respiratory toxicity of maintenance therapy in drug ...€¦ · [email protected]...
TRANSCRIPT
1
Bruno Mégarbane, MD, PhD
Department of toxicological and medical critical care, Lariboisière
Hospital, INSERM U705, Paris-Diderot University
Paris, France
Respiratory toxicity of maintenance
therapy in drug addicts:
contribution of animal models
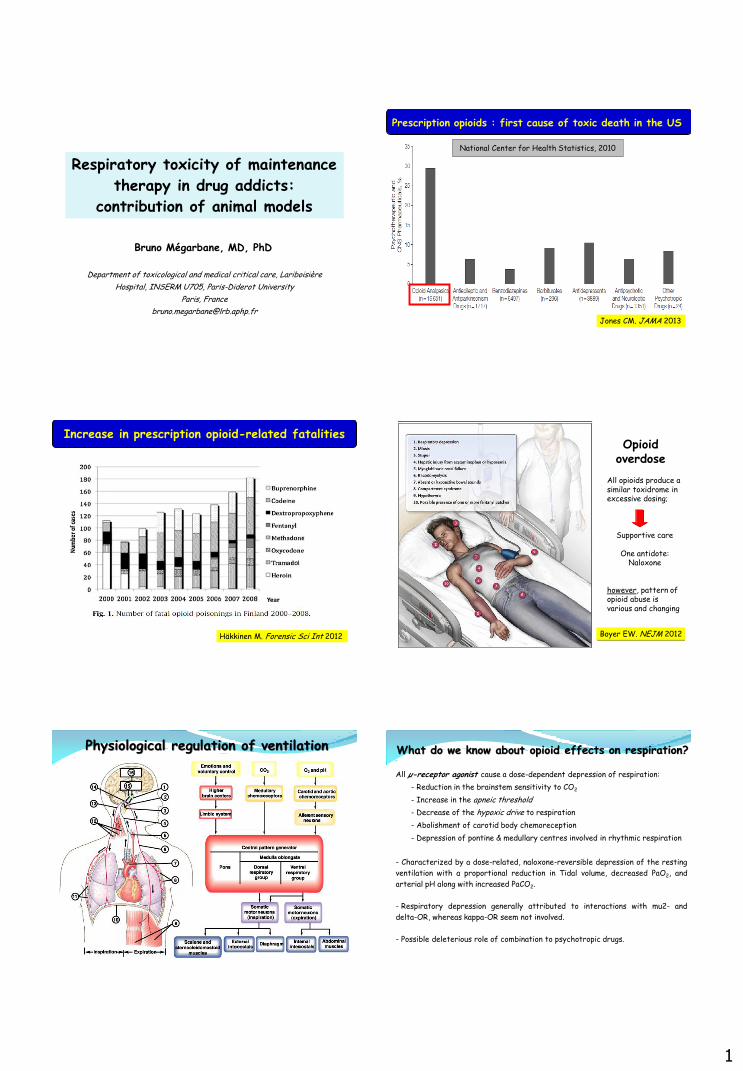
Prescription opioids : first cause of toxic death in the US
Jones CM. JAMA 2013
National Center for Health Statistics, 2010
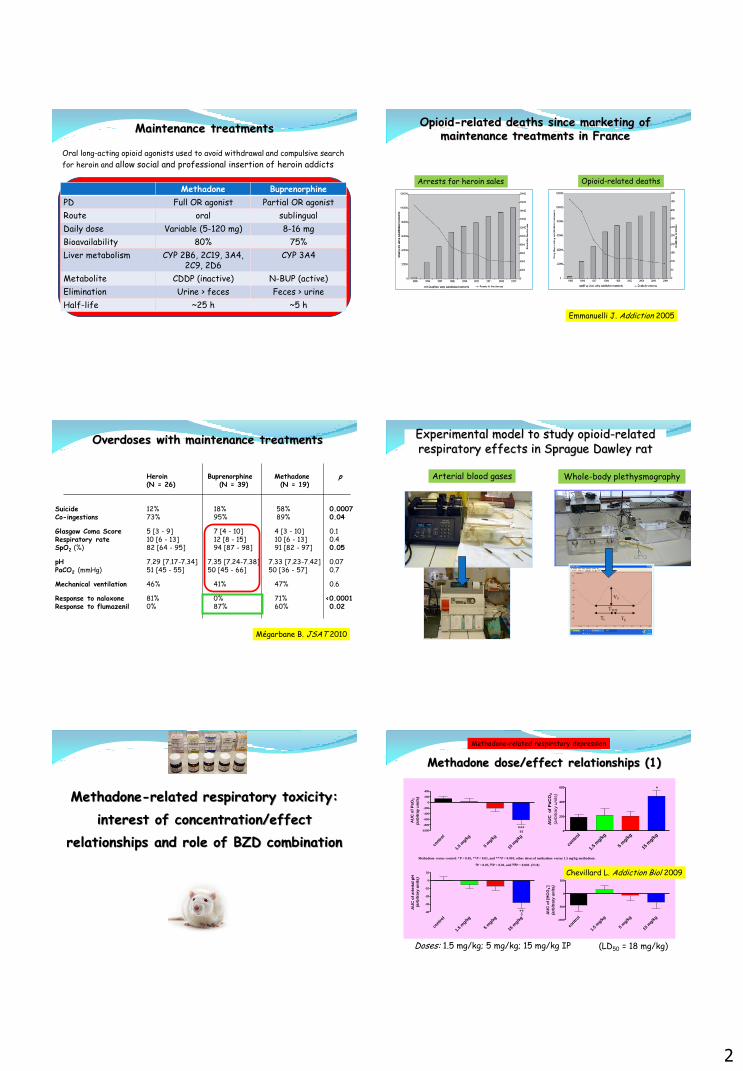
Increase in prescription opioid-related fatalities
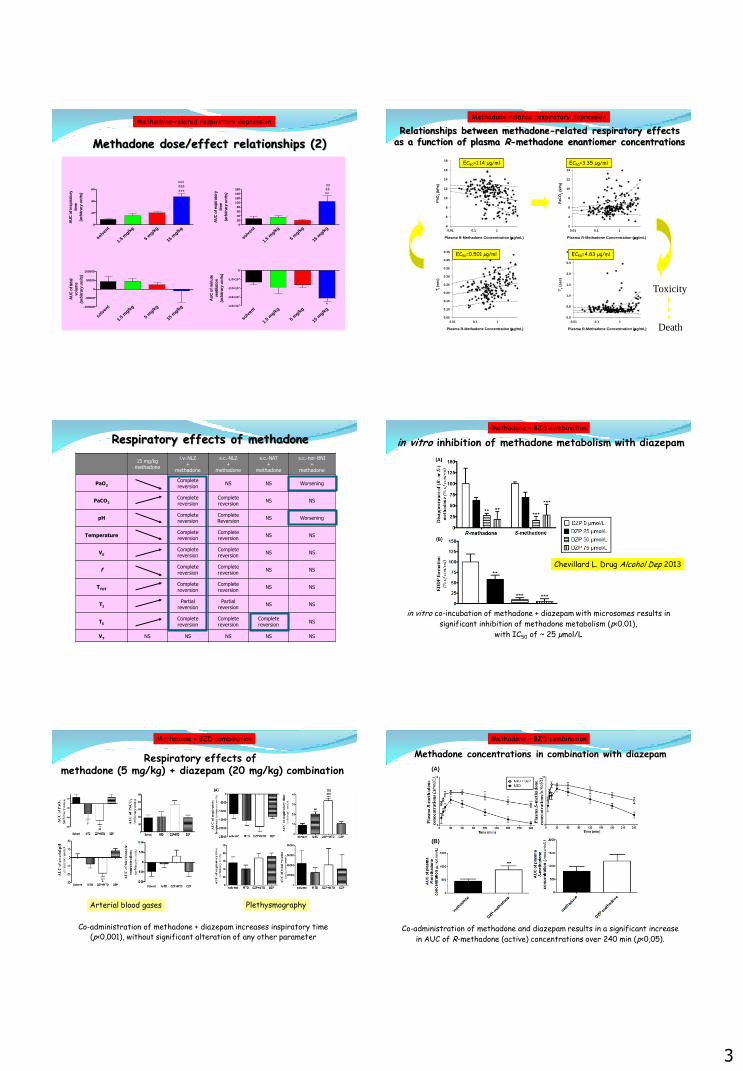
Häkkinen M. Forensic Sci Int 2012 Boyer EW. NEJM 2012
Opioid overdose
All opioids produce a similar toxidrome in excessive dosing;
Supportive care
One antidote:
Naloxone
however, pattern of opioid abuse is various and changing
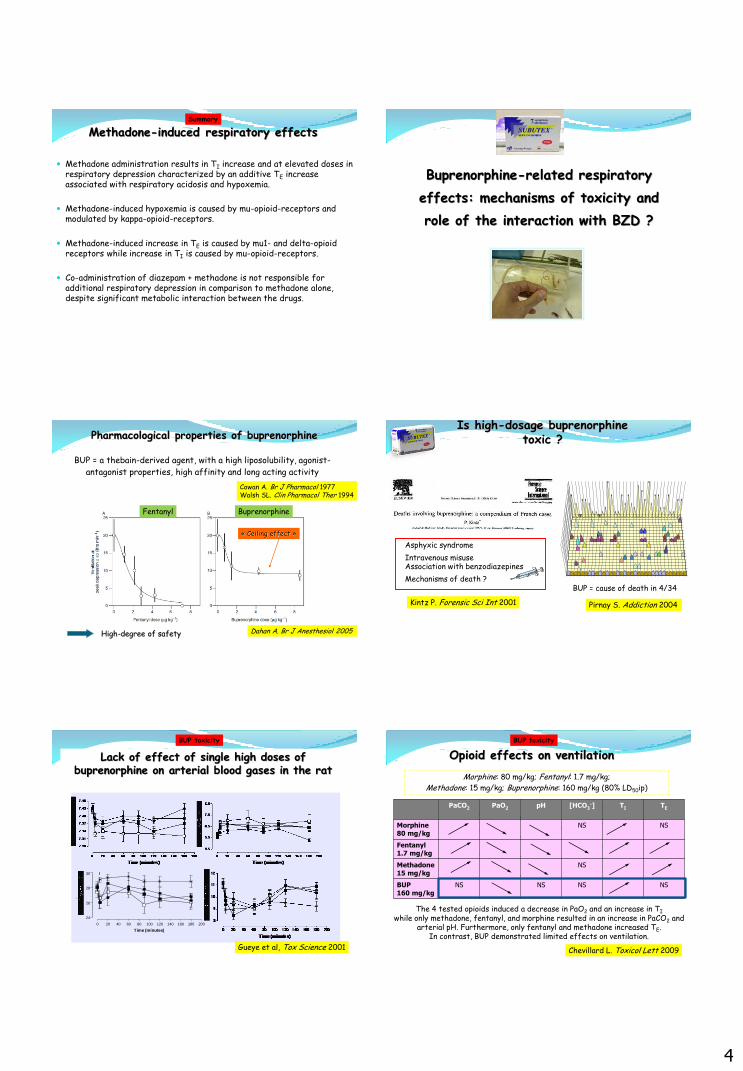
Physiological regulation of ventilation
All µ-receptor agonist cause a dose-dependent depression of respiration:
- Reduction in the brainstem sensitivity to CO2
- Increase in the apneic threshold
- Decrease of the hypoxic drive to respiration
- Abolishment of carotid body chemoreception
- Depression of pontine & medullary centres involved in rhythmic respiration
- Characterized by a dose-related, naloxone-reversible depression of the resting
ventilation with a proportional reduction in Tidal volume, decreased PaO2, and
arterial pH along with increased PaCO2.
- Respiratory depression generally attributed to interactions with mu2- and
delta-OR, whereas kappa-OR seem not involved.
- Possible deleterious role of combination to psychotropic drugs.
