CA 95203 Phone: (209) 944-5550 Fax (209) 461-3112 Website: www.dameronhospital.org San Joaquin General Hospital P.O. Box 1020 Stockton, CA 95201 Phone: (209) 468-6300 Fax: (209) 468-6988 Website: www.sjgeneralhospital.com
3.1.2 Receiving Hospitals There are five receiving hospitals in San Joaquin County: Doctors Hospital of Manteca 1205 E. North Street Manteca, CA 95336 Phone: (209) 823-3111 Fax: (209) 823-4260 Website: www.doctorsmanteca.com Kaiser Permanente Hospital Manteca 1777 West Yosemite Avenue Manteca, CA 95336 Phone: (209) 825-3700

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 14 of 48
Lodi Memorial Hospital P.O. Box 3004 Lodi, CA 95241 Phone: (209) 334-3411 Fax: (209) 368-3121 Website: www.lodihealth.org Saint Joseph's Medical Center P.O. Box 213008 Stockton, CA 95204 Phone: (209) 467-6400 Fax: (209) 461-3200 Website: www.stjosephscares.org Sutter-Tracy Community Hospital 1420 Tracy Boulevard Tracy, CA 95376 Phone: (209) 835-1500 Fax: (209) 832-6019 Website: www.suttertracy.org
3.2 Surge Capacity Bed Projections
HRSA critical benchmark standards require that San Joaquin County establish a system that allows for the triage, treatment, and disposition of 500 adult and pediatric patients per 1,000,000 population, with acute illness or trauma requiring hospitalization from a biological, chemical, radiological, or explosive terrorist incident. According to the United States (U.S) census report, the estimated population in San Joaquin County was 632,760 in 2003. The minimum recommended level of readiness for surge capacity in San Joaquin County is 315 adult and pediatric patients (1 patient per every 2,000). Based upon an analysis of average daily census versus licensed beds in the county’s seven acute care hospitals it was determined that there are an estimated 276 unoccupied licensed beds available during normal operating conditions. It was further determined that at least another 90 beds could be available for flexible bed use during a large scale incident by utilizing outpatient treatment areas (e.g. PACU, ED, and Outpatient Surgery space) for patients requiring hospital admission. The resulting number of anticipated bed availability is 366 acute care beds. See Appendix C, San Joaquin County Acute Care Surge Capacity Hospital Bed Summary.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 15 of 48
3.2.1 Flexible Bed Licensure Verbal approval for use of outpatient areas and hallways can be obtained by local hospitals by calling or faxing the local CDHS Licensing and Certification Department. The following is the local L&C contact information for San Joaquin County: Sacramento District Office 630 Bercut Drive, Suite B Sacramento, CA 95814 Phone: (916) 341-6845 Toll Free: (800) 554-0354 FAX: (916) 341-6840 Note: Licensed beds are not the equivalent of staffed hospital beds. In the event of a large scale medical incident, staffing ratios and standards of care will be impacted. See Section 4 of this plan for guidance in addressing surge capacity staffing issues and alternative levels of care. 3.3 Patient Care Categories A review of disaster related literature was conducted to determine what percentage of patients seeking medical care after an emergency incident would fall into the following categories:
Worried Well – Worried, not requiring medical attention Minor – able to recover at home after minor treatment and/or
prophylaxis Delayed – stable, requiring medical attention within four hours Immediate – Unstable, requiring immediate medical attention for
survival Deceased – Dead or dying with a < 50% probability of survival
Estimates for patients requiring admission to the hospital have been based upon an 85/15% rule where an estimated 15% of patients will require inpatient care (Hick, 2004). Another estimate provided by Dr. K. Koenig, Department of Homeland Security is based upon the study of 29 U.S. disasters, which projects an admission rate of < 20% with the majority of patients being discharged from the hospital within 24-48 hours. According to J. Hick, (2004), the following is a consistent estimate for every 1,000 people injured in a disaster:
250 dead at scene (25%) 750 seek medical care
188 will be admitted (18%) 47 will require intensive care (5%)

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 16 of 48
Based upon this data, an estimated 79 of the 315 patients requiring hospital admission would require critical care services for illness, trauma, and/or burns. There are a total of 89 critical care beds in San Joaquin County. Cancellation of elective and non emergency surgeries could provide approximately 40-60 additional critical care beds (utilizing PACU beds). 3.4 Surge Recommendations Based upon these figures, it is recommended that critically ill and/or injured patients, pediatric and medically fragile patients be given priority for admission to inpatient acute care hospitals. Non critical care patients requiring non complex medical care not available on an outpatient basis will receive second priority for admission to acute care hospitals or admitted to alternative care sites. Currently, San Joaquin County has the capability of housing 54 patients in surge capacity tents. 3.5 Hospital Surge Capacity Guidance
Recommendations for local acute care hospitals in managing surge capacity are based upon published best practice strategies (Agency for Healthcare Research and Quality, 2004). Some strategies for individual hospital planning, mitigation, and response during a mass casualty incident include:
Develop internal plans for emergency management that include surge capacity, external triage areas, facility lock down procedures, and hospital security.
Train on and practice surge capacity plans with hospital staff. Implement early discharge of appropriate patients. Establish
discharge holding areas where patients can wait for rides home. Cancel elective and non emergency surgeries. Convert outpatient procedure beds into hospital inpatient beds (e.g.
outpatient surgery, post anesthesia care unit, endoscopy, radiology procedure rooms, etc.)
Use hallways in staffed areas for non critical inpatient admissions. Utilize non patient care areas as alternative treatment areas to triage
and treat minor injuries/illnesses (e.g. conference centers, waiting rooms, classrooms).
Partner with local collaborative partners to create treatment capacity outside of the hospital and augment staffing.
Initiate cooperative mutual aid agreements with other healthcare facilities including local skilled nursing facilities for patient transfers and the sharing of equipment and staff (see Appendix E, Sample Mutual Aid Memorandum of Understanding).
3.5.1 Regulatory Information
California Statute (Health and Safety Code, § 1336.3) and the California Code of Regulations, Title 22, require each facility licensed by the Department of Health Services, Licensing and Certification Program, to

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 17 of 48
adopt a written emergency preparedness plan and have the plan available to this state department by request. Title 22 Regulations also require Community Care facilities licensed by the California Department of Social Services (DSS) to have a written disaster and mass casualty plan and training for staff (Shelter Medical Group, 2000). For a summary of emergency preparedness standards required under Title 22 for health licensure, see Appendix D, Title 22, Section 70741.
3.6 Specialty Services San Joaquin County acute care hospitals offer a variety of specialty services including cardiovascular care, hazardous material decontamination capabilities, neonatal intensive care, and neurosurgery. Deficits in specialty care that may be required during a large scale medical incident include the care of burn, trauma, and critical pediatric care. Currently, there are no burn centers, children’s hospitals, or designated trauma facilities in San Joaquin County. To facilitate rapid transfer of these types of patients to appropriate tertiary facilities a list of regional hospitals with contact information is provided as Appendix F, Tertiary Hospital Reference Guide.
3.6.1 Hazardous Materials Incidents All of the seven acute care facilities in San Joaquin County have either permanent or temporary decon facilities available on site. All hospitals have the capability to decontaminate at least one non ambulatory patient contaminated with a hazardous material. For an estimate of local hospital decontamination capabilities see Appendix G, San Joaquin County Acute Hospital Chemical Agent Response Summary of Decontamination Capabilities.
3.7 Isolation Capabilities HRSA Grant critical benchmark 2.2 standards for isolation capacity require San Joaquin County to ensure that all participating hospitals have the capacity to maintain, in negative pressure isolation, at least one suspected case of a highly infectious disease (e.g., small pox, pneumonic plague, SARS, Influenza and hemorrhagic fevers) or for any febrile patient with a suspect rash or other symptoms of concern who might possibly be developing a potentially highly communicable disease. All of the seven acute care hospitals in San Joaquin County have the capability of admitting at least one suspected highly infectious patient in a negative pressure isolation room and have adequate supplies of PPE to protect healthcare staff caring for that patient. In addition, San Joaquin General Hospital and Dameron Hospital have been identified as having the capability to care for a minimum of 10 adult and pediatric patients requiring admission to a negative pressure isolation room. 3.7.1 Isolation Beds

