recommendations for human blood pressure · pdf filerecommendations for human blood pressure...
TRANSCRIPT

Online ISSN: 1524-4539 Copyright © 1967 American Heart Association. All rights reserved. Print ISSN: 0009-7322.
Dallas, TX 72514Circulation is published by the American Heart Association. 7272 Greenville Avenue,
1967;36;980-988 CirculationEPSTEIN and EDWARD D. FREIS
WALTER M. KIRKENDALL, ALAN C. BURTON, FREDERICK H. Sphygmomanometers
Recommendations for Human Blood Pressure Determination by
http://circ.ahajournals.org/cgi/reprint/circulationaha;37/4/488page or:
An erratum has been published regarding this article. Please see the attached
http://circ.ahajournals.orgservices, is located on the World Wide Web at:
The online version of this article, along with updated information and
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected]. Fax: 410-528-8550. E-mail: Wolters Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of
http://circ.ahajournals.org/subscriptions/Subscriptions: Information about subscribing to Circulation is online at
by on November 16, 2009 circ.ahajournals.orgDownloaded from

REPORT OF A SUBCOMMITTEE OF THEPOSTGRADUATE EDUCATION COMMITTEE,
AMERICAN HEART ASSOCIATION
Recommendations for Human Blood PressureDetermination by Sphygmomanometers
By Subcommittee Members: WALTER M. KIRKENDALL, M.D., CHAIRMAN,ALAN C. BURTON, PH.D., FREDERICK H. EPSTEIN, M.D., AND
EDWARD D. FREIS, M.D.
SYSTEMIC arterial blood pressure* repre-sents a force which is the result of
cardiac output and peripheral vascular re-sistance. It is readily measured indirectly bya standard sphygmomanometer. Comparedwith intra-arterial measurements of blood pres-sure, the indirect method is imprecise. Never-theless, it is known that properly measuredindirect blood pressure readings in the upperranges and wide swings of blood pressure inthe same individual are important signs ofvascular disease. This booklet will point outcommon errors in the indirect measurementof blood pressure, indicate the means to avoidthem, and recommend certain standards toincrease the accuracy of measurement andrecording. The booklet, represents the secondrevision of the standards first proposed in1939.'1, 2
Equipment for Indirect Measurement ofBlood Pressure
A sphygmomanometer consists of a com-pression bag enclosed in an unyielding cuff,an inflating bulb, pump, or other device bywhich the pressure is increased, a manometerfrom which the applied pressure is read, anda controlled exhaust to deflate the system.
*Hereafter referred to as blood pressure.
980
A stethoscope is the other instrument neces-sary for indirect measurement of pressure.SphygmomanometerBag and CugThe inflatable bag is surrounded by an
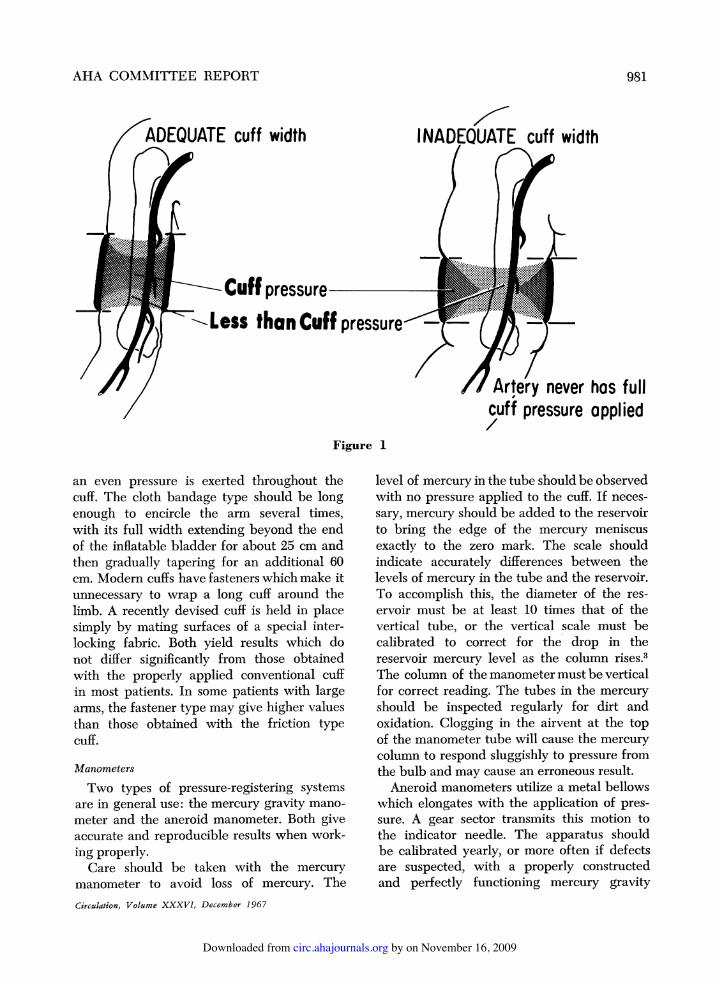
unyielding covering called "the cuff." The bagmust be the correct width for the diameterof the patient's arm; for if it is too narrow,the blood pressure reading will be erroneouslyhigh; if it is too wide, the reading may beerroneously low (fig. 1). The inflatable bagshould be 20% wider than the diameter of thelimb on which it is to be used. For the averageadult, a bag 12 to 14 cm wide has beenfound to be satisfactory. Smaller cuffs areavailable for patients with small arms (seeSection on Blood Pressure Recording in Chil-dren), as are larger (18 to 20 cm) ones formeasurement in obese persons or in the thigh.The diameter of the arm is the factor whichdetermines whether a "children's cuff" or"adult cuff" is used, not the age of the patient.The inflatable bag should be long enough
