reward-related reversal learning after surgical excisions ...odoherty+++++.pdf · reward-related...
TRANSCRIPT

Reward-related Reversal Learning after SurgicalExcisions in Orbito-frontal or Dorsolateral Prefrontal
Cortex in Humans
J Hornak1 J OrsquoDoherty3 J Bramham2 E T Rolls1 R G Morris2P R Bullock4 and C E Polkey4
Abstract
amp Neurophysiological studies in primates and neuroimagingstudies in humans suggest that the orbito-frontal cortex isinvolved in representing the reward value of stimuli and in therapid learning and relearning of associations between visualstimuli and rewarding or punishing outcomes In the presentstudy we tested patients with circumscribed surgical lesions indifferent regions of the frontal lobe on a new visualdiscrimination reversal test which in an fMRI study (OrsquoDoh-erty Kringelbach Rolls Hornak amp Andrews 2001) producedbilateral orbito-frontal cortex activation in normal subjects Inthis task touching one of two simultaneously presentedpatterns produced reward or loss of imaginary moneydelivered on a probabilistic basis to minimize the usefulnessof verbal strategies A number of types of feedback werepresent on the screen The main result was that the group ofpatients with bilateral orbito-frontal cortex lesions wereseverely impaired at the reversal task in that they accumulatedless money These patients often failed to switch their choiceof stimulus after a large loss and often did switch their choicealthough they had just received a reward The investigationshowed that bilateral lesions were required for this deficitsince patients with unilateral orbito-frontal cortex (or medialprefrontal cortex) lesions were not impaired in the proba-bilistic reversal task The task ruled out a simple motordisinhibition as an explanation of the deficit in the bilateralorbito-frontal cortex patients in that the patients wererequired to choose one of two stimuli on each trial A
comparison group of patients with dorsolateral prefrontalcortex lesions was in some cases able to do the task and inother cases was impaired Posttest debriefing showed that allthe dorsolateral prefrontal patients who were impaired at thetask had failed to pay attention to the crucial feedbackprovided on the screen after each trial about the amount wonor lost on each trial In contrast all dorsolateral patients whopaid attention to this crucial feedback performed normally onthe reversal task Further it was confirmed that the bilateralorbito-frontal cortex patients had also paid attention to thiscrucial feedback but in contrast had still performed poorly atthe task The results thus show that the orbital prefrontalcortex is required bilaterally for monitoring changes in thereward value of stimuli and using this to guide behavior in thetask whereas the dorsolateral prefrontal cortex if it producesdeficits in the task does so for reasons related to executivefunctions such as the control of attention Thus the ability todetermine which information is relevant when making a choiceof pattern can be disrupted by a dorsolateral lesion on eitherside whereas the ability to use this information to guidebehavior is not disrupted by a unilateral lesion in either the leftor the right orbito-frontal cortex but is severely impaired by abilateral lesion in this region Because both abilities areimportant in many of the tasks and decisions that arise inthe course of daily life the present results are relevant tounderstanding the difficulties faced by patients after surgicalexcisions in different frontal brain regions amp
INTRODUCTION
There is growing evidence from functional neuroimagingfrom the investigation of brain damaged patients andfrom neurophysiological and lesion studies in nonhumanprimates that the ventral parts of the frontal lobe whichinclude the orbito-frontal cortex play a crucial role inrepresenting the reward and punishment value of stimuliand in rapidly learning or reversing associations between
visual stimuli and rewards or punishments (Rolls 1999a1999b2000 2002) In so far as emotions can be defined asstates elicited by rewards and punishments (Rolls 19901999a 1999b) these findings may be relevant to under-standing the emotional changes and behavioral problemsthat can follow damage to this region in humans (HornakRolls amp Wade 1996 Rolls Hornak Wade amp McGrath1994 Rolls 1999a)
The importance of the orbito-frontal cortex in process-ing the reward value of stimuli and in reward-relatedlearning is demonstrated by the finding that singleneurons in the primate orbito-frontal cortex respond tothe relative reward value of primary reinforcers such as
1University of Oxford 2Institute of Psychiatry De CrespignyPark 3Institute of Neurology Queenrsquos Square 4Kingrsquos Neu-roscience Centre
copy 2004 Massachusetts Institute of Technology Journal of Cognitive Neuroscience 163 pp 463ndash478
taste (Rolls Sienkiewicz amp Yaxley 1989) Other orbito-frontal cortex neurons are involved in one-trial relearningof associations between visual stimuli and a taste rein-forcer in the reversal of a visual discrimination task (RollsCritchley Mason amp Wakeman 1996 Thorpe Rolls ampMaddison 1983) A visual discrimination task and itsreversal allows the learning and reversal of stimulusndashreinforcement associations to be investigated (Rolls1990 1999a 1999b 2000 2002) Correspondingly inhuman neuroimaging studies it has been shown thatthe orbito-frontal cortex is activated by rewarding andpunishing stimuli in many different modalities such astaste (OrsquoDoherty Rolls Francis McGlone amp Bowtell2001 Small et al 1999 Zald Lee Fluegel amp Pardo1998) odor (Rolls Kringelbach et al 2003 GottfriedDeichmann Winston amp Dolan 2002 OrsquoDoherty et al2000 Zald amp Pardo 1997) touch (Rolls OrsquoDoherty et al2003 Francis et al 1999) auditory (Frey Kostopoulos ampPetrides 2000 Blood Zatorre Bermudez amp Evans1999) and visual stimuli (OrsquoDoherty et al 2003 Aharonet al 2001) Furthermore neuroimaging has revealedactivation of the orbito-frontal cortex to even abstractrewards and punishments such as monetary gains andlosses (Breiter Aharon Kahneman Dale amp Shizgal2001 Knutson Fong Adams Varner amp Hommer 2001OrsquoDoherty Kringelbach Rolls Hornak amp Andrews2001b) and verbal feedback (Elliot Frith amp Dolan1997 Elliot Dolan amp Frith 2000)
Consistent with these findings lesion studies in bothnonhuman primates and in human patients furtherindicate the importance of the orbito-frontal cortexin mediating behavioral choice following rewardingor punishing feedback In visual discrimination tasksorbito-frontal cortex lesions in nonhuman primates pro-duce impairments at extinguishing or switching re-sponses from a previously rewarded stimulus when thecontingencies are altered (Meunier Bachevalier amp Mis-hkin 1997 Iversen amp Mishkin 1970 Butter 1969) Morerecently Dias Robbins and Roberts (1996) described adissociation between the effects of lesions in the orbito-frontal cortex which impaired the ability of monkeys toalter behavior in response to fluctuations in the affectivesignificance of stimuli (in lsquolsquointradimensional shiftrsquorsquo con-ditions) and of lesions in the lateral prefrontal cortex(BA 9) which caused a loss of control of attentionalselection (in lsquolsquoextradimensional shiftrsquorsquo conditions)
Human patients with damage that includes the orbito-frontal cortex have also been shown to have deficits intasks that involve using rewarding and punishing feed-back to guide behavior Bechara Damasio Damasio andAnderson (1994) reported impairments in lsquolsquoaffectiversquorsquodecision-making in a gambling task in patients withbilateral ventromedial prefrontal cortex damage (incor-porating orbito-frontal medial prefrontal and rostralanterior cingulate regions) Damage to these regionsimpaired the ability to learn to choose advantageouslyfrom a set of stimuli that yielded differing overall levels of
reward In an earlier study of visual discrimination rever-sal learning Rolls et al (1994) showed that patients withsimilar ventromedial lesions were impaired at learning tochoose advantageously in a visual discrimination reversaltask in that they repeatedly chose the previously re-warded visual pattern after the contingencies had re-versed a result consistent with a role for the humanorbito-frontal cortex in stimulusndashreward learning andspecifically in altering behavior in the face of changingreward contingencies The ventromedial prefrontal le-sions in the patients in our earlier study were producedeither by closed head injury or by severe strokes so thatthe lesions were not restricted just to the ventromedialprefrontal cortex and in some cases there was diffusedamage outside the frontal lobe A major aim of thepresent study was therefore to determine whether im-pairments at reversal learning can be produced specifi-cally by lesions of the orbito-frontal cortex An additionalaim was to determine whether unilateral damage to theorbito-frontal cortex can produce this learning impair-ment or whether it is produced by bilateral damage Wetherefore tested patients with lesions that were circum-scribed to different regions of the prefrontal cortexbecause the lesions were produced surgically
We used a new probabilistic reversal task developedspecifically to minimize the opportunity to use a verbalstrategy and to ensure that any impairment on the taskcould not be attributed to simple motor disinhibition Inthis new task two simple patterns appeared together ona touch-screen on each trial and selection of eachpattern could give and take away varying amounts ofimaginary money Choice of the lsquolsquogoodrsquorsquo pattern proba-bilistically gave more than it took overall whereas theopposite was true of the other lsquolsquobadrsquorsquo pattern Thepatientrsquos goal was to determine by trial and error whichpattern was more profitable to touch There was awarning that a reversal would occur and that this wouldhappen gradually The task was to keep track of which-ever pattern was currently the lsquolsquogoodrsquorsquo pattern and tokeep touching it until the participant thought it hadchanged and was now the lsquolsquobadrsquorsquo pattern Since the taskitself was difficult enough to avoid ceiling effects in thenormal group it was possible to give explicit instructionsexplaining that reversals would occur
In our previous study of reversal (Rolls et al 1994)only one stimulus (S+ or Siexcl) appeared at a time andthe patients had either to make or withhold a responseon each trial The perseverative touching of the old S+may therefore have had a motor component an inter-pretation that would fit with the view of some authorsthat the orbito-frontal cortex is involved in lsquolsquoinhibitorycontrolrsquorsquomdasha function that could be especially importantfor inhibiting inappropriate responses during tasks suchas the reversal of visual discrimination learning (Robertsamp Wallis 2000 Dias et al 1996) Because both stimuliappeared on each trial in the new probabilistic reversaltest and because a response was therefore required on
464 Journal of Cognitive Neuroscience Volume 16 Number 3
every trial continued selection of the previously correctstimulus could therefore no longer be open to thismotor disinhibition interpretation
A further rationale for using this new probabilisticreversal test in patients with orbito-frontal cortex dam-age was that the very same task (save for a number ofminor modifications) was used in an fMRI study of visualdiscrimination reversal learning in healthy normal sub-jects (OrsquoDoherty Kringelbach et al 2001) It was shownthat bilateral activation of the medial orbito-frontalcortex was correlated with the amount on money wonon individual trials and that bilateral activation of thelateral orbito-frontal cortex was correlated with howmuch money was lost on individual trials The presentstudy addresses whether these regions of the orbito-frontal cortex where activations were found are neces-sary for good performance in the visual discriminationreversal task
In this study we also included groups of patients withunilateral lesions in other regions of the prefrontalcortex in particular to the dorsolateral andor the medialprefrontal cortex Contrary to the functions ascribed tothe orbito-frontal cortex in reward and reward-relatedlearning the dorsolateral prefrontal cortex has beenimplicated in different functions These can be placedunder the general umbrella term of lsquolsquoexecutive func-tionsrsquorsquo and include planning (Owen 1997) workingmemory (Goldman-Rakic 1996) higher order responseselection (Wise Murray amp Gerfen 1996) inhibitorycontrol of attentional selection (Robbins 1998 Diaset al 1996) and extradimensional shift learning (RogersAndrews Grasby Brooks amp Robbins 2000) One hypoth-esis that arises from the putatively different roles ascribedto these different portions of the prefrontal cortex is thatpatients with dorsolateral prefrontal cortex lesions maybe less impaired or produce a different pattern of impair-
ments on a task designed to assess reward-related learn-ing and therefore presumed to rely more on orbito-frontal cortex function Consistent with this a partialdissociation between the effects of ventromedial anddorsolateral prefrontal cortex was reported by BecharaDamasio Tranel and Anderson (1998) in relation toaffective decision making and working memory respec-tively Consequently a further aim of the present studywas to determine whether we could dissociate effects oflesions of the orbito-frontal cortex and dorsolateral pre-frontal cortex on the reversal learning task
RESULTS
All patients succeeded in reaching criterion in thepractice session (which did not include a reversal)demonstrating that they had understood the require-ments of the task and appreciated the probabilisticnature of the reward schedule There were no significantdifferences between the patient groups in the number oftrials taken to achieve criterion in the practice sessionusing a nonparametric analysis of variance (KruskalndashWallis) (The mean number of trials to attain criterionacross all groups was 282) All groups also performedcomparably on the reversal test until the contingenciesreversed for the first time gaining approximately pound800ndash1000 over the first 10ndash13 trials Thereafter as shown inFigure 1 all of the patient groups performed like thenormal control group with the exception of the bilateralorbito-frontal cortex group and a subset of the unilateraldorsolateral prefrontal cortex patients who it wasfound had failed to attend to the essential feedback(see below) Whereas patients in these two groups lostmore and more lsquolsquomoneyrsquorsquo as the test proceeded theother groups continued to gain Statistical analyses arepresented subsequently
Figure 1 Cumulative totalamount of lsquolsquomoneyrsquorsquo won by thenormal group and by each ofthe patient groups by Trial 100BL OFC = bilateral orbito-frontal cortex UL OFC =unilateral orbito-frontal cortexMedial PFC = medial prefrontalcortex DLPFC = dorsolateralprefrontal cortex Attendedfailed to attend = the patientattended failed to attend to thecrucial feedback during thereversal test namely theamount won or lost oneach trial
Hornak et al 465
Posttest Questionnaire
Feedback Found Most Useful
Although all patients were able to use the essentialfeedback concerning the amount won or lost on eachtrial during the brief easy prereversal phase of the testthe results of the posttest questionnaire revealed animportant difference between groups in the ability toappreciate which was the essential feedback when thetest became more challenging (ie during the reversalphase of the test) Thus 8 of the 17 patients whose lesionsincluded the dorsolateral prefrontal region unilaterallywhen asked the open-ended question lsquolsquoWhat informationon the screen did you find most useful in keeping track ofwhich pattern was currently the good onersquorsquo explainedhow they had relied on various nonessential sources offeedback and when asked about the feedback showingthe amount won or lost on each trial denied that they hadfound this feedback to be the most useful (see Table 1)By contrast all of the 14 patients whose lesion (bilateralor unilateral) did not encroach on the dorsolateral pre-frontal region reported that this was the obvious feed-back to use and that they had used it to guide their choiceof stimulus This was also true for all normal controlsubjects Statistical comparison between patients withand without a dorsolateral lesion revealed a very signifi-cant difference between the numbers in each group whodid and who did not attend to the essential feedback(Fisherrsquos exact test p = 006 two-tailed)
Other Feedback Used
Patients with dorsolateral prefrontal damage who failedto attend to the amount wonlost on each trial reportedinstead that they had used a variety of subsidiary non-essential types of feedback which by themselves wouldnot allow the subject to perform the reversal tasksuccessfully (see Appendices 2A and 2B)
Total Scored by Trial 100
Group Results
We tested for a difference between the groups in thetotal money gained by trial 100 Statistical analysisrevealed a highly significant difference (KruskalndashWallisx2(4) = 2339 p lt 001) Paired comparisons betweenthe separate groups and the normal control groupas shown in Table 2 revealed a significant impairmentonly in the bilateral orbito-frontal cortex group (MannndashWhitney test p = 002 two-tailed) and the dorsolateral(failed to attend) group ( p lt 001 two-tailed) Table 2also shows the results for the other paired comparisonsbetween the groups This reveals that the bilateralorbito-frontal cortex group was significantly impairedrelative to the unilateral orbito-frontal cortex group( p = 028 two-tailed) and that there was no significantdifference between the bilateral orbito-frontal cortex
group and the unilateral dorsolateral (failed to attend)group (We note that the two critical comparisonsshown in Table 2 between the bilateral orbito-frontalcortex group and normal controls and between thelsquolsquodorsolateral prefrontal cortex failed to attendrsquorsquo groupand normal controls are still significant after Bonferronicorrection for multiple comparisons)
Individual Results
The number of standard deviations (SD) was calculatedby which each patientrsquos total (gained by trial 100) differedfrom the mean amount won by the Control group by trial100 Figure 2 and Table 1 show each patientrsquos SD inrelation to whether they attended or failed to attend tothe essential feedback Most patients with dorsolateralprefrontal lesions who were able to determine whichfeedback cue they should use and who kept using thisfeedback throughout the test performed normally (theexceptions being DB and RD) By contrast all but oneof those who failed to attend to this feedback (namelyRC) were severely impaired The other unilateralgroups those with medial and those with orbital lesions(both of whom attended to the appropriate cues) wereboth unimpaired It is important to note that the bilateralorbito-frontal cortex group was impaired although all ofthe patients had attended to the appropriate feedbackThere was no correlation between the total money wonby trial 100 and IQ (full-scale IQ as measured by theNational Adult Reading Test NART ) (Spearmanrsquos rho =277 p = 88) There was also no difference between theIQ of those with dorsolateral lesions who attended to theessential feedback and those who failed to do so (MannndashWhitney U = 165 p = 06)
Appendix 2A shows the responses to questions aboutthe other nonessential types of feedback Patients whosaid that they had used the amount wonlost on eachtrial were clear about this and generally indicated thatthey felt that this was the obvious information to useThese patients also noticedpaid attention to otherfeedback types but they were less clear about whetherthey had used this information to guide their choice ofpattern Among those with dorsolateral lesions classifiedas not having attended to the amount wonlost on eachtrial some had done so in an inconsistent andorintermittent way Most of those who failed to use theamount wonlost on each trial reported that they hadrelied upon the numerical total instead The other threetypes of feedback were noticed by most patients butthey were not always clear about whether they had beenaware of their existence or whether they had beenhelpful in making a choice
Lesion Size
There was no correlation between performance onthe reversal test (as measured by the total earned
466 Journal of Cognitive Neuroscience Volume 16 Number 3
by trial 100) and the size of the lesion measured asthe total area of prefrontal cortex excised (Spearmanrsquosrho = iexcl21 p = 26)
Other Factors Etiology and Use of Medication
No systematic patterns emerged between type of etiologyand performance on the task Only two patients hadsuffered from closed head injury VO with a bilateralorbito-frontal cortex lesion and SI with a unilateralorbitalmedial lesion and neither of these patientswas impaired It was found that 4 of the 9 patientson medication were impaired (444) compared with10 of those 23 not on medication (435) indicating thatmedication did not account for the results
Location of Lesion in the Bilateral Patients WhoWere Impaired
The lesions in the four bilateral patients who wereimpaired on the reversal test (RF VZ VU and JA)all encompassed the regions activated in normal subjectsin the parallel fMRI study using the same task (OrsquoDoh-erty Kringelbach et al 2001) and they spared regionsmore posterior and lateral to the regions of activationConversely the two unimpaired patients with bilaterallesions (VO and RR) both had lesions that wereanterior and posterior respectively to the region acti-vated in the fMRI study
Other Measures Staying with a Pattern After aReward and Switching After a Loss
As a measure of sensitivity to reward the number ofoccasions on which patients chose again a pattern fromwhich they had just gained pound80 or more was counted Asa measure of sensitivity to punishment the number ofoccasions on which patients failed to switch after lossesof pound250 or more was also counted Across all patientsboth measures were very significantly correlated withthe total money won by trial 100 (for reward sensitivitySpearmanrsquos rho = iexcl59 p = 0018 for punishmentsensitivity Spearmanrsquos rho = iexcl70 p = 0002) Furtheranalysis showed that among those patients with bilaterallesions who were impaired on the reversal AS and VWhad scores significantly higher than the mean of thecontrol group on both measures and GS only on the
Table 1 Use of Essential Feedback in Relation to Total Earnedon the Reversal Test
Reversal Performance(Number of SDs) Attended
Failedto Attend
Without dorsolateral lesion
Bilateral orbitalmedial
RFa iexcl24 +
VZa iexcl49 +
VUa iexcl55 +
JAa iexcl21 +
RR 02 +
VO iexcl13 +
Unilateral orbitalmedial
RQ 10 +
LJ iexcl09 +
CL iexcl04 +
TR 07 +
SI (L) iexcl03 +
Unilateral medial
OF (L) 11 +
FG (L) iexcl27 +
EE 02 +
With dorsolateral lesion
UC iexcl01 +
BR iexcl01 +
QG iexcl02 +
VF (L) 06 +
AR (L) iexcl03 +
DB (L) iexcl38 +
LS (L) iexcl15 +
RD (L) iexcl17 +
QO (L) iexcl05 +
RC iexcl12 +
FZ iexcl20 +
BS iexcl46 +
GE (Gave up) +
AG (L) iexcl41 +
LK (L) iexcl60 +
The number of standard deviations by which the patientsrsquo total scoresdiffered from the mean from the control group is shown in relation towhether they attended or failed to attend to the amount won or lost oneach trial and in relation to the presence of a dorsolateral lesionaThese patients had bilateral lesions that lay within the region activatedin the fMRI study in which normal control subjects performed the samereversal task SS and VO had lesions outside this region
Performed at or below fifth centile
Performed at or below first centile
Hornak et al 467
sensitivity to reward measure BK did not have signif-icantly higher scores on either measure but she mademore responses revealing insensitivity to punishmentthan responses revealing insensitivity to reward
DISCUSSION
Patients with lesions in different regions of the prefron-tal cortex were tested on a probabilistic visual discrim-ination reversal test in which it was necessary both todetermine which feedback was crucial and to use thisinformation appropriately to guide the choice of stimu-lus to maximize the reward obtained It was found that
bilateral orbitalmedial prefrontal lesions produced asevere impairment on this test whereas even largeunilateral lesions which included the orbitalmedialregion had no such effect It was also found thatpatients with unilateral medial prefrontal cortex lesionswere unimpaired at this task
The pattern of results was more complicated in thedorsolateral group all of whom had unilateral lesions inthat some patients were impaired at the task whereasothers were not This was shown to be related to whetheras indicated by the posttest questionnaire the patientshad attended to the feedback necessary to succeed on thetask namely the amount won or lost on each trial Nearlyhalf of those with dorsolateral lesions explained how theyhad attended to other nonessential sources of feedbackattempting to maximize their gains in this way Those whodid attend to the essential feedback performed normallywhereas those who did not were as impaired as the groupwith bilateral orbital lesions
The pattern of impairment shown by the dorsolateralpatients who failed to attend can be contrasted withthat shown by the patients with bilateral orbitalmediallesions Although all of these patients with bilateralorbitalmedial prefrontal lesions did attend to the rele-vant feedback they were nevertheless unable to use it toadjust their behavior Instead when stimulusndashrewardcontingencies were reversed they frequently choseagain the incorrect previously rewarded stimulus afterlarge losses or failed to stick with the correct stimulusafter gaining money on it The impairment shown bypatients with bilateral orbitalmedial lesions is consistentwith the findings from our earlier study (Rolls et al1994) in which patients with bilateral ventral prefrontalcortex lesions were found to be impaired on a gono-go
Table 2 Comparisons of the Amount of Money Earned on theReversal Test
BLOFC
ULOFC
DLPFC(Att)
DLPFC(F)
BL OFC
UL OFC p = 028
DLPFC (Att) p = 045 ns
DLPFC (F) ns p = 004 p = 011
Control group p = 002 ns ns p lt 001
Group Comparisons Using MannndashWhitney Nonparametric TestsKruskalndashWallis nonparametric one-way ANOVA revealed significantgroup difference x2 = 23391 df = 4 p lt 001 BL = bilateral UL =unilateral OFC = orbito-frontal cortex DLPFC = dorsolateralprefrontal cortex Att = the patients attended to the crucial feedbackF = the patients failed to attend to the crucial feedback
Significant at p lt 05
Significant at p lt 01
Figure 2 The number ofstandard deviations by whicheach patientrsquos total earned onthe reversal test by trial 100differed from the mean won bythe normal control group BLOFC = bilateral orbito-frontalcortex UL OFC = unilateralorbito-frontal cortex MedialPFC = medial prefrontal cortexDLPFC = dorsolateral prefrontalcortex Attendedfailed toattend = the patient attendedfailed to attend to the crucialfeedback during the reversaltest namely the amount won orlost on each trial
468 Journal of Cognitive Neuroscience Volume 16 Number 3
visual discrimination reversal test However in thisprevious study the more diffuse nature of the lesions(with some produced by closed head injury althoughnevertheless with clear damage to the ventral prefrontalcortex evident in structural MRI scans) precluded pre-cise localization of this impairment to the orbito-frontalcortex In the present study by investigating patientswith surgical and thus more circumscribed lesions of thefrontal lobes we were able to demonstrate that animpairment on reversal learning can occur followingbilateral orbital excisions These results are consistentwith findings from nonhuman primates which implicatethe orbito-frontal cortex in reward and in stimulusndashreward learning and reversal (Dias et al 1996 Rolls1990 1999b 2000) as well as with the results from ourneuroimaging study using the same probabilistic reversaltask (OrsquoDoherty Kringelbach et al 2001) which pro-duced bilateral activation in the orbito-frontal cortex innormal subjects In the present study although as agroup the patients with bilateral orbital lesions weresignificantly impaired on this test only those whoselesions included the areas activated in the fMRI studyshowed a marked impairment whereas the two patientswith bilateral lesions who were not significantly impaired(VO and RR) had small lesions restricted either to theregion anterior or to the region posterior to the regionsof activation (see Figure 3A)
In the fMRI study it was found that the medial and thelateral regions of the orbito-frontal cortex were activat-ed respectively by reward and by punishment andindeed that the degree of activation in these two regionswas correlated with the amount of lsquolsquomoneyrsquorsquo gained orlost (OrsquoDoherty Kringelbach et al 2001) In the pres-ent study the patients with bilateral orbital lesions whowere impaired on the test all had lesions that encom-passed both the more medial and the more lateralregions described in the activation study and for thatreason a difference in sensitivity to reward and topunishment would not be expected in this patientgroup Consistent with this no clear pattern of greatersensitivity to punishment or to reward was observed inthose with bilateral lesions who were impaired Furtherresearch with more discrete lesions within the orbito-frontal cortex may reveal more detailed parallels withthe fMRI study perhaps with sensitivity to reward beingimpaired by medial orbito-frontal cortex lesions andsensitivity to punishment by lateral orbito-frontal cortexlesions However since a recent fMRI study found thatventrolateral activation was associated with reversallearning independently of the effects of negative feed-back (Cools Clark Owen amp Robbins 2002) the medialndashlateral distinction (within the orbital cortex) for rewardand for punishment respectively seems less likely tohold up for this kind of test