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 18 of 48
There are a total of 59 negative pressure acute care rooms in San Joaquin County. Of these rooms, 12 rooms are located in acute care hospital emergency departments. A total of 4/7 of the acute care hospitals have negative pressure rooms located in their emergency department. See Appendix H, San Joaquin County Acute Care Biological Response Isolation Room Summary for a detailed analysis of available negative pressure isolation beds in San Joaquin County.
3.7.2 Specialty Equipment (Ventilators and PPE) San Joaquin County has purchased disposable ventilators for all seven acute care facilities as well as various forms of PPE including power air purifying respirators. In addition to disposable ventilators, there are a total of 118 ventilators on site in the seven acute care hospitals. Of these ventilators, it is estimated that 67 are available for use during the first three hours of a large scale medical incident. See Appendix H, San Joaquin County Acute Care Biological Response Isolation Room Summary for a detailed analysis of available ventilators in San Joaquin County. 3.8 Alternative Care Sites Alternative care sites for casualty collection points and field treatment sites have been identified for San Joaquin County. San Joaquin County has purchased a total of three TVI Surge Capacity Tents for use in these alternative care sites. The Stockton City MMRS Plan provides detailed information regarding alternative care sites.
3.8.1 Casualty Collection Points (CCPs) See Appendix I, San Joaquin County MMRS Designated CCPs
3.8.2 Surge Capacity Tents Surge Capacity tents have been purchased for SJGH, Dameron Hospital, and the County EMS. Surge capacity tents can be requested as mutual aid assets. See Appendix J, SJGH Surge Capacity Tent Deployment Procedures for instructions on requesting a tent. Information regarding tent set up procedures was provided by SJGH and is located in Appendix K of this manual.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 19 of 48
SECTION 4 SURGE CAPACITY STAFFING
4.1 Staffing Guidelines
During a large scale medical incident, San Joaquin County’s acute care hospitals will probably not have sufficient staff available to provide care based upon normal healthcare standards. Given the current critical nursing shortage, it is not anticipated that there will be enough registered nurses available to meet California nurse to patient staffing ratios during the initial phase of disaster medical response. The intent of this section is to provide guidance to acute care facilities in establishing plans to manage hospital staffing issues during a large scale incident.
The following staffing recommendations are intended to provide acute care hospital and surge capacity tent patients with the minimum level of care during a large scale incident. 4.1.1 Standards Every effort should be made to meet minimum staffing requirements including immediate implementation of staff call back procedures, requests for registry personnel, requests to region IV facilities for mutual aid, use of managerial staff in bedside care, and implementation of emergency credentialing policies. Medical/health professionals should only perform those duties consistent with their level of expertise and only according to their professional licensure/certification and allowable scope of practice. 4.1.1.1 Nurse – Patient Ratios Hospitals are not required to seek prior approval from DHS L&C if licensed nurse staffing levels fall below what is required in regulation during a healthcare emergency. However, Title 22 CCR 70217(q) requires hospitals to plan for routine fluctuations in patient census. A healthcare emergency is defined in the regulation as, “an unpredictable or unavoidable occurrence at unscheduled or unpredictable intervals relating to healthcare delivery requiring immediate medical interventions and care.” A healthcare emergency may be reportable to the department if it meets the definition of a “Disruption of Service” (22 CCR 70746) or is a “Reportable Event or Unusual Occurrence” (22 CCR 70747.) If the hospital can demonstrate that it made prompt efforts to try to maintain required staffing levels, then CDHS will not consider the hospital to have violated the regulations during the period of the health care emergency (DHS, 2004).

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 20 of 48
4.1.2 Staffing Patterns According to Title 22, all general acute care facilities are expected to have a staffing plan which includes staffing plans for high census fluctuations. Recommendations for staffing patterns include: not scheduling personnel to work for more than 12 hours in a 24-hour period and making staffing adjustments based on the actual number and needs of the patients in the medical treatment facility/temporary facility. 4.2 Mutual Aid Requests for additional staff can be made according to the Regional Mutual Plan. Refer to Manual 3 of this Annex for further guidance on mutual aid requests. Trained Citizen Emergency Response Team (CERT) volunteers are another local resource available to assist during a mass casualty incident. 4.3 Alternative Standards of Care According to the AHRQ (2005), the term “altered standards” is generally meant to refer to a shift in providing care and allocating scarce equipment, supplies, and personnel in a way that saves the largest number of lives in contrast to the traditional healthcare focus of saving individual lives. In a large scale mass casualty event, community healthcare needs may exceed the capability of local resources. When healthcare needs exceed available resources altered standards of care will need to be implemented during the first 24-72 hours until additional mutual aid resources are available to augment the local emergency response.
4.3.1 Goals The primary goal of healthcare first responders and receivers during a mass casualty event is to save as many lives as possible. To achieve this goal, healthcare will have to be delivered in a manner that differs from the standards of care that that apply under normal circumstances (AHRQ, 2005).

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 21 of 48
SECTION 5 LOCAL RESOURCES
5.1 American Red Cross Provides temporary mass care and sheltering to disaster victims who have been displaced from their homes. Provides the following disaster relief services:
• Shelter, feeding and first aid to people affected by disaster • May provide emergency replacement of medications and equipment if no other resources are available • Shelter staffing with at least one nurse per shift, based on population and health of residents • Mental health staff on all shifts as needed
In collaboration with local health agencies, the ARC • Will provide medical staff to assess all incoming evacuees for health care needs • If no special needs shelter is available, may provide an area for a medical treatment unit/temporary infirmary for those with special needs staffed by local health professionals or staff from evacuated facility • Will refer people needed individual care or special equipment to alternate shelter staffed by local health authorities • May request public health nurses to provide assistance to ARC as shelter nurses • May request local medical facilities to set up temporary clinics outside ARC shelters to provide advanced medical treatment, as requested and available (Shelter Medical Group, 2000).
5.2 Community Clinics There are a number of county clinics available to assist in the medical care of non critical care patients during a health care emergency. Hospitals are strongly urged to develop cooperative agreements with local clinics as referral points for non complex patient care. 5.3 San Joaquin County Public Health In the event of a public health emergency, the San Joaquin County Public Health Department will be the lead agency for incident management. See Annex F of the San Joaquin County Multi Hazard Functional Plan for a description of Public Health preparedness efforts, roles and authority during a public health emergency. 5.4 San Joaquin County Office of Emergency Services The Office of Emergency Services is the major coordinating agency for large scale emergencies in San Joaquin County. The San Joaquin County OES is

