safety and biocompatibility in perfect balance · safety and biocompatibility in perfect balance...
TRANSCRIPT
Safety and biocompatibility in perfect balance
Peritoneal Dialysis
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite U1
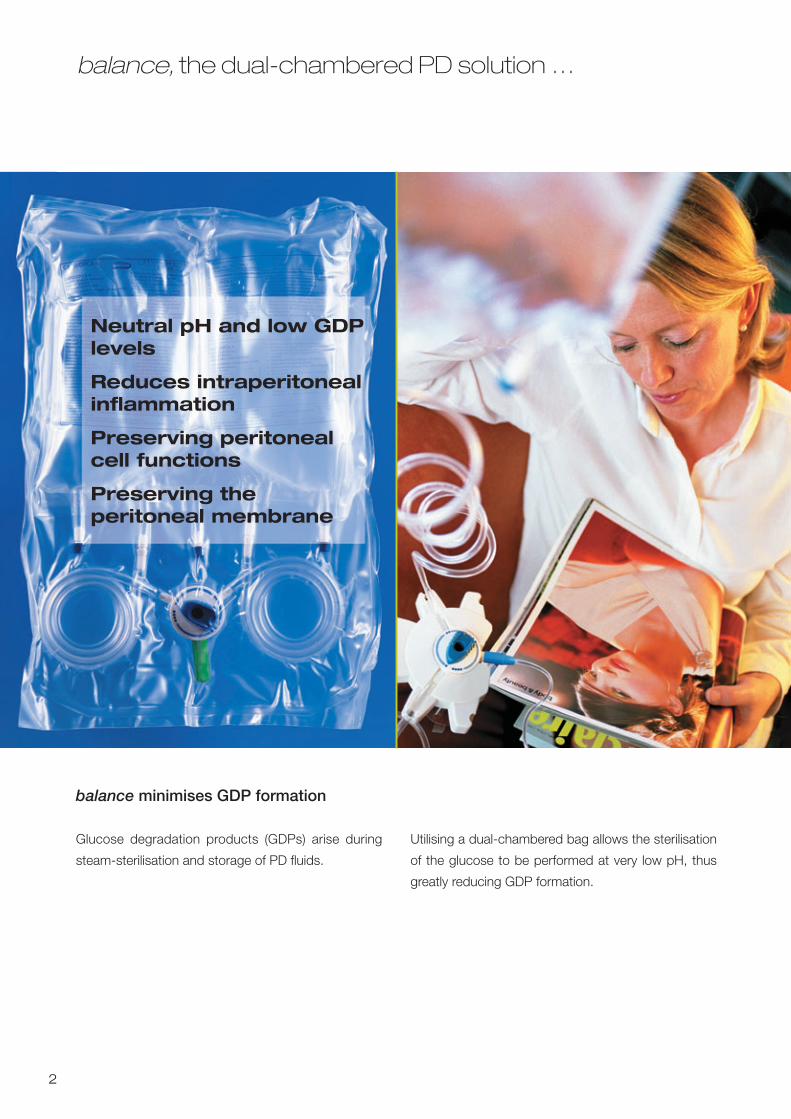
balance, the dual-chambered PD solution …
2
Glucose degradation products (GDPs) arise during
steam-sterilisation and storage of PD fluids.
Neutral pH and low GDPlevels
Reduces intraperitonealinflammation
Preserving peritonealcell functions
Preserving the peritoneal membrane
Utilising a dual-chambered bag allows the sterilisation
of the glucose to be performed at very low pH, thus
greatly reducing GDP formation.
balance minimises GDP formation
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite U2
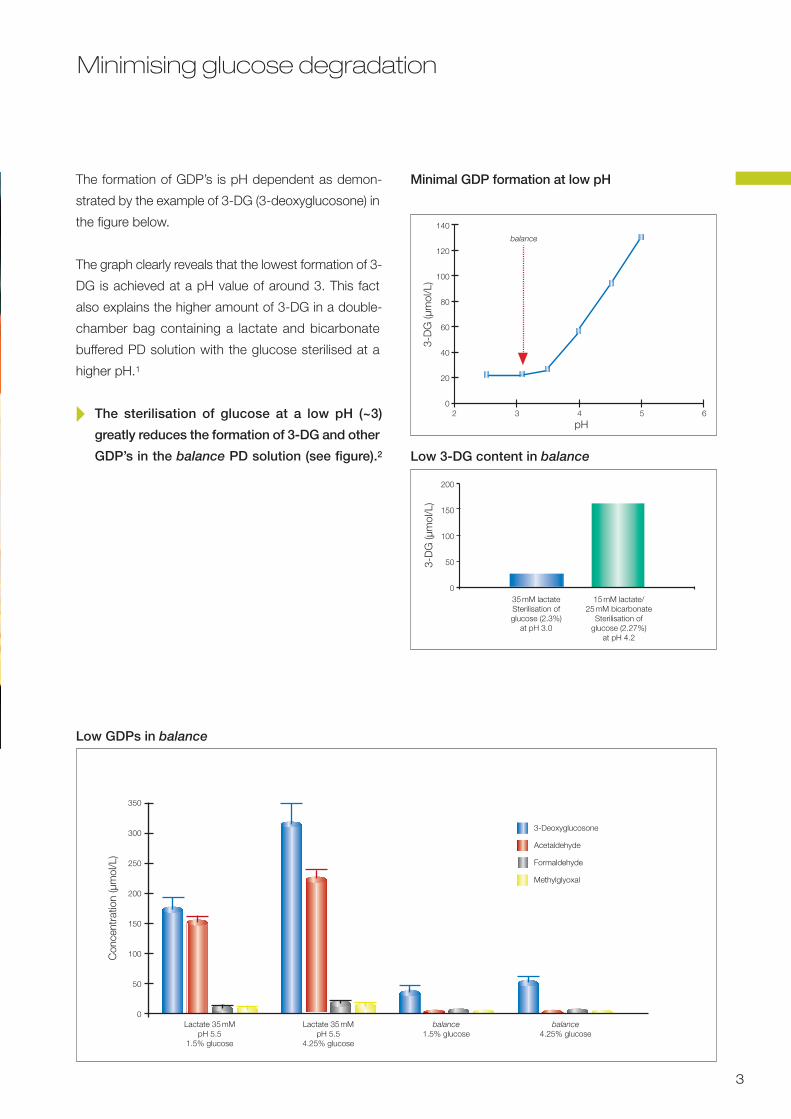
Minimising glucose degradation
3
The formation of GDP’s is pH dependent as demon-
strated by the example of 3-DG (3-deoxyglucosone) in
the figure below.
