rheumatic fever
TRANSCRIPT

Rheumatic Fever and Rheumatic heart disease
Dr. Muhammad Imran
6/2/2015 1

Learning Outcomes
After attending this presentation the audience will be able to:
• Define Rheumatic fever
• Describe the Pathogenesis of Rheumatic fever(RF)
• Illustrate the Clinical features of RF
• Write the diagnosis of Rheumatic fever
• Devise the prevention of RF
6/2/2015 2
Rheumatic Fever
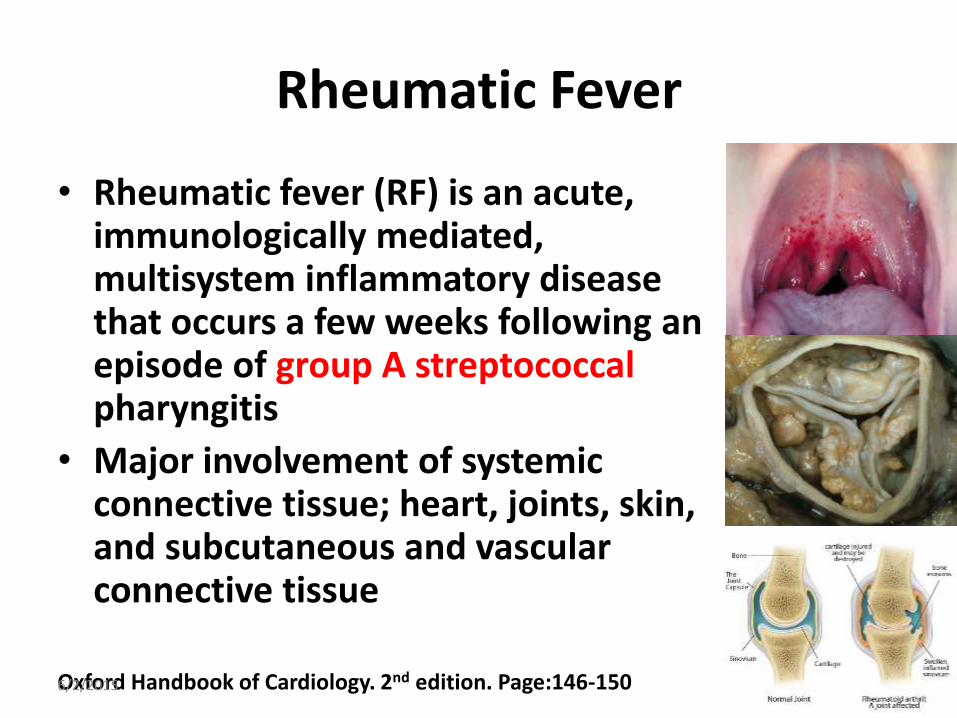
• Rheumatic fever (RF) is an acute, immunologically mediated, multisystem inflammatory disease that occurs a few weeks following an episode of group A streptococcal pharyngitis
• Major involvement of systemic connective tissue; heart, joints, skin, and subcutaneous and vascular connective tissue
Oxford Handbook of Cardiology. 2nd edition. Page:146-150 6/2/2015 3
Epidemiology
• <1:1000 in developed countries; 10:1000 schoolchildren in developing countries
