pulmonary blastoma with a striated muscle component
TRANSCRIPT

Brit. ft. Dis. Chest (x966) 60, 87.
PULMONARY BLASTOMA WITH A STRIATED MUSCLE COMPONENT
BY KRISTIN HENRY AND E. ]7,. KEAL
Brompton Hospital, London s.w.3
IN 1961 Spencer reported four unusual pulmonary tumours. He called them pulmonary blastomas, and considered them to be the pulmonary counterparts of nephroblastomas, with which they shared certain features in structure and behaviour. The four turnouts he described included that of Barnard, previously reported with Barrett (1949) as a carcinosarcoma, and then (1952) as an embryoma of lung. The other three tumours resembled that of Barnard's both in appearance and structure, in that they were all composed of epithelial-lined tubules lying in an undifferentiated embryonic type of connective tissue stroma often closely resembling foetal lung. Spencer found differentiation of the stroma towards formation of fibrous tissue and smooth muscle, but was unable to demonstrate striated muscle. He does not record the presence of cartilage, foetal or otherwise. Although only two out of the four tumours proved malig- nant with distant metastases, three out of the four tumours contained areas where the degree of differentiation was poor enough to justify a diagnosis of carcinosarcoma.
In 1961 Campesi and Sommariva described a tumour which they called an embryonal adenosarcoma and which had the features of a pulmonary blastoma; and recently a further three cases were recorded and the subject reviewed by Souza, Peasley, and Takaro (1965).
The tumour about to be described will be the ninth reported pulmonary blastoma, and as far as is known the first in which other mesodermal tissues, in particular striated muscle, have been found.
Gase History The patient, a man of 77, was admitted to hospital on 28th August I962
(Brompton Hospital No. A82187). He had been a Chief Yeoman of Signals in the Navy, and was later employed in Naval Dockyards at home and abroad, where he smoked thirty or more cigarettes a day throughout his working life.
There was a history of productive cough for twenty years; and seven years previously increased breathlessness was associated with eedema of the ankles, for which he had since taken digoxin and oral diuretics. From i955 he had attended a chest clinic, where X-rays of the chest had shown gross bullous emphysema and evidence of old bilateral upper-lobe tuberculosis.
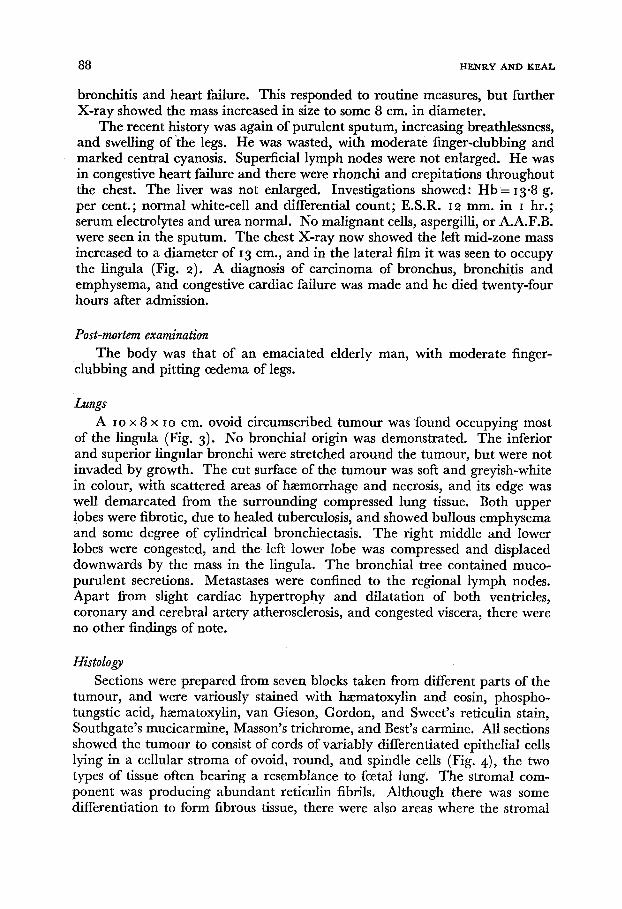
Serial X-rays were essentially unchanged until April 1962 , when a new opacity, roughly spherical and 2"5 cm. in diameter was noted in the left mid-zone (Fig. I). His general condition precluded intensive investigation, but in July 1962 he had been admitted to hospital elsewhere with an exacerbation of his
(Received for publication, aTanuary x 966 )
88 HENRY AND KEAL
bronchitis and heart failure. This responded to routine measures, but further X-ray showed the mass increased in size to some 8 cm. in diameter.
