ramon salazar catalan institute of oncology...ramon salazar catalan institute of oncology...
TRANSCRIPT

What is best for second lineRamon Salazar
Catalan Institute of Oncology
DisclosuresR Salazar has served in a consultant or advisory role for Amgen Merck
Serono Taihoo MSD Lylli BMS Roche Dx and enjoyed research funding for Roche Dx Roche Pharma and Merck Serono
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Regorafenib
Aflibercept
An
gio
gen
esis
Gro
wth TAS-102dagger
Ramucirumab
Chemo Backbone
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer a randomized GERCOR study
FOLFIRIFOLFIRI FOLFOX6FOLFOX6
OXL100 mgm2
R
FOLFOX6FOLFOX6 FOLFIRIFOLFIRI
ProgProg
Prog
Prog
Tournigand C Andreacute T Achille E et alJ Clin Oncol 2004 22 (2)
CPT11 180 mgm2N=226
Logrank
p = 026
Pro
bab
ilid
ad
00
02
04
06
08
10
0 4 8 12 16 20 24 28 32
Median (months)Folfiri85Folfox 80
Months
Pro
bab
ilid
ad
00
02
04
06
08
10
0 6 12 18
Months
Median (months)Folfiri 25Folfox 42
Logrank
p = 0003
EFFICACY VARIABLES
TIME TO 1ST LINE PROG TIME TO 2ND LINE PROG
Tournigand C Andreacute T Achille E et alJ Clin Oncol 2004 22 (2)
Overall survival curves
Tournigand C et al JCO 200422229-237
copy2004 by American Society of Clinical Oncology
35
4
FOLFIRIn = 69
63
15
FOLFOXn = 81
4049Absence of progression at 15 months
09215204Median overall survival mos
065
068
p value
115144Median overall TTP mos
8179ORR + SD
5456 ORR (CR)
FOLFOX
n = 111
FOLFIRI
n = 109
Arm A Arm B
V308 EFFICACY ENDPOINTS (5)
Tournigand C et al JCO 200422229-237
Chemo Backbone
Cancer Invest 201634(2)94-104 doi 1031090735790720151104689 Epub 2016 Feb 11XELOX vs FOLFOX in metastatic colorectal cancer An updated meta-analysis
Guo Y1 Xiong BH2 Zhang T3 Cheng Y1 Ma L4
bull Folfiri-Folfox are the preferred optionsbull Simillar PFS and OS
bull Sequence does not influence outcome (Tournigand)
bull Xelox not inferior than Folfox (Phase 3 Meta-analysis)bull But Folfox has prevailed probably because of differential toxicity profiles
bull Pooled analysis revealed that there were no statistical differences between both arms in OS and ORR XELOX arm had a higher incidence of thrombocytopenia hand-foot syndrome and diarrhea whereas neutropenia had a higher incidence in the FOLFOX group For mCRC the effect of XELOX is similar to FOLFOX
bull Xeliri not so popular (toxicity and no Phase 3 data)
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Aflibercept
An
gio
gen
esis
Gro
wth
Ramucirumab
Biological companion
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
depends on what is used first line and theevidence generated for each Chemo scheme
mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