• It is rarer, but still accounts for half of cardiac disease in the developing world
• Typically affects children aged 5–15 years from lower socio-economic
• No sex difference but mitral stenosis are more common in females
Oxford Handbook of Cardiology. 2nd edition. Page:146-150 6/2/2015 4
Pathology
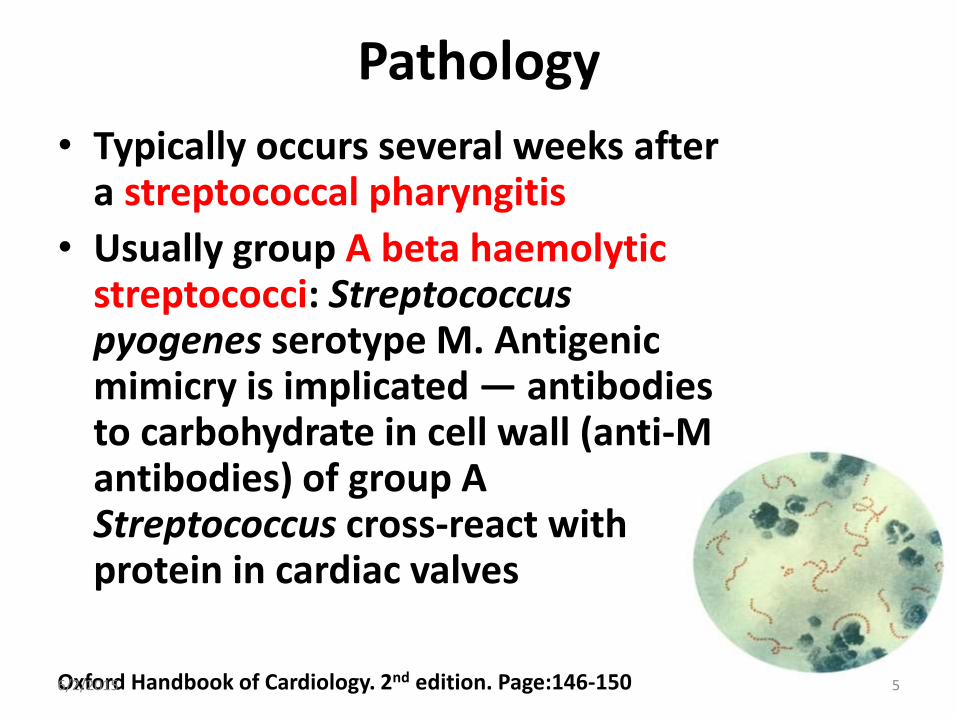
• Typically occurs several weeks after a streptococcal pharyngitis
• Usually group A beta haemolytic streptococci: Streptococcus pyogenes serotype M. Antigenic mimicry is implicated — antibodies to carbohydrate in cell wall (anti-M antibodies) of group A Streptococcus cross-react with protein in cardiac valves
Oxford Handbook of Cardiology. 2nd edition. Page:146-150 6/2/2015 5
Pathology (Continue)
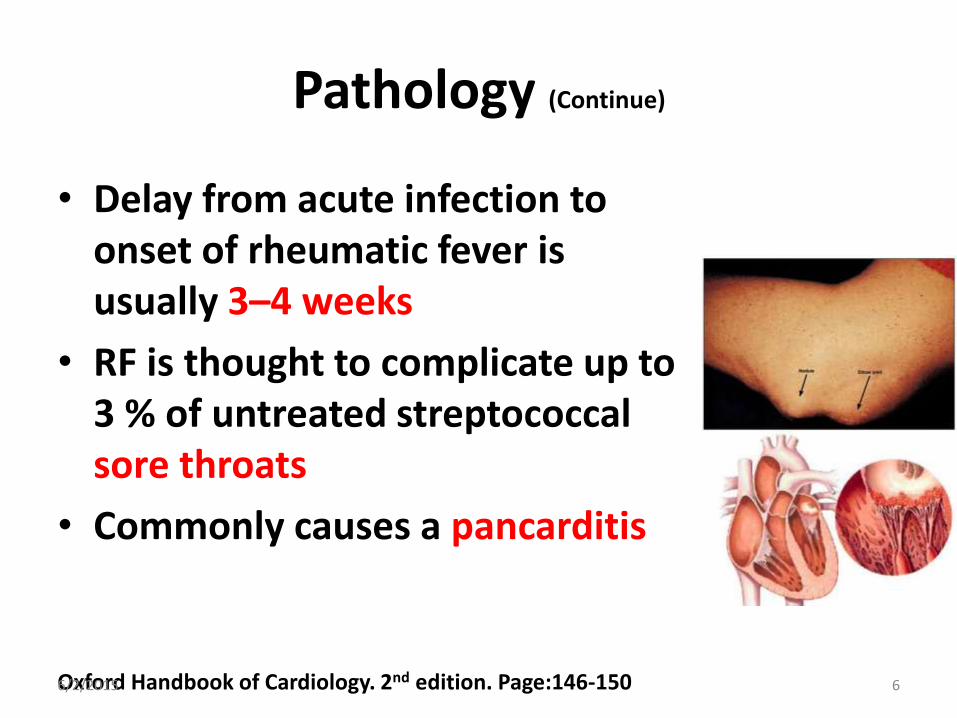
• Delay from acute infection to onset of rheumatic fever is usually 3–4 weeks
