research estimating mortality, morbidity and disability due to
TRANSCRIPT

Research
Estimating mortality, morbidity and disabilitydue to malaria among Africa's non-pregnantpopulationR.W. Snow,1, 2 M. Craig,3 U. Deichmann,4 & K. Marsh2, 5
The contribution of malaria to morbidity and mortality among people in Africa has been a subject of academic interest,political advocacy, and speculation. National statistics for much of sub-Saharan Africa have proved to be an unreliablesource of disease-specific morbidity and mortality data. Credible estimates of disease-specific burdens are required forsetting global and national priorities for health in order to rationalize the use of limited resources and lobby for financialsupport. We have taken an empirical approach to defining the limits of Plasmodium falciparum transmission across thecontinent and interpolated the distributions of projected populations in 1995. By combining a review of the literatureon malaria in Africa and models of acquired functional immunity, we have estimated the age-structured rates of thefatal, morbid and disabling sequelae following exposure to malaria infection under different epidemiologicalconditions.
Voir page 636 le re sume en francËais. En la pa gina 636 figura un resumen en espanÄ ol
Introduction
The available health information for much of sub-Saharan Africa is of very poor quality. As a result,estimates of the health impact of diseases suchas malaria have swung between semi-informedguesses and wild speculation. Previous estimates of0.5±2 million deaths from malaria in Africa each year(1±5) have proved to be a useful advocacy tool, butthere has been scepticism about their origin andvalidity. Evidence-based approaches provide greatercredibility to disease control initiatives. Following20 years of disillusionment on the part of the publichealth sector towards malaria control there is anurgent need to improve credibility for the new era of``roll back'' malaria (6).
Recognizing the limitations of national statis-tics, we have focused on the epidemiologicalassociations between climate and the likelihood of
stable Plasmodium falciparum transmission, empiricalsurvey-derived estimates of disease risks linked toepidemiological features of acquired immunity, andinterpolated models of population distribution inAfrica. This work is an extension of previous effortsto combine transmission risks, malaria mortality data,and population data for 1990 (7) with a refined effortat disease-risk and population stratification, a widerrange of empirical data, and a consideration ofburdens other than mortality among the 1995 non-pregnant population of Africa.
Data and methods
Climate suitability for P. falciparumtransmissionMalaria is governed by a large number of environ-mental factors, which affect its distribution, season-ality, and transmission intensity. The Anopheles gambiaecomplex is the major vector system in Africa andexists only in frost-free regions (8), or where theminimum temperature in winter remains above 5 oC(9). Temperature affects the transmission cycle ofP. falciparum in many different ways, but the effectson the duration of the sporogonic cycle of theparasite and vector survival are particularly impor-tant. At temperatures below about 22 oC thedetermining factor is the number of mosquitossurviving the parasite's incubation period, whichtakes 55 days at 18 oC (10) and ceases at around 16 oC.After 55 days the proportion of a cohort ofmosquitos that survives is only 0.003 (11).
1 Kenya Medical Research Institute (KEMRI)/Wellcome Trust,Collaborative Programme, P.O.Box 43460, Nairobi, Kenya(e-mail: [email protected]). Correspondence should be sent toDr R.W. Snow at this address.2 Department of Tropical Medicine, University of Oxford, John RadcliffeHospital, Headington, Oxford, England.3 National Malaria Research Programme, South African MedicalResearch Council, Congella, Durban, South Africa.4 National Center for Geographic Information and Analysis, Universityof California, Santa Barbara, CA, USA.5 Centre for Geographic Medicine, KEMRI, Kilifi, Kenya.
Reprint No. 0029
624 # World Health Organization 1999 Bulletin of the World Health Organization, 1999, 77 (8)

Rainfall provides breeding sites for mosquitosand increases the humidity, which enhances theirsurvival; the overall relationship between mosquitoabundance and rainfall has been illustrated repeatedly(12, 13). We have examined rainfall patterns in knownmalaria and non-malarious areas; an average of80 mm per month, for at least 3±5 months, is aminimum for stable malaria transmission (14).
In our work, a combination of temperature andrainfall has been used to define the vector andparasite viability for transmission within fixedseasonal windows of time. Fuzzy logic models (15)have been used to define the suitability for stablemalaria transmission across the continent at approxi-mately a 5 x 5 km resolution (14). In our model,climate data were derived from weather station datafor the period 1920 to 1980 (16) and wereinterpolated into mean monthly temperature andrainfall surfaces. The model was structured to definedistribution by setting the lower temperature cut-offat 18 oC and assuming a saturation of the temperatureeffect by 22 oC; similarly, rainfall values of 0±80 mmdemarcate the range within which transmission islimited. When combined, these features mustcoincide on a month-to-month basis for fiveconsecutive months, and a frost factor (minimumtemperature, <5 oC) would eliminate transmission atany point in a contiguous period. In North Africa, acombination of high temperatures with a rapid onsetof a short duration of rainfall allows for a limitedtransmission period of <3 months. The model wasmodified to allow for 3-month conditions for NorthAfrican areas. The model (Fig. 1) accommodates``fuzzy'' membership, or climate suitability values,ranging from 0 (unsuitable) to 1 (very suitable).Overall, the model compares well with both expertopinion maps developed between 1930 and 1960 forsouthern and East Africa and empirical parasito-logical survey data (MARA/ARMA Collaboration,unpublished observations, 1999). Because the modelis based upon long-term climatic averages, it providesa conservative estimate of stable transmissiondistribution and does not allow for epidemicpotentials among areas where transmission istraditionally limited by either rainfall or temperature.Furthermore, comparisons with expert-opinionmaps indicate that discrepancies in major river valleysresult because the model uses only rainfall to predictwater availability, while mosquitos do survive alongmajor river banks and flood plains.
Epidemiological stratification
North AfricaNorth Africa is densely populated along theMediterranean and Moroccan coast; however, themajority of these areas do not support stablePlasmodium falciparum transmission as defined throughthe fuzzy climate suitability model (Fig. 1). Inaddition, the WHO regional offices covering theseareas reported no cases of malaria mortality during
the 1995 period. These countries (Algeria, Egypt,Libyan Arab Jamahiriya, Morocco, and Tunisia) havebeen excluded from the analysis of malaria diseaseburden in Africa.
Areas of sub-Saharan Africaunsuitable for stable transmissionThe climate model described above provides a rangeof suitability estimates for stable transmission(transmission and/or new clinical cases every year).Areas classified as zero suitability are extremelyunlikely to support transmission of Plasmodiumfalciparum on an average year either on the basis oflow ambient temperatures or inadequate rainfall.Many of these areas are located at high altitude(serving as a proxy for low temperature) in EastAfrica and the Horn of Africa and among the ariddeserts at the juncture of Kenya, Ethiopia andSomalia. It must be recognized, however, that chanceepidemics could occur in these areas although theyare unlikely. In addition, Africa's population isincredibly mobile constituting a risk among migrantsfrom these areas to areas of stable or epidemictransmission.
Areas of unstable, epidemic or fringemalaria transmissionPreviously we have used a 0.5 climate suitability indexto define the limits of stable malaria transmission inAfrica (7). While this corresponds well to historically
Fig. 1. Climate suitability model for Africa derived using fuzzyprobability. Regions in dark grey are very suitable for stable Plasmodiumfalciparum transmission and regions in white are highly unsuitable for stabletransmission (14). Map courtesy of MARA (Mapping Malaria Risk in AfricaInternational Collaboration).
Malaria mortality, morbidity and disability in Africa
625Bulletin of the World Health Organization, 1999, 77 (8)