DisclosuresR Salazar has served in a consultant or advisory role for Amgen Merck
Serono Taihoo MSD Lylli BMS Roche Dx and enjoyed research funding for Roche Dx Roche Pharma and Merck Serono
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Regorafenib
Aflibercept
An
gio
gen
esis
Gro
wth TAS-102dagger
Ramucirumab
Chemo Backbone
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer a randomized GERCOR study
FOLFIRIFOLFIRI FOLFOX6FOLFOX6
OXL100 mgm2
R
FOLFOX6FOLFOX6 FOLFIRIFOLFIRI
ProgProg
Prog
Prog
Tournigand C Andreacute T Achille E et alJ Clin Oncol 2004 22 (2)
CPT11 180 mgm2N=226
Logrank
p = 026
Pro
bab
ilid
ad
00
02
04
06
08
10
0 4 8 12 16 20 24 28 32
Median (months)Folfiri85Folfox 80
Months
Pro
bab
ilid
ad
00
02
04
06
08
10
0 6 12 18
Months
Median (months)Folfiri 25Folfox 42
Logrank
p = 0003
EFFICACY VARIABLES
TIME TO 1ST LINE PROG TIME TO 2ND LINE PROG
Tournigand C Andreacute T Achille E et alJ Clin Oncol 2004 22 (2)
Overall survival curves
Tournigand C et al JCO 200422229-237
copy2004 by American Society of Clinical Oncology
35
4
FOLFIRIn = 69
63
15
FOLFOXn = 81
4049Absence of progression at 15 months
09215204Median overall survival mos
065
068
p value
115144Median overall TTP mos
8179ORR + SD
5456 ORR (CR)
FOLFOX
n = 111
FOLFIRI
n = 109
Arm A Arm B
V308 EFFICACY ENDPOINTS (5)
Tournigand C et al JCO 200422229-237
Chemo Backbone
Cancer Invest 201634(2)94-104 doi 1031090735790720151104689 Epub 2016 Feb 11XELOX vs FOLFOX in metastatic colorectal cancer An updated meta-analysis
Guo Y1 Xiong BH2 Zhang T3 Cheng Y1 Ma L4
bull Folfiri-Folfox are the preferred optionsbull Simillar PFS and OS
bull Sequence does not influence outcome (Tournigand)
bull Xelox not inferior than Folfox (Phase 3 Meta-analysis)bull But Folfox has prevailed probably because of differential toxicity profiles
bull Pooled analysis revealed that there were no statistical differences between both arms in OS and ORR XELOX arm had a higher incidence of thrombocytopenia hand-foot syndrome and diarrhea whereas neutropenia had a higher incidence in the FOLFOX group For mCRC the effect of XELOX is similar to FOLFOX
bull Xeliri not so popular (toxicity and no Phase 3 data)
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Aflibercept
An
gio
gen
esis
Gro
wth
Ramucirumab
Biological companion
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
depends on what is used first line and theevidence generated for each Chemo scheme
mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Regorafenib
Aflibercept
An
gio
gen
esis
Gro
wth TAS-102dagger
Ramucirumab
Chemo Backbone
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer a randomized GERCOR study
FOLFIRIFOLFIRI FOLFOX6FOLFOX6
OXL100 mgm2
R
FOLFOX6FOLFOX6 FOLFIRIFOLFIRI
ProgProg
Prog
Prog
Tournigand C Andreacute T Achille E et alJ Clin Oncol 2004 22 (2)
CPT11 180 mgm2N=226
Logrank
p = 026
Pro
bab
ilid
ad
00
02
04
06
08
10
0 4 8 12 16 20 24 28 32
Median (months)Folfiri85Folfox 80
Months
Pro
bab
ilid
ad
00
02
04
06
08
10
0 6 12 18
Months
Median (months)Folfiri 25Folfox 42
Logrank
p = 0003
EFFICACY VARIABLES
TIME TO 1ST LINE PROG TIME TO 2ND LINE PROG
Tournigand C Andreacute T Achille E et alJ Clin Oncol 2004 22 (2)
Overall survival curves
Tournigand C et al JCO 200422229-237
copy2004 by American Society of Clinical Oncology
35
4
FOLFIRIn = 69
63
15
FOLFOXn = 81
4049Absence of progression at 15 months
09215204Median overall survival mos
065
068
p value
115144Median overall TTP mos
8179ORR + SD
5456 ORR (CR)
FOLFOX
n = 111
FOLFIRI
n = 109
Arm A Arm B
V308 EFFICACY ENDPOINTS (5)
Tournigand C et al JCO 200422229-237
Chemo Backbone
Cancer Invest 201634(2)94-104 doi 1031090735790720151104689 Epub 2016 Feb 11XELOX vs FOLFOX in metastatic colorectal cancer An updated meta-analysis
Guo Y1 Xiong BH2 Zhang T3 Cheng Y1 Ma L4
bull Folfiri-Folfox are the preferred optionsbull Simillar PFS and OS
bull Sequence does not influence outcome (Tournigand)
bull Xelox not inferior than Folfox (Phase 3 Meta-analysis)bull But Folfox has prevailed probably because of differential toxicity profiles
bull Pooled analysis revealed that there were no statistical differences between both arms in OS and ORR XELOX arm had a higher incidence of thrombocytopenia hand-foot syndrome and diarrhea whereas neutropenia had a higher incidence in the FOLFOX group For mCRC the effect of XELOX is similar to FOLFOX
bull Xeliri not so popular (toxicity and no Phase 3 data)
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Aflibercept
An
gio
gen
esis
Gro
wth
Ramucirumab
Biological companion
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
depends on what is used first line and theevidence generated for each Chemo scheme
mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer a randomized GERCOR study
FOLFIRIFOLFIRI FOLFOX6FOLFOX6
OXL100 mgm2
R
FOLFOX6FOLFOX6 FOLFIRIFOLFIRI
ProgProg
Prog
Prog
Tournigand C Andreacute T Achille E et alJ Clin Oncol 2004 22 (2)
CPT11 180 mgm2N=226
Logrank
p = 026
Pro
bab
ilid
ad
00
02
04
06
08
10
0 4 8 12 16 20 24 28 32
Median (months)Folfiri85Folfox 80
Months
Pro
bab
ilid
ad
00
02
04
06
08
10
0 6 12 18
Months
Median (months)Folfiri 25Folfox 42
Logrank
p = 0003
EFFICACY VARIABLES
TIME TO 1ST LINE PROG TIME TO 2ND LINE PROG
Tournigand C Andreacute T Achille E et alJ Clin Oncol 2004 22 (2)
Overall survival curves
Tournigand C et al JCO 200422229-237
copy2004 by American Society of Clinical Oncology
35
4
FOLFIRIn = 69
63
15
FOLFOXn = 81
4049Absence of progression at 15 months
09215204Median overall survival mos
065
068
p value
115144Median overall TTP mos
8179ORR + SD
5456 ORR (CR)
FOLFOX
n = 111
FOLFIRI
n = 109
Arm A Arm B
V308 EFFICACY ENDPOINTS (5)
Tournigand C et al JCO 200422229-237
Chemo Backbone
Cancer Invest 201634(2)94-104 doi 1031090735790720151104689 Epub 2016 Feb 11XELOX vs FOLFOX in metastatic colorectal cancer An updated meta-analysis
Guo Y1 Xiong BH2 Zhang T3 Cheng Y1 Ma L4
bull Folfiri-Folfox are the preferred optionsbull Simillar PFS and OS
bull Sequence does not influence outcome (Tournigand)
bull Xelox not inferior than Folfox (Phase 3 Meta-analysis)bull But Folfox has prevailed probably because of differential toxicity profiles
bull Pooled analysis revealed that there were no statistical differences between both arms in OS and ORR XELOX arm had a higher incidence of thrombocytopenia hand-foot syndrome and diarrhea whereas neutropenia had a higher incidence in the FOLFOX group For mCRC the effect of XELOX is similar to FOLFOX
bull Xeliri not so popular (toxicity and no Phase 3 data)
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Aflibercept
An
gio
gen
esis
Gro
wth
Ramucirumab
Biological companion
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
depends on what is used first line and theevidence generated for each Chemo scheme
mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Logrank
p = 026
Pro
bab
ilid
ad
00
02
04
06
08
10
0 4 8 12 16 20 24 28 32
Median (months)Folfiri85Folfox 80
Months
Pro
bab
ilid
ad
00
02
04
06
08
10
0 6 12 18
Months
Median (months)Folfiri 25Folfox 42
Logrank
p = 0003
EFFICACY VARIABLES
TIME TO 1ST LINE PROG TIME TO 2ND LINE PROG
Tournigand C Andreacute T Achille E et alJ Clin Oncol 2004 22 (2)
Overall survival curves
Tournigand C et al JCO 200422229-237
copy2004 by American Society of Clinical Oncology
35
4
FOLFIRIn = 69
63
15
FOLFOXn = 81
4049Absence of progression at 15 months
09215204Median overall survival mos
065
068
p value
115144Median overall TTP mos
8179ORR + SD
5456 ORR (CR)
FOLFOX
n = 111
FOLFIRI
n = 109
Arm A Arm B
V308 EFFICACY ENDPOINTS (5)
Tournigand C et al JCO 200422229-237
Chemo Backbone
Cancer Invest 201634(2)94-104 doi 1031090735790720151104689 Epub 2016 Feb 11XELOX vs FOLFOX in metastatic colorectal cancer An updated meta-analysis
Guo Y1 Xiong BH2 Zhang T3 Cheng Y1 Ma L4
bull Folfiri-Folfox are the preferred optionsbull Simillar PFS and OS
bull Sequence does not influence outcome (Tournigand)
bull Xelox not inferior than Folfox (Phase 3 Meta-analysis)bull But Folfox has prevailed probably because of differential toxicity profiles
bull Pooled analysis revealed that there were no statistical differences between both arms in OS and ORR XELOX arm had a higher incidence of thrombocytopenia hand-foot syndrome and diarrhea whereas neutropenia had a higher incidence in the FOLFOX group For mCRC the effect of XELOX is similar to FOLFOX
bull Xeliri not so popular (toxicity and no Phase 3 data)
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Aflibercept
An
gio
gen
esis
Gro
wth
Ramucirumab
Biological companion
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
depends on what is used first line and theevidence generated for each Chemo scheme
mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Overall survival curves
Tournigand C et al JCO 200422229-237
copy2004 by American Society of Clinical Oncology
35
4
FOLFIRIn = 69
63
15
FOLFOXn = 81
4049Absence of progression at 15 months
09215204Median overall survival mos
065
068
p value
115144Median overall TTP mos
8179ORR + SD
5456 ORR (CR)
FOLFOX
n = 111
FOLFIRI
n = 109
Arm A Arm B
V308 EFFICACY ENDPOINTS (5)
Tournigand C et al JCO 200422229-237
Chemo Backbone
Cancer Invest 201634(2)94-104 doi 1031090735790720151104689 Epub 2016 Feb 11XELOX vs FOLFOX in metastatic colorectal cancer An updated meta-analysis
Guo Y1 Xiong BH2 Zhang T3 Cheng Y1 Ma L4
bull Folfiri-Folfox are the preferred optionsbull Simillar PFS and OS
bull Sequence does not influence outcome (Tournigand)
bull Xelox not inferior than Folfox (Phase 3 Meta-analysis)bull But Folfox has prevailed probably because of differential toxicity profiles
bull Pooled analysis revealed that there were no statistical differences between both arms in OS and ORR XELOX arm had a higher incidence of thrombocytopenia hand-foot syndrome and diarrhea whereas neutropenia had a higher incidence in the FOLFOX group For mCRC the effect of XELOX is similar to FOLFOX
bull Xeliri not so popular (toxicity and no Phase 3 data)
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Aflibercept
An
gio
gen
esis
Gro
wth
Ramucirumab
Biological companion
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
depends on what is used first line and theevidence generated for each Chemo scheme
mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

