qt prolongation and torsades de pointes in patients infected with human immunodeficiency virus and...
TRANSCRIPT
DW. KCNJ2 mutation results in Andersen syndrome with sex-specific cardiacand skeletal muscle phenotypes. Am J Hum Genet 2002;71:663–668.14. Tristani-Firouzi M, Jensen JL, Donaldson MR, Sansone V, Meola G, Hahn A,Bendahhou S, Kwiecinski H, Fidzianska A, Plaster NM, et al. Functional andclinical characterization of KCNJ2 mutations associated with LQT7 (Andersensyndrome). J Clin Invest 2002;110:381–388.15. Splawski I, Shen J, Timothy KW, Lehmann MH, Priori S, Robinson JL, MossAJ, Schwartz PJ, Towbin JA, Vincent GM, Keating MT. Spectrum of mutationsin long-QT syndrome genes. KVLQT1, HERG, SCN5A, KCNE1, and KCNE2.Circulation 2000;102:1178–1185.16. Benson DW, Silberbach GM, Kavanaugh-McHugh A, Cottrill C, Zhang Y,Riggs S, Smalls O, Johnson MC, Watson MS, Seidman JG, et al. Mutations inNKX2.5, a cardiac transcription factor, affect diverse cardiac developmentalpathways. J Clin Invest 1999;104:1567–1573.
17. Yang T, Snyders DJ, Roden DM. Drug block of IKr: model systemsand relevance to human arrhythmias. J Cardiovasc Pharmacol 2001;38:737–44.18. Larsen LA, Andersen PS, Kanters J, Svendsen IH, Jacobsen JR, Vuust J,Wettrell G, Tranebjaeg L, Bathen J, Christiansen M. Screening for mutations andpolymorphism in the genes KCNH2 and KCNE2 encoding the cardiac HERG/MiRP1 ion channel: implications for acquired and congenital long QT syndrome.Clin Chem 2001;47:1390–1395.19. Berthet M, Denjoy I, Donger C, Demay L, Hammoude H, Klug D, Schulze-Bahr E, Richard P, Funke H, Schwartz K, et al. C-terminal HERG mutations: therole of hypokalemia and a KCNQ1-associated mutation in cardiac event occur-rence. Circulation 1999;99:1464–1470.20. Priori SG, Napolitano C, Schwartz PJ. Low penetrance in the long-QTsyndrome: clinical impact. Circulation 1999;99:529–533.
QT Prolongation and Torsades de Pointes in PatientsInfected With Human Immunodeficiency Virus and
Treated With Methadone
Merce Gil, MD, Montserrat Sala, MD, Ignasi Anguera, MD, Olga Chapinal, MD,Manuel Cervantes, MD, Joan R. Guma, MD, and Ferran Segura, MD
Four patients infected with human immunodeficiencyvirus receiving antiretroviral treatment and highdoses of methadone (>200 mg/day) presented withseveral syncopal episodes. A significant prolongationof the QTc interval was detected in all of them, and in3 patients, >1 episode of Torsades de Pointes wasrecorded. The sequence of events in these cases sug-gests that high doses of methadone caused QT pro-longation and provided the substrate for syncope andTorsades de Pointes. �2003 by Excerpta Medica,Inc.
(Am J Cardiol 2003;92:995–997)
The introduction of highly active antiretroviral ther-apy for the treatment of human immunodeficiency
virus (HIV) infection has increased drug interactionsdue to the induction and/or inhibition of cytochromeP450. Pharmacokinetic interactions between metha-done and antiretroviral drugs (zidovudine, didanosine,stavudine, abacavir, nevirapine, efavirenz, nelfinavir,and amprenavir) have been documented. In clinicalpractice, the dose of methadone has to be increasedafter symptoms of abstinence if given together withnon-nucleoside analogous inverse transcriptase inhib-itors (efavirenz or nevirapine). There is experimentalevidence of the effects of methadone on heart functionin animal models, but evidences of the associationbetween the use of methadone in humans and thepresence of QT-interval prolongation or ventriculararrhythmias are virtually non-existent. We describe
the clinical cases of 4 patients infected with HIVreceiving antiretroviral treatment and high doses ofmethadone (�200 mg/day) who presented with sev-eral episodes of syncope. In all of them, a significantprolongation of the QTc interval (�0,45 seconds) wasdetected, and in 3 patients, �1 episode of Torsades dePointes (TdP) was recorded (Table 1).