The recent history was again of purulent sputum, increasing breathlessness, and swelling of "the legs. He was wasted, with moderate finger-clubbing and marked central cyanosis. Superficial lymph nodes were not enlarged. He was in congestive heart failure and there were rhonchi and crepitations throughout the chest. The liver was not enlarged. Investigations showed: H b = 13"8 g. per cent.; normal white-cell and differential count; E.S.R. 12 mm. in 1 hr.; serum electrolytes and urea normal. No malignant cells, aspergilli, or A.A.F.B. were seen in the sputum. The chest X-ray now showed the left mid-zone mass increased to a diameter of 13 cm., and in the lateral film it was seen to occupy the lingula (Fig. 2). A diagnosis of carcinoma of bronchus, bronchitis and emphysema, and congestive cardiac failure was made and he died twenty-four hours after admission.
Post-mortem examination The body was that of an emaciated elderly man, with moderate finger-
clubbing and pitting oedema of legs.
Lungs A i o x 8 x I o cm. ovoid circumscribed tumour was found occupying most
of the lingula (Fig. 3)- No bronchial origin was demonstrated. The inferior and superior lingular bronchi were stretched around the tumour, but were not invaded by growth. The cut surface of the turnout was soft and greyish-white in colour, with scattered areas of hmmorrhage and necrosis, and its edge was well demarcated from the surrounding compressed lung tissue. Both upper lobes were fibrodc, due to healed tuberculosis, and showed bullous emphysema and some degree of cylindrical bronchiectasis. The right middle and lower lobes were congested, and the left lower lobe was compressed and displaced downwards by the mass in the lingula. The bronchial tree contained muco- purulent secretions. Metastases were confined to the regional lymph nodes. Apart from slight cardiac hypertrophy and dilatation of both ventricles, coronary and cerebral artery atherosclerosis, and congested viscera, there were no other findings of note.
Histology Sections were prepared from seven blocks taken from different parts of the
tumour, and were variously stained with h~ematoxylin and eosin, phospho- tungstic acid, h~ematoxylin, van Gieson, Gordon, and Sweet's reticulin stain, Southgate's mucicarmine, Masson's trichrome, and Best's carmine. All sections showed the tumour to consist of cords of variably differentiated epithelial cells lying in a cellular stroma of ovoid, round, and spindle cells (Fig. 4), the two types of tissue often bearing a resemblance to foetal lung. The stromal com- ponent was producing abundant reticulin fibrils. Although there was some differentiation to form fibrous tissue, there were also areas where the stromal
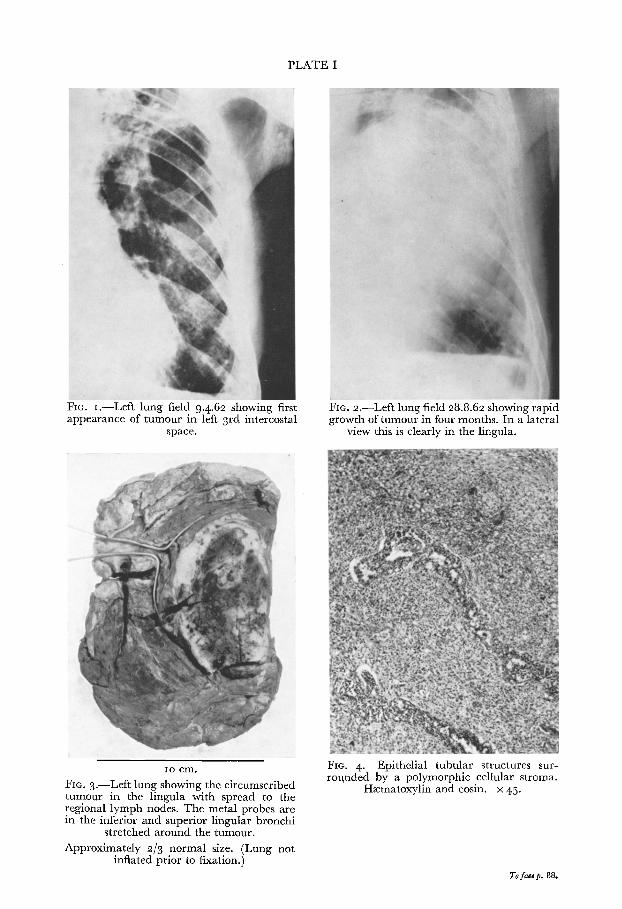
PLATE I
Fro. I.--Left lung field 9.4.62 showing first appearance of tumour in left 3rd intercostal
space.