defined boundaries of transmission in southernAfrica (14), it is too exclusive for areas in East Africa.For the present analysis we selected 0.5 as theboundary for stable transmission in southern Africaand 0.2 for the rest of Africa. This arbitraryclassification is supported by empirical observationsand historical ``expert'' opinion maps from SouthAfrica, Kenya and the United Republic of Tanzania.Among areas located within the climate suitabilityclassification of greater than zero but less than 0.5 forsouthern Africa and less than 0.2 for the rest of sub-Saharan Africa, the overall risks of disease and deathare dependent upon large between-year changes inclimate providing an unusual window of transmissionsuitability. The typology of these areas variesaccording to whether the transmission potential isreached due to exceptional rainfall and floodingamong traditionally hot, arid areas or whether smallvariations in temperature in traditionally wet areaspermit transmission. Epidemiological definitions ofunstable or epidemic malaria do not reflect the publichealth significance of the disease for these regions ofAfrica. An underlying principle for the clinicalpatterns of disease and mortality among these``fringe'' populations is that risks are equivalentamong all age groups owing to a lack of functionalimmunity acquired through repeated parasite ex-posure. A recent analysis of the ratio adult:childhoodmalaria admissions to over 50 hospital settings inKenya indicates that, among communities locatedwithin the fuzzy climate suitability regions of less than0.2, over 90% of the adult:child admission ratiosexceed 1 (Snow et al., in preparation). This provides ajustification for the selection of this climate suitabilityindex as defining a special epidemiological situationfor these ``fringe'' areas.
Areas of stable P. falciparum transmissionThe sub-Saharan areas (excluding North Africa andsouthern Africa), which lie within the arbitrary limitsof climate suitability greater than or equal to 0.2, havebeen defined as able to support stable P. falciparum
transmission. This area encompasses a wide range ofendemicities. For the present analysis we haveassumed an equivalent disease and mortality riskacross the wide range of stable endemicitiessupported in Africa. Clearly this will lead to anoverestimate of disease burden where low, stableendemic areas are treated equally with more intensetransmission areas. The disease risks among thepopulations located under low, stable endemicconditions, including large urban settlements inAfrica, will be low and result from the host's chanceencounters with the parasite. Conversely, diseaserisks among populations exposed to intense stabletransmission will be modified by acquired immuneresponses and the intensity of transmission willdefine the speed with which the population developsfunctional immunity to the severe and fatal con-sequences of infection. Recent epidemiologicalstudies (17) have demonstrated that the burden of
morbidity and mortality is concentrated among theyoungest age groups under conditions of intense,perennial, stable transmission and that while life-threatening pathologies such as cerebral malaria arerare, the incidence of severe anaemia is high. Astransmission becomes less intense, more seasonaland ultimately unstable or epidemic, the clinicalpatterns of disease increasingly include cerebralmalaria and overall life-threatening disease risk isspread across a much wider age range. The preciserelationship between frequency of parasite exposure,functional immunity and disease risk remains illdefined. However, under conditions of moderate-to-high intensity there is evidence that the cumulativerisks of severe, life-threatening disease do not varydespite marked differences in the age patterns ofdisease (17).
Southern AfricaThe southern African region has historically sup-ported transmission of malaria within well-definedecological boundaries. These boundaries are bestdefined from the fuzzy climate model among areaswith a suitability index of50.5 (14). For many yearscountries located in southern Africa have mountedrigorous malaria control strategies, involving activecase detection, mass drug administration and, mostsignificantly, aggressive vector control throughresidual house spraying. These combined strategieshave been successful in reducing the basic reproduc-tion rate of infection and disease incidence. Conse-quently, on the basis of this unique disease ecology,these areas have been identified separately from therest of sub-Saharan Africa and comprise Botswana,Lesotho, Namibia, South Africa, Swaziland, andZimbabwe.
Population distributions in Africa
A GIS (geographic information system) populationdatabase for Africa was used to define at-riskpopulations. Full details of this database arepresented elsewhere (18). The data were constructedusing population totals from the last availablecensuses for more than 4000 administrative units inAfrica. To improve the spatial resolution of thepopulation information further, the data by admin-istrative units were converted into a regular raster gridof population totals that was compatible with theclimate suitability surfaces. For this purpose auxiliaryinformation was used to distribute the populationtotal recorded for the administrative unit across theraster grid cells that fall within this unit. This processincorporated information on where people tend tolive: in or close to towns and cities, close to transportinfrastructure, outside protected areas and waterbodies, or very high elevations. Using GIS-basedinformation on the location and size of towns andcities, roads, railroads, navigable rivers and un-inhabitable areas, a weighting surface was con-structed, where a high value implies a high
Research
626 Bulletin of the World Health Organization, 1999, 77 (8)
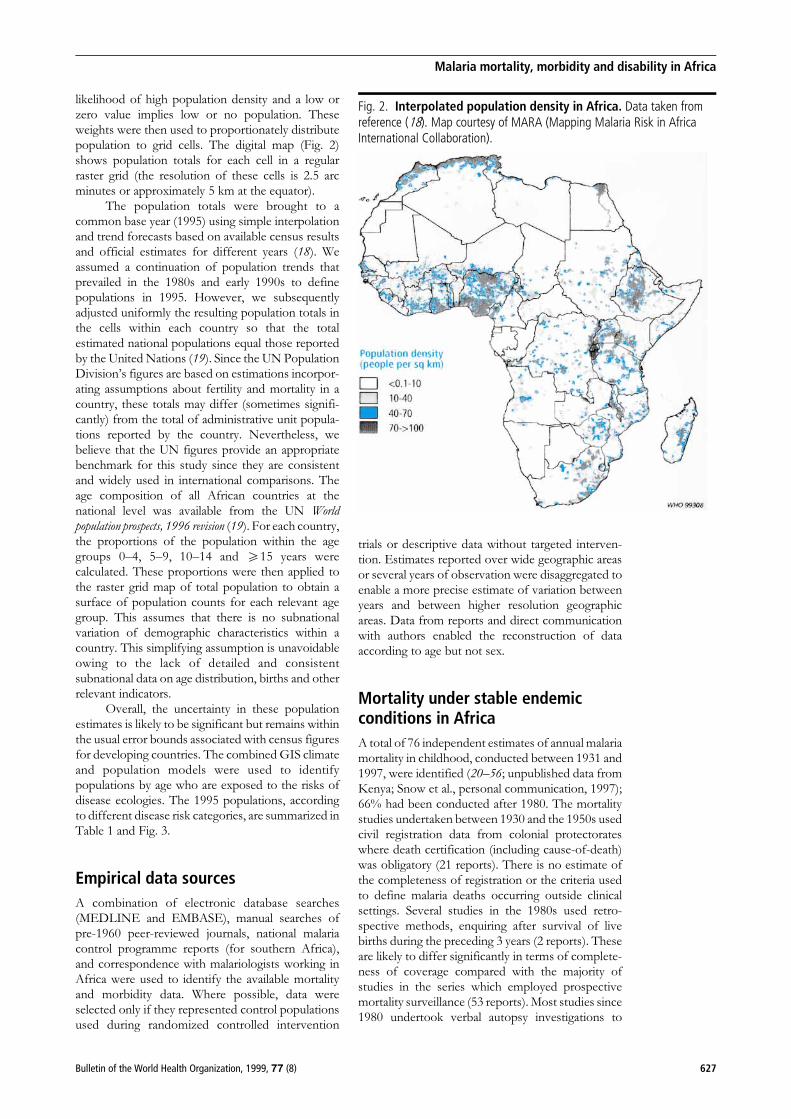
likelihood of high population density and a low orzero value implies low or no population. Theseweights were then used to proportionately distributepopulation to grid cells. The digital map (Fig. 2)shows population totals for each cell in a regularraster grid (the resolution of these cells is 2.5 arcminutes or approximately 5 km at the equator).
The population totals were brought to acommon base year (1995) using simple interpolationand trend forecasts based on available census resultsand official estimates for different years (18). Weassumed a continuation of population trends thatprevailed in the 1980s and early 1990s to definepopulations in 1995. However, we subsequentlyadjusted uniformly the resulting population totals inthe cells within each country so that the totalestimated national populations equal those reportedby the United Nations (19). Since the UN PopulationDivision's figures are based on estimations incorpor-ating assumptions about fertility and mortality in acountry, these totals may differ (sometimes signifi-cantly) from the total of administrative unit popula-tions reported by the country. Nevertheless, webelieve that the UN figures provide an appropriatebenchmark for this study since they are consistentand widely used in international comparisons. Theage composition of all African countries at thenational level was available from the UN Worldpopulation prospects, 1996 revision (19). For each country,the proportions of the population within the agegroups 0±4, 5±9, 10±14 and 515 years werecalculated. These proportions were then applied tothe raster grid map of total population to obtain asurface of population counts for each relevant agegroup. This assumes that there is no subnationalvariation of demographic characteristics within acountry. This simplifying assumption is unavoidableowing to the lack of detailed and consistentsubnational data on age distribution, births and otherrelevant indicators.
Overall, the uncertainty in these populationestimates is likely to be significant but remains withinthe usual error bounds associated with census figuresfor developing countries. The combined GIS climateand population models were used to identifypopulations by age who are exposed to the risks ofdisease ecologies. The 1995 populations, accordingto different disease risk categories, are summarized inTable 1 and Fig. 3.
Empirical data sources
A combination of electronic database searches(MEDLINE and EMBASE), manual searches ofpre-1960 peer-reviewed journals, national malariacontrol programme reports (for southern Africa),and correspondence with malariologists working inAfrica were used to identify the available mortalityand morbidity data. Where possible, data wereselected only if they represented control populationsused during randomized controlled intervention
trials or descriptive data without targeted interven-tion. Estimates reported over wide geographic areasor several years of observation were disaggregated toenable a more precise estimate of variation betweenyears and between higher resolution geographicareas. Data from reports and direct communicationwith authors enabled the reconstruction of dataaccording to age but not sex.
Mortality under stable endemicconditions in Africa
A total of 76 independent estimates of annual malariamortality in childhood, conducted between 1931 and1997, were identified (20±56; unpublished data fromKenya; Snow et al., personal communication, 1997);66% had been conducted after 1980. The mortalitystudies undertaken between 1930 and the 1950s usedcivil registration data from colonial protectorateswhere death certification (including cause-of-death)was obligatory (21 reports). There is no estimate ofthe completeness of registration or the criteria usedto define malaria deaths occurring outside clinicalsettings. Several studies in the 1980s used retro-spective methods, enquiring after survival of livebirths during the preceding 3 years (2 reports). Theseare likely to differ significantly in terms of complete-ness of coverage compared with the majority ofstudies in the series which employed prospectivemortality surveillance (53 reports). Most studies since1980 undertook verbal autopsy investigations to
Fig. 2. Interpolated population density in Africa. Data taken fromreference (18). Map courtesy of MARA (Mapping Malaria Risk in AfricaInternational Collaboration).
Malaria mortality, morbidity and disability in Africa
627Bulletin of the World Health Organization, 1999, 77 (8)

establish causes of death. These survey tools havebeen shown to lack precision for malaria diagnosis(57, 58). Many of the studies do not provide details ofhow malaria was attributed as a cause of death,although it was often through a process of aconsensus agreement from independent review bythree physicians of reports recorded from bereavedrelatives. Despite variations in mortality detectionmethods, completeness of registration, and precisionof verbal-autopsy- diagnosed causes of death, thesestudies represent our only empirical sources ofmalaria-specific mortality among African children.
Five reports presented data among age groupsnot consistent with a childhood age range of 0±4years (20, 40) and were excluded from the analysis ofmortality risks among children aged 0±4 years. Theremaining 71 studies cover 16 countries. Estimates ofendemicity (cross-sectional parasite ratio surveysamong childhood populations) were independentlyidentified for 54 of the mortality survey locations. Atotal of 50% of this series was undertaken in areaswhere cross-sectional parasite ratios among childrenwere 20±49%; 28% of the studies were undertaken inareas where the prevalence of infection was in therange 50±69%; and the remaining studies (22%) were
conducted in areas exposed to intense transmission(childhood parasite ratios 570%). The range inmortality estimates encompasses zero (29), anunlikely estimate. Nevertheless, the underlyingprinciple behind this analysis has been not to makeany value judgements on quality and precision of theestimates provided. To this end, all data have beenincluded and medians and interquartile ranges (IQR)have been used to summarize the data. The medianestimate of malaria-specific mortality among childrenaged 0±4 years was 9.4 per 1000 per annum (IQR: 7.1,12.4).
Most studies of the causal structure ofmortality in Africa have focused on childhood.Consequently, we know surprisingly little aboutmalaria mortality among older children and non-pregnant adults under endemic conditions in Africa.We have approached this paucity of data bymodelling the declining mortality risk with age inaccordance with our present knowledge on thedevelopment of functional immunity to severe, life-threatening malaria. To model declining mortalityrisks with age we have used age-specific data derivedfrom proportional, severe malaria admission ratesamong children aged 0±9 years for 14 hospital
Table 1. Population and mortality estimates for the interpolated distribution of people according to classifications oftransmission riska
African population exposed Southern Africanto different malaria risks population
(excluding southern and northern Africa)
0 climate >0 and <0.2 climate 50.2 climate <0.5 climate 50.5 climatesuitability: suitability: suitability: suitability: suitability:No malaria Epidemic malaria Stable No malaria Malaria risk
risk riska transmission risk area
Population aged 0±4 years 4 609 524 9 850 391 81 429 978 5 504 839 3 025 494
Median mortality rate per 1000 population ± NA 9.4 (7.1, 12.4)b ± 0.11 (0.02, 0.20)
Estimated numbers of deaths in 1995 0 NA 765 442 0 333(578 153±1 009 732) (61±605)
Population aged 5±9 years 3 770 381 8 174 807 67 032 624 4 893 730 2 602 153
Median mortality rate per 1000 population ± NA 2.17 (1.64, 2.86) ± 0.11 (0.02, 0.20)
Estimated numbers of deaths in 1995 0 NA 145 461 0 286(109 934±191 713) (52±520)
Population aged 10±14 years 3 097 257 6 906 370 56 360 964 4 535 489 2 359 704
Median mortality rate per 1000 population ± NA 0.80 (0.61, 1.06) ± 0.11 (0.02, 0.20)
Estimated numbers of deaths in 1995 0 NA 45 089 0 260(34 380±59 743) (47±472)
Population aged >15 years 13 329 952 29 639 097 242 110 974 24 179 130 11 422 561
Median mortality rate per 1000 population ± NA 0.13 (0.09, 0.17) ± 0.11 (0.02, 0.20)
Estimated numbers of deaths in 1995 0 NA 31 474 0 1 256(21 790±41 159) (228±2285)
Total population in 1995 24 807 114 54 570 668 446 934 540 39 113 188 19 409 912
Total deaths in 1995 [non-epidemic year] 0 NA 987 466 0 2 135(744 257±1 302 347) (389±3882)
a No reliable estimates of age-specific malaria mortality during malaria epidemics are available.b Figures in parentheses are the interquartile range.
Research
628 Bulletin of the World Health Organization, 1999, 77 (8)

