randy d ernst 1 , russell c hardie 2 , metin n gurcan 3 , aytekin oto 1 ,
DESCRIPTION
Randy D Ernst 1 , Russell C Hardie 2 , Metin N Gurcan 3 , Aytekin Oto 1 , Steve K Rogers 3 , Jeffrey W Hoffmeister 3 1. Department of Radiology, The University of Texas Medical Branch, Galveston TX 2. iCAD Inc. and University of Dayton, Dayton OH 3. iCAD Inc., Beavercreek OH. - PowerPoint PPT PresentationTRANSCRIPT
CAD Performance Analysis for Pulmonary Nodule Detection: Comparison of Thick- and Thin-
Slice Helical CT Scans
Randy D Ernst1, Russell C Hardie2, Metin N Gurcan3, Aytekin Oto1,
Steve K Rogers3, Jeffrey W Hoffmeister3
1. Department of Radiology, The University of Texas Medical Branch, Galveston TX
2. iCAD Inc. and University of Dayton, Dayton OH 3. iCAD Inc., Beavercreek OH

Introduction
This study compares the performance of a CAD (QuickCue™, iCAD, Inc.) system in detecting lung nodules from thick- and thin-slice multi-detector row CT scans, and to evaluate the potential benefit of CAD on radiologist sensitivity.

Methods and Materials
57 reports reviewed retrospectively Case selection:Obtained during a 5-month periodReferred from multiple departmentsContain at least 1 pulmonary nodule but
fewer than 10 nodules to localizeHave no significant breathing miss -
registration, post surgical changes, pleural effusions & atelectasis
Methods and Materials
4-detector LightSpeed QX/I Scanner, GE systems
HQ setting with 5.0 collimation, helical pitch of 0.75/1.0
Standard-dose (160 - 270 mA, 120 kVp)
Images were reconstructed at 5 mm (thick) and 2.5 mm (thin) slice thicknesses.

Methods and Materials140 nodules (3 mm - 25 mm) were identified pre-CAD by radiologists From thick-slice cases only.
Cases with multiple nodules were excluded.Truth marks were mapped to the thin-slice dataMean nodule size 7.3 ± 4.2 mm (3 – 25 mm)Gold standard for nodule truth comes for post-CAD Radiologist review One gold standard for thick-slice and one for thin-
slice

CAD System (QuickCue™, iCAD Inc.)
3D LungSegmentation
3D CandidateSegmentation
CalculateFeatures
DICOMImages
Classifier
DetectionMask

CAD detected 72.1% (101/140) of the pre-CAD truth nodules
CAD detected 35 additional radiologist-confirmed nodules, an increase of 25% (35/140) in sensitivity
5.6 (317/57) false-positives per case55 due to atelectasis18 due to scarring
Review of Thick-Slice CAD Results
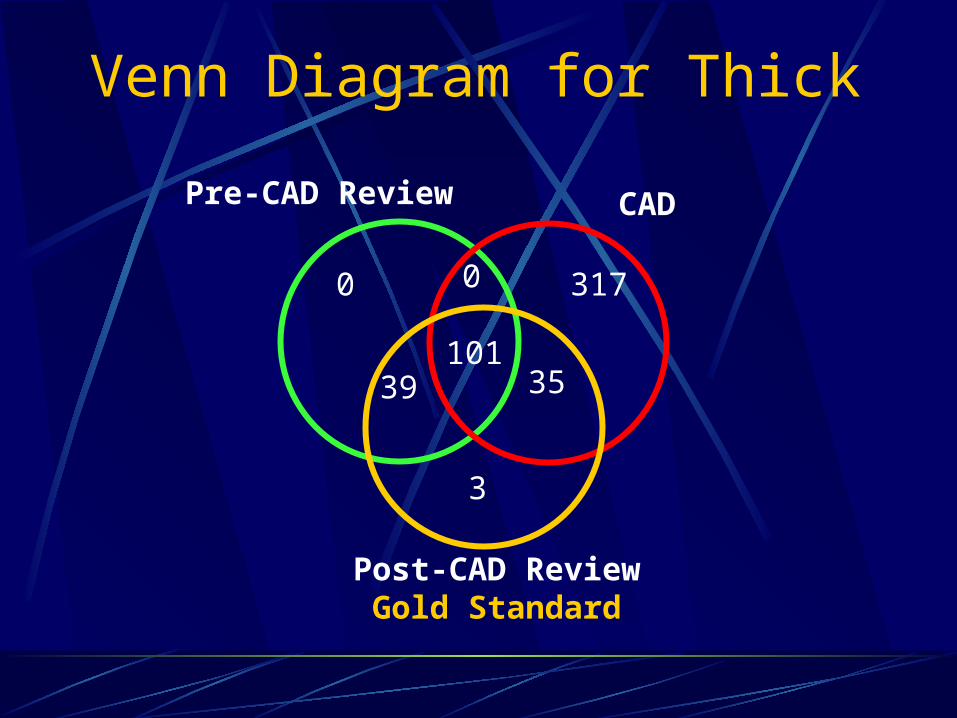
Venn Diagram for Thick
3
39 35
317
CADPre-CAD Review
Post-CAD ReviewGold Standard
101
0 0