The graph clearly reveals that the lowest formation of 3-
DG is achieved at a pH value of around 3. This fact
also explains the higher amount of 3-DG in a double-
chamber bag containing a lactate and bicarbonate
buffered PD solution with the glucose sterilised at a
higher pH.1
� The sterilisation of glucose at a low pH (~3)
greatly reduces the formation of 3-DG and other
GDP’s in the balance PD solution (see figure).2
350
300
250
200
150
100
50
0
3-Deoxyglucosone
Acetaldehyde
Formaldehyde
Methylglyoxal
Low GDPs in balance
Con
cent
ratio
n (µ
mol
/L)
Lactate 35mM Lactate 35mM balance balancepH 5.5 pH 5.5 1.5% glucose 4.25% glucose
1.5% glucose 4.25% glucose
2 3 4 5 6
pH
140
120
100
80
60
40
20
0
Minimal GDP formation at low pH
balance
3-D
G (µ
mol
/L)
Low 3-DG content in balance
200
150
100
50
035mM lactateSterilisation ofglucose (2.3%)
at pH 3.0
15mM lactate/25mM bicarbonate
Sterilisation ofglucose (2.27%)
at pH 4.2
3-D
G (µ
mol
/L)
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite 3
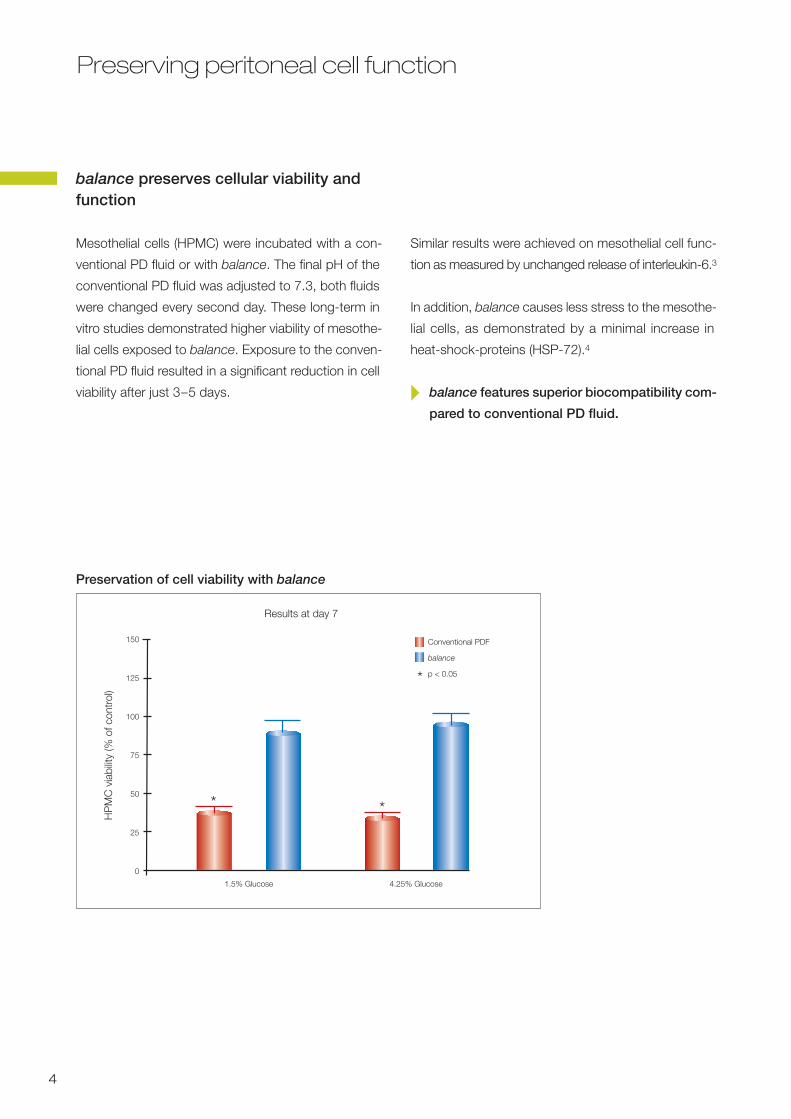
Preserving peritoneal cell function
4
balance preserves cellular viability andfunction
Mesothelial cells (HPMC) were incubated with a con-
ventional PD fluid or with balance. The final pH of the
conventional PD fluid was adjusted to 7.3, both fluids
were changed every second day. These long-term in
vitro studies demonstrated higher viability of mesothe-
lial cells exposed to balance. Exposure to the conven-
tional PD fluid resulted in a significant reduction in cell
viability after just 3–5 days.