35
4
FOLFIRIn = 69
63
15
FOLFOXn = 81
4049Absence of progression at 15 months
09215204Median overall survival mos
065
068
p value
115144Median overall TTP mos
8179ORR + SD
5456 ORR (CR)
FOLFOX
n = 111
FOLFIRI
n = 109
Arm A Arm B
V308 EFFICACY ENDPOINTS (5)
Tournigand C et al JCO 200422229-237
Chemo Backbone
Cancer Invest 201634(2)94-104 doi 1031090735790720151104689 Epub 2016 Feb 11XELOX vs FOLFOX in metastatic colorectal cancer An updated meta-analysis
Guo Y1 Xiong BH2 Zhang T3 Cheng Y1 Ma L4
bull Folfiri-Folfox are the preferred optionsbull Simillar PFS and OS
bull Sequence does not influence outcome (Tournigand)
bull Xelox not inferior than Folfox (Phase 3 Meta-analysis)bull But Folfox has prevailed probably because of differential toxicity profiles
bull Pooled analysis revealed that there were no statistical differences between both arms in OS and ORR XELOX arm had a higher incidence of thrombocytopenia hand-foot syndrome and diarrhea whereas neutropenia had a higher incidence in the FOLFOX group For mCRC the effect of XELOX is similar to FOLFOX
bull Xeliri not so popular (toxicity and no Phase 3 data)
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Aflibercept
An
gio
gen
esis
Gro
wth
Ramucirumab
Biological companion
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
depends on what is used first line and theevidence generated for each Chemo scheme
mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Chemo Backbone
Cancer Invest 201634(2)94-104 doi 1031090735790720151104689 Epub 2016 Feb 11XELOX vs FOLFOX in metastatic colorectal cancer An updated meta-analysis
Guo Y1 Xiong BH2 Zhang T3 Cheng Y1 Ma L4
bull Folfiri-Folfox are the preferred optionsbull Simillar PFS and OS
bull Sequence does not influence outcome (Tournigand)
bull Xelox not inferior than Folfox (Phase 3 Meta-analysis)bull But Folfox has prevailed probably because of differential toxicity profiles
bull Pooled analysis revealed that there were no statistical differences between both arms in OS and ORR XELOX arm had a higher incidence of thrombocytopenia hand-foot syndrome and diarrhea whereas neutropenia had a higher incidence in the FOLFOX group For mCRC the effect of XELOX is similar to FOLFOX
bull Xeliri not so popular (toxicity and no Phase 3 data)
OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Aflibercept
An
gio
gen
esis
Gro
wth
Ramucirumab
Biological companion
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
depends on what is used first line and theevidence generated for each Chemo scheme
mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