It is important that in the present study the groupwith unilateral orbital lesions on either side was unim-paired indicating that it is necessary for the orbital
damage to extend bilaterally before impairments areshown on visual discrimination reversal learning Thissuggests that either the left or the right orbito-frontalcortex on its own can carry out the functions necessaryfor normal performance It is very unlikely that lesionsize per se can explain this effect because somepatients with unilateral orbital lesions who were unim-paired had a larger total area of prefrontal cortexexcised than some of the patients with bilateral orbitallesions who were impaired This was confirmed by thefact that there was no correlation between the totallesion size (amount of prefrontal cortex excised) andperformance on the task
The design of the probabilistic reversal task meansthat two interpretations of the impairment shown bypatients with bilateral orbitalmedial lesions can beexcluded First the repeated touching of the previouslyrewarded stimulus cannot be explained in terms ofsimple motor perseveration (ie as a failure of inhibitorycontrol of the armhand with which the patients reachedout to touch the now-incorrect stimulus) Because aresponse was required and made on every trial thecontinued selection of the old S+ must reflect insteadthe patientrsquos difficulty when reinforcement contingen-cies are reversed in altering the previous associationformed between the stimulus and reward or that be-tween the stimulus and the response he should make toit Although the present study does not distinguishbetween these two interpretations the results are con-sistent with the hypothesis (Rolls 1990 1999b 20002002) that one important function of the orbito-frontalcortex consists in representing the reward and punish-ment value of stimuli and in particular since all patientssucceeded in the early stages of the task (before the firstreversal) in updating the associations between stimuliand reward or punishment value when these change
Secondly the clear instructions that explained thatreversals would occur and that subjects were to alter theirchoice of stimulus accordingly exclude an interpretationin terms of lack of initiative This might have explainedsome of the problems shown by patients in our earlierstudy (Rolls et al 1994) in which no warning was giventhat the contingencies would change The fact that clearexplanation was given about this in the present study atleast excludes an explanation in these terms Howeverwe cannot exclude the possibility that some of thepatients with dorsolateral lesions who were impaired atthe test and who failed to attend to the essential feedbackhad failed fully to understand the task requirements andif so this itself may be viewed as an aspect of executivedysfunction Interestingly among those who failed toattend to the amount won or lost on each trial somedid attend to this for some of the time but did notappreciate its importance and started to attend to othersources of feedback instead (Appendix 2B)
The difficulty in selecting the appropriate feedback orusing it in a consistent manner which was shown by
Hornak et al 469
almost half of the patients in the dorsolateral group andwhich resulted in severely impaired performance on thereversal test has parallels in work with nonhumanprimates in which dorsolateral lesions impaired theability to lsquolsquomonitor multiple stimulirsquorsquo (Petrides amp Pandya1999) as well as with neuroimaging studies of executivefunctions such as those involved in dual-task perfor-mance (Szameitat Torsten Muller amp von Cramon2002) On the posttest questionnaire the patients inthis study reported that instead of using the amountwon or lost on each trial to guide their choice of patternthey had attended instead to other nonessential sourcesof information such as the cumulative total (as anumber or as a bar chart) whether they had won orlost on each trial (ignoring the amount) or the colors orsounds that were associated with gains or losses (Wenote that the self-report provided by these patients withcircumscribed frontal lesions was sufficiently reliablethat across the group the self-report about attention tothe essential feedback was strongly related to the level ofperformance on the task Indeed there was a significant
difference between the proportions of patients whowere impaired who attended 29 and who failed toattend 78 Fisherrsquos exact test p = 02 two-tailed) It isof interest that the dorsolateral group who failed toattend or who failed to attend consistently to theessential feedback during the main reversal phase ofthe test were able to appreciate which feedback to use inthe far easier practice session of the test in which noreversals occurred A similar effect of task difficulty inrevealing impairments in patients with dorsolateral le-sions has been reported by Morris et al (2002) whofound that the ability to employ the appropriate strategyin a test of planning ability was not apparent in the earlypart of the test but became apparent only in the laterharder phase Similarly in Szameitat et alrsquos (2002) studydorsolateral prefrontal cortex activation was producedonly when the task difficulty was increased
In the present study three of the four (R C F Zand B S) whose lesions were confined to the dorso-lateral prefrontal region all failed to attend to the amountwonlost on each trial suggesting that a dorsolateral
Figure 3 Brain maps showinglesion sites Within each groupwith unilateral lesions thosewith right-sided lesions areshown first (A) Bilateral orbito-frontal cortex (or orbital plusmedial prefrontal cortex) (B)Unilateral orbito-frontal (ororbital plus medial) (C) Uni-lateral medial prefrontal cortex(D) Unilateral dorsolateralprefrontal (or dorsolateral plusmedial prefrontal) (E)Unilateral orbito-frontal plusmedial prefrontal plusdorsolateral prefrontal cortex
470 Journal of Cognitive Neuroscience Volume 16 Number 3
lesion may be sufficient to produce this cognitiveexecu-tive impairment In those cases where the dorsolaterallesions extended down into the medial region there arealso parallels with imaging studies in which the moredorsal regions of anterior cingulate described by theauthors as its cognitive division are activated in normalsubjects during tasks involving stimulusndashresponse selec-tion in the face of competing streams of information(Bush Luu amp Posner 2000) The dorsolateral prefrontalcortex lesions did in fact extend into this lsquolsquocognitivedivisionrsquorsquo region of the anterior cingulate cortex in theother five patients with dorsolateral lesions (GE GDOR AG and LK) who also failed to attend to theappropriate feedback However since other patients withcomparable lesions extending into these regions suc-ceeded in attending to this feedback this suggestionmust remain tentative It will be of interest to developour reversal task in the future to simplify the feedbackprovided in the expectation that this will make the taskperformable without deficit by patients with dorsolateralprefrontal cortex lesions but still sensitive to the effectsof lesions to the orbito-frontal cortex due to the reversalcomponent of the task
The findings reported in this study suggest that theprobabilistic reversal test makes demands on differentfunctions attributed respectively to the dorsolateraland to the orbital regions of the prefrontal cortex (cfBechara et al 1998 who reported a study in whichlesions in these regions had dissociable effects ondecision making and on working memory) Thus inthe present study the need to determine which ofmultiple competing sources of feedback should beattended to to maintain attention to this throughoutthe test ignoring other visually salient but noncrucialtypes of feedback (flashing lights total sum displayedcolored bar charts etc) are among the many functionsthat have been attributed to the dorsolateral prefrontalcortex (Szameitat et al 2002 Duncan amp Owen 2000)For a subject who is capable of attending consistently tothe appropriate feedback it is also necessary to use theinformation about the current level of reward associatedwith each pattern to guide his choice on each trial andas such the test also makes demands on functionsattributed to the orbito-frontal cortex (Rolls 19901999a 1999b 2000) The results of the present studyshow that it is possible to be severely impaired on thisprobabilistic visual discrimination reversal test for eitherof these two reasons and in the context that perfor-mance on the test can be independently disrupted bythe effects of dorsolateral and of orbital lesions we haveshown a dissociation between the effects of lesions inthese two regions The ability to attend to the crucialfeedback can be disrupted by a dorsolateral lesion oneither side whereas the ability to use this information tochoose advantageously can be supported by eitherorbital region on its own (after a unilateral orbitallesion) but is abolished by a bilateral orbital lesion
These results are consistent with the view that whereasthe dorsolateral frontal cortex forms part of a network ofprefrontal regions recruited to solve diverse cognitiveproblems especially those with an lsquolsquoexecutiversquorsquo compo-nent (in this case appreciating which feedback is rele-vantimportant) (Bush et al 2000 Duncan amp Owen2000) the orbito-frontal cortex is involved in the repre-sentation of the changing reward value of stimuli (Rolls1990 1999b 2000 2002) so that behavior can be mod-ified accordingly As such the present study contributesboth to our understanding of the different functions ofthese two regions of frontal lobe and to how theseregions need to cooperate on complex tasks such as theone used here A similar argument is made by Manes et al(2002) who showed how the ventral and dorsal aspects ofthe prefrontal cortex must interact in the maintenance ofrational and lsquolsquononriskyrsquorsquo decision-making tasks
One of the underlying hypotheses of the researchdescribed here is that some of the reasons for thebehavioral and emotional changes that follow damageto the prefrontal cortex may be related to deficits indecoding the reward and punishment value of stimuliand using the results of the decoding to modify behaviorand the ongoing emotional or mood state (Rolls 19901999a 1999b Rolls et al 1994) In this context it is ofinterest that the patients with bilateral orbito-frontalcortex damage who were impaired at the visual discrim-ination reversal task (see Table 1) had high scores onparts of a social behavior questionnaire in which thepatients were rated on behaviors such as the recognitionof emotion in others (eg their sad angry or disgustedmood) in interpersonal relationships (such as not caringwhat others think and not being close to the family) insociability (is not sociable and has difficulty making ormaintaining close relationships) emotional empathy(eg when others are happy is not happy for them)public behavior (is uncooperative) antisocial behavior (iscritical of and impatient with others) and impulsivity(does things without thinking) (Hornak Bramham RollsMorris OrsquoDoherty amp Polkey 2003) all of which couldreflect less behavioral sensitivity to different types ofpunishment and reward Further in a subjective emo-tional change questionnaire in which the patients re-ported on any changes in the intensity andor frequencyof their own experience of emotions since surgery thebilateral orbito-frontal cortex patients with deficits in thevisual discrimination reversal task reported a number ofchanges including changes in sadness anger fear andhappiness and were as a group significantly different inthese respects from the dorsolateral prefrontal cortexlesion group included in that comparison (Hornak et al2003) However it must also be pointed out that thepatients with unilateral orbito-frontalanterior cingulatelesions (the BA 9ACC and BA 9ACC + orbital groups ofthat article) also reported marked emotional changes andthey were also less well-adjusted socially than the dorso-lateral group but had no measured deficit in reversal The
Hornak et al 471
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3

taste (Rolls Sienkiewicz amp Yaxley 1989) Other orbito-frontal cortex neurons are involved in one-trial relearningof associations between visual stimuli and a taste rein-forcer in the reversal of a visual discrimination task (RollsCritchley Mason amp Wakeman 1996 Thorpe Rolls ampMaddison 1983) A visual discrimination task and itsreversal allows the learning and reversal of stimulusndashreinforcement associations to be investigated (Rolls1990 1999a 1999b 2000 2002) Correspondingly inhuman neuroimaging studies it has been shown thatthe orbito-frontal cortex is activated by rewarding andpunishing stimuli in many different modalities such astaste (OrsquoDoherty Rolls Francis McGlone amp Bowtell2001 Small et al 1999 Zald Lee Fluegel amp Pardo1998) odor (Rolls Kringelbach et al 2003 GottfriedDeichmann Winston amp Dolan 2002 OrsquoDoherty et al2000 Zald amp Pardo 1997) touch (Rolls OrsquoDoherty et al2003 Francis et al 1999) auditory (Frey Kostopoulos ampPetrides 2000 Blood Zatorre Bermudez amp Evans1999) and visual stimuli (OrsquoDoherty et al 2003 Aharonet al 2001) Furthermore neuroimaging has revealedactivation of the orbito-frontal cortex to even abstractrewards and punishments such as monetary gains andlosses (Breiter Aharon Kahneman Dale amp Shizgal2001 Knutson Fong Adams Varner amp Hommer 2001OrsquoDoherty Kringelbach Rolls Hornak amp Andrews2001b) and verbal feedback (Elliot Frith amp Dolan1997 Elliot Dolan amp Frith 2000)
Consistent with these findings lesion studies in bothnonhuman primates and in human patients furtherindicate the importance of the orbito-frontal cortexin mediating behavioral choice following rewardingor punishing feedback In visual discrimination tasksorbito-frontal cortex lesions in nonhuman primates pro-duce impairments at extinguishing or switching re-sponses from a previously rewarded stimulus when thecontingencies are altered (Meunier Bachevalier amp Mis-hkin 1997 Iversen amp Mishkin 1970 Butter 1969) Morerecently Dias Robbins and Roberts (1996) described adissociation between the effects of lesions in the orbito-frontal cortex which impaired the ability of monkeys toalter behavior in response to fluctuations in the affectivesignificance of stimuli (in lsquolsquointradimensional shiftrsquorsquo con-ditions) and of lesions in the lateral prefrontal cortex(BA 9) which caused a loss of control of attentionalselection (in lsquolsquoextradimensional shiftrsquorsquo conditions)
Human patients with damage that includes the orbito-frontal cortex have also been shown to have deficits intasks that involve using rewarding and punishing feed-back to guide behavior Bechara Damasio Damasio andAnderson (1994) reported impairments in lsquolsquoaffectiversquorsquodecision-making in a gambling task in patients withbilateral ventromedial prefrontal cortex damage (incor-porating orbito-frontal medial prefrontal and rostralanterior cingulate regions) Damage to these regionsimpaired the ability to learn to choose advantageouslyfrom a set of stimuli that yielded differing overall levels of
reward In an earlier study of visual discrimination rever-sal learning Rolls et al (1994) showed that patients withsimilar ventromedial lesions were impaired at learning tochoose advantageously in a visual discrimination reversaltask in that they repeatedly chose the previously re-warded visual pattern after the contingencies had re-versed a result consistent with a role for the humanorbito-frontal cortex in stimulusndashreward learning andspecifically in altering behavior in the face of changingreward contingencies The ventromedial prefrontal le-sions in the patients in our earlier study were producedeither by closed head injury or by severe strokes so thatthe lesions were not restricted just to the ventromedialprefrontal cortex and in some cases there was diffusedamage outside the frontal lobe A major aim of thepresent study was therefore to determine whether im-pairments at reversal learning can be produced specifi-cally by lesions of the orbito-frontal cortex An additionalaim was to determine whether unilateral damage to theorbito-frontal cortex can produce this learning impair-ment or whether it is produced by bilateral damage Wetherefore tested patients with lesions that were circum-scribed to different regions of the prefrontal cortexbecause the lesions were produced surgically
We used a new probabilistic reversal task developedspecifically to minimize the opportunity to use a verbalstrategy and to ensure that any impairment on the taskcould not be attributed to simple motor disinhibition Inthis new task two simple patterns appeared together ona touch-screen on each trial and selection of eachpattern could give and take away varying amounts ofimaginary money Choice of the lsquolsquogoodrsquorsquo pattern proba-bilistically gave more than it took overall whereas theopposite was true of the other lsquolsquobadrsquorsquo pattern Thepatientrsquos goal was to determine by trial and error whichpattern was more profitable to touch There was awarning that a reversal would occur and that this wouldhappen gradually The task was to keep track of which-ever pattern was currently the lsquolsquogoodrsquorsquo pattern and tokeep touching it until the participant thought it hadchanged and was now the lsquolsquobadrsquorsquo pattern Since the taskitself was difficult enough to avoid ceiling effects in thenormal group it was possible to give explicit instructionsexplaining that reversals would occur
In our previous study of reversal (Rolls et al 1994)only one stimulus (S+ or Siexcl) appeared at a time andthe patients had either to make or withhold a responseon each trial The perseverative touching of the old S+may therefore have had a motor component an inter-pretation that would fit with the view of some authorsthat the orbito-frontal cortex is involved in lsquolsquoinhibitorycontrolrsquorsquomdasha function that could be especially importantfor inhibiting inappropriate responses during tasks suchas the reversal of visual discrimination learning (Robertsamp Wallis 2000 Dias et al 1996) Because both stimuliappeared on each trial in the new probabilistic reversaltest and because a response was therefore required on
464 Journal of Cognitive Neuroscience Volume 16 Number 3
every trial continued selection of the previously correctstimulus could therefore no longer be open to thismotor disinhibition interpretation
A further rationale for using this new probabilisticreversal test in patients with orbito-frontal cortex dam-age was that the very same task (save for a number ofminor modifications) was used in an fMRI study of visualdiscrimination reversal learning in healthy normal sub-jects (OrsquoDoherty Kringelbach et al 2001) It was shownthat bilateral activation of the medial orbito-frontalcortex was correlated with the amount on money wonon individual trials and that bilateral activation of thelateral orbito-frontal cortex was correlated with howmuch money was lost on individual trials The presentstudy addresses whether these regions of the orbito-frontal cortex where activations were found are neces-sary for good performance in the visual discriminationreversal task
In this study we also included groups of patients withunilateral lesions in other regions of the prefrontalcortex in particular to the dorsolateral andor the medialprefrontal cortex Contrary to the functions ascribed tothe orbito-frontal cortex in reward and reward-relatedlearning the dorsolateral prefrontal cortex has beenimplicated in different functions These can be placedunder the general umbrella term of lsquolsquoexecutive func-tionsrsquorsquo and include planning (Owen 1997) workingmemory (Goldman-Rakic 1996) higher order responseselection (Wise Murray amp Gerfen 1996) inhibitorycontrol of attentional selection (Robbins 1998 Diaset al 1996) and extradimensional shift learning (RogersAndrews Grasby Brooks amp Robbins 2000) One hypoth-esis that arises from the putatively different roles ascribedto these different portions of the prefrontal cortex is thatpatients with dorsolateral prefrontal cortex lesions maybe less impaired or produce a different pattern of impair-
ments on a task designed to assess reward-related learn-ing and therefore presumed to rely more on orbito-frontal cortex function Consistent with this a partialdissociation between the effects of ventromedial anddorsolateral prefrontal cortex was reported by BecharaDamasio Tranel and Anderson (1998) in relation toaffective decision making and working memory respec-tively Consequently a further aim of the present studywas to determine whether we could dissociate effects oflesions of the orbito-frontal cortex and dorsolateral pre-frontal cortex on the reversal learning task
RESULTS
All patients succeeded in reaching criterion in thepractice session (which did not include a reversal)demonstrating that they had understood the require-ments of the task and appreciated the probabilisticnature of the reward schedule There were no significantdifferences between the patient groups in the number oftrials taken to achieve criterion in the practice sessionusing a nonparametric analysis of variance (KruskalndashWallis) (The mean number of trials to attain criterionacross all groups was 282) All groups also performedcomparably on the reversal test until the contingenciesreversed for the first time gaining approximately pound800ndash1000 over the first 10ndash13 trials Thereafter as shown inFigure 1 all of the patient groups performed like thenormal control group with the exception of the bilateralorbito-frontal cortex group and a subset of the unilateraldorsolateral prefrontal cortex patients who it wasfound had failed to attend to the essential feedback(see below) Whereas patients in these two groups lostmore and more lsquolsquomoneyrsquorsquo as the test proceeded theother groups continued to gain Statistical analyses arepresented subsequently
Figure 1 Cumulative totalamount of lsquolsquomoneyrsquorsquo won by thenormal group and by each ofthe patient groups by Trial 100BL OFC = bilateral orbito-frontal cortex UL OFC =unilateral orbito-frontal cortexMedial PFC = medial prefrontalcortex DLPFC = dorsolateralprefrontal cortex Attendedfailed to attend = the patientattended failed to attend to thecrucial feedback during thereversal test namely theamount won or lost oneach trial
Hornak et al 465
Posttest Questionnaire
Feedback Found Most Useful
Although all patients were able to use the essentialfeedback concerning the amount won or lost on eachtrial during the brief easy prereversal phase of the testthe results of the posttest questionnaire revealed animportant difference between groups in the ability toappreciate which was the essential feedback when thetest became more challenging (ie during the reversalphase of the test) Thus 8 of the 17 patients whose lesionsincluded the dorsolateral prefrontal region unilaterallywhen asked the open-ended question lsquolsquoWhat informationon the screen did you find most useful in keeping track ofwhich pattern was currently the good onersquorsquo explainedhow they had relied on various nonessential sources offeedback and when asked about the feedback showingthe amount won or lost on each trial denied that they hadfound this feedback to be the most useful (see Table 1)By contrast all of the 14 patients whose lesion (bilateralor unilateral) did not encroach on the dorsolateral pre-frontal region reported that this was the obvious feed-back to use and that they had used it to guide their choiceof stimulus This was also true for all normal controlsubjects Statistical comparison between patients withand without a dorsolateral lesion revealed a very signifi-cant difference between the numbers in each group whodid and who did not attend to the essential feedback(Fisherrsquos exact test p = 006 two-tailed)
Other Feedback Used
Patients with dorsolateral prefrontal damage who failedto attend to the amount wonlost on each trial reportedinstead that they had used a variety of subsidiary non-essential types of feedback which by themselves wouldnot allow the subject to perform the reversal tasksuccessfully (see Appendices 2A and 2B)
Total Scored by Trial 100
Group Results
We tested for a difference between the groups in thetotal money gained by trial 100 Statistical analysisrevealed a highly significant difference (KruskalndashWallisx2(4) = 2339 p lt 001) Paired comparisons betweenthe separate groups and the normal control groupas shown in Table 2 revealed a significant impairmentonly in the bilateral orbito-frontal cortex group (MannndashWhitney test p = 002 two-tailed) and the dorsolateral(failed to attend) group ( p lt 001 two-tailed) Table 2also shows the results for the other paired comparisonsbetween the groups This reveals that the bilateralorbito-frontal cortex group was significantly impairedrelative to the unilateral orbito-frontal cortex group( p = 028 two-tailed) and that there was no significantdifference between the bilateral orbito-frontal cortex
group and the unilateral dorsolateral (failed to attend)group (We note that the two critical comparisonsshown in Table 2 between the bilateral orbito-frontalcortex group and normal controls and between thelsquolsquodorsolateral prefrontal cortex failed to attendrsquorsquo groupand normal controls are still significant after Bonferronicorrection for multiple comparisons)
Individual Results
The number of standard deviations (SD) was calculatedby which each patientrsquos total (gained by trial 100) differedfrom the mean amount won by the Control group by trial100 Figure 2 and Table 1 show each patientrsquos SD inrelation to whether they attended or failed to attend tothe essential feedback Most patients with dorsolateralprefrontal lesions who were able to determine whichfeedback cue they should use and who kept using thisfeedback throughout the test performed normally (theexceptions being DB and RD) By contrast all but oneof those who failed to attend to this feedback (namelyRC) were severely impaired The other unilateralgroups those with medial and those with orbital lesions(both of whom attended to the appropriate cues) wereboth unimpaired It is important to note that the bilateralorbito-frontal cortex group was impaired although all ofthe patients had attended to the appropriate feedbackThere was no correlation between the total money wonby trial 100 and IQ (full-scale IQ as measured by theNational Adult Reading Test NART ) (Spearmanrsquos rho =277 p = 88) There was also no difference between theIQ of those with dorsolateral lesions who attended to theessential feedback and those who failed to do so (MannndashWhitney U = 165 p = 06)
Appendix 2A shows the responses to questions aboutthe other nonessential types of feedback Patients whosaid that they had used the amount wonlost on eachtrial were clear about this and generally indicated thatthey felt that this was the obvious information to useThese patients also noticedpaid attention to otherfeedback types but they were less clear about whetherthey had used this information to guide their choice ofpattern Among those with dorsolateral lesions classifiedas not having attended to the amount wonlost on eachtrial some had done so in an inconsistent andorintermittent way Most of those who failed to use theamount wonlost on each trial reported that they hadrelied upon the numerical total instead The other threetypes of feedback were noticed by most patients butthey were not always clear about whether they had beenaware of their existence or whether they had beenhelpful in making a choice
Lesion Size
There was no correlation between performance onthe reversal test (as measured by the total earned
466 Journal of Cognitive Neuroscience Volume 16 Number 3
by trial 100) and the size of the lesion measured asthe total area of prefrontal cortex excised (Spearmanrsquosrho = iexcl21 p = 26)
Other Factors Etiology and Use of Medication
No systematic patterns emerged between type of etiologyand performance on the task Only two patients hadsuffered from closed head injury VO with a bilateralorbito-frontal cortex lesion and SI with a unilateralorbitalmedial lesion and neither of these patientswas impaired It was found that 4 of the 9 patientson medication were impaired (444) compared with10 of those 23 not on medication (435) indicating thatmedication did not account for the results
Location of Lesion in the Bilateral Patients WhoWere Impaired