What do we know about opioid effects on respiration?
2
Maintenance treatments
Methadone Buprenorphine
PD Full OR agonist Partial OR agonist
Route oral sublingual
Daily dose Variable (5-120 mg) 8-16 mg
Bioavailability 80% 75%
Liver metabolism CYP 2B6, 2C19, 3A4, 2C9, 2D6
CYP 3A4
Metabolite CDDP (inactive) N-BUP (active)
Elimination Urine > feces Feces > urine
Half-life ~25 h ~5 h
Oral long-acting opioid agonists used to avoid withdrawal and compulsive search
for heroin and allow social and professional insertion of heroin addicts
Emmanuelli J. Addiction 2005
Arrests for heroin sales Opioid-related deaths
Opioid-related deaths since marketing of maintenance treatments in France
Overdoses with maintenance treatments
Heroin Buprenorphine Methadone p
(N = 26) (N = 39) (N = 19) Suicide 12% 18% 58% 0.0007 Co-ingestions 73% 95% 89% 0.04
Glasgow Coma Score 5 [3 - 9] 7 [4 - 10] 4 [3 - 10] 0.1 Respiratory rate 10 [6 - 13] 12 [8 - 15] 10 [6 - 13] 0.4 SpO2 (%) 82 [64 - 95] 94 [87 - 98] 91 [82 - 97] 0.05
pH 7.29 [7.17-7.34] 7.35 [7.24-7.38] 7.33 [7.23-7.42] 0.07 PaCO2 (mmHg) 51 [45 - 55] 50 [45 - 66] 50 [36 - 57] 0.7
Mechanical ventilation 46% 41% 47% 0.6
Response to naloxone 81% 0% 71% <0.0001 Response to flumazenil 0% 87% 60% 0.02
Mégarbane B. JSAT 2010
Whole-body plethysmography
Experimental model to study opioid-related respiratory effects in Sprague Dawley rat
VT
TTOT
TI TE
Arterial blood gases
Methadone-related respiratory toxicity:
interest of concentration/effect
relationships and role of BZD combination
Methadone dose/effect relationships (1)
Methadone-related respiratory depression
