q & a. greetings from new orleans & the ochsner clinic
TRANSCRIPT

Q & AQ & A

Greetings from New Orleans
&
The Ochsner Clinic

Restorative Proctocolectomy
“The Pelvic Pouch Procedure in 2004”
The Royal Infirmary Manchester U.K.April 1, 2004
Terry C. Hicks, M.D.Terry C. Hicks, M.D.

GOALS:
IIndicationsndications
TechniqueTechnique
ComplicationsComplications
ControversiesControversies
IIndicationsndications
TechniqueTechnique
ComplicationsComplications
ControversiesControversies

Know the Enemy!Know the Enemy!

Restorative ProctocolectomyThe Disease of Concern
Ulcerative ColitisUlcerative Colitis
Familial adenomatous polyposisFamilial adenomatous polyposis
Crohn’s diseaseCrohn’s disease
Indeterminate ColitisIndeterminate Colitis

Ulcerative Colitis
Ulcerative Colitis is an inflammatory Ulcerative Colitis is an inflammatory disorder. It affects the rectum and disorder. It affects the rectum and extends proximally to affect a variable extends proximally to affect a variable extent of the colon. extent of the colon.
The cause of the disease, and the The cause of the disease, and the factors determining its chronic course factors determining its chronic course are unknown.are unknown.



150 years after the discovery of this 150 years after the discovery of this disease by Samuel Wilkes, the etiology of disease by Samuel Wilkes, the etiology of ulcerative colitis remains unknown. ulcerative colitis remains unknown.
The major hypotheses in 2003 include: The major hypotheses in 2003 include: infection, allergy to dietary components, infection, allergy to dietary components, immune responses to bacterial or self-immune responses to bacterial or self-antigens, and the psychosomatic theory. antigens, and the psychosomatic theory.
Etiology of Ulcerative Colitis

Incidence of Ulcerative Colitis
Period of INCIDENCE
Study (Per 100,000)
USAUSA Minnesota 1935-64Minnesota 1935-64 7.27.2 Baltimore Baltimore 1960-631960-63 4.64.6UKUK OxfordOxford 1951-601951-60 6.56.5 WalesWales 1968-771968-77 7.27.2 AberdeenAberdeen 1967-761967-76 11.3 11.3DenmarkDenmark CopenhagenCopenhagen 1962-781962-78 8.18.1 1981-881981-88 9.59.5Holland Holland LeidenLeiden 1979-831979-83 6.86.8Sweden Sweden Stockholm CountyStockholm County 1975-791975-79 4.34.3IIsrael srael Tel-AvivTel-Aviv 1961-701961-70 3.63.6

Medical Management of Ulcerative ColitisActive diseaseActive disease
Mild-moderate diseaseMild-moderate disease Distal colitis Distal colitis
Sulfasalazine or 5-ASA preparation Sulfasalazine or 5-ASA preparation
(oral or rectal)(oral or rectal)Topical corticosteroidTopical corticosteroid
Extensive colitis Extensive colitisSulfasalazine or oral 5-ASA Sulfasalazine or oral 5-ASA
preparationpreparation Moderate-severe diseaseModerate-severe disease
Distal colitis Distal colitisTopical corticosteroidTopical corticosteroidPrednisonePrednisone
Extensive colitis Extensive colitisPrednisonePrednisone
Severe-fulminant diseaseSevere-fulminant diseaseExtensive colitisExtensive colitisParenteral corticosteroidParenteral corticosteroidIntravenous cyclosporine Intravenous cyclosporine
IInfliximab (Remicade) reports of nfliximab (Remicade) reports of small bowl tumorssmall bowl tumors
Inactive diseaseInactive disease• Distal colitisDistal colitis Sulfasalazine or 5-ASA Sulfasalazine or 5-ASA preparation (oral or rectal)preparation (oral or rectal) Azathioprine or 6-MP Azathioprine or 6-MP• Extensive colitisExtensive colitis Sulfasalazine or oral 5-ASA Sulfasalazine or oral 5-ASA preparationpreparation Azathioprine or 6-MP Azathioprine or 6-MP

“Familial Adenomatous PolyposisSyndrome”

“Familial Adenomatous Polyposis Syndrome”
Gastrointestinal polyposis refers to the presence Gastrointestinal polyposis refers to the presence of numerous polyps throughout the GI tract. Most of numerous polyps throughout the GI tract. Most of these syndromes are inherited, and most are of these syndromes are inherited, and most are associated with an increased colon cancer risk. associated with an increased colon cancer risk.
FAP is the most common adenomatous polyposis FAP is the most common adenomatous polyposis syndrome. Patients develop hundreds to syndrome. Patients develop hundreds to thousands of adenomas, and if the colon is not thousands of adenomas, and if the colon is not removed, colon cancer is inevitable. removed, colon cancer is inevitable.
This disease is autosomal dominant with 80% to This disease is autosomal dominant with 80% to 100% penetrance and a prevalence of 1:7500. 100% penetrance and a prevalence of 1:7500.