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 22 of 48
charged with coordinating the preparation of local disaster response plans and procedures. 5.5 Skilled Nursing Facilities There are a number of sub acute or skilled nursing facilities in San Joaquin County that can be utilized to admit non critical patients during a large scale emergency. Each of the seven acute care hospitals is “tied” to skilled nursing facilities for emergency response. See Appendix A for a list of these relationships. 5.6 Stockton Fire Department Stockton Fire Department has undertaken the coordination and administration efforts to develop and implement a local MMRS Plan.
5.6.1 MMRS Plan and Resources Resources for additional equipment and guidance can be accessed through the Stockton Fire Department including MMRS equipment cache and disaster trailers containing pharmaceuticals, trauma bags, Intravenous solutions, and other medical supplies. These resources are obtained by contacting the Medical Health Operational Area Coordinator through the Stockton Fire Dispatch Center.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 23 of 48
SECTION 6 APPENDICES
6.1 Appendix A San Joaquin County Acute Care Hospital and SNF Partnerships 6.2 Appendix B Notification Algorithm for Large Scale MCIs 6.3 Appendix C San Joaquin County Acute Care Surge Capacity Hospital Bed Summary 6.4 Appendix D Title 22, Section 70741 6.5 Appendix E Tertiary Hospital Reference Guide 6.6 Appendix F Sample Mutual Aid Memorandum of Understanding 6.7 Appendix G San Joaquin County Acute Hospital Chemical Agent Response Summary of Decontamination Capabilities 6.8 Appendix H San Joaquin County Acute Care Biological Response Isolation Room Summary 6.9 Appendix I San Joaquin County MMRS Designated CCPs 6.10 Appendix J San Joaquin General Hospital Surge Capacity Tent Deployment Procedures 6.11 Appendix K San Joaquin General Hospital Surge Capacity Tent Set Up Procedures

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 24 of 48
Appendix A San Joaquin County Acute Care Hospital and SNF Partnerships Skilled Nursing Facilities are assigned to an acute care facility for purposes of mutual support and assistance, and collection of facility status reports.
• Dameron Hospital Delta Valley Convalescent 466-6341 Pleasant Care of Northern California 956-9606 Plymouth Square Convalescent 466-4341 Sunrise Hampton Care Center 466-0456 Wagner Heights 477-5252 Whispering Hope Convalescent 473-3004 • Doctor’s Hospital Manteca Palm Haven Convalescent 823-1788 • Lodi Memorial Hospital Arbor Convalescent Hospital 333-1222 Crescent Court Nursing Home 367-7400 Delta Convalescent 334-3825 Fairmont Rehabilitation 368-0693 Gross Convalescent 333-3760 Lodi Health Care Center 368-6641 Lodi Memorial Hospital TCU 333-3042 Vienna Convalescent 368-7141 • Kaiser Hospital Manteca Bethany Home 599-4221 Sunrise Care and Rehab Center 239-1222
• Saint Joseph’s Medical Center Beverly Health Care Center 477-0271 La Salette Convalescent 466-2066 Meadow Wood 956-3444 St. Joseph Behavior Health 948-2100 St. Joseph Medical Center SNF 467-6394 Valley Gardens Health Care Center 957-4539
• San Joaquin General Hospital Beverly Manor of Stockton 466-3522 Chateau Convalescent 477-2664 Crestwood Manor Convalescent 478-2060

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 25 of 48
Elmhaven Convalescent 477-4817 Good Samaritan 948-8762 Heritage of Stockton 478-6488
• Sutter Tracy Community Hospital New Hope Care Center 832-2273 Tracy Convalescent 835-6034

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 26 of 48
Appendix B
Notification Algorithm for Large Scale MCIs
Local Incident Occurs
Receiving Hospitals utilize local cooperative partners for mutual aid
(E.g. SNFs, Sister Facilities, Tertiary Care
Centers)
DCF Notified of Large Scale MCI or Incident
DCF Contacts Receiving Hospitals
Receiving Hospitals Implement Internal
Surge Capacity Plans
County EOC activated. Local Emergency Resources deployed (MMRS, Public Health, OES, etc).
Regional DCF contacted for Mutual
Aid Support
State Emergency Operations Center
contacted for assistance
Federal Emergency Management Agency assistance requested
Federal Assets Deployed
(E.g. DMATs, DMORTS)
State Emergency Mutual Aid Assets
Deployed
Regional Assets Deployed for Mutual Aid

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 27 of 48
Appendix C
San Joaquin County Acute Care Surge Capacity Hospital Bed Summary
Bed Capacity Estimates
Dam
eron
H
ospi
tal
Doc
tors
H
ospi
tal o
f M
ante
ca
Lodi
M
emor
ial
Hos
pita
l
Kai
ser
Hos
pita
l M
ante
ca
San
Joaq
uin
Gen
eral
H
ospi
tal
St. J
osep
h’s
Med
ical
C
ente
r
Sutte
r Tra
cy
Com
mun
ity
Hos
pita
l
# Licensed Acute Care Beds
188
73
172
61
196
294
80
# Emergency Dept. Beds
19
11
16
10
19
36
14
# ICU Beds
12
8
10
6
16
29
8
# Coronary Beds 12
0
0
24
37
16
0
#NICU Beds
16
0
3
0
25
14
0
# PACU Beds
6
6
7
9
13
13
4
Average Daily Census
188
45
105
32
138
235
45
Projected Flex Surge Capacity (1/4 ED + PACU
Beds)
11
8
11
12
18
22
8
ADC Remaining Licensed Beds
0
28
67
29
58
59
35
Approx. Surge Capabilities
(Licensed and Flex)
11
36
78
41
76
81
43
Total licensed General Acute Care Beds = 1064
Total Estimated Acute Care Surge Capacity = 366

