radiotherapy and skin reaction
TRANSCRIPT

Effect of Ionizing Radiation on Skin The Good, the Bad, and the Ugly
BOG July 2015
Dr. Lokesh Viswanath M.D.Professor & Head of Unit
Department of Radiation OncologyKidwai Memorial Institute of Oncology

Radiation Induced skin reactions
• Domains
Radiation Induced Skin
Reactions
During Radiation Therapy : Acute Effects and Late
effects
Accidental exposures : Industrial/ wartime
Nuclear exposures /
Open isotopes
Radiation Workers /
Public exposure monitoring
Introduction : Radiation induced skin toxicities
• ~ 95% of patients receiving RT for cancer• negatively affect the quality of a patient's life : pain
and premature interruption of RT• ranges in severity from mild erythema to moist
desquamation and ulceration.• ionizing radiation damage is somewhat similar to
atopic dermatitis• a common form of eczema• ~20% of children• profound effect on the stratum corneum function• increased transepidermal water loss

History• Skin burn attributed to radiation : 1901
• Skin erythema : Holzkencht`s chromoradiometer 1902

Radiation skin injury
• morphological • functional changes
• The degree of radiation injury »– Total radiation dose, Dose /Fr– proportion of body irradiated– volume of tissues irradiated– time interval of the radiation dose received
(Fr/week, No of Day, OTT)

most radiosensitive cells in the body
– high proliferative index– Tissue oxygen
• The most radiosensitive organ systems are :-– bone marrow– reproductive and gastrointestinal systems– Skin ←– Muscle– Brain– etc
function of skin• effective barrier against the surrounding environment
– Physical– immunological
• The epidermis – stratifying layers of keratinocytes– primary barrier and biosensor
• The dermis– provide structural strength – connective tissue produced by dermal fibroblasts.

Skin is susceptible to radiation damage • continuously renewing organ • rapidly proliferating and maturing cells• highly radiosensitive
– basal keratinocytes– hair follicle stem cells– melanocytes
• Radiation skin injury– immediate damage to basal keratinocytes and hair follicle stem cells– Inflammation– 1st keratinocytes
• disruption in the self-renewing property of the epidermis• repeated exposures do not allow time for cells to repair tissue or DNA
damage.• continually destroyed with each fraction

Radiation skin injury: categorized
• Acute injury : within hours to weeks
• late injury (i.e., chronic) : months to years after radiation exposure