settings in Africa (17, 59±63). While there is a widerange of age-specific patterns, these 14 studiesencompass the ranges of endemicity covered by theidentified mortality data. The hospital data wereaggregated to provide an age-risk function curveusing a reciprocal quadratic function to model risksthrough childhood into adulthood (Fig. 4). Thisfunction was applied to the median and IQR base-estimate in the 0±4-year group to derive estimates atolder age groups (Table 1).
Morbidity under conditionsof stable endemicity in Africa
The mild clinical consequences of P. falciparuminfection often present as fever and a variety ofassociated symptoms including rigors, headache,body pains, cough and diarrhoea. The age-specificpatterns of clinical manifestations of P. falciparum formild, acute malaria disease in endemic Africa areprovided by Rogier et al. (64). For most individuals inendemic settings these clinical events will be eithereffectively treated or treated with only partial successdue to inappropriate drugs or dosages, or the patientwill spontaneously recover in the absence of anyintervention. A minority of these events will progressto severe pathological complications, which mayresult in death.
Field-based epidemiological studies of mildmorbidity frequently use fever and accompanyinghigh parasite densities as characterizing a clinicalevent. These events are either detected throughactive surveillance or passively detected at referralcentres among well-defined cohorts of children. Ofthese, passive detection best reflects what the localcommunity perceives as ill health, but it will notdetect all mild, transitory clinical events. Activesurveillance relies heavily on the attribution of afebrile event to the associated parasitaemia, which inmany endemic settings will be present among themajority of asymptomatic hosts; statistical methodshave been developed to attribute risk for specificparasite density cut-offs (65).
A total of 51 studies of febrile clinical episodesof malaria in childhood were identified through theliterature and unpublished data-sets in areas of stableendemicity (22±24, 27, 32, 36±38, 40, 56, 66±92;unpublished data from Kenya: Snow et al., personalcommunication, 1997). These surveys had actively orpassively surveyed for febrile malaria episodes inchildhood. The frequency of surveillance determinesthe likely chances of detecting events. For example inthe Gambia, weekly surveillance detected 75% ofevents identified by daily surveillance and monthlysurveillance detected 25% of weekly surveillanceevents (93). Data reported from active surveillancestudies have been corrected to annualized (ortransmission season) risks as would have beendefined through weekly surveillance, according towhether they made single, cross-sectional, weekly ormonthly observations. Five studies did not include
parasitological examinations of detected febrileevents and these were excluded from subsequentanalysis. The remaining studies were conducted in13 countries; 18 were undertaken in areas with achildhood cross-sectional parasite ratio of <50%, 7 inareas where childhood prevalence of infection was50±69%, and 21 studies in areas where the prevalenceof infection was 570%.
Case definitions for clinical episodes of malariaare complex. Many of the studies reported thenumber of children seen, the number with a raised
Fig. 3. Zones of climate suitability. Zones define people exposed to thefollowing: malaria transmission in southern Africa (black), stable transmissionin sub-Saharan Africa (pale blue), epidemic-prone areas of sub-SaharanAfrica (dark blue), negligible malaria risk areas (grey). The following wereexcluded: north African countries (not shown) and unpopulated areas(white). Map courtesy of MARA (Mapping Malaria Risk in Africa InternationalCollaboration).
Fig. 4. Proportional age-specific malaria mortality. Proportional age-specific malaria mortality was predicted by extrapolating a reciprocalquadratic model derived from proportional malaria admissions throughoutchildhood (17, 60). Modelled curve is shown for the data points (.).
Malaria mortality, morbidity and disability in Africa
629Bulletin of the World Health Organization, 1999, 77 (8)

temperature or reported fever, and the number withdetectable P. falciparum infection in the peripheralblood (and sometimes those with elevated parasitedensities). It is not possible to provide a uniform casedefinition under every setting since etiologicalfractions of fever and parasite density will be afunction of the risks of super-infection and immunityby age. Consequently the data have been presentedinitially according to ``any'' level of infection as themost basic common denominator between thestudies. Ten studies (37, 55, 76±77, 88±90; unpub-lished data from Kenya; Snow et al., personalcommunication, 1997) reported both rates for anylevel of infection and a qualifying parasite densityconsistent with the background levels of parasitedensity in that population. The relative differencesbetween the two definitions (any versus an elevatedparasite density) ranged from 1.2 to 2.5 and theaverage difference was 1.84. Studies were thereforecategorized as: 1) those providing a corrected parasitedensity qualification for a case; and 2) those whereany level of infection was used. The latter werecorrected according to a 1.84 lower incidence derivedfrom the 10 studies providing both estimates. These46 clinical attack rate estimates provide a medianestimate for attack rate for malaria of 998.5 per1000 children per annum (IQR: 462.0, 1720.0).
Only four studies provided rates of disease byage throughout childhood (23, 78, 82, 85) and thereare no published single-year age-group estimates ofmorbidity risk to define a risk-function curve as wascalculated for mortality. The four studies combinedsuggest an average decline in attack rates of 4.19between the two age groups 0±4 years and 5±9 years.When applied to our base estimate of 998.5 per1000 children aged 0±4 years per annum, one wouldexpect an attack rate of 238.5 per 1000 per annumamong children aged 5±9 years.
Fewer studies exist for adults and only10 estimates could be identified (64, 66, 94±97).The median attack rate for clinical malaria, as definedby this series, was 939 per 1000 adults per annum(IQR 400, 1400). These combined empirical ob-servations suggest that morbidity risks would besimilar to those of early childhood; however, weknow little about changing patterns of severity ordebilitation with increasing age. While it is generallyaccepted that the nature of immunity to malaria iscomplex, with important differences between im-mune mechanisms targeted at reducing fatal out-comes and those targeted at fever modulation,immunity to mild clinical attacks is acquired withage. One possible explanation for this discrepancy isthat malaria case definitions for adult attacks have notbeen well defined and we have not employedcorrection factors in accordance with parasite densitycriteria. The most rigorous contemporary studyconducted among African adults living in a highlyendemic area was that undertaken among theresidents of Dielmo village in Senegal, who partici-pated in daily parasitological and clinical observationsover 3 years (64). The authors defined a malaria attack
rate of 400 per 1000 adults per annum. It seemsplausible that morbidity risks increase in old age andamong pregnant women through a weakening ofoverall immune responses. While there is evidence tosupport this weakening (98), there is a paucity ofclinical epidemiological evidence among non-pregnant adults living in endemic areas of Africa. Inour analysis we have assumed approximately 1 clinicalattack of malaria per child aged 0±4 years, 0.25 perchild aged 5±14 years, and 0.4 per adult per annum.
Mortality and morbidityin southern Africa
Data for southern Africa were derived from nationalsurveillance reports which reported on combinationsof active surveillance, case reporting of malaria(malaria is a notifiable disease in all these countries),and civil registration data. While there can be noclaims to completeness of notification, the southernAfrican countries have invested heavily in malariasurveillance to support control operations. Estimatesof mortality were available from Botswana, Namibia,South Africa, and Zimbabwe (99±106). Only pro-vinces, districts or regions within the 50.5 climatesuitability limits were included. Reports presentingdata by age indicated very little variation in risks byage, consistent with a population with little functionalimmunity. In South Africa several fatalities will havebeen included among migrants from Mozambiqueand it was not possible to separate out these events.The median mortality rate from 15 reports was 0.104per 1000 total population per annum (IQR: 0.02,0.20). From similar areas we identified 35 estimates ofmalaria morbidity from malaria control programmereports (99±107). These reports, covering the last10 years, provide a median estimate of 11 episodesper 1000 total population per annum (IQR = 4.4,29.4), representing an average of one episode perperson every 10 years.
Mortality and morbidity amongpopulations exposed to epidemics
A significant proportion of the population in south-ern and East Africa and in the Horn of Africa areexposed to unstable malaria, giving rise to epidemics.A total of 15 published and unpublished reports onmorbidity and mortality risks among populationsexposed to unnatural epidemics were identified(108±114). These data have been reported as risksper day and, in the majority of mortality reports, relateto all-cause mortality. Mortality estimates for malariaalone are only available for four areas recorded duringthe 1958 malaria epidemic in Ethiopia (ranging from59.64 to 350 per 1000 population per annum) (109);the median was 235.13 per 1000 total population perannum (IQR = 103, 350). These risks demonstratethe devastating effects of malaria epidemics; how-ever, they derive from a single crisis situation among a
Research
630 Bulletin of the World Health Organization, 1999, 77 (8)