**
Results at day 7
Similar results were achieved on mesothelial cell func-
tion as measured by unchanged release of interleukin-6.3
In addition, balance causes less stress to the mesothe-
lial cells, as demonstrated by a minimal increase in
heat-shock-proteins (HSP-72).4
� balance features superior biocompatibility com-
pared to conventional PD fluid.
Conventional PDF
balance
p < 0.05*
150
125
100
75
50
25
0
HP
MC
via
bilit
y (%
of c
ontr
ol)
1.5% Glucose 4.25% Glucose
Preservation of cell viability with balance
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite 4
Preserving the peritoneal membrane
5
balance reduces AGE formation
GDPs rather than glucose play a paramount role as
promotors for the formation of AGEs (advanced glyca-
tion end products), in particular 3-DG 5, 6, 7. Accu-
mulation of AGEs in the peritoneal membrane is asso-
ciated with increased permeability of the peritoneal
membrane and ultrafiltration reduction.8,9
Human serum albumin (HSA) was incubated with dif-
ferent commercially available PD solutions and a con-
trol solution. The formation of the AGE product CML
(Nε-(Carboxymethyl)lysine) was measured.
� In vitro AGE formation with balance is as low as
with sterile filtered control PD solution. 10
AGE formation is due to GDPs rather than high glucose concentration
Conventional PDF pH neutral; 4.25% glucose
Sterile filtered PDf pH neutral; 4.25% glucose (Control)
balance pH neutral; 4.25% glucose
1.0
0.8
0.6
0.4
0.2
0
0 10 20 30 40
Days of incubation
CM
L (u
nits
/mg
HS
A)
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite 5
Less peritoneal damage by balance
6
Rats were exposed twice daily for six weeks to con-
ventional PD fluid or balance, both with 4.25% glucose
concentration. At the beginning and at the end of the
study a 4-hour dwell was performed to evaluate signs
of intraperitoneal inflammation. Additionally, after six
weeks, the rats were sacrificed and the peritoneal
membranes were histologically evaluated according to
a semiquantitative scale.
In rats treated with conventional PD fluid signs of
intraperitoneal inflammation did not change during the
study, whereas with balance the intensity of inflamma-
tion decreased (cell count, p<0.01; neutrophil/ macro-
phage ratio, p<0.05; hyaluronan, p<0.05).11
Less peritoneal fibrosis with balance
� Long-term exposure to balance causes less
peritoneal inflammation, less collagen synthe-
sis and less fibrosis in animals.
Lightmicroscopy, semiquantitive scale:
• peritoneal thickening• presence of the peritoneal stratification• presence of neovascularisation
p < 0.05
Conventional balancePDF
8
7
6
5
4
3
2
1
0
Mic
rosc
opic
sca
le
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite 6
Less vasodilation with balance
7
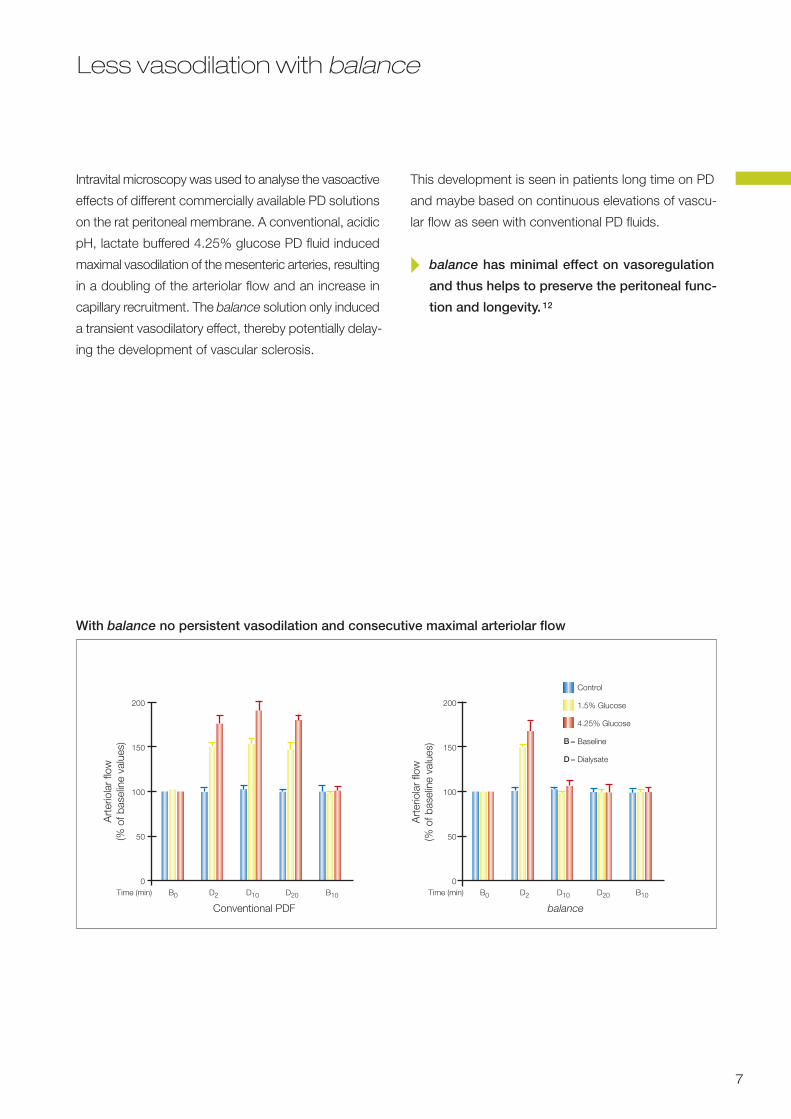
Intravital microscopy was used to analyse the vasoactive
effects of different commercially available PD solutions
on the rat peritoneal membrane. A conventional, acidic
pH, lactate buffered 4.25% glucose PD fluid induced
maximal vasodilation of the mesenteric arteries, resulting
in a doubling of the arteriolar flow and an increase in
capillary recruitment. The balance solution only induced
a transient vasodilatory effect, thereby potentially delay-
ing the development of vascular sclerosis.