The lesions in the four bilateral patients who wereimpaired on the reversal test (RF VZ VU and JA)all encompassed the regions activated in normal subjectsin the parallel fMRI study using the same task (OrsquoDoh-erty Kringelbach et al 2001) and they spared regionsmore posterior and lateral to the regions of activationConversely the two unimpaired patients with bilaterallesions (VO and RR) both had lesions that wereanterior and posterior respectively to the region acti-vated in the fMRI study
Other Measures Staying with a Pattern After aReward and Switching After a Loss
As a measure of sensitivity to reward the number ofoccasions on which patients chose again a pattern fromwhich they had just gained pound80 or more was counted Asa measure of sensitivity to punishment the number ofoccasions on which patients failed to switch after lossesof pound250 or more was also counted Across all patientsboth measures were very significantly correlated withthe total money won by trial 100 (for reward sensitivitySpearmanrsquos rho = iexcl59 p = 0018 for punishmentsensitivity Spearmanrsquos rho = iexcl70 p = 0002) Furtheranalysis showed that among those patients with bilaterallesions who were impaired on the reversal AS and VWhad scores significantly higher than the mean of thecontrol group on both measures and GS only on the
Table 1 Use of Essential Feedback in Relation to Total Earnedon the Reversal Test
Reversal Performance(Number of SDs) Attended
Failedto Attend
Without dorsolateral lesion
Bilateral orbitalmedial
RFa iexcl24 +
VZa iexcl49 +
VUa iexcl55 +
JAa iexcl21 +
RR 02 +
VO iexcl13 +
Unilateral orbitalmedial
RQ 10 +
LJ iexcl09 +
CL iexcl04 +
TR 07 +
SI (L) iexcl03 +
Unilateral medial
OF (L) 11 +
FG (L) iexcl27 +
EE 02 +
With dorsolateral lesion
UC iexcl01 +
BR iexcl01 +
QG iexcl02 +
VF (L) 06 +
AR (L) iexcl03 +
DB (L) iexcl38 +
LS (L) iexcl15 +
RD (L) iexcl17 +
QO (L) iexcl05 +
RC iexcl12 +
FZ iexcl20 +
BS iexcl46 +
GE (Gave up) +
AG (L) iexcl41 +
LK (L) iexcl60 +
The number of standard deviations by which the patientsrsquo total scoresdiffered from the mean from the control group is shown in relation towhether they attended or failed to attend to the amount won or lost oneach trial and in relation to the presence of a dorsolateral lesionaThese patients had bilateral lesions that lay within the region activatedin the fMRI study in which normal control subjects performed the samereversal task SS and VO had lesions outside this region
Performed at or below fifth centile
Performed at or below first centile
Hornak et al 467
sensitivity to reward measure BK did not have signif-icantly higher scores on either measure but she mademore responses revealing insensitivity to punishmentthan responses revealing insensitivity to reward
DISCUSSION
Patients with lesions in different regions of the prefron-tal cortex were tested on a probabilistic visual discrim-ination reversal test in which it was necessary both todetermine which feedback was crucial and to use thisinformation appropriately to guide the choice of stimu-lus to maximize the reward obtained It was found that
bilateral orbitalmedial prefrontal lesions produced asevere impairment on this test whereas even largeunilateral lesions which included the orbitalmedialregion had no such effect It was also found thatpatients with unilateral medial prefrontal cortex lesionswere unimpaired at this task
The pattern of results was more complicated in thedorsolateral group all of whom had unilateral lesions inthat some patients were impaired at the task whereasothers were not This was shown to be related to whetheras indicated by the posttest questionnaire the patientshad attended to the feedback necessary to succeed on thetask namely the amount won or lost on each trial Nearlyhalf of those with dorsolateral lesions explained how theyhad attended to other nonessential sources of feedbackattempting to maximize their gains in this way Those whodid attend to the essential feedback performed normallywhereas those who did not were as impaired as the groupwith bilateral orbital lesions
The pattern of impairment shown by the dorsolateralpatients who failed to attend can be contrasted withthat shown by the patients with bilateral orbitalmediallesions Although all of these patients with bilateralorbitalmedial prefrontal lesions did attend to the rele-vant feedback they were nevertheless unable to use it toadjust their behavior Instead when stimulusndashrewardcontingencies were reversed they frequently choseagain the incorrect previously rewarded stimulus afterlarge losses or failed to stick with the correct stimulusafter gaining money on it The impairment shown bypatients with bilateral orbitalmedial lesions is consistentwith the findings from our earlier study (Rolls et al1994) in which patients with bilateral ventral prefrontalcortex lesions were found to be impaired on a gono-go
Table 2 Comparisons of the Amount of Money Earned on theReversal Test
BLOFC
ULOFC
DLPFC(Att)
DLPFC(F)
BL OFC
UL OFC p = 028
DLPFC (Att) p = 045 ns
DLPFC (F) ns p = 004 p = 011
Control group p = 002 ns ns p lt 001
Group Comparisons Using MannndashWhitney Nonparametric TestsKruskalndashWallis nonparametric one-way ANOVA revealed significantgroup difference x2 = 23391 df = 4 p lt 001 BL = bilateral UL =unilateral OFC = orbito-frontal cortex DLPFC = dorsolateralprefrontal cortex Att = the patients attended to the crucial feedbackF = the patients failed to attend to the crucial feedback
Significant at p lt 05
Significant at p lt 01
Figure 2 The number ofstandard deviations by whicheach patientrsquos total earned onthe reversal test by trial 100differed from the mean won bythe normal control group BLOFC = bilateral orbito-frontalcortex UL OFC = unilateralorbito-frontal cortex MedialPFC = medial prefrontal cortexDLPFC = dorsolateral prefrontalcortex Attendedfailed toattend = the patient attendedfailed to attend to the crucialfeedback during the reversaltest namely the amount won orlost on each trial
468 Journal of Cognitive Neuroscience Volume 16 Number 3
visual discrimination reversal test However in thisprevious study the more diffuse nature of the lesions(with some produced by closed head injury althoughnevertheless with clear damage to the ventral prefrontalcortex evident in structural MRI scans) precluded pre-cise localization of this impairment to the orbito-frontalcortex In the present study by investigating patientswith surgical and thus more circumscribed lesions of thefrontal lobes we were able to demonstrate that animpairment on reversal learning can occur followingbilateral orbital excisions These results are consistentwith findings from nonhuman primates which implicatethe orbito-frontal cortex in reward and in stimulusndashreward learning and reversal (Dias et al 1996 Rolls1990 1999b 2000) as well as with the results from ourneuroimaging study using the same probabilistic reversaltask (OrsquoDoherty Kringelbach et al 2001) which pro-duced bilateral activation in the orbito-frontal cortex innormal subjects In the present study although as agroup the patients with bilateral orbital lesions weresignificantly impaired on this test only those whoselesions included the areas activated in the fMRI studyshowed a marked impairment whereas the two patientswith bilateral lesions who were not significantly impaired(VO and RR) had small lesions restricted either to theregion anterior or to the region posterior to the regionsof activation (see Figure 3A)
In the fMRI study it was found that the medial and thelateral regions of the orbito-frontal cortex were activat-ed respectively by reward and by punishment andindeed that the degree of activation in these two regionswas correlated with the amount of lsquolsquomoneyrsquorsquo gained orlost (OrsquoDoherty Kringelbach et al 2001) In the pres-ent study the patients with bilateral orbital lesions whowere impaired on the test all had lesions that encom-passed both the more medial and the more lateralregions described in the activation study and for thatreason a difference in sensitivity to reward and topunishment would not be expected in this patientgroup Consistent with this no clear pattern of greatersensitivity to punishment or to reward was observed inthose with bilateral lesions who were impaired Furtherresearch with more discrete lesions within the orbito-frontal cortex may reveal more detailed parallels withthe fMRI study perhaps with sensitivity to reward beingimpaired by medial orbito-frontal cortex lesions andsensitivity to punishment by lateral orbito-frontal cortexlesions However since a recent fMRI study found thatventrolateral activation was associated with reversallearning independently of the effects of negative feed-back (Cools Clark Owen amp Robbins 2002) the medialndashlateral distinction (within the orbital cortex) for rewardand for punishment respectively seems less likely tohold up for this kind of test
It is important that in the present study the groupwith unilateral orbital lesions on either side was unim-paired indicating that it is necessary for the orbital
damage to extend bilaterally before impairments areshown on visual discrimination reversal learning Thissuggests that either the left or the right orbito-frontalcortex on its own can carry out the functions necessaryfor normal performance It is very unlikely that lesionsize per se can explain this effect because somepatients with unilateral orbital lesions who were unim-paired had a larger total area of prefrontal cortexexcised than some of the patients with bilateral orbitallesions who were impaired This was confirmed by thefact that there was no correlation between the totallesion size (amount of prefrontal cortex excised) andperformance on the task
The design of the probabilistic reversal task meansthat two interpretations of the impairment shown bypatients with bilateral orbitalmedial lesions can beexcluded First the repeated touching of the previouslyrewarded stimulus cannot be explained in terms ofsimple motor perseveration (ie as a failure of inhibitorycontrol of the armhand with which the patients reachedout to touch the now-incorrect stimulus) Because aresponse was required and made on every trial thecontinued selection of the old S+ must reflect insteadthe patientrsquos difficulty when reinforcement contingen-cies are reversed in altering the previous associationformed between the stimulus and reward or that be-tween the stimulus and the response he should make toit Although the present study does not distinguishbetween these two interpretations the results are con-sistent with the hypothesis (Rolls 1990 1999b 20002002) that one important function of the orbito-frontalcortex consists in representing the reward and punish-ment value of stimuli and in particular since all patientssucceeded in the early stages of the task (before the firstreversal) in updating the associations between stimuliand reward or punishment value when these change
Secondly the clear instructions that explained thatreversals would occur and that subjects were to alter theirchoice of stimulus accordingly exclude an interpretationin terms of lack of initiative This might have explainedsome of the problems shown by patients in our earlierstudy (Rolls et al 1994) in which no warning was giventhat the contingencies would change The fact that clearexplanation was given about this in the present study atleast excludes an explanation in these terms Howeverwe cannot exclude the possibility that some of thepatients with dorsolateral lesions who were impaired atthe test and who failed to attend to the essential feedbackhad failed fully to understand the task requirements andif so this itself may be viewed as an aspect of executivedysfunction Interestingly among those who failed toattend to the amount won or lost on each trial somedid attend to this for some of the time but did notappreciate its importance and started to attend to othersources of feedback instead (Appendix 2B)
The difficulty in selecting the appropriate feedback orusing it in a consistent manner which was shown by
Hornak et al 469
almost half of the patients in the dorsolateral group andwhich resulted in severely impaired performance on thereversal test has parallels in work with nonhumanprimates in which dorsolateral lesions impaired theability to lsquolsquomonitor multiple stimulirsquorsquo (Petrides amp Pandya1999) as well as with neuroimaging studies of executivefunctions such as those involved in dual-task perfor-mance (Szameitat Torsten Muller amp von Cramon2002) On the posttest questionnaire the patients inthis study reported that instead of using the amountwon or lost on each trial to guide their choice of patternthey had attended instead to other nonessential sourcesof information such as the cumulative total (as anumber or as a bar chart) whether they had won orlost on each trial (ignoring the amount) or the colors orsounds that were associated with gains or losses (Wenote that the self-report provided by these patients withcircumscribed frontal lesions was sufficiently reliablethat across the group the self-report about attention tothe essential feedback was strongly related to the level ofperformance on the task Indeed there was a significant
difference between the proportions of patients whowere impaired who attended 29 and who failed toattend 78 Fisherrsquos exact test p = 02 two-tailed) It isof interest that the dorsolateral group who failed toattend or who failed to attend consistently to theessential feedback during the main reversal phase ofthe test were able to appreciate which feedback to use inthe far easier practice session of the test in which noreversals occurred A similar effect of task difficulty inrevealing impairments in patients with dorsolateral le-sions has been reported by Morris et al (2002) whofound that the ability to employ the appropriate strategyin a test of planning ability was not apparent in the earlypart of the test but became apparent only in the laterharder phase Similarly in Szameitat et alrsquos (2002) studydorsolateral prefrontal cortex activation was producedonly when the task difficulty was increased
In the present study three of the four (R C F Zand B S) whose lesions were confined to the dorso-lateral prefrontal region all failed to attend to the amountwonlost on each trial suggesting that a dorsolateral
Figure 3 Brain maps showinglesion sites Within each groupwith unilateral lesions thosewith right-sided lesions areshown first (A) Bilateral orbito-frontal cortex (or orbital plusmedial prefrontal cortex) (B)Unilateral orbito-frontal (ororbital plus medial) (C) Uni-lateral medial prefrontal cortex(D) Unilateral dorsolateralprefrontal (or dorsolateral plusmedial prefrontal) (E)Unilateral orbito-frontal plusmedial prefrontal plusdorsolateral prefrontal cortex
470 Journal of Cognitive Neuroscience Volume 16 Number 3
lesion may be sufficient to produce this cognitiveexecu-tive impairment In those cases where the dorsolaterallesions extended down into the medial region there arealso parallels with imaging studies in which the moredorsal regions of anterior cingulate described by theauthors as its cognitive division are activated in normalsubjects during tasks involving stimulusndashresponse selec-tion in the face of competing streams of information(Bush Luu amp Posner 2000) The dorsolateral prefrontalcortex lesions did in fact extend into this lsquolsquocognitivedivisionrsquorsquo region of the anterior cingulate cortex in theother five patients with dorsolateral lesions (GE GDOR AG and LK) who also failed to attend to theappropriate feedback However since other patients withcomparable lesions extending into these regions suc-ceeded in attending to this feedback this suggestionmust remain tentative It will be of interest to developour reversal task in the future to simplify the feedbackprovided in the expectation that this will make the taskperformable without deficit by patients with dorsolateralprefrontal cortex lesions but still sensitive to the effectsof lesions to the orbito-frontal cortex due to the reversalcomponent of the task
The findings reported in this study suggest that theprobabilistic reversal test makes demands on differentfunctions attributed respectively to the dorsolateraland to the orbital regions of the prefrontal cortex (cfBechara et al 1998 who reported a study in whichlesions in these regions had dissociable effects ondecision making and on working memory) Thus inthe present study the need to determine which ofmultiple competing sources of feedback should beattended to to maintain attention to this throughoutthe test ignoring other visually salient but noncrucialtypes of feedback (flashing lights total sum displayedcolored bar charts etc) are among the many functionsthat have been attributed to the dorsolateral prefrontalcortex (Szameitat et al 2002 Duncan amp Owen 2000)For a subject who is capable of attending consistently tothe appropriate feedback it is also necessary to use theinformation about the current level of reward associatedwith each pattern to guide his choice on each trial andas such the test also makes demands on functionsattributed to the orbito-frontal cortex (Rolls 19901999a 1999b 2000) The results of the present studyshow that it is possible to be severely impaired on thisprobabilistic visual discrimination reversal test for eitherof these two reasons and in the context that perfor-mance on the test can be independently disrupted bythe effects of dorsolateral and of orbital lesions we haveshown a dissociation between the effects of lesions inthese two regions The ability to attend to the crucialfeedback can be disrupted by a dorsolateral lesion oneither side whereas the ability to use this information tochoose advantageously can be supported by eitherorbital region on its own (after a unilateral orbitallesion) but is abolished by a bilateral orbital lesion
These results are consistent with the view that whereasthe dorsolateral frontal cortex forms part of a network ofprefrontal regions recruited to solve diverse cognitiveproblems especially those with an lsquolsquoexecutiversquorsquo compo-nent (in this case appreciating which feedback is rele-vantimportant) (Bush et al 2000 Duncan amp Owen2000) the orbito-frontal cortex is involved in the repre-sentation of the changing reward value of stimuli (Rolls1990 1999b 2000 2002) so that behavior can be mod-ified accordingly As such the present study contributesboth to our understanding of the different functions ofthese two regions of frontal lobe and to how theseregions need to cooperate on complex tasks such as theone used here A similar argument is made by Manes et al(2002) who showed how the ventral and dorsal aspects ofthe prefrontal cortex must interact in the maintenance ofrational and lsquolsquononriskyrsquorsquo decision-making tasks
One of the underlying hypotheses of the researchdescribed here is that some of the reasons for thebehavioral and emotional changes that follow damageto the prefrontal cortex may be related to deficits indecoding the reward and punishment value of stimuliand using the results of the decoding to modify behaviorand the ongoing emotional or mood state (Rolls 19901999a 1999b Rolls et al 1994) In this context it is ofinterest that the patients with bilateral orbito-frontalcortex damage who were impaired at the visual discrim-ination reversal task (see Table 1) had high scores onparts of a social behavior questionnaire in which thepatients were rated on behaviors such as the recognitionof emotion in others (eg their sad angry or disgustedmood) in interpersonal relationships (such as not caringwhat others think and not being close to the family) insociability (is not sociable and has difficulty making ormaintaining close relationships) emotional empathy(eg when others are happy is not happy for them)public behavior (is uncooperative) antisocial behavior (iscritical of and impatient with others) and impulsivity(does things without thinking) (Hornak Bramham RollsMorris OrsquoDoherty amp Polkey 2003) all of which couldreflect less behavioral sensitivity to different types ofpunishment and reward Further in a subjective emo-tional change questionnaire in which the patients re-ported on any changes in the intensity andor frequencyof their own experience of emotions since surgery thebilateral orbito-frontal cortex patients with deficits in thevisual discrimination reversal task reported a number ofchanges including changes in sadness anger fear andhappiness and were as a group significantly different inthese respects from the dorsolateral prefrontal cortexlesion group included in that comparison (Hornak et al2003) However it must also be pointed out that thepatients with unilateral orbito-frontalanterior cingulatelesions (the BA 9ACC and BA 9ACC + orbital groups ofthat article) also reported marked emotional changes andthey were also less well-adjusted socially than the dorso-lateral group but had no measured deficit in reversal The
Hornak et al 471
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
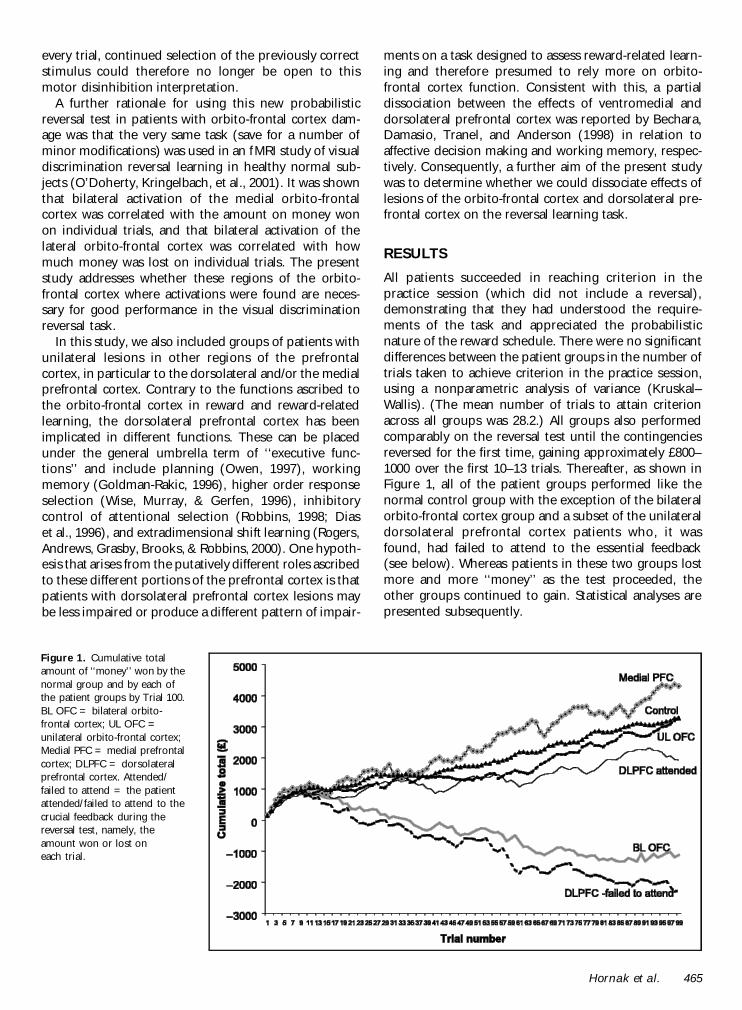
every trial continued selection of the previously correctstimulus could therefore no longer be open to thismotor disinhibition interpretation
A further rationale for using this new probabilisticreversal test in patients with orbito-frontal cortex dam-age was that the very same task (save for a number ofminor modifications) was used in an fMRI study of visualdiscrimination reversal learning in healthy normal sub-jects (OrsquoDoherty Kringelbach et al 2001) It was shownthat bilateral activation of the medial orbito-frontalcortex was correlated with the amount on money wonon individual trials and that bilateral activation of thelateral orbito-frontal cortex was correlated with howmuch money was lost on individual trials The presentstudy addresses whether these regions of the orbito-frontal cortex where activations were found are neces-sary for good performance in the visual discriminationreversal task
In this study we also included groups of patients withunilateral lesions in other regions of the prefrontalcortex in particular to the dorsolateral andor the medialprefrontal cortex Contrary to the functions ascribed tothe orbito-frontal cortex in reward and reward-relatedlearning the dorsolateral prefrontal cortex has beenimplicated in different functions These can be placedunder the general umbrella term of lsquolsquoexecutive func-tionsrsquorsquo and include planning (Owen 1997) workingmemory (Goldman-Rakic 1996) higher order responseselection (Wise Murray amp Gerfen 1996) inhibitorycontrol of attentional selection (Robbins 1998 Diaset al 1996) and extradimensional shift learning (RogersAndrews Grasby Brooks amp Robbins 2000) One hypoth-esis that arises from the putatively different roles ascribedto these different portions of the prefrontal cortex is thatpatients with dorsolateral prefrontal cortex lesions maybe less impaired or produce a different pattern of impair-
ments on a task designed to assess reward-related learn-ing and therefore presumed to rely more on orbito-frontal cortex function Consistent with this a partialdissociation between the effects of ventromedial anddorsolateral prefrontal cortex was reported by BecharaDamasio Tranel and Anderson (1998) in relation toaffective decision making and working memory respec-tively Consequently a further aim of the present studywas to determine whether we could dissociate effects oflesions of the orbito-frontal cortex and dorsolateral pre-frontal cortex on the reversal learning task
RESULTS
All patients succeeded in reaching criterion in thepractice session (which did not include a reversal)demonstrating that they had understood the require-ments of the task and appreciated the probabilisticnature of the reward schedule There were no significantdifferences between the patient groups in the number oftrials taken to achieve criterion in the practice sessionusing a nonparametric analysis of variance (KruskalndashWallis) (The mean number of trials to attain criterionacross all groups was 282) All groups also performedcomparably on the reversal test until the contingenciesreversed for the first time gaining approximately pound800ndash1000 over the first 10ndash13 trials Thereafter as shown inFigure 1 all of the patient groups performed like thenormal control group with the exception of the bilateralorbito-frontal cortex group and a subset of the unilateraldorsolateral prefrontal cortex patients who it wasfound had failed to attend to the essential feedback(see below) Whereas patients in these two groups lostmore and more lsquolsquomoneyrsquorsquo as the test proceeded theother groups continued to gain Statistical analyses arepresented subsequently
Figure 1 Cumulative totalamount of lsquolsquomoneyrsquorsquo won by thenormal group and by each ofthe patient groups by Trial 100BL OFC = bilateral orbito-frontal cortex UL OFC =unilateral orbito-frontal cortexMedial PFC = medial prefrontalcortex DLPFC = dorsolateralprefrontal cortex Attendedfailed to attend = the patientattended failed to attend to thecrucial feedback during thereversal test namely theamount won or lost oneach trial
Hornak et al 465
Posttest Questionnaire
Feedback Found Most Useful
Although all patients were able to use the essentialfeedback concerning the amount won or lost on eachtrial during the brief easy prereversal phase of the testthe results of the posttest questionnaire revealed animportant difference between groups in the ability toappreciate which was the essential feedback when thetest became more challenging (ie during the reversalphase of the test) Thus 8 of the 17 patients whose lesionsincluded the dorsolateral prefrontal region unilaterallywhen asked the open-ended question lsquolsquoWhat informationon the screen did you find most useful in keeping track ofwhich pattern was currently the good onersquorsquo explainedhow they had relied on various nonessential sources offeedback and when asked about the feedback showingthe amount won or lost on each trial denied that they hadfound this feedback to be the most useful (see Table 1)By contrast all of the 14 patients whose lesion (bilateralor unilateral) did not encroach on the dorsolateral pre-frontal region reported that this was the obvious feed-back to use and that they had used it to guide their choiceof stimulus This was also true for all normal controlsubjects Statistical comparison between patients withand without a dorsolateral lesion revealed a very signifi-cant difference between the numbers in each group whodid and who did not attend to the essential feedback(Fisherrsquos exact test p = 006 two-tailed)
Other Feedback Used
Patients with dorsolateral prefrontal damage who failedto attend to the amount wonlost on each trial reportedinstead that they had used a variety of subsidiary non-essential types of feedback which by themselves wouldnot allow the subject to perform the reversal tasksuccessfully (see Appendices 2A and 2B)
Total Scored by Trial 100
Group Results
We tested for a difference between the groups in thetotal money gained by trial 100 Statistical analysisrevealed a highly significant difference (KruskalndashWallisx2(4) = 2339 p lt 001) Paired comparisons betweenthe separate groups and the normal control groupas shown in Table 2 revealed a significant impairmentonly in the bilateral orbito-frontal cortex group (MannndashWhitney test p = 002 two-tailed) and the dorsolateral(failed to attend) group ( p lt 001 two-tailed) Table 2also shows the results for the other paired comparisonsbetween the groups This reveals that the bilateralorbito-frontal cortex group was significantly impairedrelative to the unilateral orbito-frontal cortex group( p = 028 two-tailed) and that there was no significantdifference between the bilateral orbito-frontal cortex
group and the unilateral dorsolateral (failed to attend)group (We note that the two critical comparisonsshown in Table 2 between the bilateral orbito-frontalcortex group and normal controls and between thelsquolsquodorsolateral prefrontal cortex failed to attendrsquorsquo groupand normal controls are still significant after Bonferronicorrection for multiple comparisons)
Individual Results
The number of standard deviations (SD) was calculatedby which each patientrsquos total (gained by trial 100) differedfrom the mean amount won by the Control group by trial100 Figure 2 and Table 1 show each patientrsquos SD inrelation to whether they attended or failed to attend tothe essential feedback Most patients with dorsolateralprefrontal lesions who were able to determine whichfeedback cue they should use and who kept using thisfeedback throughout the test performed normally (theexceptions being DB and RD) By contrast all but oneof those who failed to attend to this feedback (namelyRC) were severely impaired The other unilateralgroups those with medial and those with orbital lesions(both of whom attended to the appropriate cues) wereboth unimpaired It is important to note that the bilateralorbito-frontal cortex group was impaired although all ofthe patients had attended to the appropriate feedbackThere was no correlation between the total money wonby trial 100 and IQ (full-scale IQ as measured by theNational Adult Reading Test NART ) (Spearmanrsquos rho =277 p = 88) There was also no difference between theIQ of those with dorsolateral lesions who attended to theessential feedback and those who failed to do so (MannndashWhitney U = 165 p = 06)