FIe. 2.--Left lung field 28.8.62 showing rapid growth of tumour in four months. In a lateral
view this is clearly in the lingula.
Io cm. FIG. 3.--Left lung showing the circumscribed tumour in the lingula with spread to the regional lymph nodes. The metal probes are in the inferior and superior lingular bronchi
stretched around the tumour. Approximately 2/3 normal size. (Lung not
inflated prior to fixation.)
Fro. 4.--Epithelial tubular structures sur- rounded by a polymorphic cellular stroma.
H~ematoxylin and eosin, x 45.
To face p. 88.
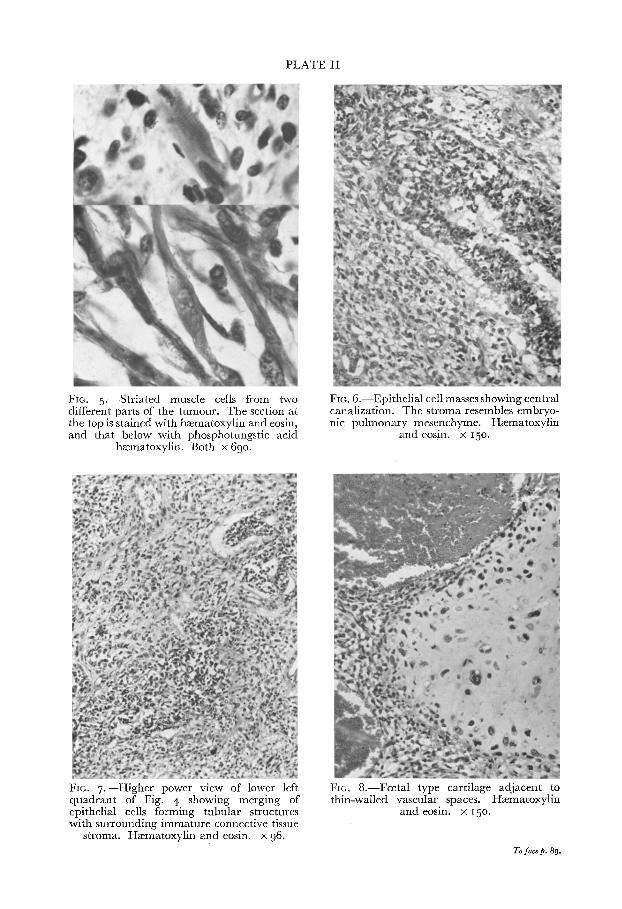
PLATE II
FIG. 5 . - -Str ia ted muscle cells from two different parts of the turnout. The section at the top is stained with haematoxylin and eosin, and that below with phosphotungstic acid
heematoxylin. Both x 69o.
FIC. 6.--Epithel ial cell masses showing central canalization. The stroma resembles embryo- nic pulmonary mesenchyme. H~ematoxylin
and eosin, x 15o.