population with virtually no immunity and no accessto curative services. Such epidemic scenarios arelikely to be uncommon, occurring perhaps every30 years. More typical are the effects among partiallyimmune populations located in the highlands of EastAfrica and the Horn of Africa. The periodicity andclinical-epidemiological descriptions of malaria inthese altitude-epidemic-prone areas are poorly de-fined. Indeed, we have no empirical basis on which todefine the risks of fatal outcomes among thesepopulations and these have therefore been omittedfrom Table 1.
Seven reports of clinical attack rates per1000 total population per day during epidemics inarid and altitude areas were identified (108, 109, 111,113, 114). The median annualized estimate for thesestudies is 976 per 1000 population (IQR 149, 1176).Despite the paucity of data, this would appear to be areasonable estimate as all new infections will probablylead to clinical disease and this rate is consistent withsemi-immune young children exposed to stableendemic malaria. We have assumed these epidemicrisks last for approximately 3 months and occur onaverage every 3±5 years affecting all age groupsequally.
Sequelae from cerebral malariaamong children living under stableendemic conditions
Cerebral malaria is defined in clinical terms as thepresence of coma due to malaria (115). Its pathologystems from a series of complex mechanisms whichmay operate independently, but all result in a braininsult. Several factors may increase the risk ofneurological sequelae following cerebral malaria,including hypoglycaemia, multiple seizures, reducedcerebral perfusion pressure associated with raisedintracranial pressure, hypoxia associated with micro-vascular obstruction, and tissue damage followinginduction of cytokine cascades (116).
Waller et al. (117) identified 29 studies ofcerebral malaria in African children publishedbetween 1956 and 1994, which included reports onthe incidence of neurological sequelae. A total of 206of 2612 (7.8%) children were reported to havesequelae. However, there were major differences inthe methodologies and definitions of cerebral malariaused, and this is reflected in the wide range ofreported incidence (0±25%). We have thereforeconcentrated on six more recent studies (118±122;
Table 2. Morbidity estimates for the interpolated distribution of people according to classificationsof transmission risk
African population exposed to different malaria risks Southern African(excluding southern and northern Africa) population
>0 and < 0.2 climate 50.2 climate 50.5 climatesuitability: suitability: suitability:
Epidemic malaria riska Stable transmission Malaria risk area
Median morbidity rate per 1000 population 976 (149, 1176)b 998.5 (462, 1720) 11.0 (4.4, 29.4)aged 0±4 years population
Estimated numbers of clinical attacks 2 403 495 81 307 833 33 280among 0±4-year-olds in 1995 366 927±2 896 015c 37 620 650±140 059 562 13 312±88 950
Median morbidity rate per 1000 population 976 (149, 1176) 238.5 (110, 411) 11.0 (4.4, 29.4)aged 5±9 years
Estimated numbers of clinical attacks 1 994 653 15 987 281 28 624among 5±9 year-olds in 1995 304 512±2 403 393 7 373 589±27 550 408 11 449±76 503
Median morbidity rate per 1000 population 976 (149, 1176) 238.5 (110, 411) 11.0 (4.4, 29.4)aged 10±14 years
Estimated numbers of clinical attacks 1 685 154 13 442 090 25 957among 10±14-year-olds in 1995 257 262±2 030 473 6 199 706±23 164 356 10 383±69 375
Median morbidity rate per 1000 population 976 (149, 1176) 400 (110, 1000) 11.0 (4.4, 29.4)aged >15 years
Estimated numbers of clinical attacks 7 231 940 96 844 390 125 648among >15 year-olds in 1995 1 104 056±8 713 895 26 632 207±242 110 974 50 259±335 823
Total numbers of clinical attacks in 1995 13 315 242 207 581 594 213 509[non-epidemic yearc] 2 032 757±16 043 776 77 826 152±432 885 300 85 403±570 651
[150 069: 60 028±401 094]
a Epidemic estimates assume 3 months of risk and that rates and burden occur every 3±5 years.b Figures in parentheses are the interquartile range.c Figures in italics are the range.d Estimates for non-epidemic year provided for the entire population in parentheses and are based upon risks associated with conditions in southern Africa.
Malaria mortality, morbidity and disability in Africa
631Bulletin of the World Health Organization, 1999, 77 (8)

unpublished data from Kenya, Peshu et al., personalcommunication, 1998), which used comparablediagnostic criteria. These studies report on a totalof 1854 children with cerebral malaria, 302 (16.3%) ofwhom died, while 248 (16% of survivors) werereported to have neurological sequelae at discharge.Even using standardized criteria for the definition ofcerebral malaria, the reported incidence varied from9% (118) to 23% (122). Most of this variationprobably stems from differences in what is taken toconstitute a significant deficit on discharge; manychildren examined within a few days of an encephalo-pathic illness will have residual problems such asataxia which resolve rapidly over the next few weeksor months. More significant are those neurologicalsequelae that are persistent. Five studies differed infollow-up schedules and completeness of follow-up,but four of the studies (119, 120, 122; unpublisheddata from Kenya, Peshu et al., personal communica-tion, 1998) covering 1258 children had follow-upperiods of at least 6 months; among this series theoverall rate for persisting neurological sequelae was5.6%. Although there may continue to be improve-ment beyond 6 months, we have used this rate in thecalculations of the risks of long-term sequelae givenbelow.
The sequelae reported (in approximate order offrequency) included the following: hemiplegia/hemiparesis (weakness in one or both limbs on oneside of the body), speech disorders, behaviouraldisorders, blindness, hearing impairment, cerebralpalsy (also called spastic paresis in some studies Ðthese children have a generalized increase in muscletone and are very severely disabled, requiringconstant attention from a carer) and epilepsy.Children often have multiple sequelae and it is notpossible to disaggregate the data from the publishedstudies to give absolute rates for each type ofsequelae.
To define the annual risks of cerebral malariapresenting to hospital, we selected 10 demographi-cally and geographically defined communities within15 km of a hospital setting with upgraded diagnosticfacilities and a prospective epidemiological surveil-lance system (17, 60). These clinical sites weresituated among a wide range of endemicities rangingfrom cross-sectional, prevalence infection ratesamong children aged 0±9 years of 2% in the Gambiato >80% in Kenya and the United Republic ofTanzania. Median estimates described through thesestudies have been used to define the risks of cerebralmalaria among children aged 0±4 years and 5±9 yearsfor communities with easy access to tertiary-levelcare. These estimates were 1.82 per 1000 childrenaged 0±4 years per annum (IQR: 0.26, 2.60) and 0.35per 1000 children aged 5±9 years per annum (IQR:0.13, 0.61). Not all of these children will surviveadmission because cerebral malaria has a poorprognosis even under optimal care. Application ofthe case-fatality estimate (16.3%) defined aboveindicated that only 83.7% survive admission and aresubject to the risks of neurological sequelae. We have
assumed these survival risks are similar across bothage groups.
Also we have assumed that children whoexperience cerebral malaria and do not reach hospitaldo not spontaneously recover and would probably beincluded in mortality estimates. To derive an estimateof the proportions of children living in stableendemic areas of Africa within similar reach ofessential clinical services capable of managingcerebral malaria cases, we used seven nationaldemographic and health survey reports (Uganda,1995; Kenya, 1995; United Republic of Tanzania,1991±92; Mali, 1995±96; Central African Republic,1994±95; Chad, 1996±97; and Cameroon, 1991)which describe the proportions of randomly selectedhouseholds within 15 km of hospital care. Theaverage estimate from these community-basedsurveys was 35.9% (range, 22±65%).
By combining the rates of cerebral malaria per1000 children exposed to stable transmission with (i)correction factors for access to hospital and case-fatality and (ii) risks of persistent sequelae, weestimated the numbers of events likely to occuramong children living under these conditions in 1995(Table 3). These estimates do not allow for multiplesyndromes within the same child and thereforecorrespond to numbers of events. No data areavailable on the risks of residual sequelae amongadults exposed to cerebral malaria in Africa. Severalconservative assumptions were made in derivingthese figures: for example, in practice many childrenare brought to hospital from communities that liemuch further than 15 km from hospitals; a propor-tion of children treated inadequately outside hospitalwill none the less survive; and the figures are derivedfrom settings with a level of clinical managementconsiderably higher than that which may apply inmany ordinary hospitals. These figures shouldtherefore be viewed as minimum estimates and thetrue impact is likely to be considerably higher.
Severe anaemia, blood transfusionand HIV risks among children livingunder stable endemic conditions
Severe anaemia is a feature of life-threatening malariawith a complex etiology combining a rapid haemo-lysis during acute infection and/or a slow insidiousprocess compounded by antimalarial drug resistance.Severe anaemia is a life-threatening condition inyoung children and often warrants blood transfusionat a hospital setting. Greenberg et al. examined thehuman immunodeficiency virus (HIV) and malariaserostatus of 167 paediatric admissions to anemergency ward at the Mama Yemo Hospital,Kinshasa, Zaire (now called Democratic Republicof the Congo) (123). Of 112 malaria diagnoses,68 had received blood transfusions and 44 had not.HIV infection rates on discharge were 15% among
Research
632 Bulletin of the World Health Organization, 1999, 77 (8)

the transfused group compared with 2% among thenontransfused group. An unadjusted odds ratio foracquired HIV infection of 3.5 was proposed formalaria patients transfused once, rising to 21.5 and43.0, respectively, for those transfused twice andthree times during a single admission. HIV infectionrates at the blood bank in Kinshasa were 6.3%. Thissingle observation increases the significance ofsequelae of severe malaria. Transfusion is a commonpaediatric practice in Africa. Criteria for its use varybetween clinical settings, but we identified ten studies(123±132) where transfusion rates were provided forchildren who presented at hospital with a haemoglo-bin level 45.0 g/dl; the average transfusion rateamong this series was 70%.
Among the 10 hospital community-linkedstudies described above, 7 settings recorded haemo-globin concentrations on every admission (17, 60).The median annual rate of presentation to hospitalwith severe malaria anaemia (a primary diagnosis ofmalaria and an accompanying haemoglobin of<5.1g/dl) was 7.61 per 1000 children aged 0±4 years(IQR: 3.99, 11.61) and 0.47 per 1000 children aged5±9 years (IQR: 0.11, 0.72). Similar correction factorswere applied to the childhood populations at risk, asdefined above, to calculate the number of childrenliving within 15 km of a hospital. The average case-fatality rate for paediatric severe malaria anaemiafrom 11 reports (17, 60, 126±132) from hospitalslocated in endemic areas was 9.7% (90.3% survived).Combining these parameter estimates provides ameans to calculate the numbers of children whodeveloped severe malaria anaemia, were admitted tohospital, survived, and were treated with bloodtransfusion, and their subsequent increased risks ofdeveloping HIV infection in accordance with therisks described by Greenberg et al. (Table 3).
Summary of estimates of the malariaburden
The biological basis of transmission and acquiredimmunity and the application of new GIS technol-ogies using continental-scale databases have drivenour approach to defining the malaria burden inAfrica. Given the unreliability of national statistics inmuch of sub-Saharan Africa, we have used empirical,survey-derived data on the risks of mortality,morbidity and disability. We were able to identifyover 200 published sources on the health impact ofmalaria across a wide range of endemicities anddisease ecologies common to Africa. In the presentanalysis we have selected direct estimates or morbidand fatal risks rather than proportional risksattributable to malaria intervention, as defined byrandomized controlled trials. Trial data available forsuch an analysis only cover a small area of Africa(6 studies in total) and none achieved completecoverage or 100% efficacy. We have analysed thesestudies previously, and the results compared favour-
ably with the direct estimation of malaria mortality inthe same areas using verbal autopsies (7).
Through a combination of approaches we haveestimated that, among populations exposed to stableendemic malaria in sub-Saharan Africa, approxi-mately 987 466 people may have died in 1995 fromdirect consequences of P. falciparum infection. Thiswould have included 765 442 children below the ageof 5 years. We used a combined estimate of mortalityrisk derived over many years (predominantly since1980), and there is mounting evidence that mortalityrisks have increased significantly, coinciding with therise in failures with chloroquine, the widely used first-line treatment (52, 59). Also, our estimates onlyconsider the direct consequences of infection. Wehave not considered any indirect consequences ofinfection with P. falciparum upon fatal outcomes fromother causes of death, particularly in childhood, and
Table 3. Sequelae risks and events following admission to hospitalamong children living in stable endemic areas of Africa
Outcome Age group (years)
0±4 5±9
Risk of cerebral malaria admission from 1.815 0.345communities within 15 km of a hospital (0.26, 2.60)a (0.13, 0.61)(per 1000 population per annum)
Risk of surviving hospitalization 1.472 0.280with cerebral malaria (0.211, 2.11) (0.11, 0.495)
Risk of surviving hospitalization with cerebral 0.528 0.101malaria, allowing for the proportion (0.076, 0.756) (0.040, 0.178)of population within 15 km of hospital
Neurological sequelae risk of residual 0.030 0.006effects after six months (0.004, 0.042) (0.002, 0.010)(per 1000 children per annum )
No. of neurological sequelae events 2443 402356±3420b 134±670
Risk of SMAc admission from communities 7.61 0.47within 15 km of a hospital (3.99, 11.61) (0.11, 0.72)(per 1000 population per annum)
Risk of surviving hospitalization with SMA 6.87 0.42(per 1000 population per annum) (3.60, 10.49) (0.01, 0.65)
Risk of surviving SMA admission 4.81 0.29and receiving a blood transfusion (2.52, 7.34) (0.007, 0.46)(per 1000 population per annum)
Risk of surviving hospitalization 1.73 0.10with transfused SMA allowing for proportion (0.905, 2.64) (0.003, 0.165)of population within 15 km of hospital(per 1000 population per annum)
Risk of survivors with SMA who had a blood 0.225 0.013transfusion, who acquire HIV when (0.118, 0.343) (0.0004, 0.022)background risks apply to those in Kinshasain late 1980s (per 1000 population per annum).
No. of HIV events arising from blood transfusions 18 322 871of severe malaria anaemia 9609±27 930 29±1475
a Figures in parentheses are the interquartile range.b Figures in italics are the range.c SMA = severe malaria anaemia.
Malaria mortality, morbidity and disability in Africa
633Bulletin of the World Health Organization, 1999, 77 (8)