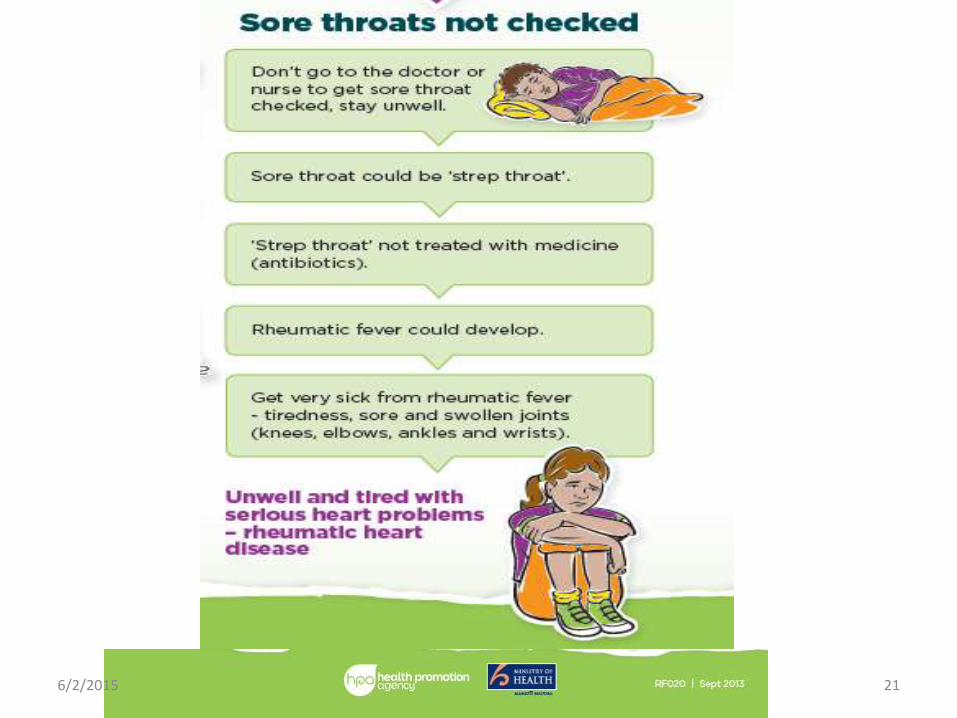
• RF is thought to complicate up to 3 % of untreated streptococcal sore throats
• Commonly causes a pancarditis
Oxford Handbook of Cardiology. 2nd edition. Page:146-150 6/2/2015 6
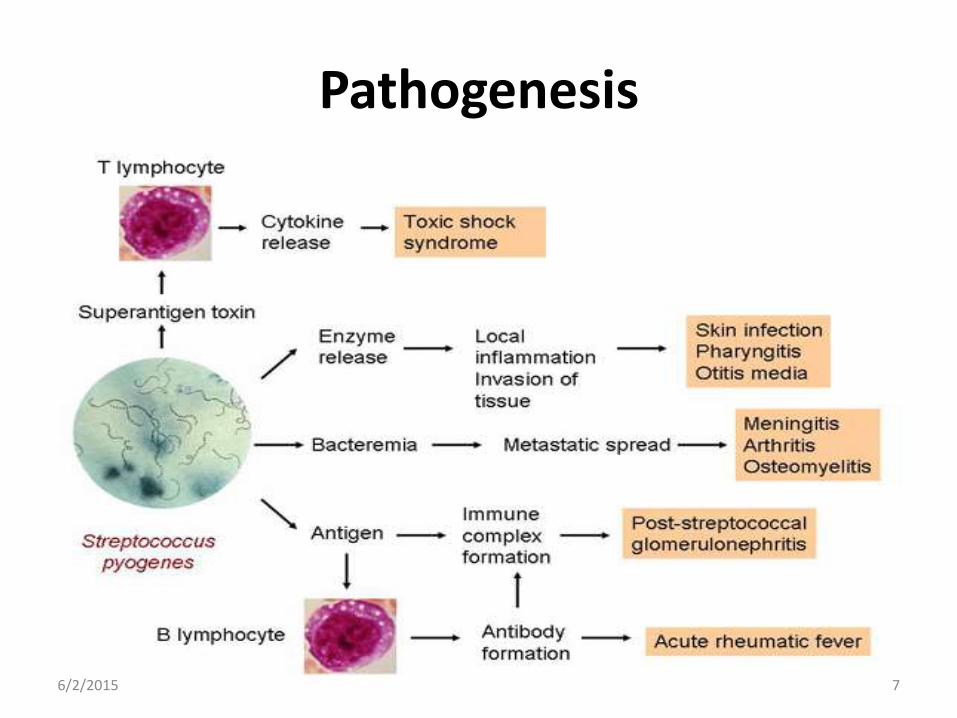
Pathogenesis
6/2/2015 7
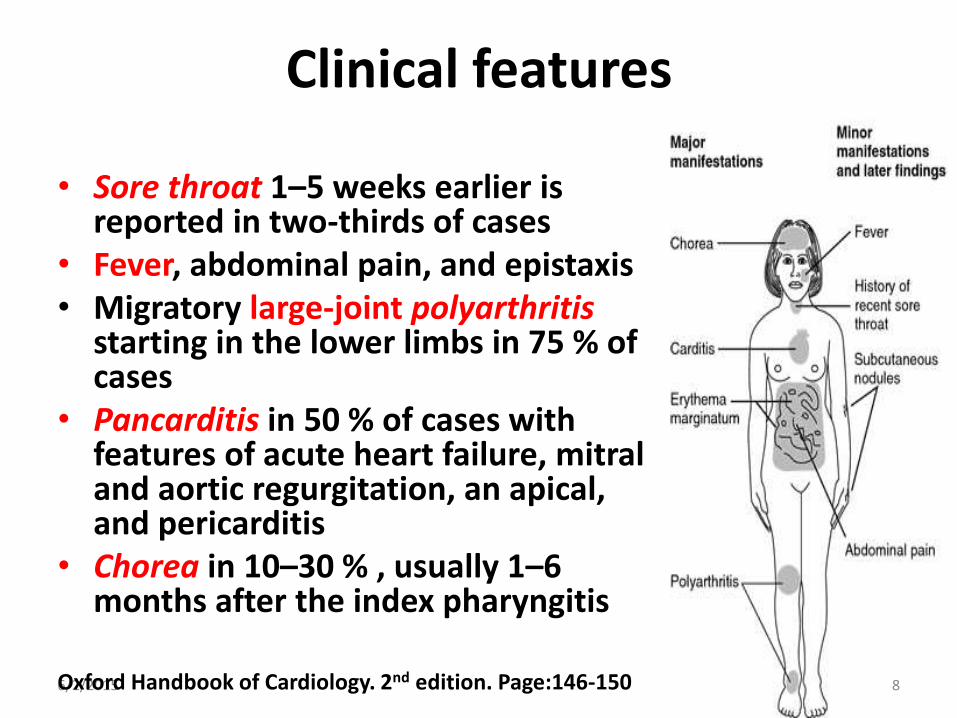
Clinical features
• Sore throat 1–5 weeks earlier is reported in two-thirds of cases
• Fever, abdominal pain, and epistaxis • Migratory large-joint polyarthritis
starting in the lower limbs in 75 % of cases
• Pancarditis in 50 % of cases with features of acute heart failure, mitral and aortic regurgitation, an apical, and pericarditis
• Chorea in 10–30 % , usually 1–6 months after the index pharyngitis
6/2/2015 8 Oxford Handbook of Cardiology. 2nd edition. Page:146-150
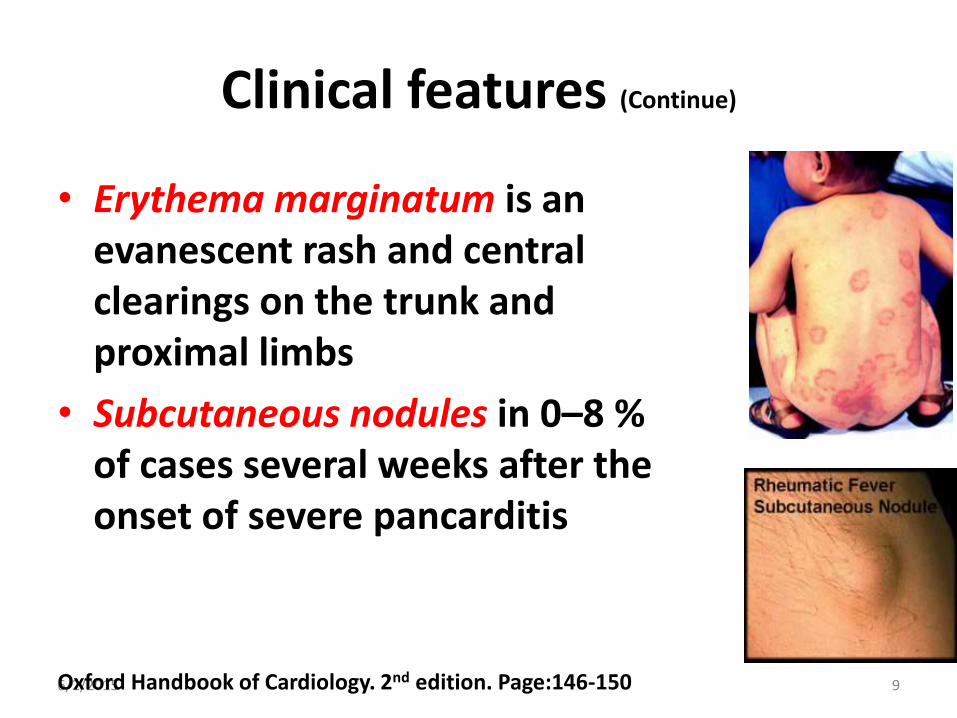
Clinical features (Continue)