“Familial Adenomatous Polyposis Syndrome”
IIn 1987, a gene for FAP was isolated, and genetic n 1987, a gene for FAP was isolated, and genetic testing is now available to identify family members testing is now available to identify family members that are carriers.that are carriers.
The average age of detectable polyps is 15 years.The average age of detectable polyps is 15 years. Average age of cancer is 10-15 years after the Average age of cancer is 10-15 years after the
onset of the polyps. onset of the polyps. Associated findings: Associated findings:
Gastric polyps – 30 to 100%Gastric polyps – 30 to 100% Duodenal polyps – 60 to 90%Duodenal polyps – 60 to 90% Papilla Vater Adenomatous Changes – 50 to 85%Papilla Vater Adenomatous Changes – 50 to 85% Duodenal Cancer Lifetime Risks – 4 to 12% Duodenal Cancer Lifetime Risks – 4 to 12% Desmoid Tumors – 4 to 32%Desmoid Tumors – 4 to 32%

Familial Adenomatous Polyposis Familial Adenomatous Polyposis

Crohn’s Crohn’s




The “Crohn’s Disease” Trio in 1932The “Crohn’s Disease” Trio in 1932

Crohn’s Morphology

Endoscopic Features of Ulcerative Colitis and Crohn's Disease
CharacteristicsCharacteristics UlcerativeUlcerative Crohn's Crohn's Colitis Colitis Disease Disease
DistributionDistribution SymmetricSymmetric AsymmetricAsymmetricRectal involvementRectal involvement AlwaysAlways VariableVariableSkip lesionsSkip lesions NoNo YesYesVascular patternVascular pattern BluntedBlunted Frequently normalFrequently normalFriabilityFriability FrequentFrequent InfrequentInfrequentErythemaErythema FrequentFrequent Less frequentLess frequentAphthous ulcersAphthous ulcers NoNo YesYesLinear ulcersLinear ulcers RareRare FrequentFrequentSerpiginous ulcersSerpiginous ulcersRareRare FrequentFrequentCobblestoningCobblestoning NoNo YesYesPseudo-polypsPseudo-polyps FrequentFrequent FrequentFrequent

The Case Against R.P. for Crohn’s Disease
• High complication rate (vs UC)• High pouch failure rate (vs UC)• Pouch excision risky, complicated• Small bowel loss is failure• Salvage surgery…High failure rate• Literature reports…Where presumptive diagnosis was UC
or indeterminate

Final Thoughts on Crohn’s
• Rarely should restorative proctocolectomy be Rarely should restorative proctocolectomy be advised if a diagnosis of Crohn’s is known prior to advised if a diagnosis of Crohn’s is known prior to surgery. surgery.
• One stage restorative proctocolectomy should be One stage restorative proctocolectomy should be resisted in nearly all emergency situations. resisted in nearly all emergency situations.
• At all times, it is the duty of the surgeon to inspect At all times, it is the duty of the surgeon to inspect the resected specimen before pouch construction. the resected specimen before pouch construction. If there are questions as to the diagnosis (even after If there are questions as to the diagnosis (even after frozen sections) forego pouch formation. frozen sections) forego pouch formation.
• If patients with a pouch later develop clear evidence If patients with a pouch later develop clear evidence of Crohn’s, judge each case on its merits (i.e. of Crohn’s, judge each case on its merits (i.e. Function: Are complications amenable to further Function: Are complications amenable to further surgical treatment?)surgical treatment?)

Forrest says, “Inflammatory Bowel Disease is like a box of choc-lits”

“Indeterminate Colitis”
• Those five to ten percent of inflammatory Those five to ten percent of inflammatory bowel disease patients that can not be bowel disease patients that can not be clearly diagnosed as either Crohn’s or clearly diagnosed as either Crohn’s or ulcerative colitis. ulcerative colitis.

IPAA for Indeterminate Colitis at CCF
Indeterminate Ulcerative p
Stool frequency 6.0 6.0 0.99
Night frequency 2.0 1.0 0.001
Q. Of life 9 9 0.06
Q. Of health 8 9 0.07
L. Of energy 8 8 0.21
L. Of happiness 10 10 0.28
IPAA again? (%) 93.3 97.9 0.05
IPAA for others? (%) 97.9 98.2 0.99

Surveillance for Colorectal Cancer Surveillance for Colorectal Cancer in Ulcerative Colitisin Ulcerative Colitis

Surveillance for Colorectal Cancer in Ulcerative Colitis
Colorectal cancer occurs in approximately six Colorectal cancer occurs in approximately six percent of patients with extensive disease and will percent of patients with extensive disease and will be the cause of death in about three percent. be the cause of death in about three percent.
The risk of developing colorectal cancer increases The risk of developing colorectal cancer increases over time, is greater in patients with extensive over time, is greater in patients with extensive disease, older age at the onset of symptoms, and disease, older age at the onset of symptoms, and in those with cholestatic liver disease and in those with cholestatic liver disease and sclerosing cholangitis . sclerosing cholangitis .
The frequency of surveillance colonoscopies is The frequency of surveillance colonoscopies is contentious. contentious.
Goal of surveillance is to detect dysplasia. Goal of surveillance is to detect dysplasia.

Surveillance for Colorectal Cancer in Ulcerative Colitis (cont’)
Low-grade dysplasia progresses or is Low-grade dysplasia progresses or is synchronous with cancer 18% to 30% of synchronous with cancer 18% to 30% of patients.patients.
High-grade dysplasia is concurrent with High-grade dysplasia is concurrent with cancer or progresses to cancer in 40% of cancer or progresses to cancer in 40% of patients. patients.
IIt is suggested that four biopsies be taken t is suggested that four biopsies be taken at ten centimeter intervals throughout the at ten centimeter intervals throughout the colon. colon.

Normal Normal UCUC
Colonoscopic ViewColonoscopic View

NormalNormal UC UC UC UC

SURGICAL INDICATIONS FOR ULCERATIVE COLITIS
UrgentUrgent Non-urgentNon-urgentSevere/fulminant colitisSevere/fulminant colitis Medically refractory disease Medically refractory diseaseToxic megacolonToxic megacolon Unacceptable medication-related toxicity Unacceptable medication-related toxicity PerforationPerforation Dysplasia, DALM, or suspected cancer Dysplasia, DALM, or suspected cancerMassive hemorrhageMassive hemorrhage Selected extraintestinal manifestations Selected extraintestinal manifestationsAcute colonic obstructionAcute colonic obstruction Growth failure in children Growth failure in childrenColon cancerColon cancer
DALM = dysplasia-associated lesion or massDALM = dysplasia-associated lesion or massIImmediate surgery warrantedmmediate surgery warrantedPrompt but not immediate surgery warrantedPrompt but not immediate surgery warrantedRefractory to medical therapyRefractory to medical therapyRefractory to 5-aminosalicylic acid, corticosteroids, and immunomodulatorsRefractory to 5-aminosalicylic acid, corticosteroids, and immunomodulators