the estimates we have provided may be considered aminimum. For morbidity, despite fewer empiricalobservations and additional problems of precise case-definition, we estimate that over 207.5 million clinicalattacks of malaria may have occurred in Africa amongpeople resident under stable endemic conditions in1995. This estimate relates only to a strictly definedrisk of a clinical episode of malaria allowing for thepresence of asymptomatic infection. A far greaternumber of people would have been presumptivelydiagnosed and/or treated for malaria in 1995.
The definitions used to describe zero-risk,unstable or epidemic-prone areas of Africa arefraught with technical difficulties (14); these ``fringe''areas demand further epidemiological research.Nevertheless, we have used arbitrary selection criteriaderived from climate suitability models to define tworegions of sub-Saharan Africa which either supportunstable transmission conditions or where long-termclimate data suggest areas are always unsuitable fortransmission. Under both conditions, malaria willpose some burden every year where highly mobile,nonimmune populations migrate between theirresidence and areas of stable endemic transmission.We have no estimates of these ``mobility'' risks andhave no reliable estimates of mortality amongpopulations exposed to epidemics in Africa. How-ever, information was available for morbidity risksamong populations exposed to unstable transmis-sion. There was a striking similarity in the clinicalattack rate described in the literature among totalpopulations exposed to epidemic malaria (976 per1000 per annum) and that described for children bornunder stable endemic conditions (998.5 per 1000 perannum). These observations support the idea thatsuch populations have no acquired functionalimmune responses. We have assumed that malariaepidemics last for 3 months and occur on averageevery 3±5 years. During nonepidemic years we haveassumed a minimum risk described for southernAfrica that would account for 150 000 clinical attacks.It has been argued that the periodicity of epidemicsmay be changing over time, with decreasing intervalsbetween epidemics (133), possibly leading to achange in the estimates of the longer-term, projectedmalaria burden.
Among the populations located in southernAfrica, we were able to identify malaria controlsurveillance reports for five countries among districtslocated within a boundary of likely malaria transmis-sion (Fig. 3). Applying the annualized median risksfor mortality and morbidity suggests that, in 1995,this population may have experienced 2135 deathsand 213 509 clinical attacks due to chance encounterswith infections not prevented by aggressive controland by prompt and effective treatment. Of interestare the derived case-fatality estimates for southernAfrica (1.0%) versus those defined for areas of stabletransmission in sub-Saharan Africa (0.48%). Both arehigh, indicating how potent malaria has been inselecting for host polymorphisms such as sickle cell,but they also highlight the potential significance of
naturally acquired immunity against the fatal con-sequences of infection through repeated parasiteexposure.
There are several health outcomes ofP. falciparum infection which we have not considered,including the potential effects of undernutrition,potentiating effects from other infectious diseases,cognitive impairment and behavioural disturbances(as a consequence of cerebral malaria), possible risksof epilepsy following repeated seizures, and adversedrug reactions to increasingly used second-lineantimalarial drugs. Of significance are the effects ofmalaria infection in pregnancy, which are beingconsidered separately (Guyatt et al., in preparation).However, by way of demonstrating the value ofempirical evidence-based approaches, we haveselected two sequelae of severe, life-threateningmalaria: residual neurological disability followingcerebral malaria; and HIV risks consequent upontransfusion for severe malaria anaemia. We havecalculated these effects only for children aged<10 years living in areas of stable endemicity insub-Saharan Africa. Approximately 3000 disablinglong-term events may have occurred among survi-vors of cerebral malaria in this area of Africa in 1995.We have calculated only those events which are likelyto be lifelong. Thus, the last decade may havewitnessed a cohort of 30 000 children who have beenleft with residual effects such as ``spasticity'' andepilepsy attributable to a brain insult caused bymalaria. Furthermore, we have estimated that over19 000 children, aged 0±9 years and residing in thestable endemic areas of Africa, may have survivedblood transfusion for their severe malaria anaemiabut would have acquired HIV. These estimatesstemmed from a single study in Kinshasa where HIVprevalence was 6% in 1986 (123). In the absence offurther data on these effects under operationalconditions (including screening) in Africa, thesignificance of these estimates must be judged withcaution. On the assumption that these are real threatsto paediatric patients with severe malaria anaemia, thenext decade may lead to 200 000 children acquiringHIV directly as a consequence of blood transfusionsfor life-threatening anaemia associated with malaria.
Discussion
The risks of disease and death from malaria aredependent upon a wide range of factors, includingthe frequency of protective genetic polymorphisms,acquired immunity, access and use of curativeservices, drug resistance, and the protective beha-viours of communities against infection. Thesefactors will vary significantly across the Africancontinent, resulting in significant differences indisease outcomes between areas. Perhaps the mostsignificant of these is acquired functional immunity.There is now good evidence that the intensity ofP. falciparum transmission determines the age atwhich functional immunity is acquired in a given
Research
634 Bulletin of the World Health Organization, 1999, 77 (8)

population. Throughout the present analysis of themalaria burden, we have assumed that under stabletransmission conditions cumulative disease andmortality risks reach an equilibrium irrespective oftheir endemicity (17). Such an approach does notreflect reduced risks of mortality and disease underconditions of very low stable transmission. Withinthe series of reports used in this paper, five wereconducted under conditions where point prevalenceinfection rates among the childhood population aged0±9 years were below 20% (74, 77, 93), and indicate a10-fold lower risk of clinical disease relative to themedian estimate derived from the studies conductedunder conditions of higher endemicity (wheremortality risk varied little with increasing intensityof transmission). Of particular relevance is theepidemiology of parasite transmission under urbanconditions. There are several examples wheretransmission intensity is in reality much lower thanwould be predicted from climate-driven models. Forexample, among the peri-urban population in Bakau,in the Gambia, infection rates are <5%, while lessthan 10 km away in a rural area they exceed 30%(17, 77). Urbanization in Africa is a rapidly prolifera-ting demographic change and needs to be capturedwithin the population models for future burden ofdisease estimates.
One of the principal objectives of the Mappingmalaria risk in Africa/Atlas du risque de la malaria enAfrique (MARA/ARMA) collaboration is to provideempirical data and modelled maps showing the highresolution distribution of endemicity risk acrossAfrica (134, 135). This project is in its nascent stagesand endemicity risk maps are only available for Kenya(136) and Mali (Magran et al., in preparation). Withinthe framework of the MARA/ARMA collaboration,these models of spatial heterogeneity of endemicityand risk will provide the basis for a wider and moredetailed analysis of burden for the year 2000 andallow for dynamic models which capture changingfeatures such as urbanization and drug resistance.
While we cannot claim to have provided anexhaustive research bibliography of malaria's impacton mortality and morbidity in Africa, it is striking howlittle detailed epidemiological work has been under-taken on the clinical consequences of infection. Theprocess of using evidence-based descriptions ofdisease burden allows us to define both what we donot know and what we do know. To this end, ouranalysis has highlighted several key weaknesses in theliterature, which must be corrected to provideinformed approaches to morbidity and mortalityrisks in Africa. These include the epidemiologicalpatterns and risks of morbidity and mortality acrosswider age groups, particularly adults, among popula-tions living in urban and epidemic settings, and
improved GIS descriptions of unstable malaria,urbanization and higher resolution age-correctedpopulation distributions for the continent. Thecombined challenge is for epidemiologists, geogra-phers and demographers to redress these deficienciesin our present knowledge by providing moreinformed estimates of the malaria burden in Africa.
Our estimates of approximately 1 million deathsdue to malaria among the African population in 1995are well within the range described for sub-SaharanAfrica by Murray & Lopez (4) for the 1990population and are consistent with several pre-1990estimates (2). Some may therefore argue that ``back ofan envelope'' or expert opinions are robust enoughmethods. We would, however, argue that ourapproach provides a more rational basis for definingdisease burden, which is transparent in its inputs,assumptions, limitations and caveats. Such anapproach allows for new evidence, empiricallyderived confidence limits, and modelled predictionsof change. Within the limitations of the evidence andassumptions on disease distribution, we feel con-fident to claim that P. falciparum causes approximately1 million deaths and over 200 million clinical eventsamong the people of Africa each year. Our estimatesof mortality risk were predominantly derived duringan era when first-line therapeutic drugs wereeffective; as this situation changes, so will themortality burden. The ``roll back'' malaria effort hasmany challenges ahead and will be faced with adisease in Africa that kills thousands of people eachday rather than hundreds. n
AcknowledgementsThis work was undertaken as part of the MARA/ARMA collaboration and was supported by fundsfrom The Wellcome Trust, United Kingdom; theInternational Development Research Centre,Canada; the South African Medical ResearchCouncil; and the Kenya Medical Research Institute(KEMRI). Additional funds were provided by theWorld Health Organization.
The authors are indebted to several people whoassisted in the compilation of the data contained inthis report, including Judy Omumbo, Lucy Muhu-nyo, Lydiah Mwangi, and the many colleagues whohelped by re-analysing their published data. We thankDr Charles Newton for assistance with the neuro-logical sequelae data and members of the MARA/ARMA collaboration, particularly Dave Le Sueur,Brian Sharp and Don de Savigny. One author (RWS)receives support from The Wellcome Trust as part oftheir Senior Fellowships in Basic Biomedical SciencesProgramme (#033340). This paper is published withthe permission of the Director, KEMRI.
Malaria mortality, morbidity and disability in Africa
635Bulletin of the World Health Organization, 1999, 77 (8)