Acute radiation skin toxicty• primarily involves cellular alterations and inflammation in the epidermis and
the dermis. Acute changes1. Erythema2. Edema3. pigment changes4. Depilation
histological analysis: • Hyper-proliferation of the epidermis• thickening of the stratum corneum• Trans-epidermal water loss – Significantly increased (a measure for skin
barrier integrity)• Severe radiation injury
– complete loss of the epidermis– persistent fibrinous exudates – edema. – Re-epithelialization begins within 10–14 days after radiation exposure in the absence
of infection
one year after radiation exposure• skin
– thin– Hypo-vascularized– Tight – susceptible to trauma or infection
• Chronic radiation skin injury– delayed wound healing – delayed ulcers– Fibrosis– telangiectasias
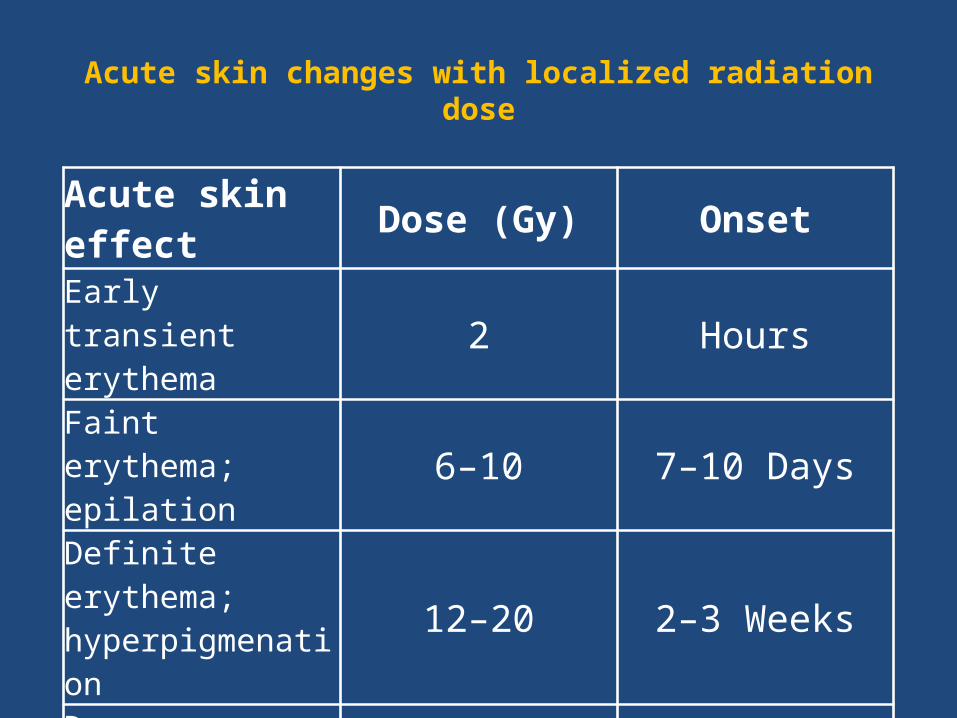
Acute skin changes with localized radiation dose
Acute skin effect Dose (Gy) OnsetEarly transient erythema 2 HoursFaint erythema; epilation 6–10 7–10 Days
Definite erythema; hyperpigmenation 12–20 2–3 Weeks
Dry desquamation 20–25 3–4 WeeksMoist desquamation 30–40 4 WeeksUlceration >40 6 Weeks

Threshold doses

PathophysiologyRT Skin Injury is different for thermal burn1. dose-dependent clinical pattern, which includes dry
desquamation at 12–20 Gy, moist desquamation at 20 Gy, and necrosis at >35 Gy
2. radiation Skin injury are associated with opiate-resistant chronic pain
1. most complicating factor is the unpredictable successive inflammatory waves occurring weeks to years after radiation exposure
2. difficult to delineate the radiation-injured tissue from noninjured tissue
3. healing of radiation skin lesion is extensive and unpredictable.

Risk factors• patient-related factors :
– obesity, age, gender, chronic sun exposure, and smoking– Older female patients– ataxia telangiectasia and hereditary nevoid basal cell
carcinoma syndrome (Gorlin Syndrome) require dose alterations or avoidance of radiation exposure
• AT = mutations in the ATM gene, are highly susceptible to severe radiation dermatitis
• GS: irradiation of individuals could produce widespread cutaneous tumors.
• Other disorders : – connective tissue disorders (lupus, scleroderma), chromosomal
breakage syndromes (Fanconi's anemia, Bloom syndrome), xeroderma pigmentosa, Gardner's syndrome, hereditary malignant melanoma, and dysplastic nevus syndrome

Risk Factor 2• Technical factors :
– radiation dose to skin – irradiation site :
• most sensitive - anterior of the neck, extremities, chest, abdomen, and face , hair follicles on the scalp and breast tissue
– fractionation timing– total exposure time– angle of radiation beam
• Other risk factors– increased transepidermal water loss – infiltration of pathogens or bacteria into the skin– Host antimicrobial defenses are severely compromised by
radiation and/or skin trauma combined with radiation