FIO. 7 . - -Higher power view of lower left quadrant of Fig. 4 showing merging of epithelial cells forming tubular structures with surrounding immature connective tissue
stroma. Hzematoxylin and eosin, x 9 6.
Fro. 8.--Fcetal type cartilage adjacent to thin-walled vascular spaces. H~ematoxylin
andeosin, x i5 ° .
To face p. 89.
PULMONARY BLASTOMA WITH A STRIATED MUSCLE COMPONENT 89
celIs were so poorly differentiated, exhibiting such cellular pleomorphism, nuclear hyperchromatism, and marked mitotic activity, that the appearances were frankly sarcomatous. Scattered through the cellular connective tissue, and mainly in relation to the epithelial tubular structures, were aggregates of large, rounded, and multinucleate cells with abundant eosinophilic cytoplasm, and strap, tadpole, and fusiform cells in which cross-striation could be demon- strated (Fig. 5). The cords of epithelial cells had mostly undergone central canalization to form tubular structures, which in some areas merged impercep- tibly with the surrounding stroma (Figs. 6 and 7) from which they appeared to have been derived. The most differentiated epithelium formed a single layer of columnar, mucus-secreting cells, whereas the least differentiated appeared to be undergoing neoplastic change to a poorly differentiated adenocarcinoma. There was no differentiation on the part of the epithelial component towards a squamous appearance, nor were cilia demonstrated. The h~emorrhagic macroscopic appearance of the tumour was largely due to the presence of dilated thin-walled blood-filled spaces, and it was near one of these vascular areas that a few islands of foetal-type cartilage were found (Fig. 8). On the whole the tumour edge was distinct and bounded by a false capsule of com- pressed lung, but at some points there was invasion by tumour cells into the surrounding lung, and invasion of an occasional pulmonary vein by the stromal component could be seen. The lymph node metastasis consisted only of the stromal component, which was of a less malignant appearance than some parts of the tumour.
The tumour was classified as a pulmonary blastoma. The upper lobes showed the appearance of healed pulmonary tuberculosis, with much associated fibrosis, emphysema, and mild bronchiectasis. The bronchial tree showed the changes of acute on chronic bronchitis. In view of the history of thirty years' work in a naval dockyard, evidence of asbestosis was looked for, but none was found.
The changes in the other organs were confined to those due to congestive changes and to generalized atherosclerosis.
D i s c u s s i o n Blastomas are tumours derived from pluripotential embryonic cells of one
germ layer, and are capable of progressive and sometimes unlimited invasive growth. Hamartomas differ from blastomas in that they are malformations of tissue constituents normally present in the organ concerned, and their expansile but non-invasive growth is confined to a limited anatomical field. Embryonic tumours include blastomas, and not only is their time of possible origin in a given organ limited to the period during which the tissue components remain immature, but they can only produce what the organ field or blastema is capable of producing. Teratomas lack this organ-specificity, and produce a variety of tissues quite foreign to the organ in which they arise. In other words they are derived from tissue still regionally undetermined and capable of diver- gent differentiation in many directions (Willis, 1958).
