acute rheumatic fever (arf) & rheumatic
TRANSCRIPT

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 1/18
ACUTE RHEUMATIC FEVER (ARF) &
RHEUMATIC HEART DISEASE (RHD)
SYARIF HIDAYAT
RSUD SERANG

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 2/18
INTRODUCTION, DEFINITION,
PATHOPHYSIOLOGY
Streptococcusgroup A β
haemolyticusARF RHD

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 3/18
An immune-mediated, multisystem inflammatorydisease that follows group a streptococcal
infection.
Characterized by tissue inflammation that givesrise to typical clinical characteristics, includingcarditis, valvulitis, arthritis, chorea, erythemamarginatum, and subcutaneous nodules.
Carditis occurs in 30 –80% of patients with ARF, andat least 60% of untreated patients develop chronicRHD.
A
c
ut
e
R
he
u
m
a
ti
c
F
e
ve
r

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 4/18
Inflammation leads to neo vascularization, which enables furtherrecruitment of t cells, leading to granulomatous inflammation
Molecular mimicry between group a streptococcal antigens and human hosttissue is thought to be the basis of this cross-reactivity.
Both cross-reactive anti-bodies and cross-reactive t cells are believed to havea role in the disease.
Interaction between a group a streptococcal strain and a host seems to leadto an abnormal immune response and the development of autoimmunity.
8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 5/18
Predominantly affects the mitral valve and, less commonly, the aorticvalve.
Mitral insufficiency is the most common valvular lesion, particularly inthe early stages of the disease.
Mitral stenosis develops later as a result of persistent or recurrentvalvulitis, although rapid progression has been described in somedeveloping countries.
Patients with mitral insufficiency can remain relatively asymptomatic forup to 10 years, as a result of compensatory left atrial and left ventriculardilatation before the onset of left ventricular systolic dysfunction.
Tricuspid regurgitation can occur as a result of volume overload, usuallycaused by mitral stenosis.
R
h
eu
m
a
t
i
c
H
e
ar
t
D
i
s
e
a
s
e

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 6/18
DIAGNOSTIC CRITERIA & CATEGORY FOR
ARF & RHD
D
I
A
G
N
O
S
T
I
C
C
R
I
T
E
R
I
A
F
O
R
A
R
F
&
R
H
D
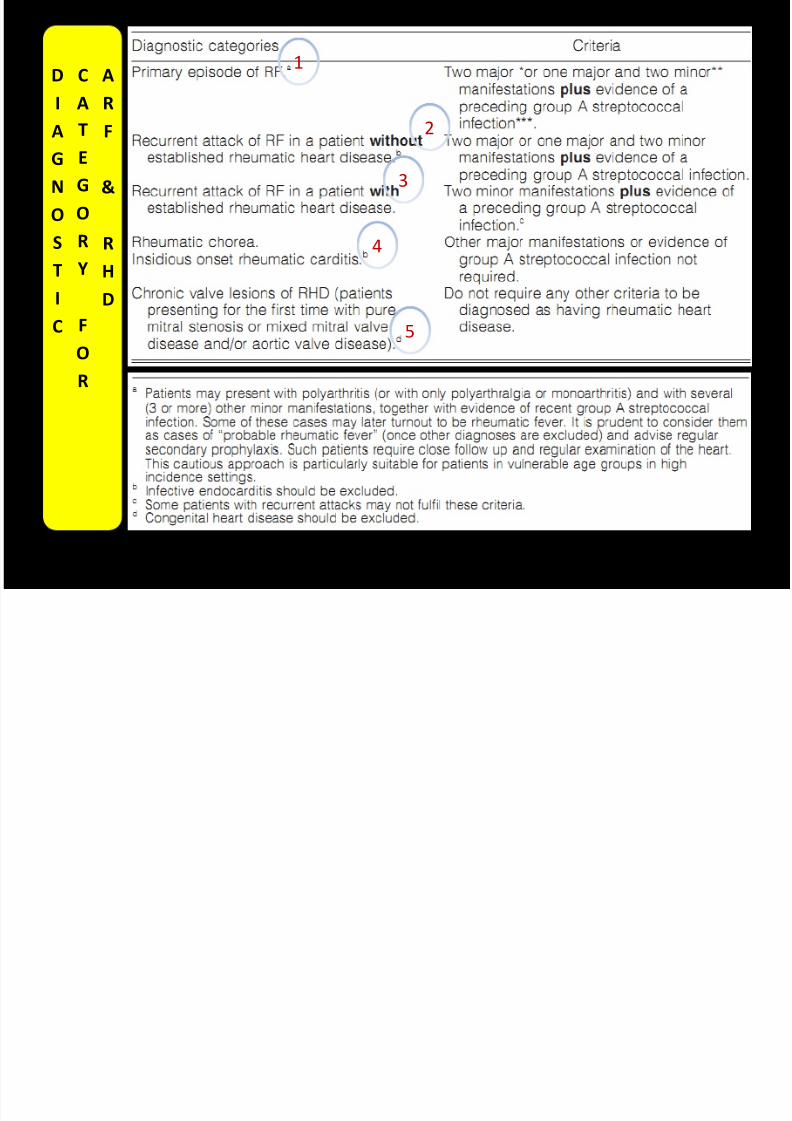
1) 2 MAYOR/ 1 MAYOR + 2 MINORMANIFESTATIONS PLUS …
2) 2 MINOR MANIFESTATIONS PLUS …
… PLUS EVIDENCE OF A PRECEDING GROUP
A STREPTOCOCCAL INFECTION
8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 7/18
D
I
AG
N
O
S
TI
C
C
A
TE
G
O
R
Y
F
O
R
A
R
F
&
R
HD
1
2
3
4
5