• • •In this report, we describe the clinical association
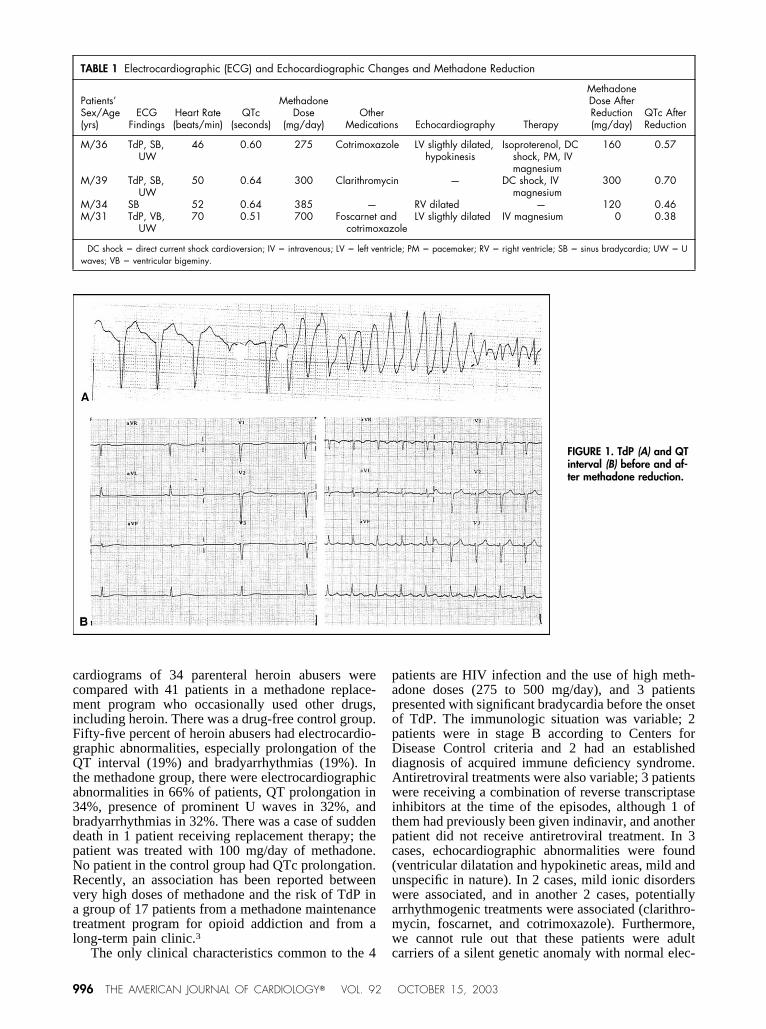
of 4 patients infected with HIV receiving antiretroviraltreatment who presented several syncopal episodeswhile receiving high doses of methadone (�200 mg/day). In all patients, a significant prolongation of theQTc interval was detected, and in 3 of them, �1episode of TdP was recorded (Figure 1).