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 28 of 48
Appendix D Title 22, Section 70741
TITLE 22 CALIFORNIA CODE OF REGULATIONS §70741 §70741. Disaster and Mass Casualty Program. (a) A written disaster and mass casualty program shall be developed and maintained in consultation with representatives of the medical staff, nursing staff, administration and fire and safety experts. The program shall be in conformity with the California Emergency Plan of October 10, 1972 developed by the State Office of Emergency Services and the California Emergency Medical Mutual Aid Plan of March 1974 developed by the Office of Emergency Services, Department of Health. The program shall be approved by the medical staff and administration. A copy of the program shall be available on the premises for review by the Department. (b) The program shall cover disasters occurring in the community and widespread disasters. It shall provide for at least the following:
(1) Availability of adequate basic utilities and supplies, including gas, water, food and essential medical and supportive materials.
(2) An efficient system of notifying and assigning personnel. (3) Unified medical command. (4) Conversion of all usable space into clearly defined areas for efficient triage, for
patient observation and for immediate care. (5) Prompt transfer of casualties, when necessary and after preliminary medical or
surgical services have been rendered, to the facility most appropriate for administering definite care.
(6) A special disaster medical record, such as an appropriately designed tag, that accompanies the casualty as he is moved.
(7) Procedures for the prompt discharge or transfer of patients already in the hospital at the time of the disaster who can be moved without jeopardy.
(8) Maintaining security in order to keep relatives and curious persons out of the triage area.
(9) Establishment of a public information center and assignment of public relations liaison duties to a qualified individual. Advance arrangements with communications media will be made to provide organized dissemination of information.
(c) The program shall be brought up-to-date, at least annually, and all personnel shall be instructed in its requirements. There shall be evidence in the personnel files, e.g., orientation checklist or elsewhere, indicating that all new employees have been oriented to the program and procedures within a reasonable time after commencement of their employment. (d) The disaster plan shall be rehearsed at least twice a year. There shall be a written report and evaluation of all drills. The actual evacuation of patients to safe areas during the drill is optional.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 29 of 48
Appendix E Tertiary Hospital Reference Guide
Burn Centers: Emergency Number San Francisco General Hospital 415-206-8111 San Francisco, CA San Pablo Doctors Medical Center 510-970-5000 San Pablo, CA Santa Clara Valley Medical Center 408-885-5000 San Jose, CA Shriner’s Medical Center 916-453-2352 Sacramento, CA Pediatric Burn UC Davis Medical Center 916-734-2011 Sacramento, CA Microsurgery (Reimplantation) Emergency Number California Pacific Medical Center 888-637-2762 San Francisco, CA San Francisco General Hospital 415-206-8111 San Francisco, CA Stanford Medical Center 650-723-7570 Palo Alto, CA Pediatrics (Critical Care and Trauma) Emergency Number Children’s Hospital of Central California 559-353-5437 Madera, CA Children’s Hospital Oakland 510-428-3259 Oakland, California Stanford Medical Center 650-723-7570 Palo Alto, CA UC Davis Medical Center 916-734-2011 Sacramento, CA
San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 30 of 48
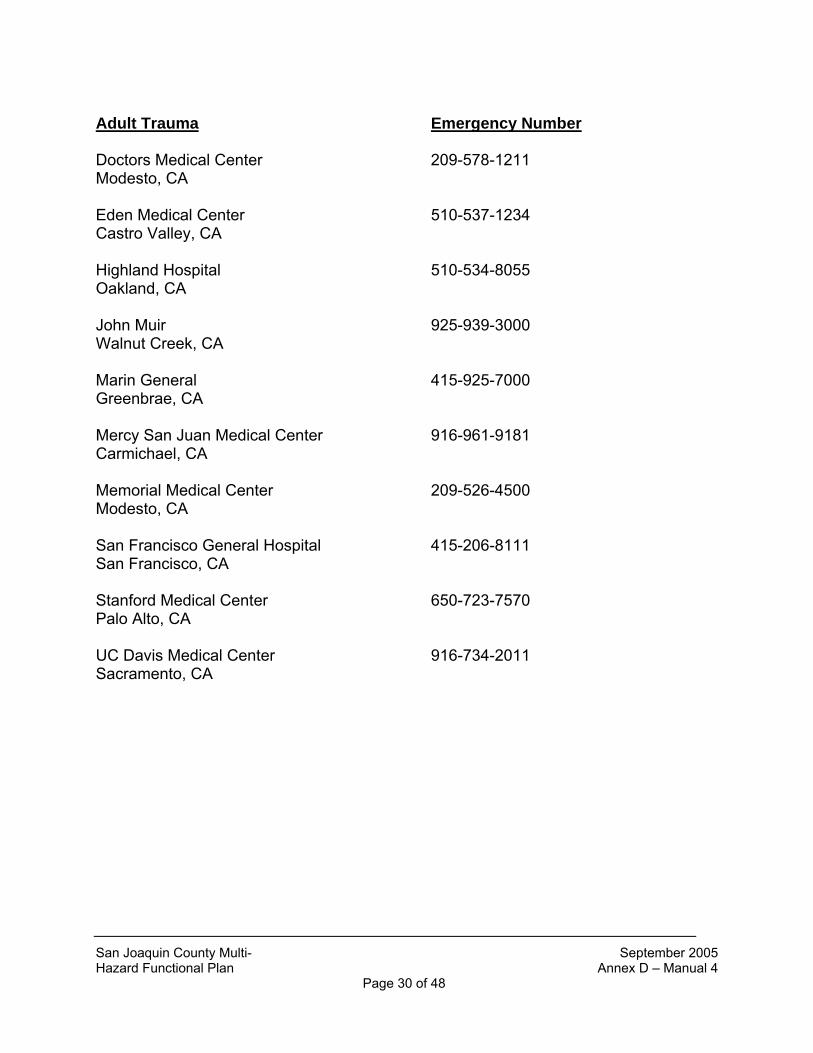
Adult Trauma Emergency Number Doctors Medical Center 209-578-1211 Modesto, CA Eden Medical Center 510-537-1234 Castro Valley, CA Highland Hospital 510-534-8055 Oakland, CA John Muir 925-939-3000 Walnut Creek, CA Marin General 415-925-7000 Greenbrae, CA Mercy San Juan Medical Center 916-961-9181 Carmichael, CA Memorial Medical Center 209-526-4500 Modesto, CA San Francisco General Hospital 415-206-8111 San Francisco, CA Stanford Medical Center 650-723-7570 Palo Alto, CA UC Davis Medical Center 916-734-2011 Sacramento, CA

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 31 of 48
Appendix F Sample Mutual Aid Memorandum of Understanding
Statement of Understanding
BETWEEN XYZ HOSPITAL
AND XYZ EXTENDED CARE FACILTY
I. PURPOSE The purpose of this Statement of Understanding is to define the relationship between XYZ Medical Center and XYZ Extended Care Facility, in preparing for, and responding to the physical and emotional needs of individuals, groups, and families in disaster relief situations. This disaster relief and response may be met through the joint efforts of XYZ Medical Center and XYZ Extended Care Facility. II. AREAS OF AGREEMENT AND COOPERATION XYZ Medical Center and XYZ Extended Care Facility, agree to when possible to cooperate in the following areas of endeavor:
Cooperative utilization of volunteer and paid staff to meet the community’s healthcare needs in the event of a disaster. XYZ Hospital is responsible for the care of individuals who are admitted to the hospital and require medical care, special medical equipment and/or continuing medical surveillance. In the event of a major disaster, local hospital resources may be overwhelmed with patients requiring acute care services. Patients that are not requiring critical care services may need to be transferred to alternative care sites in order to ensure that critically ill or injured individuals are able to be care for in an acute care setting. In such an event, XYZ Hospital would seek the cooperation of XYZ Extended Care Facilty as an alternative care site for stable patients requiring ongoing admission.
Transferal of all persons requiring a fully equipped and properly staffed facility will be a high priority and will be coordinated jointly by the San Joaquin County Disaster Control Facility.
Prior to seeking emergency transfer of stable patients, XYZ Hospital will:
● Utilize internal disaster procedures to implement surge capacity procedures including:

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 32 of 48
o Activation of the Facility Emergency Operations Center o Implementation of disaster staffing procedures (including medical staff) o Discharge of all appropriate inpatients o Cancellation of all elective surgeries
● Utilize state and local mutual aid agreements and the county Disaster Control Facility to seek acute care facility transfer arrangements.
● Provide all patient records, necessary equipment, and medications to ensure continuity of care for transferred patients.
XYZ Extended Care Facilty agrees to serve as an alternative care site for stable XYZ Hospital inpatients requiring ongoing medical care during a major disaster. Acceptance of transfer is not mandated by this agreement. It is understood by both parties that this is a good faith agreement based upon a desire to serve public health needs during extreme circumstances. Additionally, it is agreed that both agencies will participate in city/county disaster drills to enhance their understanding of roles and responsibilities. Both agencies agree to formulate internal emergency management plans and adopt local Operational Area Response Plans to address and detail the operational policies and procedures to outline the cooperative efforts under this Statement of Understanding. IV. PUBLICATION AND DISSEMINATION OF DIRECTIVES Both agencies agree to jointly publish this agreement and to disseminate its content through appropriate methods and channels to its executive, managerial, and supervisory staffs, any volunteer or paid staff providing disaster relief services, and as a basis of coordination with superior, affiliated, associated, or subservient units, departments, divisions, or organizations. V. EFFECTIVE DATE, MODIFICATION, AND TERMINATION This agreement shall become effective upon the execution by authorized individuals of both organizations. It must be ratified by appropriate authority within two years of its execution and may continue in force with or without subsequent modification or amendment until terminated. Modifications shall be by the same means as original execution, including the same obligations of publication and dissemination of such modifications. Termination may be by either party to the other with a minimum of thirty calendar days’ prior written notice. This agreement shall not be construed to be an instrument of binding performance, contractual obligation, or any other form of enforceable instrument. It is designed to communicate the intentions of the two organizations to cooperate in various means, methods, and areas of endeavors.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 33 of 48
SIGNATURES AUTHORIZED BY: (CEO) XYZ Hospital Date: ____________ (CEO) XYZ Extended Care Facility Date: ____________

