region 7 emergency medical services systems intermediate life support standing medical orders
DESCRIPTION
REGION 7 EMERGENCY MEDICAL SERVICES SYSTEMS INTERMEDIATE LIFE SUPPORT STANDING MEDICAL ORDERS. PowerPoint Study Guide. - PowerPoint PPT PresentationTRANSCRIPT

REGION 7EMERGENCY MEDICAL SERVICES SYSTEMS
INTERMEDIATE LIFE SUPPORTSTANDING MEDICAL ORDERS
PowerPoint Study Guide
Revised 01/01/12Effective 05/01/98ILS
The following Powerpoint only highlights major changes in ILS SMO’s for 2012. Please consult the entire SMO book for details of changes that may not be addressed here. Your SMO exam can address any change, whether highlighted here or not.

Code 1INITIAL MEDICAL CARE
ROUTINE CARDIAC CAREGENERAL PATIENT ASSESSMENT
1. Prehospital providers shall always assess the scene to assure the safety of all personnel.2. Patient care and treatment begins at the “bedside.”3. Prehospital personnel shall take all reasonable precautions to prevent exposure to blood and/or body fluids of any patient. Use fluid repellent gowns, masks and goggles as situation dictates.4. For Pediatric Dosing, utilize a length based Pediatric Tape or Chart.
GENERAL PATIENT ASSESSMENT1. Initial Assessment A. Airway - Establish and/or maintain an airway (cervical spine control, if indicated) B. Breathing - Assist ventilation as required C. Circulation (pulse) and hemorrhage control (if indicated) D. Disability (Level of Consciousness) 1. “Alert” 2. “Verbal” - (responds to verbal stimuli) 3. “Pain” - (responds to painful stimuli) 4. “Unresponsive” E. Exposure and examine (if indicated)2. Focused Assessment A. Vital signs, and where applicable, Glasgow Coma Scoring parameters B. Systematic head - to - toe detailed assessment C. History of present illness/injury
INITIAL MEDICAL CARE/ROUTINE CARDIAC CARE1. Reassure patient, provide comfort and loosen tight clothing.2. Sit patient in semi-Fowler’s or position of comfort (if applicable)3. Obtain Pulse Oximeter value prior to oxygen delivery Deliver OXYGEN 2-6 L by nasal cannula or 12-15L by mask, unless otherwise specified.4. Evaluate cardiac rhythm, if indicated. Consider use of 12-lead, if available. (All ALS patients do not necessarily require continuous ECG monitoring or transmission of a strip to the hospital.)5. If patient’s condition warrants, obtain IV access (Saline lock or NS). Attempt x2 unless requested to continue.6. For adult and pediatrics ≥ 1 year old experiencing nausea, consider Zofran ODT 4mg tab x 1 dose only.7. Contact hospital as soon as patient’s condition permits. Transmit assessment information and await orders. If no radio contact can be established or patient’s condition requires immediate treatment, refer to appropriate SMO and begin intervention immediately.8. Recheck vitals and other pertinent signs at least every 15 minutes and record, noting times.9. Transport to closest hospital. NOTE: By law, a physician must certify that the benefits outweigh the risk of transport to a facility other than the nearest hospital. If the patient refuses care or transport to the closest hospital, refer to policy and document signatures and situation.NOTE: In a combative or uncooperative patient, the requirement to initiate initial routine medical care, as written,may be altered or waived in favor of rapidly transporting the patient for definitive care. Document the patient'sactions or behaviors which interfered with the performance of any assessments and/or interventions.
OUTLINE FOR RADIO REPORT (Transmit using as few words as possible)
1. Name and vehicle number of provider 6. Pertinent Medical History:2. Requested destination, closest hospital, - Allergies and estimated time of arrival -Medications3. Age, sex, and approximate weight of patient -Past History of Current Illness4. Chief Complaint, to include symptoms -Last Meal and degree of distress -Events surrounding incident5. History of present illness/injury 7. Clinical condition: -Focused and detailed patient assessment findings
8. Treatment initiated and Response
Revised 12/01/11Effective 05/01/98ILS

Code 6 VENTRICULAR FIBRILLATION/
PULSELESS VENTRICULAR TACHYCARDIA
-ABCs-Perform CPR until defibrillator attached
-VF/VT present on monitor
Give 1 shockBiphasic Device Specific (120-200J)
Monophasic 360JResume CPR Immediately
-
Revised 01/01/12Effective 05/01/98ILS
Continue CPR – minimize any interruptions throughout resuscitation -Intubate if unable to BVM -Consider King tube -IV/IO NS without interrupting CPR
Perform 5 cycles of CPR
Check Rhythm
Shockable rhythm?
Continue CPR while Defibrillator is charging
Biphasic device specific (120-200J) or Monophasic 360J
Resume CPR immediately after the shock Epinephrine 1:10,000 mg IV/IO
Repeat every 3-5 minutes as long a rhythm persists
Perform 5 cycles of CPR
Check rhythm
Shockable rhythm?
Continue CPR while Defibrillator is charging
Give 1 shock
Biphasic Device Specific (120-200J)
or Monophasic 360J
Resume CPR immediately after shock
Consider antiarrhythmics; give during CPR
Lidocaine 1.5mg/kg IV/IO first dose
May repeat 0.75 mg/kg IV/IO
Maximum 3mg/kg
TRANSPORT