CAD detected 80.7% (113/140) of the pre-CAD truth nodules.
CAD detected 94 additional radiologist-confirmed nodules, an increase of 67.1% (94/140).
4.6 (262/57) false-positives per case.70 due to atelectasis39 due to scarring
Review of Thin-Slice CAD Results

Venn Diagram for Thin
0
26 94
262
CAD using thin-slice
Pre-CAD Review using thick-slice with detections mapped to thin-slice
Post-CAD Review of thin-sliceGold Standard
113
0 0
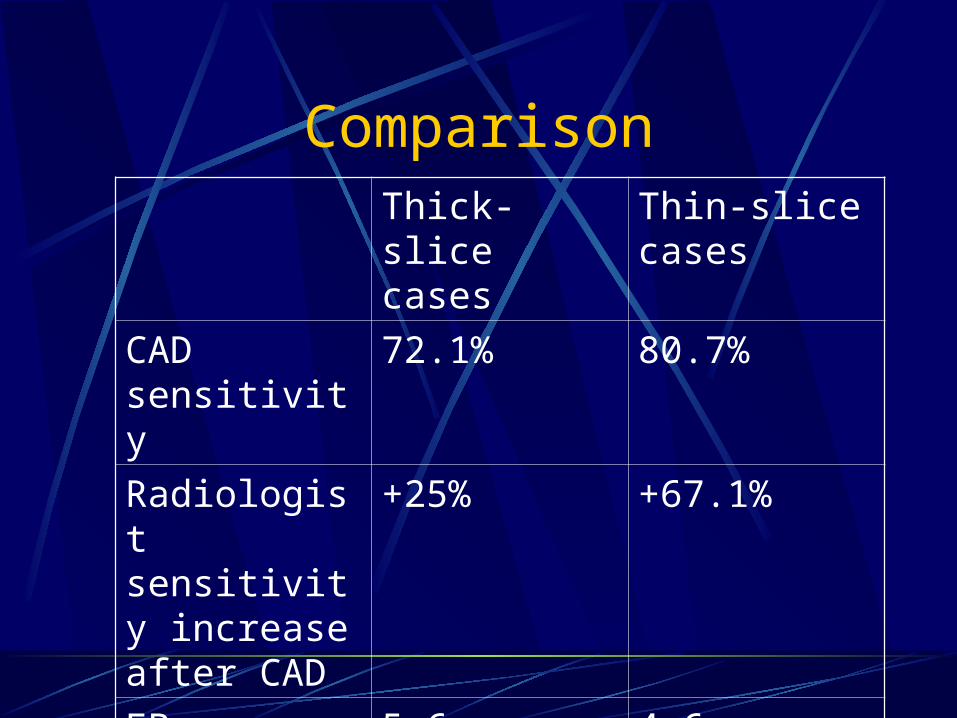
ComparisonThick-slice cases
Thin-slice cases
CAD sensitivity
72.1% 80.7%
Radiologist sensitivity increase after CAD
+25% +67.1%
FPs 5.6 4.6