contr
ol
1.5
mg/k
g
5 m
g/kg
15 m
g/kg
-1000
-800
-600
-400
-200
0
200
400
***§§
AU
C o
f P
aO
2
(arb
itra
y u
nit
s)
contr
ol
1.5
mg/k
g
5 m
g/kg
15 m
g/kg
0
200
400
600 *
AU
C
of
Pa
CO
2
(arb
itra
ry u
nits)
contr
ol
1.5
mg/k
g
5 m
g/kg
15 m
g/kg
-40
-30
-20
-10
0
10
**§
AU
C o
f a
rte
ria
l p
H
(arb
itra
ry u
nit
s)
contr
ol
1.5
mg/k
g
5 m
g/kg
15 m
g/kg
-1000
-500
0
500
AU
C o
f [H
CO
3- ]
(arb
itra
ry u
nit
s)
Methadone versus control: *P < 0.05, **P < 0.01, and ***P < 0.001; other doses of methadone versus 1.5 mg/kg methadone:
§P < 0.05, §§P < 0.01, and §§§P < 0.001. (N=8)
(LD50 = 18 mg/kg) Doses: 1.5 mg/kg; 5 mg/kg; 15 mg/kg IP
Chevillard L. Addiction Biol 2009
3
solv
ent
1.5
mg/k
g
5 m
g/kg
15 m
g/kg
0
20
40
60***
§§§
###
AU
C o
f in
sp
irato
ry
tim
e
(arb
itra
ry u
nit
s)
solv
ent
1.5
mg/k
g
5 m
g/kg
15 m
g/kg
0
20
40
60
80
100
120
140
160
**§§##
AU
C o
f exp
irato
ry
tim
e
(arb
itra
ry u
nit
s)
solv
ent
1.5
mg/k
g
5 m
g/kg
15 m
g/kg-100000
-50000
0
50000
100000
AU
C o
f tid
al
vo
lum
e
(arb
itra
ry u
nit
s)
solv
ent
1.5
mg/k
g
5 m
g/kg
15 m
g/kg
-4.0×10 7
-3.0×10 7
-2.0×10 7
-1.0×10 7
0
*
AU
C o
f m
inu
te
ven
tila
tio
n
(arb
itra
ry u
nit
s)
Methadone dose/effect relationships (2)
Methadone-related respiratory depression
Relationships between methadone-related respiratory effects as a function of plasma R-methadone enantiomer concentrations
Plasma R-Methadone Concentration (g/mL)
0.01 0.1 1
Pa
O2 (
kP
a)
4
6
8
10
12
14
16
18
Plasma R-Methadone Concentration (g/mL)
0.01 0.1 1
Pa
CO
2 (
kP
a)
2
4
6
8
10
12
14
16
Plasma R-Methadone Concentration (g/mL)
0.01 0.1 1
Ti (
sec
)
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