to go halfway around the limb if care istaken to put the bag directly over the com-pressible artery. A bag, 30 cm in length, thatnearly (or completely) encircles the limbobviates any risk of misapplication.The cuff should be made of a nondis-
tensible material, so that as far as possibleCirculation, Volume XXXVI, December 1967
by on November 16, 2009 circ.ahajournals.orgDownloaded from
AHA COMMITTEE REPORT
ADEQUATE cuff width
Cuff pressureq-loss than Cuff pressure--
I NADEQUATE cuff width
2 lr
Artery never has fullcuff pressure applied
Figure 1
an even pressure is exerted throughout thecuff. The cloth bandage type should be longenough to encircle the arm several times,with its full width extending beyond the endof the inflatable bladder for about 25 cm andthen gradually tapering for an additional 60cm. Modern cuffs have fasteners which make itunnecessary to wrap a long cuff around thelimb. A recently devised cuff is held in placesimply by mating surfaces of a special inter-locking fabric. Both yield results which donot differ significantly from those obtainedwith the properly applied conventional cuffin most patients. In some patients with largearms, the fastener type may give higher valuesthan those obtained with the friction typecuff.
Manometers
Two types of pressure-registering systemsare in general use: the mercury gravity mano-meter and the aneroid manometer. Both giveaccurate and reproducible results when work-ing properly.Care should be taken with the mercury
manometer to avoid loss of mercury. TheCirculation, Volume XXXVI, December 1967
level of mercury in the tube should be observedwith no pressure applied to the cuff. If neces-sary, mercury should be added to the reservoirto bring the edge of the mercury meniscusexactly to the zero mark. The scale shouldindicate accurately differences between thelevels of mercury in the tube and the reservoir.To accomplish this, the diameter of the res-ervoir must be at least 10 times that of thevertical tube, or the vertical scale must becalibrated to correct for the drop in thereservoir mercury level as the column rises.3The column of themanometermustbeverticalfor correct reading. The tubes in the mercuryshould be inspected regularly for dirt andoxidation. Clogging in the airvent at the topof the manometer tube will cause the mercurycolumn to respond sluggishly to pressure fromthe bulb and may cause an erroneous result.Aneroid manometers utilize a metal bellows
which elongates with the application of pres-sure. A gear sector transmits this motion tothe indicator needle. The apparatus shouldbe calibrated yearly, or more often if defectsare suspected, with a properly constructedand perfectly functioning mercury gravity
981
by on November 16, 2009 circ.ahajournals.orgDownloaded from

AHA COMMITTEE REPORT
manometer. This examination should be madeat several points over the entire pressurerange, since no single correlation of figuresguarantees accuracy over the whole range.Such calibration can be made by interposinga Y connector in the tube from the cuff toa mercury manometer and attaching thesphygmomanometer to be tested to the freeend of the connector.
Inflating System, Exhaust Valve, and TubingThese should be checked frequently for
significant leaks in pressure (i.e., more than1 mm Hg/sec) and for competent, smoothfunctioning of the input system and of thebulb exhaust valves. One should be able toinflate the system gradually or rapidly.StethoscopeThe stethoscope should be of a standard
variety and in good condition.