Re sumeÂ
Evaluation de la mortalite , de la morbidite et des incapacite s dues au paludisme dans lespopulations africaines, femmes enceintes excepte esLe roà le du paludisme dans la morbidite et la mortalite despopulations africaines a fait l'objet de travaux universi-taires, de plaidoyers politiques et de spe culations. Pourune grande partie de l'Afrique subsaharienne, lesstatistiques nationales n'ont pas e te une source fiablede donne es sur la morbidite et la mortalite associe es auxdiffe rentes maladies. Des estimations cre dibles de lacharge de chaque maladie sont indispensables pour fixerles priorite s sanitaires nationales et mondiales afin derationaliser l'utilisation des ressources limite es disponi-bles et de rechercher des appuis financiers. Nous avonssuivi une de marche empirique pour de finir les limites dela transmission de Plasmodium falciparum aÁ travers lecontinent et interpole la distribution de la population surla base des projections de mographiques de 1995. Ennous fondant sur l'examen de la documentationconcernant le paludisme en Afrique et sur des modeÁ lesd'immunite fonctionnelle acquise, nous avons e value lestaux, selon l'aà ge, des se quelles mortelles, pathologiqueset incapacitantes conse cutives aÁ l'exposition aÁ l'infesta-tion palude enne dans diffe rentes conditions e pide mio-logiques.
Nous estimons aÁ 0,99 million le nombre des de ceÁ sdirectement imputables aÁ l'infestation par P. falciparumen Afrique en 1995; 75% de ces de ceÁ s auraient toucheÂdes enfants de moins de 5 ans. L'incidence, selon l'aà ge,des atteintes cliniques strictement de finies dans lespopulations expose es aÁ diffe rents risques de transmis-
sion du paludisme donne aÁ penser que le nombre dese pisodes de morbidite aurait avoisine les 208 millions enAfrique en 1995 (auxquels s'ajouteraient 13 millionsd'e pisodes supple mentaires pendant les e pide mies). Lacharge de morbidite occulte en situation d'ende miestable, telle que les se quelles neurologiques conse cutivesau neuropaludisme ou l'infection aÁ VIH due aÁ unetransfusion sanguine chez un malade pre sentant uneane mie se veÁ re associe e au paludisme, laisse supposerpour ces dix dernieÁ res anne es quelque 3000 casd'atteintes ce re brales irre versibles et 19 000 casnouveaux d'infection aÁ VIH parmi les enfants ayantsurve cu au paludisme grave.
L'utilisation des systeÁ mes d'information ge ogra-phique, des de terminants biologiques de la transmissionde P. falciparum, de nos connaissances accrues dessche mas e pide miologiques de la maladie et del'immunite et des quelque 150 sources de donne esempiriques nous donne de solides informations poure valuer le fardeau que repre sente le paludisme. Cetteapproche re veÁ le ne anmoins des faiblesses dans nossources existantes de donne es e pide miologiques et nosconnaissances qu'il convient de corriger pour e laborer aÁl'avenir des modeÁ les d'impact sanitaire dynamiques.Malgre ces limites, nous pensons pouvoir affirmer que lepaludisme est directement responsable d'environun million de de ceÁ s par an en Afrique.
Resumen
Estimacio n de la mortalidad, la morbilidad y la discapacidad por paludismo entre lapoblacio n de A frica, excluidas las mujeres embarazadasEl tema de la contribucio n del paludismo a la morbilidad yla mortalidad entre la poblacio n de A frica ha suscitadointere s teo rico y ha sido objeto de promocio n yespeculacio n. Las estadõÂsticas nacionales de gran partedel A frica subsahariana han demostrado ser una fuentede datos poco fiable respecto a la morbilidad ymortalidad por enfermedades especõÂficas. Se requierenestimaciones fiables sobre la carga de enfermedadesconcretas para fijar las prioridades sanitarias mundiales ynacionales a fin de racionalizar el uso de unos recursoslimitados y de ejercer presiones para obtener apoyofinanciero. Hemos adoptado un enfoque empõÂrico paradefinir los lõÂmites de la transmisio n de Plasmodiumfalciparum a trave s del continente, e interpolado ladistribucio n de la poblacio n a partir de las proyeccionesdemogra ficas de 1995. Combinando el ana lisis de laliteratura sobre el paludismo en A frica y modelos de lainmunidad funcional adquirida, hemos estimado lastasas estructuradas por edades de las secuelas demortalidad, morbilidad y discapacidad resultantes de laexposicio n a la infeccio n palu dica en diferentescondiciones epidemiolo gicas.
Estimamos que 990 000 personas pueden habermuerto como consecuencia directa de la infeccio n por
P. falciparum en A frica durante 1995; el 75% de esasdefunciones corresponderõÂan a ninÄ os menores de cincoanÄ os. La incidencia por edades de ataques clõÂnicosestrictamente definidos entre poblaciones expuestas adiferentes riesgos de transmisio n del paludismo indicaque durante 1995 se habrõÂan producido en A fricaaproximadamente 208 millones de episodios morbosos(ma s 13 millones en situaciones de epidemia). La cargaoculta en condiciones ende micas estables, como lassecuelas neurolo gicas por paludismo cerebral y elcontagio por el VIH a trave s de transfusiones de sangrerealizadas para paliar la anemia grave por paludismo,llevan a pensar que a lo largo de los diez anÄ os puedenhaberse producido aproximadamente 3000 casos dedanÄ o cerebral permanente y 19 000 de nuevasinfecciones por el VIH entre los ninÄ os que han sobrevividoal paludismo grave.
El uso de sistemas de informacio n geogra fica, delos determinantes biolo gicos de la transmisio n deP. falciparum, de nuestros mayores conocimientos sobrelos modelos epidemiolo gicos de la enfermedad y lainmunidad y de ma s de 150 fuentes de datos empõÂricosproporciona una perspectiva informada para realizarestimaciones de la carga de paludismo. Sin embargo,
Research
636 Bulletin of the World Health Organization, 1999, 77 (8)
dicha perspectiva pone de relieve que nuestras fuentesde datos epidemiolo gicos y nuestros conocimientospresentan algunos puntos de biles, que es menestercorregir con miras al futuro desarrollo de modelos
dina micos del impacto sanitario. Pese a esas limitacio-nes, creemos que podemos afirmar con seguridad que elpaludismo se cobra de forma directa cada anÄ o en A fricaaproximadamente un millo n de vidas.
References
1. Sturchler D. How much malaria is there world-wide?Parasitology today, 1989, 5: 39±40.
2. Greenwood BM. Populations at risk. Parasitology today,1990, 6: 188.
3. Schwartlander B. Global burden of disease. Lancet, 1997,350: 141±142.
4. Murray CJL, Lopez AD. Mortality by cause for eight regionsof the world: Global Burden of Disease Study. Lancet, 1997,349: 1269±1276.
5. Ad hoc Committee of Health Research relating to futureintervention options. Investing in health research and develop-ment. Geneva, World Health Organization, 1996 (unpublisheddocument TDR/Gen/96.1; available upon request from: SpecialProgramme for Research and Training in Tropical Diseases, WorldHealth Organization, 1211 Geneva 27, Switzerland).
6. African Initiative for malaria control in the 21st century.Brazzaville, WHO Regional Office for Africa, May 1998(unpublished document).
7. Snow RW et al. A continental risk map for malaria mortalityamong African children. Parasitology today, 1999, 15: 99±104.
8. Gilles MT, De Meillion. The Anophelinae of Africa southof the Sahara. South African Institute for Medical Research,Publication 54, 1968.
9. Leeson HS. Anopheline mosquitoes in Southern Rhodesia.London, London School of Hygiene and Tropical Medicine, 1931(Occasional Paper).
10. Detinova TS. Age-grouping methods in Diptera of medicalimportance, with special reference to some vectors of malaria.Geneva, World Health Organization, 1962 (WHO MonographSeries No. 47).
11. Martens WJM. Health impacts of climate change and ozonedepletion: An eco-epidemiological modelling approach.PhD thesis, Maastrict University, Netherlands, 1997.
12. Molineaux L, Gramiccia G. The Gharki project: research on theepidemiology and control of malaria in Sudan Savanna of WestAfrica. Geneva, World Health Organization, 1980.
13. Le Sueur D, Sharp BL. The breeding requirements of threemembers of the Anopheles gambiae Giles complex (Diptera:Culicidae) in the endemic malaria area in Natal, South Africa.Bulletin of entomological research, 1988, 78: 549±560.
14. Craig MH, Snow RW, Le Sueur D. African climatic model ofmalaria transmission based on monthly rainfall and temperature.Parasitology today, 1999, 15: 105±111.
15. Kosko B. Fuzzy thinking. The new science of fuzzy logic. London,Flamingo Press, 1994.
16. Hutchinson MF et al. Africa Ð a topographic and climaticdatabase, version 1.0. Canberra, Centre for Resource andEnvironmental Studies, Australian National University, 1995.
17. Snow RW et al. Relation between severe malaria morbidity inchildren and level of Plasmodium falciparum transmission inAfrica. Lancet, 1997, 349: 1650±1654.
18. Deichmann U. African population database. Digital databaseand documentation. Santa Barbara, CA, National Center forGeographic Information and Analysis,1996.
19. World population prospects: the 1996 revision. New York,Population Division, United Nations Department for Economicand Social Information and Policy Analysis, 1997.
20. D'Allessandro U et al. Mortality and morbidity from malaria inGambian children after introduction of an impregnated bed netprogramme. Lancet, 1995, 345: 479±483.
21. Alonso PL et al. The effect of insecticide-treated bed nets onmortality of Gambian children. Lancet, 1991, 337: 1499±1502.
22. Alonso PL et al. Randomised trial of efficacy of SPf66 vaccineagainst Plasmodium falciparum malaria in children in SouthernTanzania. Lancet, 1994, 344: 1175±1181.
23. Barnish G et al. Malaria in a rural area of Sierra Leone. I: initialresults. Annals of tropical medicine and parasitology, 1993,87: 125±136.
24. Binka FN et al. Patterns of morbidity and mortality in children innorthern Ghana. Transactions of the Royal Society of TropicalMedicine and Hygiene, 1994, 88: 381±385.
25. Binka FN et al. Impact of permethrin-impregnated bed nets onchild mortality in Kassena-Nakana district, Ghana: a randomisedcontrolled trial. Tropical medicine and international health, 1996,1: 147±154.
26. Bradley AK, Gilles HM. Malumfashi Endemic DiseasesResearch Project, XXI: Pointers to causes of death in theMalumfashi area, northern Nigeria. Annals of tropical medicineand parasitology, 1984, 78: 265±271.
27. Bradley-Moore AM et al. Malaria chemoprophylaxis withchloroquine in young Nigerian children. I: Its effect on mortality,morbidity and prevalence of malaria. Annals of tropical medicineand parasitology, 1985, 79: 549±562.
28. Bruce-Chwatt LJ. Malaria in African infants and children insouthern Nigeria. Annals of tropical medicine and parasitology,1952, 46: 173±200.
29. Carme B et al. Etude retrospective sur la mortalite de l'enfantde moins de 5 ans dans une zone rurale de la re gion de Brazzaville(R.P.Congo). Bulletin de la Socie te de Pathologie Exotique etde ses Filiales, 1984, 77: 104±114.
30. Colborne MJ, Edington GM. Mortality from malaria in Accra.Journal of tropical medicine and hygiene, 1954, 57: 203±210.
31. Delacollette C et al. Etude de la mortalite globale et de lamortalite lie e au paludisme dans le Kivu montagneux, Zaire.Revue e pidemiologique et sante publique, 1989, 37: 161±166.
32. Delacollette C, Barutwanayo M. Mortalite et morbidite auxjeunes aà ges dans une region aÁ paludisme hyperende mique stable,comme de Nyanza lac, Imbo Sud, Burundi. Bulletin de la Socie teÂde Pathologie Exotique et de ses Filiales, 1993, 86: 1±7.
33. Duren AN. Essai d'e tude sur l'importance du paludisme dans lamortalite au Congo belge. Annales Societe belge de Me decinetropicale, 1951, 31: 129±148.
34. Garenne M, Fontaine O. Assessing probable causes of deathusing a standardised questionnaire: a study in rural Senegal.Seminar on comparative studies of mortality and morbidity: oldand new approaches to measurement and analysis. Siena,International Union for the Scientific Study of Population and theInstitute of Statistics, University of Siena, 1986.
35. Ghana VAST Study Team. Vitamin A supplementation innorthern Ghana: effects on clinic attendances, hospital admis-sions and child mortality. Lancet, 1993, 342: 7±12.
36. Greenwood BM et al. Mortality and morbidity from malariaamong children in a rural area of the Gambia, West Africa.Transactions of the Royal Society of Tropical Medicine andHygiene, 1987, 81: 478±486.
37. Greenwood BM et al. Comparison of two strategies for thecontrol of malaria within a primary health care programme in theGambia. Lancet, 1988, 1: 1121±1127.
38. Greenwood BM et al. Mortality and morbidity from malariaafter stopping malaria chemoprophylaxis. Transactions of theRoyal Society of Tropical Medicine and Hygiene, 1995,89: 629±633.
Malaria mortality, morbidity and disability in Africa
637Bulletin of the World Health Organization, 1999, 77 (8)