With balance no persistent vasodilation and consecutive maximal arteriolar flow
This development is seen in patients long time on PD
and maybe based on continuous elevations of vascu-
lar flow as seen with conventional PD fluids.
� balance has minimal effect on vasoregulation
and thus helps to preserve the peritoneal func-
tion and longevity. 12
Control
1.5% Glucose
4.25% Glucose
Baseline
Dialysate
B=
D=
Time (min) B0 D2 D10 D20 B10 Time (min) B0 D2 D10 D20 B10
Conventional PDF balance
200
150
100
50
0
200
150
100
50
0
Art
erio
lar
flow
(% o
f bas
elin
e va
lues
)
Art
erio
lar
flow
(% o
f bas
elin
e va
lues
)
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite 7
European Balance Trial EBT
8
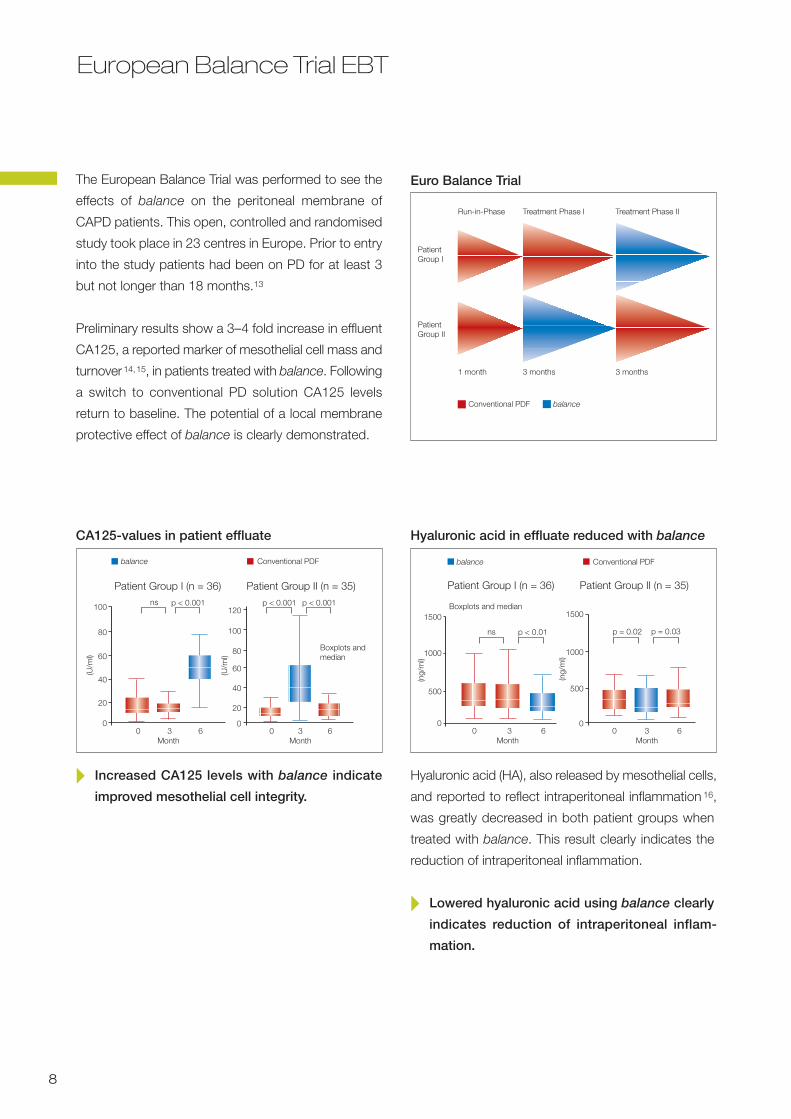
The European Balance Trial was performed to see the
effects of balance on the peritoneal membrane of
CAPD patients. This open, controlled and randomised
study took place in 23 centres in Europe. Prior to entry
into the study patients had been on PD for at least 3
but not longer than 18 months.13
Preliminary results show a 3–4 fold increase in effluent
CA125, a reported marker of mesothelial cell mass and
turnover14,15, in patients treated with balance. Following
a switch to conventional PD solution CA125 levels
return to baseline. The potential of a local membrane
protective effect of balance is clearly demonstrated.
Euro Balance Trial
Run-in-Phase Treatment Phase I Treatment Phase II
1 month 3 months 3 months
Conventional PDF balance
PatientGroup I
PatientGroup II
� Increased CA125 levels with balance indicate
improved mesothelial cell integrity.
Hyaluronic acid (HA), also released by mesothelial cells,
and reported to reflect intraperitoneal inflammation 16,
was greatly decreased in both patient groups when
treated with balance. This result clearly indicates the
reduction of intraperitoneal inflammation.