Determination of Blood PressureThe ObserverThe observer should be trained in taking
the blood pressure. He should be able tohear well enough to recognize the faintersounds and to see well enough to read themanometer. When observing the pressure, hiseyes should be level with the meniscus of themercury column. The observer should avoidbeing in a strained position at the time thepressure is recorded.A single casual blood pressure reading does
not characterize the person's blood pressureaccurately. Several blood pressure readingsby independent observers, or on differentoccasions by the same observer when he isaware, or preferably unaware, of his previousreadings, are a better index.The PatientThe patient should be comfortably seated,
with the arm slightly flexed and with thewhole forearm supported at heart level on asmooth surface. Readings taken in any otherposition should be specified. There are prob-ably no great differences in blood pressuresrecorded in the supine, sitting, and standingpositions in normal persons with the arm held
at heart level. However, in certain personsthere is a striking difference in blood pressuresin different positions, and if the patient is insome position besides sitting, this should benoted. When other positions are used, theyshould be specified with the following ab-breviations: L (lying) or St. (standing),R.A. (right arm), L.A. (left arm), i.e., R.A.148/78/70, St.; L.A. 148/76/72, L.One attempts to obtain a reading which is
representative of the patient's blood pressureunder ordinary circumstances. Therefore, bi-ological factors which alter blood pressureshould be recognized and noted. Anxiety, emo-tional turmoil, meals, tobacco, bladder disten-tion, climate variation, exertion, and pain, allmay influence blood pressure. When possible,all such stimuli should be controlled oravoided. When this is not possible, extraneousinfluences should be listed.
Suggested standard conditions for indirectmeasurement of the blood pressure are thatthe patient be in a quiet room at a comfort-able temperature, with his arm unconstrictedby clothing or other material. He shouldavoid exertion, exposure to cold, and eatingor smoking for a half hour before the measure-ment; there should be no postural change for5 minutes before recording.
TechniqueOn the initial examination it is usually best
to record the pressure in both arms, usingabbreviations, i.e., R.A. 140/82/74; L.A. 152/86/74. In subsequent examinations the armfound to have the higher pressure initiallyshould be used.Under the environmental conditions already
noted, the deflated cuff should be applied withthe lower margin about 232 cm above the ante-cubital space, with the rubber bag over theinner aspect of the arm. A preliminary palpa-tory determination of systolic pressure givesthe examiner an estimate of the maximalpressure to which the system needs to be ele-vated in subsequent determinations.The stethoscope should be applied to the
antecubital space over the previously pal-pated brachial artery. The stethoscope head
Circulation, Volume XXXVI, December 1967
982
by on November 16, 2009 circ.ahajournals.orgDownloaded from

AHA COMMITTEE REPORT
should be applied firmly, but with as littlepressure as possible, and with no space be-tween the skin and the stethoscope. Heavypressure will distort the artery and producesounds heard below the diastolic pressure.The stethoscope should not touch clothingor the pressure cuff.With the stethoscope in place, the pressure
is raised approximately 30 mm Hg above thepoint at which the radial pulse disappearsand then released at a rate of 2 to 3 mm Hg/sec. Faster or slower deflation will causesystematic errors.As the pressure falls, the Korotkoff sounds
become audible over the artery below the cuffand pass through four phases as the pressuredeclines and sounds disappear:Phase I: The period marked by the first ap-
pearance of faint, clear tapping soundswhich gradually increase in intensity.
Phase II: The period during which a murmuror swishing quality is heard.
Phase III: The period during which soundsare crisper and increase in intensity.
Phase IV: The period marked by the distinct,abrupt muffling of sound so that a soft,blowing quality is heard.
Phase V: The point at which sounds dis-appear.The muffling and disappearance are com-
monly referred to as the "fourth and fifthpoints."
Sometimes, particularly in some hyperten-sive patients, the usual sounds heard over thebrachial artery, when the cuff pressure is high,disappear as the pressure is reduced and thenreappear at a lower level. This early, tem-porary disappearance of sound is called theauscultatory gap and occurs during the lat-ter part of phase I and phase II. Becausethis gap may cover a range of 40 mm Hg, onecan seriously underestimate the systolic pres-sure or overestimate the diastolic, unless itspresence is excluded by first palpating fordisappearance of the radial pulse as the cuffpressure is raised.When all sounds have disappeared, the
cuff should be deflated rapidly and com-pletely. One to two minutes should elapseCirculation, Volume XXXVI, December 1967
for the release of blood trapped in the veinsbefore further determinations are made.
Systolic Pressure Determination
The systolic pressure is the point at whichthe initial tapping sound is heard for at leasttwo consecutive beats. When the palpatorysystolic pressure is higher, it should be re-corded and noted as systolic pressure.