Spencer (I96I, I962 ) believes that the pulmonary tumours he described

9 ° HENRY AND KEAL
develop from bipotential pulmonary blastema capable of differentiating into both epithelial and stromal constituents. He considers that in their mode of development and in certain other respects they resemble nephroblastomas, and he named them pulmonary blastomas. However, he pointed out that their existence can be explained only by accepting the evidence of Waddell (1949) that the peripheral respiratory portion of lung is derived from mesoderm, and not, as formerly supposed, from the endoderm of the laryngo-tracheal bud. While we accept Waddell's evidence on lung development and believe that pulmonary blastomas are mesodermal in origin, we question the view that the histogenesis of these pulmonary tumours is similar to that of nephroblastomas. Nephroblastomas are true embryonic tumours derived from tissues still im- mature, and the vast majority occur in infancy and early childhood. The pulmonary blastomas, however, occur in very much older patients, their ages ranging from nineteen to seventy-seven years. Spencer attributes their late occurrence to the continuing development of lung tissue up to ten years of age, whereas renal development is virtually complete at birth. Nevertheless, it is difficult to understand how the primitive totipotential cells of the embryonic pulmonary blastema can remain dormant until late in adult life and then give rise to tumour formation. However, Willis (196o) reminds us that adult mesenchymal tissue may contain plastic undifferentiated cells which can revert to the embryonic state when they multiply, and that to make a sharp distinction between primarily embryonic mesenchymomas and mesenchymous tumours with re-acquired embryonic qualities in adults is probably impossible. A good example of this capacity of adult mesenchyme for proliferation and redifferentia- tion is provided by the group of mixed mesodermal tumours of the uterus occurring in post-menopausal women. These uterine growths are composed of a variety of mesodermal tissues including a stromal component often closely resembling embryonic mesenchyme, and striated muscle elements. Willis (I 960) considers that it is from the cellular undifferentiated stromal tissue that all other tissues are derived, even the cancerous epithelium which is sometimes present.
It is felt that the rapidly growing tumour described above is sufficiently characteristic of what Spencer called pulmonary blastomas to classify it as such, rather than as a hamartoma in which malignant change had occurred, a teratoma, or the more common (but still rare) variety of pulmonary carcino- sarcoma. The tumour is peripheral, well demarcated from surrounding lung, and without any demonstrable bronchial origin. I twas large (io x 8 x io cm.), metastases were confined to the regional lymph nodes, and death was due to other causes. As in six of the eight reported blastomas, the tumour was found in the left lung of a male patient. Histologically it is composed of epithelial structures and stroma which vary in appearances from those of foetal lung to those of a malignant invasive tumour. The additional finding of striated muscle is hardly surprising. Both the mixed mesodermal tumours of the uterus and the nephroblastomas commonly contain a striated muscle component, which indeed may form the major part of some nephroblastomas. In his discussion on pul- monary rhabdomyosarcomas, Spencer (i 962) suggests that the "endodermal" elements described in these tumours by Helbing (I 898 ) and Zipkin (i 907) may

PULMONARY BLASTOMA W I T H A STRIATED MUSCLE COMPONENT 9I
well have been mistaken for the immature bronchiolar structures normally to be found in pulmonary blastomas, and that these tumours, far from being a form of in t rapu lmonary teratoma, could well be polymorphic rhabdomyo- sarcomas forming the main part of pulmonary blastomas. Depending on one's views on the histogenesis of the pulmonary blastomas, one may explain the presence of striated muscle in these tumours either as being a product of aberrant differentiation from embryonic cellular mesenchyme, or as a deriva- tive from adult mesenchyme which has undergone a process of proliferation and aberrant re-differentiation.
The tumour under discussion is not a hamartoma, since we have already defined this lesion as a malformation capable of expansile but non-invasive growth. Malignant change in a hamartoma is extremely rare, and of the few cases reported all are open to some doubt. We feel we can exclude this prob- ability on histological grounds. In none of the tumours reported as malignant hamartomas by Greenspan (I933) , Lowell and Tuhy (i949) , Kuyjer (i955) , Adams (I957), Cavin, Masters, and Moody (I958), and Jensen and Schiodt (I96o) was there a resemblance to foetal lung; and the lesion reported by Simon and Ballon (1947) was an obvious hamartoma, but of questionable malignancy. The absence of any radiographic lesion in our case until the age of 77 years does not of itself preclude a diagnosis of hamartoma, since Jensen and Schiodt (I958) showed that, of their 22 proven cases of hamartoma of lung, 5 had had several negative chest X-rays before developing the typical lung opacities.
It is unnecessary to entertain the idea that our tumour is a pulmonary teratoma. The only tissue present which is foreign to lung is striated muscle, and this can be explained by a process of aberrant differentiation on the part of undifferentiated mesenchymal cells.