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 34 of 48
Appendix G San Joaquin County Acute Hospital Chemical Agent Response
Summary of Decontamination Capabilities
Acute Care
Decon Abilities
Dam
eron
H
ospi
tal
Doc
tors
H
ospi
tal o
f M
ante
ca
Lodi
M
emor
ial
Hos
pita
l
Kai
ser
Hos
pita
l M
ante
ca
San
Joaq
uin
Gen
eral
H
ospi
tal
St. J
osep
h’s
Med
ical
C
ente
r
Sutte
r Tra
cy
Com
mun
ity
Hos
pita
l
Permanent Indoor Decon
Facilities
0 0 0 0 1 0 0
Permanent Outdoor Decon
Facilities
0 1 0 0 0 0 0
Temporary Outdoor Decon
Facilities
1 0 1 1 1 1 1
Anticipated Hourly Pt.
Capacity of Decon
Facilities
12 10 5 3 60 10 10
Summary: All local acute care hospitals have permanent indoor/outdoor decontamination facilities and/or temporary outdoor decontamination facilities. Estimated hourly emergency decontamination capacity totals 110 patients per hour.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 35 of 48
Appendix H
San Joaquin County Acute Care Biological Response Isolation Room Summary
Isolation Room
Estimates
Dam
eron
H
ospi
tal
Doc
tors
H
ospi
tal o
f M
ante
ca
Lodi
M
emor
ial
Hos
pita
l
Kai
ser
Hos
pita
l M
ante
ca
San
Joaq
uin
Gen
eral
H
ospi
tal
St. J
osep
h’s
Med
ical
C
ente
r
Sutte
r Tra
cy
Com
mun
ity
Hos
pita
l
# Negative Pressure Rooms
19 4 4 3 19 8 2
#Negative Pressure Rooms in ED
6 0 0 1 4 1 0
# Ventilators on hand
16 9 37 6 24 20 6
Average # Ventilators in daily
use
8 3 17 2 10 10 1
Ventilators available (above normal use) = 67 Total Acute Care Isolation Rooms = 59

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 36 of 48
Appendix I San Joaquin County MMRS Designated CCPs CCP’s or FTS may be established when local hospitals become overwhelmed. CCP’s, serve as victim treatment sites, collection areas and transferring of patients outside the Operational Area and Region IV. The following CCP locations are listed below in priority:
• The Stockton Metropolitan Airport San Joaquin County runs the airport. The airport is suitable for large fixed wing aircraft; including a 747 and rotorcraft. The airport has vacant hangers, fire department (Montezuma Fire Department), and other real estate near the airport that could be made available on short notice.
• Rough and Ready Island This island covers 1,459 acres, and is located west of Stockton adjacent to the Stockton Port. This facility has several empty warehouses, two fire stations, and several acres of vacant land suitable for landing large helicopters. • San Joaquin County Fairgrounds
The facility has a large parking lot, suitable for helicopter landing. Potential casualty treatment areas include the racetrack, arena, and parking lot. The parking lot may also be used for evacuation via helicopter.
• Oak Grove Regional Park
This county park in North Stockton has a flat, wide-open field and few structures. It is suitable for landing large military helicopters. Other parks and golf courses are also available, but have limited aircraft access.
• University of the Pacific Sports Fields
The fields are located in the City of Stockton. They are suitable for landing smaller helicopters. Patients could be staged in the parking lot.
San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 37 of 48
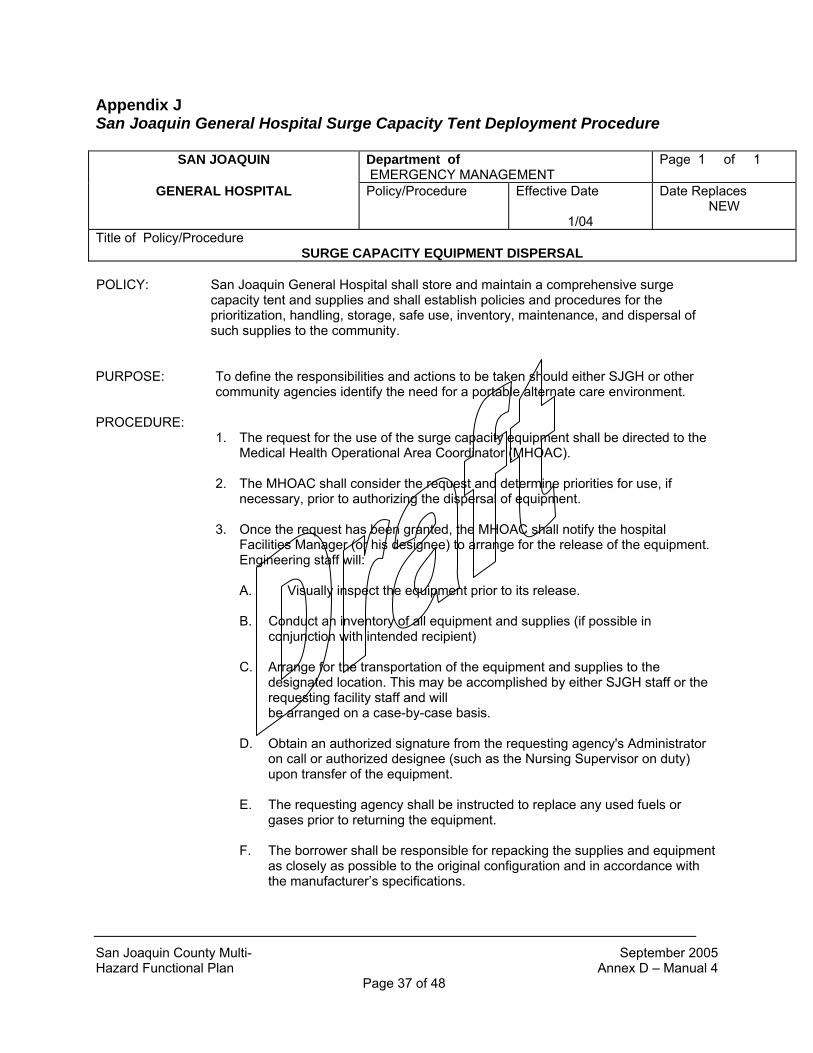
Appendix J San Joaquin General Hospital Surge Capacity Tent Deployment Procedure
SAN JOAQUIN Department of EMERGENCY MANAGEMENT
Page 1 of 1
GENERAL HOSPITAL Policy/Procedure
Effective Date
1/04
Date Replaces NEW
Title of Policy/Procedure
SURGE CAPACITY EQUIPMENT DISPERSAL POLICY: San Joaquin General Hospital shall store and maintain a comprehensive surge
capacity tent and supplies and shall establish policies and procedures for the prioritization, handling, storage, safe use, inventory, maintenance, and dispersal of such supplies to the community.
PURPOSE: To define the responsibilities and actions to be taken should either SJGH or other
community agencies identify the need for a portable alternate care environment. PROCEDURE:
1. The request for the use of the surge capacity equipment shall be directed to the Medical Health Operational Area Coordinator (MHOAC).
2. The MHOAC shall consider the request and determine priorities for use, if
necessary, prior to authorizing the dispersal of equipment.
3. Once the request has been granted, the MHOAC shall notify the hospital Facilities Manager (or his designee) to arrange for the release of the equipment. Engineering staff will:
A. Visually inspect the equipment prior to its release.
B. Conduct an inventory of all equipment and supplies (if possible in conjunction with intended recipient)
C. Arrange for the transportation of the equipment and supplies to the
designated location. This may be accomplished by either SJGH staff or the requesting facility staff and will be arranged on a case-by-case basis.
D. Obtain an authorized signature from the requesting agency's Administrator
on call or authorized designee (such as the Nursing Supervisor on duty) upon transfer of the equipment.
E. The requesting agency shall be instructed to replace any used fuels or gases prior to returning the equipment.
F. The borrower shall be responsible for repacking the supplies and equipment
as closely as possible to the original configuration and in accordance with the manufacturer’s specifications.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 38 of 48
G. Upon return of the equipment, all equipment and supplies shall be re-inventoried by the responsible individuals from both agencies. Replacement of any missing or damaged items shall be the responsibility of the borrower.
AUTHOR: Medical Health Operational Area Coordinator Plant Manager Emergency Management Committee Chair