Diastolic Pressure Determination
Muffling occurs when the crisp Korotkoffsounds change and represents sudden dim-inution or disappearance of sound energy atfrequencies greater than 60 cycles/sec. Theonset of muffling is the fourth phase andshould be regarded as the best index of di-astolic pressure. Numerous studies indicatethat muffling occurs at pressures 7 to 10 mmHg higher than direct intra-arterial diastolicpressures.The fifth phase occurs when sounds become
inaudible. This usually occurs with cuff pres-sure near intra-arterial diastolic pressure butmay fall far below under conditions mentionedin the "Appendix." The accuracy of deter-mining the fifth phase depends on the effi-ciency of the stethoscope and the auditoryacuity of the observer. If there is a differencebetween the fourth and fifth phases, as fre-quently happens, both pressures should berecorded as follows: 142/82/78 (82=4thphase, 78=5th). If the two levels are iden-tical, this should be recorded as 144/76/76.Effect of Arm Position on Blood PressureMeasurementThe effect on indirect auscultatory blood
pressure of random vertical arm displacementaround heart level is a consistent increase inpressure as the arm is lowered. The effectis largely explained by the hydrostatic pres-sure. This is the reason why standard po-sitioning of the forearm at the horizontallevel of the fourth intercostal space at thesternum is recommended for blood pressuremeasurement in the sitting and upright po-sitions. When the patient is supine on a flatsurface, the arm is near enough to heart levelso that no adjustment is necessary.
983
by on November 16, 2009 circ.ahajournals.orgDownloaded from

AHA COMMITTEE REPORT
Disregard of this factor can cause a syste-matic error in blood pressure readings of asmuch as 10 mm Hg in both systolic anddiastolic pressures.4 If the arm is not at thestandard level during a blood pressure de-termination, a correction for the hydrostaticpressure must be made. For each centimeterof vertical height above or below the heartlevel, 0.7 mm Hg must be substracted oradded, respectively, to the pressures observed.The aneroid manometer may be at any height;the mercury manometer should be level withthe observer's eyes.
Blood Pressure in ThighBlood pressure in the thigh is measured
by use of an 18- to 20-cm bag (6 cm widerthan the arm bag) and an appropriatelylarger cuff. Although there is no consensusabout the exact cuff size for thighs of differentdiameters and shapes, it is important that thecuff be both wider and longer than that forthe arm to allow for the greater girth. Thepatient lies on his abdomen, and the cuff isapplied with the compression bag over theposterior aspect of the midthigh. The stetho-scope is placed over the artery in the poplitealfossa, and the Korotkoff sounds are heard asthe cuff pressure is diminished in the samemanner as it is in the arms. If the patient isunable to lie on his abdomen, the thighpressure may be obtained with the patientsupine by flexing the knee just enough topermit application of the stethoscope overthe popliteal space. The 18- to 20-cm cuffusually records systolic pressure in the thighsas higher (by 10 to 40 mm Hg) than that inthe arms, but the diastolic pressure is essen-tially the same. Comparison of intra-arterialblood pressures in the arms and legs in hu-mans shows that the femoral systolic pressureis only a few millimeters of mercury higher,and the diastolic a few millimeters lower, thancomparable arm pressures are.5
Basal Blood PressureThe basal blood pressure is the level ob-
tained when physical, metabolic, mental, andemotional stimuli which elevate blood pres-
sure have been eliminated.6 Since, under theconditions in which blood pressure usuallyis measured, all such influences are not elim-inated, the termn "basal" blood pressure isused to denote a level approximating thebasal state.The basal blood pressure is approximated
after several days of rest in the hospital whenthe patient has become acclimated to thehospital situation and to the procedure ofhaving his blood pressure taken repeatedly.Even in this environment, blood pressuresrecorded by the nurse tend to be lower thanthose taken by the doctor because of theemotional response generated by the presenceof the physician.Nearly basal blood pressures also can be
taken in the home preferably by a memberof the family.7 Daily recordings taken in thehome usually trend downward during thefirst week to a lower, more constant level. Ifit is necessary for the patient to record hisown blood pressure, it is best to use a cuffin which the stethoscope head is incorporated,although slight inaccuracies may be intro-duced by this placement. The patient shouldbe instructed to pump up the cuff with thebulb in the contralateral hand to avoid exer-cising the forearm muscles of the cuffedextremity. Instruments of special design areavailable which permit correct application ofthe cuff and stethoscope head by the patienton his own arm.