Plasma R-Methadone Concentration (g/mL)
0.01 0.1 1
Te (
se
c)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
EC50=1.14 µg/ml EC50=3.35 µg/ml
EC50=0.501 µg/ml EC50=4.83 µg/ml
Toxicity
Death
Methadone-related respiratory depression
Respiratory effects of methadone
15 mg/kg methadone
i.v.-NLZ +
methadone
s.c.-NLZ +
methadone
s.c.-NAT +
methadone
s.c.-nor-BNI +
methadone
PaO2 Complete reversion
NS NS Worsening
PaCO2 Complete reversion
Complete reversion
NS NS
pH Complete reversion
Complete Reversion
NS Worsening
Temperature Complete reversion
Complete reversion
NS NS
VE Complete reversion
Complete reversion
NS NS
f Complete reversion
Complete reversion
NS NS
TTOT Complete reversion
Complete reversion
NS NS
TI Partial
reversion Partial
reversion NS NS
TE Complete reversion
Complete reversion
Complete reversion
NS
VT NS NS NS NS NS
in vitro inhibition of methadone metabolism with diazepam
in vitro co-incubation of methadone + diazepam with microsomes results in
significant inhibition of methadone metabolism (p<0.01),
with IC50 of ~ 25 µmol/L
Chevillard L. Drug Alcohol Dep 2013
Methadone + BZD combination
Respiratory effects of methadone (5 mg/kg) + diazepam (20 mg/kg) combination
Arterial blood gases Plethysmography
Co-administration of methadone + diazepam increases inspiratory time (p<0,001), without significant alteration of any other parameter
Methadone + BZD combination
(A)
(B)
Methadone concentrations in combination with diazepam
Co-administration of methadone and diazepam results in a significant increase
in AUC of R-methadone (active) concentrations over 240 min (p<0,05).