39. Jaffar S et al. Changes in the pattern of infant and childhoodmortality in Upper River Division, the Gambia, from 1989 to1993. Tropical medicine and international health, 1997,2: 28±37.
40. Kaute Defo B. Epidemiology and control of infant and earlychildhood malaria: a competing risks analysis. Internationaljournal of epidemiology, 1995, 24: 204±217.
41. Mirza NM et al. Mortality patterns in a rural Kenya community.East African medical journal, 1990, 67: 823±829.
42. Molbak K et al. Persistent and acute diarrhoea as the leadingcauses of child mortality in urban Guinea-Bissau. Transactions ofthe Royal Society of Tropical Medicine and Hygiene, 1992,86: 216±220.
43. Mtango FDE, Neuvians D. Acute respiratory infections inchildren under five years: a control project in Bagamoyo District,Tanzania. Transactions of the Royal Society of Tropical Medicineand Hygiene, 1986, 80: 851±858.
44. N'Guessan Diplo L et al. La mortalite infantile et ses causesdans une sous-pre fecture de Coà te d'Ivoire. Me dicine tropicale,1990, 50: 430±432.
45. Omondi-Odhiambo J, van Ginneken JK, Voorhoeve AM.Mortality by cause of death in a rural area of Machakos District,Kenya in 1975±78. Journal of biosocial sciences, 1990,22: 63±75.
46. Pison G et al. Rapid decline in child mortality in a rural area ofSenegal. International journal of epidemiology, 1993,22: 72±80.
47. Premji Z et al. Community-based studies on childhood mortalityin a malaria holoendemic area on the Tanzanian coast. Actatropica, 1997, 63: 101±109.
48. Salum FM et al. Mortality of under fives in a rural area ofholoendemic malaria transmission. Acta tropica, 1994,58: 29±34.
49. Slutsker L et al. Infant and second year mortality in ruralMalawi: causes and descriptive epidemiology. American journaltropical medicine and hygiene, 1996, 55: 77±81.
50. Smedman L et al. Survival at 0±6 years of age in a peri-urbancommunity in Guinea-Bissau: a longitudinal assessment. Annalsof tropical paediatrics, 1986, 6: 67±72.
51. Spencer HC et al. Impact on mortality and fertility of acommunity-based malaria control programme in Saradidi,Kenya. Annals of tropical medicine and parasitology, 1987,81 (suppl. 2): 36±45.
52. Trape JF et al. Impact of chloroquine resistance on malariamortality. Comptes rendus de l'Acade mie des Sciences, Paris,Se rie III, 1998, 321: 689±697.
53. Van den Broeck J, Eeckels R, Vulylsteke A. Influence ofnutritional status on child mortality in rural Zaire. Lancet, 1993,341: 1491±1495.
54. Vella VV et al. Determinants of child mortality in south-westUganda. Journal of biosocial sciences, 1992, 24: 103±112.
55. Velema JP et al. Childhood mortality among users and non-users of primary health care in a rural West African community.International journal of epidemiology, 1991, 20: 474±479.
56. Velema JP et al. Malaria morbidity and mortality in childrenunder three years of age on the coast of Benin, West Africa.Transactions of the Royal Society of Tropical Medicine andHygiene, 1991, 85: 430±435.
57. Snow RW et al. Childhood deaths in Africa: uses and limitationsof verbal autopsies. Lancet, 1992, 340: 351±356.
58. Todd JE et al. The limitations of verbal autopsy in a malariaendemic region. Annals of tropical paediatrics, 1994, 4: 31±36.
59. Greenberg AE et al. Hospital-based surveillance of malariarelated paediatric morbidity and mortality, Kinshasa, Zaire.Bulletin of the World Health Organization, 1989, 67: 189±196.
60. Marsh K, Snow RW. The clinical epidemiology of falciparummalaria among African children. Parassitologia, in press.
61. Seboxa T, Snow RW. Epidemiological features of severepaediatric malaria in Humera district, North Western Ethiopia.East African medical journal, 1997, 74: 780±783.
62. Snow RW et al. Severe childhood malaria in two areas ofmarkedly different falciparum malaria transmission in East Africa.Acta tropica, 1994, 57: 289±300.
63. Trape JF et al. Malaria and urbanisation in Central Africa: theexample of Brazzaville. Part V: Pernicious attacks and mortality.Transactions of the Royal Society of Tropical Medicine andHygiene, 1987, 81 (suppl. 2): 34±42.
64. Rogier C et al. Plasmodium falciparum clinical malaria inDielmo, a holoendemic area in Senegal: no influence of acquiredimmunity on initial symptomatology and severity of malariaattacks. American journal of tropical medicine and hygiene,1999, 60: 410±420.
65. Smith T, Armstrong-Schellenberg JRM, Hayes R. Attribu-table fraction estimates and case definitions for malaria inendemic areas. Statistics in medicine, 1994, 13: 2345±2358.
66. Afari EA et al. Malaria infection, morbidity and transmission intwo ecological zones in Southern Ghana. African journal of healthsciences, 1995, 2: 312±315.
67. Akanmori BD et al. A longitudinal study of malaria infection,morbidity and antibody titres in infants of a rural community inGhana. Transactions of the Royal Society of Tropical Medicineand Hygiene, 1995, 89: 560±561.
68. Alonso PL et al. A malaria control trial using insecticide-treatedbed nets and targeted chemoprophylaxis in a rural area of theGambia, West Africa. 2: Mortality and morbidity from malaria inthe study area. Transactions of the Royal Society of TropicalMedicine and Hygiene, 1993, 87 (Suppl. 2): 13±17.
69. Alonso PL et al. A malaria control trial using insecticide-treatedbed nets and targeted chemoprophylaxis in a rural area of theGambia, West Africa. 6: The Impact of the interventions onmortality and morbidity. Transactions of the Royal Society ofTropical Medicine and Hygiene, 1993, 87 (Suppl. 2): 37±44.
70. Beach RF et al. Effectiveness of permethrin-impregnated bednets and curtains for malaria control in a holoendemic area ofWestern Kenya. American journal of tropical medicine andhygiene, 1993, 49: 290±300.
71. Bjorkman A et al. Monthly antimalarial chemotherapy tochildren in a holoendemic area of Liberia. Annals of tropicalmedicine and parasitology, 1986, 80: 155±167.
72. Ellman R et al. Malaria and anaemia at different altitudes in theMuheza district of Tanzania: childhood morbidity in relation tolevel of exposure to infection. Annals of tropical medicine andparasitology,1998, 92: 741±754.
73. Farnert A et al. Complexity of Plasmodium falciparuminfections is consistent over time and protects against clinicaldisease in Tanzanian children. Journal of infectious diseases,1999, 179: 989±995.
74. Hall SA, Wilks NE. A trial of chloroquine-medicated salt formalaria suppression in Uganda. American journal of tropicalmedicine and hygiene, 1967, 16: 429±442.
75. Kitua AY et al. Plasmodium falciparum malaria in the first yearof life in an area of intense and perennial transmission. Tropicalmedicine and international health, 1996, 1: 475±484.
76. Lemenge MM et al. Maloprim malaria prophylaxis in childrenliving in a holoendemic village in north-eastern Tanzania.Transactions of the Royal Society of Tropical Medicine andHygiene, 1997, 91: 68±73.
77. Lindsay SW et al. Malaria in a peri-urban area of theGambia. Annals of tropical medicine and parasitology, 1990,84: 553±562.
78. Marsh K et al. Anti-sporozoite antibodies and immunity tomalaria in a rural Gambian population. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 1988, 82: 532±537.
79. Menendez C et al. Randomised placebo-controlled trial of ironsupplementation and malaria chemoprophylaxis for preventionof severe anaemia and malaria in Tanzanian infants. Lancet,1997, 350: 844±850.
80. Mnzava AEP et al. The effects of house spraying with DDT orlambda-cyhalothrin against Anopheles arabiensis on measures ofmalarial morbidity in children in Tanzania. Acta tropica, 1993,54: 141±151.
Research
638 Bulletin of the World Health Organization, 1999, 77 (8)