Late skin effect
Dose (Gy) Onset
Delayed ulceration >45 Weeks after
radiation
Dermal necrosis/atrophy >45 Months after
radiation
Fibrosis >45 6 Months to 1 year after radiation
Telangiectasia >45 6 Months to 1 year after radiation
Skin immune response following radiation
• skin provides : immune surveillance > maintains homeostasis and is poised to respond to environmental insults. – Key cells : Langerhans cells (LCs)– keratinocytes : important role because : producing large
amounts of cytokines, * IL-1α and tumor necrosis factor-α• The LCs + dermal dendritic cells (DCs) = antigen-
presenting cells – uptake of antigens that may breach the skin barrier
• The dermis : mast cells & T cells :> radiation-induced immune response
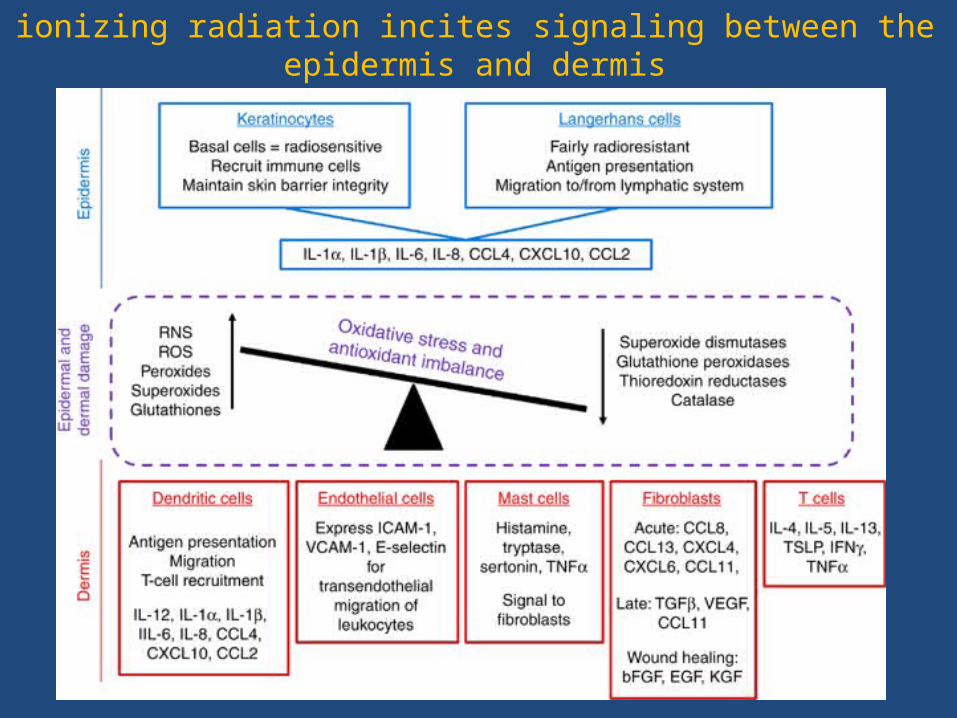
ionizing radiation incites signaling between the epidermis and dermis
• Keratinocytes, fibroblasts, and endothelial cells in the skin stimulate resident (i.e., LCs, DCs, mast cells, T cells) and circulating immune cells
• Numerous cytokines and chemokines are produced in response to these activation signals, which act on the endothelial cells of local vessels, causing the upregulation of adhesion molecules
• Transendothelial migration of immune cells, such as neutrophils, macrophages, and leukocytes, from circulation to irradiated skin is considered a “hallmark” of radiation-induced skin injury
• Acute radiation skin toxicity has been correlated with increased formation of various cytokines and chemokines, most notably IL-1α, IL-1β, tumor necrosis factor-α, IL-6, IL-8, CCL4, CXCL10, and CCL2
late-radiation injury
• fibroblasts - fibrosis and other• key mediators
• Transforming growth factor-β (TGFβ)• Smad3• vascular endothelial growth factor• CCL11 (eotaxin)