Contraindications to Restorative Proctocolectomy Ulcerative Colitis
AbsoluteAbsolute• Acute, fulminant colitis, especially with clinical toxicity, Acute, fulminant colitis, especially with clinical toxicity,
peritonitis, or perforation of the colonperitonitis, or perforation of the colon• Known Crohn’s disease at time of operationKnown Crohn’s disease at time of operation• Severe anal sphincter dysfunctionSevere anal sphincter dysfunction• Carcinoma of the distal rectumCarcinoma of the distal rectum
Relative contraindicationsRelative contraindications• Morbid obesityMorbid obesity• Severe malnutrition or debilitySevere malnutrition or debility• Age > 65 yearsAge > 65 years• Psychologically impaired or patients at high risk for non-Psychologically impaired or patients at high risk for non-
compliance.compliance.

Age and IPAA
• Early restrictions• Safety as experience increases• Expansion of age limits• Patient assessment of quality of life vs. function
Function Quality of Life
Under 60 years +++ +++61–70 years ++ +++70 years plus + ++

The Presence of Cancer…..Does it Rule Out IPAA?
• The presence of colon cancer does not preclude IPAA (adherence to traditional
standards of oncologic resection need to be maintained).
• If advanced mid or low rectal cancer is diagnosed, this may preclude IPAA.

Ulcerative ColitisSurgical Options
• Proctocolectomy and Proctocolectomy and IIleostomyleostomy
• Colectomy and Colectomy and Ileostomyleostomy
• Colectomy and Colectomy and IIleorectostomyleorectostomy
• Proctocolectomy and Continent Proctocolectomy and Continent IIleostomyleostomy
• Restorative ProctocolectomyRestorative Proctocolectomy

Continent Ileostomies
- Kock pouch (1969-1972)- Kock pouch (1969-1972)

Continent Ileostomies
• StomaStomaSmaller & FlushSmaller & FlushLower in AbdomenLower in Abdomen




Late Complications
• Valve Slippage: 3 - 25%Valve Slippage: 3 - 25%• Fistula : 3%Fistula : 3%• Skin Level Stenosis : 8%Skin Level Stenosis : 8%• Prolapse : 3%Prolapse : 3%• Pouchitis : 5 - 43%Pouchitis : 5 - 43%

Restorative Proctocolectomy
• Major OperationMajor Operation• Cures DiseaseCures Disease• Evacuation vs Normal RouteEvacuation vs Normal Route• Bowel FunctionBowel Function• Technical Variations or Technical Variations or
ControversyControversy

Restorative Proctocolectomy
Variations or ControversyVariations or Controversy• Pouch DesignPouch Design
J , S , W , HJ , S , W , H• AnastomosisAnastomosis
Double-StapledDouble-Stapled MucosectomyMucosectomy
• DiversionDiversion





• Original Original IIPAA was hand sewn “S” configuration by Parks [BMJ 1978; 2:85-88].PAA was hand sewn “S” configuration by Parks [BMJ 1978; 2:85-88].
• IIngenious thinking and the use of stapling techniques now provide multiple ngenious thinking and the use of stapling techniques now provide multiple options for constructing pouches J, W, K, H, B, & U.options for constructing pouches J, W, K, H, B, & U.
• IInitially the “S” pouch required pouch intubation in up to 50% of patients.nitially the “S” pouch required pouch intubation in up to 50% of patients.
• Subsequent shortening of the efferent limbs to 2-3 cm, reduced this condition.Subsequent shortening of the efferent limbs to 2-3 cm, reduced this condition.
• Manovolumetic studies demonstrate that “S” pouches have a greater median Manovolumetic studies demonstrate that “S” pouches have a greater median volume than “J” pouches 420 ml vs. 305 ml but without functional differences. volume than “J” pouches 420 ml vs. 305 ml but without functional differences. (Hallgren, INT J Col. Dis. 1989, 4:156;160)(Hallgren, INT J Col. Dis. 1989, 4:156;160)
• Major advantage of the “S” pouch is on extra couple of centimeters in length Major advantage of the “S” pouch is on extra couple of centimeters in length than other pouches, helping form a tension free than other pouches, helping form a tension free IIPAA.PAA.
• The “W” pouch proposed by Nicholls in 1985 has the major problem of being The “W” pouch proposed by Nicholls in 1985 has the major problem of being bulky and difficult to advance in the narrow pelvis. bulky and difficult to advance in the narrow pelvis.
Pouch Design

Johnston [Gut 1996] 60 pts. Johnston [Gut 1996] 60 pts. no difference no difference
Keighley [BR J Surg 1988] 33 pts. Keighley [BR J Surg 1988] 33 pts. no difference no difference
Salvaggi [DC&R 2000] 24 pts. Salvaggi [DC&R 2000] 24 pts. daily defecation daily defecation frequency of three in “W” pouches and five in “J” frequency of three in “W” pouches and five in “J” pouches (at 12 months). The “W” also had less night pouches (at 12 months). The “W” also had less night time defecation and less anti-diarrheal usage. time defecation and less anti-diarrheal usage.
Farock [Ann Surg 2000] Farock [Ann Surg 2000] “J” pouch stool frequency “J” pouch stool frequency per day :per day :
six in males six in males seven in femalesseven in females
“J” pouch vs. “W” pouch

What is missing in the analysis? Sphincter functionSphincter function Stool consistencyStool consistency Patterns of motilityPatterns of motility Capacity of the pelvis to Capacity of the pelvis to
accommodate the pouchaccommodate the pouch
Comparing Pouch Design & Function

