regional referral centers pilot study affiliated tribes of nw indians airway heights, wa september...
TRANSCRIPT

Regional Referral Regional Referral Centers Pilot Study Centers Pilot Study
Affiliated Tribes of NW IndiansAffiliated Tribes of NW Indians
Airway Heights, WAAirway Heights, WA
September 21, 2010September 21, 2010
Portland Area Facilities Advisory Portland Area Facilities Advisory CommitteeCommittee

2
What are Regional Referral Centers?– A facility where specialty care services are
provided on a referral basis by surrounding health programs.
– A facility that might provide colonoscopy, endoscopic, cardiac stress tests, etc. (Priority 2 types of services)
– A program that does not have the high costs of maintaining a hospital
– Culturally competent care – Does not fit within current IHS facility structure
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport

3
What are the benefits of Regional Centers?– Address CHS Dependency and equity concerns
– Provide some level of specialty care service for the Portland Area
– Provide a vehicle for telemedicine services
– Improve access to care and improve quality of care
– Cost savings for Tribal CHS programs
– Generate third party reimbursements that can be used to provide additional services
– Provide culturally competent care
– Reduce the amount of construction funding required
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport
4
Why was this concept proposed?– Healthcare Facilities Construction Priority System
• No Portland Area representation since early ‘90s• Regional Referral Centers cannot be prioritized
– Facilities funding received is inadequate• Limited to Small Ambulatory and Dental Programs
– Rarely has fully funded any projects (requiring tribal contributions)
– No funding for staffing or operations
– Recurring funding increases favor new facilities • Recurring Pay Act and Inflation increases are greater• More staff, more patient visits generate more 3rd-party collections
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport

5
How was the concept developed?IHS Areas directed to develop master plans– Memo, Acting Director, IHS, Feb. 11, 2003
• Define the healthcare needs for the Area– Identify healthcare needs of the Area Service Population– Identify type and location of facilities needed– $150,000 provided to each Area Office to assist in completing
master plans
• All PAO Tribes given 2 options for completing master plans– 26 PSAs (21 Tribes) master plans completed by contract– 22 Tribes provided partial funding to complete individually
PAFAC 2010 – Regional Referral Center Pilot Study PAFAC 2010 – Regional Referral Center Pilot Study Status ReportStatus Report
6
How was the concept developed?– Criteria defined by Tribes participating in master
planning contract• Primary Care will remain a local service• Share referrals to justify specialty services• Facilities recommended
– 55 Primary Service Areas (includes 3 urban, 4 new)– 3 outpatient specialty Regional Referral Centers– 1 Area-wide Medical Center (hospital)
– Concept presented to NPAIHB, ATNI• Supporting resolutions passed• Portland Area Health Services Master Plan Final Report
– Completed and submitted October 1, 2005
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport
7
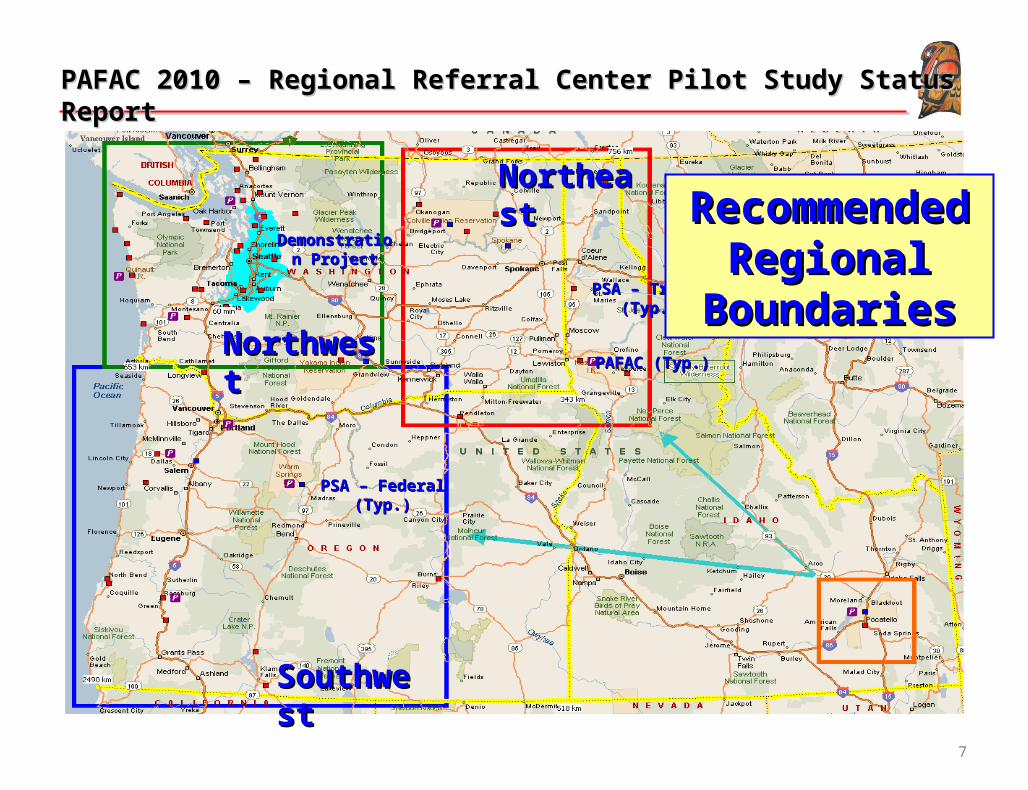
NorthwestNorthwest
NortheastNortheast
SouthwestSouthwest
PSAPSA – Tribal (Typ.)– Tribal (Typ.)
PSA – Federal (Typ.)PSA – Federal (Typ.)
Demonstration Demonstration ProjectProject
PAFACPAFAC (Typ.)(Typ.)
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport
Recommended Recommended Regional Regional
BoundariesBoundaries