Methadone + BZD combination
4
Methadone-induced respiratory effects
Methadone administration results in TI increase and at elevated doses in respiratory depression characterized by an additive TE increase associated with respiratory acidosis and hypoxemia.
Methadone-induced hypoxemia is caused by mu-opioid-receptors and modulated by kappa-opioid-receptors.
Methadone-induced increase in TE is caused by mu1- and delta-opioid receptors while increase in TI is caused by mu-opioid-receptors.
Co-administration of diazepam + methadone is not responsible for additional respiratory depression in comparison to methadone alone, despite significant metabolic interaction between the drugs.
Summary
Buprenorphine-related respiratory
effects: mechanisms of toxicity and
role of the interaction with BZD ?
Pharmacological properties of buprenorphine
High-degree of safety
Cowan A. Br J Pharmacol 1977 Walsh SL. Clin Pharmacol Ther 1994
BUP = a thebain-derived agent, with a high liposolubility, agonist-
antagonist properties, high affinity and long acting activity
Dahan A. Br J Anesthesiol 2005
« Ceiling effect »
Fentanyl Buprenorphine
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34
BUPRENORPHINE
LEVOMEPROMAZINE
BROMAZEPAM
PARACETAMOL
CODEINE
METHADONE
CYAMEMAZINE (toxique et létal)
MEPROBAMATE (létal)l
PHENOBARBITAL (létal)
COCAINE (letal)
PROPOXYPHENE (létal)
ALCOOL sup 0.3 g/l
PATHOLOGIE IMPORTANTE
CONTEXTE JUDICIAIRE
MORPHINE
ACEPROMETAZINE (létal)
HEROINE (létal)
PETHIDINE
ALIMEMAZINE
CLOMIPRAMINE (létal)
AUTRES DROGUES ASSOCIEES A TAUX NON TOXIQUE
5
3
0
4 4
3
1 1
0
1
2
8
5
1 1
5
44
11
5
22
55
3
8
4
6
7
2
3
5
3
Pirnay S. Addiction 2004
BUP = cause of death in 4/34
Is high-dosage buprenorphine toxic ?
Asphyxic syndrome
Intravenous misuse Association with benzodiazepines
Mechanisms of death ?
Kintz P. Forensic Sci Int 2001
0 20 40 60 80 100 120 140 160 180 200
24
26
28
30
Time (minutes)
Lack of effect of single high doses of buprenorphine on arterial blood gases in the rat
BUP toxicity
Gueye et al, Tox Science 2001
Opioid effects on ventilation
Morphine: 80 mg/kg; Fentanyl: 1.7 mg/kg;
Methadone: 15 mg/kg; Buprenorphine: 160 mg/kg (80% LD50ip)
NS NS NS NS BUP 160 mg/kg
NS Methadone 15 mg/kg
Fentanyl 1.7 mg/kg
NS NS Morphine 80 mg/kg
TE TI [HCO3-] pH PaO2 PaCO2
The 4 tested opioids induced a decrease in PaO2 and an increase in TI
while only methadone, fentanyl, and morphine resulted in an increase in PaCO2 and arterial pH. Furthermore, only fentanyl and methadone increased TE.
In contrast, BUP demonstrated limited effects on ventilation.