PULSELESS ARRESTPerform CPR
Attach monitor/defibrillator
Asystole/PEA
Resume CPR immediately for 5 cyclesWhen IV available
Epinephrine 1:10,000 - 1 mg IV/IO
Repeat every 3 to 5 minutes
Consider Treatment for possible causes
TRANSPORT
Go to Code 6
Code 9
AT DISCRETION OF A PHYSICIAN/ECRN:ALS MUTUAL AID
Revised 01/01/12Effective 05/01/98ILS
Hypothermia ------------------------------> Follow appropriate SMOHypovolemia -----------------------------> Fluid challenge (200ml of current IV)Tension Pneumothorax ----------------> Pleural DecompressionAcidosis/Hypoxemia --------------------> Ventilate with 100% OXYGEN (Check tube placement)Pulmonary Embolism ------------------> Rapid TRANSPORT with 100% OXYGEN
Shockable
Perform 5 cycles of CPR
Check rhythm
Shockable rhythm?
Not Shockable
PULSELESS ELECTRICAL ACTIVITY/ASYSTOLE
Continue CPR – minimize any interruptions throughout resuscitation -Intubate if unable to BVM -Consider King tube -IV/IO NS without interrupting CPR

Code 12
SUSPECTED CARDIAC PATIENT
INITIAL MEDICAL CAREPerform 12-Lead ECG and Transmit, if available
SBP 90-110mmHgSBP <90mmHg
Refer to appropriate
SMO
SBP >110mmHg
TRANSPORT
NOTE TO PREHOSPITAL PROVIDERS:
*Contraindications to ASPIRIN would include ASPIRIN allergy & history of gastrointestinal bleeding. ** Contact Medical Control prior to administration of NITRATES if patient is taking erectile dysfunctional medications ( i.e. Viagra, Levietra, Cialis).
Revised 01/01/12Effective 05/01/98ILS
4 tabs *BABY ASPIRIN POunless
contraindicated*
NITROGLYCERIN** gr 1/150 tab OR spray SL May repeat X 2 in 5 minutes (If no IV, consider hospital contact prior to administration)
Repeat vital signs
4 tabs *BABY ASPIRIN PO
unless contraindicated*
TRANSPORT
4 tabs *BABY ASPIRIN POunless
contraindicated*
Consider 12-Lead EKG for complaints of: (may be deferred if patient unstable)•Chest pain/Discomfort/Pressure•Arm Pain (non-traumatic)•Jaw Pain (non-traumatic)•Upper back pain (non-traumatic)•Unexplained diaphoresis•Vomiting without fever or diarrhea•Shortness of breath•Dizziness/syncope•Epigastric pain•Fall in the elderly (unexplained)•Weakness/Fatigue•Bradycardia or Tachycardia

Code 13
PULMONARY EDEMA DUE TO HEART FAILURE
INITIAL MEDICAL CARE
If wheezing:ALBUTEROL (Ventolin)
2.5mg via nebulizer(May repeat X 1)
SBP >110mmHg
Consider CPAP enroute, if available Refer to CONTINUOUS POSITIVE AIRWAY PRESSURE ADMINISTRATION
CODE 76
TRANSPORT
Revised 01/01/12Effective 05/01/98ILS
Refer to CARDIOGENIC SHOCK
CODE 5
NITROGLYCERIN*gr 1/150 tab OR spray SL
(May repeat X 2 in 5 minutes)(If no IV, consider hospital contact
prior to administration)
TRANSPORT
If wheezing: ALBUTEROL (Ventolin)
2.5mg via nebulizer (May repeat X 1)
If wheezing: ALBUTEROL (Ventolin) 2.5mg via nebulizer (May repeat X 1)
NOTE TO PREHOSPITAL PROVIDERS:* Contact Medical Control prior to administration of NITRATES if patient is taking erectile dysfunctional medications ( i.e. Viagra, Levietra, Cialis).
SBP 90 - 110mmHgSBP < 90mmHg
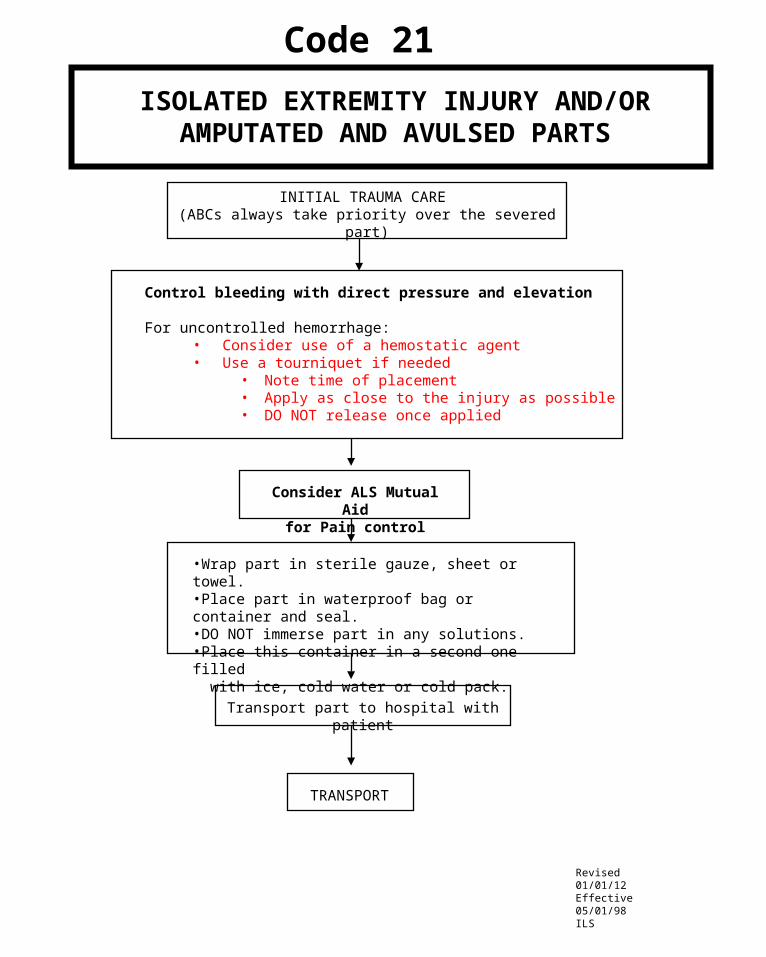
Code 21
ISOLATED EXTREMITY INJURY AND/ORAMPUTATED AND AVULSED PARTS
INITIAL TRAUMA CARE (ABCs always take priority over the severed part)
Consider ALS Mutual Aidfor Pain control
Control bleeding with direct pressure and elevation
For uncontrolled hemorrhage:• Consider use of a hemostatic agent• Use a tourniquet if needed
• Note time of placement• Apply as close to the injury as possible• DO NOT release once applied
•Wrap part in sterile gauze, sheet or towel.•Place part in waterproof bag or container and seal. •DO NOT immerse part in any solutions.•Place this container in a second one filled with ice, cold water or cold pack.
Transport part to hospital with patient
TRANSPORT
Revised 01/01/12Effective 05/01/98ILS