acute radiation skin injury scoring systemsScore ObservationRadiation Therapy Oncology Group 0 No change over baseline 1 Erythema; dry desquamation; epilation 2 Bright erythema; moist desquamation; edema 3 Confluent moist desquamation; pitting edema 4 Ulceration, hemorrhage, necrosis NIH CTCAE 0 None 1 Faint erythema or dry desquamation 2 Moderate to brisk erythema 3 Confluent moist desquamation 4 Skin necrosis or ulceration Oncology Nursing Society 0 No change 1.0 Faint or dull erythema 1.5 Bright erythema 2.0 Dry desquamation with or without erythema
2.5 Small to moderate amount of moist desquamation
3.0 Confluent moist desquamation 3.5 Ulceration, hemorrhage, or necrosis

Score ObservationDouglas & Fowler 0 Normal 0.25 50/50, Doubtful if any difference from normal 0.5 Very slight reddening 0.75 Definite but slight reddening 1 Severe reddening 1.25 Severe reddening with white scale; “papery” appearance of skin 1.5 Moist breakdown in one very small area with scaly or crusty appearance 1.75 Moist desquamation in more than one small area 2 Moist desquamation in 25% of irradiated area 2.25 Moist desquamtion in 33% of irradiated area 2.5 Moist desquamation in 50% of irradiated area 2.75 Moist desquamation in 66% of irradiated area 3 Moist desquamation in most of irradiated area 3.25 Moist desquamation in most of irradiated area with slight moist exudate 3.5 Moist desquamation in most of irradiated area with moist exudates; necrosis Radiation dermatitis severity scale 0.0 Normal or none 0.5 Patchy faint/slight follicular eyrthema; faint hyperpigmentation 1.0 Faint and diffuse erythema; diffuse hyperpigmentation; mild epilation 1.5 Definite erythema; extreme darkening/hyperpigmentation 2.0 Definite erythema/hyperpigmentation with fine dry desquamation; mild edema 2.5 Definite erythema/hyperpigmentation with branny/scaly desquamation 3.0 Deep red erythema with diffuse dry desquamation; peeling in sheets
3.5 Violaceous erythema with early moist desquamation; peeling in sheets; patchy crusting
4.0 Violaceous erythema with diffuse moist desquamation; patchy crusting; ulceration; necrosis

Radiation Therapy Oncology Group : Late Skin Toxicity Scoring
Onset Grade0 1 2 3 4 5
Chronic None Slight atrophy.
Patch atrophy. Moderate telangiectasia. Total hair loss.
Marked atrophy. Gross telangiectasia.
Ucleration Death

management of radiation skin injury
Conservative
Medical LineSurgical

management of radiation skin injury • washing with mild soap (open isotopes)• using unscented, lanolin-free, water-based moisturizing cream,• corticosteroid and nonsteroidal creams appeared to reduce
the severity of skin reactions, there was no clear indication of a preferred topical agent.
• Amifostine and oral enzymes emerged as somewhat effective preventative agents
• pentoxifylline reduced late, but not acute, effects of radiation on the skin
• Long treatment (3 years) of pentoxifylline and tocopherol (i.e., vitamin E) significantly reduced radiation-induced fibrosis. – Unfortunately, cessation of pentoxifylline–tocopherol treatment
before 3 years resulted in a “rebound effect” and more severe radiation-induced fibrosis

radiation mitigators • Targeted gene therapy• potential targets:
– TGFβ1 pathway inhibitor synthetic superoxide dismutase– catalase mimetics recombinant IL-12 toll-like receptor– 5 agonist inhibitors of cyclin-dependent kinases
• pravastatin reduced radiation skin injury by maintaining endothelial cell function after radiation exposure by increasing endothelial nitric oxide synthase
• Curcumin, a component of turmeric, has also demonstrated the ability to reduce radiation skin toxicity through its potent antioxidant and anti-inflammatory activities
• acceleration of radiation delayed wound healing in mice upon stimulation of TGFβ-1 and basic fibroblast growth factor, suggesting that the growth factor treatment may mitigate radiation skin injury.
• Stem cell therapy combined with surgical excision has demonstrated success in improving wound repair of severe radiation
• mesenchymal stem cell injections around the lesion at the cutaneous and muscular levels, as well as in the bed of the lesion under the skin graft
• adipose tissue–derived stem cells also promote wound healing in mice