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 39 of 48
Appendix K San Joaquin General Hospital Surge Capacity Tent Set Up Procedure
Dept. of Emergency Management
Page 1 of 8
SAN JOAQUIN GENERAL HOSPITAL Policy/Procedure
Effective 5/05 Replaces NEW
Title: Surge Capacity Equipment Use
POLICY: San Joaquin General Hospital stores and maintains surge capacity equipment for San Joaquin County Homeland Security.
PURPOSE: To provide additional patient care areas in order to decompress the Emergency Departments of San Joaquin County responding to a mass causality event and outline the setup and take down of the surge capacity equipment. PROCEDURE: Authorized agencies within San Joaquin County may have access to the surge capacity equipment in accordance with the Surge Capacity Equipment Dispersal Policy. The policy indicates that equipment may be obtained by authorization of the Medical Health Operational Area Coordinator (MHOAC). Upon authorized release, the surge capacity equipment will be delivered to a designated deployment site as arranged by the MHOAC.
SHELTER SETUP: 1. Establish a setup crew with a minimum of 6 people referred to as person A, B, C, D, E, F, etc.
2. Deposit surge capacity equipment near deployment site.
3. Place the bagged shelter near the site it is to be erected.
4. Release the outer retainer straps of the bag.
5. Open the two outer flap covers of the bag.
6. Remove the ground cloth and place it in the center of the deployment site.
• Colored straps should be toward the ends of the shelter.
7. Person A grasps the red straps. Person B grasps the black straps. Each person steps backward pulling the ground cloth open.
8. Place the shelter in the center of the ground cloth. Align the reflective markers with the black Velcro strips.
9. Release the two inner retainer straps of the bag.
10. Open the inner flap covers of the bag.
11. One person stands on the side of the bag toward the side of the ground cloth.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 40 of 48
Dept. of Emergency Management
Page 2 of 8
SAN JOAQUIN GENERAL HOSPITAL
Policy/Procedure Effective 5/05
Replaces NEW
Title: Surge Capacity Equipment Use
12. Each person grasps a corner edge of the cover and pulls the bag open.
• A sharp yank will aid in separating the Velcro.
13. Spread out the four cover flaps, so they are lying flat and smooth on the ground cloth.
14. Release the yellow colored compression belt around center of shelter. The shelter is now ready to erect.
15. Persons A, B, C, and D go to the four corners of the shelter. Working together, each person lifts the shelter slightly and steps backward, pulling the shelter open.
16. Each person steps backwards diagonally, and expands the shelter until the roof center is about one foot off the ground.
• Be careful to center the shelter on the ground cloth.
17. Remove all end wall fabric from the roof (top) of the shelter.
18. Remove any fabric that is looped over an upright portion of the frame.
19. Check the corners to ensure that no fabric is looped under the lower corner node.
20. Persons A, B, C, and D go to the ends (where the doors will be) and lift the ends of the shelter up. Persons E and F, with push poles in hand, enter the shelter.
21. Persons A, B, C, and D hold the shelter above their heads.
22. With persons A, B, C, and D holding fast in the arms raised position, persons E and F quickly place the ends of the push poles on a node (where the metal ribs intersect with the plastic junction)
23. Persons E and F slowly raise the roof of the shelter by steadily, and in unison pushing upward on the push poles until the shelter is generally in an upright position.
24. Persons A, B, C, and D push on a node with one hand, while lifting slightly and pulling in on the red handle with the other hand, so that the wall is vertical.
25. Once vertical, persons A, B, C, and D attach the shelter to the ground cloth at the outside corner locations first, then the inside four snaps.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 41 of 48
Dept. of Emergency Management
Page 3 of 8
SAN JOAQUIN GENERAL HOSPITAL
Policy/Procedure Effective 5/05
Replaces NEW
Title: Surge Capacity Equipment Use
26. Persons A, B, C, and D snap together the red locking straps, located waist high right next to the
red handle. 27. Anchor the shelter using the appropriate anchors (stakes or sand bags).
GENERATOR SETUP: 1. Locate the generator in close proximity to the shelter.
• Set up down wind of shelter, if possible. 2. Ensure that the generator has adequate fuel and oil. 3. Run extension cords for the lights and portable A/C through the side openings provided for the
cords. LIGHT SETUP: 1. Attach light fixtures to frame of shelter in location desired. 2. Attach lights together using male and female connections to establish a single line of lights,
with one power source. 3. Push the extension cord out of one of the ports. 4. Attach the extension cord to power source (generator) via outlet adapter. PORTABLE BLOWER/HEATER SETUP: 1. Locate the blower/heater unit in close proximity to the shelter. 2. Attach the air duct between the unit and shelter. 3. Attach the extension cord to the power source (generator). 4. Attach regulator to propane tank. COT SETUP: 1. Assemble cots and place them inside the shelter for patient use (20 cots/shelter).
• Recommend 16 cots per shelter to allow for medical staff and equipment.
TAKE DOWN: 1. All equipment must be properly cleaned and decontaminated prior to take down and storage. Follow standard disinfection/decontamination guidelines to prevent cross contamination.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 42 of 48
Dept. of Emergency Management
Page 4 of 8
SAN JOAQUIN GENERAL HOSPITAL
Policy/Procedure Effective 5/05
Replaces NEW
Title: Surge Capacity Equipment Use
2. Disassemble cots and return to storage bags.
3. Disassemble portable blower/heater setup. Return ducts to storage bags.
4. Disassemble lights and power cords.
5. Disconnect generator and propane tank.
6. Remove any remaining equipment from the shelter.
7. Remove any cable or wiring lines pulled into the shelter.
8. Locate and lay out all shelter storage bags.
9. Release the door tie back lines and fully open all door closures.
10. Remove any objects (sandbags, stakes) securing shelter to ground.
11. Persons A, B, C, D, E, and F enter the shelter.
12. Persons E and F raise their push poles to ceiling, placing end on a node, and push and hold.
13. Persons A, B, C, and D release the inner ground cloth snaps, leaving the four outer corner snaps
in place.
14. Persons A, B, C, and D unsnap the red lock straps inside the shelter.
15. Verify all red straps are disconnected. • Caution: It is critical that all red lock straps be disconnected prior to dropping the shelter.
16. Use caution when performing the steps below. The shelter may drop on its own once the
supporting straps and snaps have been disconnected. Keep personnel clear of shelter at this stage.
17. Persons A, B, C, and D exit the shelter.
18. Persons E and F back out of the shelter as quickly as possible at each end, lowering the push
poles as they exit. Caution: All personnel must exit the shelter, it is unsafe to occupy.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 43 of 48
Dept. of Emergency Management
Page 5 of 8
SAN JOAQUIN GENERAL HOSPITAL
Policy/Procedure Effective 5/05
Replaces NEW
Title: Surge Capacity Equipment Use
19. Persons A and B go to the corners of the outside of the shelter on the same side. Persons A and B position themselves by the red straps on the outside edge of the shelter near the ground.
20. Persons A and B reach into the shelter with hand only and grasp the metal frame. Then disconnect the remaining corner ground cloth snaps at their locations.
• Caution: Do not enter the shelter, only reach in.
21. Persons C, D, E, and F should grasp the metal frame to prevent the shelter from dropping while cloth snaps are being released.
22. Persons A and B locate themselves 45 degrees from the shelter.
23. Grasp the ground level pull strap (on the frame), lift up slightly, and pull the bottom of the side of
the shelter outward.
24. Continue to move backward, holding the shelter side slightly off the ground, until the roof section falls down and inward.
25. Now the shelter is collapsed on the ground cloth. Persons A and B now disconnect the remaining
two ground cloth snaps.
26. Persons A, B, C and D grasp red straps at the corners. Pushing in and lifting slightly, walk and compact the shelter.
• Caution: Be careful to not step on shelter fabric as you compact the shelter.
27. Pull out end section and place on top of the frame. 28. With one person on each side, lift and pull the canopy from down between the upright scissor
beams, and place all canopy fabric on top of the frame. • Note: Removal of fabric from between the frame enables the shelter to be packed more
tightly.
29. With persons A, B, C, and D on each side, push the shelter together a final time.
30. Place compression strap around shelter, and tighten using “quick-release” method: Slide strap through, tighten, take slack of strap and double over without yet sliding through the D rings. When strap is doubled over in a loop, slide through the top D ring only, and tighten.
31. Rock shelter over onto its side. The weight of the shelter when on it’s side tends to squeeze it together more snuggly.
32. Rock the shelter again (toward one of the wide sides of the ground cloth) until the shelter is
upside down. Keep shelter on ground cloth to prevent soiling. Be sure to remember which sides are the doors. This is important for repacking.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 44 of 48
Dept. of Emergency Management
Page 6 of 8
SAN JOAQUIN GENERAL HOSPITAL
Policy/Procedure Effective 5/05
Replaces NEW
Title: Surge Capacity Equipment Use
33. Open the bag so that it is in the shape of a cross, and place it over the shelter. Place bag over
the shelter so that the two corner flaps are toward the sides of the shelter (the long sides). • Remember that the shelter is upside down at this point.
34. Attach a few inches of the Velcro on all four sides.
35. Roll shelter back to upright position, being careful to maintain the bag in its correctly centered position.
36. Pull up on flaps all around to settle shelter in bag, making the fit as snug and straight as possible.
37. Lay over flap that attached to Velcro on other side (this will be the set of flaps that does not have
the “Data Plate” on it).
38. Attach the two interior straps (if provided) fairly taut to compress the shelter. • At this stage, only two flaps remain. One has the “Data Plate” on it. That flap is the last flap
to be placed.
39. Attach any remaining portions of the Velcro. 40. Lift and remove the partially bagged shelter off of the ground cloth.
41. Brush and shake the ground cloth to remove dirt and other debris.
42. Carefully fold the ground cloth, using the “accordion” or “parachute fold.”
43. Fold first length-wise and then end-to-end, and make a finished fold about 3 feet square.
44. Make sure the label is on top and the red and black pair of pull straps are visible at each end.
45. Place the ground cloth on top of the shelter. Make sure the label is on top. Lift the two exterior
flap covers over the top of the shelter.
46. Pull taut and straight. Make sure that the label is visible. 47. Attach the two exterior straps. Crossing them will make the finished cube more compact.
48. Pull the closure flaps as straight and as taut as possible. 49. Realign and reattach the Velcro as necessary to ensure complete closure.
50. Align and tighten each strap as much as possible to compact the shelter.
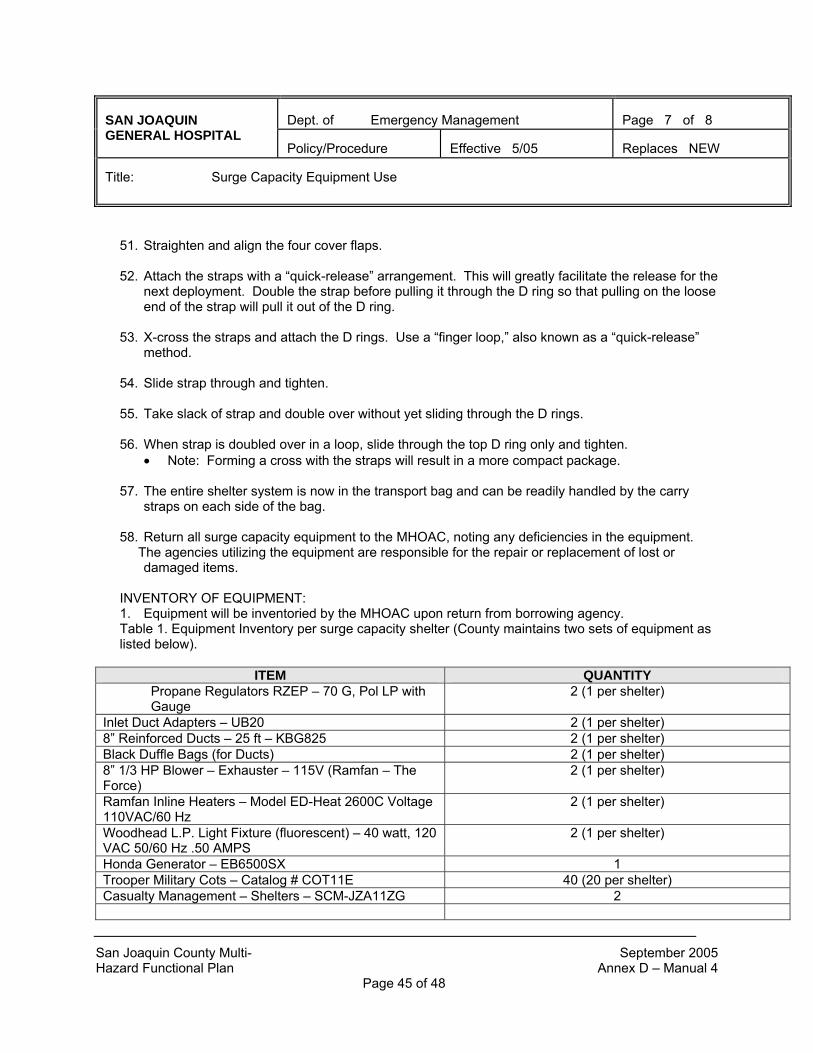
San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 45 of 48
Dept. of Emergency Management
Page 7 of 8
SAN JOAQUIN GENERAL HOSPITAL
Policy/Procedure Effective 5/05
Replaces NEW
Title: Surge Capacity Equipment Use
51. Straighten and align the four cover flaps.
52. Attach the straps with a “quick-release” arrangement. This will greatly facilitate the release for the next deployment. Double the strap before pulling it through the D ring so that pulling on the loose end of the strap will pull it out of the D ring.
53. X-cross the straps and attach the D rings. Use a “finger loop,” also known as a “quick-release”
method.
54. Slide strap through and tighten.
55. Take slack of strap and double over without yet sliding through the D rings.
56. When strap is doubled over in a loop, slide through the top D ring only and tighten. • Note: Forming a cross with the straps will result in a more compact package.
57. The entire shelter system is now in the transport bag and can be readily handled by the carry
straps on each side of the bag.
58. Return all surge capacity equipment to the MHOAC, noting any deficiencies in the equipment. The agencies utilizing the equipment are responsible for the repair or replacement of lost or damaged items. INVENTORY OF EQUIPMENT: 1. Equipment will be inventoried by the MHOAC upon return from borrowing agency. Table 1. Equipment Inventory per surge capacity shelter (County maintains two sets of equipment as listed below).
ITEM QUANTITY Propane Regulators RZEP – 70 G, Pol LP with Gauge
2 (1 per shelter)
Inlet Duct Adapters – UB20 2 (1 per shelter) 8” Reinforced Ducts – 25 ft – KBG825 2 (1 per shelter) Black Duffle Bags (for Ducts) 2 (1 per shelter) 8” 1/3 HP Blower – Exhauster – 115V (Ramfan – The Force)
2 (1 per shelter)
Ramfan Inline Heaters – Model ED-Heat 2600C Voltage 110VAC/60 Hz
2 (1 per shelter)
Woodhead L.P. Light Fixture (fluorescent) – 40 watt, 120 VAC 50/60 Hz .50 AMPS
2 (1 per shelter)
Honda Generator – EB6500SX 1 Trooper Military Cots – Catalog # COT11E 40 (20 per shelter) Casualty Management – Shelters – SCM-JZA11ZG 2