All use 30-40 cm of terminal ileumAll use 30-40 cm of terminal ileum
Small differences in function and designSmall differences in function and design
The “J” is easy to construct and The “J” is easy to construct and conserves operative time and provides conserves operative time and provides equivalent functionequivalent function
Pouches – My Choice

Restorative Proctocolectomy
J - Pouch

Preoperative Preparation
• Confer with patient and family so they Confer with patient and family so they understand the nature of the operation, understand the nature of the operation, the necessity for surgery, alternative the necessity for surgery, alternative therapies, operative hazards, possible therapies, operative hazards, possible complications, and potential benefits.complications, and potential benefits.
• Understanding of the nature of an Understanding of the nature of an ileostomy.ileostomy.
• Possibility of awareness of possible Possibility of awareness of possible function impairment.function impairment.
• Offer male patients cryopreservation of Offer male patients cryopreservation of sperm prior to operation.sperm prior to operation.
• Selection of ileostomy site.Selection of ileostomy site.

Preoperative Preparation (cont’)
• Correct specific medical problems Correct specific medical problems (anemia, hyperglycemia, electrolyte (anemia, hyperglycemia, electrolyte abnormalities)abnormalities)
• Bowel preparationBowel preparation• Stress steroid therapyStress steroid therapy• Antibiotic prophylaxis Antibiotic prophylaxis

Pitfalls and Danger Points
• IInjury to pelvic autonomic nerves with njury to pelvic autonomic nerves with resultant sexual and urinary dysfunction. resultant sexual and urinary dysfunction.
• Ureteral injuries.Ureteral injuries.• Fecal contamination with risk of intra-Fecal contamination with risk of intra-
abdominal sepsis and wound infections.abdominal sepsis and wound infections.• Presacral venous bleeding.Presacral venous bleeding.• IImproper ileostomy placement and mproper ileostomy placement and
construction.construction.• Splenic injury.Splenic injury.

Operative Strategies
• Wide surgical dissection with radical Wide surgical dissection with radical mesentery resection is unnecessary mesentery resection is unnecessary and meddlesome (unless invasive and meddlesome (unless invasive carcinoma is suspected). carcinoma is suspected).
• Close adherence to rectal wall during Close adherence to rectal wall during lateral and posterior dissection to lateral and posterior dissection to avoid injury to pelvic nerves. avoid injury to pelvic nerves.



Exploration
• Look for manifestations of possible Look for manifestations of possible Crohn’s disease.Crohn’s disease.
• IIf diagnosis is unclear, need for f diagnosis is unclear, need for total proctocolectomy needs total proctocolectomy needs reassessment.reassessment.



Proctectomy
a. Avoid injury to the pelvic autonomic nerves.
b. We use mesorectal dissection; bloodless plane . Impotence: injury during antero-lateral dissection of
the rectum (necessary with both close or mesorectal resection) Injury at upper rectum: hurts the hypogastric nerves = retrograde ejaculation
c. At S3; the anterior ® angle turn of the rectum occurs, so don’t dig deep into the presacral fascia.
d. Continue posterior dissection to a palpable coccyx.
e. Circumferential mobilization of rectum @ levators.
f. Pressing in on perineum may give better exposure.




Magnitude of the problem of 74 pouches that could not be constructed in the Mayo series, 32 were due to length problems. [Browning A, J.AM.Col. Surg. 1998 ) of the pouch should reach the inferior border of the pubic symphysis.
Maneuvers to obtain extra length
a. Division of terminal ileum should be done within tow to three cm. of the cecum.
b. Divide adhesions; mobilize the terminal ileal mesentery to the level of the duodenum
c. Mesenteric peritoneum division in stair step technique
d. Retest length before pouch formation
e. Division of the terminal divisions of the SMA or the ileal-colic artery (IC); confirming adequate vascularity of the ileum.
f. Clamp the vessels for at least 15 minutes prior to ligation
g. “S” pouch is always an alternative
Achieving Length



Controversies in IPAA

Mucosectomy vs. Double Staple Technique
• The aim of IPAA is to remove all of the diseased colonic and rectal mucosa.
• The double stapled technique leaves a cuff of anal transitional zone (ATZ).
• The ATZ contains residual columnar mucosa.• Anastomosis at this point gives better function than anastomosis at the dentate line.• Inherent risks of leaving the ATZ are malignancy and recurrent inflammation (cuffitis).• The theories for poorer function with mucosectomy
include trauma to anal sphincter during dissection and removal of the anal transition zone.

ZIV et al report stapled IPAA are safer than handsewn (fewer septic complications).
ZIV found the rate of anastomosis disruption and parapouch abscess were higher in the handsewn group.
Gecim (Mayo Clinic) stated the rate of abscess or fistula may be influenced by the surgeons experience.
Gecim pointed to long term steroids and other immunomodulants as contributors to fistula formations.
Gecim found no difference in perianal abscess rate or fistula rate in stapled vs. handsewn pouches.
1) ZIV Y, AM J Surg 1996; 172(3): 320-32) Gecim IE, Dis Colon Rectum 2000; 43(9): 1241-5
Type of Anastomosis (handsewn vs. stapled) and The Rate of Sepsis

Function Following Mucosectomy and Double Staple Technique
DOUBLE STAPLEDReilly [Ann Surg 1997] Notes occ. episodes of incontinence is 38% in stapled group and 64% in mucosectomy group.
Anal canal resting pressures stapled 78.3 mm Hg mucosectomy 49.4 mm Hg
Squeeze pressures
stapled 195 mm Hg mucosectomy 144 mm HG
Hallgren EUR, J Surg 1995, 161, 95 pg 21, found similar results
MUCOSECTOMYSew-Chen BR J. Surg 1991
Luukkeon Arch Surg 1993
Both randomized trials found no difference in function between the two techniques.