Grade 1

Grade 2

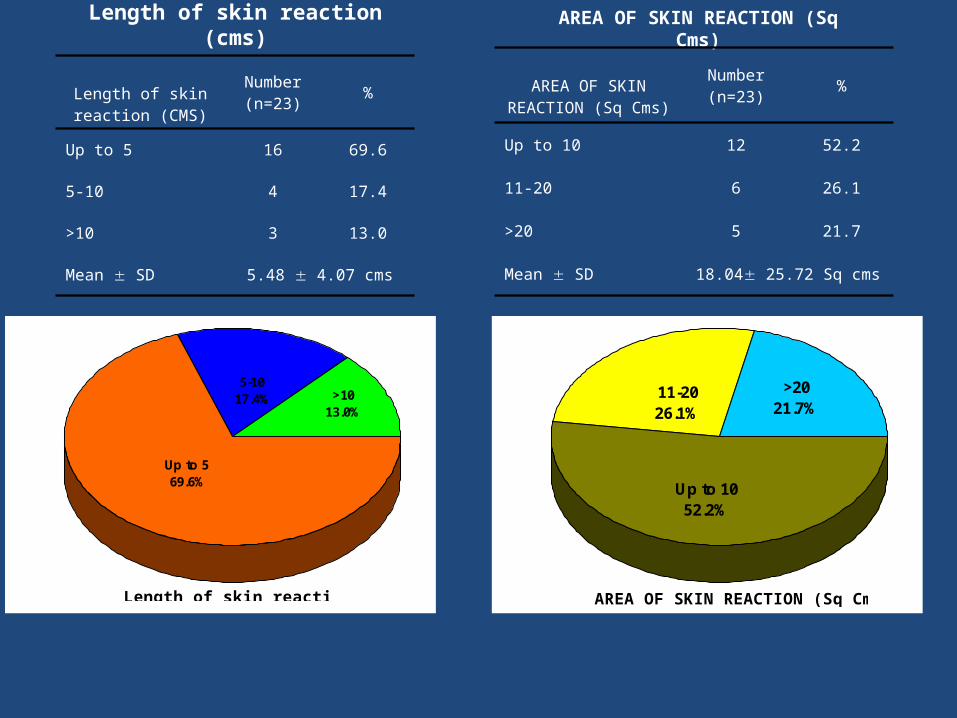
Length of skin reaction (cms)
Length of skin reaction (CMS)
Number(n=23)
%
Up to 5 16 69.6
5-10 4 17.4
>10 3 13.0
Mean SD 5.48 4.07 cms
Up to 569.6%
5-1017.4% >10
13.0%
Length of skin reaction (CMS)
AREA OF SKIN REACTION (Sq Cms)
AREA OF SKIN REACTION (Sq Cms)
Number(n=23)
%
Up to 10 12 52.2
11-20 6 26.1
>20 5 21.7
Mean SD 18.04 25.72 Sq cms
11-2026.1%
>2021.7%
Up to 1052.2%
AREA OF SKIN REACTION (Sq Cms)