Code 22
BURNSBurn patients are often victims of multiple trauma.
Treatment of major traumatic injuries takes precedence over wound management.Isolated burn injury patients should be transferred to the closest available hospital
ASSESS•Total body surface area: use rule of 9s or estimate using patient’s palmar surface as 1%•Depth of burn: partial or full thickness, consider exposure to products of combustion and treat as soon as possible.
CHEMICALTHERMAL ELECTRICAL
INITIAL TRAUMA CARE INITIAL TRAUMA CARE Without placing self at risk forinjury, remove patient from sourceof electricity or have power cut off.
OXYGEN 100% (Use humidifiedOxygen, if available). Note presenceof hoarseness, wheezing, stridor orproductive cough and document.If present, refer to ACCELERATED TRANSPORT CODE 26
Brush off excess drychemicals
INITIAL TRAUMA CARE
Irrigate or flush with copiousamounts of water or saline
unless contraindicated.
For eye exposures Refer toHAZARDOUS MATERIALS-EYE
CODE 40
Perform spinal immobilization,apply monitor and treat
dysrhythmias per appropriate SMO.
Burn Wound Care
Note quality of distal pulse inextremity burns and document.
Burn Wound Care - Moderate to Critical Burn
Follow routine Burn Wound CareAssess for entry and exit wounds,
neurovascular status of affected parts.
No cooling necessary
Wear sterile gloves and masksuntil burn wounds are covered.Remove clothing, jewelry, etc.Do not pull away clothing thatis stuck to burn wound.
TRANSPORT
Cover with dry, sterile dressings
TRANSPORT
COOL BURN with sterile water or saline until skin feels cool to your touch. Don’t overcool any majorburn. Do not use ICE directly on burn. Cover burnwound with sterile dressing. Moisten with NormalSaline. DO NOT BREAK BLISTERS. DO NOTAPPLY CREAMS, OINTMENTS OR ANTIDOTES TO BURNS.
NOTE TO PREHOSPITAL PROVIDER:FOR ALL TYPES OF BURNS:Consider ALS Mutual Aid
>20%2° or 3°
Apply sterile dry dressing.
Open sterile sheet on stretcher before placing patient for TRANSPORT.Cover patient with dry, sterile sheets and blanket to maintain body temperature.
Revised 01/01/12Effective 05/01/98ILS

Code 24
TRAUMA IN PREGNANCY
Principles of Management
A. Routine Trauma Care
B. Increased IV volume is needed. Establish IV. If total transport time is less than 30 minutes, no IV should be attempted unless it will not delay transport to the nearest Trauma Center
C. Check externally for uterine contractions.
D. Check externally for vaginal bleeding.
E. Unless spinal injury is suspected, transport the patient on her left side to minimize uterine compression of the inferior vena cava.
F. If a patient with suspected spinal injury becomes hypotensive while supine on backboard, elevate right side of backboard to relieve pressure on vena cava from uterus.
G. Manually displace the uterus to the left side during CPR.
Revised 01/01/12Effective 05/01/98ILS