Blood Pressure Recording in SpecialConditions
ArrhythmiasIf the cardiac rhythm is very irregular, the
determination of blood pressure is inaccuratebecause both stroke volume and blood pres-sure vary from one cardiac cycle to the next.The systolic blood pressure is related directlyto the duration of the preceding pulse cycleand the stroke volume, whereas the pulsepressure is related inversely to the durationof the pulse cycle. A long pulse cycle resultsin a decrease in the diastolic pressure of thatcycle and an increase in systolic pressure ofthe next one.
Circulation, Volume XXXVI, December 1967
984
by on November 16, 2009 circ.ahajournals.orgDownloaded from

AHA COMMITTEE REPORT
An occasional premature contraction can beignored. When of frequent occurrence or inatrial fibrillation, both diastolic and systolicreadings should be recorded as only approxi-mate. For patients with atrial fibrillation, oneshould record the average of a series ofreadings for the appearance of the first soundas the systolic pressure and similar averages forthe fourth and fifth phases as the diastolicpressure. The diagnosis, if not stated else-where on the patients chart, should be notedwith the blood pressure recording.
Clinical ShockBrachial arterial pulsations and Korotkoff
sounds may be greatly diminished or absentin clinical shock. Comparisons between aus-cultatory pressures in the arm and direct arter-ial readings taken with a needle inserted intothe femoral artery frequently reveal that thedirect femoral pressure is considerably higherthan the pressure recorded in the arm bythe auscultatory method.8 Diminution or dis-appearance of Korotkoff sounds is most apt tobe found in shock states associated withgreatly reduced cardiac output and elevatedtotal peripheral resistance as occurs in cen-tral blood volume depletion. Because of highvascular resistance in the forearm, bloodflow in the upper extremities falls to such lowlevels that Korotkoff sounds are not gen-erated. Under these circumstances the indi-rect auscultatory method may be grosslyinaccurate, so that a direct method of bloodpressure recording is needed to follow thesecritically ill patients.
Determination of Blood Pressure in Infantsand Children
Blood pressure can be determined by theauscultatory method as accurately in infantsand children as in adults, providing attentionis paid to the apprehensiveness and activityof the patient and to the principles discussedon page 982. The chief source of error arisesfrom the selection of a poorly supported orinappropriately sized cuff. A general rule forcuff size is that it cover two thirds of the armabove the elbow. In addition to the standardCirculation, Volume XXXVI, December 1967
cuff, cuffs of 2.5, 5, 8, and 12 cm in widthshould be available. In children the muffling,not the complete cessation, of vascular soundis the best index of diastolic pressure.9' 10The patient should be in the supine or re-
clining posture so that the arm can be main-tained in a comfortable position. For infantsa bottle or pacifier may be offered to keepthem quiet. The technique for children isotherwise identical to that for adults. Thepatient who is apprehensive, excited, or hasexercised recently may have an elevated pres-sure. Crying in an infant may raise his systolicblood pressure as much as 30 to 50 mm Hg.If the auscultatory method so disturbs thepatient that accurate reflection of the restingblood pressure cannot be obtained, it maybe necessary to leave the cuff on the arm andmake the determination when the patient isasleep or sedated, or to determine the systolicpressure by palpation.
In infants under 1 year of age the ausculta-tory sounds may occasionally be too faint tobe heard; consequently, other indirect methodsare used. The most common is the flush meth-od,1' but oscillometry12 or instrumental mea-surement of pulsation distal to the cuff13 is sen-sitive and sufficiently easy to use to beregarded as the method of choice by certainauthors.To measure blood pressure by the flush
method, a suitable cuff is placed on the fore-arm or calf, the extremity is elevated, andthat portion distal to the cuff is compressedby wrapping it firmly with an elastic bandage.When compression is complete, the extremityis lowered to heart level and the cuff israpidly inflated to 200 mm Hg. The bandageis removed, and the manometer pressure isgradually lowered at a rate not exceeding 5mm Hg/sec. The end point of the determina-tion is the appearance of a flush in the ex-tremity distal to the cuff. The measurementshould be made in a well-lighted room, andaccuracy is increased if two observers arepresent so that the pressure at which flushingoccurs can be noted promptly. If the deter-mination is done by a single observer, themanometer should be placed so that it and
985
by on November 16, 2009 circ.ahajournals.orgDownloaded from

AHA COMMITTEE REPORT
the extremity can be observed simultaneously.The pressure thus obtained most nearly reflectsthe mean, not the systolic, blood pressure.14
Epidemiological MethodsInferences from the findings of epidemio-
logical studies are largely based on com-parisons between different population seg-ments. The studies compared are spread overdifferent places and countries and involverecordings by many different groups and ob-servers. How can one be sure that differencesin findings are not due to variations intechnique and various sources of observerbias?'5' 16
All measurements, including blood pressure,are subject to two sources of uncertainty:biological variation and measurement error.As a result, single casual blood pressure re-cordings may be inadequate to characterizean individual with sufficient accuracy.7' 18
Biological variation in the patient has beendiscussed on page 982. The possible effects ofseason, temperature, altitude, diurnal varia-tions, fluctuations from basal level, and otherphysical factors must be taken into accountand should be controlled in the design ofstudies and the analysis of data.Measurement ErrorsThese errors relate to the instrument, the
observer, the observed, and their interactions.