Filgastrim Treatment ProtocolStep 1: Aseptic precautions were taken during the procedure – injection of a single
dose of 300 μg of Filgrastim was administered, subcutaneously in the unirradiated normal skin around the periphery of the moist desquamation (2 or 4 quadrant zones).
Step 2: Proper wound care was advised – air drying and rest to the part of the body that is affected for 2 to 3 days, mainly to prevent skin fold from rubbing against the exposed skin and aggravating the lesion and to clothes from sticking to the exposed skin wound.
Step 3: Sprinkling of Neosporin® – antibiotic powder (contains Neomycin & Polymixin B sulfates & Bacitracin zinc) ever 6 hours was advised (instructions were not to touch the exposed skin with cotton swab or apply ointments).
Step 4: Appropriate oral antibiotics (such as Amoxicillin & Cloxacillin for 7 days or Ciprofloxacilllin with or without Tinidazole) when necessary were given to patients
Step 5: Analgesic & anti inflammatory drugs: oral Ibuprofen if subject is symptomatic for 1–2 days.
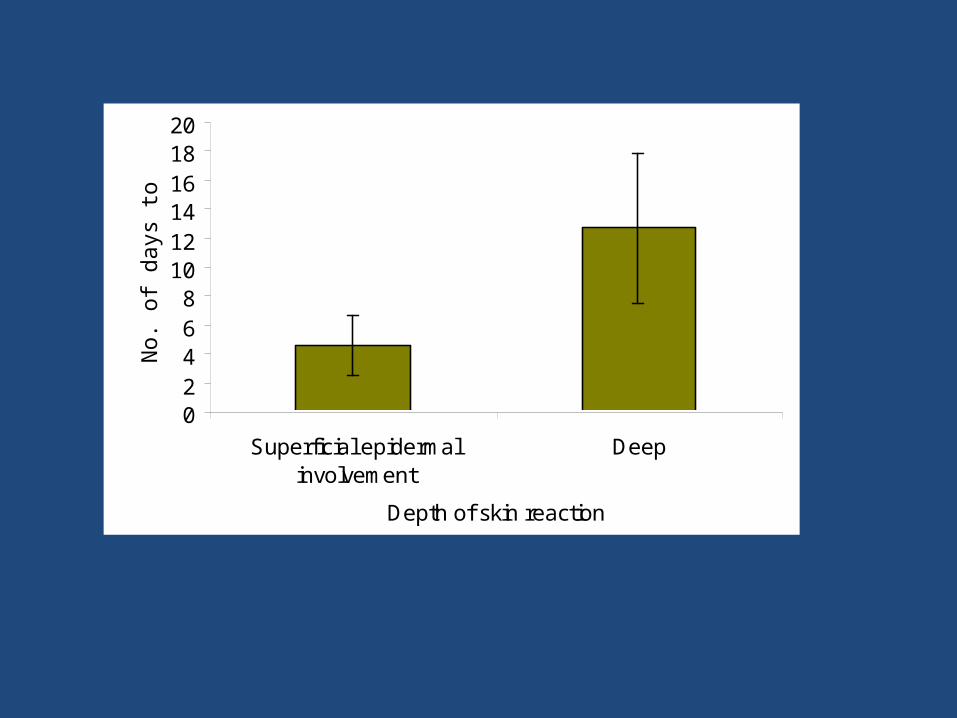
02468
101214161820
Superficial epidermalinvolvement
Deep
Depth of skin reaction
No
. o
f d
ays
to
he
al.

Number of Days required to Heal
No of Days required to Heal
Superficial epidermal
involvementDeep Total
Up to 5 days 13 (76.5%) - 13(56.5%)
5-10 days 4 (23.5%) 3 (50.0%) 7 (30.4%)
>10 days - 3 (50.0%) 3 (13.0%)
Total 17 6 23
Mean SD(Min-max)
4.53 2.07(2-9)
12.66 5.12(7-20)
6.65 4.73(2-20)
76.5
0
23.5
50
0
50
05
101520253035404550556065707580
Per
cen
tag
es
Up to 5 days 5-10 days >10 days
Sup.epdermal invol.
Deep
Number of days required to heal

Time to heal (Literature Review)Time (days) Mean Authors
Duo Derm 4-6 4.6 Margolin et al 1990
G V paint 5 - 22 11
Hydrocortisone Cream
21 - 28 Chen et al 1997
Gel Dressing 7 - 14
N. Saline 30 - 35
Dermofilm dressing
11 - 16 See et al 1998
Inj GCSF s/c 2-20 6.65 Lokesh .V et al 2006
superficial 2-9 4.53
deep 7-20 12.66


Female patient who completed 50Gy in 25 fractions radiotherapy for a Breast Cancer presented with grade III moist dequmation in the Axillary fold (Superficial dermal
exposure) (1a). The patient was referred to us for cytokine therapy. The skin ulceration healed in the next 4 days after GCSF injection (1b).