Chevillard L. Toxicol Lett 2009
BUP toxicity
5
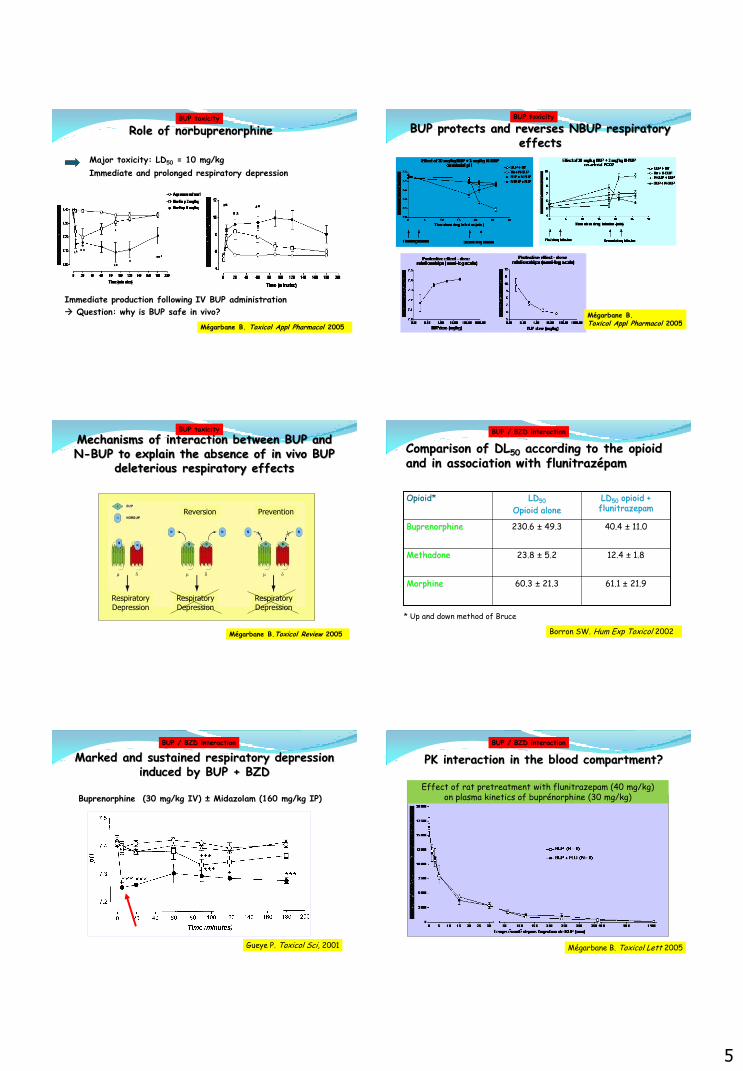
Role of norbuprenorphine
Major toxicity: LD50 = 10 mg/kg
Immediate and prolonged respiratory depression
Immediate production following IV BUP administration
Question: why is BUP safe in vivo?
Mégarbane B. Toxicol Appl Pharmacol 2005
BUP toxicity
Mégarbane B. Toxicol Appl Pharmacol 2005
BUP protects and reverses NBUP respiratory effects
BUP toxicity
Mechanisms of interaction between BUP and N-BUP to explain the absence of in vivo BUP
deleterious respiratory effects
Reversion Prevention
Respiratory Depression
Respiratory Depression
Respiratory Depression
Mégarbane B.Toxicol Review 2005
BUP toxicity
Comparison of DL50 according to the opioid and in association with flunitrazépam
61.1 ± 21.9
60.3 ± 21.3 Morphine
12.4 ± 1.8
23.8 ± 5.2 Methadone
40.4 ± 11.0
230.6 ± 49.3 Buprenorphine
LD50 opioid + flunitrazepam
LD50
Opioid alone
Opioid*
* Up and down method of Bruce
Borron SW. Hum Exp Toxicol 2002
BUP / BZD interaction
Buprenorphine (30 mg/kg IV) ± Midazolam (160 mg/kg IP)
Gueye P. Toxicol Sci, 2001
Marked and sustained respiratory depression induced by BUP + BZD
BUP / BZD interaction
Effect of rat pretreatment with flunitrazepam (40 mg/kg) on plasma kinetics of buprénorphine (30 mg/kg)
PK interaction in the blood compartment?
Mégarbane B. Toxicol Lett 2005
BUP / BZD interaction
6
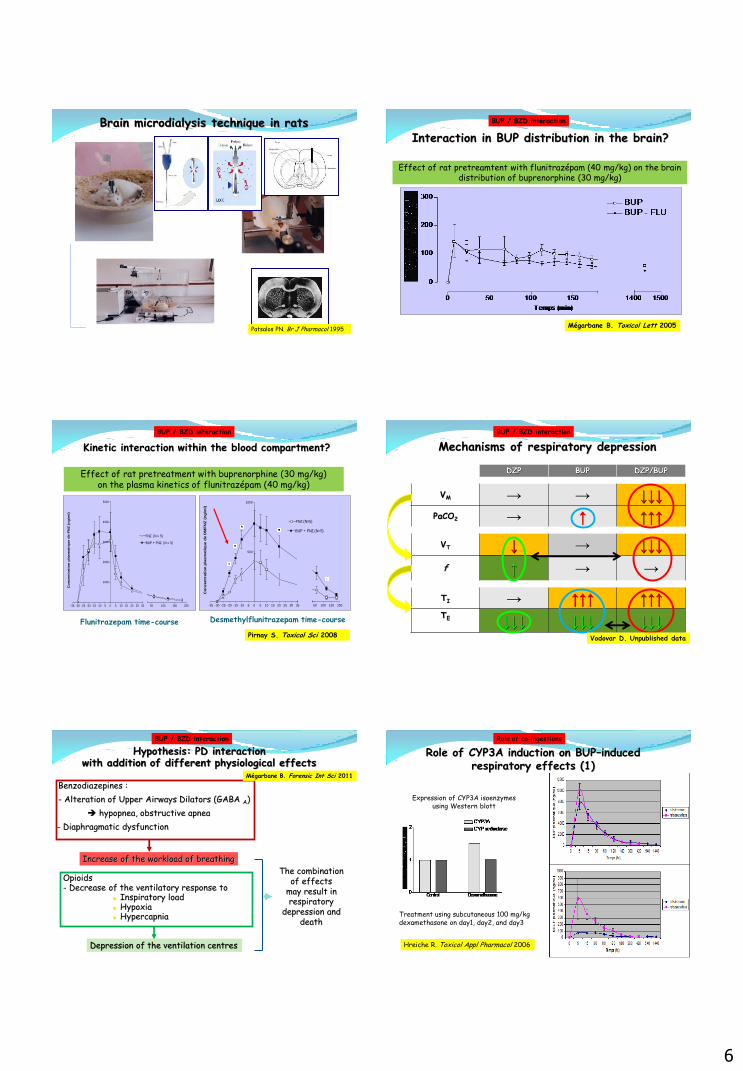
Brain microdialysis technique in rats
a
. Patsalos PN. Br J Pharmacol 1995
Effect of rat pretreamtent with flunitrazépam (40 mg/kg) on the brain distribution of buprenorphine (30 mg/kg)
Interaction in BUP distribution in the brain?
Mégarbane B. Toxicol Lett 2005
BUP / BZD interaction
Effect of rat pretreatment with buprenorphine (30 mg/kg) on the plasma kinetics of flunitrazépam (40 mg/kg)