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 46 of 48
Dept. of Emergency Management
Page 8 of 8
SAN JOAQUIN GENERAL HOSPITAL
Policy/Procedure Effective 5/05
Replaces NEW
Title: Surge Capacity Equipment Use
SAFETY PRECAUTIONS:
• Never climb on shelter • Use the correct number of people for shelter carry, shelter deployment, and shelter strike. • Immediately vacate shelter upon releasing locking straps prior to collapsing shelter. • Keep open flames away from shelter fabrics. • Properly ventilate shelter when using fuel burning devices such as heaters and cooking
stoves. • Use the proper number of wind lines and stakes. • Use proper stakes for various soil types and soil conditions. • Avoid placing stakes and wind lines in front of doors, paths, and walkways. • Regularly inspect and adjust wind lines and ground stakes. • Prepare for expected harsh weather by adding ground stakes, wind lines, and sandbags. • Remove accumulated snow from the roof of the shelter. • Secure shelter during gusty winds by closing doors and window covers. • Change to correct stakes if soil conditions change such as after prolonged rain or thawing. • When carrying or deploying the shelter keep your back straight and lift with your legs and
arms • The system has been designed for rugged performance in rough field conditions. However, the shelter can be damaged if handled improperly. The following precautions in handling and storage must be carefully observed:
• Lift or push the shelters by grasping a node, fabric strap, or lift strap only. • Avoid lifting, pulling, or pushing the shelter with the fabric. • Stack the stored shelter only in its upright position and not on its side. Beams should be standing up, with nodes on the bottom and top. • When off-loading or loading, do not let the shelter drop or fall from the transport vehicle. • Do not over tighten the compression belt strap around the center of the shelter when compacting the shelter for re-packing in the transport bag. Compression belts at the top or bottom around the array of nodes may be pulled as tight as possible. • Do not place the shelter directly on the lift arms of a forklift; first place it on a pallet.
MAINTAINANCE: Pending SJGH Engineering response WRITTEN BY: San Joaquin General Hospital Emergency Department
REFERENCES: Surge Capacity Equipment Dispersal Policy Consequence Response Decontamination Shelter (CRDS) Operations Manual CC: San Joaquin County OES, San Joaquin County EMS, Dameron Hospital, St. Joseph’s Hospital Lodi Memorial Hospital, Doctor’s Hospital of Manteca, Kaiser Hospital of Manteca Sutter Tracy Hospital, Stockton Fire Department, San Joaquin General Hospital Engineering Department, Montezuma Fire Department APPROVED BY: Safety Committee (pending)