OralIV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Aflibercept
An
gio
gen
esis
Gro
wth
Ramucirumab
Biological companion
bull Slide courtesy of M PeetersFluorouracil (25 mgmL injection) Summary of Product Characteristics Hospira Capecitabine (XELODAreg) Summary of Product Characteristics Roche Raltitrexed (Tomudexreg) Summary of Product Characteristics Hospira Irinotecan (Camptoreg) Summary of Product Characteristics Pfizer Oxaliplatin (Eloxatinreg) Summary of Product Characteristics Sanofi Bevacizumab (Avastinreg) Summary of Product Characteristics Roche Aflibercept (Zaltrapreg) Summary of Product Characteristics Sanofi Regorafenib (Stivargareg) Summary of Product Characteristics Bayer Cetuximab (Erbituxreg) Summary of Product Characteristics Merck Serono Panitumumab(Vectibixreg) Summary of Product Characteristics Amgen PR Newswire 02-03-15 Available at httpwwwprnewswirecouknews-releasestaiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511html Accessed 21-04-15
daggerMarketing Authorisation Application
submitted to the to the European Medicines
Agency in March 2015 for TAS-102
for use in the treatment of refractory mCRC
depends on what is used first line and theevidence generated for each Chemo scheme
mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

mCRCmdashSecond-line randomized phase III trials
1
8
Studies Treatment N Prior Bevacizumab OSHR PFSHR
Aflibercept(VELOUR)
FOLFIRI + aflibercept 612 304vs 0817 0758
FOLFIRI + placebo 614 305 P=00032 P=000007
Panitumumab(study 20050181)
2
FOLFIRI + panitumumab 303 18vs 085 0732
FOLFIRI 294 20 P=012 P=00036
Ramucirumab FOLFIRI + ramucirumab vs folfiri
Cetuximab(Study CA225006)
3
irinotecan + cetuximab 97 NAvs 129 0773
irinotecan 95 NA P=01755 P=00953
Bevacizumab(ECOG 3200)4
FOLFOX + bevacizumab 293 0vs 075 052
FOLFOX 292 0 P=0001 Plt00001
Bevacizumab(ML18147)5
Oxali-Iri-CT + bevacizumab 409 100
vs 083 068
Oxali-Iri-containing CT 411 100 P=00062 Plt00001
1 Van Cutsem et al J Clin Oncol 2012 2 Assessment report for Vectibix Procedure EMEAHC000741II0017 3 Assessment report for Erbitux Procedure EMEAHC000558II0020 4 Assessment report for Avastin Procedure EMEAHC000582II0014 5 Arnold ASCO 2012 Abstract CRA3503
folfiri
folfox
Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Bevacizumab
E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

E3200
bullObj Primario supervivencia
bullObj Secundario RR
Previously treated metastatic CRC
(n=822)
mainly bolus
irinotecan + 5-
FU + LV [IFL]
Oxaliplatin5-FULV (n=290)
Bevacizumab monotherapy10mgkg every 2 weeks
(n=243)
Oxaliplatin5-FULV + Bevacizumab 10mgkg
every2 weeks(n=289)
PD
PD
PD
Arm closed to enrolment
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

E3200 PFS
Pro
babili
ty o
f bein
g p
rogre
ssio
n f
ree
10
08
06
04
02
0
Progression-free survival (months)0 2 4 6 8 10 12 14 16 18 20
HR=064
A vs B plt00001
B vs C plt00001
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
27 7248
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

E3200 SG
MedianTotal
A FOLFOX4 + Bevacizumab 289 129
B FOLFOX4 290 108
C Bevacizumab 243 102
HR = hazard ratio
Pro
babili
ty o
f su
rviv
al
10
08
06
04
02
0
Time (months)
HR=076
A vs B p=00018
B vs C p=095
102 129
108
0 3 6 9 12 15 18 21 24 27 30 33 36
A FOLFOX4 + Bevacizumab
C Bevacizumab
B FOLFOX4
Giantonio BJ et al J Clin Oncol 200523 (June 1 Suppl)1s (Abstract 2)
FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

FOLFOX4 + Avastin (n=271)
FOLFOX4 (n=271)
Avastin (n=230)
Overall response () 218 92 30
Complete response () 19 07 0
Partial response () 199 85 30
Stable disease () 517 450 291
Estudio E3200 tasa de respuestas
FOLFOX + Bevacizumab versus FOLFOX plt00001
Giantonio BJ et al J Clin Oncol 200523(June 1 Suppl)1s (Abstract 2)
BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

BEV + standard first-line CT (either oxaliplatin or
irinotecan-based)(n=820)
Randomise 11
Standard second-line CT (oxaliplatin or irinotecan-based) until PD
BEV (25 mgkgwk) + standard second-line CT (oxaliplatin
or irinotecan-based) until PD
PD
ML18147 study design (phase III)
CT switch
Oxaliplatin rarr Irinotecan
Irinotecan rarr Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint bull Overall survival (OS) from randomisation
Secondary endpoints
included
bull Progression-free survival (PFS)
bull Best overall response rate
bull Safety
Stratification factors bull First-line CT (oxaliplatin-based irinotecan-based)
bull First-line PFS (le9 months gt9 months)
bull Time from last BEV dose (le42 days gt42 days)
bull ECOG PS at baseline (01 2)
Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Second-line chemotherapy during study Randomised patients
Second-line CT regimen
CT
(n=407)
BEV + CT
(n=407)
Irinotecan-based CT 43 42
FOLFIRI 14 16
LV5FU2 + CPT11 (Douillard regimen1) 7 7
XELIRI 12 12
Other regimens 10 7
Oxaliplatin-based CT 57 58
FOLFOX4 mFOLFOX4 18 19
FOLFOX6 13 16
FUFOX 9 6
XELOX 11 14
Other regimens 6 4
1 Douillard et al Lancet 20003551041ndash7
PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

PFS ITT population
PFS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42
No at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2 0
CT (n=410)BEV + CT (n=409)
41 mo 57 mo
Unstratifieda HR 068 (95 CI (059ndash078)
plt00001 (log-rank test)
Stratifiedb HR 067 (95 CI 058ndash078)
plt00001 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