Appendix 2A shows the responses to questions aboutthe other nonessential types of feedback Patients whosaid that they had used the amount wonlost on eachtrial were clear about this and generally indicated thatthey felt that this was the obvious information to useThese patients also noticedpaid attention to otherfeedback types but they were less clear about whetherthey had used this information to guide their choice ofpattern Among those with dorsolateral lesions classifiedas not having attended to the amount wonlost on eachtrial some had done so in an inconsistent andorintermittent way Most of those who failed to use theamount wonlost on each trial reported that they hadrelied upon the numerical total instead The other threetypes of feedback were noticed by most patients butthey were not always clear about whether they had beenaware of their existence or whether they had beenhelpful in making a choice
Lesion Size
There was no correlation between performance onthe reversal test (as measured by the total earned
466 Journal of Cognitive Neuroscience Volume 16 Number 3
by trial 100) and the size of the lesion measured asthe total area of prefrontal cortex excised (Spearmanrsquosrho = iexcl21 p = 26)
Other Factors Etiology and Use of Medication
No systematic patterns emerged between type of etiologyand performance on the task Only two patients hadsuffered from closed head injury VO with a bilateralorbito-frontal cortex lesion and SI with a unilateralorbitalmedial lesion and neither of these patientswas impaired It was found that 4 of the 9 patientson medication were impaired (444) compared with10 of those 23 not on medication (435) indicating thatmedication did not account for the results
Location of Lesion in the Bilateral Patients WhoWere Impaired
The lesions in the four bilateral patients who wereimpaired on the reversal test (RF VZ VU and JA)all encompassed the regions activated in normal subjectsin the parallel fMRI study using the same task (OrsquoDoh-erty Kringelbach et al 2001) and they spared regionsmore posterior and lateral to the regions of activationConversely the two unimpaired patients with bilaterallesions (VO and RR) both had lesions that wereanterior and posterior respectively to the region acti-vated in the fMRI study
Other Measures Staying with a Pattern After aReward and Switching After a Loss
As a measure of sensitivity to reward the number ofoccasions on which patients chose again a pattern fromwhich they had just gained pound80 or more was counted Asa measure of sensitivity to punishment the number ofoccasions on which patients failed to switch after lossesof pound250 or more was also counted Across all patientsboth measures were very significantly correlated withthe total money won by trial 100 (for reward sensitivitySpearmanrsquos rho = iexcl59 p = 0018 for punishmentsensitivity Spearmanrsquos rho = iexcl70 p = 0002) Furtheranalysis showed that among those patients with bilaterallesions who were impaired on the reversal AS and VWhad scores significantly higher than the mean of thecontrol group on both measures and GS only on the
Table 1 Use of Essential Feedback in Relation to Total Earnedon the Reversal Test
Reversal Performance(Number of SDs) Attended
Failedto Attend
Without dorsolateral lesion
Bilateral orbitalmedial
RFa iexcl24 +
VZa iexcl49 +
VUa iexcl55 +
JAa iexcl21 +
RR 02 +
VO iexcl13 +
Unilateral orbitalmedial
RQ 10 +
LJ iexcl09 +
CL iexcl04 +
TR 07 +
SI (L) iexcl03 +
Unilateral medial
OF (L) 11 +
FG (L) iexcl27 +
EE 02 +
With dorsolateral lesion
UC iexcl01 +
BR iexcl01 +
QG iexcl02 +
VF (L) 06 +
AR (L) iexcl03 +
DB (L) iexcl38 +
LS (L) iexcl15 +
RD (L) iexcl17 +
QO (L) iexcl05 +
RC iexcl12 +
FZ iexcl20 +
BS iexcl46 +
GE (Gave up) +
AG (L) iexcl41 +
LK (L) iexcl60 +
The number of standard deviations by which the patientsrsquo total scoresdiffered from the mean from the control group is shown in relation towhether they attended or failed to attend to the amount won or lost oneach trial and in relation to the presence of a dorsolateral lesionaThese patients had bilateral lesions that lay within the region activatedin the fMRI study in which normal control subjects performed the samereversal task SS and VO had lesions outside this region
Performed at or below fifth centile
Performed at or below first centile
Hornak et al 467
sensitivity to reward measure BK did not have signif-icantly higher scores on either measure but she mademore responses revealing insensitivity to punishmentthan responses revealing insensitivity to reward
DISCUSSION
Patients with lesions in different regions of the prefron-tal cortex were tested on a probabilistic visual discrim-ination reversal test in which it was necessary both todetermine which feedback was crucial and to use thisinformation appropriately to guide the choice of stimu-lus to maximize the reward obtained It was found that
bilateral orbitalmedial prefrontal lesions produced asevere impairment on this test whereas even largeunilateral lesions which included the orbitalmedialregion had no such effect It was also found thatpatients with unilateral medial prefrontal cortex lesionswere unimpaired at this task
The pattern of results was more complicated in thedorsolateral group all of whom had unilateral lesions inthat some patients were impaired at the task whereasothers were not This was shown to be related to whetheras indicated by the posttest questionnaire the patientshad attended to the feedback necessary to succeed on thetask namely the amount won or lost on each trial Nearlyhalf of those with dorsolateral lesions explained how theyhad attended to other nonessential sources of feedbackattempting to maximize their gains in this way Those whodid attend to the essential feedback performed normallywhereas those who did not were as impaired as the groupwith bilateral orbital lesions
The pattern of impairment shown by the dorsolateralpatients who failed to attend can be contrasted withthat shown by the patients with bilateral orbitalmediallesions Although all of these patients with bilateralorbitalmedial prefrontal lesions did attend to the rele-vant feedback they were nevertheless unable to use it toadjust their behavior Instead when stimulusndashrewardcontingencies were reversed they frequently choseagain the incorrect previously rewarded stimulus afterlarge losses or failed to stick with the correct stimulusafter gaining money on it The impairment shown bypatients with bilateral orbitalmedial lesions is consistentwith the findings from our earlier study (Rolls et al1994) in which patients with bilateral ventral prefrontalcortex lesions were found to be impaired on a gono-go
Table 2 Comparisons of the Amount of Money Earned on theReversal Test
BLOFC
ULOFC
DLPFC(Att)
DLPFC(F)
BL OFC
UL OFC p = 028
DLPFC (Att) p = 045 ns
DLPFC (F) ns p = 004 p = 011
Control group p = 002 ns ns p lt 001
Group Comparisons Using MannndashWhitney Nonparametric TestsKruskalndashWallis nonparametric one-way ANOVA revealed significantgroup difference x2 = 23391 df = 4 p lt 001 BL = bilateral UL =unilateral OFC = orbito-frontal cortex DLPFC = dorsolateralprefrontal cortex Att = the patients attended to the crucial feedbackF = the patients failed to attend to the crucial feedback
Significant at p lt 05
Significant at p lt 01
Figure 2 The number ofstandard deviations by whicheach patientrsquos total earned onthe reversal test by trial 100differed from the mean won bythe normal control group BLOFC = bilateral orbito-frontalcortex UL OFC = unilateralorbito-frontal cortex MedialPFC = medial prefrontal cortexDLPFC = dorsolateral prefrontalcortex Attendedfailed toattend = the patient attendedfailed to attend to the crucialfeedback during the reversaltest namely the amount won orlost on each trial
468 Journal of Cognitive Neuroscience Volume 16 Number 3
visual discrimination reversal test However in thisprevious study the more diffuse nature of the lesions(with some produced by closed head injury althoughnevertheless with clear damage to the ventral prefrontalcortex evident in structural MRI scans) precluded pre-cise localization of this impairment to the orbito-frontalcortex In the present study by investigating patientswith surgical and thus more circumscribed lesions of thefrontal lobes we were able to demonstrate that animpairment on reversal learning can occur followingbilateral orbital excisions These results are consistentwith findings from nonhuman primates which implicatethe orbito-frontal cortex in reward and in stimulusndashreward learning and reversal (Dias et al 1996 Rolls1990 1999b 2000) as well as with the results from ourneuroimaging study using the same probabilistic reversaltask (OrsquoDoherty Kringelbach et al 2001) which pro-duced bilateral activation in the orbito-frontal cortex innormal subjects In the present study although as agroup the patients with bilateral orbital lesions weresignificantly impaired on this test only those whoselesions included the areas activated in the fMRI studyshowed a marked impairment whereas the two patientswith bilateral lesions who were not significantly impaired(VO and RR) had small lesions restricted either to theregion anterior or to the region posterior to the regionsof activation (see Figure 3A)
In the fMRI study it was found that the medial and thelateral regions of the orbito-frontal cortex were activat-ed respectively by reward and by punishment andindeed that the degree of activation in these two regionswas correlated with the amount of lsquolsquomoneyrsquorsquo gained orlost (OrsquoDoherty Kringelbach et al 2001) In the pres-ent study the patients with bilateral orbital lesions whowere impaired on the test all had lesions that encom-passed both the more medial and the more lateralregions described in the activation study and for thatreason a difference in sensitivity to reward and topunishment would not be expected in this patientgroup Consistent with this no clear pattern of greatersensitivity to punishment or to reward was observed inthose with bilateral lesions who were impaired Furtherresearch with more discrete lesions within the orbito-frontal cortex may reveal more detailed parallels withthe fMRI study perhaps with sensitivity to reward beingimpaired by medial orbito-frontal cortex lesions andsensitivity to punishment by lateral orbito-frontal cortexlesions However since a recent fMRI study found thatventrolateral activation was associated with reversallearning independently of the effects of negative feed-back (Cools Clark Owen amp Robbins 2002) the medialndashlateral distinction (within the orbital cortex) for rewardand for punishment respectively seems less likely tohold up for this kind of test
It is important that in the present study the groupwith unilateral orbital lesions on either side was unim-paired indicating that it is necessary for the orbital
damage to extend bilaterally before impairments areshown on visual discrimination reversal learning Thissuggests that either the left or the right orbito-frontalcortex on its own can carry out the functions necessaryfor normal performance It is very unlikely that lesionsize per se can explain this effect because somepatients with unilateral orbital lesions who were unim-paired had a larger total area of prefrontal cortexexcised than some of the patients with bilateral orbitallesions who were impaired This was confirmed by thefact that there was no correlation between the totallesion size (amount of prefrontal cortex excised) andperformance on the task
The design of the probabilistic reversal task meansthat two interpretations of the impairment shown bypatients with bilateral orbitalmedial lesions can beexcluded First the repeated touching of the previouslyrewarded stimulus cannot be explained in terms ofsimple motor perseveration (ie as a failure of inhibitorycontrol of the armhand with which the patients reachedout to touch the now-incorrect stimulus) Because aresponse was required and made on every trial thecontinued selection of the old S+ must reflect insteadthe patientrsquos difficulty when reinforcement contingen-cies are reversed in altering the previous associationformed between the stimulus and reward or that be-tween the stimulus and the response he should make toit Although the present study does not distinguishbetween these two interpretations the results are con-sistent with the hypothesis (Rolls 1990 1999b 20002002) that one important function of the orbito-frontalcortex consists in representing the reward and punish-ment value of stimuli and in particular since all patientssucceeded in the early stages of the task (before the firstreversal) in updating the associations between stimuliand reward or punishment value when these change
Secondly the clear instructions that explained thatreversals would occur and that subjects were to alter theirchoice of stimulus accordingly exclude an interpretationin terms of lack of initiative This might have explainedsome of the problems shown by patients in our earlierstudy (Rolls et al 1994) in which no warning was giventhat the contingencies would change The fact that clearexplanation was given about this in the present study atleast excludes an explanation in these terms Howeverwe cannot exclude the possibility that some of thepatients with dorsolateral lesions who were impaired atthe test and who failed to attend to the essential feedbackhad failed fully to understand the task requirements andif so this itself may be viewed as an aspect of executivedysfunction Interestingly among those who failed toattend to the amount won or lost on each trial somedid attend to this for some of the time but did notappreciate its importance and started to attend to othersources of feedback instead (Appendix 2B)
The difficulty in selecting the appropriate feedback orusing it in a consistent manner which was shown by
Hornak et al 469
almost half of the patients in the dorsolateral group andwhich resulted in severely impaired performance on thereversal test has parallels in work with nonhumanprimates in which dorsolateral lesions impaired theability to lsquolsquomonitor multiple stimulirsquorsquo (Petrides amp Pandya1999) as well as with neuroimaging studies of executivefunctions such as those involved in dual-task perfor-mance (Szameitat Torsten Muller amp von Cramon2002) On the posttest questionnaire the patients inthis study reported that instead of using the amountwon or lost on each trial to guide their choice of patternthey had attended instead to other nonessential sourcesof information such as the cumulative total (as anumber or as a bar chart) whether they had won orlost on each trial (ignoring the amount) or the colors orsounds that were associated with gains or losses (Wenote that the self-report provided by these patients withcircumscribed frontal lesions was sufficiently reliablethat across the group the self-report about attention tothe essential feedback was strongly related to the level ofperformance on the task Indeed there was a significant
difference between the proportions of patients whowere impaired who attended 29 and who failed toattend 78 Fisherrsquos exact test p = 02 two-tailed) It isof interest that the dorsolateral group who failed toattend or who failed to attend consistently to theessential feedback during the main reversal phase ofthe test were able to appreciate which feedback to use inthe far easier practice session of the test in which noreversals occurred A similar effect of task difficulty inrevealing impairments in patients with dorsolateral le-sions has been reported by Morris et al (2002) whofound that the ability to employ the appropriate strategyin a test of planning ability was not apparent in the earlypart of the test but became apparent only in the laterharder phase Similarly in Szameitat et alrsquos (2002) studydorsolateral prefrontal cortex activation was producedonly when the task difficulty was increased
In the present study three of the four (R C F Zand B S) whose lesions were confined to the dorso-lateral prefrontal region all failed to attend to the amountwonlost on each trial suggesting that a dorsolateral
Figure 3 Brain maps showinglesion sites Within each groupwith unilateral lesions thosewith right-sided lesions areshown first (A) Bilateral orbito-frontal cortex (or orbital plusmedial prefrontal cortex) (B)Unilateral orbito-frontal (ororbital plus medial) (C) Uni-lateral medial prefrontal cortex(D) Unilateral dorsolateralprefrontal (or dorsolateral plusmedial prefrontal) (E)Unilateral orbito-frontal plusmedial prefrontal plusdorsolateral prefrontal cortex
470 Journal of Cognitive Neuroscience Volume 16 Number 3
lesion may be sufficient to produce this cognitiveexecu-tive impairment In those cases where the dorsolaterallesions extended down into the medial region there arealso parallels with imaging studies in which the moredorsal regions of anterior cingulate described by theauthors as its cognitive division are activated in normalsubjects during tasks involving stimulusndashresponse selec-tion in the face of competing streams of information(Bush Luu amp Posner 2000) The dorsolateral prefrontalcortex lesions did in fact extend into this lsquolsquocognitivedivisionrsquorsquo region of the anterior cingulate cortex in theother five patients with dorsolateral lesions (GE GDOR AG and LK) who also failed to attend to theappropriate feedback However since other patients withcomparable lesions extending into these regions suc-ceeded in attending to this feedback this suggestionmust remain tentative It will be of interest to developour reversal task in the future to simplify the feedbackprovided in the expectation that this will make the taskperformable without deficit by patients with dorsolateralprefrontal cortex lesions but still sensitive to the effectsof lesions to the orbito-frontal cortex due to the reversalcomponent of the task
The findings reported in this study suggest that theprobabilistic reversal test makes demands on differentfunctions attributed respectively to the dorsolateraland to the orbital regions of the prefrontal cortex (cfBechara et al 1998 who reported a study in whichlesions in these regions had dissociable effects ondecision making and on working memory) Thus inthe present study the need to determine which ofmultiple competing sources of feedback should beattended to to maintain attention to this throughoutthe test ignoring other visually salient but noncrucialtypes of feedback (flashing lights total sum displayedcolored bar charts etc) are among the many functionsthat have been attributed to the dorsolateral prefrontalcortex (Szameitat et al 2002 Duncan amp Owen 2000)For a subject who is capable of attending consistently tothe appropriate feedback it is also necessary to use theinformation about the current level of reward associatedwith each pattern to guide his choice on each trial andas such the test also makes demands on functionsattributed to the orbito-frontal cortex (Rolls 19901999a 1999b 2000) The results of the present studyshow that it is possible to be severely impaired on thisprobabilistic visual discrimination reversal test for eitherof these two reasons and in the context that perfor-mance on the test can be independently disrupted bythe effects of dorsolateral and of orbital lesions we haveshown a dissociation between the effects of lesions inthese two regions The ability to attend to the crucialfeedback can be disrupted by a dorsolateral lesion oneither side whereas the ability to use this information tochoose advantageously can be supported by eitherorbital region on its own (after a unilateral orbitallesion) but is abolished by a bilateral orbital lesion
These results are consistent with the view that whereasthe dorsolateral frontal cortex forms part of a network ofprefrontal regions recruited to solve diverse cognitiveproblems especially those with an lsquolsquoexecutiversquorsquo compo-nent (in this case appreciating which feedback is rele-vantimportant) (Bush et al 2000 Duncan amp Owen2000) the orbito-frontal cortex is involved in the repre-sentation of the changing reward value of stimuli (Rolls1990 1999b 2000 2002) so that behavior can be mod-ified accordingly As such the present study contributesboth to our understanding of the different functions ofthese two regions of frontal lobe and to how theseregions need to cooperate on complex tasks such as theone used here A similar argument is made by Manes et al(2002) who showed how the ventral and dorsal aspects ofthe prefrontal cortex must interact in the maintenance ofrational and lsquolsquononriskyrsquorsquo decision-making tasks
One of the underlying hypotheses of the researchdescribed here is that some of the reasons for thebehavioral and emotional changes that follow damageto the prefrontal cortex may be related to deficits indecoding the reward and punishment value of stimuliand using the results of the decoding to modify behaviorand the ongoing emotional or mood state (Rolls 19901999a 1999b Rolls et al 1994) In this context it is ofinterest that the patients with bilateral orbito-frontalcortex damage who were impaired at the visual discrim-ination reversal task (see Table 1) had high scores onparts of a social behavior questionnaire in which thepatients were rated on behaviors such as the recognitionof emotion in others (eg their sad angry or disgustedmood) in interpersonal relationships (such as not caringwhat others think and not being close to the family) insociability (is not sociable and has difficulty making ormaintaining close relationships) emotional empathy(eg when others are happy is not happy for them)public behavior (is uncooperative) antisocial behavior (iscritical of and impatient with others) and impulsivity(does things without thinking) (Hornak Bramham RollsMorris OrsquoDoherty amp Polkey 2003) all of which couldreflect less behavioral sensitivity to different types ofpunishment and reward Further in a subjective emo-tional change questionnaire in which the patients re-ported on any changes in the intensity andor frequencyof their own experience of emotions since surgery thebilateral orbito-frontal cortex patients with deficits in thevisual discrimination reversal task reported a number ofchanges including changes in sadness anger fear andhappiness and were as a group significantly different inthese respects from the dorsolateral prefrontal cortexlesion group included in that comparison (Hornak et al2003) However it must also be pointed out that thepatients with unilateral orbito-frontalanterior cingulatelesions (the BA 9ACC and BA 9ACC + orbital groups ofthat article) also reported marked emotional changes andthey were also less well-adjusted socially than the dorso-lateral group but had no measured deficit in reversal The
Hornak et al 471
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3

Posttest Questionnaire
Feedback Found Most Useful
Although all patients were able to use the essentialfeedback concerning the amount won or lost on eachtrial during the brief easy prereversal phase of the testthe results of the posttest questionnaire revealed animportant difference between groups in the ability toappreciate which was the essential feedback when thetest became more challenging (ie during the reversalphase of the test) Thus 8 of the 17 patients whose lesionsincluded the dorsolateral prefrontal region unilaterallywhen asked the open-ended question lsquolsquoWhat informationon the screen did you find most useful in keeping track ofwhich pattern was currently the good onersquorsquo explainedhow they had relied on various nonessential sources offeedback and when asked about the feedback showingthe amount won or lost on each trial denied that they hadfound this feedback to be the most useful (see Table 1)By contrast all of the 14 patients whose lesion (bilateralor unilateral) did not encroach on the dorsolateral pre-frontal region reported that this was the obvious feed-back to use and that they had used it to guide their choiceof stimulus This was also true for all normal controlsubjects Statistical comparison between patients withand without a dorsolateral lesion revealed a very signifi-cant difference between the numbers in each group whodid and who did not attend to the essential feedback(Fisherrsquos exact test p = 006 two-tailed)
Other Feedback Used
Patients with dorsolateral prefrontal damage who failedto attend to the amount wonlost on each trial reportedinstead that they had used a variety of subsidiary non-essential types of feedback which by themselves wouldnot allow the subject to perform the reversal tasksuccessfully (see Appendices 2A and 2B)
Total Scored by Trial 100
Group Results
We tested for a difference between the groups in thetotal money gained by trial 100 Statistical analysisrevealed a highly significant difference (KruskalndashWallisx2(4) = 2339 p lt 001) Paired comparisons betweenthe separate groups and the normal control groupas shown in Table 2 revealed a significant impairmentonly in the bilateral orbito-frontal cortex group (MannndashWhitney test p = 002 two-tailed) and the dorsolateral(failed to attend) group ( p lt 001 two-tailed) Table 2also shows the results for the other paired comparisonsbetween the groups This reveals that the bilateralorbito-frontal cortex group was significantly impairedrelative to the unilateral orbito-frontal cortex group( p = 028 two-tailed) and that there was no significantdifference between the bilateral orbito-frontal cortex
group and the unilateral dorsolateral (failed to attend)group (We note that the two critical comparisonsshown in Table 2 between the bilateral orbito-frontalcortex group and normal controls and between thelsquolsquodorsolateral prefrontal cortex failed to attendrsquorsquo groupand normal controls are still significant after Bonferronicorrection for multiple comparisons)
Individual Results
The number of standard deviations (SD) was calculatedby which each patientrsquos total (gained by trial 100) differedfrom the mean amount won by the Control group by trial100 Figure 2 and Table 1 show each patientrsquos SD inrelation to whether they attended or failed to attend tothe essential feedback Most patients with dorsolateralprefrontal lesions who were able to determine whichfeedback cue they should use and who kept using thisfeedback throughout the test performed normally (theexceptions being DB and RD) By contrast all but oneof those who failed to attend to this feedback (namelyRC) were severely impaired The other unilateralgroups those with medial and those with orbital lesions(both of whom attended to the appropriate cues) wereboth unimpaired It is important to note that the bilateralorbito-frontal cortex group was impaired although all ofthe patients had attended to the appropriate feedbackThere was no correlation between the total money wonby trial 100 and IQ (full-scale IQ as measured by theNational Adult Reading Test NART ) (Spearmanrsquos rho =277 p = 88) There was also no difference between theIQ of those with dorsolateral lesions who attended to theessential feedback and those who failed to do so (MannndashWhitney U = 165 p = 06)
Appendix 2A shows the responses to questions aboutthe other nonessential types of feedback Patients whosaid that they had used the amount wonlost on eachtrial were clear about this and generally indicated thatthey felt that this was the obvious information to useThese patients also noticedpaid attention to otherfeedback types but they were less clear about whetherthey had used this information to guide their choice ofpattern Among those with dorsolateral lesions classifiedas not having attended to the amount wonlost on eachtrial some had done so in an inconsistent andorintermittent way Most of those who failed to use theamount wonlost on each trial reported that they hadrelied upon the numerical total instead The other threetypes of feedback were noticed by most patients butthey were not always clear about whether they had beenaware of their existence or whether they had beenhelpful in making a choice
Lesion Size
There was no correlation between performance onthe reversal test (as measured by the total earned
466 Journal of Cognitive Neuroscience Volume 16 Number 3
by trial 100) and the size of the lesion measured asthe total area of prefrontal cortex excised (Spearmanrsquosrho = iexcl21 p = 26)
Other Factors Etiology and Use of Medication
No systematic patterns emerged between type of etiologyand performance on the task Only two patients hadsuffered from closed head injury VO with a bilateralorbito-frontal cortex lesion and SI with a unilateralorbitalmedial lesion and neither of these patientswas impaired It was found that 4 of the 9 patientson medication were impaired (444) compared with10 of those 23 not on medication (435) indicating thatmedication did not account for the results
Location of Lesion in the Bilateral Patients WhoWere Impaired
The lesions in the four bilateral patients who wereimpaired on the reversal test (RF VZ VU and JA)all encompassed the regions activated in normal subjectsin the parallel fMRI study using the same task (OrsquoDoh-erty Kringelbach et al 2001) and they spared regionsmore posterior and lateral to the regions of activationConversely the two unimpaired patients with bilaterallesions (VO and RR) both had lesions that wereanterior and posterior respectively to the region acti-vated in the fMRI study
Other Measures Staying with a Pattern After aReward and Switching After a Loss