81. Modiano D et al. Different response to Plasmodium falciparummalaria in West African sympatric ethnic groups. Proceedings ofthe National Academy of Sciences, 1996, 93: 13 206±13 211.
82. Mshana RN et al. In vitro lymphoproliferative responses tomalaria antigens: a prospective study of residents of aholoendemic area with perennial malaria transmission. Parasiteimmunology, 1993, 15: 35±45.
83. Mutinga MJ et al. Malaria prevalence and morbidity in relationto the use of permethrin-treated wall cloths in Kenya. East Africanmedical journal, 1993, 70: 756±762.
84. Procacci PG et al. Permethrin-impregnated curtains in malariacontrol. Transactions of the Royal Society of Tropical Medicineand Hygiene, 1991, 85: 181±185.
85. Rogier C, Trape JF. Malaria attacks in children exposed to hightransmission: who is protected? Transactions of the Royal Societyof Tropical Medicine and Hygiene, 1993, 87: 245±246.
86. Rooth I, Bjorkman A. Fever episodes in a holendemic malariaarea of Tanzania: parasitological and clinical findings anddiagnostic aspects related to malaria. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 1992, 86: 479±482.
87. Smith T et al. Absence of seasonal variation in malariaparasitaemia in an area of intense seasonal transmission.Acta tropica, 1993, 54: 55±72.
88. Snow RW, Rowan KM, Greenwood BM. A trial ofpermethrin-treated bed nets in the prevention of malaria inGambian children. Transactions of the Royal Society of TropicalMedicine and Hygiene, 1987, 81: 563±567.
89. Snow RW et al. A trial of bed nets (mosquito nets) as a malariacontrol strategy in a rural area of the Gambia, West Africa.Transactions of the Royal Society of Tropical Medicine andHygiene, 1988, 82: 212±215.
90. Snow RW et al. Perimethrin-treated bed nets (mosquito nets)prevent malaria in Gambian children. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 1988, 82: 838±842.
91. Trape JF, Zoulani A, Quinet MC. Assessment of the incidenceand prevalence of clinical malaria in semi-immune childrenexposed to intense and perennial transmission. American journalof epidemiology, 1987, 126: 193±201.
92. Trape JF et al. Malaria morbidity among children exposed tolow seasonal transmission in Dakar, Senegal, and its implicationsfor malaria control in tropical Africa. American journal of tropicalmedicine and hygiene, 1993, 48: 748±756.
93. Snow RW, Menon A, Greenwood BM. Measuring morbidityfrom malaria. Annals of tropical medicine and parasitology,1989, 83: 321±323.
94. Bruce-Chwatt LJ. A longitudinal survey of natural malariainfection in a group of West African adults. Part 1. West Africanmedical journal, 1963, 10: 141±173.
95. Lepers JP et al. Transmission and epidemiology of newlytransmitted falciparum malaria in the central highland plateaux ofMadagascar. Annals of tropical medicine and parasitology, 1991,85: 297±304.
96. Miller MJ. Observations on the natural history of malaria in thesemi-immune resistant West African. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 1958, 52: 152±168.
97. Petersen E et al. Clinical and parasitological studies on malariain Liberian adults living under intense malaria transmission.Annals of tropical medicine and parasitology, 1991,85: 577±584.
98. McGregor IA. Epidemiology, malaria and pregnancy. Annals oftropical medicine and parasitology, 1984, 33: 517±525.
99. Diseko R. Malaria in Botswana. Minutes of the Annual MalariaConference, St. Lucia, South Africa, October 1994 (unpublisheddocument).
100. Freeman T. A review of the epidemiology of malariatransmission and distribution in Zimbabwe and the relationship ofmalaria outbreaks to preceding meteorological conditions.Report for German Society for Technical Cooperation (DTZ), 1995(unpublished document).
101. Kunene S. Malaria in Swaziland. Minutes of the Annual MalariaConference, St. Lucia, South Africa, October 1994 (unpublisheddocument).
102. Kwa Zulu Department of Health. Annual report on malaria in1990. Kozi Bay, South Africa, Ministry of Health, October 1991(unpublished document).
103. Ministry of Health, South Africa. Annual malaria report.KwaZulu Natal Health Department, 1989.
104. Ministry of Health, Zimbabwe. Mashonland East: malariaand schistosomiasis. Report by the Regional Medical Director,September 1995.
105. Ministry of Health, Zimbabwe. Matabeleland SouthProvince: malaria report. National Malaria Conference,Victoria Falls, September 1996.
106. Ngoxongo S. Malaria annual report, KwaZulu, 1987. Reportpublished by KwaZulu Department of Health, South AfricanMinistry of Health, 1987.
107. Strebel PM, Hansford CF, Kustner HGV. The geographicdistribution of malaria in South Africa in 1986. The southernAfrica journal of epidemiology and infection, 1988, 3: 4±8.
108. Farnsworth-Anderson TF. Report on an investigation ofhealth conditions of farms in the Trans-Nzoia, with specialreference to malaria. Kenya and East Africa medical journal,1930, 6: 274±308.
109. Fontaine RE, Najjar AE, Prince JS. The 1958 malaria epidemicin Ethiopia. American journal of tropical medicine and hygiene,1961, 10: 795±803.
110. Brown V et al. Epidemic of malaria in north-eastern Kenya.Lancet, 1998, 352: 1356±1357.
111. Strangeways-Dixon D. Paludrine (proguanil) as a malariaprophylactic amongst African labour in Kenya. East Africanmedical journal, 1950, 27: 125±130.
112. Le Sueur D, Sharp BL, Appleton CC. Historical perspective ofthe malaria problem in Natal with emphasis on the period 1928±1932. South African journal of science, 1993, 89: 232±239.
113. Warsame M et al. An epidemic of Plasmodium falciparummalaria in Balcad, Somalia, and its causation. Transactions ofthe Royal Society of Tropical Medicine and Hygiene, 1995,89: 142±145.
114. Lepers JP et al. Newly transmitted Plasmodium falciparummalaria in the central highland plateaux of Madagascar:assessment of clinical impact in a rural community. Bulletin of theWorld Health Organization, 1990, 68: 217±222.
115. Warrell DA. Cerebral malaria: clinical features, pathophysiologyand treatment. Annals of tropical medicine and parasitology,1997, 91: 875±884.
116. Marsh K. Neurological sequelae of cerebral malaria. Paperprepared for WHO/TDR meeting, 4±8 December 1995, Geneva.
117. Waller D et al. Clinical features and outcome of severemalaria in Gambian children. Clinical infectious diseases, 1997,21: 577±587.
118. Molyneux ME et al. Clinical features and prognostic indicatorsin paediatric cerebral malaria: a study of 131 comatose Malawianchildren. Quarterly journal of medicine, 1989, 71: 441±459.
119. Brewster DR, Kwiatkowski D, White NJ. Neurologicalsequelae of cerebral malaria in children. Lancet, 1990,336: 1039±1043.
120. Bondi FS. The incidence and outcome of neurologicalabnormalities in childhood cerebral malaria: a long-term follow-up of 62 survivors. Transactions of the Royal Society of TropicalMedicine and Hygiene, 1992, 86: 17±19.
121. Carme B, Bouquety JC, Plassart H. Mortality and sequelaedue to cerebral malaria in African children in Brazzaville, Congo.American journal of tropical medicine and hygiene, 1993,48: 216±221.
122. Van Hensbroek MB et al. Residual neurological sequelae afterchildhood cerebral malaria. Journal of paediatrics, 1997,131: 125±129.
Malaria mortality, morbidity and disability in Africa
639Bulletin of the World Health Organization, 1999, 77 (8)

123. Greenberg AE et al. The association between malaria, bloodtransfusions and HIV seropositivity in a paediatric population inKinshasa, Zaire. Journal of the American Medical Association,1988, 259: 545±549.
124. Schmutzhard E, Rainer J, Rwechungura RI. Treatment ofsevere malarial anaemia in East Africa's under fives: anunsolvable problem since the advent of AIDS? Transactions of theRoyal Society of Tropical Medicine and Hygiene, 1988, 82: 220.
125. Schapira A et al. Comparison of intramuscular and intravenousquinine for the treatment of severe and complicated malaria inchildren. Transactions of the Royal Society of Tropical Medicine &Hygiene, 1993, 87: 299±302.
126. Bojang KA et al. Management of severe malarial anaemia inGambian children. Transactions of the Royal Society of TropicalMedicine and Hygiene, 1997, 91: 557±561.
127. Brewster DR, Greenwood BM. Seasonal variation ofpaediatric diseases in the Gambia, West Africa. Annals of tropicalpaediatrics, 1993, 13: 133±146.
128. Dorward JA, Knowles JK, Dorward IM. Treatment of severeanaemia in children in a rural hospital. Tropical doctor, 1989,19: 155±158.
129. Emerton DGC. An audit of the management of malaria in aTanzanian district hospital. Transactions of the Royal Society ofTropical Medicine and Hygiene, 1992, 86: 476±478.
130. Lackritz EM et al. Effect of blood transfusion on survival amongchildren in a Kenyan hospital. Lancet, 1992, 340: 524±528.
131. Marsh K et al. Life-threatening malaria in African children:clinical spectrum and simplified prognostic criteria. New Englandjournal of medicine, 1995, 332: 1399±1404.
132. Slutsker L et al. In-hospital morbidity and mortality due tomalaria-associated severe anaemia in two areas of Malawi withdifferent patterns of malaria infection. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 1994, 88: 548±551.
133. Lindsay SW, Martens WJM. Malaria in the African Highlands:past, present and future. Bulletin of the World HealthOrganization, 1998, 76: 33±45.
134. Snow RW, Marsh K, Le Sueur D. The need for maps oftransmission intensity to guide malaria control in Africa.Parasitology today, 1996, 12: 455±457.
135. Le Sueur D et al. An atlas of malaria in Africa. Africa health,1997, 19: 23±24.
136. Snow RW et al. Models to predict the intensity of Plasmodiumfalciparum transmission: applications to the burden of disease inKenya. Transactions of the Royal Society of Tropical Medicine andHygiene, 1998, 92: 601±606.
Research
640 Bulletin of the World Health Organization, 1999, 77 (8)