OS ITT population
OS
est
imat
e
Time (months)
10
08
06
04
02
00 6 12 18 24 30 36 42 48
No at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
CT (n=410)BEV + CT (n=409)
98 mo 112 mo
Unstratifieda HR 081 (95 CI 069ndash094)
p=00062 (log-rank test)
Stratifiedb HR 083 (95 CI 071ndash097)
p=00211 (log-rank test)
aPrimary analysis method bStratified by first-line CT (oxaliplatin-based irinotecan-based) first-line PFS (le9 months gt9 months) time from last dose
of BEV (le42 days gt42 days) ECOG performance status at baseline (0 ge1)
Median follow-up CT 96 months (range 0ndash455) BEV + CT 111 months (range 03ndash440)
Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Subgroup analysis of OS ITT population
aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when
study was transferred to Roche All patients listed under AIO were included in primary analysis
Category Subgroup n HR (95 CI)
All All 819 081 (069ndash094)
Patient populationa AIO 260 086 (067ndash111)
ML18147 559 078 (064ndash094)
Gender Female 294 099 (077ndash128)
Male 525 073 (060ndash088)
Age lt65 years 458 079 (065ndash098)
ge65 years 361 083 (066ndash104)
ECOG performance status 0 357 074 (059ndash094)
ge1 458 087 (071ndash106)
First-line PFS le9 months 449 089 (073ndash109)
gt9 months 369 073 (058ndash092)
First-line CT Oxaliplatin-based 343 079 (062ndash100)
Irinotecan-based 476 082 (067ndash100)
Time from last BEV le42 days 630 082 (069ndash097)
gt42 days 189 076 (055ndash106)
Liver metastasis only No 592 081 (067ndash097)
Yes 226 079 (059ndash105)
No of organs
with metastasis
1 307 083 (064ndash108)
gt1 511 077 (064ndash094)
HR 0 1 2
Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Best overall response Measurable disease population
aPatients with a best overall response of confirmed complete or partial responsebThis analysis was not prespecifiedcIncludes lsquonot-evaluablersquo or lsquono tumour assessmentrsquo following baseline visit
Outcome
CT
(n=406)
BEV + CT
(n=404)
Respondersa n () 16 (39) 22 (54)
p-value (unstratified) 03113
p-value (stratified) 04315
Complete response n () 2 (lt1) 1 (lt1)
Partial response n () 14 (3) 21 (5)
Stable disease n () 204 (50) 253 (63)
Disease control rate n () 220 (54) 275 (68)
p-valueb lt00001
PD n () 142 (35) 87 (22)
Missingc n () 44 (11) 42 (10)
Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Aflibercept
VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

VELOUR trial
38
PROGRESIOacuteN DE LA ENFERMEDAD
MUERTE
FACTORES DE ESTRATIFICACIOacuteN
Prior Bevacizumab (YN)ECOG PS (0 vs 1 vs 2)
Pacientes con caacutencer colorrectal metastaacutesico
despueacutes del fracaso de un reacutegimen basado en
oxaliplatino12
R 11
614 pts
612 pts
Aflibercept 4 mgkg IV+ FOLFIRI q 2 semanas
Placebo + FOLFIRIq 2 semanas
1 Clinicaltrialsgov NCT00561470 2 Van Cutsem Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Poblacioacuten de estudio1226 randomizados 1216 tratadosAnaacutelisis final de 863 OS eventos
Objetivo primario SG
Objetivos secundarios TR SLP seguridad FC
VELOUR acroacutenimo VEGF Trap(aflibercept) with irinotecan in colorectal cancer after failure of oxaliplatin regimen
614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

614 355 171 94 46 24 9
612 420 247 99 43 17 7
VELOUR Progression Free SurvivalITT Population Independent Review Committee
42
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
0 3 6 9 12 15 18 21 24 27 30
NUMBERAT RISK
Stratified HR = 0758 [9999 CI 0578ndash0995]Log-rank P = 000007
Censor
AfliberceptFOLFIRI median = 69 monthsPlaceboFOLFIRI median = 467 months
10
09
08
07
06
05
04
03
02
01
00
KA
PLA
N-M
EIE
RE
ST
IMA
TE
TIM
E(m
ont
hs) Cut-off date May 6 2011
43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

43
1 Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain 2 Joulain et al ASCO 2012 abstract 36023 Tabernero et al Eur J Cancer 201147(2) Abstract 6LBA and presentation at ESMO 2011 EMCC September 23ndash27 2011 Stockholm Sweden
10
09
08
07
06
05
04
03
02
01
00
KA
PL
AN
-ME
IER
ES
TIM
AT
E
TIEMPO (meses)
Fecha de corte Febrero 7 2011
Seguimiento mediano 2228 meses
PROBABILIDAD DE SUPERVIVEacuteNCIA3
Estratificado HR=0817[9534 CI 0713ndash0937]
Log-rank P=00032
AfliberceptFOLFIRImediana SGsup1=135 mesesmedia SGsup2=232 meses75 quartile 2559 (2201ndash3170)
PlaceboFOLFIRImediana SGsup1=121 mesesmedia SGsup2=203 meses75 quartile 2103 (1892ndash2280)
791 503 309 187 120
819 561 385 280 223 AfliberceptFOLFIRI
PlaceboFOLFIRI
Censor
Δ=14 months2
Δ=26 months2
Δ=44 months2
0 3 6 9 12 15 18 21 24 27 30 33 36 39
El beneficio absoluto en supervivencia del estudio se incrementa con el tiempo de seguimiento mdash la mejora en supervivencia a los 2 antildeos fue del 50 (280 con aflibercept vs 187 con
placebo) Y casi el doble a los 30 meses (223 vs 120)
EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

EVALUABLE POPULATION () PLACEBO (N=530) AFLIBERCEPT (N=531)
BEST OVERALL RESPONSE
Complete response 04 0
Partial response 108 198
Stable disease 649 659
Progressive disease 215 104
Not evaluable 25 40
OVERALL RESPONSE RATE
CR or PR 111 198
95 CI 85ndash138 164ndash232
P-value 00001
VELOUR Response Rate Independent Review Committee
44
Van Cutsem et al Ann Oncol 201122(suppl 5) Abstract O-0024 and presentation at ESMO 13th WCGIC June 22-25 2011 Barcelona Spain
Evaluable population Patients with measurable target lesions that have agreed for third party reviewStratified Cochran Mantel test
POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