As a measure of sensitivity to reward the number ofoccasions on which patients chose again a pattern fromwhich they had just gained pound80 or more was counted Asa measure of sensitivity to punishment the number ofoccasions on which patients failed to switch after lossesof pound250 or more was also counted Across all patientsboth measures were very significantly correlated withthe total money won by trial 100 (for reward sensitivitySpearmanrsquos rho = iexcl59 p = 0018 for punishmentsensitivity Spearmanrsquos rho = iexcl70 p = 0002) Furtheranalysis showed that among those patients with bilaterallesions who were impaired on the reversal AS and VWhad scores significantly higher than the mean of thecontrol group on both measures and GS only on the
Table 1 Use of Essential Feedback in Relation to Total Earnedon the Reversal Test
Reversal Performance(Number of SDs) Attended
Failedto Attend
Without dorsolateral lesion
Bilateral orbitalmedial
RFa iexcl24 +
VZa iexcl49 +
VUa iexcl55 +
JAa iexcl21 +
RR 02 +
VO iexcl13 +
Unilateral orbitalmedial
RQ 10 +
LJ iexcl09 +
CL iexcl04 +
TR 07 +
SI (L) iexcl03 +
Unilateral medial
OF (L) 11 +
FG (L) iexcl27 +
EE 02 +
With dorsolateral lesion
UC iexcl01 +
BR iexcl01 +
QG iexcl02 +
VF (L) 06 +
AR (L) iexcl03 +
DB (L) iexcl38 +
LS (L) iexcl15 +
RD (L) iexcl17 +
QO (L) iexcl05 +
RC iexcl12 +
FZ iexcl20 +
BS iexcl46 +
GE (Gave up) +
AG (L) iexcl41 +
LK (L) iexcl60 +
The number of standard deviations by which the patientsrsquo total scoresdiffered from the mean from the control group is shown in relation towhether they attended or failed to attend to the amount won or lost oneach trial and in relation to the presence of a dorsolateral lesionaThese patients had bilateral lesions that lay within the region activatedin the fMRI study in which normal control subjects performed the samereversal task SS and VO had lesions outside this region
Performed at or below fifth centile
Performed at or below first centile
Hornak et al 467
sensitivity to reward measure BK did not have signif-icantly higher scores on either measure but she mademore responses revealing insensitivity to punishmentthan responses revealing insensitivity to reward
DISCUSSION
Patients with lesions in different regions of the prefron-tal cortex were tested on a probabilistic visual discrim-ination reversal test in which it was necessary both todetermine which feedback was crucial and to use thisinformation appropriately to guide the choice of stimu-lus to maximize the reward obtained It was found that
bilateral orbitalmedial prefrontal lesions produced asevere impairment on this test whereas even largeunilateral lesions which included the orbitalmedialregion had no such effect It was also found thatpatients with unilateral medial prefrontal cortex lesionswere unimpaired at this task
The pattern of results was more complicated in thedorsolateral group all of whom had unilateral lesions inthat some patients were impaired at the task whereasothers were not This was shown to be related to whetheras indicated by the posttest questionnaire the patientshad attended to the feedback necessary to succeed on thetask namely the amount won or lost on each trial Nearlyhalf of those with dorsolateral lesions explained how theyhad attended to other nonessential sources of feedbackattempting to maximize their gains in this way Those whodid attend to the essential feedback performed normallywhereas those who did not were as impaired as the groupwith bilateral orbital lesions
The pattern of impairment shown by the dorsolateralpatients who failed to attend can be contrasted withthat shown by the patients with bilateral orbitalmediallesions Although all of these patients with bilateralorbitalmedial prefrontal lesions did attend to the rele-vant feedback they were nevertheless unable to use it toadjust their behavior Instead when stimulusndashrewardcontingencies were reversed they frequently choseagain the incorrect previously rewarded stimulus afterlarge losses or failed to stick with the correct stimulusafter gaining money on it The impairment shown bypatients with bilateral orbitalmedial lesions is consistentwith the findings from our earlier study (Rolls et al1994) in which patients with bilateral ventral prefrontalcortex lesions were found to be impaired on a gono-go
Table 2 Comparisons of the Amount of Money Earned on theReversal Test
BLOFC
ULOFC
DLPFC(Att)
DLPFC(F)
BL OFC
UL OFC p = 028
DLPFC (Att) p = 045 ns
DLPFC (F) ns p = 004 p = 011
Control group p = 002 ns ns p lt 001
Group Comparisons Using MannndashWhitney Nonparametric TestsKruskalndashWallis nonparametric one-way ANOVA revealed significantgroup difference x2 = 23391 df = 4 p lt 001 BL = bilateral UL =unilateral OFC = orbito-frontal cortex DLPFC = dorsolateralprefrontal cortex Att = the patients attended to the crucial feedbackF = the patients failed to attend to the crucial feedback
Significant at p lt 05
Significant at p lt 01
Figure 2 The number ofstandard deviations by whicheach patientrsquos total earned onthe reversal test by trial 100differed from the mean won bythe normal control group BLOFC = bilateral orbito-frontalcortex UL OFC = unilateralorbito-frontal cortex MedialPFC = medial prefrontal cortexDLPFC = dorsolateral prefrontalcortex Attendedfailed toattend = the patient attendedfailed to attend to the crucialfeedback during the reversaltest namely the amount won orlost on each trial
468 Journal of Cognitive Neuroscience Volume 16 Number 3
visual discrimination reversal test However in thisprevious study the more diffuse nature of the lesions(with some produced by closed head injury althoughnevertheless with clear damage to the ventral prefrontalcortex evident in structural MRI scans) precluded pre-cise localization of this impairment to the orbito-frontalcortex In the present study by investigating patientswith surgical and thus more circumscribed lesions of thefrontal lobes we were able to demonstrate that animpairment on reversal learning can occur followingbilateral orbital excisions These results are consistentwith findings from nonhuman primates which implicatethe orbito-frontal cortex in reward and in stimulusndashreward learning and reversal (Dias et al 1996 Rolls1990 1999b 2000) as well as with the results from ourneuroimaging study using the same probabilistic reversaltask (OrsquoDoherty Kringelbach et al 2001) which pro-duced bilateral activation in the orbito-frontal cortex innormal subjects In the present study although as agroup the patients with bilateral orbital lesions weresignificantly impaired on this test only those whoselesions included the areas activated in the fMRI studyshowed a marked impairment whereas the two patientswith bilateral lesions who were not significantly impaired(VO and RR) had small lesions restricted either to theregion anterior or to the region posterior to the regionsof activation (see Figure 3A)
In the fMRI study it was found that the medial and thelateral regions of the orbito-frontal cortex were activat-ed respectively by reward and by punishment andindeed that the degree of activation in these two regionswas correlated with the amount of lsquolsquomoneyrsquorsquo gained orlost (OrsquoDoherty Kringelbach et al 2001) In the pres-ent study the patients with bilateral orbital lesions whowere impaired on the test all had lesions that encom-passed both the more medial and the more lateralregions described in the activation study and for thatreason a difference in sensitivity to reward and topunishment would not be expected in this patientgroup Consistent with this no clear pattern of greatersensitivity to punishment or to reward was observed inthose with bilateral lesions who were impaired Furtherresearch with more discrete lesions within the orbito-frontal cortex may reveal more detailed parallels withthe fMRI study perhaps with sensitivity to reward beingimpaired by medial orbito-frontal cortex lesions andsensitivity to punishment by lateral orbito-frontal cortexlesions However since a recent fMRI study found thatventrolateral activation was associated with reversallearning independently of the effects of negative feed-back (Cools Clark Owen amp Robbins 2002) the medialndashlateral distinction (within the orbital cortex) for rewardand for punishment respectively seems less likely tohold up for this kind of test
It is important that in the present study the groupwith unilateral orbital lesions on either side was unim-paired indicating that it is necessary for the orbital
damage to extend bilaterally before impairments areshown on visual discrimination reversal learning Thissuggests that either the left or the right orbito-frontalcortex on its own can carry out the functions necessaryfor normal performance It is very unlikely that lesionsize per se can explain this effect because somepatients with unilateral orbital lesions who were unim-paired had a larger total area of prefrontal cortexexcised than some of the patients with bilateral orbitallesions who were impaired This was confirmed by thefact that there was no correlation between the totallesion size (amount of prefrontal cortex excised) andperformance on the task
The design of the probabilistic reversal task meansthat two interpretations of the impairment shown bypatients with bilateral orbitalmedial lesions can beexcluded First the repeated touching of the previouslyrewarded stimulus cannot be explained in terms ofsimple motor perseveration (ie as a failure of inhibitorycontrol of the armhand with which the patients reachedout to touch the now-incorrect stimulus) Because aresponse was required and made on every trial thecontinued selection of the old S+ must reflect insteadthe patientrsquos difficulty when reinforcement contingen-cies are reversed in altering the previous associationformed between the stimulus and reward or that be-tween the stimulus and the response he should make toit Although the present study does not distinguishbetween these two interpretations the results are con-sistent with the hypothesis (Rolls 1990 1999b 20002002) that one important function of the orbito-frontalcortex consists in representing the reward and punish-ment value of stimuli and in particular since all patientssucceeded in the early stages of the task (before the firstreversal) in updating the associations between stimuliand reward or punishment value when these change
Secondly the clear instructions that explained thatreversals would occur and that subjects were to alter theirchoice of stimulus accordingly exclude an interpretationin terms of lack of initiative This might have explainedsome of the problems shown by patients in our earlierstudy (Rolls et al 1994) in which no warning was giventhat the contingencies would change The fact that clearexplanation was given about this in the present study atleast excludes an explanation in these terms Howeverwe cannot exclude the possibility that some of thepatients with dorsolateral lesions who were impaired atthe test and who failed to attend to the essential feedbackhad failed fully to understand the task requirements andif so this itself may be viewed as an aspect of executivedysfunction Interestingly among those who failed toattend to the amount won or lost on each trial somedid attend to this for some of the time but did notappreciate its importance and started to attend to othersources of feedback instead (Appendix 2B)
The difficulty in selecting the appropriate feedback orusing it in a consistent manner which was shown by
Hornak et al 469
almost half of the patients in the dorsolateral group andwhich resulted in severely impaired performance on thereversal test has parallels in work with nonhumanprimates in which dorsolateral lesions impaired theability to lsquolsquomonitor multiple stimulirsquorsquo (Petrides amp Pandya1999) as well as with neuroimaging studies of executivefunctions such as those involved in dual-task perfor-mance (Szameitat Torsten Muller amp von Cramon2002) On the posttest questionnaire the patients inthis study reported that instead of using the amountwon or lost on each trial to guide their choice of patternthey had attended instead to other nonessential sourcesof information such as the cumulative total (as anumber or as a bar chart) whether they had won orlost on each trial (ignoring the amount) or the colors orsounds that were associated with gains or losses (Wenote that the self-report provided by these patients withcircumscribed frontal lesions was sufficiently reliablethat across the group the self-report about attention tothe essential feedback was strongly related to the level ofperformance on the task Indeed there was a significant
difference between the proportions of patients whowere impaired who attended 29 and who failed toattend 78 Fisherrsquos exact test p = 02 two-tailed) It isof interest that the dorsolateral group who failed toattend or who failed to attend consistently to theessential feedback during the main reversal phase ofthe test were able to appreciate which feedback to use inthe far easier practice session of the test in which noreversals occurred A similar effect of task difficulty inrevealing impairments in patients with dorsolateral le-sions has been reported by Morris et al (2002) whofound that the ability to employ the appropriate strategyin a test of planning ability was not apparent in the earlypart of the test but became apparent only in the laterharder phase Similarly in Szameitat et alrsquos (2002) studydorsolateral prefrontal cortex activation was producedonly when the task difficulty was increased
In the present study three of the four (R C F Zand B S) whose lesions were confined to the dorso-lateral prefrontal region all failed to attend to the amountwonlost on each trial suggesting that a dorsolateral
Figure 3 Brain maps showinglesion sites Within each groupwith unilateral lesions thosewith right-sided lesions areshown first (A) Bilateral orbito-frontal cortex (or orbital plusmedial prefrontal cortex) (B)Unilateral orbito-frontal (ororbital plus medial) (C) Uni-lateral medial prefrontal cortex(D) Unilateral dorsolateralprefrontal (or dorsolateral plusmedial prefrontal) (E)Unilateral orbito-frontal plusmedial prefrontal plusdorsolateral prefrontal cortex
470 Journal of Cognitive Neuroscience Volume 16 Number 3
lesion may be sufficient to produce this cognitiveexecu-tive impairment In those cases where the dorsolaterallesions extended down into the medial region there arealso parallels with imaging studies in which the moredorsal regions of anterior cingulate described by theauthors as its cognitive division are activated in normalsubjects during tasks involving stimulusndashresponse selec-tion in the face of competing streams of information(Bush Luu amp Posner 2000) The dorsolateral prefrontalcortex lesions did in fact extend into this lsquolsquocognitivedivisionrsquorsquo region of the anterior cingulate cortex in theother five patients with dorsolateral lesions (GE GDOR AG and LK) who also failed to attend to theappropriate feedback However since other patients withcomparable lesions extending into these regions suc-ceeded in attending to this feedback this suggestionmust remain tentative It will be of interest to developour reversal task in the future to simplify the feedbackprovided in the expectation that this will make the taskperformable without deficit by patients with dorsolateralprefrontal cortex lesions but still sensitive to the effectsof lesions to the orbito-frontal cortex due to the reversalcomponent of the task
The findings reported in this study suggest that theprobabilistic reversal test makes demands on differentfunctions attributed respectively to the dorsolateraland to the orbital regions of the prefrontal cortex (cfBechara et al 1998 who reported a study in whichlesions in these regions had dissociable effects ondecision making and on working memory) Thus inthe present study the need to determine which ofmultiple competing sources of feedback should beattended to to maintain attention to this throughoutthe test ignoring other visually salient but noncrucialtypes of feedback (flashing lights total sum displayedcolored bar charts etc) are among the many functionsthat have been attributed to the dorsolateral prefrontalcortex (Szameitat et al 2002 Duncan amp Owen 2000)For a subject who is capable of attending consistently tothe appropriate feedback it is also necessary to use theinformation about the current level of reward associatedwith each pattern to guide his choice on each trial andas such the test also makes demands on functionsattributed to the orbito-frontal cortex (Rolls 19901999a 1999b 2000) The results of the present studyshow that it is possible to be severely impaired on thisprobabilistic visual discrimination reversal test for eitherof these two reasons and in the context that perfor-mance on the test can be independently disrupted bythe effects of dorsolateral and of orbital lesions we haveshown a dissociation between the effects of lesions inthese two regions The ability to attend to the crucialfeedback can be disrupted by a dorsolateral lesion oneither side whereas the ability to use this information tochoose advantageously can be supported by eitherorbital region on its own (after a unilateral orbitallesion) but is abolished by a bilateral orbital lesion
These results are consistent with the view that whereasthe dorsolateral frontal cortex forms part of a network ofprefrontal regions recruited to solve diverse cognitiveproblems especially those with an lsquolsquoexecutiversquorsquo compo-nent (in this case appreciating which feedback is rele-vantimportant) (Bush et al 2000 Duncan amp Owen2000) the orbito-frontal cortex is involved in the repre-sentation of the changing reward value of stimuli (Rolls1990 1999b 2000 2002) so that behavior can be mod-ified accordingly As such the present study contributesboth to our understanding of the different functions ofthese two regions of frontal lobe and to how theseregions need to cooperate on complex tasks such as theone used here A similar argument is made by Manes et al(2002) who showed how the ventral and dorsal aspects ofthe prefrontal cortex must interact in the maintenance ofrational and lsquolsquononriskyrsquorsquo decision-making tasks
One of the underlying hypotheses of the researchdescribed here is that some of the reasons for thebehavioral and emotional changes that follow damageto the prefrontal cortex may be related to deficits indecoding the reward and punishment value of stimuliand using the results of the decoding to modify behaviorand the ongoing emotional or mood state (Rolls 19901999a 1999b Rolls et al 1994) In this context it is ofinterest that the patients with bilateral orbito-frontalcortex damage who were impaired at the visual discrim-ination reversal task (see Table 1) had high scores onparts of a social behavior questionnaire in which thepatients were rated on behaviors such as the recognitionof emotion in others (eg their sad angry or disgustedmood) in interpersonal relationships (such as not caringwhat others think and not being close to the family) insociability (is not sociable and has difficulty making ormaintaining close relationships) emotional empathy(eg when others are happy is not happy for them)public behavior (is uncooperative) antisocial behavior (iscritical of and impatient with others) and impulsivity(does things without thinking) (Hornak Bramham RollsMorris OrsquoDoherty amp Polkey 2003) all of which couldreflect less behavioral sensitivity to different types ofpunishment and reward Further in a subjective emo-tional change questionnaire in which the patients re-ported on any changes in the intensity andor frequencyof their own experience of emotions since surgery thebilateral orbito-frontal cortex patients with deficits in thevisual discrimination reversal task reported a number ofchanges including changes in sadness anger fear andhappiness and were as a group significantly different inthese respects from the dorsolateral prefrontal cortexlesion group included in that comparison (Hornak et al2003) However it must also be pointed out that thepatients with unilateral orbito-frontalanterior cingulatelesions (the BA 9ACC and BA 9ACC + orbital groups ofthat article) also reported marked emotional changes andthey were also less well-adjusted socially than the dorso-lateral group but had no measured deficit in reversal The
Hornak et al 471
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
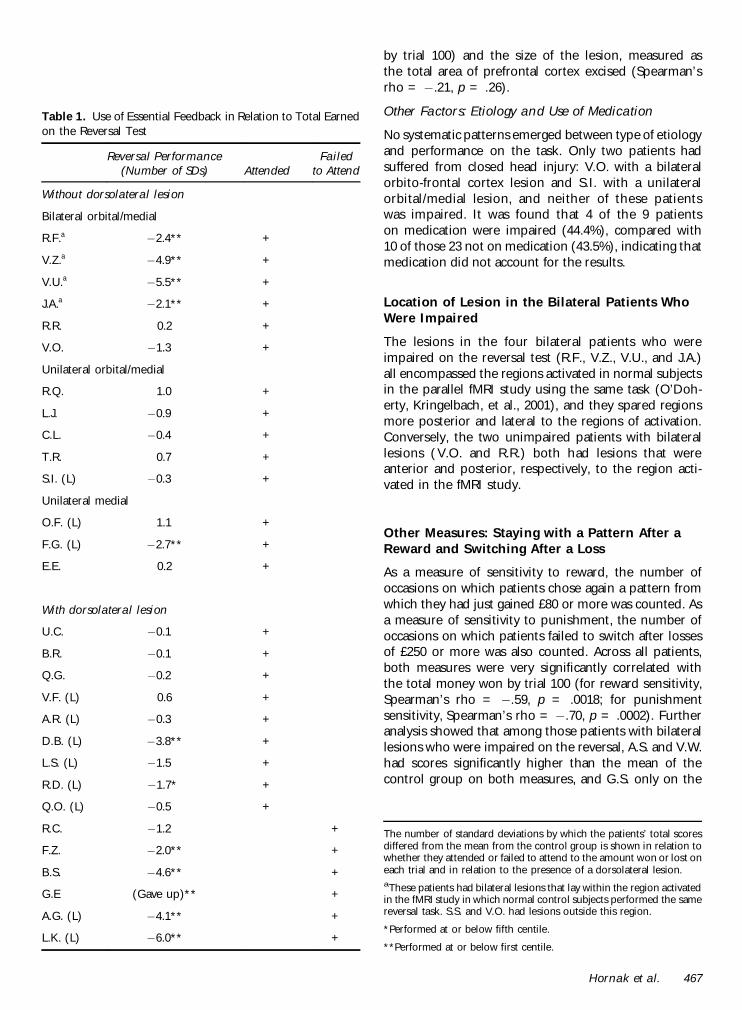
by trial 100) and the size of the lesion measured asthe total area of prefrontal cortex excised (Spearmanrsquosrho = iexcl21 p = 26)
Other Factors Etiology and Use of Medication
No systematic patterns emerged between type of etiologyand performance on the task Only two patients hadsuffered from closed head injury VO with a bilateralorbito-frontal cortex lesion and SI with a unilateralorbitalmedial lesion and neither of these patientswas impaired It was found that 4 of the 9 patientson medication were impaired (444) compared with10 of those 23 not on medication (435) indicating thatmedication did not account for the results
Location of Lesion in the Bilateral Patients WhoWere Impaired
The lesions in the four bilateral patients who wereimpaired on the reversal test (RF VZ VU and JA)all encompassed the regions activated in normal subjectsin the parallel fMRI study using the same task (OrsquoDoh-erty Kringelbach et al 2001) and they spared regionsmore posterior and lateral to the regions of activationConversely the two unimpaired patients with bilaterallesions (VO and RR) both had lesions that wereanterior and posterior respectively to the region acti-vated in the fMRI study
Other Measures Staying with a Pattern After aReward and Switching After a Loss
As a measure of sensitivity to reward the number ofoccasions on which patients chose again a pattern fromwhich they had just gained pound80 or more was counted Asa measure of sensitivity to punishment the number ofoccasions on which patients failed to switch after lossesof pound250 or more was also counted Across all patientsboth measures were very significantly correlated withthe total money won by trial 100 (for reward sensitivitySpearmanrsquos rho = iexcl59 p = 0018 for punishmentsensitivity Spearmanrsquos rho = iexcl70 p = 0002) Furtheranalysis showed that among those patients with bilaterallesions who were impaired on the reversal AS and VWhad scores significantly higher than the mean of thecontrol group on both measures and GS only on the
Table 1 Use of Essential Feedback in Relation to Total Earnedon the Reversal Test
Reversal Performance(Number of SDs) Attended
Failedto Attend
Without dorsolateral lesion
Bilateral orbitalmedial
RFa iexcl24 +
VZa iexcl49 +
VUa iexcl55 +
JAa iexcl21 +
RR 02 +
VO iexcl13 +
Unilateral orbitalmedial
RQ 10 +
LJ iexcl09 +
CL iexcl04 +
TR 07 +
SI (L) iexcl03 +
Unilateral medial
OF (L) 11 +
FG (L) iexcl27 +
EE 02 +
With dorsolateral lesion
UC iexcl01 +
BR iexcl01 +
QG iexcl02 +
VF (L) 06 +
AR (L) iexcl03 +
DB (L) iexcl38 +
LS (L) iexcl15 +
RD (L) iexcl17 +
QO (L) iexcl05 +
RC iexcl12 +
FZ iexcl20 +
BS iexcl46 +
GE (Gave up) +
AG (L) iexcl41 +
LK (L) iexcl60 +
The number of standard deviations by which the patientsrsquo total scoresdiffered from the mean from the control group is shown in relation towhether they attended or failed to attend to the amount won or lost oneach trial and in relation to the presence of a dorsolateral lesionaThese patients had bilateral lesions that lay within the region activatedin the fMRI study in which normal control subjects performed the samereversal task SS and VO had lesions outside this region
Performed at or below fifth centile
Performed at or below first centile
Hornak et al 467
sensitivity to reward measure BK did not have signif-icantly higher scores on either measure but she mademore responses revealing insensitivity to punishmentthan responses revealing insensitivity to reward
DISCUSSION
Patients with lesions in different regions of the prefron-tal cortex were tested on a probabilistic visual discrim-ination reversal test in which it was necessary both todetermine which feedback was crucial and to use thisinformation appropriately to guide the choice of stimu-lus to maximize the reward obtained It was found that
bilateral orbitalmedial prefrontal lesions produced asevere impairment on this test whereas even largeunilateral lesions which included the orbitalmedialregion had no such effect It was also found thatpatients with unilateral medial prefrontal cortex lesionswere unimpaired at this task
The pattern of results was more complicated in thedorsolateral group all of whom had unilateral lesions inthat some patients were impaired at the task whereasothers were not This was shown to be related to whetheras indicated by the posttest questionnaire the patientshad attended to the feedback necessary to succeed on thetask namely the amount won or lost on each trial Nearlyhalf of those with dorsolateral lesions explained how theyhad attended to other nonessential sources of feedbackattempting to maximize their gains in this way Those whodid attend to the essential feedback performed normallywhereas those who did not were as impaired as the groupwith bilateral orbital lesions
The pattern of impairment shown by the dorsolateralpatients who failed to attend can be contrasted withthat shown by the patients with bilateral orbitalmediallesions Although all of these patients with bilateralorbitalmedial prefrontal lesions did attend to the rele-vant feedback they were nevertheless unable to use it toadjust their behavior Instead when stimulusndashrewardcontingencies were reversed they frequently choseagain the incorrect previously rewarded stimulus afterlarge losses or failed to stick with the correct stimulusafter gaining money on it The impairment shown bypatients with bilateral orbitalmedial lesions is consistentwith the findings from our earlier study (Rolls et al1994) in which patients with bilateral ventral prefrontalcortex lesions were found to be impaired on a gono-go
Table 2 Comparisons of the Amount of Money Earned on theReversal Test
BLOFC
ULOFC
DLPFC(Att)
DLPFC(F)
BL OFC
UL OFC p = 028
DLPFC (Att) p = 045 ns
DLPFC (F) ns p = 004 p = 011
Control group p = 002 ns ns p lt 001
Group Comparisons Using MannndashWhitney Nonparametric TestsKruskalndashWallis nonparametric one-way ANOVA revealed significantgroup difference x2 = 23391 df = 4 p lt 001 BL = bilateral UL =unilateral OFC = orbito-frontal cortex DLPFC = dorsolateralprefrontal cortex Att = the patients attended to the crucial feedbackF = the patients failed to attend to the crucial feedback
Significant at p lt 05
Significant at p lt 01
Figure 2 The number ofstandard deviations by whicheach patientrsquos total earned onthe reversal test by trial 100differed from the mean won bythe normal control group BLOFC = bilateral orbito-frontalcortex UL OFC = unilateralorbito-frontal cortex MedialPFC = medial prefrontal cortexDLPFC = dorsolateral prefrontalcortex Attendedfailed toattend = the patient attendedfailed to attend to the crucialfeedback during the reversaltest namely the amount won orlost on each trial
468 Journal of Cognitive Neuroscience Volume 16 Number 3
visual discrimination reversal test However in thisprevious study the more diffuse nature of the lesions(with some produced by closed head injury althoughnevertheless with clear damage to the ventral prefrontalcortex evident in structural MRI scans) precluded pre-cise localization of this impairment to the orbito-frontalcortex In the present study by investigating patientswith surgical and thus more circumscribed lesions of thefrontal lobes we were able to demonstrate that animpairment on reversal learning can occur followingbilateral orbital excisions These results are consistentwith findings from nonhuman primates which implicatethe orbito-frontal cortex in reward and in stimulusndashreward learning and reversal (Dias et al 1996 Rolls1990 1999b 2000) as well as with the results from ourneuroimaging study using the same probabilistic reversaltask (OrsquoDoherty Kringelbach et al 2001) which pro-duced bilateral activation in the orbito-frontal cortex innormal subjects In the present study although as agroup the patients with bilateral orbital lesions weresignificantly impaired on this test only those whoselesions included the areas activated in the fMRI studyshowed a marked impairment whereas the two patientswith bilateral lesions who were not significantly impaired(VO and RR) had small lesions restricted either to theregion anterior or to the region posterior to the regionsof activation (see Figure 3A)
In the fMRI study it was found that the medial and thelateral regions of the orbito-frontal cortex were activat-ed respectively by reward and by punishment andindeed that the degree of activation in these two regionswas correlated with the amount of lsquolsquomoneyrsquorsquo gained orlost (OrsquoDoherty Kringelbach et al 2001) In the pres-ent study the patients with bilateral orbital lesions whowere impaired on the test all had lesions that encom-passed both the more medial and the more lateralregions described in the activation study and for thatreason a difference in sensitivity to reward and topunishment would not be expected in this patientgroup Consistent with this no clear pattern of greatersensitivity to punishment or to reward was observed inthose with bilateral lesions who were impaired Furtherresearch with more discrete lesions within the orbito-frontal cortex may reveal more detailed parallels withthe fMRI study perhaps with sensitivity to reward beingimpaired by medial orbito-frontal cortex lesions andsensitivity to punishment by lateral orbito-frontal cortexlesions However since a recent fMRI study found thatventrolateral activation was associated with reversallearning independently of the effects of negative feed-back (Cools Clark Owen amp Robbins 2002) the medialndashlateral distinction (within the orbital cortex) for rewardand for punishment respectively seems less likely tohold up for this kind of test