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 47 of 48
SECTION 7 REFERENCES
Agency for Healthcare Research and Quality (April, 2005). Altered standards of care in mass casualty events. Retrieved on September 11, 2005 from: http://www.ahrq.gov/research/altstand/altstand.pdf Agency for Healthcare Research and Quality (January, 2004). Optimizing surge capacity: Hospital assessment and planning. United States Department of Health Bioterrorism Brief # 3. Retrieved on March 28, 2005 from: http://www.ahrq.gov/news/ulp/btbriefs/btbrief3.htm American Hospital Association. Model Hospital Mutual Aid Memorandum of Understanding. Retrieved on September 9, 2005 from: http://www.hospitalconnect.com/aha/key_issues/disaster_readiness/resources/content/ModelHospitalMou.doc. Benson, M., Koenig, K., Schultz, C. (1996). Disaster triage: START then SAVE - a new method of dynamic triage for victims of a catastrophic earthquake. Prehospital Disaster Medicine 11(2), pp. 117-124. CNA Corporation (2004). Medical surge capacity and capability: A management system fro integrating medical and health resources during large scale emergencies. United States Department of Health and Human Services. Department of Health Services (2004). Nurse to patient staffing ratios for general acute care hospitals: Frequently asked questions. Retrieved on September 19, 2005 from: http://www.dhs.ca.gov/lnc/pubnotice/NTPR/R-37-01_FAQ2182004.pdf Garan, Lucow, & Miller (2005). EMTALA and Disasters. Retrieved on September 19, 2005 from: http://www.emtala.com/ Hick, J. (2004). No vacancy: Healthcare surge capacity in disasters. Retrieved on March 28, 2005 from: http://www.premierinc.com/all/safety/publications/08-04-downloads/08-surge-amacdc-email.ppt JCAHO (2003). Healthcare at the crossroads: Strategies for creating and sustaining community-wide emergency preparedness strategies. Koenig, K. (n.d.). Emergency management in the age of terrorism: Key policy issues for healthcare facilities. Retrieved on March 28, 2005 from: http://www.dtic.mil/ndia/2003terrorism/koenig.ppt.

San Joaquin County Multi- September 2005 Hazard Functional Plan Annex D – Manual 4 Page 48 of 48
Shelter Medical Group (2000). Shelter medical group report: Evacuation, care, and sheltering of the medically fragile. Stockton Fire Department (2003). City of Stockton response plan for terrorist incidents involving weapons of mass destruction or nuclear, biological, or chemical agents. MMRS Response Plan. United States Census Bureau (2005). California quick facts: San Joaquin County. Retrieved on March 28, 2005 from:http://quickfacts.census.gov/qfd/states/06/06077.html