POBLACIOacuteN ITT () PLACEBO (N=614) AFLIBERCEPT (N=612)
Discontinuacioacuten del tratamiento de estudio 974 969
Progresioacuten de enfermedad 712 498
Acontecimiento adverso 121 266
Otro 03 05
Peticioacuten del paciente 70 126
Decisioacuten del investigador 34 33
Cirugiacutea metaacutestasis 16 20
Otras causas 21 26
Tratamiento de estudio en curso 18 23
VELOUR treatment interruption
48
Van Cutsem et al Ann Oncol 201122(suppl 5) Resumen O-0024 y presentacioacuten en ESMO 13th WCGIC 22-25 de junio de 2011 Barcelona Espantildea
Otras causas incluyen retirada del consentimiento peacuterdida en el seguimiento incumplimiento y otras razones no clasificadas
Drug related Dearhs (23 vs 07)The adverse events (all grades) leading most frequently to permanent discontinuation of study treatment were asthenicconditions (38 v 13 respectively) infections (34 v 17) diarrhea (23 v 07) and hypertension (23 v 0)
Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Ramucirumab
bull RAISE phase 3 trial second line
bull disease progression during or within 6 months of the last dose of first-line therapy withbevacizumab oxaliplatin and a fluoropyrimidine for metastatic disease
bullTabernero J Yoshino T Cohn A Obermannova R Bodoky G Garcia-Carbonero R et al
(2015) Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with
metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab
oxaliplatin and a fluoropyrimidine (RAISE) a randomised double-blind multicentre phase III
study Lancet Oncol 16 499ndash508 [PubMed]
Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Response Rate134 vs 125
Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Panitumumab
Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Tx Arm 1
Panitumumab
60 mgkg Q2W +
FOLFIRI Q2W
E
N
R
O
L
L
M
E
N
T
E
N
D
O
F
T
R
E
A
T
M
E
N
T
L
O
N
G
T
E
R
M
F
O
L
L
O
W
U
PDisease assessments
every 8 weeks
Tx Arm 2
FOLFIRI Q2W
Study
20050181
Countries
United
States
RussiaJapan
FranceBelgiumThe NetherlandsGermanySwitzerlandAustriaItalyCzech RepublicSlovakiaPolandLithuania
Australia
Enrollment Target
1100 patients
Randomization stratification
bull ECOG score 0-1 vs 2
bullPrior oxaliplatin exposure for mCRC
bullPrior bevacizumab exposure for mCRC
S
C
R
E
E
N
I
N
G
UkraineRomaniaBulgariaUnited KingdomIrelandPortugalSpainNorwaySwedenFinland
181 TRIAL Study Schema and Stratification
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

20181614121086420
00
01
02
03
04
05
06
07
08
09
10
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
Months
HR = 073 (95 CI 059 090)
Log-rank p-value = 0004
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
178303 (59) 59 (55-67)
FOLFIRI 203294 (69) 39 (37-53)
WT KRAS Significant Improvement of Progression-Free Survival
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

10
Panitumumab
+ FOLFIRIFOLFIRI alone
Patients at risk
89303 288 264 235 217 189 168 147 65111
74294 278 249 223 187 166 146 121 5893
1843 929
1646 726
0 04
1 05
20181614121086420
01
02
03
04
05
06
07
08
09
Months
323028262422 34
Su
rv iva
l P
rob
ab
ility
00
HR = 085 (95 CI 070 104)
Log-rank p-value = 012
EventsN ()
Median (95 CI) months
Panitumumab + FOLFIRI
200 (66) 145 (130 - 160)
FOLFIRI alone 207 (70) 125 (112 - 142)
WT KRAS Trend for Overall Survival Benefit
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Subsequent Use of EGFR mAb 10 pmab arm vs 31 FOLFIRI arm
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov
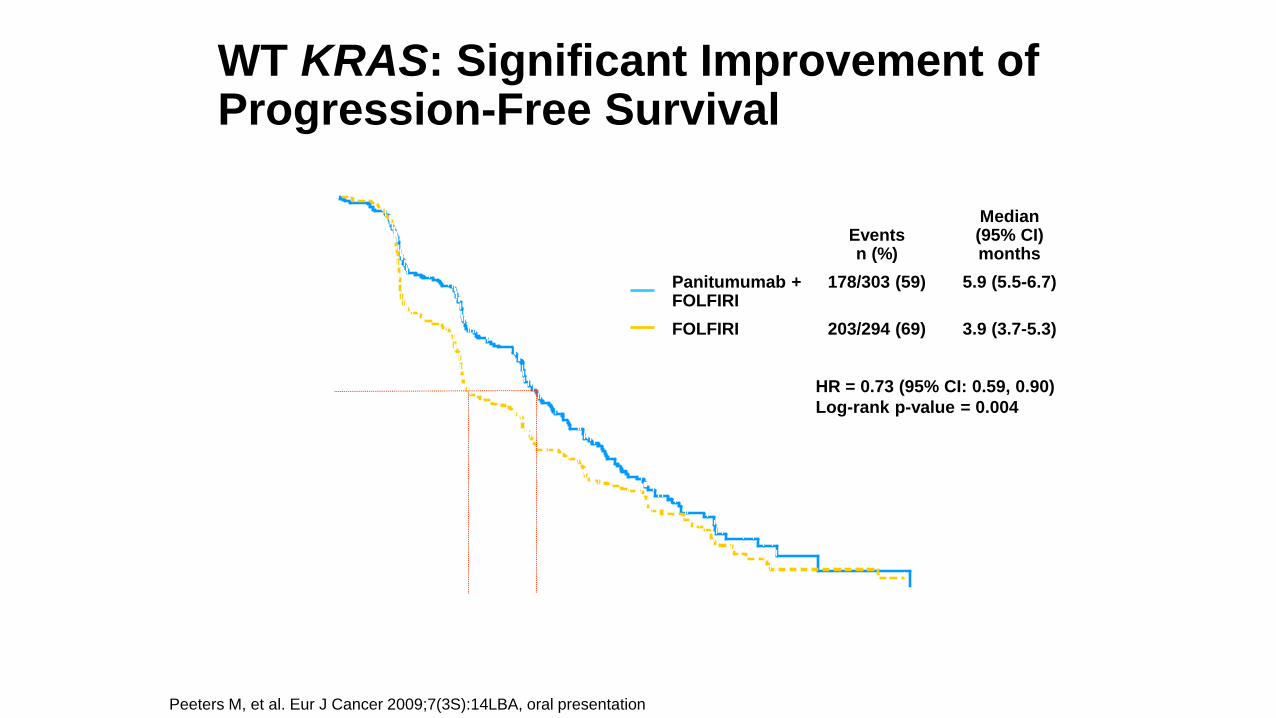
62
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)12
Panitumumab trialsTumor location analyses ndash RAS WT
Trial(line)
TreatmentsTumorlocation
Patients n ORR
PFS OS
Median months
HR (95 CI)
Median months
HR (95 CI)
Phase III PRIME(1st line)
Pani + FOLFOX4 vs FOLFOX4
Left 169 vs 159 68 vs 53 129 vs 92072
(057ndash090)303 vs 236
073 (057ndash093)
Right 39 vs 49 42 vs 35 75 vs 70080
(050ndash126)111 vs 154
087 (055ndash137)
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 53 vs 54 64 vs 57 146 vs 115068
(021ndash200)434 vs 320
077 (022ndash327)
Right 22 vs 14 63 vs 50 87 vs 126 104
(018ndash379)175 vs 210
067 (008ndash249)
Phase III Study 181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 150 vs 148 50 vs 13 80 vs 58088
(069ndash112)201 vs 166
096 (074ndash123)
Right 31 vs 39 13 vs 3 48 vs 24075
(045ndash127)103 vs 81
114 (068ndash189)
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
Bev bevacizumab pani panitumumab Adjusted for BRAF status prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided subgroup of PRIME
NO APPARENT SIDE INTERACTION IN SECOND LINE
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20
Pro
gre
ssio
n-f
ree
Pro
ba
blil
ity
HR = 085 (95 CI 068 106)
Log-rank p-value = 014
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
162 238 (68) 50 (38 - 56)
FOLFIRI 161 248 (65) 49 (36 - 56)
00
01
02
03
04
05
06
07
08
09
10
Months
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Su
rv iva
l P
rob
ab
ility
Eventsn ()
Median (95 CI) months
Panitumumab + FOLFIRI
181 238 (76) 118 (104 - 133)
FOLFIRI 193 248 (78) 111 (103 - 124)
HR = 094 (95 CI 076 115)
Log-rank p-value = 055
PFS OS
No Benefit or Detrimental Effect in Patients with KRAS Mutant Tumors
Peeters M et al Eur J Cancer 20097(3S)14LBA oral presentation
Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Panitumumab
+ FOLFIRI
(n = 297)
FOLFIRI
(n = 285)
Objective response rate (95 CI)
35(30 ndash 41)
10(7 ndash 14)
Complete response 0 0
Partial response 35 10
Stable disease 39 55
Progressive disease 18 26
All responses were confirmed no earlier than 28 days after the
response criteria were first met
WT KRAS Objective Response (Central Review)
Peeters M et al ASCO-GI 2010 282 oral presentation
1For wt KRAS subset p lt 0001(descriptive) exact test of odds ratio stratified by randomization factors
Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Radiological Response By Tumor Side
Trial(line)
Treatments Tumor location Patients n ORR
Phase III PRIME(1st line)12
Pani + FOLFOX4 vs FOLFOX4
Left 156 vs 148 703 vs 548
Right 26 vs 32 520 vs 412
Phase II PEAK (1st line)3
Pani + mFOLFOX6 vs bev + mFOLFOX6
Left 52 vs 53 635 vs 585
Right 13 vs 13 692 vs 462
Phase III Study181 (2nd line)4
Pani + FOLFIRI vs FOLFIRI
Left 143 vs 144 507 vs 135
Right 22 vs 26 190 vs 38
1 Peeters M et al Oral presentation at ESMO 20162 Boeckx C et al ESMO 2016 (Abstract No 89P)
3 Rivera F et al ECC 2015 (Abstract No 2014)4 Peeters M et al Clin Cancer Res 2015215469ndash5479
PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