� Lowered hyaluronic acid using balance clearly
indicates reduction of intraperitoneal inflam-
mation.
balance Conventional PDF
100
80
60
40
20
0
120
100
80
60
40
20
00 3 6 0 3 6
(U/m
l)
(U/m
l)
CA125-values in patient effluate
ns p < 0.001
Month Month
p < 0.001 p < 0.001
Boxplots andmedian
Patient Group I (n = 36) Patient Group II (n = 35)
balance Conventional PDF
Hyaluronic acid in effluate reduced with balance
Patient Group I (n = 36) Patient Group II (n = 35)
p < 0.01 p = 0.02 p = 0.03ns
0 3 6Month
0 3 6Month
(ng/
ml)
(ng/
ml)
1500
1000
500
0
1500
1000
500
0
Boxplots and median
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite 8
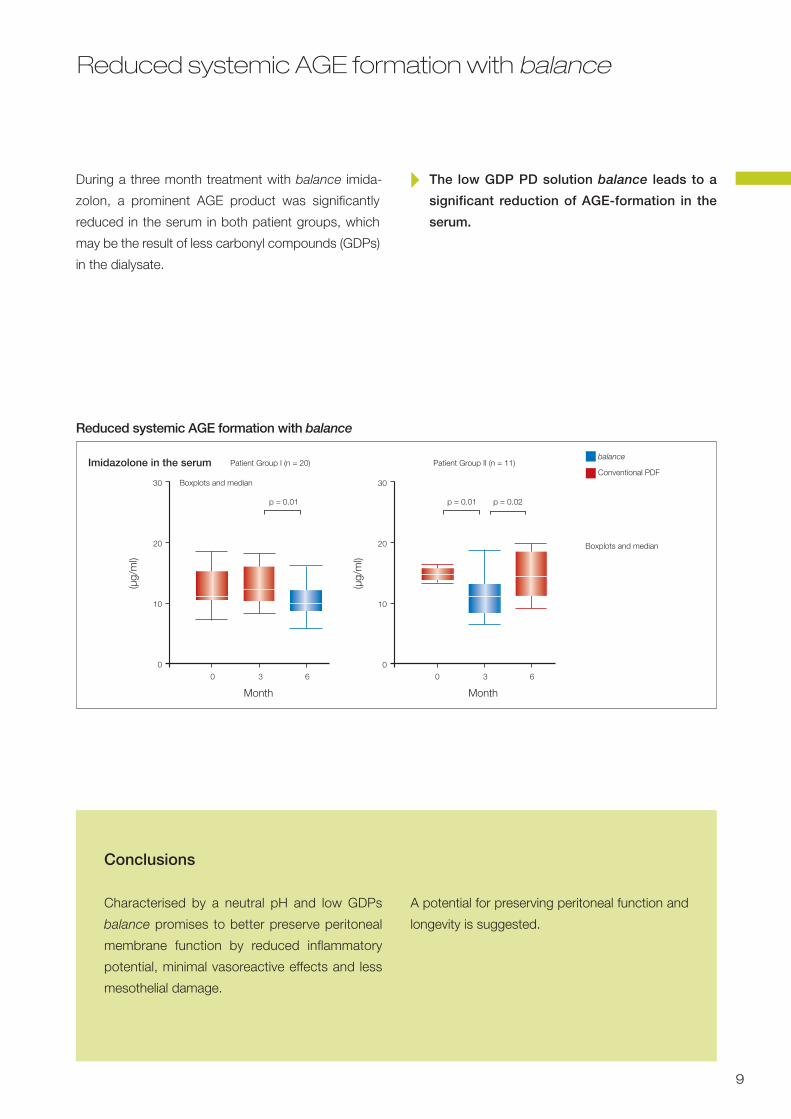
Reduced systemic AGE formation with balance
9
During a three month treatment with balance imida-
zolon, a prominent AGE product was significantly
reduced in the serum in both patient groups, which
may be the result of less carbonyl compounds (GDPs)
in the dialysate.
Conclusions
Characterised by a neutral pH and low GDPs
balance promises to better preserve peritoneal
membrane function by reduced inflammatory
potential, minimal vasoreactive effects and less
mesothelial damage.
A potential for preserving peritoneal function and
longevity is suggested.
� The low GDP PD solution balance leads to a
significant reduction of AGE-formation in the
serum.