Flunitrazepam time-course Desmethylflunitrazepam time-course
-35 -30 -25 -20 -15 -10 -5 0 5 10 15 20 25 30
1000
2000
3000
4000
5000
FNZ (N = 5)
BUP + FNZ (N = 5)
50 100 150 200
Co
ncen
trati
on
pla
sm
ati
qu
e d
e F
NZ
(n
g/m
l)
-35 -30 -25 -20 -15 -10 -5 0 5 10 15 20 25 30 35
500
1000
FNZ (N=5)
BUP + FNZ (N=5)
50 100 150 200
Co
ncen
trati
on
pla
sm
ati
qu
e d
e D
MF
NZ
(n
g/m
l)
Kinetic interaction within the blood compartment?
Pirnay S. Toxicol Sci 2008
BUP / BZD interaction
DZP BUP DZP/BUP
VM → → ↓↓↓ PaCO2 → ↑ ↑↑↑
VT ↓ → ↓↓↓
f ↑ → →
TI → ↑↑↑ ↑↑↑ TE
↓↓↓ ↓↓↓ ↓↓↓
Mechanisms of respiratory depression
Vodovar D. Unpublished data
BUP / BZD interaction
Benzodiazepines :
- Alteration of Upper Airways Dilators (GABA A)
hypopnea, obstructive apnea
- Diaphragmatic dysfunction
The combination of effects
may result in respiratory
depression and death
Hypothesis: PD interaction with addition of different physiological effects
Opioids - Decrease of the ventilatory response to
Inspiratory load Hypoxia Hypercapnia
Increase of the workload of breathing
Depression of the ventilation centres
Mégarbane B. Forensic Int Sci 2011
BUP / BZD interaction
Treatment using subcutaneous 100 mg/kg dexamethasone on day1, day2, and day3
Expression of CYP3A isoenzymes using Western blott
Hreiche R. Toxicol Appl Pharmacol 2006
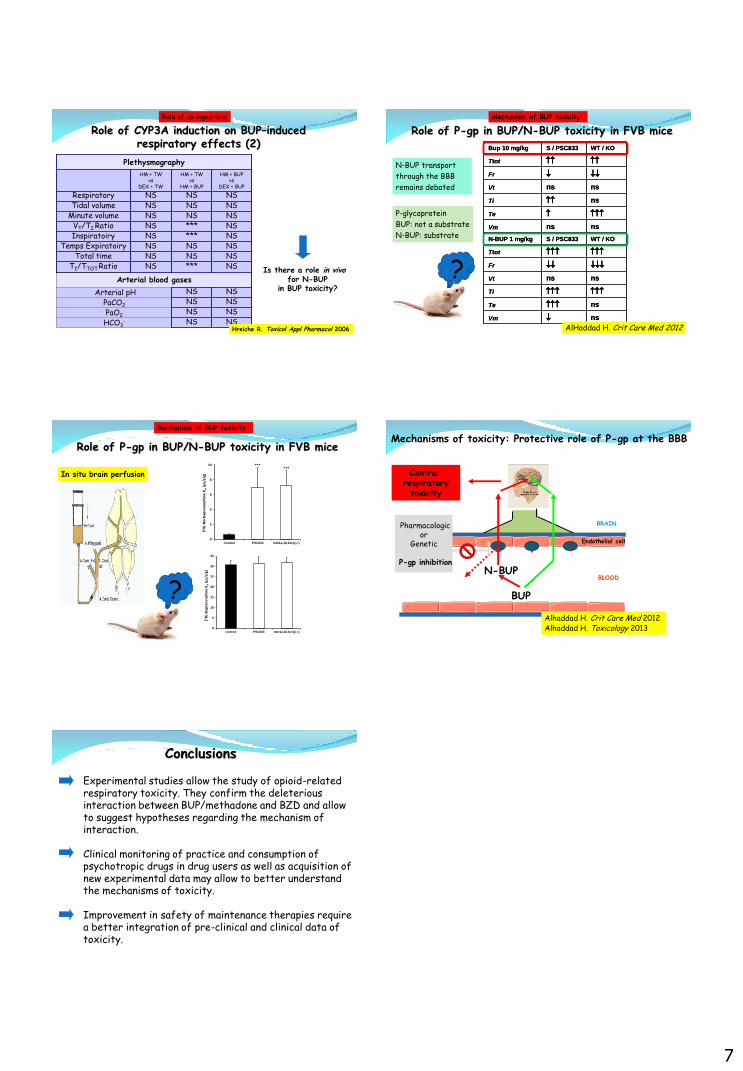
Role of CYP3A induction on BUP–induced respiratory effects (1)
Role of co-ingestions
7
NS NS HCO3-
NS NS PaO2
NS NS PaCO2
NS NS Arterial pH
Arterial blood gases
NS *** NS TI/TTOT Ratio NS NS NS Total time NS NS NS Temps Expiratoiry NS *** NS
Temps Inspiratoiry
NS *** NS VT/TI Ratio NS NS NS Minute volume NS NS NS Tidal volume NS NS NS
Fréquence Respiratory
HM + BUP vs