InstrumentIn epidemiological, as in clinical situations,
faithful recording is essential.19 (Specifica-tions have been discussed on page 980). Thereis further need to develop devices for theautomatic recording of blood pressure duringsurvey examinations, or portable instrumentsfor continuous monitoring under the conditionsof "daily living." Such instruments greatly re-duce observer error and variation.Observer ErrorAn observer may record the blood pressure
inaccurately because of sensory impairment,inattention, carelessness, or subconscious bias.An example of such bias is "digit preference,"a well-documented phenomenon resulting in
recording pressures ending with zero (e.g.,140 systolic or 90 diastolic) more often thanexpected by chance. Another bias relates tothe physician's preconceived notion of anormal pressure; if he knows that a diastolicpressure above 95 mm Hg will be classified as"hypertensive," he may be more likely to re-cord "96" in a heavy, middle-aged man but"94" in a thin teen-ager. An observer maybe influenced also by knowledge of earlierreadings. The London School of Hygienemachine developed by Rose and associates"'and the Zero-Muddler,20 while not automaticblood pressure recorders, are instrumentswhich overcome observer bias, but not theother errors mentioned. A further advance con-cerns the training of observers in hearingthe right sounds at the proper time by theuse of phonographic records and tapes.21 22The ObservedThe position of the subject and the con-
dition under which the measurement is takenare discussed on page 982.
Clinical ImplicationsIf the aim were merely to establish whether
a person's pressure is in the normal range ornot, the measurement errors discussed abovewould be of limited consequence. However,many clinical situations call for valid serialobservations, e.g., among patients on anti-hypertensive therapy. Moreover, many clinicaldata are also often used for research pur-poses. The avoidance of errors in blood pres-sure readings is as important as the need foraccurate diagnosis of a murmur or for ac-curacy in a clinical chemistry laboratory.Sphygmomanometry leaves much to be de-sired, and biological variation in the sameperson further complicates the picture. Thisis all the more reason to eliminate all avoid-able errors in measurement.
APPENDIXNote Regarding Criteria for Diastolic
PressureIt is important to emphasize that both the
fourth and fifth phases should be recordedwhen listing the blood pressure. Nevertheless,
Circulation, Volume XXXVI, December 1967
986
by on November 16, 2009 circ.ahajournals.orgDownloaded from

AHA COMMITTEE REPORT
the adoption of the fourth phase, or muffling,as the best index of diastolic pressure is achange from the recommendation of the com-mittee which edited "Recommendations forHuman Blood Pressure Determination bySphygmomanometers" for the American HeartAssociation in 1951.2 That committee reversedthe recommendations for the determinationof diastolic pressure in the 1939 publication.1"Standardization of Blood Pressure Readings,"a joint recommendation of the American HeartAssociation and the Cardiac Society of GreatBritain and Ireland.' The World Health Or-ganization recommends recording both fourthand fifth phases.The present recommendations stem from
the following reasoning. Since streamline flowis silent, the presence of sound in the circu-lation depends on such critical conditions asvelocity of flow, diameter of channels, anddisturbed flow, including turbulence and vor-tices. As the cuff pressure falls, the narrowingof the artery and hence, the pressure gradientacross the compressed segment, become less,so that the velocity of flow diminishes andthe conditions necessary for sound productionno longer exist. When cuff pressure exceedsdiastolic pressure, tissue pressure under thecuff closes the artery briefly at the end ofeach diastole. The artery again is open duringthe subsequent upstroke of the pressure pulse,at which time the "staccato" sounds are gen-erated. When the compressed segment is nolonger completely closed in diastole, the phys-ical conditions necessary to produce vibra-tions of high frequency no longer exist. Thischange in frequency content is the mufflingand occurs when the artery is no longersufficiently collapsed by the cuff pressure.