Boxplots and median
Boxplots and median
Reduced systemic AGE formation with balance
30
20
10
0
(µg/
ml)
0 3 6
Month
0 3 6
Month
30
20
10
0
(µg/
ml)
balance
Conventional PDF
p = 0.01 p = 0.01 p = 0.02
Patient Group I (n = 20) Patient Group II (n = 11)Imidazolone in the serum
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite 9
The details make the difference
10
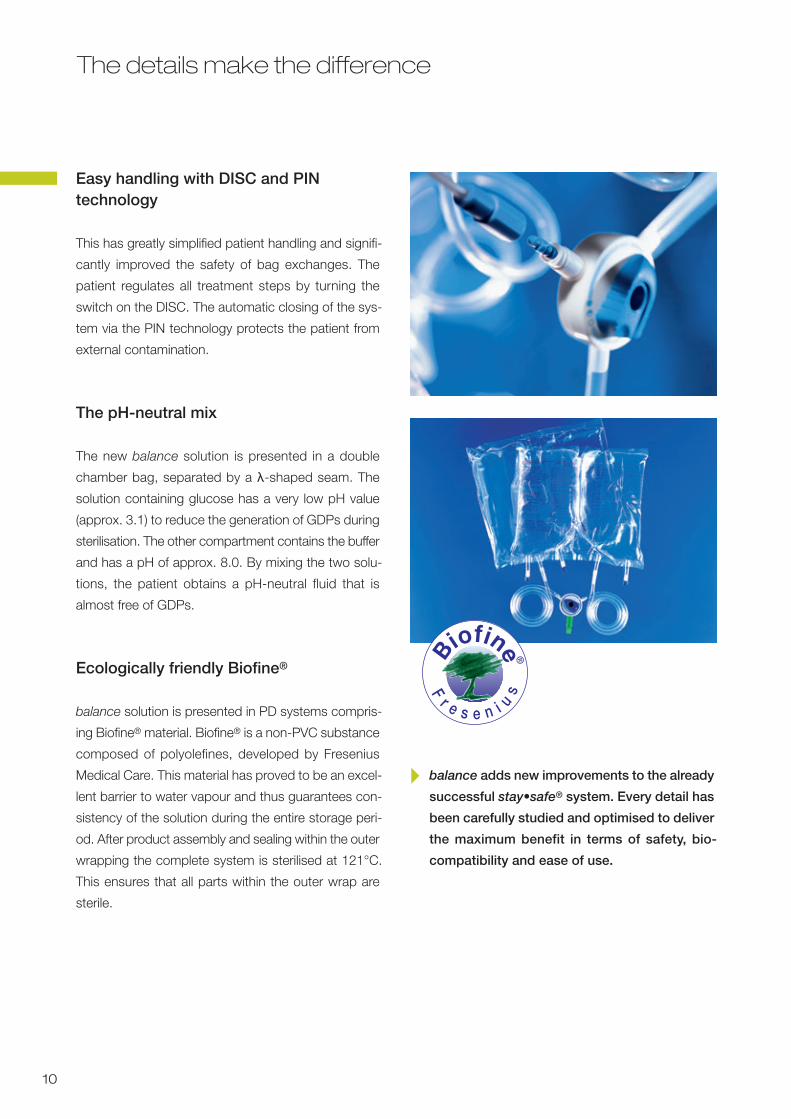
Easy handling with DISC and PIN technology
This has greatly simplified patient handling and signifi-
cantly improved the safety of bag exchanges. The
patient regulates all treatment steps by turning the
switch on the DISC. The automatic closing of the sys-
tem via the PIN technology protects the patient from
external contamination.
The pH-neutral mix
The new balance solution is presented in a double
chamber bag, separated by a λ-shaped seam. The
solution containing glucose has a very low pH value
(approx. 3.1) to reduce the generation of GDPs during
sterilisation. The other compartment contains the buffer
and has a pH of approx. 8.0. By mixing the two solu-
tions, the patient obtains a pH-neutral fluid that is
almost free of GDPs.
Ecologically friendly Biofine®
balance solution is presented in PD systems compris-
ing Biofine® material. Biofine® is a non-PVC substance
composed of polyolefines, developed by Fresenius
Medical Care. This material has proved to be an excel-
lent barrier to water vapour and thus guarantees con-
sistency of the solution during the entire storage peri-
od. After product assembly and sealing within the outer
wrapping the complete system is sterilised at 121°C.
This ensures that all parts within the outer wrap are
sterile.
� balance adds new improvements to the already
successful stay•safe® system. Every detail has
been carefully studied and optimised to deliver
the maximum benefit in terms of safety, bio-
compatibility and ease of use.
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite 10
References
11
1 Zimmeck T, Tauer A, Fuenfrocken M, Pischetsrieder M. How to reduce3-deoxyglucosone and acetaldehyde in peritoneal dialysis fluids. PeritDial Int. 2002;22(3): 350-6.
2 Tauer A, Schmitt R, Knerr T, et al. Formation of the glucose degradationproduct 3-deoxyglucosone and other carbonyl-compounds in single- ordouble-chamber peritoneal dialysis fluids. Perit Dial Int. 2000;20:142.
3 Witowski J, Bender TO, Wisniewska-Elnur J, et al. Mesothelial toxicityof peritoneal dialysis fluids is related primarily to glucose degradationproducts, not to glucose per se. Perit Dial Int. 2003;23(4):381-90.
4 Arbeiter K, Bidmon B, Endemann M, et al. Peritoneal dialysate fluidcomposition determines heat shock protein expression patterns inhuman mesothelial cells. Kidney Int. 2001;60:1930-7.
5 Niwa H, Takeda A, Wakai M, et al. Accelerated formation of N epsilon-(carboxymethyl) lysine, an advanced glycation end product, by glyoxaland 3-deoxyglucosone in cultured rat sensory neurons. BiochemBiophys Res Commun. 1998;248:93-7.
6 Lamb EJ, Cattell WR, Dawnay AB. In vitro formation of advanced glycationend products in peritoneal dialysis fluid. Kidney Int. 1995;47:1768-1774.
7 Schalkwijk CG, Posthuma N, ten Brink HJ, ter Wee PM, Teerlink T.Induction of 1,2-dicarbonyl compounds, intermediates in the formationof advanced glycation end-products, during heat-sterilization of glu-cose-based peritoneal dialysis fluids. Perit Dial Int. 1999;19:325-333.
8 Nakayama M, Kawaguchi Y, Yamada K, et al. Immunohistochemicaldetection of advanced glycosylation end-products in the peritoneumand its possible pathophysiological role in CAPD. Kidney Int.1997;51:182-6.
9 Honda K, Nitta K, Horita S, Yumura W, Nihei H, Nagai R, Ikeda K,Horiuchi S. Accumulation of advanced glycation end products in theperitoneal vasculature of continuous ambulatory peritoneal dialysispatients with low ultrafiltration. Nephrol Dial Transplant. 1999;14:1541-9.