Code 30ACUTE ASTHMA/COPD WITH WHEEZING
INITIAL MEDICAL CARE*
TRANSPORT IMMEDIATELYDO ALL TREATMENT ENROUTE
Continue TRANSPORT
NOTE TO PREHOSPITAL PROVIDERS: 1) *OXYGEN @ 2 - 6L/min. If severe respiratory distress or cyanosis, 15L NRB 2) IV optional unless patient is in severe respiratory distress or pending failure 3) For pediatric patients, refer to PEDIATRIC RESPIRATORY DISTRESS CODE 55. 4) If intubation required, may give ALBUTEROL (Ventolin) in-line via ET tube. 5) For prolonged geographical transport, consider METHYLPREDNISOLONE (Solu-Medrol) 125mg IV push.
Reviewed 01/01/12Effective 05/01/98ILS
ALBUTEROL (Ventolin)2.5mg via nebulizer
(may repeat x1)
AT THE DESCRETION OF A PHYSICIAN/ECRN:1. Administer EPINEPHRINE 1:1000 @ 0.01mg/kg up to 0.3mg IM (may repeat in 15 minutes).
May administer patient’s EPINEPHRINE PEN, if available
2. CPAP if available

DIABETIC/GLUCOSE EMERGENCIES
Obtain blood sugar level reading
If patient is awake and gag reflex intact, administer small amountsof sugar solution sublingually if unable to establish IV.
TRANSPORT
TRANSPORT
Blood sugar level >180 orsigns & symptoms of
Ketoacidosis
IV NS – 200ml bolusMay repeat at Physician
discretion
INITIAL MEDICAL CARE(Include history of time last medication taken and whether or not patient has eaten.)
Blood sugar level <60 orsigns & symptoms of Insulin
Shock or Hypoglycemia
50% DEXTROSE 50ml IVOR
GLUCAGON 1mg IM/IN, if available (If IV not able to be established)
If none or limited response:may repeat DEXTROSE IVP
Revised 01/01/12Effective 05/01/98ILS
Code 32

Code 33*DRUG OVERDOSE
ALCOHOL RELATED EMERGENCIES/POISONING
Obtain Blood Glucose Reading
If suspected narcotic or synthetic narcotic overdose and respiratory rate <12 Administer NALOXONE (Narcan) 2mg IV/IM/IN
(Consider restraints prior to administration.) May be repeated every 5 minutes as necessary, up to 6mg.
If blood sugarlevel <60:
DEXTROSE 50% 50ml IVPOR
GLUCAGON 1mg IM/IN(If IV not able to be established)
TRANSPORT
SUSPECTED TRICYCLIC ANTIDEPRESSANT OVERDOSE**
INITIAL MEDICAL CARE
Consider ALS Mutual Aid
TRANSPORT
**TRICYCLIC ANTIDEPRESSANTS INCLUDE:AMITRIPTYLINE, AMOXAPINE, ASCENDIN, DESIPRAMINE, DESYREL, ELAVIL, ENDEP,IMIPRAMINE, LUDIOMIL, NORPARAMINE, PAMELOR, SINEQUAN, TRIAVIL, TOFRANIL , and others
Revised 01/01/12Effective 05/01/98ILS
INITIAL MEDICAL CARE
NOTE TO PREHOSPITAL PROVIDERS:*Refer to PEDIATRIC ALTERED LEVELOF CONSCIOUSNESS CODE 60, as needed