PICCOLO TRIAL
WT
mut
OS
OS
PFS
PFS
Seymour et alLancetOncology2013 14 749-759
CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

CetuximabEPIC TRIAL
bull within 6 months of the last-dose of
bull first-line fluoropyrimidine and oxaliplatin treatment for metastatic disease was required
bull Previous irinotecan or anti-EGFR therapies were excluded
bull prior bevacizumab was allowed
bull NO KRAS SELECTION OR ANALYSIS
bull NO TUMOR SIDE ANALYSIS
PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

PR
OP
OR
TIO
N P
RO
GR
ES
SIO
N F
RE
E
MONTHS
00
02
04
06
08
10
0 3 6 9 12 15 18
40 mo
26 mo
HR = 069
p lt 00001
ERBITUX in pretreated mCRC EPIC Progression free survival amp response rate
4
46
16
61
0
10
20
30
40
50
60
70
Response rate Disease Control
()
Irinotecan (N=650) ERBITUX + irinotecan (N=648)
Response Rate
Sobrero et al AACR 2007
p lt 00001
p lt 00001
PFS
PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

PR
OP
OR
TIO
N A
LIV
EHR = 0975
p = 0712
ERBITUX + IRINOTECAN N = 648
Median OS = 107 mo
IRINOTECAN N = 650
Median OS = 100 mo
00
01
02
03
04
05
06
07
08
09
10
0 3 6 9 12 15 18 21 24 27 30 33 36
ERBITUX in pretreated mCRC EPIC Overall Survival
MONTHS
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Recommendation 20 Second-line combinations with targeted agents
Patients who are bevacizumab naiumlve should be considered for treatment with an antiangiogenic (bevacizumab or aflibercept) second-line [I A] The use of aflibercept should be restricted to combination with FOLFIRI for patients progressing on an oxaliplatin-containing regimen [I A]
Patients who received bevacizumab first-line should be considered for treatment with
bull Bevacizumab post-continuation strategy [I A]
bull Aflibercept or ramucirumab (in combination with FOLFIRI) when treated in first line with oxaliplatin [I A]
bull EGFR antibodies in combination with FOLFIRIirinotecan for patients with RAS wild-type (BRAF wild-type) disease
bull Relative benefit of EGFR antibodies is similar in later lines compared with second-line [II A]
Patients who are fast progressors on first-line bevacizumab-containing regimens should be considered for treatment with aflibercept or ramucirumab (only in combination with FOLFIRI) [II B] and - in the case of patients with RAS wild-type disease and no pre-treatment with anti-EGFR therapy - EGFR antibody therapy preferably in combination with chemotherapy [II B]
Van Cutsem E Cervantes A Arnold D et al ESMO Consensus 2016
Online Ann Oncol July 2016
Treatment of metastatic disease
ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