• Erythema marginatum is an evanescent rash and central clearings on the trunk and proximal limbs
• Subcutaneous nodules in 0–8 % of cases several weeks after the onset of severe pancarditis
6/2/2015 9 Oxford Handbook of Cardiology. 2nd edition. Page:146-150

Diagnosis Criteria
Oxford Handbook of Cardiology. 2nd edition. Page:146-150 6/2/2015 10
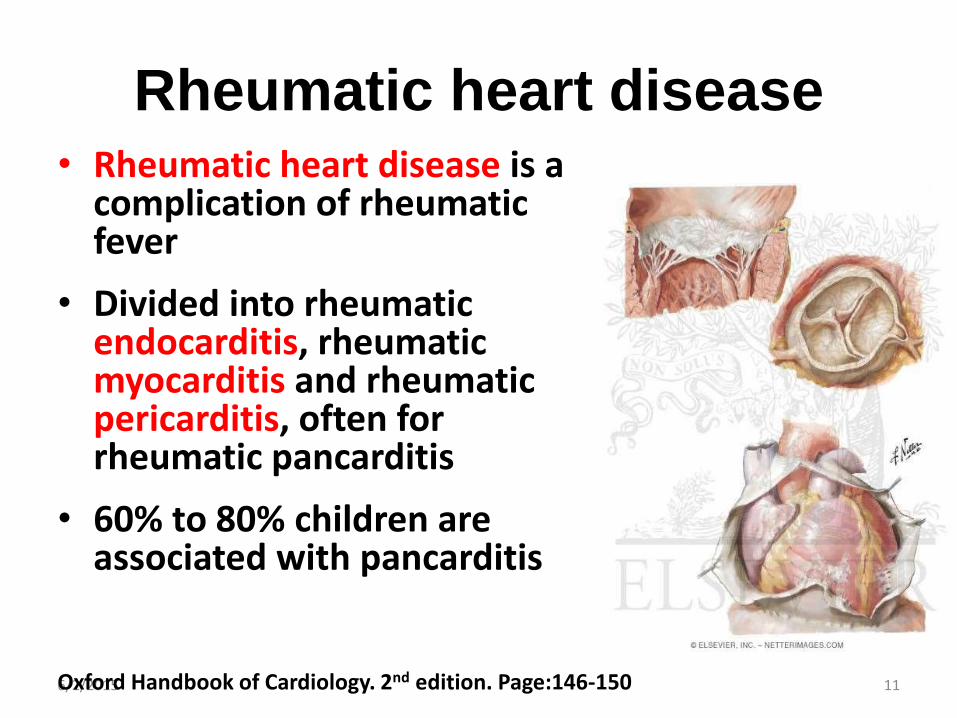
Rheumatic heart disease • Rheumatic heart disease is a
complication of rheumatic fever
• Divided into rheumatic endocarditis, rheumatic myocarditis and rheumatic pericarditis, often for rheumatic pancarditis
• 60% to 80% children are associated with pancarditis
6/2/2015 11 Oxford Handbook of Cardiology. 2nd edition. Page:146-150

6/2/2015 12
Key morphologic
features of acute
rheumatic heart
disease
Prevention
• The only known way to prevent rheumatic fever is to treat strep. throat infections promptly with a full course of appropriate antibiotics