High methadone doses have been found to affectheart function in experimental studies of guinea pigheart cell preparations.1 Methadone potentiates theinotropic cardiac response to sympathetic nerve stim-ulation in a dose-dependent manner; this effect isantagonized by an increase in extracellular calciumconcentration. Methadone also enhances the dose-in-otropic response curve of exogenous norepinephrine.The cardiac response to parasympathetic stimulationwas antagonized by the drug through a postsynapticeffect; the responses to histamine and isoprenalinewere also antagonized in a noncompetitive way. Inisolated sheep Purkinje fibers, methadone at concen-trations of 10 �M and higher significantly affectstransmembrane action potential parameters by chieflydecreasing the maximum rate of depolarization andincreasing the action potential duration. High concen-trations of methadone can affect several parameters ofcardiac function through an unspecific mechanism dif-ferent from the stimulation of opiate receptors, and allthese effects may account for a prolongation of the QTinterval.
There is little evidence on the effect of methadoneon the human heart. In a previous study,2 the electro-
From the Internal Medicine Department, Infectious Diseases Unit andCardiology Department, Corporacio Sanitaria Parc Taulı-Hospital deSabadell; and CAS de Drogodependencies de Sabadell, Barcelona,Spain. Dr. Anguera’s address is: Cardiology Department, Hospital deSabadell, Institut Universitari Parc Taulı-UAB, Parc Taulı s/n, 08208Sabadell (Barcelona), Spain. E-mail: [email protected]. Manuscriptreceived February 6, 2003; revised manuscript received and ac-cepted June 16, 2003.
995©2003 by Excerpta Medica, Inc. All rights reserved. 0002-9149/03/$–see front matterThe American Journal of Cardiology Vol. 92 October 15, 2003 doi:10.1016/S0002-9149(03)00906-8
cardiograms of 34 parenteral heroin abusers werecompared with 41 patients in a methadone replace-ment program who occasionally used other drugs,including heroin. There was a drug-free control group.Fifty-five percent of heroin abusers had electrocardio-graphic abnormalities, especially prolongation of theQT interval (19%) and bradyarrhythmias (19%). Inthe methadone group, there were electrocardiographicabnormalities in 66% of patients, QT prolongation in34%, presence of prominent U waves in 32%, andbradyarrhythmias in 32%. There was a case of suddendeath in 1 patient receiving replacement therapy; thepatient was treated with 100 mg/day of methadone.No patient in the control group had QTc prolongation.Recently, an association has been reported betweenvery high doses of methadone and the risk of TdP ina group of 17 patients from a methadone maintenancetreatment program for opioid addiction and from along-term pain clinic.3
The only clinical characteristics common to the 4