Code 34
COMA OF UNKNOWN ORIGIN(NO HISTORY OF TRAUMA)
Assess level of consciousnessusing Glasgow Coma Scale
If respiratory rate <12Administer NALOXONE (Narcan) 2mg IV/IM/IN, if available
(Consider restraints prior to administration)May be repeated every 5 minutes as necessary, up to 6mg.
Monitor neuro status, vital signs, ECG andtransport patient secured to backboard.Protect airway - be prepared to suctionand/or intubate if no gag reflex present.
Revised 01/01/12Effective 05/01/98ILS
INITIAL MEDICAL CARE
Obtain Blood Glucose ReadingIf <60
DEXTROSE 50ml of 50% IVPOR
GLUCAGON 1mg IM/IN, if available(If IV not able to be established)
TRANSPORT
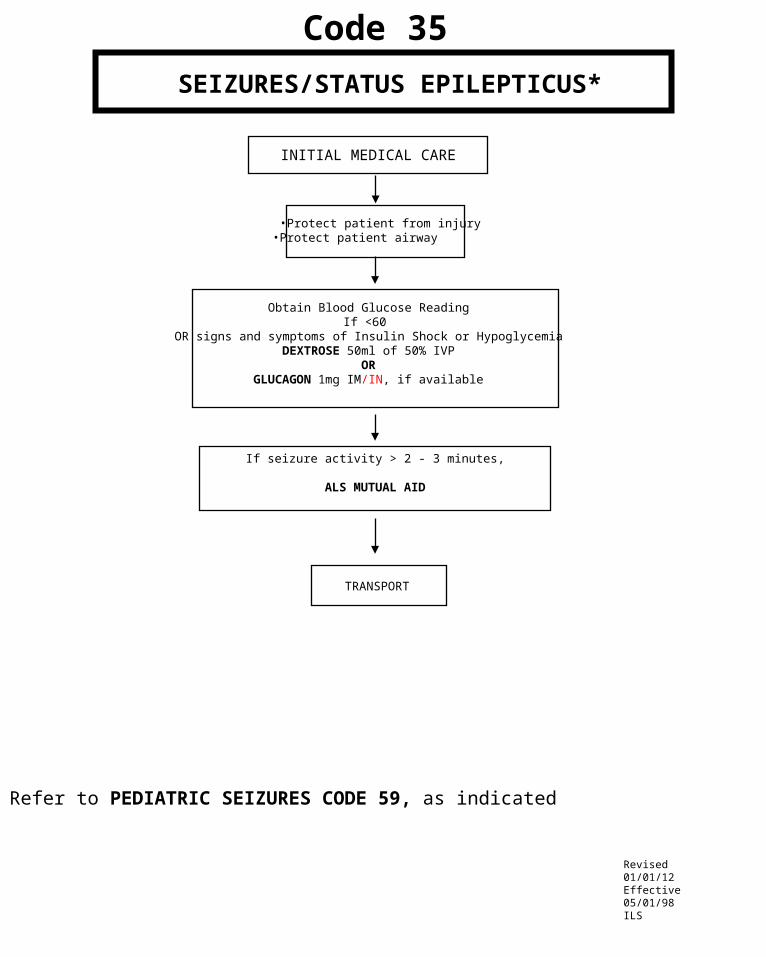
Code 35
SEIZURES/STATUS EPILEPTICUS*
INITIAL MEDICAL CARE
•Protect patient from injury•Protect patient airway
Obtain Blood Glucose ReadingIf <60
OR signs and symptoms of Insulin Shock or HypoglycemiaDEXTROSE 50ml of 50% IVP
ORGLUCAGON 1mg IM/IN, if available
If seizure activity > 2 - 3 minutes,
ALS MUTUAL AID
Revised 01/01/12Effective 05/01/98ILS
* Refer to PEDIATRIC SEIZURES CODE 59, as indicated
TRANSPORT

Code 48RESUSCITATION AND CARE OF THE NEWBORN
Infant Care
Begin Infant Prehospital Care Report
Document time of delivery
Is meconium present?No
Yes
Quickly dry baby & continueairway support. Spontaneousrespirations should beginwithin 15 seconds afterstimulating reflexes. If not,begin ventilations at 40-60breaths per minute. If nobrachial pulse or pulse <60,begin CPR at 3 to 1 and accelerated transport. Refer to Code 51
No
Clear airwayIntubate as soon as possible. Refer to MECONIUM ASPIRATOR (CODE 84) 1 time. Attempt to ventilate with BVM
Able to ventilate?Obtain one minute APGAR SCORE
Wait for cord pulsations tostop. Clamp cord 6-8 inchesfrom infant’s body. Cut between clamps with sterileknife or scissors.
Yes
No
Continue to repeat MECONIUM ASPIRATOR (CODE 84) and attempt to ventilate with BVM until able to ventilate
ACCELERATED TRANSPORTDry baby, wrap in chux or blanket to maintain body heat. Utilize an infant hat, if available. If in cold environment, wrap aluminum foil or silver swaddler around blanket to insulate. If placenta has delivered, it may be used as aheat source. Place placenta in plastic bag and wrap infant and placenta in blanket insulated with foil.
Place infant on side, preferably head lower than trunk, suction as needed. IF INFANT IS CYANOTIC, BUT BREATHING SPONTANEOUSLY, place adult face mask next to infant’s face & administer OXYGEN at 6L/minute.
Obtain five minute APGAR SCORE and document on report form.
Place ID tags on mother and infant. TRANSPORTReviewed 01/01/12Effective 05/01/98ILS
THE APGAR SCORE Score 1 min 5 min Sign 0 1 2
Appearance Blue, pale Body pink, Completely pink (Skin Color) extremities blue
Pulse Rate Absent Below 100 Above 100 (Heart Rate)
Grimace No Response Grimaces Cries (Irritability)
Activity Limp Some flexion of Active Motion extremities
Respiratory Absent slow and Strong Cry (Effort) irregular TOTAL SCORE=
Is infant limp?
Yes

Assess Airway
•Administer 100% OXYGEN•Support ventilation with BVM •Age appropriate rate
Relieve Upper Airway Obstruction•Reposition airway•Consider back slaps, chest/abdominal thrusts (age dependent)•Direct laryngoscopy, foreign body removal with Magill forceps if indicated• Secure airway as appropriate• Consider needle cricothyrotomy
•Administer 100% OXYGEN•Support ventilation with BVM as indicated•Secure airway as appropriate•Establish vascular access IV/IO NS @ TKO•Consider NALOXONE (Narcan) IV/IO/IM if respiratory rate <12: per length based Pediatric Tape•Consider blood glucose test and administration of:
•D25% IV/IO: 2ml/kg OR•D12.5% IV/IO for infants under 2 months* IV/IO 4ml/kg
Refer to PEDIATRICSHOCK CODE 57or PEDIATRICCARDIAC ARREST CODE 51
•Support ABCs•Complete initial assessment•Cardiac monitor•Pulse oximetry•Observe•Keep warm•TRANSPORT
•Perform airway maneuver, maintaining in-line C-spine stabilization.
• jaw thrust or chin lift/head tilt• suction• oropharyngeal airway
• C-spine immobilization as indicated
NOTE TO PREHOSPITAL PROVIDERS:Respiratory arrest may be a presenting sign of a toxic ingestion or metabolic disorder.
**Refer to PEDIATRIC ASSESSMENT AND TRAUMA SCORE CODE 28
Chest Rise Inadequate
Revised 01/01/12Effective 05/01/98ILS
Hypoperfusion** Normal Perfusion**
*1. To make D25% dilute D50 % 1:1 with sterile water or normal saline. 2. To make D12.5% dilute D25% 1:1 with sterile water or normal saline. 3. To make D12.5% from D50% follow steps 1 & 2
Code 56PEDIATRIC RESPIRATORY ARREST
Not BreathingBreathing resumed
Chest Rise Adequate