DEX + BUP
HM + TW vs
HM + BUP
HM + TW vs
DEX + TW
Plethysmography
Is there a role in vivo for N-BUP
in BUP toxicity?
Hreiche R. Toxicol Appl Pharmacol 2006
Role of CYP3A induction on BUP–induced respiratory effects (2)
Role of co-ingestions
nsVm
nsTe
Ti
nsnsVt
Fr
Ttot
WT / KOS / PSC833N-BUP 1 mg/kg
nsnsVm
Te
nsTi
nsnsVt
Fr
Ttot
WT / KOS / PSC833Bup 10 mg/kg
nsVm
nsTe
Ti
nsnsVt
Fr
Ttot
WT / KOS / PSC833N-BUP 1 mg/kg
nsnsVm
Te
nsTi
nsnsVt
Fr
Ttot
WT / KOS / PSC833Bup 10 mg/kg
Role of P-gp in BUP/N-BUP toxicity in FVB mice
AlHaddad H. Crit Care Med 2012
Mechanism of BUP toxicity
P-glycoprotein
BUP: not a substrate
N-BUP: substrate
N-BUP transport
through the BBB
remains debated
?
Role of P-gp in BUP/N-BUP toxicity in FVB mice
Mechanism of BUP toxicity
? 0
5
10
15
20
25
30
35
Control PSC833 mdr1a,1b,bcrp(-/-)
[3H
]-B
up
ren
orp
hin
e K
in(µ
L/s/
g)
0
2
4
6
8
10
Control PSC833 mdr1a,1b,bcrp(-/-)
[3H
]-N
orb
up
ren
orp
hin
e K
in(µ
L/s/
g)
******
In situ brain perfusion
Endothelial cell
BLOOD
BRAIN
Mechanisms of toxicity: Protective role of P-gp at the BBB
BUP
Pharmacological effect
N-BUP
Alhaddad H. Crit Care Med 2012 Alhaddad H. Toxicology 2013
Central respiratory toxicity
Pharmacologic or
Genetic
P-gp inhibition
Conclusions
Experimental studies allow the study of opioid-related respiratory toxicity. They confirm the deleterious interaction between BUP/methadone and BZD and allow to suggest hypotheses regarding the mechanism of interaction. Clinical monitoring of practice and consumption of psychotropic drugs in drug users as well as acquisition of new experimental data may allow to better understand the mechanisms of toxicity. Improvement in safety of maintenance therapies require a better integration of pre-clinical and clinical data of toxicity.