patients are HIV infection and the use of high meth-adone doses (275 to 500 mg/day), and 3 patientspresented with significant bradycardia before the onsetof TdP. The immunologic situation was variable; 2patients were in stage B according to Centers forDisease Control criteria and 2 had an establisheddiagnosis of acquired immune deficiency syndrome.Antiretroviral treatments were also variable; 3 patientswere receiving a combination of reverse transcriptaseinhibitors at the time of the episodes, although 1 ofthem had previously been given indinavir, and anotherpatient did not receive antiretroviral treatment. In 3cases, echocardiographic abnormalities were found(ventricular dilatation and hypokinetic areas, mild andunspecific in nature). In 2 cases, mild ionic disorderswere associated, and in another 2 cases, potentiallyarrhythmogenic treatments were associated (clarithro-mycin, foscarnet, and cotrimoxazole). Furthermore,we cannot rule out that these patients were adultcarriers of a silent genetic anomaly with normal elec-
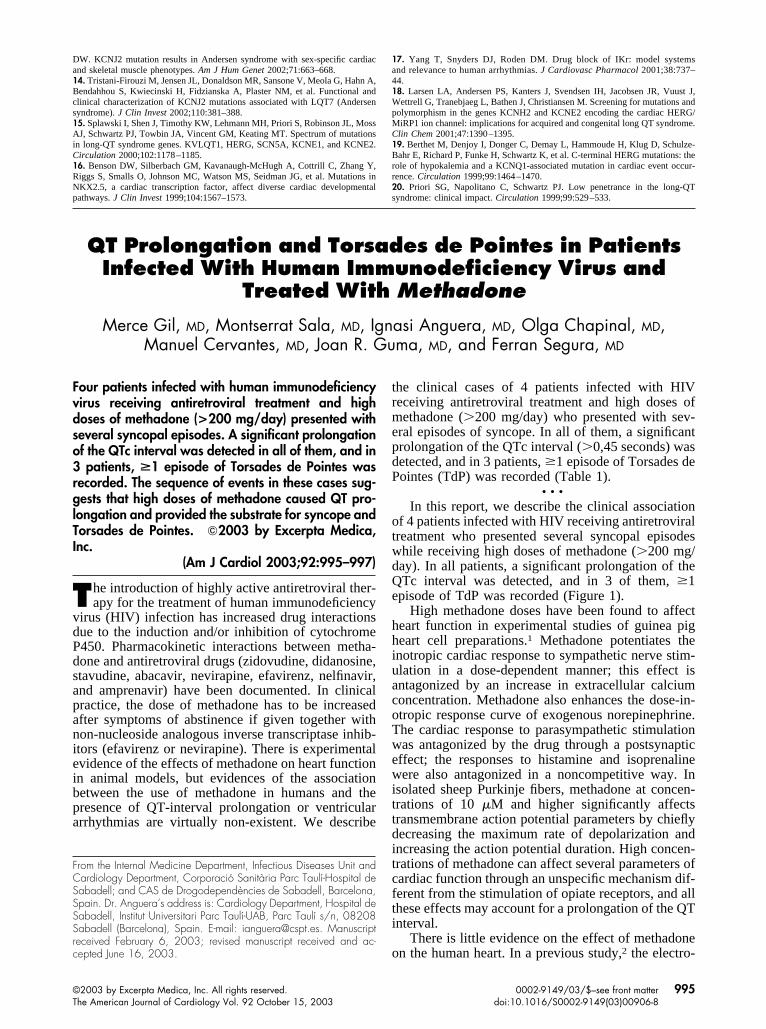
TABLE 1 Electrocardiographic (ECG) and Echocardiographic Changes and Methadone Reduction
Patients’Sex/Age(yrs)
ECGFindings
Heart Rate(beats/min)
QTc(seconds)
MethadoneDose
(mg/day)Other
Medications Echocardiography Therapy
MethadoneDose AfterReduction(mg/day)
QTc AfterReduction
M/36 TdP, SB,UW
46 0.60 275 Cotrimoxazole LV sligthly dilated,hypokinesis
Isoproterenol, DCshock, PM, IVmagnesium
160 0.57
M/39 TdP, SB,UW
50 0.64 300 Clarithromycin — DC shock, IVmagnesium
300 0.70
M/34 SB 52 0.64 385 — RV dilated — 120 0.46M/31 TdP, VB,
UW70 0.51 700 Foscarnet and
cotrimoxazoleLV sligthly dilated IV magnesium 0 0.38
DC shock � direct current shock cardioversion; IV � intravenous; LV � left ventricle; PM � pacemaker; RV � right ventricle; SB � sinus bradycardia; UW � Uwaves; VB � ventricular bigeminy.
FIGURE 1. TdP (A) and QTinterval (B) before and af-ter methadone reduction.
996 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 92 OCTOBER 15, 2003

trocardiographic phenotype, and that the high metha-done doses could have unmasked this hidden geneticmutation, causing the prolongation of the QT interval.Although some nonpharmacologic factors existed inall patients that may potentially prolong the QT inter-val, interestingly, shortening of the QT interval oc-curred when methadone doses were reduced in 2 of 3patients in whom this was possible.
• • •Although a higher prevalence of acquired long QT
has been described in patients infected with HIV,4probably related to viral cardiomyopathies or autono-mous neuropathies,5 QT prolongation in these patientsis also frequently associated with drugs (macrolides,quinolones, clindamycin, trimethoprim/sulfametox-azole, fluconazole, foscarnet, and pentamidine) usedin the treatment of opportunistic or other types ofinfection.6 Currently, no association between long QTand antiretroviral drugs has been described. In patientsinfected with HIV, electrolyte disorders caused orenhanced by the use of some of the previously men-tioned drugs may prolong the QT interval.