6/2/2015 13 Oxford Handbook of Cardiology. 2nd edition. Page:146-150
Prevention (Continue)
• If you have or suspect you have rheumatic fever see your doctor or local health clinic
• If you have had rheumatic fever make sure you always have your regular penicillin injections
• Get regular check-ups at your local health clinic
• Do not ignore a sore throat. Consult your doctor
6/2/2015 14 Oxford Handbook of Cardiology. 2nd edition. Page:146-150
Prevention (Continue)
• Keep sores clean and covered
• Wash hands regularly
• Watch out for symptoms in children – people aged between 5 and 14
• Eat a healthy diet
6/2/2015 15 Oxford Handbook of Cardiology. 2nd edition. Page:146-150

Prevention (Continue)
Primary Prevention:
Primary prevention of rheumatic fever is possible with a 10-day course of penicillin therapy for streptococcal pharyngitis. However, primary prevention is not possible in all patients
Park's Pediatric Cardiology for Practitioners. 6th edition. Page: 603-610 6/2/2015 16

Secondary Prevention
Who should receive prophylaxis?
Patients with documented histories of rheumatic fever, including those with isolated
chorea and those without evidence of rheumatic heart disease, must receive prophylaxis
Park's Pediatric Cardiology for Practitioners. 6th edition. Page: 603-610 6/2/2015 17
Secondary Prevention (Continue)
For how long?
Ideally, patients should receive prophylaxis indefinitely. For patients who had acute rheumatic fever without carditis, the prophylaxis should continue for at least 5 years or until the person is 21 years of age
Park's Pediatric Cardiology for Practitioners. 6th edition. Page: 603-610 6/2/2015 18
Key message
6/2/2015 19

6/2/2015 20
6/2/2015 21

6/2/2015 22

6/2/2015 23