It is important that in the present study the groupwith unilateral orbital lesions on either side was unim-paired indicating that it is necessary for the orbital
damage to extend bilaterally before impairments areshown on visual discrimination reversal learning Thissuggests that either the left or the right orbito-frontalcortex on its own can carry out the functions necessaryfor normal performance It is very unlikely that lesionsize per se can explain this effect because somepatients with unilateral orbital lesions who were unim-paired had a larger total area of prefrontal cortexexcised than some of the patients with bilateral orbitallesions who were impaired This was confirmed by thefact that there was no correlation between the totallesion size (amount of prefrontal cortex excised) andperformance on the task
The design of the probabilistic reversal task meansthat two interpretations of the impairment shown bypatients with bilateral orbitalmedial lesions can beexcluded First the repeated touching of the previouslyrewarded stimulus cannot be explained in terms ofsimple motor perseveration (ie as a failure of inhibitorycontrol of the armhand with which the patients reachedout to touch the now-incorrect stimulus) Because aresponse was required and made on every trial thecontinued selection of the old S+ must reflect insteadthe patientrsquos difficulty when reinforcement contingen-cies are reversed in altering the previous associationformed between the stimulus and reward or that be-tween the stimulus and the response he should make toit Although the present study does not distinguishbetween these two interpretations the results are con-sistent with the hypothesis (Rolls 1990 1999b 20002002) that one important function of the orbito-frontalcortex consists in representing the reward and punish-ment value of stimuli and in particular since all patientssucceeded in the early stages of the task (before the firstreversal) in updating the associations between stimuliand reward or punishment value when these change
Secondly the clear instructions that explained thatreversals would occur and that subjects were to alter theirchoice of stimulus accordingly exclude an interpretationin terms of lack of initiative This might have explainedsome of the problems shown by patients in our earlierstudy (Rolls et al 1994) in which no warning was giventhat the contingencies would change The fact that clearexplanation was given about this in the present study atleast excludes an explanation in these terms Howeverwe cannot exclude the possibility that some of thepatients with dorsolateral lesions who were impaired atthe test and who failed to attend to the essential feedbackhad failed fully to understand the task requirements andif so this itself may be viewed as an aspect of executivedysfunction Interestingly among those who failed toattend to the amount won or lost on each trial somedid attend to this for some of the time but did notappreciate its importance and started to attend to othersources of feedback instead (Appendix 2B)
The difficulty in selecting the appropriate feedback orusing it in a consistent manner which was shown by
Hornak et al 469
almost half of the patients in the dorsolateral group andwhich resulted in severely impaired performance on thereversal test has parallels in work with nonhumanprimates in which dorsolateral lesions impaired theability to lsquolsquomonitor multiple stimulirsquorsquo (Petrides amp Pandya1999) as well as with neuroimaging studies of executivefunctions such as those involved in dual-task perfor-mance (Szameitat Torsten Muller amp von Cramon2002) On the posttest questionnaire the patients inthis study reported that instead of using the amountwon or lost on each trial to guide their choice of patternthey had attended instead to other nonessential sourcesof information such as the cumulative total (as anumber or as a bar chart) whether they had won orlost on each trial (ignoring the amount) or the colors orsounds that were associated with gains or losses (Wenote that the self-report provided by these patients withcircumscribed frontal lesions was sufficiently reliablethat across the group the self-report about attention tothe essential feedback was strongly related to the level ofperformance on the task Indeed there was a significant
difference between the proportions of patients whowere impaired who attended 29 and who failed toattend 78 Fisherrsquos exact test p = 02 two-tailed) It isof interest that the dorsolateral group who failed toattend or who failed to attend consistently to theessential feedback during the main reversal phase ofthe test were able to appreciate which feedback to use inthe far easier practice session of the test in which noreversals occurred A similar effect of task difficulty inrevealing impairments in patients with dorsolateral le-sions has been reported by Morris et al (2002) whofound that the ability to employ the appropriate strategyin a test of planning ability was not apparent in the earlypart of the test but became apparent only in the laterharder phase Similarly in Szameitat et alrsquos (2002) studydorsolateral prefrontal cortex activation was producedonly when the task difficulty was increased
In the present study three of the four (R C F Zand B S) whose lesions were confined to the dorso-lateral prefrontal region all failed to attend to the amountwonlost on each trial suggesting that a dorsolateral
Figure 3 Brain maps showinglesion sites Within each groupwith unilateral lesions thosewith right-sided lesions areshown first (A) Bilateral orbito-frontal cortex (or orbital plusmedial prefrontal cortex) (B)Unilateral orbito-frontal (ororbital plus medial) (C) Uni-lateral medial prefrontal cortex(D) Unilateral dorsolateralprefrontal (or dorsolateral plusmedial prefrontal) (E)Unilateral orbito-frontal plusmedial prefrontal plusdorsolateral prefrontal cortex
470 Journal of Cognitive Neuroscience Volume 16 Number 3
lesion may be sufficient to produce this cognitiveexecu-tive impairment In those cases where the dorsolaterallesions extended down into the medial region there arealso parallels with imaging studies in which the moredorsal regions of anterior cingulate described by theauthors as its cognitive division are activated in normalsubjects during tasks involving stimulusndashresponse selec-tion in the face of competing streams of information(Bush Luu amp Posner 2000) The dorsolateral prefrontalcortex lesions did in fact extend into this lsquolsquocognitivedivisionrsquorsquo region of the anterior cingulate cortex in theother five patients with dorsolateral lesions (GE GDOR AG and LK) who also failed to attend to theappropriate feedback However since other patients withcomparable lesions extending into these regions suc-ceeded in attending to this feedback this suggestionmust remain tentative It will be of interest to developour reversal task in the future to simplify the feedbackprovided in the expectation that this will make the taskperformable without deficit by patients with dorsolateralprefrontal cortex lesions but still sensitive to the effectsof lesions to the orbito-frontal cortex due to the reversalcomponent of the task
The findings reported in this study suggest that theprobabilistic reversal test makes demands on differentfunctions attributed respectively to the dorsolateraland to the orbital regions of the prefrontal cortex (cfBechara et al 1998 who reported a study in whichlesions in these regions had dissociable effects ondecision making and on working memory) Thus inthe present study the need to determine which ofmultiple competing sources of feedback should beattended to to maintain attention to this throughoutthe test ignoring other visually salient but noncrucialtypes of feedback (flashing lights total sum displayedcolored bar charts etc) are among the many functionsthat have been attributed to the dorsolateral prefrontalcortex (Szameitat et al 2002 Duncan amp Owen 2000)For a subject who is capable of attending consistently tothe appropriate feedback it is also necessary to use theinformation about the current level of reward associatedwith each pattern to guide his choice on each trial andas such the test also makes demands on functionsattributed to the orbito-frontal cortex (Rolls 19901999a 1999b 2000) The results of the present studyshow that it is possible to be severely impaired on thisprobabilistic visual discrimination reversal test for eitherof these two reasons and in the context that perfor-mance on the test can be independently disrupted bythe effects of dorsolateral and of orbital lesions we haveshown a dissociation between the effects of lesions inthese two regions The ability to attend to the crucialfeedback can be disrupted by a dorsolateral lesion oneither side whereas the ability to use this information tochoose advantageously can be supported by eitherorbital region on its own (after a unilateral orbitallesion) but is abolished by a bilateral orbital lesion
These results are consistent with the view that whereasthe dorsolateral frontal cortex forms part of a network ofprefrontal regions recruited to solve diverse cognitiveproblems especially those with an lsquolsquoexecutiversquorsquo compo-nent (in this case appreciating which feedback is rele-vantimportant) (Bush et al 2000 Duncan amp Owen2000) the orbito-frontal cortex is involved in the repre-sentation of the changing reward value of stimuli (Rolls1990 1999b 2000 2002) so that behavior can be mod-ified accordingly As such the present study contributesboth to our understanding of the different functions ofthese two regions of frontal lobe and to how theseregions need to cooperate on complex tasks such as theone used here A similar argument is made by Manes et al(2002) who showed how the ventral and dorsal aspects ofthe prefrontal cortex must interact in the maintenance ofrational and lsquolsquononriskyrsquorsquo decision-making tasks
One of the underlying hypotheses of the researchdescribed here is that some of the reasons for thebehavioral and emotional changes that follow damageto the prefrontal cortex may be related to deficits indecoding the reward and punishment value of stimuliand using the results of the decoding to modify behaviorand the ongoing emotional or mood state (Rolls 19901999a 1999b Rolls et al 1994) In this context it is ofinterest that the patients with bilateral orbito-frontalcortex damage who were impaired at the visual discrim-ination reversal task (see Table 1) had high scores onparts of a social behavior questionnaire in which thepatients were rated on behaviors such as the recognitionof emotion in others (eg their sad angry or disgustedmood) in interpersonal relationships (such as not caringwhat others think and not being close to the family) insociability (is not sociable and has difficulty making ormaintaining close relationships) emotional empathy(eg when others are happy is not happy for them)public behavior (is uncooperative) antisocial behavior (iscritical of and impatient with others) and impulsivity(does things without thinking) (Hornak Bramham RollsMorris OrsquoDoherty amp Polkey 2003) all of which couldreflect less behavioral sensitivity to different types ofpunishment and reward Further in a subjective emo-tional change questionnaire in which the patients re-ported on any changes in the intensity andor frequencyof their own experience of emotions since surgery thebilateral orbito-frontal cortex patients with deficits in thevisual discrimination reversal task reported a number ofchanges including changes in sadness anger fear andhappiness and were as a group significantly different inthese respects from the dorsolateral prefrontal cortexlesion group included in that comparison (Hornak et al2003) However it must also be pointed out that thepatients with unilateral orbito-frontalanterior cingulatelesions (the BA 9ACC and BA 9ACC + orbital groups ofthat article) also reported marked emotional changes andthey were also less well-adjusted socially than the dorso-lateral group but had no measured deficit in reversal The
Hornak et al 471
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
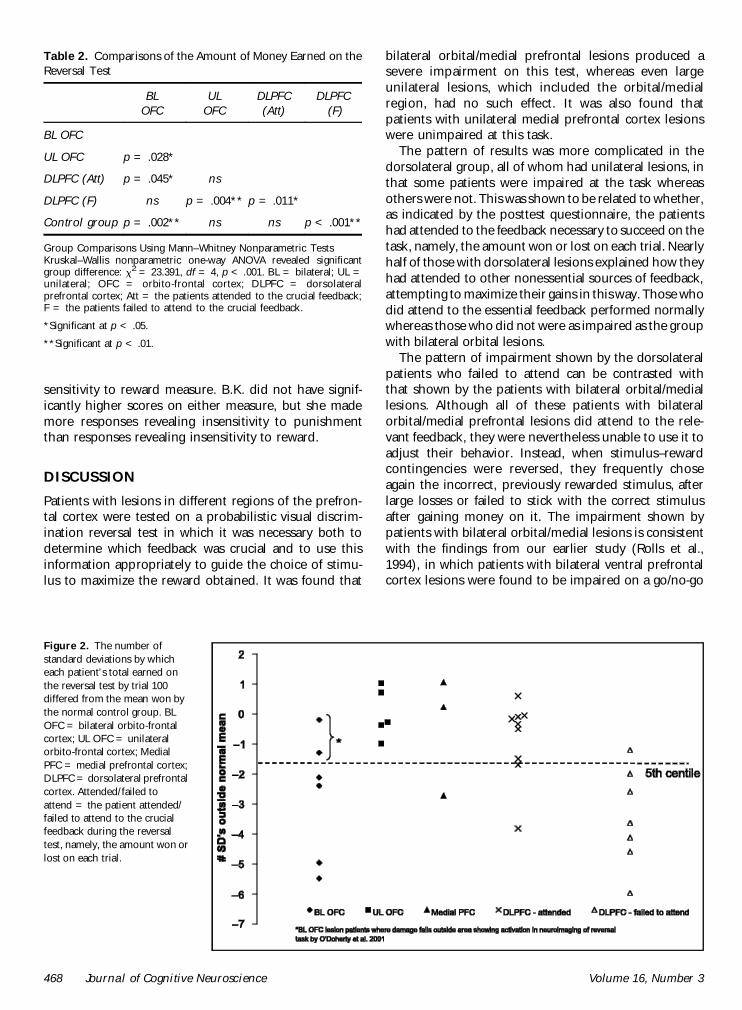
sensitivity to reward measure BK did not have signif-icantly higher scores on either measure but she mademore responses revealing insensitivity to punishmentthan responses revealing insensitivity to reward
DISCUSSION
Patients with lesions in different regions of the prefron-tal cortex were tested on a probabilistic visual discrim-ination reversal test in which it was necessary both todetermine which feedback was crucial and to use thisinformation appropriately to guide the choice of stimu-lus to maximize the reward obtained It was found that
bilateral orbitalmedial prefrontal lesions produced asevere impairment on this test whereas even largeunilateral lesions which included the orbitalmedialregion had no such effect It was also found thatpatients with unilateral medial prefrontal cortex lesionswere unimpaired at this task
The pattern of results was more complicated in thedorsolateral group all of whom had unilateral lesions inthat some patients were impaired at the task whereasothers were not This was shown to be related to whetheras indicated by the posttest questionnaire the patientshad attended to the feedback necessary to succeed on thetask namely the amount won or lost on each trial Nearlyhalf of those with dorsolateral lesions explained how theyhad attended to other nonessential sources of feedbackattempting to maximize their gains in this way Those whodid attend to the essential feedback performed normallywhereas those who did not were as impaired as the groupwith bilateral orbital lesions
The pattern of impairment shown by the dorsolateralpatients who failed to attend can be contrasted withthat shown by the patients with bilateral orbitalmediallesions Although all of these patients with bilateralorbitalmedial prefrontal lesions did attend to the rele-vant feedback they were nevertheless unable to use it toadjust their behavior Instead when stimulusndashrewardcontingencies were reversed they frequently choseagain the incorrect previously rewarded stimulus afterlarge losses or failed to stick with the correct stimulusafter gaining money on it The impairment shown bypatients with bilateral orbitalmedial lesions is consistentwith the findings from our earlier study (Rolls et al1994) in which patients with bilateral ventral prefrontalcortex lesions were found to be impaired on a gono-go
Table 2 Comparisons of the Amount of Money Earned on theReversal Test
BLOFC
ULOFC
DLPFC(Att)
DLPFC(F)
BL OFC
UL OFC p = 028
DLPFC (Att) p = 045 ns
DLPFC (F) ns p = 004 p = 011
Control group p = 002 ns ns p lt 001
Group Comparisons Using MannndashWhitney Nonparametric TestsKruskalndashWallis nonparametric one-way ANOVA revealed significantgroup difference x2 = 23391 df = 4 p lt 001 BL = bilateral UL =unilateral OFC = orbito-frontal cortex DLPFC = dorsolateralprefrontal cortex Att = the patients attended to the crucial feedbackF = the patients failed to attend to the crucial feedback
Significant at p lt 05
Significant at p lt 01
Figure 2 The number ofstandard deviations by whicheach patientrsquos total earned onthe reversal test by trial 100differed from the mean won bythe normal control group BLOFC = bilateral orbito-frontalcortex UL OFC = unilateralorbito-frontal cortex MedialPFC = medial prefrontal cortexDLPFC = dorsolateral prefrontalcortex Attendedfailed toattend = the patient attendedfailed to attend to the crucialfeedback during the reversaltest namely the amount won orlost on each trial
468 Journal of Cognitive Neuroscience Volume 16 Number 3
visual discrimination reversal test However in thisprevious study the more diffuse nature of the lesions(with some produced by closed head injury althoughnevertheless with clear damage to the ventral prefrontalcortex evident in structural MRI scans) precluded pre-cise localization of this impairment to the orbito-frontalcortex In the present study by investigating patientswith surgical and thus more circumscribed lesions of thefrontal lobes we were able to demonstrate that animpairment on reversal learning can occur followingbilateral orbital excisions These results are consistentwith findings from nonhuman primates which implicatethe orbito-frontal cortex in reward and in stimulusndashreward learning and reversal (Dias et al 1996 Rolls1990 1999b 2000) as well as with the results from ourneuroimaging study using the same probabilistic reversaltask (OrsquoDoherty Kringelbach et al 2001) which pro-duced bilateral activation in the orbito-frontal cortex innormal subjects In the present study although as agroup the patients with bilateral orbital lesions weresignificantly impaired on this test only those whoselesions included the areas activated in the fMRI studyshowed a marked impairment whereas the two patientswith bilateral lesions who were not significantly impaired(VO and RR) had small lesions restricted either to theregion anterior or to the region posterior to the regionsof activation (see Figure 3A)
In the fMRI study it was found that the medial and thelateral regions of the orbito-frontal cortex were activat-ed respectively by reward and by punishment andindeed that the degree of activation in these two regionswas correlated with the amount of lsquolsquomoneyrsquorsquo gained orlost (OrsquoDoherty Kringelbach et al 2001) In the pres-ent study the patients with bilateral orbital lesions whowere impaired on the test all had lesions that encom-passed both the more medial and the more lateralregions described in the activation study and for thatreason a difference in sensitivity to reward and topunishment would not be expected in this patientgroup Consistent with this no clear pattern of greatersensitivity to punishment or to reward was observed inthose with bilateral lesions who were impaired Furtherresearch with more discrete lesions within the orbito-frontal cortex may reveal more detailed parallels withthe fMRI study perhaps with sensitivity to reward beingimpaired by medial orbito-frontal cortex lesions andsensitivity to punishment by lateral orbito-frontal cortexlesions However since a recent fMRI study found thatventrolateral activation was associated with reversallearning independently of the effects of negative feed-back (Cools Clark Owen amp Robbins 2002) the medialndashlateral distinction (within the orbital cortex) for rewardand for punishment respectively seems less likely tohold up for this kind of test
It is important that in the present study the groupwith unilateral orbital lesions on either side was unim-paired indicating that it is necessary for the orbital
damage to extend bilaterally before impairments areshown on visual discrimination reversal learning Thissuggests that either the left or the right orbito-frontalcortex on its own can carry out the functions necessaryfor normal performance It is very unlikely that lesionsize per se can explain this effect because somepatients with unilateral orbital lesions who were unim-paired had a larger total area of prefrontal cortexexcised than some of the patients with bilateral orbitallesions who were impaired This was confirmed by thefact that there was no correlation between the totallesion size (amount of prefrontal cortex excised) andperformance on the task
The design of the probabilistic reversal task meansthat two interpretations of the impairment shown bypatients with bilateral orbitalmedial lesions can beexcluded First the repeated touching of the previouslyrewarded stimulus cannot be explained in terms ofsimple motor perseveration (ie as a failure of inhibitorycontrol of the armhand with which the patients reachedout to touch the now-incorrect stimulus) Because aresponse was required and made on every trial thecontinued selection of the old S+ must reflect insteadthe patientrsquos difficulty when reinforcement contingen-cies are reversed in altering the previous associationformed between the stimulus and reward or that be-tween the stimulus and the response he should make toit Although the present study does not distinguishbetween these two interpretations the results are con-sistent with the hypothesis (Rolls 1990 1999b 20002002) that one important function of the orbito-frontalcortex consists in representing the reward and punish-ment value of stimuli and in particular since all patientssucceeded in the early stages of the task (before the firstreversal) in updating the associations between stimuliand reward or punishment value when these change
Secondly the clear instructions that explained thatreversals would occur and that subjects were to alter theirchoice of stimulus accordingly exclude an interpretationin terms of lack of initiative This might have explainedsome of the problems shown by patients in our earlierstudy (Rolls et al 1994) in which no warning was giventhat the contingencies would change The fact that clearexplanation was given about this in the present study atleast excludes an explanation in these terms Howeverwe cannot exclude the possibility that some of thepatients with dorsolateral lesions who were impaired atthe test and who failed to attend to the essential feedbackhad failed fully to understand the task requirements andif so this itself may be viewed as an aspect of executivedysfunction Interestingly among those who failed toattend to the amount won or lost on each trial somedid attend to this for some of the time but did notappreciate its importance and started to attend to othersources of feedback instead (Appendix 2B)
The difficulty in selecting the appropriate feedback orusing it in a consistent manner which was shown by
Hornak et al 469
almost half of the patients in the dorsolateral group andwhich resulted in severely impaired performance on thereversal test has parallels in work with nonhumanprimates in which dorsolateral lesions impaired theability to lsquolsquomonitor multiple stimulirsquorsquo (Petrides amp Pandya1999) as well as with neuroimaging studies of executivefunctions such as those involved in dual-task perfor-mance (Szameitat Torsten Muller amp von Cramon2002) On the posttest questionnaire the patients inthis study reported that instead of using the amountwon or lost on each trial to guide their choice of patternthey had attended instead to other nonessential sourcesof information such as the cumulative total (as anumber or as a bar chart) whether they had won orlost on each trial (ignoring the amount) or the colors orsounds that were associated with gains or losses (Wenote that the self-report provided by these patients withcircumscribed frontal lesions was sufficiently reliablethat across the group the self-report about attention tothe essential feedback was strongly related to the level ofperformance on the task Indeed there was a significant
difference between the proportions of patients whowere impaired who attended 29 and who failed toattend 78 Fisherrsquos exact test p = 02 two-tailed) It isof interest that the dorsolateral group who failed toattend or who failed to attend consistently to theessential feedback during the main reversal phase ofthe test were able to appreciate which feedback to use inthe far easier practice session of the test in which noreversals occurred A similar effect of task difficulty inrevealing impairments in patients with dorsolateral le-sions has been reported by Morris et al (2002) whofound that the ability to employ the appropriate strategyin a test of planning ability was not apparent in the earlypart of the test but became apparent only in the laterharder phase Similarly in Szameitat et alrsquos (2002) studydorsolateral prefrontal cortex activation was producedonly when the task difficulty was increased
In the present study three of the four (R C F Zand B S) whose lesions were confined to the dorso-lateral prefrontal region all failed to attend to the amountwonlost on each trial suggesting that a dorsolateral
Figure 3 Brain maps showinglesion sites Within each groupwith unilateral lesions thosewith right-sided lesions areshown first (A) Bilateral orbito-frontal cortex (or orbital plusmedial prefrontal cortex) (B)Unilateral orbito-frontal (ororbital plus medial) (C) Uni-lateral medial prefrontal cortex(D) Unilateral dorsolateralprefrontal (or dorsolateral plusmedial prefrontal) (E)Unilateral orbito-frontal plusmedial prefrontal plusdorsolateral prefrontal cortex
470 Journal of Cognitive Neuroscience Volume 16 Number 3
lesion may be sufficient to produce this cognitiveexecu-tive impairment In those cases where the dorsolaterallesions extended down into the medial region there arealso parallels with imaging studies in which the moredorsal regions of anterior cingulate described by theauthors as its cognitive division are activated in normalsubjects during tasks involving stimulusndashresponse selec-tion in the face of competing streams of information(Bush Luu amp Posner 2000) The dorsolateral prefrontalcortex lesions did in fact extend into this lsquolsquocognitivedivisionrsquorsquo region of the anterior cingulate cortex in theother five patients with dorsolateral lesions (GE GDOR AG and LK) who also failed to attend to theappropriate feedback However since other patients withcomparable lesions extending into these regions suc-ceeded in attending to this feedback this suggestionmust remain tentative It will be of interest to developour reversal task in the future to simplify the feedbackprovided in the expectation that this will make the taskperformable without deficit by patients with dorsolateralprefrontal cortex lesions but still sensitive to the effectsof lesions to the orbito-frontal cortex due to the reversalcomponent of the task
The findings reported in this study suggest that theprobabilistic reversal test makes demands on differentfunctions attributed respectively to the dorsolateraland to the orbital regions of the prefrontal cortex (cfBechara et al 1998 who reported a study in whichlesions in these regions had dissociable effects ondecision making and on working memory) Thus inthe present study the need to determine which ofmultiple competing sources of feedback should beattended to to maintain attention to this throughoutthe test ignoring other visually salient but noncrucialtypes of feedback (flashing lights total sum displayedcolored bar charts etc) are among the many functionsthat have been attributed to the dorsolateral prefrontalcortex (Szameitat et al 2002 Duncan amp Owen 2000)For a subject who is capable of attending consistently tothe appropriate feedback it is also necessary to use theinformation about the current level of reward associatedwith each pattern to guide his choice on each trial andas such the test also makes demands on functionsattributed to the orbito-frontal cortex (Rolls 19901999a 1999b 2000) The results of the present studyshow that it is possible to be severely impaired on thisprobabilistic visual discrimination reversal test for eitherof these two reasons and in the context that perfor-mance on the test can be independently disrupted bythe effects of dorsolateral and of orbital lesions we haveshown a dissociation between the effects of lesions inthese two regions The ability to attend to the crucialfeedback can be disrupted by a dorsolateral lesion oneither side whereas the ability to use this information tochoose advantageously can be supported by eitherorbital region on its own (after a unilateral orbitallesion) but is abolished by a bilateral orbital lesion
These results are consistent with the view that whereasthe dorsolateral frontal cortex forms part of a network ofprefrontal regions recruited to solve diverse cognitiveproblems especially those with an lsquolsquoexecutiversquorsquo compo-nent (in this case appreciating which feedback is rele-vantimportant) (Bush et al 2000 Duncan amp Owen2000) the orbito-frontal cortex is involved in the repre-sentation of the changing reward value of stimuli (Rolls1990 1999b 2000 2002) so that behavior can be mod-ified accordingly As such the present study contributesboth to our understanding of the different functions ofthese two regions of frontal lobe and to how theseregions need to cooperate on complex tasks such as theone used here A similar argument is made by Manes et al(2002) who showed how the ventral and dorsal aspects ofthe prefrontal cortex must interact in the maintenance ofrational and lsquolsquononriskyrsquorsquo decision-making tasks