10 Tauer A, Knerr T, Niwa T, et al. In vitro formation of Nε-(Carboxymethyl)-lysine and imidazolones under conditions similar to continuous ambula-tory peritoneal dialysis. Biochem Biophys Res Commun.2001;280:1408-14.
11 Wieczorowska-Tobis K, Polubinska A, Schaub T P, et al. Influence ofneutral-pH dialysis solutions on the peritoneal membrane: a long-terminvestigation in rats. Perit Dial Int. 2001;21 Suppl 3:S108-13.
12 Mortier S, De Vriese AS, Van De Voorde et al. Hemodynamic effects ofperitoneal dialysis solutions on the peritoneal membrane: Role of acidity,buffer choice, glucose concentration, and glucose degradation prod-ucts. J Am Soc Nephrol. 2002;13:480-9.
13 Williams JD, Topley N, Craig KJ, Mackenzie RK, Pischetsrieder M, LageC, Passlick-Deetjen J, on behalf of the Euro Balance Trial group. TheEuro-Balance Trial: The effect of a new biocompatible peritoneal dialysisfluid (balance) on the peritoneal membrane. Kidney International in press.
14 Krediet RT. Dialysate cancer antigen 125 concentration as marker ofperitoneal membrane status in patients treated with chronic peritonealdialysis. Perit Dial Int. 2001;21:560-7.
15 Visser CE, Brouwer-Steenbergen JJ, Betjes MG, et al. Cancer antigen125: a bulk marker for the mesothelial mass in stable peritoneal dialysispatients. Nephrol Dial Transplant. 1995;10:64-9.
16 Yung S, Coles GA, Williams JD, et al. The source and possible significanceof hyaluronan in the peritoneal cavity. Kidney Int. 1994;46(2):527-33.
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite 11
Fresenius Medical Care Deutschland GmbH · 61346 Bad Homburg v. d. H. · Germany · Phone: +49 (0) 6172-609-0 · Fax: +49 (0) 6172-609-2191Head office: Else-Kröner-Straße 1 · 61352 Bad Homburg v. d. H. · Germany
www.fmc-ag.com
732
729
1/3
GB
(0 P
UR
09.
06)
© C
opyr
ight
200
6 Fr
esen
ius
Med
ical
Car
e D
euts
chla
nd G
mb
H
Information
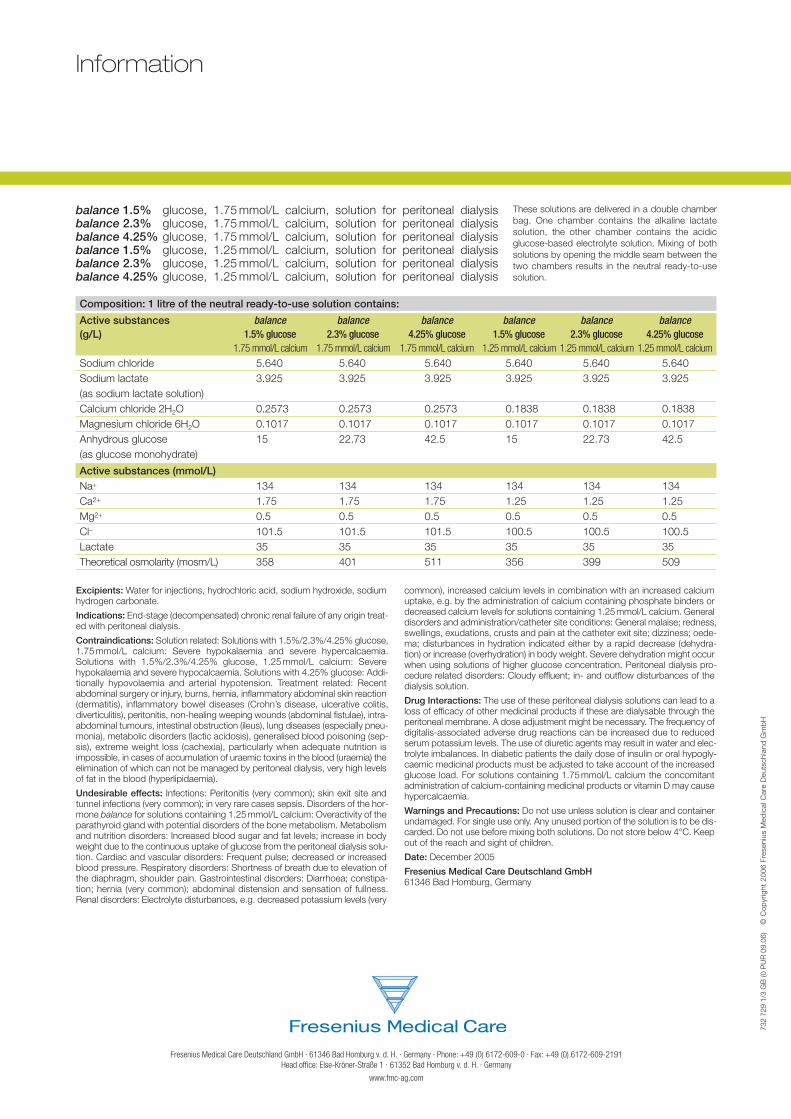
balance 1.5% glucose, 1.75 mmol/L calcium, solution for peritoneal dialysisbalance 2.3% glucose, 1.75 mmol/L calcium, solution for peritoneal dialysisbalance 4.25% glucose, 1.75 mmol/L calcium, solution for peritoneal dialysisbalance 1.5% glucose, 1.25 mmol/L calcium, solution for peritoneal dialysisbalance 2.3% glucose, 1.25 mmol/L calcium, solution for peritoneal dialysisbalance 4.25% glucose, 1.25 mmol/L calcium, solution for peritoneal dialysis
Composition: 1 litre of the neutral ready-to-use solution contains:
Active substances balance balance balance balance balance balance(g/L) 1.5% glucose 2.3% glucose 4.25% glucose 1.5% glucose 2.3% glucose 4.25% glucose
1.75 mmol/L calcium 1.75 mmol/L calcium 1.75 mmol/L calcium 1.25 mmol/L calcium 1.25 mmol/L calcium 1.25 mmol/L calcium
Sodium chloride 5.640 5.640 5.640 5.640 5.640 5.640Sodium lactate 3.925 3.925 3.925 3.925 3.925 3.925(as sodium lactate solution)Calcium chloride 2H2O 0.2573 0.2573 0.2573 0.1838 0.1838 0.1838Magnesium chloride 6H2O 0.1017 0.1017 0.1017 0.1017 0.1017 0.1017Anhydrous glucose 15 22.73 42.5 15 22.73 42.5(as glucose monohydrate)
Active substances (mmol/L)Na+ 134 134 134 134 134 134Ca2+ 1.75 1.75 1.75 1.25 1.25 1.25Mg2+ 0.5 0.5 0.5 0.5 0.5 0.5Cl– 101.5 101.5 101.5 100.5 100.5 100.5Lactate 35 35 35 35 35 35Theoretical osmolarity (mosm/L) 358 401 511 356 399 509
Excipients: Water for injections, hydrochloric acid, sodium hydroxide, sodiumhydrogen carbonate.