The Factors in Choosing Mucosectomy vs. Double Stapled
What is safest and best for patient.
In the presence of mucosal neoplastic change
perform mucosectomy.
If double-stapled technique is used, you must:
Do yearly follow-up of the anal transition zone with digital examination and endoscopy with biopsy.

What is The Role of a Defunctioning Ileostomy?
Pelvic sepsis occurs in 4.8% of patients undergoing IPAA [Farouk etal, Dis Colon Rectum 1998].
In patients with pelvic sepsis, the pouch failure rate (permanent diversion or excision) was 26% compared to 5.9% in patient without pelvic sepsis.
Patients with pelvic sepsis who retained their pouch had similar evacuation rates as non- pelvic sepsis patients but retained their protective pad use, incontinence rates, and medication rates were all increased.
Pelvic sepsis can be life threatening.
The Role of Ileostomy in IPAA
• Sugerman reported an abscess or enteric leak rate of 12% in patients who underwent one stage procedures without
ileostomy.• Tjandra et al reported a higher rate of septic complications in patients without an ileostomy.• ZIV at the same institution reported that as the number of IPAA without ileostomy cases have increased the two groups of patients are showing a nonstatistical difference in complication rate.• Remzi reported on 1,725 patients with ileostomy vs. 277 patients without ileostomy.• Remzi found no differences between the groups in respect to: sepsis, leaks, or fistula occurrence.
1) Sugerman H J et al. Ann Surg 2000;232(4):530-41. 2) Tjandra et al. Dis Colon Rectum 1993; 36(11):1007-14. 3) ZIV Y et al. AM J Surg 1996; 171(3):320-3. 4) Remzi FH, et al. Dis Colon Rectum 2003.
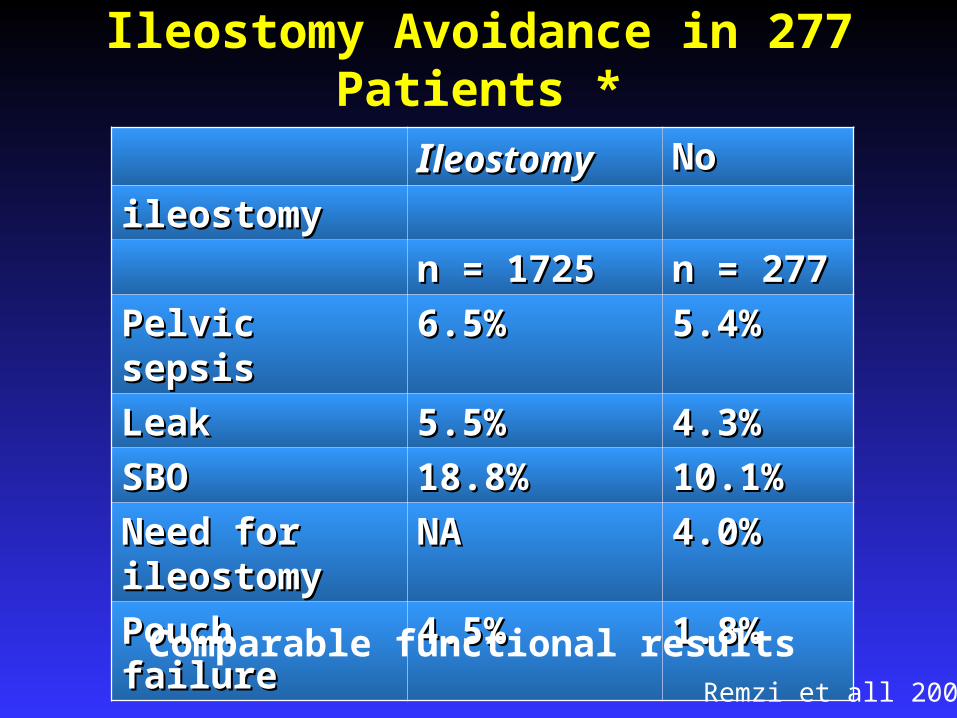
Ileostomy Avoidance in 277 Patients *
IIleostomyleostomy NoNo
ileostomyileostomy
n = 1725n = 1725 n = 277n = 277
Pelvic sepsisPelvic sepsis 6.5%6.5% 5.4%5.4%
LeakLeak 5.5%5.5% 4.3%4.3%
SBOSBO 18.8%18.8% 10.1%10.1%
Need for Need for ileostomyileostomy
NANA 4.0%4.0%
Pouch failurePouch failure 4.5%4.5% 1.8%1.8%
Comparable functional resultsRemzi et all 2002

Grobler [BR. J Surg 1992;79:903-906]Grobler [BR. J Surg 1992;79:903-906] 23 patients with IPA and loop ileostomy23 patients with IPA and loop ileostomy 22 patients with IPAA without loop ileostomy22 patients with IPAA without loop ileostomy No patients taking steroidsNo patients taking steroids All operations without intra-op complicationsAll operations without intra-op complications All were double stapled “J” pouchesAll were double stapled “J” pouches No statistically significant differences in No statistically significant differences in
postoperative complication rates or pouch postoperative complication rates or pouch function function
OUTCOMESTemporary Diversion vs. Single Stage Procedures

Galandiuk [Dis Colon Rectum 1991;34:870-873]Galandiuk [Dis Colon Rectum 1991;34:870-873]
37 pts with diversion 37 pts without diversion37 pts with diversion 37 pts without diversion
Complication rate NSD NSD
Reoperation NSD NSD
Functional outcomes NSD NSD
OUTCOMESTemporary Diversion vs. Single Stage Procedures

Defunctioning ileostomy may help reduce the incidence of pelvic sepsis, but is not a risk free procedure.
Mechanical and functional complications may follow construction and closure of the stoma.
[Metcalf Dis Colon Rectum 1986] 157 temporary loop ileostomies 39 patients had mechanical complications
Retraction 15.9% Prolapse 1.3% Fistula .6% Abscess .6% Bowel obstruction (stoma related)
Potential Complications Associated with Defunctioning Ileostomy