Thus, even though intra-arterial diastolicblood pressure is approximately 10 mm Hglower than that found with muffling, the lawsof physics associate the point of mufflingwith diastolic pressure. There is no logicalconnection between the disappearance ofsound and diastolic pressure. Indeed, in nor-mal subjects, after vigorous exercise whenflow is increased and the opportunity forcreation of turbulence is greater, the fifth phaseCirculation, Volume XXXVI, December 1967
falls far below the diastolic pressure.The cuff pressure at which sound disap-
pears depends on the efficiency with whichthe sound is heard. This in turn depends onthe proximity of the stethoscope to the optimalposition over the artery, the efficiency of con-duction of sound waves by the stethoscope,and the sensitivity of the observer's hearing.On the other hand the muffling, or fourthphase, is a change in the quality of the sound,rather than its intensity, and so is lessaffected by the efficiency of detection.When flow within the arterial circulation
is increased, as it is after exercise in normalsubjects or in patients with hyperthyroidismand other high output states, the cuff pressureat which muffling and disappearance occurbecomes widely separated, for instance, byas much as 40 mm Hg after exercise. Themuffling, or fourth phase, remains approxi-mately correct for intra-arterial diastolic pres-sure. The fifth phase, or disappearance, fallsto values that are well below the diastolicpressure. Theory would predict that with in-creased velocity of disturbed flow the con-ditions for turbulence and sound will persistin an artery that is less compressed by thecuff pressure. Thus, we could expect to findsound to zero pressure in some instances. Itis of interest in this regard that muffling hasbeen found to be the more reliable index ofdiastolic pressure in children in whom thevelocity of flow is often high.9Recording the values for both phases, as
recommended, will make it possible (1) to re-late these figures to previous ones recordedwith the disappearance as the diastolic pres-sure and (2) to equate theme with values ob-tained elsewhere by observers who use onlymuffling as the diastolic pressure. The spreadbetween the muffling and disappearance ofsound also adds further physiological informa-tion as to the state of the vessels and the flowin them.
References1. JOINT RECOMMENDATIONS OF THE AMERICAN
HEART ASSOCIATION AND THE CARDIAC SO-CIETY OF GREAT BRITAIN AND IRELAND: Stan-dardization of blood pressure readings. New
987
by on November 16, 2009 circ.ahajournals.orgDownloaded from

AHA COMMITTEE REPORT
York, American Heart Association, Inc., July,1939.
2. COMMITTEE TO REVISE STANDARDIZATION OF HIGHBLOOD PRESSURE READINGS: Recommendationsfor human blood pressure determinations bysphygmomanometers. New York, AmericanHeart Association, October, 1951.
3. BURCH, G. E., AND DEPASQUALE, N. P.: Primerof Clinical Measurement of Blood Pressure.St. Louis, Missouri, C. V. Mosby Co., 1962.
4. MITCHELL, P. L., PARLIN, R. W., AND BLACK-BURN, H.: Effect of vertical displacement ofthe arm on indirect blood pressure measure-ment. New Eng J Med 271: 72, 1964.
5. PASCARELLI, E. F., AND BERTRAND, C. A.: Com-parison of blood pressures in the arms and legs.New Eng J Med 270: 693, 1964.
6. VEALE, A. M., HAMILTON, M., IRVINE, R. O.,AND SMIRK, F. H.: Population survey of casualand near-basal blood pressures: With commentson survey techniques. New Zeal Med J 61:65, 1962.
7. FREIS, E. D.: Home compared to hospital re-cordings of blood pressure as estimates of thebasal level. In The Pathogenesis of EssentialHypertension, 1960, Prague Symposium.Prague, States Medical Publishing House,1961, p. 111.
8. COHN, J. N., AND DADDARIO, R. C.: Mechanismof disappearance of Korotkoff sounds in clin-ical shock. Circulation 32 (suppl. II): II-69,1965.
9. Moss, A. J., AND ADAMS, F. H.: Index of in-direct estimation of diastolic blood pressure.Amer J Dis Child 106: 364, 1963.
10. Moss, A. J., AND ADAMS, F. H.: Problems ofBlood Pressure in Childhood. Springfield, Il-linois, Charles C Thomas, Publisher, 1962.
1 1. GOLDRING, D., AND WOHLTMANN, H.: Flushmethod for blood pressure determinations innewborn infants. J Pediat 40: 285, 1952.
12. KEITH, J. D., Row, R. D., AND VLAD, P.: HeartDisease in Infancy and Childhood. New York,Macmillan Co., 1958.
13. ASHWORTH, A. M., NELIGAN, G. A., AND ROGERS,J. E.: Sphygmomanometer for the newborn.Lancet 1: 801, 1959.
14. GUNTEROTH, W. G., AND NADAS, A. S.: Bloodpressure measurements in infants and chil-dren. Pediat Clin N Amer (Feb.) 257, 1955.