• Ass
ess
AB
Cs
• Sec
ure
airw
ay a
s ap
prop
riate
• Adm
inis
ter
100%
OX
YG
EN
• Com
plet
e in
itial
ass
essm
ent
• Car
diac
mon
itor
• Sup
ine
posi
tion
Co
de
57
PE
DIA
TR
IC S
HO
CK
DE
TE
RM
INE
ET
IOL
OG
Y O
F S
HO
CK
HY
PO
VO
LE
MIC
SH
OC
K(S
usp
ect
ed d
ehy
dra
tion
/vo
lum
e lo
ss/
he
mo
rrha
gic
sho
ck)
• Est
ab
lish
va
scu
lar
acc
ess
IV
/IO
NS
@ T
KO
• Adm
inis
ter
flu
id b
olu
s 2
0m
l/kg
• If
no
resp
onse
to
initi
al f
luid
bol
us,
re
pea
t a
t 2
0m
l/kg
as
ind
ica
ted
to
ma
xim
um
of
60m
l/kg
.
• Sup
port
AB
Cs
• Pul
se o
xim
etry
• Obs
erve
• Kee
p w
arm
• TR
AN
SP
OR
T
DIS
TR
IBU
TIV
E S
HO
CK
(S
usp
ect
ed s
ep
sis/
an
aph
yla
xis)
• Est
ab
lish
va
scu
lar
acc
ess
IV
/IO
NS
@ T
KO
• Adm
inis
ter
flu
id b
olu
s 2
0m
l/kg
• If
susp
ect
ed a
llerg
ic r
eac
tion
, re
fer
to P
ED
IAT
RIC
A
LL
ER
GIC
RE
AC
TIO
N/A
NA
PH
YL
AX
IS C
OD
E 5
8 I
f n
o re
spon
se t
o in
itia
l flu
id b
olu
s a
nd
his
tory
of
feve
r/in
fect
ion,
re
pea
t flu
id b
olu
ses
of 2
0m
l/kg
as
ind
ica
ted
to
a m
axi
mu
m
of
60m
l/kg
.
CA
RD
IOG
EN
IC S
HO
CK
(His
tory
con
ge
nita
l he
art
dis
eas
e/c
ard
iac
su
rge
ry/r
hyth
m d
istu
rba
nce
/po
st-c
ard
iac
arr
est
)• E
sta
blis
h v
asc
ula
r a
cce
ss I
V/I
O N
S @
TK
O• I
de
ntify
any
ca
rdia
c rh
yth
m d
istu
rban
ce a
nd r
efe
r to
ap
pro
pria
te D
YS
RH
YT
HM
IA C
OD
E• P
er m
edic
al c
ontr
ol,
con
sid
er f
luid
bo
lus
and
/or
DO
PA
MIN
E*
pe
r le
ng
th b
ase
d P
edi
atr
ic T
ap
e o
r C
hart
.
NO
TE
TO
PR
EH
OS
PIT
AL
PR
OV
IDE
RS
:• C
auti
on
- F
luid
s m
ay n
eed
to b
e re
stric
ted
in C
ardi
ogen
ic S
hock
.*D
OP
AM
INE
mus
t be
adm
inis
tere
d pe
r m
ini d
rip tu
bing
.
Eff
ectiv
e
01
/01/
12IL
S