111 patients had functional complications
Peristomal irritation 53.5% Leakage 7.6% High output 3.8% Incomplete diversion 5.7% After closure: Bowel obstruction 14.7% Peritonitis 7.4% Wound infections 1.6%
Advantages of omitting a loop ileostomy
Required one hospital admission Avoid potential complications of ileostomy closure Financial advantage
Potential Complications Associated with Defunctioning Ileostomy (con’t)

Generalized good healthGeneralized good health
No chronic steroid therapyNo chronic steroid therapy
Tension free anastomosisTension free anastomosis
No intraoperative complicationsNo intraoperative complications
Generalized good healthGeneralized good health
No chronic steroid therapyNo chronic steroid therapy
Tension free anastomosisTension free anastomosis
No intraoperative complicationsNo intraoperative complications
Which Patients are Candidates for Single Stage Procedure?

Young – Faddock [Gastroenterology 2001 Young – Faddock [Gastroenterology 2001 II A-452-2302 A-452-2302 Seven laparoscopic Seven laparoscopic IIPAA vs. seven open PAA vs. seven open IIPAA PAA
(matched controls)(matched controls)
Laparoscopic IPAA vs. Open IPAA
2 days 2 days
4 4
NSD NSD
340 min. 340 min.
7 days p=0.0107 days p=0.010
99
NSDNSD
237 min.237 min.
Laparoscopic IPAA OPEN IPAA
I.V. narcotic useResumption of diet Hospital stayComplication rateOperation Time

Schmitt suggested no reduction in ileus or Schmitt suggested no reduction in ileus or postoperative length of stay with laparoscopic postoperative length of stay with laparoscopic vs. open [vs. open [IInt J Colorectal0 Dis 1994;9:134-137nt J Colorectal0 Dis 1994;9:134-137
Dunker [DC&R 2001, 44, 1800-1807] Reports Dunker [DC&R 2001, 44, 1800-1807] Reports functional outcomes and quality of life are no functional outcomes and quality of life are no different in open vs. laparoscopic different in open vs. laparoscopic IIPAAPAA
Patient satisfaction with the cosmetic result is Patient satisfaction with the cosmetic result is higher with laparoscopic higher with laparoscopic IIPAAPAA
Laparoscopic Laparoscopic IIPAA may reduce adhesion PAA may reduce adhesion formationformation
Other Considerations With Laparoscopic IPAA

ComplicationsComplications

The mortality rate after IPAA is less than 1%
Patients are typically young
Patients usually do not have co-morbid disease
Operations are generally performed in tertiary centers on selected patients
Mortality After IPAA
Blumberg , Opelka, HicksSouth Med J 2001;94(5):467-71

In early studies major complications were reported to be as high as 54%
With increased experience the rated has dropped to approximately 19%
Complications after IPAA may be categorized as early [within 30 days after surgery and late (after ileostomy closure)]
For one stage procedures early (within 30 days after surgery) and late (after 30 days post surgery)
Morbidity After IPAA
Marcello PW et alArch Surg 1993;128(5) 500-3;
Meagher AP et al BR J Surg 1998; 85(6): 800-3

The most common early complications are pelvic sepsis, anastomosis leaks, small bowel obstruction, and pouch bleeding
Early Complications

Pelvic sepsis is the most serious early IPAA complication, and it one of the main causes of pouch failure.
The rate of sepsis after IPAA ranges from 5% to 24%. The etiology may be suture line leaks, or bacterial
contamination of the surgical space during the operation. Risks factors for pelvic sepsis: malnutrition, prolonged
steroid use, hypoalbuminemia, anemia, and hypoxemia. The most common presenting signs are: fever, perineal
pain, purulent discharge, and leukocytosis. Early sepsis after IPAA usually presents between the third
and sixth postoperative day.
Sepsis
1) McMullen K, Hicks TC, World J Surg 1991; 15(6):763-62) Hyman et al, Dis Colon Rectum 1991;34(8):653-7

Leaks After IPAA
• Overall leak rate after IPAA ranges between 5 % and 18%.
• Leaks may develop from pouch-anal anastomosis, pouch itself, or from the tip of the “J” pouch.
• The two major factors associated with leaks are anastomotic tension and bowel ischemia.
• Elderly patients, males, and those patients on corticosteroids are also at greater risk for leak development.
Matty P et al. Ann Chir 1993; 47 (10) 1020-5 Fazio V et al. Ann Surg 1995; 222 (2):120-7

Small Bowel Obstruction After IPAA
• The overall incidence of small bowel obstruction after IPAA ranges from 15% to 44%.• The incidence of obstruction requiring operative intervention ranges from 5% to 20%.• Remzi reported on 2002 IPAA patients:
1725 had a diverting ileostomy with an 18% SBO rate 277 had no diverting ileostomy with a 10% SB0 rate
• Remzi also noted that the ileostomy group required more laparotomies for SBO than the non-diverted group.• MacLean reported on 1,178 IPAA patients• The cumulative risk of small bowel obstruction was 9% at 30 days; 18% at one year; 27% at five years; and 31% at ten years. • MacLean noted that 32%of the obstructions were due to the pelvic adhesions and the ileostomy closure site.• The surgical window = 2nd to 6th week is the most dangerous time
Francois Y et al. Ann Surg 19889; 209(1):46-50

Pouch Bleeding
• Postoperative bleeding from the pouch may arise from the suture line or because of pouch ischemia.
• Fazio reported bleeding from the pouch in 38 (3.8%) of 1005 patients.
• Thirty patients were treated with local irrigation of .9% saline and adrenaline 1:200,000
• Eight patients were treated with trans-anal suturing
• Significant bleeding occurring five to seven days post surgery may suggest a partial dehiscence.
Chalikonda S, Podium Presentation ASCRS 2003 New Orleans, La. Fazio VW, Ann Surg 1995; 222(2):120-7