In a recent review of drugs that may prolong QT,among the opiate agents, levacetylmethadol (withclinical evidence), methadone, and meperidine (onlyin cell cultures) were mentioned.6 Methadone is a drugthat has experienced a generalization of its use inrecent years for replacement therapy of opioid depen-dence and for long-term pain. Some patients receivingmethadone replacement therapy are also infected withHIV. With the introduction of highly active antiretro-viral therapy, drug interactions have increased due tothe inhibitory and/or inducing effects of cytochromeP450. Among these, the most important is the need toincrease the dose of methadone, substrate of isoform3A of cytochrome P450 (CYP3A), when given incombination with some antiretroviral drugs, especiallynon-nucleoside analogous reverse transcriptase inhib-itors. These drugs are occasionally abandoned withouta parallel decrease of methadone doses by the patient,who may continue to receive high doses of the opiatederivative. Furthermore, although there seems to be areasonable relation in the literature between the given
methadone doses and their plasma levels in long-termtherapies,7 these levels seem to be highly variablewhen the patient is receiving antiretroviral treatment.8
In conclusion, there is experimental evidence sup-porting the possibility that methadone prolongs theQT interval through a dose-dependent mechanism.Methadone given at high doses may be responsible forthe prolongation of the QT interval in humans—withthe subsequent arrhythmogenic risk—probablyboosted by electrolyte disorders, the presence of sinusbradycardia, the probable silent heart involvement dueto HIV infection, and the association with other po-tentially arrhythmogenic drugs. However, furtherstudies are needed to confirm this hypothesis. Thesequence of events in these cases suggests that meth-adone caused QT prolongation and provided the sub-strate for syncope and TdP. This clinical note is in-tended as an alarm in view of the risk of using highmethadone doses, which may not be free of danger.We recommend measurement of the QT interval be-fore the initiation of treatment with methadone and tomonitor the QT interval especially in cases of anincrease in the dosage of methadone.
1. Mantelli L, Corti V, Vini R, Cerbai E, Ledda F. Effect of dl-methadone on theresponse to physiological transmitters and on several functional parameters of theisolated guinea-pig heart. Arch Int Pharmacodyn 1986;282:298–313.2. Lipski J, Stimmel B, Donoso E. The effect of heroin and multiple drug abuseon the electrocardiogram. Am Heart J 1973;86:663–668.3. Krantz MJ, Lewkowiez L, Hays H, Woodroffe MA, Robertson AD, Mehler P.Torsade de Pointes associated with very-high-dose methadone. Ann Intern Med2002;137:501–504.4. Kocheril AG, Bokhari SA, Batsford WP, Sinusas AJ. Long QTc and Torsadesde Pointes in human immunodeficiency virus disease. Pacing Clin Electrophysiol1997;20:2810–2816.5. Villa A, Foresti V, Confalonieri F. Autonomic neutopathy and prolongation ofQT interval in human immunodeficiency virus infection. Clin Auton Res 1995;5:48–52.6. De Ponti F, Poluzzi E. Organising evidence of QT prolongation and occurrenceof Torsades de Pointes with non-antiarrhytmic drugs: a call for consensus. EurJ Clin Pharmacol 2001;57:185–209.7. Verebely K, Volavka J, Mule S, Resnick R. Methadone in man: pharmacoki-netic and excretion studies in acute and chronic treatment. Clin PharmacolTherap 1975;18:180–190.8. Beauverie P, Taburet AM, Desalles MC, Furlan V, Touzeau D. Therapeuticdrug monitoring of methadone in HIV-infected patients receiving protease inhib-itors. AIDS 1998;12:2510–2511.
BRIEF REPORTS 997