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 8/18
CARDITIS
POLYARTHITISMIGRANS
CHOREA
ERYTHEMAMARGINATUM
SUBCUTANEUSNODUL
Commonly presents as a heart murmur; Chest pain and/ordifficulty breathing may be present in more severe cases
Pain and swelling in more than one large joint (ankles, knees,wrists); Often the first complaint; Usually ‘migratory’ – finishesin one joint, begins in another
Twitchy, jerking movements and muscle weakness (most obvious in the face,hands and feet); May occur on both sides or only one side of body; Morecommon in teenagers and females (rare after age 20); May begin up to 3-6months after the streptococcal throat infection, and often occurs withoutother symptoms; Usually resolves within 6 weeks rarely (may last 6 monthsor more)
Painless, flat pink patches on the skin that spread outward in acircular pattern; Usually occurs early, may last months, rarelylasts years; Usually on the back or front of body, almost neveron the face; Hard to see in dark-skinned people
Painless lumps on the outside surfaces of elbows, wrists, knees,ankles in groups of 3-4 (up to 12) ; The skin is not red orinflamed; Last 1-2 weeks (rarely more than 1 month); Nodulesare more common when Carditis is also present

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 9/18
MANAGEMENT &
PREVENTION OF ARF
& RHD
Secondary
Primary

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 10/18
Group AStreptococcus β
heamolyticus
infection
ACUTE RHEUMATICFEVER
PRIMARY
PREVENTION
P
R
IM
A
R
Y
P
R
EV
E
N
T
IO
N
SORE THROATTREATMENT (Y)
VACCINE (N)
1) Oral penicillin V 500mg 2 –3 times per
day for 10 days [250mg for children], 50mg/kg amoxicillin per day for 10 days, or
2) A single 1,200,000u [600,000u forchildren ≤27 kg] dose of intramuscular
benzathine penicillin G

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 11/18
CLINICAL GROUPS BED REST (WEEKS) MOBILIZATION (WEEKS)
CARDITIS (+),ARTHRITIS (-)
2 2
CARDITIS (+),
CARDIOMEGALY (-)
4 4
CARDITIS (+),
CARDIOMEGALY (+)
6 6
CARDITIS (+), CHF (+) > 6 > 12Paracetamol; Salisilat : 100mg/kg in 4-5 dose (Max 6mg/d)
2weeks then 60-70mg/kg/d for 3-6weeks; Prednison :
2mg/kg/d (max 80mg/d) 2weeks tappering off 20-25% every
week; Carbamazepine, valproic acid, diazepam
FEVER,ARTHRITIS,CHOREA
Eradication; For 10days; QIDERYTHROMYCIN
Eradication; For 10days; 25-20mg/kg/d in 3
dose (max adults 50-1000mg/d)AMOXCILLINA
c
ut
e
R
he
u
m
a
ti
c
F
e
ve
r
DIURETICS, ACE-I/ARB, DIGOXIN, BB, A-THROMBOTIC
CARDITIS(PERICARDITIS,MYOCARDITIS,ENDOCARDITIS)

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 12/18

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 13/18
RHD MORBIDITY (CHF, AF, IE, CVD)
DEATH
CLINICAL MANAGEMENT
CHF MEDICATION
A-COAGULANTSURGERY/ INVASIVE NON
SURGERY
M
A
NA
G
E
M
EN
T
O
F
E
S
TA
B
L
I
SH
E
D
RH
D
SYMPTOMATIC THERAPY
MONITORING INR IN A-COAGULANT TH/ FOR AF &
POST REPLACEMENTSURGERY
SURGERY : REPAIR ORREPLACEMENT
INVASIVE NON SURGERY :BMV

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 14/18
CHF
AF
IE
CVD
DIURETICS, ACE-I/ARB, DIGOXIN, BB, A-THROMBOTIC
DIGOXIN, BB, A-THROMBOTIC, A-COAGULANT
ANTIBIOTICS, OPERATION
CARDIAC EMBOLI IN AF/ VEGETATIONS IN IE(CONTROLED AF, A-COAGULANT, OPERATION);NEUROLOGIST
C
L
IN
I
C
A
L
M
A
NA
G
E
M
EN
T

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 15/18
M
A
N
AG
E
M
E
N
T
O
F
P
A
T
IE
N
T
S
W
I
T
H
R
H
D
(
S
T
R
AT
I
F
I
E
D
B
Y
D
I
S
EA
S
E
S
E
V
E
R
I
T
Y )

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 16/18

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 17/18
Eritema marginatum = RF
Nodul subkutan = RF

8/12/2019 Acute Rheumatic Fever (Arf) & Rheumatic
http://slidepdf.com/reader/full/acute-rheumatic-fever-arf-rheumatic 18/18