Pouchitis• The most common complication following IPAA.
• Symptoms: Increased frequency, urgency, cramping pain, bright red bleeding, incontinence, diarrhea, and fever.
• Extraintestinal manifestations: Arthritis, iritis, and Pyoderma Gangrenosum.
• Histology: Acute granulocyte infiltration.
• Prevalence: Varies from 15% to 50%. • Etiology: Unknown. Theories include genetic, immune, microbial, and toxic mediators.
• Most popular theory: Fecal stasis with an increased anaerobe/aerobe bacterial ratio.
• Rarely seen with FAP.
• Male predominance. Nicholls RJ, World J Surg 1998;22(4):347-51 Subraman:K Gut; 1993, 34(11):1539-42

Diagnosis of Pouchitis
• Diagnosis should be made on the basis of clinical, endoscopic, and histologic features.
• Pouch disease activity index (PDAI) is the most commonly used diagnostic instrument.
• The PDAI has three separate scales: clinical symptoms, endoscopic findings, and histologic changes.
• Total score of seven or higher is defined as Pouchitis.
• Because the PDAI is costly, a modified scale was introduced in which the histology is omitted.
• This modified scale offers similar sensitivity, decreases cost, and avoids delay in diagnosis awaiting histology report.
Shen B, Drs Colon Rectum 2003, 46(6):748-53 Sandborn, Mayo Clinic Proc 1994; 69(5):409-15

Pouchitis Disease Activity Index
• Stool frequencyStool frequency
• Rectal BleedingRectal Bleeding
• Fecal urgency or abdominal crampsFecal urgency or abdominal cramps
• Fever (temperature>37.8° C)Fever (temperature>37.8° C)
• Endoscopic inflammationEndoscopic inflammation
• Acute histological inflammationAcute histological inflammation
• Ulceration per low-power field (mean)

Treatment for Pouchitis
• Includes antibiotic therapy and symptomatic relief with anti-diarrheal agents.
• Most effective agents are metronidazole and ciprofloxacin.
• 80% of pouchitis patients are successfully treated with metronidazole alone.
• Steroids, 5 – aminosalicylates, azathioprine, and six- mercaptopurine compromise the other major category of treatment. • Surgery? Bertoni: G, Dis Colon Rectum 2003;46(6):748-53

Refractory or Prolapsing Pouchitis
• 5% to 10% of pouchitis patients will develop refractory or relapsing symptoms.
• Probiotics are effective in these clinical situations
• A recent trial using VSL #3 (probiotic) was shown to be therapeutic for patients with acute relapsing pouchitis.
• These patients were induced into remission using ciprofloxacin and rifaximin.
• In follow-up only 15% in the probiotic group relapsed within nine months, whereas 100% of the placebo group
developed a relapse. 1) Shen B, Inflamm Bowel Dis 2001, 7 (4) 301-5 2) Sarton RB, Gastroenterology 200; 119(2):584-7

Mechanism of Action of Probiotics
• Suppression of resident pathogenic bacteria.
• Stimulation of mucin glycoprotein by intestinal epithelial cells.
• Prevention of adhesion of pathogenic strains to epithelial cells.
• Induction of host immune responses.
Sartor R.B. Gastroenterology 2000; 119(2):584-7

Irritable Pouch Syndrome (IPS)
• Patients with IPAA who have Pouchitis symptoms but normal endoscopic and histologic findings.
• They have a PDAI of < 7 and the absence of cuffitis.
• The etiology of IPS is unclear, and there is no algorithm for its management.
• 50% of IPS patients respond to irritable bowel treatments.
• This includes reassurance, diet modification, fiber supplements, anti-diarrheal, antispasmodics, and antidepressants.
Giochetti P, Gastroenterology 2000; 119(2):305-9
Shen B, AM J Gastroenterol 2002; 97(4):972-7

Cuffitis
• The 1 to 2 cm. of anal canal mucosa retained after IPAA (without mucosectomy) can become inflamed.
• Cuffitis has endoscopic and histologic inflammation of the pouch.
• 4% of patients with preserved anal mucosa after IPAA develop cuffitis.
• Most patients respond to local therapy with hydrocortisone suppositories or enemas.
Lavery IC, Dis Colon Rectum 1995;38(8):803-6

FISTULA• Usually a late complication
• 6% of IPAA patients develop a fistula
• Most common sites: vaginal, perineal, cutaneous, and presacral
• Options for therapy: fistulotomy, seton, advancement flap, prolonged ileal diversion, antibiotics, and fibrin glue.
• Fistula may represent undiagnosed Crohn’s.
• Postoperative pathologic diagnosis of Crohn’s leads to a pouch failure rate of 25%.
1) Fazio VW, Ann Surg 1995; 222(2):125-7 2) Ozuner G, Dis Colon Rectum 1997; 40(5) 543-7
•

Pouch – Vaginal Fistula (PVF)
• Leads to poor functional results and is a major cause of pouch failure.• Etiology: Sepsis, leaks, and “technical error”.• Most patients can be managed by local procedures.• The trans-anal ileal advancement flap is often successful.• SHAH reported on 60 patients with PVF. • 65% of the SHAH group had a diverting ileostomy. • 44% had a primary healing.• 4 patients had repeat flap advancement and closed the fistula.• Recurrence and pouch failure rates are high.• Patients with fistula formation diagnosed within six months
of surgery have better outcomes.• Those with > six month PVF presentation may be related to Crohn’s.• When local therapy fails, pouch reconstruction is an option.
1) SHAH NS, Dis Colon Rectum 2003