Co
de
62P
ED
IAT
RIC
HE
AT
EM
ER
GE
NC
IES
• Pro
foun
d w
eakn
ess
and
fatig
ue• V
omiti
ng, d
iarr
hea
• Hyp
oper
fusi
on• M
uscl
e cr
amps
• Ass
ess
AB
Cs
• Adm
inis
ter
100%
OX
YG
EN
• Com
plet
e in
itial
ass
essm
ent.
Ass
ess
for:
• Hot
, dry
, flu
shed
or
ashe
n sk
in• T
achy
card
ia• T
achy
pnea
• Dia
phor
esis
• Dec
reas
ing
cons
ciou
snes
s• A
sses
s sc
ene
for
envi
ronm
enta
l ris
ks• P
lace
in a
coo
l env
ironm
ent
• Rem
ove
clot
hing
as
appr
opria
te• C
ardi
ac M
onito
r
No
rmal
Lev
el o
f C
on
scio
usn
ess
&
Dia
ph
ore
sis
Dec
reas
ed C
on
scio
usn
ess,
D
ry S
kin
Ade
qu
ate
Re
spir
ato
ry
E
ffort
Ina
deq
ua
te
Res
pir
ato
ry
E
ffort
Sys
tolic
BP
> 1
00H
ypo
per
fusi
on
*o
r P
rese
nce
of
Nau
sea/
Vo
mit
ing
• Giv
e c
oo
l liq
uid
s P
O• P
er M
edic
al C
on
tro
l, c
ons
ide
r va
scu
lar
acc
ess
IV N
S @
TK
O
• Sup
po
rt A
BC
s• O
bse
rve
• TR
AN
SP
OR
T
**N
OT
E T
O P
RE
HO
SP
ITA
L P
RO
VID
ER
S:
Co
oli
ng
Te
ch
niq
ue
s• A
pply
co
ol p
ack
to h
ea
d, n
eck
, arm
pits
, g
roin
, b
ehi
nd
kn
ees
an
d to
late
ral c
hest
.• T
epi
d w
ate
r p
er s
po
nge
/sp
ray
• Ma
nu
ally
fa
n b
ody
to e
vap
ora
te a
nd c
oo
l• S
top
co
oli
ng
if
sh
ive
rin
g o
ccu
rs.
*Ref
er t
o P
ED
IAT
RIC
AS
SE
SS
ME
NT
AN
D T
RA
UM
A S
CO
RE
CO
DE
28
• Sec
ure
air
wa
y a
s a
ppr
op
riat
e• S
upp
ort
ve
ntil
atio
n
with
BV
M
• Est
ab
lish
va
scu
lar
acc
ess
IV
/IO
NS
@ T
KO
• Flu
id b
olu
s w
ith 2
0m
l/kg
• Rep
ea
t if
no
imp
rove
me
nt t
o m
axi
mu
m
of
60m
l/kg
**In
itiat
e c
ool
ing
• Ref
er
to P
ED
IAT
RIC
SE
IZU
RE
S C
OD
E 5
9 a
s n
ee
ded
Eff
ectiv
e
01
/01/
12IL
S

Maintain situational awareness and scene safety. Introduce yourself to the patient, and attempt to gain their confidence in a non-threatening manner. If the patient refuses assistance, attempt to determine their mental status. This includes determining their orientation and the presence of anything that could produce an altered mental status, such as drug/alcohol intoxication or withdrawal, trauma (head injury), hypoxia, hypotension, hypoglycemia, stroke, infections, psychological emergencies (i.e. homicidal, suicidal, psychosis, etc.) or dementia (i.e. acute or chronic organic brain syndromes).
If the mental status is judged to be abnormal, prehospital personnel must carry out treatment andtransport in the patient’s best interest.
In any form of intervention, prehospital personnel must ALWAYS CONSIDER THEIR OWN SAFETY FIRST!
1. Again attempt to verbally reassure the patient and seek their willing cooperation.2. If it is necessary to physically restrain a patient, perform all the following: A. Prepare all the necessary equipment. B. Use police and /or fire personnel if needed. If available, have one person assigned to each extremity and one to hold equipment. C. Apply the restraints as loosely as possible to maintain a safe situation, but prevent neurovascular compromise and undue patient discomfort. Apply restraints over clothing when possible. D. Never place restraints over a patient's chest or on the abdomen of a pregnant patient. E. Perform routine and specific medical care as indicated by the patient’s condition. Routinely document the neurovascular status of the patient’s extremities distal to the restraints. F. Notify the receiving hospital of the situation, and request security assistance upon arrival. G. Continue to attempt to verbally reassure the patient and seek their cooperation. Inform the patient’s family of the reasons for the use of restraints. H. Thoroughly document the situation including the reasons for using restraints and how they were applied. I. At no time will towels, washcloths or other devices be placed over the mouth and/or nose of a restrained patient for any reason. J. Never restrain a patient in the prone position. K. For reasons of medical safety, any patient who is under police hold and requires handcuffs, must have a police officer accompany the patient in the back of the ambulance while enroute to the hospital or provide the transporting EMS personnel with keys to the handcuffs.
Code 68
RESTRAINTS AND BEHAVIORAL EMERGENCIES
No
Revised 01/01/12Effective 05/01/98ILS
NOTE TO PREHOSPITAL PROVIDERS: Once restrained, continue to be conscious of the patient’s airway and other medical needs.

PEDIATRIC MANUALINTRAOSSEOUS NEEDLE INSERTION
• Equipment– IV fluid and tubing – Intraosseous needle– Cleansing prep– Tape, 4x4 gauze– 10ml syringe– Sterile gloves– 60ml syringe
• Procedure– Prepare equipment.– Identify landmarks: anteromedial aspect of the proximal tibia, 1-3cm below the tibial
tuberosity. (Distal femur or distal tibia may also be used.)– Prep the site with cleansing prep– Using a twisting motion, introduce the needle at a 90-degree angle, directing away from
the knee. There will be a “pop” as the needle enters the marrow. – Remove the stylet (discard in sharps box) and aspirate with a 10ml syringe to confirm
needle placement.– Remove the syringe, attach IV fluids to be given. Flush with 5ml of Normal Saline.– Secure the needle.– Bolus fluid by hand, using 60ml syringe.
Code 73
Effective 01/01/12ILS
Page 1 of 3