Indications: End-stage (decompensated) chronic renal failure of any origin treat-ed with peritoneal dialysis.
Contraindications: Solution related: Solutions with 1.5%/2.3%/4.25% glucose,1.75 mmol/L calcium: Severe hypokalaemia and severe hypercalcaemia.Solutions with 1.5%/2.3%/4.25% glucose, 1.25 mmol/L calcium: Severehypokalaemia and severe hypocalcaemia. Solutions with 4.25% glucose: Addi-tionally hypovolaemia and arterial hypotension. Treatment related: Recentabdominal surgery or injury, burns, hernia, inflammatory abdominal skin reaction(dermatitis), inflammatory bowel diseases (Crohn’s disease, ulcerative colitis,diverticulitis), peritonitis, non-healing weeping wounds (abdominal fistulae), intra-abdominal tumours, intestinal obstruction (ileus), lung diseases (especially pneu-monia), metabolic disorders (lactic acidosis), generalised blood poisoning (sep-sis), extreme weight loss (cachexia), particularly when adequate nutrition isimpossible, in cases of accumulation of uraemic toxins in the blood (uraemia) theelimination of which can not be managed by peritoneal dialysis, very high levelsof fat in the blood (hyperlipidaemia).
Undesirable effects: Infections: Peritonitis (very common); skin exit site andtunnel infections (very common); in very rare cases sepsis. Disorders of the hor-mone balance for solutions containing 1.25mmol/L calcium: Overactivity of theparathyroid gland with potential disorders of the bone metabolism. Metabolismand nutrition disorders: Increased blood sugar and fat levels; increase in bodyweight due to the continuous uptake of glucose from the peritoneal dialysis solu-tion. Cardiac and vascular disorders: Frequent pulse; decreased or increasedblood pressure. Respiratory disorders: Shortness of breath due to elevation ofthe diaphragm, shoulder pain. Gastrointestinal disorders: Diarrhoea; constipa-tion; hernia (very common); abdominal distension and sensation of fullness.Renal disorders: Electrolyte disturbances, e.g. decreased potassium levels (very
common), increased calcium levels in combination with an increased calciumuptake, e.g. by the administration of calcium containing phosphate binders ordecreased calcium levels for solutions containing 1.25mmol/L calcium. Generaldisorders and administration/catheter site conditions: General malaise; redness,swellings, exudations, crusts and pain at the catheter exit site; dizziness; oede-ma; disturbances in hydration indicated either by a rapid decrease (dehydra-tion) or increase (overhydration) in body weight. Severe dehydration might occurwhen using solutions of higher glucose concentration. Peritoneal dialysis pro-cedure related disorders: Cloudy effluent; in- and outflow disturbances of thedialysis solution.
Drug Interactions: The use of these peritoneal dialysis solutions can lead to aloss of efficacy of other medicinal products if these are dialysable through theperitoneal membrane. A dose adjustment might be necessary. The frequency ofdigitalis-associated adverse drug reactions can be increased due to reducedserum potassium levels. The use of diuretic agents may result in water and elec-trolyte imbalances. In diabetic patients the daily dose of insulin or oral hypogly-caemic medicinal products must be adjusted to take account of the increasedglucose load. For solutions containing 1.75 mmol/L calcium the concomitantadministration of calcium-containing medicinal products or vitamin D may causehypercalcaemia.
Warnings and Precautions: Do not use unless solution is clear and containerundamaged. For single use only. Any unused portion of the solution is to be dis-carded. Do not use before mixing both solutions. Do not store below 4°C. Keepout of the reach and sight of children.
Date: December 2005
Fresenius Medical Care Deutschland GmbH61346 Bad Homburg, Germany
These solutions are delivered in a double chamberbag. One chamber contains the alkaline lactate solution, the other chamber contains the acidic glucose-based electrolyte solution. Mixing of bothsolutions by opening the middle seam between thetwo chambers results in the neutral ready-to-usesolution.
balance_09.06_GB.qxd 27.09.2006 9:09 Uhr Seite U4