Anastomotic Strictures
• Anastomosis is considered strictured if it will not allow the admission of an index finger DIP joint or is less than 1 cm. in diameter.
• If stricture is severe, it can lead to outlet obstruction, pouch dilatation, and bacterial overgrowth.
• The rate of stricture ranges from 7.8% to 14%• St. Marks reported a 14% rate in handsewn and 40%
with stapled anastomosis.• Mayo reported a 12% rate with handsewn group
having the greatest problems. • Treatment options : Hegar dilators (office) #13 to #18
vs. surgical incision. (OR) • For complex stricture pouch advancement and neo-
ileal anastomosis. (good for strictures < 5 cm in length)
Fazio BR J Surg 1992; 27(7):694-6 Senapati A. INT J Colorectal Dis 1996, (2):57-59

Impotence, Retrograde Ejaculation, and Dyspareunia
• 1.5% of men will develop impotence.
• 4% of men will develop retrograde ejaculation.
• 7% of women develop dyspareunia.
• 49% of women note sexual dysfunction preoperatively. Their sexual activity increases dramatically after surgery.

Olsen reported fertility [B. J Surg 1999;PL:493-495
Theory of Etiology: Pelvic Adhesions
IPAA for Ulcerative Colitis Does it Affect Female Fertility?

Dysplasia and Malignancy
• The ileal pouch undergoes a series of histologic changes.
• The changes include slight villous atrophy to colonic metaplasia.
• Colonic metaplasia may be a premalignant condition.
• In 1997 Cox et al. reports an invasive adenocarcinoma in a longstanding Koch pouch.
• Heuschen et al. reported an IPAA pouch developed cancer.
• Baratris reported an adenocarcinoma in the anus after IPAA for U.C.
• Mucosectomy does not provide 100% removal of rectal mucosa.
• The anal transitional zone (ATZ) in the double stapled technique is at risk for dysplasia or cancer.
• The risk of dysplasia was studied in 178 patients (double stapled IPAA) over ten years.
• The risk of dysplasia was 4.5% without cancer being reported.
Baretsis et al. Dis Colon Rectum 2002 45(5):687-91 Remzi FH et al. Dis Colon Rectum 2503 :46(1):6-13

• O’Connell published data showing residual rectal mucosa in 7% of their IPAA patients with mucosectomy.
• Remzi reports ten year follow-up of the double staple technique with dysplasia in the residual anal transition zone to be 4.5% DC&R 2003, 46:6-13
• Cancer has been reported after both techniques.
Dysplasia and Cancer Following IPAA

Pouch Failure
• 6% of IPAA patients require either pouch excision or permanent ileostomy.
• Most frequent causes of failure are pelvic sepsis, high stool volume, Crohn’s disease, uncontrolled fecal incontinence. • A scoring system for calculating the risk of pouch failure identified eight risk factors: 1) Crohn’s 2) Patient co-morbidity 3) Prior anal pathology 4) Diminished sphincter manometry measurements 5) Anastomotic separation 6) Anastomotic stricture 7) Pelvic sepsis and 8) Perineal fistula formation.
• Overall salvage rates from pouches is 86%.
• 97% of patients who underwent pouch revision said they would undergo it again if necessary.
Fazio BR J Surg 1992; 27(7):694-6 Senapati A. INT J Colorectal Dis 1996, (2):57-59

Incidence of Pouch Failure
CENTERCENTER YEARYEAR # PATIENTS# PATIENTS % FAILURE% FAILURE
Mayo 19981998 13101310 10.210.2
ClevelandCleveland 19951995 10051005 4.54.5
TorontoToronto 19971997 551551 10.510.5
LaheyLahey 19931993 460460 3.53.5
OxfordOxford 19971997 200200 8.08.0
Buenos AiresBuenos Aires 19981998 178178 6.16.1
OchsnerOchsner 19951995 145145 3.03.0
U of MinnU of Minn 19981998 505505 8.88.8

Zmora 61
1991-1999
Dayton 52Dayton 52
1983-19991983-1999
Heuschen 48
1988-1999
Mc Lean 51
1982-2000
Fazio 50
1983-1998
Sagar Sagar 6262
1981-1981-19951995
Baixauli 53Baixauli 53
1985-20011985-2001
Institution FloridaFlorida Salt LakeSalt Lake HeidelbergHeidelberg TorontoToronto ClevelandCleveland MayoMayo ClevelandCleveland
No. patientsNo. patients 411411 650650 706706 12001200 16801680 17001700 ------
ReoperationReoperation 3232 2929 107107 5757 3535 2323 112112
Repeat Repeat IPAAIPAA
55 66 44 1717 3131 ------ 101101
Septic Septic complicatiocomplicationsns
1616 ------ 107107 1414 3535 44 6464
FistulaFistula 33 33 8787 2323 2525 44 4747
Stricture Stricture 11 ------ ------ 55 1414 11 3535
AbscessAbscess ------ 11 88 ------ 2525 44 4646
SalvageSalvage 21(84%)21(84%) 29 (100%)29 (100%) 99 (92%)99 (92%) 42 (77%)42 (77%) 80 (86%)80 (86%) 17 17 (74%)(74%)
70 (82%)70 (82%)
Pouch failure
44 0 8 15 5 0 14
Complications after reop.
99 6 --- 32 34 6 46
Repeat (IPAA) to Salvage Complication of Pelvic Pouches

Rocket Rocket Science?Science?Rocket Rocket
Science?Science?

Ileal pouch anal anastomosis has evolved over the last 25 years
Now it is the procedure of choice for patients requiring proctocolectomy for ulcerative colitis and selected FAP patients
As technical developments have emerged controversies have arisen
With continued commitment to research for pouch surgery hopefully these dilemmas will be resolved
CONCLUSION

“All at present known in
medicine is almost nothing in comparison
with what remains to be discovered”
R. Descartes (1596-1650) R. Descartes (1596-1650)