FROC Curve for CAD
0 2 4 6 8 10 12 140
0.2
0.4
0.6
0.8
1
Average False Positives Per Case
Pro
bab
ility
of
Det
ecti
on
Thin SliceThick Slice
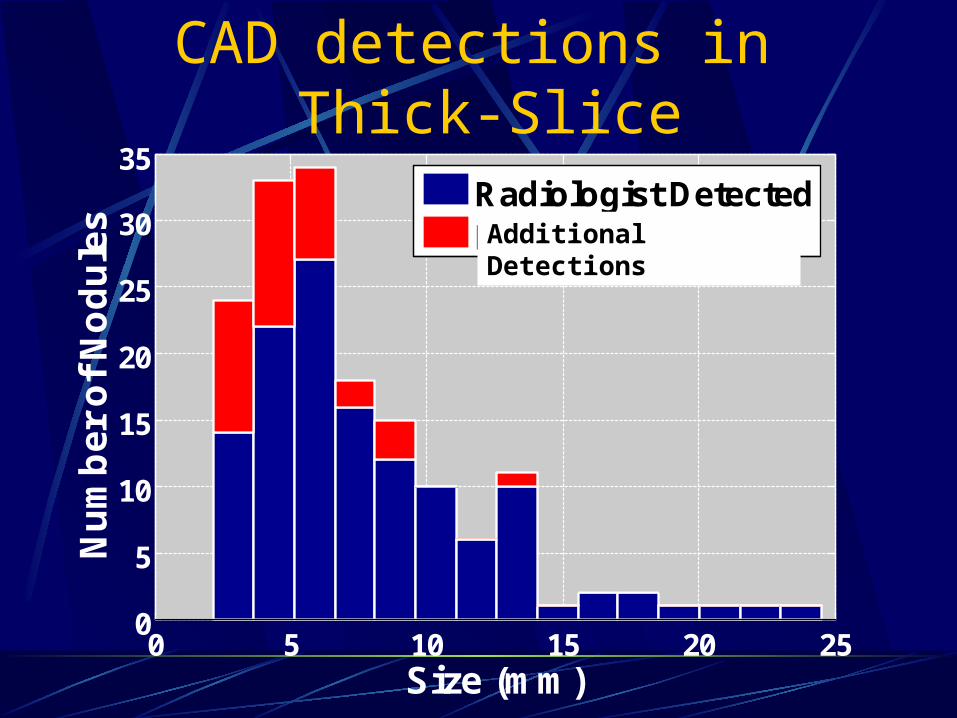
CAD detections in Thick-Slice
0 5 10 15 20 250
5
10
15
20
25
30
35
Size (mm)
Nu
mb
er
of
No
du
les
Radiologist DetectedRadiologist MissedAdditional Detections

CAD detections in Thin-Slice
0 5 10 15 20 250
10
20
30
40
50
Size (mm)
Nu
mb
er
of
No
du
les Radiologist Detected
Radiologist MissedAdditional Detections

5 primary lung cancers
24 cases of metastatic cancer including 7 lymphomas, 4 breast, 4 head and neck, 2
colon, 2 pancreas, 1 carcinoid, 1 seminoma, 1 ovarian, 1 melanoma and 1 tracheal papillomatosis
23 cases of infection, including19 granulomatous disease either calcified,
stable on follow-up or biopsy proven. 4 were presumed infection that resolved with follow-up
1 case proved to be a thrombosed AVM
4 cases lost to follow up
Case Follow-up