One of the underlying hypotheses of the researchdescribed here is that some of the reasons for thebehavioral and emotional changes that follow damageto the prefrontal cortex may be related to deficits indecoding the reward and punishment value of stimuliand using the results of the decoding to modify behaviorand the ongoing emotional or mood state (Rolls 19901999a 1999b Rolls et al 1994) In this context it is ofinterest that the patients with bilateral orbito-frontalcortex damage who were impaired at the visual discrim-ination reversal task (see Table 1) had high scores onparts of a social behavior questionnaire in which thepatients were rated on behaviors such as the recognitionof emotion in others (eg their sad angry or disgustedmood) in interpersonal relationships (such as not caringwhat others think and not being close to the family) insociability (is not sociable and has difficulty making ormaintaining close relationships) emotional empathy(eg when others are happy is not happy for them)public behavior (is uncooperative) antisocial behavior (iscritical of and impatient with others) and impulsivity(does things without thinking) (Hornak Bramham RollsMorris OrsquoDoherty amp Polkey 2003) all of which couldreflect less behavioral sensitivity to different types ofpunishment and reward Further in a subjective emo-tional change questionnaire in which the patients re-ported on any changes in the intensity andor frequencyof their own experience of emotions since surgery thebilateral orbito-frontal cortex patients with deficits in thevisual discrimination reversal task reported a number ofchanges including changes in sadness anger fear andhappiness and were as a group significantly different inthese respects from the dorsolateral prefrontal cortexlesion group included in that comparison (Hornak et al2003) However it must also be pointed out that thepatients with unilateral orbito-frontalanterior cingulatelesions (the BA 9ACC and BA 9ACC + orbital groups ofthat article) also reported marked emotional changes andthey were also less well-adjusted socially than the dorso-lateral group but had no measured deficit in reversal The
Hornak et al 471
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3

visual discrimination reversal test However in thisprevious study the more diffuse nature of the lesions(with some produced by closed head injury althoughnevertheless with clear damage to the ventral prefrontalcortex evident in structural MRI scans) precluded pre-cise localization of this impairment to the orbito-frontalcortex In the present study by investigating patientswith surgical and thus more circumscribed lesions of thefrontal lobes we were able to demonstrate that animpairment on reversal learning can occur followingbilateral orbital excisions These results are consistentwith findings from nonhuman primates which implicatethe orbito-frontal cortex in reward and in stimulusndashreward learning and reversal (Dias et al 1996 Rolls1990 1999b 2000) as well as with the results from ourneuroimaging study using the same probabilistic reversaltask (OrsquoDoherty Kringelbach et al 2001) which pro-duced bilateral activation in the orbito-frontal cortex innormal subjects In the present study although as agroup the patients with bilateral orbital lesions weresignificantly impaired on this test only those whoselesions included the areas activated in the fMRI studyshowed a marked impairment whereas the two patientswith bilateral lesions who were not significantly impaired(VO and RR) had small lesions restricted either to theregion anterior or to the region posterior to the regionsof activation (see Figure 3A)
In the fMRI study it was found that the medial and thelateral regions of the orbito-frontal cortex were activat-ed respectively by reward and by punishment andindeed that the degree of activation in these two regionswas correlated with the amount of lsquolsquomoneyrsquorsquo gained orlost (OrsquoDoherty Kringelbach et al 2001) In the pres-ent study the patients with bilateral orbital lesions whowere impaired on the test all had lesions that encom-passed both the more medial and the more lateralregions described in the activation study and for thatreason a difference in sensitivity to reward and topunishment would not be expected in this patientgroup Consistent with this no clear pattern of greatersensitivity to punishment or to reward was observed inthose with bilateral lesions who were impaired Furtherresearch with more discrete lesions within the orbito-frontal cortex may reveal more detailed parallels withthe fMRI study perhaps with sensitivity to reward beingimpaired by medial orbito-frontal cortex lesions andsensitivity to punishment by lateral orbito-frontal cortexlesions However since a recent fMRI study found thatventrolateral activation was associated with reversallearning independently of the effects of negative feed-back (Cools Clark Owen amp Robbins 2002) the medialndashlateral distinction (within the orbital cortex) for rewardand for punishment respectively seems less likely tohold up for this kind of test
It is important that in the present study the groupwith unilateral orbital lesions on either side was unim-paired indicating that it is necessary for the orbital
damage to extend bilaterally before impairments areshown on visual discrimination reversal learning Thissuggests that either the left or the right orbito-frontalcortex on its own can carry out the functions necessaryfor normal performance It is very unlikely that lesionsize per se can explain this effect because somepatients with unilateral orbital lesions who were unim-paired had a larger total area of prefrontal cortexexcised than some of the patients with bilateral orbitallesions who were impaired This was confirmed by thefact that there was no correlation between the totallesion size (amount of prefrontal cortex excised) andperformance on the task
The design of the probabilistic reversal task meansthat two interpretations of the impairment shown bypatients with bilateral orbitalmedial lesions can beexcluded First the repeated touching of the previouslyrewarded stimulus cannot be explained in terms ofsimple motor perseveration (ie as a failure of inhibitorycontrol of the armhand with which the patients reachedout to touch the now-incorrect stimulus) Because aresponse was required and made on every trial thecontinued selection of the old S+ must reflect insteadthe patientrsquos difficulty when reinforcement contingen-cies are reversed in altering the previous associationformed between the stimulus and reward or that be-tween the stimulus and the response he should make toit Although the present study does not distinguishbetween these two interpretations the results are con-sistent with the hypothesis (Rolls 1990 1999b 20002002) that one important function of the orbito-frontalcortex consists in representing the reward and punish-ment value of stimuli and in particular since all patientssucceeded in the early stages of the task (before the firstreversal) in updating the associations between stimuliand reward or punishment value when these change
Secondly the clear instructions that explained thatreversals would occur and that subjects were to alter theirchoice of stimulus accordingly exclude an interpretationin terms of lack of initiative This might have explainedsome of the problems shown by patients in our earlierstudy (Rolls et al 1994) in which no warning was giventhat the contingencies would change The fact that clearexplanation was given about this in the present study atleast excludes an explanation in these terms Howeverwe cannot exclude the possibility that some of thepatients with dorsolateral lesions who were impaired atthe test and who failed to attend to the essential feedbackhad failed fully to understand the task requirements andif so this itself may be viewed as an aspect of executivedysfunction Interestingly among those who failed toattend to the amount won or lost on each trial somedid attend to this for some of the time but did notappreciate its importance and started to attend to othersources of feedback instead (Appendix 2B)
The difficulty in selecting the appropriate feedback orusing it in a consistent manner which was shown by
Hornak et al 469
almost half of the patients in the dorsolateral group andwhich resulted in severely impaired performance on thereversal test has parallels in work with nonhumanprimates in which dorsolateral lesions impaired theability to lsquolsquomonitor multiple stimulirsquorsquo (Petrides amp Pandya1999) as well as with neuroimaging studies of executivefunctions such as those involved in dual-task perfor-mance (Szameitat Torsten Muller amp von Cramon2002) On the posttest questionnaire the patients inthis study reported that instead of using the amountwon or lost on each trial to guide their choice of patternthey had attended instead to other nonessential sourcesof information such as the cumulative total (as anumber or as a bar chart) whether they had won orlost on each trial (ignoring the amount) or the colors orsounds that were associated with gains or losses (Wenote that the self-report provided by these patients withcircumscribed frontal lesions was sufficiently reliablethat across the group the self-report about attention tothe essential feedback was strongly related to the level ofperformance on the task Indeed there was a significant
difference between the proportions of patients whowere impaired who attended 29 and who failed toattend 78 Fisherrsquos exact test p = 02 two-tailed) It isof interest that the dorsolateral group who failed toattend or who failed to attend consistently to theessential feedback during the main reversal phase ofthe test were able to appreciate which feedback to use inthe far easier practice session of the test in which noreversals occurred A similar effect of task difficulty inrevealing impairments in patients with dorsolateral le-sions has been reported by Morris et al (2002) whofound that the ability to employ the appropriate strategyin a test of planning ability was not apparent in the earlypart of the test but became apparent only in the laterharder phase Similarly in Szameitat et alrsquos (2002) studydorsolateral prefrontal cortex activation was producedonly when the task difficulty was increased
In the present study three of the four (R C F Zand B S) whose lesions were confined to the dorso-lateral prefrontal region all failed to attend to the amountwonlost on each trial suggesting that a dorsolateral
Figure 3 Brain maps showinglesion sites Within each groupwith unilateral lesions thosewith right-sided lesions areshown first (A) Bilateral orbito-frontal cortex (or orbital plusmedial prefrontal cortex) (B)Unilateral orbito-frontal (ororbital plus medial) (C) Uni-lateral medial prefrontal cortex(D) Unilateral dorsolateralprefrontal (or dorsolateral plusmedial prefrontal) (E)Unilateral orbito-frontal plusmedial prefrontal plusdorsolateral prefrontal cortex
470 Journal of Cognitive Neuroscience Volume 16 Number 3
lesion may be sufficient to produce this cognitiveexecu-tive impairment In those cases where the dorsolaterallesions extended down into the medial region there arealso parallels with imaging studies in which the moredorsal regions of anterior cingulate described by theauthors as its cognitive division are activated in normalsubjects during tasks involving stimulusndashresponse selec-tion in the face of competing streams of information(Bush Luu amp Posner 2000) The dorsolateral prefrontalcortex lesions did in fact extend into this lsquolsquocognitivedivisionrsquorsquo region of the anterior cingulate cortex in theother five patients with dorsolateral lesions (GE GDOR AG and LK) who also failed to attend to theappropriate feedback However since other patients withcomparable lesions extending into these regions suc-ceeded in attending to this feedback this suggestionmust remain tentative It will be of interest to developour reversal task in the future to simplify the feedbackprovided in the expectation that this will make the taskperformable without deficit by patients with dorsolateralprefrontal cortex lesions but still sensitive to the effectsof lesions to the orbito-frontal cortex due to the reversalcomponent of the task
The findings reported in this study suggest that theprobabilistic reversal test makes demands on differentfunctions attributed respectively to the dorsolateraland to the orbital regions of the prefrontal cortex (cfBechara et al 1998 who reported a study in whichlesions in these regions had dissociable effects ondecision making and on working memory) Thus inthe present study the need to determine which ofmultiple competing sources of feedback should beattended to to maintain attention to this throughoutthe test ignoring other visually salient but noncrucialtypes of feedback (flashing lights total sum displayedcolored bar charts etc) are among the many functionsthat have been attributed to the dorsolateral prefrontalcortex (Szameitat et al 2002 Duncan amp Owen 2000)For a subject who is capable of attending consistently tothe appropriate feedback it is also necessary to use theinformation about the current level of reward associatedwith each pattern to guide his choice on each trial andas such the test also makes demands on functionsattributed to the orbito-frontal cortex (Rolls 19901999a 1999b 2000) The results of the present studyshow that it is possible to be severely impaired on thisprobabilistic visual discrimination reversal test for eitherof these two reasons and in the context that perfor-mance on the test can be independently disrupted bythe effects of dorsolateral and of orbital lesions we haveshown a dissociation between the effects of lesions inthese two regions The ability to attend to the crucialfeedback can be disrupted by a dorsolateral lesion oneither side whereas the ability to use this information tochoose advantageously can be supported by eitherorbital region on its own (after a unilateral orbitallesion) but is abolished by a bilateral orbital lesion
These results are consistent with the view that whereasthe dorsolateral frontal cortex forms part of a network ofprefrontal regions recruited to solve diverse cognitiveproblems especially those with an lsquolsquoexecutiversquorsquo compo-nent (in this case appreciating which feedback is rele-vantimportant) (Bush et al 2000 Duncan amp Owen2000) the orbito-frontal cortex is involved in the repre-sentation of the changing reward value of stimuli (Rolls1990 1999b 2000 2002) so that behavior can be mod-ified accordingly As such the present study contributesboth to our understanding of the different functions ofthese two regions of frontal lobe and to how theseregions need to cooperate on complex tasks such as theone used here A similar argument is made by Manes et al(2002) who showed how the ventral and dorsal aspects ofthe prefrontal cortex must interact in the maintenance ofrational and lsquolsquononriskyrsquorsquo decision-making tasks
One of the underlying hypotheses of the researchdescribed here is that some of the reasons for thebehavioral and emotional changes that follow damageto the prefrontal cortex may be related to deficits indecoding the reward and punishment value of stimuliand using the results of the decoding to modify behaviorand the ongoing emotional or mood state (Rolls 19901999a 1999b Rolls et al 1994) In this context it is ofinterest that the patients with bilateral orbito-frontalcortex damage who were impaired at the visual discrim-ination reversal task (see Table 1) had high scores onparts of a social behavior questionnaire in which thepatients were rated on behaviors such as the recognitionof emotion in others (eg their sad angry or disgustedmood) in interpersonal relationships (such as not caringwhat others think and not being close to the family) insociability (is not sociable and has difficulty making ormaintaining close relationships) emotional empathy(eg when others are happy is not happy for them)public behavior (is uncooperative) antisocial behavior (iscritical of and impatient with others) and impulsivity(does things without thinking) (Hornak Bramham RollsMorris OrsquoDoherty amp Polkey 2003) all of which couldreflect less behavioral sensitivity to different types ofpunishment and reward Further in a subjective emo-tional change questionnaire in which the patients re-ported on any changes in the intensity andor frequencyof their own experience of emotions since surgery thebilateral orbito-frontal cortex patients with deficits in thevisual discrimination reversal task reported a number ofchanges including changes in sadness anger fear andhappiness and were as a group significantly different inthese respects from the dorsolateral prefrontal cortexlesion group included in that comparison (Hornak et al2003) However it must also be pointed out that thepatients with unilateral orbito-frontalanterior cingulatelesions (the BA 9ACC and BA 9ACC + orbital groups ofthat article) also reported marked emotional changes andthey were also less well-adjusted socially than the dorso-lateral group but had no measured deficit in reversal The
Hornak et al 471
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
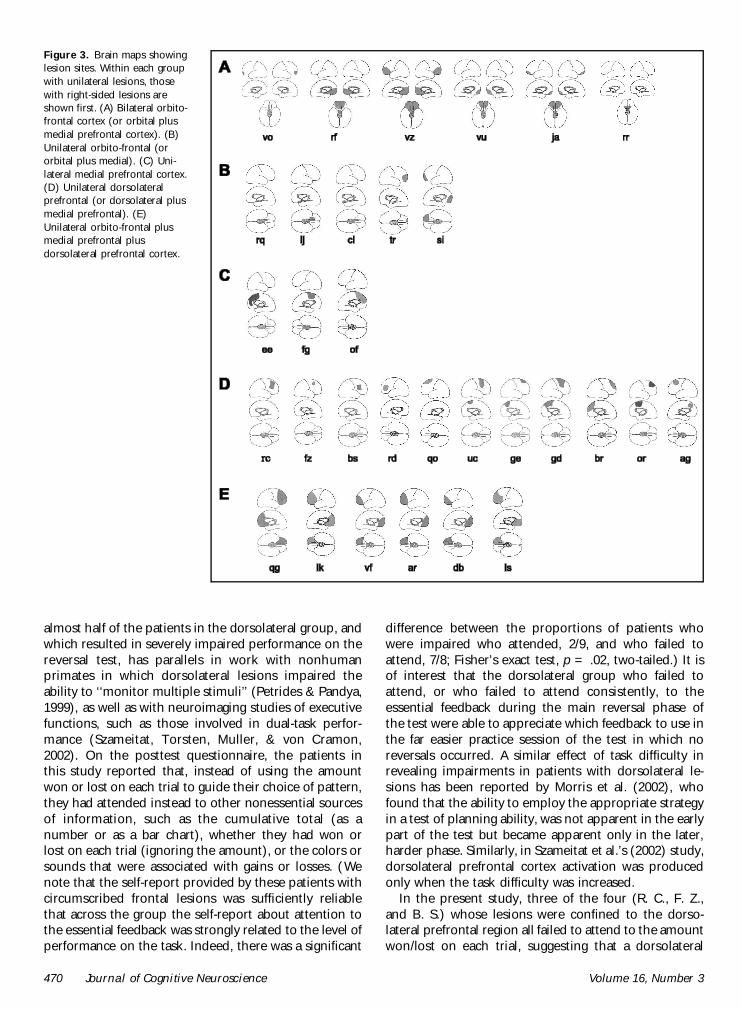
almost half of the patients in the dorsolateral group andwhich resulted in severely impaired performance on thereversal test has parallels in work with nonhumanprimates in which dorsolateral lesions impaired theability to lsquolsquomonitor multiple stimulirsquorsquo (Petrides amp Pandya1999) as well as with neuroimaging studies of executivefunctions such as those involved in dual-task perfor-mance (Szameitat Torsten Muller amp von Cramon2002) On the posttest questionnaire the patients inthis study reported that instead of using the amountwon or lost on each trial to guide their choice of patternthey had attended instead to other nonessential sourcesof information such as the cumulative total (as anumber or as a bar chart) whether they had won orlost on each trial (ignoring the amount) or the colors orsounds that were associated with gains or losses (Wenote that the self-report provided by these patients withcircumscribed frontal lesions was sufficiently reliablethat across the group the self-report about attention tothe essential feedback was strongly related to the level ofperformance on the task Indeed there was a significant
difference between the proportions of patients whowere impaired who attended 29 and who failed toattend 78 Fisherrsquos exact test p = 02 two-tailed) It isof interest that the dorsolateral group who failed toattend or who failed to attend consistently to theessential feedback during the main reversal phase ofthe test were able to appreciate which feedback to use inthe far easier practice session of the test in which noreversals occurred A similar effect of task difficulty inrevealing impairments in patients with dorsolateral le-sions has been reported by Morris et al (2002) whofound that the ability to employ the appropriate strategyin a test of planning ability was not apparent in the earlypart of the test but became apparent only in the laterharder phase Similarly in Szameitat et alrsquos (2002) studydorsolateral prefrontal cortex activation was producedonly when the task difficulty was increased
In the present study three of the four (R C F Zand B S) whose lesions were confined to the dorso-lateral prefrontal region all failed to attend to the amountwonlost on each trial suggesting that a dorsolateral
Figure 3 Brain maps showinglesion sites Within each groupwith unilateral lesions thosewith right-sided lesions areshown first (A) Bilateral orbito-frontal cortex (or orbital plusmedial prefrontal cortex) (B)Unilateral orbito-frontal (ororbital plus medial) (C) Uni-lateral medial prefrontal cortex(D) Unilateral dorsolateralprefrontal (or dorsolateral plusmedial prefrontal) (E)Unilateral orbito-frontal plusmedial prefrontal plusdorsolateral prefrontal cortex
470 Journal of Cognitive Neuroscience Volume 16 Number 3
lesion may be sufficient to produce this cognitiveexecu-tive impairment In those cases where the dorsolaterallesions extended down into the medial region there arealso parallels with imaging studies in which the moredorsal regions of anterior cingulate described by theauthors as its cognitive division are activated in normalsubjects during tasks involving stimulusndashresponse selec-tion in the face of competing streams of information(Bush Luu amp Posner 2000) The dorsolateral prefrontalcortex lesions did in fact extend into this lsquolsquocognitivedivisionrsquorsquo region of the anterior cingulate cortex in theother five patients with dorsolateral lesions (GE GDOR AG and LK) who also failed to attend to theappropriate feedback However since other patients withcomparable lesions extending into these regions suc-ceeded in attending to this feedback this suggestionmust remain tentative It will be of interest to developour reversal task in the future to simplify the feedbackprovided in the expectation that this will make the taskperformable without deficit by patients with dorsolateralprefrontal cortex lesions but still sensitive to the effectsof lesions to the orbito-frontal cortex due to the reversalcomponent of the task
The findings reported in this study suggest that theprobabilistic reversal test makes demands on differentfunctions attributed respectively to the dorsolateraland to the orbital regions of the prefrontal cortex (cfBechara et al 1998 who reported a study in whichlesions in these regions had dissociable effects ondecision making and on working memory) Thus inthe present study the need to determine which ofmultiple competing sources of feedback should beattended to to maintain attention to this throughoutthe test ignoring other visually salient but noncrucialtypes of feedback (flashing lights total sum displayedcolored bar charts etc) are among the many functionsthat have been attributed to the dorsolateral prefrontalcortex (Szameitat et al 2002 Duncan amp Owen 2000)For a subject who is capable of attending consistently tothe appropriate feedback it is also necessary to use theinformation about the current level of reward associatedwith each pattern to guide his choice on each trial andas such the test also makes demands on functionsattributed to the orbito-frontal cortex (Rolls 19901999a 1999b 2000) The results of the present studyshow that it is possible to be severely impaired on thisprobabilistic visual discrimination reversal test for eitherof these two reasons and in the context that perfor-mance on the test can be independently disrupted bythe effects of dorsolateral and of orbital lesions we haveshown a dissociation between the effects of lesions inthese two regions The ability to attend to the crucialfeedback can be disrupted by a dorsolateral lesion oneither side whereas the ability to use this information tochoose advantageously can be supported by eitherorbital region on its own (after a unilateral orbitallesion) but is abolished by a bilateral orbital lesion
These results are consistent with the view that whereasthe dorsolateral frontal cortex forms part of a network ofprefrontal regions recruited to solve diverse cognitiveproblems especially those with an lsquolsquoexecutiversquorsquo compo-nent (in this case appreciating which feedback is rele-vantimportant) (Bush et al 2000 Duncan amp Owen2000) the orbito-frontal cortex is involved in the repre-sentation of the changing reward value of stimuli (Rolls1990 1999b 2000 2002) so that behavior can be mod-ified accordingly As such the present study contributesboth to our understanding of the different functions ofthese two regions of frontal lobe and to how theseregions need to cooperate on complex tasks such as theone used here A similar argument is made by Manes et al(2002) who showed how the ventral and dorsal aspects ofthe prefrontal cortex must interact in the maintenance ofrational and lsquolsquononriskyrsquorsquo decision-making tasks
One of the underlying hypotheses of the researchdescribed here is that some of the reasons for thebehavioral and emotional changes that follow damageto the prefrontal cortex may be related to deficits indecoding the reward and punishment value of stimuliand using the results of the decoding to modify behaviorand the ongoing emotional or mood state (Rolls 19901999a 1999b Rolls et al 1994) In this context it is ofinterest that the patients with bilateral orbito-frontalcortex damage who were impaired at the visual discrim-ination reversal task (see Table 1) had high scores onparts of a social behavior questionnaire in which thepatients were rated on behaviors such as the recognitionof emotion in others (eg their sad angry or disgustedmood) in interpersonal relationships (such as not caringwhat others think and not being close to the family) insociability (is not sociable and has difficulty making ormaintaining close relationships) emotional empathy(eg when others are happy is not happy for them)public behavior (is uncooperative) antisocial behavior (iscritical of and impatient with others) and impulsivity(does things without thinking) (Hornak Bramham RollsMorris OrsquoDoherty amp Polkey 2003) all of which couldreflect less behavioral sensitivity to different types ofpunishment and reward Further in a subjective emo-tional change questionnaire in which the patients re-ported on any changes in the intensity andor frequencyof their own experience of emotions since surgery thebilateral orbito-frontal cortex patients with deficits in thevisual discrimination reversal task reported a number ofchanges including changes in sadness anger fear andhappiness and were as a group significantly different inthese respects from the dorsolateral prefrontal cortexlesion group included in that comparison (Hornak et al2003) However it must also be pointed out that thepatients with unilateral orbito-frontalanterior cingulatelesions (the BA 9ACC and BA 9ACC + orbital groups ofthat article) also reported marked emotional changes andthey were also less well-adjusted socially than the dorso-lateral group but had no measured deficit in reversal The
Hornak et al 471
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3

lesion may be sufficient to produce this cognitiveexecu-tive impairment In those cases where the dorsolaterallesions extended down into the medial region there arealso parallels with imaging studies in which the moredorsal regions of anterior cingulate described by theauthors as its cognitive division are activated in normalsubjects during tasks involving stimulusndashresponse selec-tion in the face of competing streams of information(Bush Luu amp Posner 2000) The dorsolateral prefrontalcortex lesions did in fact extend into this lsquolsquocognitivedivisionrsquorsquo region of the anterior cingulate cortex in theother five patients with dorsolateral lesions (GE GDOR AG and LK) who also failed to attend to theappropriate feedback However since other patients withcomparable lesions extending into these regions suc-ceeded in attending to this feedback this suggestionmust remain tentative It will be of interest to developour reversal task in the future to simplify the feedbackprovided in the expectation that this will make the taskperformable without deficit by patients with dorsolateralprefrontal cortex lesions but still sensitive to the effectsof lesions to the orbito-frontal cortex due to the reversalcomponent of the task
The findings reported in this study suggest that theprobabilistic reversal test makes demands on differentfunctions attributed respectively to the dorsolateraland to the orbital regions of the prefrontal cortex (cfBechara et al 1998 who reported a study in whichlesions in these regions had dissociable effects ondecision making and on working memory) Thus inthe present study the need to determine which ofmultiple competing sources of feedback should beattended to to maintain attention to this throughoutthe test ignoring other visually salient but noncrucialtypes of feedback (flashing lights total sum displayedcolored bar charts etc) are among the many functionsthat have been attributed to the dorsolateral prefrontalcortex (Szameitat et al 2002 Duncan amp Owen 2000)For a subject who is capable of attending consistently tothe appropriate feedback it is also necessary to use theinformation about the current level of reward associatedwith each pattern to guide his choice on each trial andas such the test also makes demands on functionsattributed to the orbito-frontal cortex (Rolls 19901999a 1999b 2000) The results of the present studyshow that it is possible to be severely impaired on thisprobabilistic visual discrimination reversal test for eitherof these two reasons and in the context that perfor-mance on the test can be independently disrupted bythe effects of dorsolateral and of orbital lesions we haveshown a dissociation between the effects of lesions inthese two regions The ability to attend to the crucialfeedback can be disrupted by a dorsolateral lesion oneither side whereas the ability to use this information tochoose advantageously can be supported by eitherorbital region on its own (after a unilateral orbitallesion) but is abolished by a bilateral orbital lesion
These results are consistent with the view that whereasthe dorsolateral frontal cortex forms part of a network ofprefrontal regions recruited to solve diverse cognitiveproblems especially those with an lsquolsquoexecutiversquorsquo compo-nent (in this case appreciating which feedback is rele-vantimportant) (Bush et al 2000 Duncan amp Owen2000) the orbito-frontal cortex is involved in the repre-sentation of the changing reward value of stimuli (Rolls1990 1999b 2000 2002) so that behavior can be mod-ified accordingly As such the present study contributesboth to our understanding of the different functions ofthese two regions of frontal lobe and to how theseregions need to cooperate on complex tasks such as theone used here A similar argument is made by Manes et al(2002) who showed how the ventral and dorsal aspects ofthe prefrontal cortex must interact in the maintenance ofrational and lsquolsquononriskyrsquorsquo decision-making tasks