ldquoSPECTAColor Platform for Molecular Analysisrdquo
Results with Potential Implications for Novel Therapeutic Approaches
Genetic Alteration Prevalence Potential TreatmentRASRAF mutation
co-present
Multi-gene sequencing
BRCA12 mutation 10457 (22) PARP inhibitor 510 (50)
TSC12 mutation 6457 (13) mTOR inhibitor 46 (67)
IDH12 mutation 4457 (09) IDH inhibitor 34 (75)
ERBB2 (HER2) amplification 4146 (27) HER2 MAb 04 (0)
FGFR12 amplification 4146 (27) FGFR inhibitor 24 (50)
Gene fusion (2x ROS2 1x ALK) 3251 (12) ROS1 inhibitor 13 (33)
PCR QC amp IHC MMR
RAS 55 NO EGFR inhibitor 0BRAF 5 EGFR + BRAF inhibitor 0
MSI3 PD1 inhibitor (50)
328-Gene Panel in the First 457 Tumor Samples (440 patients)
Sanger 14G UK Lab Analysis Dresden Molecular Pathology Lab
Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Microsatellites
bull Microsatellites are repeats of 1 to 10 nucleotides variable in length (from 5 to 50 repeats)
bull A A A A A A A -gt 7 poly-A microsatellite
bull GT GT GT GT -gt 4 poly-GT microsatellite
bull ACGTCC-ACGTCC-ACGTCC -gt 3 poly ACGTCC
bull Localized in coding or non-coding regions of DNA
Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Biologic importance of microsatellites
bull Microsatellites cause DNA polymerase slips in the replicative fork causing DNA mismatches and ultimately protein mutations
bull Zones of accumulations of mutations
bull Commonly frame shifts
Vilar E Nat Clin Oncol 2010
DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

DNA mismatch repair system
bull Evolution endowed eukaryotic cells with a dedicated system to repair mismatches in DNA
The loss of mismatch repairsystem causes mutationsand ultimately cancer
Vilar E Nat Clin Oncol 2010
n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

n = 13
n = 9CACACACACACACACACACACACACA
CACACACACACACACACA
N T TN
MSI phenotype
TN
Normal
TN
LOH
MSI
MSI
Microsatellite Loci
Microsatellite instability
Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Therapeutic implications of MSI status
bull The higher mutational tumor load the higher immune activation and T lymphocyte infiltrates
Dung T lee ASCO 2015
MSI tumor
MSS tumor
Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Therapeutic implications of MSI statusbull MSI tumors have significant high mutation tumor load amp
mutation ldquoof qualityrdquo
Chen DS amp Mellman I Immunity 2013
Giannakis M ASCO 2015MSI tumors haverdquo high qualityrdquo mutationsrdquoStadler Z JCO 2016
Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Clinical data of MSI tumor and immunotherapy
bull Pembrolizumab in MSI-H tumors
Dung T lee NEJM 2015
Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Overman M ASCO 2016
Clinical data of MSI tumor and immunotherapy
bull NIVOLUMAB in MSI-H CRC
Report ORR
Pembro ASCO 2015 60
Pembro NEJM 2015
40
NivoASCO 2016
27
Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Immunotherapy in unselected CRC population
Drug ORR
Nivolumab 0
Pembrolizumab 0
Atezolizumab 0
Topalian NEJM 2012
Patnaik Clin Can Res 2015
Herbst R ASCO 2013
Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Next steps in CRC immune-therapies
bull Increase the benefit from immunotherapy (fight resistance or adaptation)
bull Increase the of patients that benefit from immunotherapy
MSS
MSIH
Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Overman ASCO 2016
Future directions
bull Nivolumab plus Ipilimumab in MSI-H CRC
POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

POLE EDM TCGA
ICO LrsquoHospitalet
Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Adapted from Becht E et al Oncoimmunology 2015
Immune vs Transcriptomic subtypes of CRC
Supervised immune infiltration analysis
Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Redefining mCRC
The Consensus
Molecular Subtypes Perspective CONSENSUS SUBTYPES
Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Proposed taxonomy of colorectal cancer
Inmune checkpointsblockade +
BEVACIZUMAB
TGF-
inhibition+ Inmune
checkpointblockade
Prognosis
Drugresponse
prediction
Metabolismamp
DNA damage
Oncogenedrivers
Amplifications
(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

(almost all) molecular subtypes of CRC have MEK over-activation
Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Biomarkers CD8 T-cell Accumulation and MHC I Expression
Presented By Johanna Bendell at 2016 ASCO Annual Meeting
MEK activation lead to decrease on MHC-1
expression and therefore impairs antigen
presentation (2)
FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

FUTURE DIRECTIONS
Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov

Examples of anti-PDL1PD1 therapies currently under investigation in CRC
Target Therapy Phase Trial Design Trial ID
Anti-PDL1
Atezolizumab (engineered IgG1
no ADCC)
I Solid tumours NCT01375842
Ib Solid tumours (+ bevacizumab plusmn FOLFOX) NCT01633970
II mCRC (+ bevacizumab + fluoropyrimidine) NCT02291289
MEDI4736(modified IgG1
no ADCC)II mCRC NCT02227667
Anti-PD1
Nivolumab(IgG4)
III mCRC (plusmn ipilimumab) (CheckMate 142) NCT02060188
III Solid tumours (+INCB24360) NCT02327078
III Solid tumours (+ chemotherapy) NCT02423954
III Solid tumours (+ varlilumab) NCT02335918
Pembrolizumab(IgG4 humanised)
I Solid tumours (+ aflibercept) NCT02298959
III GI cancers (+mFOLFOX6) NCT02268825
III WT mCRC (+ cetuximab) NCT02318901
II mCRC (+ radiotherapy or ablation) NCT02437071
II mCRC (+ chemotherapy) NCT02375672
II mCRC (+ azacitidine andor romidepsin) NCT02512172
II MSI-positive-negative CRC NCT01876511
bull Recruiting studies bull Clinicaltrialsgov