Example TPs
Examples of nodules that are detected by both radiologist and CAD





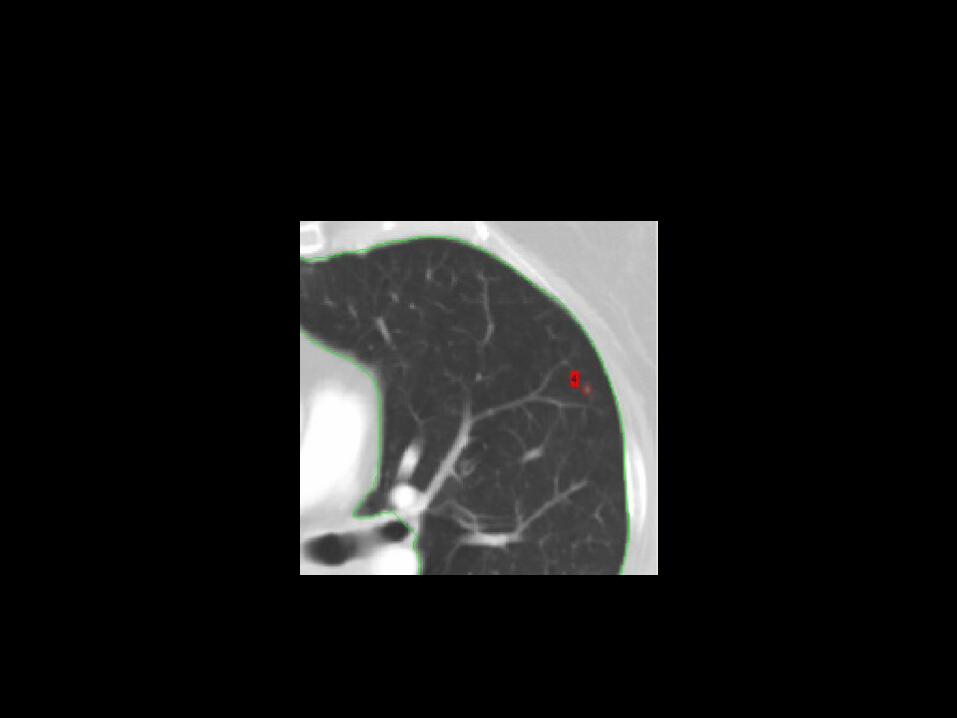
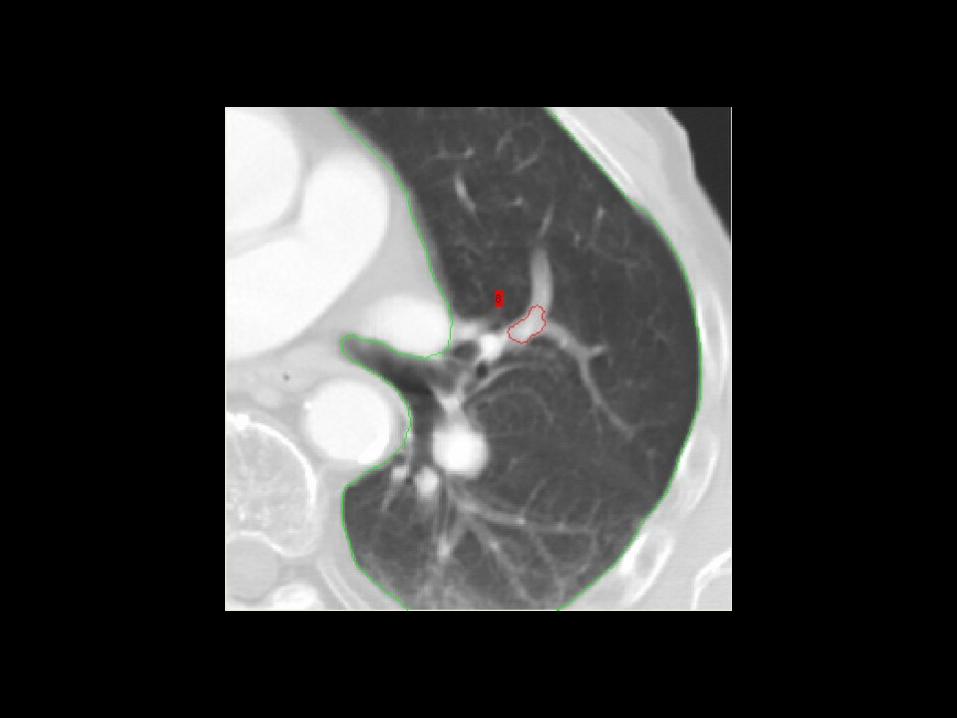
Example TPs
Examples of nodules that are initially missed by radiologists then detected after reviewing CAD