One of the underlying hypotheses of the researchdescribed here is that some of the reasons for thebehavioral and emotional changes that follow damageto the prefrontal cortex may be related to deficits indecoding the reward and punishment value of stimuliand using the results of the decoding to modify behaviorand the ongoing emotional or mood state (Rolls 19901999a 1999b Rolls et al 1994) In this context it is ofinterest that the patients with bilateral orbito-frontalcortex damage who were impaired at the visual discrim-ination reversal task (see Table 1) had high scores onparts of a social behavior questionnaire in which thepatients were rated on behaviors such as the recognitionof emotion in others (eg their sad angry or disgustedmood) in interpersonal relationships (such as not caringwhat others think and not being close to the family) insociability (is not sociable and has difficulty making ormaintaining close relationships) emotional empathy(eg when others are happy is not happy for them)public behavior (is uncooperative) antisocial behavior (iscritical of and impatient with others) and impulsivity(does things without thinking) (Hornak Bramham RollsMorris OrsquoDoherty amp Polkey 2003) all of which couldreflect less behavioral sensitivity to different types ofpunishment and reward Further in a subjective emo-tional change questionnaire in which the patients re-ported on any changes in the intensity andor frequencyof their own experience of emotions since surgery thebilateral orbito-frontal cortex patients with deficits in thevisual discrimination reversal task reported a number ofchanges including changes in sadness anger fear andhappiness and were as a group significantly different inthese respects from the dorsolateral prefrontal cortexlesion group included in that comparison (Hornak et al2003) However it must also be pointed out that thepatients with unilateral orbito-frontalanterior cingulatelesions (the BA 9ACC and BA 9ACC + orbital groups ofthat article) also reported marked emotional changes andthey were also less well-adjusted socially than the dorso-lateral group but had no measured deficit in reversal The
Hornak et al 471
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
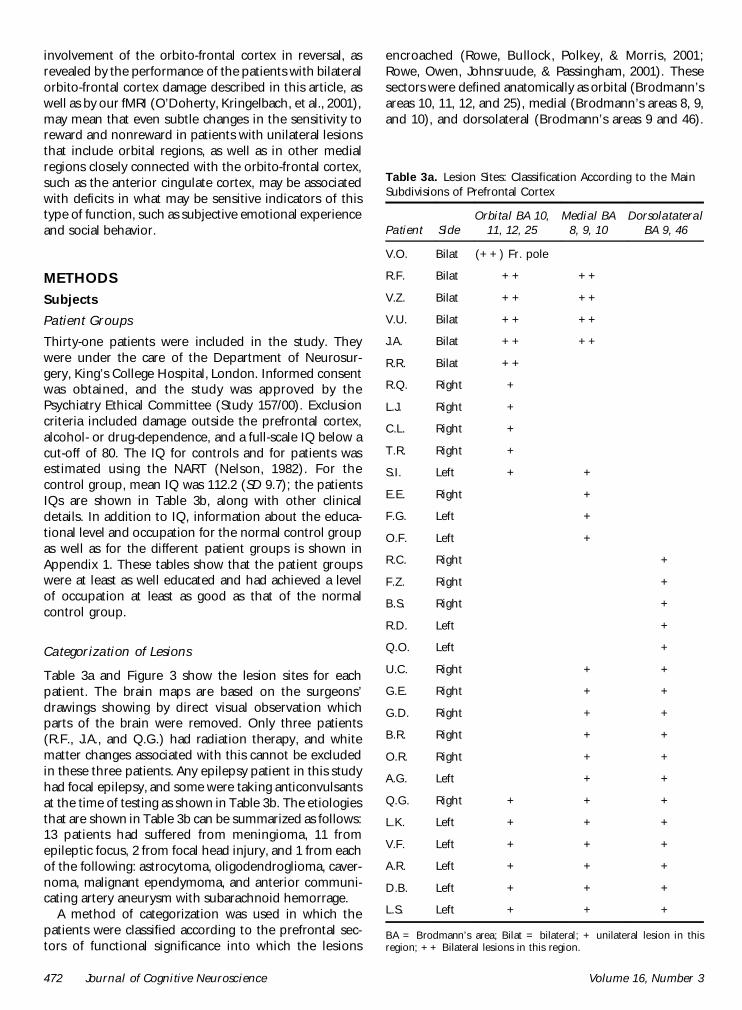
involvement of the orbito-frontal cortex in reversal asrevealed by the performance of the patients with bilateralorbito-frontal cortex damage described in this article aswell as by our fMRI (OrsquoDoherty Kringelbach et al 2001)may mean that even subtle changes in the sensitivity toreward and nonreward in patients with unilateral lesionsthat include orbital regions as well as in other medialregions closely connected with the orbito-frontal cortexsuch as the anterior cingulate cortex may be associatedwith deficits in what may be sensitive indicators of thistype of function such as subjective emotional experienceand social behavior
METHODS
Subjects
Patient Groups
Thirty-one patients were included in the study Theywere under the care of the Department of Neurosur-gery Kingrsquos College Hospital London Informed consentwas obtained and the study was approved by thePsychiatry Ethical Committee (Study 15700) Exclusioncriteria included damage outside the prefrontal cortexalcohol- or drug-dependence and a full-scale IQ below acut-off of 80 The IQ for controls and for patients wasestimated using the NART (Nelson 1982) For thecontrol group mean IQ was 1122 (SD 97) the patientsIQs are shown in Table 3b along with other clinicaldetails In addition to IQ information about the educa-tional level and occupation for the normal control groupas well as for the different patient groups is shown inAppendix 1 These tables show that the patient groupswere at least as well educated and had achieved a levelof occupation at least as good as that of the normalcontrol group
Categorization of Lesions
Table 3a and Figure 3 show the lesion sites for eachpatient The brain maps are based on the surgeonsrsquodrawings showing by direct visual observation whichparts of the brain were removed Only three patients(RF JA and QG) had radiation therapy and whitematter changes associated with this cannot be excludedin these three patients Any epilepsy patient in this studyhad focal epilepsy and some were taking anticonvulsantsat the time of testing as shown in Table 3b The etiologiesthat are shown in Table 3b can be summarized as follows13 patients had suffered from meningioma 11 fromepileptic focus 2 from focal head injury and 1 from eachof the following astrocytoma oligodendroglioma caver-noma malignant ependymoma and anterior communi-cating artery aneurysm with subarachnoid hemorrage
A method of categorization was used in which thepatients were classified according to the prefrontal sec-tors of functional significance into which the lesions
encroached (Rowe Bullock Polkey amp Morris 2001Rowe Owen Johnsruude amp Passingham 2001) Thesesectors were defined anatomically as orbital (Brodmannrsquosareas 10 11 12 and 25) medial (Brodmannrsquos areas 8 9and 10) and dorsolateral (Brodmannrsquos areas 9 and 46)
Table 3a Lesion Sites Classification According to the MainSubdivisions of Prefrontal Cortex
Patient SideOrbital BA 10
11 12 25Medial BA
8 9 10Dorsolatateral
BA 9 46
VO Bilat (++) Fr pole
RF Bilat ++ ++
VZ Bilat ++ ++
VU Bilat ++ ++
JA Bilat ++ ++
RR Bilat ++
RQ Right +
LJ Right +
CL Right +
TR Right +
SI Left + +
EE Right +
FG Left +
OF Left +
RC Right +
FZ Right +
BS Right +
RD Left +
QO Left +
UC Right + +
GE Right + +
GD Right + +
BR Right + +
OR Right + +
AG Left + +
QG Right + + +
LK Left + + +
VF Left + + +
AR Left + + +
DB Left + + +
LS Left + + +
BA = Brodmannrsquos area Bilat = bilateral + unilateral lesion in thisregion ++ Bilateral lesions in this region
472 Journal of Cognitive Neuroscience Volume 16 Number 3
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
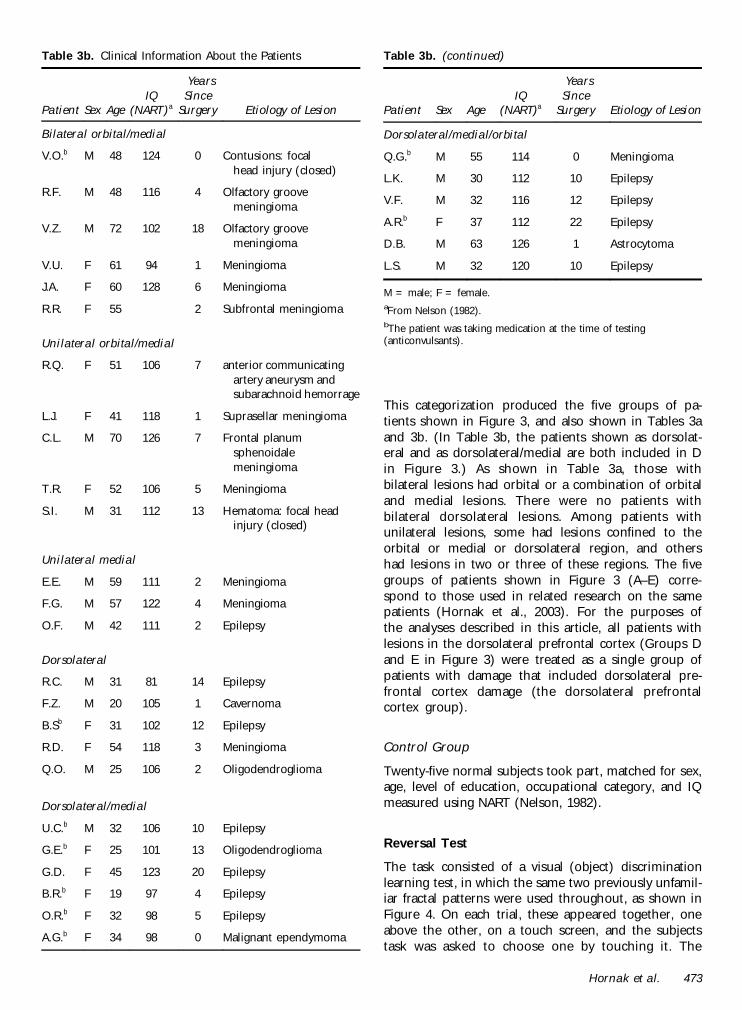
This categorization produced the five groups of pa-tients shown in Figure 3 and also shown in Tables 3aand 3b (In Table 3b the patients shown as dorsolat-eral and as dorsolateralmedial are both included in Din Figure 3) As shown in Table 3a those withbilateral lesions had orbital or a combination of orbitaland medial lesions There were no patients withbilateral dorsolateral lesions Among patients withunilateral lesions some had lesions confined to theorbital or medial or dorsolateral region and othershad lesions in two or three of these regions The fivegroups of patients shown in Figure 3 (AndashE) corre-spond to those used in related research on the samepatients (Hornak et al 2003) For the purposes ofthe analyses described in this article all patients withlesions in the dorsolateral prefrontal cortex (Groups Dand E in Figure 3) were treated as a single group ofpatients with damage that included dorsolateral pre-frontal cortex damage (the dorsolateral prefrontalcortex group)
Control Group
Twenty-five normal subjects took part matched for sexage level of education occupational category and IQmeasured using NART (Nelson 1982)
Reversal Test
The task consisted of a visual (object) discriminationlearning test in which the same two previously unfamil-iar fractal patterns were used throughout as shown inFigure 4 On each trial these appeared together oneabove the other on a touch screen and the subjectstask was asked to choose one by touching it The
Table 3b Clinical Information About the Patients
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Bilateral orbitalmedial
VOb M 48 124 0 Contusions focalhead injury (closed)
RF M 48 116 4 Olfactory groovemeningioma
VZ M 72 102 18 Olfactory groovemeningioma
VU F 61 94 1 Meningioma
JA F 60 128 6 Meningioma
RR F 55 2 Subfrontal meningioma
Unilateral orbitalmedial
RQ F 51 106 7 anterior communicatingartery aneurysm andsubarachnoid hemorrage
LJ F 41 118 1 Suprasellar meningioma
CL M 70 126 7 Frontal planumsphenoidalemeningioma
TR F 52 106 5 Meningioma
SI M 31 112 13 Hematoma focal headinjury (closed)
Unilateral medial
EE M 59 111 2 Meningioma
FG M 57 122 4 Meningioma
OF M 42 111 2 Epilepsy
Dorsolateral
RC M 31 81 14 Epilepsy
FZ M 20 105 1 Cavernoma
BSb F 31 102 12 Epilepsy
RD F 54 118 3 Meningioma
QO M 25 106 2 Oligodendroglioma
Dorsolateralmedial
UCb M 32 106 10 Epilepsy
GEb F 25 101 13 Oligodendroglioma
GD F 45 123 20 Epilepsy
BRb F 19 97 4 Epilepsy
ORb F 32 98 5 Epilepsy
AGb F 34 98 0 Malignant ependymoma
Table 3b (continued)
Patient Sex AgeIQ
(NART)a
YearsSince
Surgery Etiology of Lesion
Dorsolateralmedialorbital
QGb M 55 114 0 Meningioma
LK M 30 112 10 Epilepsy
VF M 32 116 12 Epilepsy
ARb F 37 112 22 Epilepsy
DB M 63 126 1 Astrocytoma
LS M 32 120 10 Epilepsy
M = male F = femaleaFrom Nelson (1982)bThe patient was taking medication at the time of testing(anticonvulsants)
Hornak et al 473
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
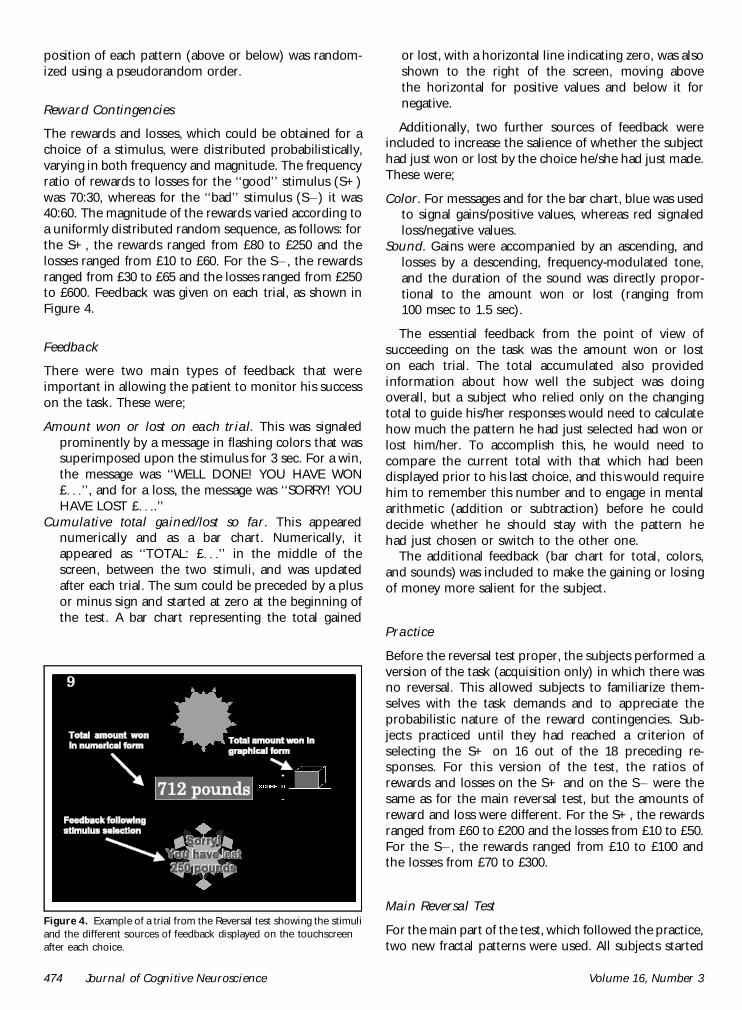
position of each pattern (above or below) was random-ized using a pseudorandom order
Reward Contingencies
The rewards and losses which could be obtained for achoice of a stimulus were distributed probabilisticallyvarying in both frequency and magnitude The frequencyratio of rewards to losses for the lsquolsquogoodrsquorsquo stimulus (S+)was 7030 whereas for the lsquolsquobadrsquorsquo stimulus (Siexcl) it was4060 The magnitude of the rewards varied according toa uniformly distributed random sequence as follows forthe S+ the rewards ranged from pound80 to pound250 and thelosses ranged from pound10 to pound60 For the Siexcl the rewardsranged from pound30 to pound65 and the losses ranged from pound250to pound600 Feedback was given on each trial as shown inFigure 4
Feedback
There were two main types of feedback that wereimportant in allowing the patient to monitor his successon the task These were
Amount won or lost on each trial This was signaledprominently by a message in flashing colors that wassuperimposed upon the stimulus for 3 sec For a winthe message was lsquolsquoWELL DONE YOU HAVE WONpound rsquorsquo and for a loss the message was lsquolsquoSORRY YOUHAVE LOST pound rsquorsquo
Cumulative total gainedlost so far This appearednumerically and as a bar chart Numerically itappeared as lsquolsquoTOTAL pound rsquorsquo in the middle of thescreen between the two stimuli and was updatedafter each trial The sum could be preceded by a plusor minus sign and started at zero at the beginning ofthe test A bar chart representing the total gained
or lost with a horizontal line indicating zero was alsoshown to the right of the screen moving abovethe horizontal for positive values and below it fornegative
Additionally two further sources of feedback wereincluded to increase the salience of whether the subjecthad just won or lost by the choice heshe had just madeThese were
Color For messages and for the bar chart blue was usedto signal gainspositive values whereas red signaledlossnegative values
Sound Gains were accompanied by an ascending andlosses by a descending frequency-modulated toneand the duration of the sound was directly propor-tional to the amount won or lost (ranging from100 msec to 15 sec)
The essential feedback from the point of view ofsucceeding on the task was the amount won or loston each trial The total accumulated also providedinformation about how well the subject was doingoverall but a subject who relied only on the changingtotal to guide hisher responses would need to calculatehow much the pattern he had just selected had won orlost himher To accomplish this he would need tocompare the current total with that which had beendisplayed prior to his last choice and this would requirehim to remember this number and to engage in mentalarithmetic (addition or subtraction) before he coulddecide whether he should stay with the pattern hehad just chosen or switch to the other one
The additional feedback (bar chart for total colorsand sounds) was included to make the gaining or losingof money more salient for the subject
Practice
Before the reversal test proper the subjects performed aversion of the task (acquisition only) in which there wasno reversal This allowed subjects to familiarize them-selves with the task demands and to appreciate theprobabilistic nature of the reward contingencies Sub-jects practiced until they had reached a criterion ofselecting the S+ on 16 out of the 18 preceding re-sponses For this version of the test the ratios ofrewards and losses on the S+ and on the Siexcl were thesame as for the main reversal test but the amounts ofreward and loss were different For the S+ the rewardsranged from pound60 to pound200 and the losses from pound10 to pound50For the Siexcl the rewards ranged from pound10 to pound100 andthe losses from pound70 to pound300
Main Reversal Test
For the main part of the test which followed the practicetwo new fractal patterns were used All subjects started
Figure 4 Example of a trial from the Reversal test showing the stimuliand the different sources of feedback displayed on the touchscreenafter each choice
474 Journal of Cognitive Neuroscience Volume 16 Number 3
with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3

with pound0 After a criterion of nine selections of the S+out of the preceding 10 trials was reached the firstreversal began This was achieved by gradually revers-ing in incremental steps over a period of 10 trials thereward contingencies of the two stimuli The probabil-ities shifted in a regular stepwise fashion over the 10trials The test stopped after 100 trials for all subjectsThe subjectrsquos comments were tape-recorded duringthe test
Instructions to the Subject
Practice The subjects were informed that each patternwhen touched could either give or take away varyingamounts of imaginary lsquolsquomoneyrsquorsquo and that this wouldbe displayed on the screen The different types offeedback were described and demonstrated on thescreen It was explained that one pattern gave morethan it took overall (the lsquolsquogoodrsquorsquo pattern) and thatone took more than it gave overall (the lsquolsquobadrsquorsquopattern) The subjects were told that if they keptchoosing the good pattern they would earn lots oflsquolsquomoneyrsquorsquo whereas if they kept choosing the lsquolsquobadrsquorsquopattern they would lose a lot of money and wouldlsquolsquogo more and more into the redrsquorsquo (into minusfigures) Their task was to determine by trial anderror which pattern it was more profitable to choose(by touching it) and to stick with it
Reversal test The subjects were told that this part of thetest would start in the same way as the practice butthat once they had found out which was the goodpattern and had touched it consistently a number oftimes it would gradually become lsquolsquobadrsquorsquo and that thebad pattern would become gradually becomelsquolsquogoodrsquorsquo The instructions were
Your aim is to adjust your choices accordinglymdashtostart choosing the pattern that had been bad atthe beginning and to avoid choosing the patternwhich had started off being good Once youhave successfully switched your choice of patternand have chosen it consistently a certain numberof times there will be a second reversal back tohow things were at the beginning and later athird reversal and so on Your aim is to win asmuch money as possible by keeping track ofwhich pattern is currently the good patternand choosing it consistently until you thinkit is changing and becoming the bad pattern
Posttest QuestionnaireDirectly after the subject had completed 100 trials thesubject was asked the open-ended question lsquolsquoWhatinformation on the screen did you find most useful inkeeping track of which pattern was currently the goodonersquorsquo After the subjects had answered this questionthey were then probed about each of the other
sources of feedback in turn Their responses weretape-recorded The testing and the posttest question-naire were carried out before details of the patientsrsquolesions were available and in this sense the testing wasperformed blind
Acknowledgments
This research was supported by the Medical Research CouncilInterdisciplinary Research Centre in Cognitive Neuroscience
Reprint requests should be sent to E T Rolls Department ofExperimental Psychology University of Oxford South ParksRoad Oxford OX1 3UD UK or via e-mail edmundrollspsyoxacuk
REFERENCES
Aharon I Etcoff N Ariely D Chabris C F OrsquoConnor Eamp Breiter H C (2001) Beautiful faces have variable rewardvalue fMRI and behavioral evidence Neuron 32 537ndash551
Bechara A Damasio A R Damasio H amp Anderson S W(1994) Insensitivity to future consequences followingdamage to human prefrontal cortex Cognition 50 7ndash15
Bechara A Damasio H Tranel D amp Anderson S W (1998)Dissociation of working memory from decision makingwithin the human prefrontal cortex Journal ofNeuroscience 18 428ndash437
Blood A J Zatorre R J Bermudez P amp Evans A C (1999)Emotional responses to pleasant and unpleasant musiccorrelate with activity in paralimbic brain regions NatureNeuroscience 2 382ndash387
Breiter H C Aharon I Kahneman D Dale A amp Shizgal P(2001) Functional imaging of neural responses to expectancyof monetary gains and losses Neuron 30 619ndash639
Bush G Luu P amp Posner M I (2000) Cognitive andemotional influences in anterior cingulate cortex Trendsin Cognitive Sciences 4 215ndash222
Butter C M (1969) Perseveration in extinction and indiscrimination reversal tasks following selective prefrontalablations in Macaca mulatta Physiology and Behavior 4163ndash171
Cools R Clark L Owen A amp Robbins T (2002) Definingthe neural mechanisms of probabilistic reversal learningusing event-related functional magnetic resonance imagingJournal of Neuroscience 22 4563ndash4567
Dias R Robbins T W amp Roberts A C (1996) Dissociation inprefrontal cortex of affective and attentional shifts Nature380 69ndash72
Duncan J amp Owen A M (2000) Common regions of thehuman frontal lobe recruited by diverse cognitive demandsTrends in Neuroscience 23 457ndash483
Elliott R Dolan R J amp Frith C D (2000) Dissociablefunctions in the medial and lateral orbitofrontal cortexEvidence form human neuroimaging studies CerebralCortex 10 308ndash317
Elliot R Frith C D amp Dolan R J (1997) Differential neuralresponse to positive and negative feedback in planning andguessing tasks Neuropsychologia 35 1395ndash1404
Francis S Rolls E T Bowtell R McGlone F OrsquoDoherty JBrowning A Clare S amp Smith E (1999) The representationof pleasant touch in the brain and its relationship with tasteand olfactory areas NeuroReport 10 453ndash459
Frey P Kostopoulos P amp Petrides M (2000) Orbitofrontalinvolvement in the processing of unpleasant auditoryinformation European Journal of Neuroscience 123709ndash3712
Hornak et al 475
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
Goldman-Rakic P S (1996) Regional and cellular fractionationof working memory Proceedings of the National Academyof Sciences USA 93 13473ndash13480
Gottfried J A Deichmann R Winston J S amp Dolan R J(2002) Functional heterogeneity in human olfactory cortexAn event-related functional magnetic resonance imagingstudy Journal of Neuroscience 22 10819ndash10828
Hornak J Bramham J Rolls E T Morris R G OrsquoDohertyJ Bullock P R amp Polkey C E (2003) Changes in emotionafter circumscribed surgical lesions of the orbitofrontal andcingulate cortices Brain 126 1691ndash1712
Hornak J Rolls E T amp Wade D (1996) Face and voiceexpression identification in patients with emotional andbehavioural changes following ventral frontal lobe damageNeuropsychologia 34 247ndash261
Iversen S D amp Mishkin M (1970) Perseverative interferencein monkey following selective lesions of the inferiorprefrontal convexity Experimental Brain Research 11376ndash386
Knutson B Fong G W Adams C M Varner J L amp HommerD (2001) Dissociation of reward anticipation and outcomewith event-related fMRI NeuroReport 12 3683ndash3687
Manes F Sahakian B B Clark L Rogers R Antoun NAitken M amp Robbins T (2002) Decision-making processesfollowing damage to the prefrontal cortex Brain 125624ndash639
Meunier M Bachevalier J amp Mishkin M (1997) Effects oforbital frontal and anterior cingulate lesions on object andspatial memory in rhesus monkeys Neuropsychologia 35999ndash1015
Morris R G Kotisa M Brooks B Rose F D Bullock P ampPolkay C E (2002) Virtual reality investigations ofplanning ability following focal prefrontal cortical lesionsPaper presented at the 19th Annual British PsychologicalSociety Cognitive Psychology Section Conference Kent UK
Nelson E H (1982) National Adult Reading Test (NART) TestManual Windsor NFER-Nelson
OrsquoDoherty J Kringelbach M L Rolls E T Hornak J ampAndrews C (2001) Abstract reward and punishmentrepresentations in the human orbitofrontal cortex NatureNeuroscience 4 95ndash102
OrsquoDoherty J Rolls E T Francis S Bowtell R McGlone FKobal G Renner B amp Ahne G (2000) Sensory-specificsatiety related olfactory activation of the humanorbitofrontal cortex NeuroReport 11 893ndash897
OrsquoDoherty J Rolls E T Francis S McGlone F amp Bowtell R(2001) Representation of pleasant and aversive taste in thehuman brain Journal of Neurophysiology 85 1315ndash1321
OrsquoDoherty J Winston J Critchley H Perrett D Burt DM amp Dolan R J (2003) Beauty in a smile The role ofmedial orbitofrontal cortex in facial attractivenessNeuropsychologia 41 147ndash155
Owen A M (1997) Cognitive planning in humansNeuropsychological neuroanatomical andneuropharmacological perspectives Progress inNeurobiology 53 431ndash450
Petrides M amp Pandya D N (1999) Dorsolateral prefrontalcortex Comparative cytoarchitectonic analysis in the humanand macaque brain and cortico-cortical connection patternsEuropean Journal of Neuroscience 11 1011ndash1036
Robbins T W (1998) Dissociating executive functions of theprefrontal cortex In A C Roberts (Ed) Functions of theprefrontal cortex (pp 117ndash130) Oxford Oxford UniversityPress
Roberts A C amp Wallis J D (2000) Inhibitory control andaffective processing in the prefrontal cortexNeuropsychological studies in the common marmosetCerebral Cortex 10 252ndash262
Rogers R D Andrews T C Grasby P M Brooks D J ampRobbins T W (2000) Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversallearning in humans Journal of Cognitive Neuroscience 12142ndash162
Rolls E T (1990) A theory of emotion and its application tounderstanding the neural basis of emotion Cognition andEmotion 4 161ndash190
Rolls E T (1999a) The functions of the orbitofrontal cortexNeurocase 5 301ndash312
Rolls E T (1999b) The brain and emotion Oxford OxfordUniversity Press
Rolls E T (2000) The orbitofrontal cortex and rewardCerebral Cortex 10 284ndash294
Rolls E T (2002) The functions of the orbitofrontal cortex InD T Stuss amp R T Knight (Eds) Principles of frontal lobefunction (chap 23 pp 354ndash375) New York OxfordUniversity Press
Rolls E T Critchley H Mason R amp Wakeman E A (1996)Orbitofrontal cortex neurons Role in olfactory and visualassociation learning Journal of Neurophysiology 751970ndash1981
Rolls E T Hornak J Wade D amp McGrath J (1994)Emotion-related learning in patients with social andemotional changes associated with frontal lobe damageJournal of Neurology Neurosurgery and Psychiatry 571518ndash1524
Rolls E T Kringelbach M L De Araujo I E T (2003)Different representations of pleasant and unpleasant odorsin the human brain European Journal of Neuroscience 18695ndash703
Rolls E T OrsquoDoherty J Kringelbach M L Francis SBowtell R amp McGlone F (2003) Representations ofpleasant and painful touch in the human orbitofrontaland cingulate cortices Cerebral Cortex 13 308ndash317
Rolls E T Sienkiewicz Z J amp Yaxley S (1989) Hungermodulates the responses to gustatory stimuli of singleneurons in the caudolateral orbitofrontal cortex of themacaque monkey European Journal of Neuroscience 153ndash60
Rowe A D Bullock P R Polkey C E amp Morris R G (2001)lsquolsquoTheory of mindrsquorsquo impairments and their relationships toexecutive functioning following frontal lobe excisionsBrain 124 101ndash117
Rowe A D Owen A M Johnsruude I S amp Passingham R E(2001) Imaging the mental components of a planning taskNeuropsychologia 39 315ndash327
Small D M Zald D H Jones Gotman M Zatorre R JPardo J V Frey S amp Petrides M (1999) Human corticalgustatory areas A review of functional neuroimaging dataNeuroReport 10 7ndash14
Szameitat A J Torsten S Muller K amp von Cramon (2002)Localization of executive function in dual-task performancewith fMRI Journal of Cognitive Neuroscience 141184ndash1199
Thorpe S J Rolls E T amp Maddison S (1983) Neuronalactivity in the orbitofrontal cortex of the behaving monkeyExperimental Brain Research 49 93ndash115
Wise S P Murray E A amp Gerfen C R (1996) The frontalcortexndashbasal ganglia system in primates Critical Reviews inNeurobiology 10 317ndash356
Zald D H Lee J T Fluegel K W amp Pardo J V (1998)Aversive gustatory stimulation activates limbic circuits inhumans Brain 121 1143ndash1154
Zald D H amp Pardo J V (1997) Emotion olfaction and thehuman amygdala Amygdala activation during aversiveolfactory stimulation Proceedings of the National Academyof Sciences USA 94 4119ndash4124
476 Journal of Cognitive Neuroscience Volume 16 Number 3
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
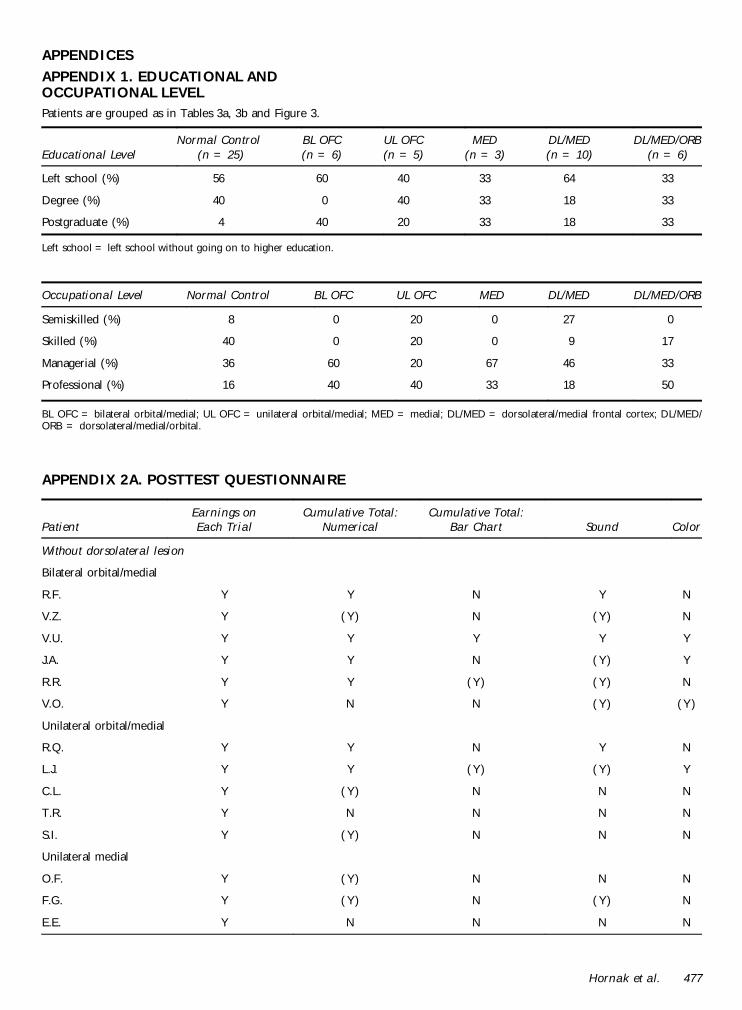
APPENDICES
APPENDIX 1 EDUCATIONAL ANDOCCUPATIONAL LEVELPatients are grouped as in Tables 3a 3b and Figure 3
Educational LevelNormal Control
(n = 25)BL OFC(n = 6)
UL OFC(n = 5)
MED(n = 3)
DLMED(n = 10)
DLMEDORB(n = 6)
Left school () 56 60 40 33 64 33
Degree () 40 0 40 33 18 33
Postgraduate () 4 40 20 33 18 33
Left school = left school without going on to higher education
Occupational Level Normal Control BL OFC UL OFC MED DLMED DLMEDORB
Semiskilled () 8 0 20 0 27 0
Skilled () 40 0 20 0 9 17
Managerial () 36 60 20 67 46 33
Professional () 16 40 40 33 18 50
BL OFC = bilateral orbitalmedial UL OFC = unilateral orbitalmedial MED = medial DLMED = dorsolateralmedial frontal cortex DLMEDORB = dorsolateralmedialorbital
APPENDIX 2A POSTTEST QUESTIONNAIRE
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
Without dorsolateral lesion
Bilateral orbitalmedial
RF Y Y N Y N
VZ Y (Y) N (Y) N
VU Y Y Y Y Y
JA Y Y N (Y) Y
RR Y Y (Y) (Y) N
VO Y N N (Y) (Y )
Unilateral orbitalmedial
RQ Y Y N Y N
LJ Y Y (Y) (Y) Y
CL Y (Y) N N N
TR Y N N N N
SI Y (Y) N N N
Unilateral medial
OF Y (Y) N N N
FG Y (Y) N (Y) N
EE Y N N N N
Hornak et al 477
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3
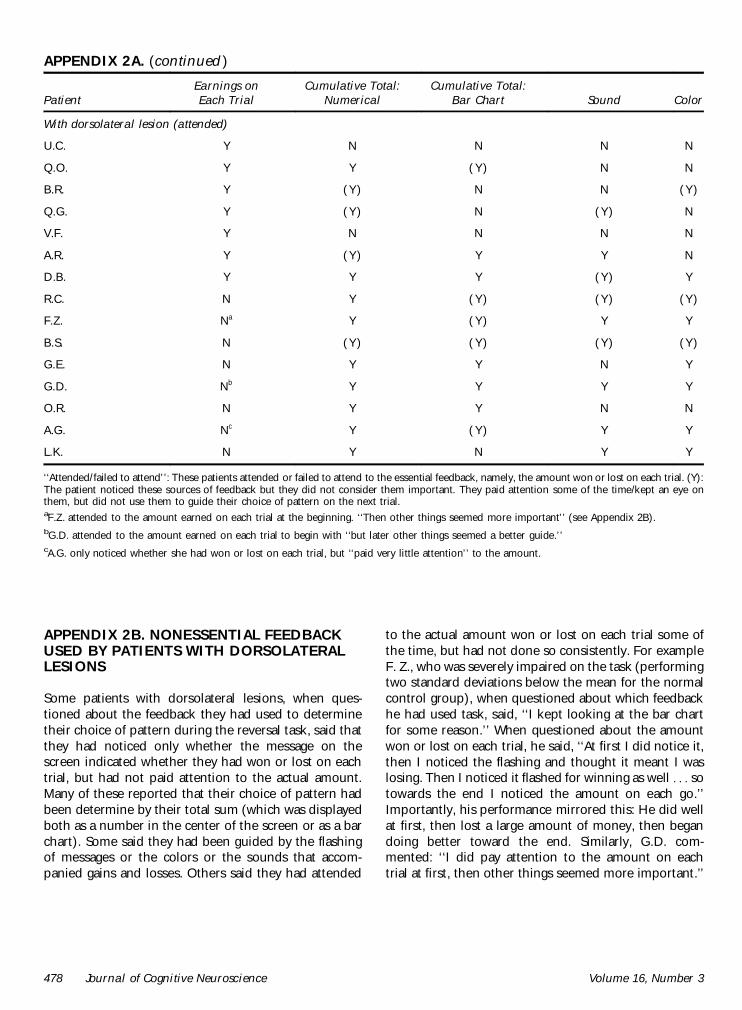
APPENDIX 2B NONESSENTIAL FEEDBACKUSED BY PATIENTS WITH DORSOLATERALLESIONS
Some patients with dorsolateral lesions when ques-tioned about the feedback they had used to determinetheir choice of pattern during the reversal task said thatthey had noticed only whether the message on thescreen indicated whether they had won or lost on eachtrial but had not paid attention to the actual amountMany of these reported that their choice of pattern hadbeen determine by their total sum (which was displayedboth as a number in the center of the screen or as a barchart) Some said they had been guided by the flashingof messages or the colors or the sounds that accom-panied gains and losses Others said they had attended
to the actual amount won or lost on each trial some ofthe time but had not done so consistently For exampleF Z who was severely impaired on the task (performingtwo standard deviations below the mean for the normalcontrol group) when questioned about which feedbackhe had used task said lsquolsquoI kept looking at the bar chartfor some reasonrsquorsquo When questioned about the amountwon or lost on each trial he said lsquolsquoAt first I did notice itthen I noticed the flashing and thought it meant I waslosing Then I noticed it flashed for winning as well sotowards the end I noticed the amount on each gorsquorsquoImportantly his performance mirrored this He did wellat first then lost a large amount of money then begandoing better toward the end Similarly GD com-mented lsquolsquoI did pay attention to the amount on eachtrial at first then other things seemed more importantrsquorsquo
APPENDIX 2A (continued )
PatientEarnings onEach Trial
Cumulative TotalNumerical
Cumulative TotalBar Chart Sound Color
With dorsolateral lesion (attended)
UC Y N N N N
QO Y Y (Y) N N
BR Y (Y) N N (Y)
QG Y (Y) N (Y) N
VF Y N N N N
AR Y (Y) Y Y N
DB Y Y Y (Y) Y
RC N Y (Y) (Y) (Y)
FZ Na Y (Y) Y Y
BS N (Y) (Y) (Y) (Y)
GE N Y Y N Y
GD Nb Y Y Y Y
OR N Y Y N N
AG Nc Y (Y) Y Y
LK N Y N Y Y
lsquolsquoAttendedfailed to attendrsquorsquo These patients attended or failed to attend to the essential feedback namely the amount won or lost on each trial (Y)The patient noticed these sources of feedback but they did not consider them important They paid attention some of the timekept an eye onthem but did not use them to guide their choice of pattern on the next trialaFZ attended to the amount earned on each trial at the beginning lsquolsquoThen other things seemed more importantrsquorsquo (see Appendix 2B)bGD attended to the amount earned on each trial to begin with lsquolsquobut later other things seemed a better guidersquorsquocAG only noticed whether she had won or lost on each trial but lsquolsquopaid very little attentionrsquorsquo to the amount
478 Journal of Cognitive Neuroscience Volume 16 Number 3