8
• Recommended Participating Tribes by Region
1Region to be selected by Tribe.
Northeast Northwest Southwest
1. Coeur D’Alene Chehalis Samish Burns Paiute
2. Colville Hoh River Sauk-Suiattle Chemawa
3. Kalispel Jamestown Shoalwater CLUSTI
4. Kootenai Lower Elwha Skokomish Coquille
5. Nez Perce Lummi Snoqualmie Cow Creek
6. NW Band of Shoshone1 Makah Squaxin Island Cowlitz
7. Shoshone-Bannock1 Muckleshoot Stillaguamish Grand Ronde
8. Spokane Nisqually Suquamish Klamath
9. Umatilla Nooksack Swinomish Siletz
10. Port Gamble Tulalip Warm Springs
11. Puyallup Upper Skagit
12. Quileute Yakama
13. Quinault
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport

9
PSA – Tribal (Typ.)PSA – Tribal (Typ.)
PSA – Federal (Typ.)PSA – Federal (Typ.)
Demonstration Demonstration Project Project
BoundaryBoundary
PAFAC (Typ.)PAFAC (Typ.)
PAFAC 2010 – Regional Referral Center Pilot Study PAFAC 2010 – Regional Referral Center Pilot Study Status ReportStatus Report
Recommended Recommended Demonstration Demonstration
ProjectProject

10
• Recommended Demonstration Project
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport
Recommended Participants* Possible Services
1. Stillaguamish Audiology
2. Tulalip Medical Specialties
3. Snoqualmie Surgical Specialties
4. Muckleshoot Ambulatory Surgery
5. Puyallup Advanced Imaging (Fluor, Mammo, CT, MRI)
6. Nisqually Occupational Therapy
7. Port Gamble S’Klallam Speech Therapy
Telemedicine
*Initial workload will be based on a 60-minute drive time resulting in 24,000 primary care users in the NW region.

11
What's transpired?Proposed regional facilities were entered into current priority system
– Regional referral centers could not be prioritized
•Needs can be defined for large, centralized populations•Smaller, geographically dispersed populations left out
– A Pilot Study was proposed to•Develop preliminary planning criteria to size
regional referral centers for small, dispersed populations
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport

12
What's transpired?– HQ-Area discussions generated 3 questions
• Specialty referral rates• Distance patients are willing to travel• Impacts of alternative care sources
– HQ agreed to fund the Pilot Study• To provide recommendations on the modification of
planning criteria for geographically dispersed, multi-tribal populations.
– For National application (CA, OK, NS, BE Areas are interested)– Allow referral centers to be prioritized– Overseen by the PAFAC
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport

13
What's transpired?– The Pilot Study determined insufficient data
is available for preliminary planning• Recommended a demonstration project to:
– Gather data to establish planning thresholds
– Focus on specialty care only
– Test assumptions on the viability of Regional Referral Centers
• PAFAC requested funding for a demonstration project November 2009
– Awaiting Headquarters response
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport
14
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport
Summary – the demonstration project will:
1. be new funding for the Area with a recurring staffing package.
2. not diminish current funding or services for tribes.
3. provide only specialty care; primary care will continue to be provided at local sites.
4. is the first of a 3-phase master plan.
5. be available to ALL Tribes for referral to the facility.
6. reduce Tribes dependency on CHS, allowing CHS funding to be stretched further.
7. result in better continuity of care.

15
Requesting a resolution adopted by ATNI:to support the planning and design of the Portland Area Regional Referral Center demonstration project.
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport
16
Questions…?Questions…?
To review full study you can access at NPAIHB’s websiteTo review full study you can access at NPAIHB’s websitewww.npaihb/XXXXXwww.npaihb/XXXXX
PAFAC 2010 – Regional Referral Center Pilot Study Status PAFAC 2010 – Regional Referral Center Pilot Study Status ReportReport