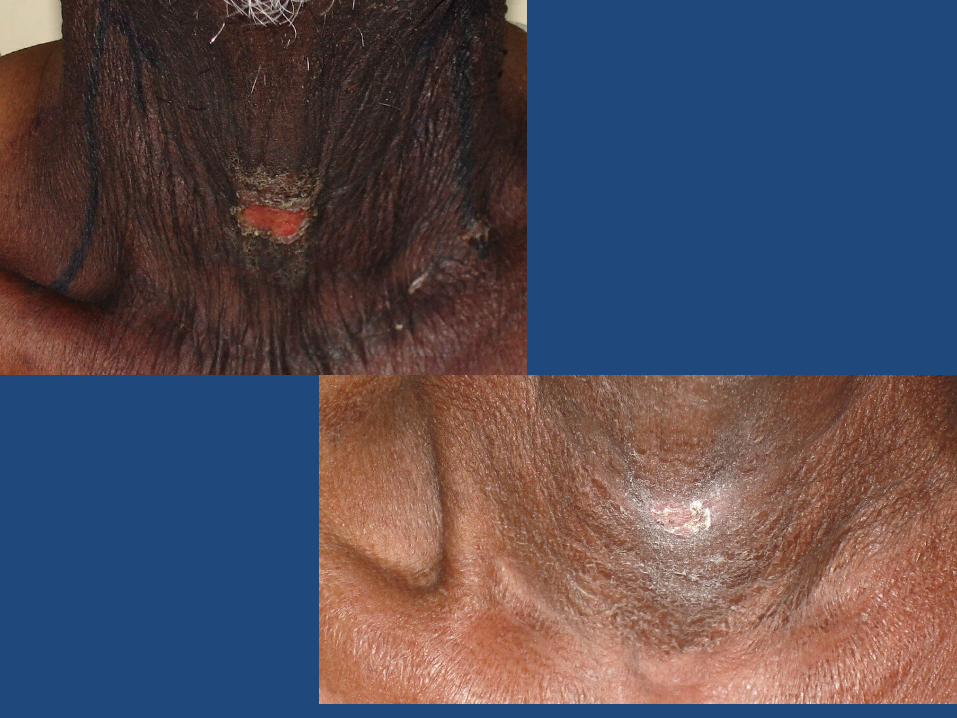
• shows a 55year male who completed treatment with external radiotherapy 5000cG in 25 fractions on Telcobalt Machine for a head and neck malignancy developed grade 3 moist desquamation of the skin (Deep skin lesions). The picture shows an unresolved desquamation in spite of gentian violet application.
• same patient with remarkable resolution of lesion by day 5. He was able to reassume treatment within a week


a Female patient who completed radiotherapy 50Gy in 25 fractions 5 fractions per week, for Cancer Cervix. She presented with grade III moist desquamation of the skin with deep dermal exposure. The patient was referred to us for cytokine therapy. Picture 2 a - Before cytokine
injection, Picture 2 b - day 2, Picture 2 c – day3 , Picture 2 d – day4, Picture 2 e – day 5 Shows Complete healing.

Summary• there is no effective treatment to prevent or mitigate radiation
skin injury. Simple solutions to prevent: • No touch policy• Megavoltage X Rays for RT• Advanced Radiation techniqes : IMRT , Rotational Modulated Arcs
etc• Use of multiple beams• careful RT contouring & planning• use of higher energies in obese patients• Protons• Amifostine