Indications:
• See appropriate SMOs
Contraindications:
• Infection at the site selected for insertion (choose alternate site)
• Fracture of the bone selected for IO infusion (choose alternate site)
• Excessive tissue preventing identification of landmarks (choose alternate site)
• Previous significant orthopedic procedures, such as a prosthesis (choose alternate site)
• Previous IO insertion attempt to this site within the last 24 hours (choose alternate site)
“Power driver” Insertion Steps:1. BSI.2. Aseptic technique.3. Locate insertion site (Approved sites: proximal tibia or proximal humerous).4. Prepare insertion site.5. Prepare infusion system.6. Ensure that the driver and needle set are securely seated.7. Remove and discard the needle set safety cap from the IO needle set installed on the power driver.8. Insert.
Important: Do not touch the needle set with your hand or fingers.Important: Control the patient's movement prior to and during the needle set insertion.
a. Position driver at insertion site with the needle set at a 90-degree angle to the bone. Gently power or press needle set until needle set tip touches bone.b. Ensure at least 5 mm of the catheter is visible.c. Penetrate bone cortex by squeezing the driver’s trigger and applying gentle, steady
downward pressure.d. Release driver’s trigger and stop insertion process when:
1. A sudden “give” or “pop” is felt upon entry into the medullary space. 2. A desired depth is obtained.
Important: Use gentle-steady pressure. Do not use excessive force. Allow the catheter tip rotation and gentle downward pressure to provide the
penetrating action. Note: If the driver stalls and will not penetrate the bone you may be applying too much downward pressure.
Code 73
OTHER INTRAOSSEOUS NEEDLE INSERTION
Page 2 of 3
Effective 01/01/12ILS

“Power driver” Insertion Steps continued:
• Remove power driver and stylet.• Confirm catheter stability.• Attach primed extension set to catheter hub’s luer lock.
Do not attach a syringe directly to the catheter hub.12. Flush the adult catheter with 10ml of Normal Saline. Flush the pediatric catheter
with 5ml of Normal Saline.Important: Prior to flush consider the aspiration of a small amount
of blood to confirm placement.
* No Flush = No Flow Failure to appropriately flush the IO catheter may result in limited or no flow.
* Once IO catheter has been flushed, administer fluids or medications as indicated.Note: Frequently monitor the insertion site for extravasation.
Code 73
Page 3 of 3
OTHER INTRAOSSEOUS NEEDLE INSERTION
Effective 01/01/12ILS

Code 76
CONTINUOUS POSITIVE AIRWAY PRESSURE ADMINISTRATION
• Observe body substance isolation at all times• Oxygenate the patient with 15 liters via non-rebreather mask while setting up CPAP• Connect fixed generator to portable oxygen regulator• Open CPAP disposable package and attach patient corrugated tubing to bottom of generator and add filter to side of generator• Attach other end of patient tubing to bottom of mask• Attach 10cm isobaric peep valve to front of mask• Connect head strap to top of one side of mask• Turn oxygen tank on• Encourage patient to place mask over mouth and nose, then firmly attach mask using final connection on side of mask• When patient has been placed in the ambulance, “quick connect” generator to on-board oxygen• Monitor patient’s level of consciousness and vital signs continuously. If patient develops decreased mental status or decreased blood pressure-DISCONTINUE CPAP.• Continuous cardiac monitoring and pulse oximetry required
Note: If aerosol medication treatment is indicated, cut the patient’s corrugated tubing atfirst smooth part closest to the patient’s face. Place a “t” connector between the tubing and follow ALBUTEROL administration protocol.
If port is available for Albuterol administration, follow manufacturers guidelines.
Effective 01/01/12ILS

INTRANASAL ADMINISTRATION
Code 85
Effective: 01/01/12ILS
• Observe body substance isolation at all times• Assess ABC’s and support ventilation as needed• Inspect medication
- Identify concentration- Inspect for contamination- Check expiration date
• For suspected Opiate overdose,• Remove the medication atomization device (MAD) tip from the syringe • Draw up NALOXONE (Narcan) 2ml (1mg/ml) and replace the MAD Intransasal
Atomizer tip (OR place the MAD tip on a luer-lock prefilled syringe)• Tilt the patients head back, if possible• Place atomizer in the nare opening and advance it until the cone tip is sealed against
the opening.• Depress the plunger and administer 1ml briskly in each nostril• Remove the device• Monitor the patient for desirable and undesirable effects• Continue to support respirations as needed
Important note: If a patient fails to awaken after intranasal Narcan, they may still respond to intravenous administration.
• For hypoglycemia (blood sugar < 60) and altered level of consciousness when an IV is not able to be established,
• Reconstitute GLUCAGON 1mg in 1ml sterile water• Remove the medication atomization device (MAD) tip from the syringe• Draw up the reconstitued GLUCAGON (1mg/ml) and replace the MAD Intranasal
Atomizer to syringe• Tilt the patient’s head back, if possible• Place atomizer in the nare opening and advance it until the cone tip is sealed against
the opening.• Depress the plunger and administer 0.5 ml briskly in each nostril• Remove the device• Continue to monitor closely for desirable and undesirable effects