15. AMERICAN HEART ASSOCIATION-NATIONAL HEARTINSTITUTE: Epidemiology of cardiovascular dis-eases, methodology, hypertension and arterio-sclerosis, edited by H. Pollack, and D. E.Kruger. Amer J Public Health 50 (suppl. toNo. 10): 1960.
16. RoSE, G. A., HOLLAND, W. W., AND CROWLEY,E. A.: Sphygmomanometer for epidemiologists.Lancet 1: 296, 1964.
17. ARMITAGE, P., AND ROSE, G. A.: Variability ofmeasurements of casual blood pressure: I. Alaboratory study. Clin Sci 30: 325, 1966.
18. ARMITAGE, P., Fox, W., ROSE, G. A., AND TINK-ER, C. M.: Variability of measurements ofcasual blood pressure: II. Survey experience.Clin Sci 30: 337, 1966.
19. BURGESS, A. M., JR., FEJFAR, Z., AND KAGAN,A. R.: Arterial hypertension and ischemicheart disease: Comparison in epidemiologicalstudies. WHO Chron 17: 97, 1963.
20. GARROw, J. S.: Zero-muddler for unprejudicedsphygmomanometry. Lancet 2: 1205, 1963.
21. WILCOX, J.: Observer factors in the measurementof blood pressure. Nurs Rev 10: 4, 1961.
22. ROSE, G.: Standardization of observers in blood-pressure measurement. Lancet 1: 673, 1965.
Circulataon, Voiume XXXVI, December 1967
988
by on November 16, 2009 circ.ahajournals.orgDownloaded from

LEVIN ET AL.
phases of the cardiac cycle: I. Duration ofthe consecutive phases of the cardiac cycleand criteria for their precise determination.Amer J Physiol 65: 415, 1921.
10. UHLEY, M. H.: Lutembacher's syndrome and anew concept of the dynamics of interatrialseptal defect. Amer Heart J 24: 315, 1942.
11. BRANNON, E. S., WEENS, H. S., AND WARREN,J. V.: Atrial septal defect: Study of hemody-namics by the techniques of right heartcatheterization. Amer J Med Sci 210: 480,1945.
12. HULL, E.: Cause and effects of flow throughdefects of the atrial septum. Amer Heart J38: 350, 1949.
13. NADAS, A. S.: Pediatric Cardiology, ed. 2.Philadelphia, W. B. Saunders Co., 1963, p.369.
14. DEXTER, L.: Atrial septal defect. Brit Heart J18: 209, 1956.
15. COURNAND, A., MOTLEY, H. L., HiMELSTEIN,A., DRESDALE, D., AND BALDWIN, J.: Re-cording of blood pressure from the left auricleand pulmonary veins in human subjects withinterauricular septal defect. Amer J Physiol150: 267, 1947.
16. SHAFFER, A. B., SILBER, E. M., AND KATZ,L. N.: Observations on the interatrial pressuregradients in man. Circulation 10: 527, 1954.
17. MCDONALD, D. A.: Blood flow in arteries.Baltimore, Williams & Wilkins Co., 1960.
18. WENNEVOLD, A.: Diastolic murmur of atrialseptal defects as detected by intracardiacphonocardiography. Circulation 34: 132, 1966.
19. USHER, H. L.: Diagnostic value of intracardiacphonocardiography. Heart Bull 16: 32, 1967.
20. GAMBLE, J. W., HUGENHOLTZ, P. G., MONROE,R. C., POLANYI, M., AND NADAS, A. S.: Useof fiberoptics in clinical cardiac catheteriza-tion. Circulation 31: 328, 1965.
21. WIGGERS, C. J.: Pressure pulses in the cardio-vascular system. New York, Longmans, Green& Co., 1928.
22. BRAUNWALD, E., FISHMAN, A. P., AND COUR-NAND, A.: Time relationship of dynamicevents in the cardiac chambers, pulmonaryartery and aorta in man. Circulation Research4: 100, 1956.
23. KILBURN, K. H., AND SIEKER, H. O.: Hemo-dynamic effects of continuous positive andnegative pressure breathing in normal man.Circulation Research 8: 660, 1960.
CorrectionOn page 985 (vol. 36, 1967) of the "Recommendations for Human Blood Pressure
Determinations by Sphygmomanometers" it is stated "To measure blood pressure bythe flush method, a suitable cuff is placed on the forearm or calf...." This is in errorand should read "To measure blood pressure by the flush method, a suitable cuff isplaced on the wrist or ankle....'
Circulation, Volume XXXVII, April 1968
488
by on November 16, 2009 circ.ahajournals.orgDownloaded from