We agree with Spencer (196I, I962 ) and Souza, Peasley, and Takaro (1965) that pulmonary blastomas are a distinct form of carcinosarcoma of lung. Carcinosarcomas consist usually of squamous carcinoma in a sarcomatons stroma, and neither they nor the three tumours with adenocarcinomatous com- ponents described by Frank (i915) , Ogowa (i929) , and Weber (i939) re- sembled foetal lung. Furthermore, about one-third of reported carcinosarcomas are described as polypoid endobronchial or endotracheal tumours. (Bargmann, Ackerman, and Kempler, 1951 ; Drury and Strickland, 1959; Moore, 1961 ; Taylor and Rae, I952. )
Summary A pulmonary blastoma with striated muscle and other mesodermal com-
ponents is described, and reasons are given for classifying it as such. The presence of striated muscle and the views on the histogenesis of these rare pulmonary tumours are discussed. There is some doubt whether they are true embryonic tumours. However, it is felt that because of their resemblance to foetal lung and their mesodermal nature the term pulmonary blastoma is fuUy justified, and we agree that they should be considered as a separate entity from carcinosarcoma of the lung.
92 HENRY AND KEAL
ACKNOWLEDGEMENTS We are grateful to Dr. W. D. W. Brooks and Dr. K. F. W. Hinson for permission to publish
this case, to Dr. K. F. W. Hinson for his advice and encouragement, and to Professor H. Spencer for his confirmation of the histological appearances.
We thank Mr. K. Morman of the Chester Beatty Institute for the photomicrographs and the Marsden photographic department for the reproductions of the chest X-rays.
REFERENCES
ADAMS, M . J . T . (i957). Thorax, i2, =68. BARNARD, W. G. (1952). Thorax, 7, 299. BARRETT, N. R., & BARNARD, W. G. (i945). Brit. 07. Surg., 32, 447. BARGMANN, M., ACKERMA~, L. V., & KEMPLER, R. L. (x95I). Cancer, 4, 9x9 • CAMPESI, G., & SOMMARIVA, V. (I96I), Arch. De Vecchi Anat. pat., 35, Io9. CAVIN, E., MASTERS, J. H., & MOODY, J. (x958). 07. thorac. Surg., 35, 816. DRURY, R. A. B., & STRICKLAND, R. M. (I959). 07. Path. Bact., 77, 543- FRANK, A. (x9x5). Schmidts07b. ges. Med., 322, I45. GREENSPAN, E. B. (I933). Amer. 07. Cancer, I8, 6o3. HELBINO, C. (x898). Zbl. allg. Path., 9, 433- JENSEN, K. G., & SCHIODT, T. (1958). Thorax, x3, ==3. JENSEN, K. G., & SCmODT, T. (I96O). Thorax, I5, I=O. KUYJER, P. J. (1955). Ned. T. Geneesk., 99, x884. LOWELL, L. M., & TUHY, J. E. (i949). 07. thorac. Surg., i8, 476. MOORE, T. C. (I961). Surgery, 5o, 866. OGOWA, K. (I929). Folia orient, intern. Med., xx, i33. SIMON, M. A., & BALLON, H. C. (1947). aV. thorac. Surg., x6, 379. SOUZA, R. C., PEASLEY, E. D., & TAKARO, T. (x965). Ann. thorac. Surg., x, 259- SPBNCER, H. (x96I). 07. Path. Bact., 82, I61. SPENCER, H. (I96=). In Pathology of the Lung. New York: Macmillan. TAYLOR, H. E., & RAE, M. V. (I95=). 07. thorac. Surg., 24, 93- WADDELL, W. R. (I949). Arch. Path., 47, 2=7. WEBER, F. (I939). Zbl. allg. Path., 72, 113. WILLIS, R. A. (1958). Borderland of Embryology and Pathology, ist ed. London: Butterworth. WILLIS, R. A. (196o). Pathology of Tumours, 3rd ed. London: Butterworth. ZIPKIN, R. (x9o7). Virchows Arch. path. Anat., x87, 244-