Review of CAD ResultsSources of false positivesVessel intersections Inaccurate lung segmentationPartial volume effectsOther lung abnormalities (scarring,
atelectasis)

Example FPs


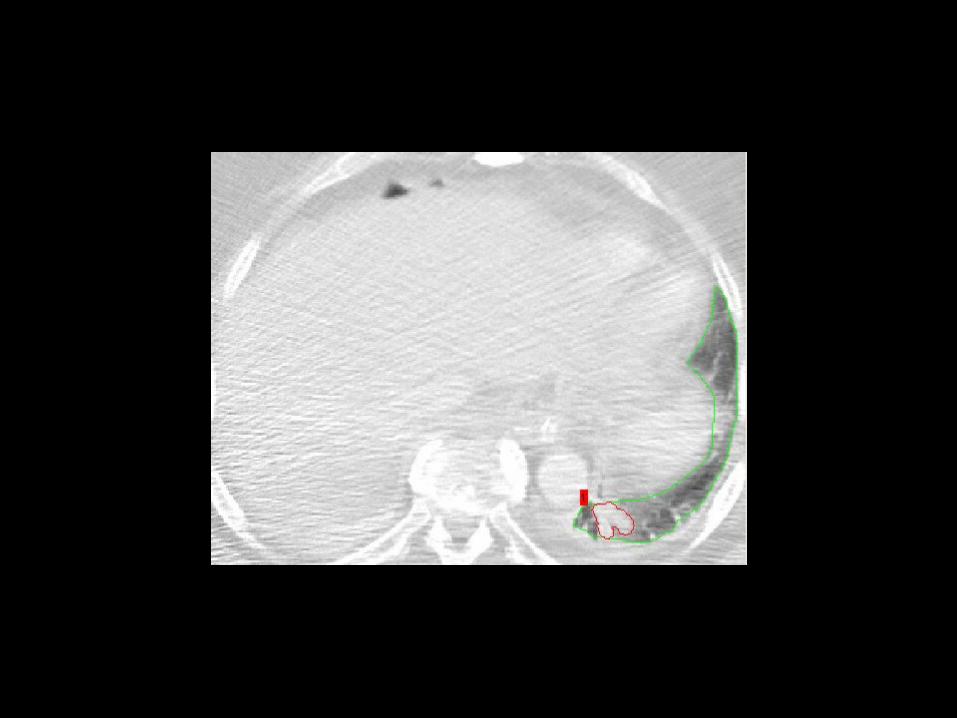

Review of CAD ResultsSources of false negatives (missed nodules)Low density, irregularStrong connectivity with vessels Imperfect candidate segmentation Inaccurate lung segmentation

Example FNs





Conclusions
Preliminary results indicate that both sensitivity and specificity of the CAD system increases when used with thin-slice scans versus thick-slice scans.The CAD system operating on both thick- and thin-slice scans improved radiologist sensitivity Improvement was greater for CAD
operating on thin-slice scans