protection v. patient care* meeting 27-… · · 2008-04-18diagnosis survivors treatment burial...
TRANSCRIPT
ProtectionProtection v. v. Patient Care*Patient Care*
Dr Simon N. MardelOBE MSc DTM&H FFARCS FRCS
*including the *including the health of the publichealth of the public

** There is often a wider There is often a wider picturepicture

Surveillance
Sensibilisation
Health worker education
Referral
Diagnosis
TreatmentSurvivors
Burial
Epidemic control: a smooth running machine-
-that communicates well
Ebola Uganda: 31 cases of nosocomial transmission among staff SARS worldwide: 21% of all probable cases were health care workers
Precautions should be based on
Mode of Transmission –however---• Agent - Don’t know
• Man - Don’t care / We can’t afford (to be seen) not to
• Environment - Don’t have enough resources / We cant afford to
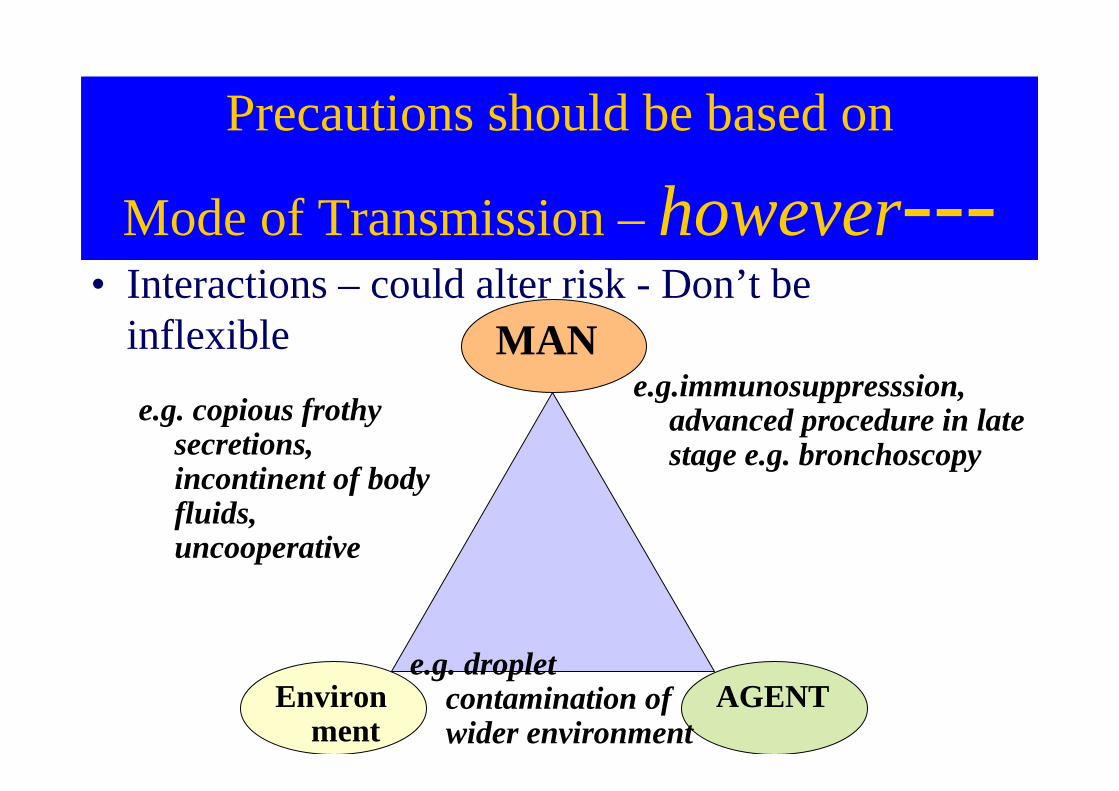
Precautions should be based on
Mode of Transmission –however---• Interactions – could alter risk - Don’t be
inflexible
Environment
MAN
AGENT
e.g. copious frothy secretions, incontinent of body fluids, uncooperative
e.g.immunosuppresssion, advanced procedure in late stage e.g. bronchoscopy
e.g. droplet contamination of wider environment

NosocomialNosocomial transmission of VHF and transmission of VHF and
SARS is usually obvious SARS is usually obvious --
Disease Zoonotic Arboviral Person-to-person
Dengue - + -
Yellow Fever + + -
Crimean-Congo HF + + ++
Rift Valley Fever + + +/-
Hantavirus disease (HFRS) + - -
Lassa Fever + . +
AHF, BHF, VHF, BrHF + - +
Ebola HF, Marburg HF +/- ? ++

--extent of extent of nosocomialnosocomial transmission is often transmission is often
not appreciated.not appreciated.
E.g.WHOSIGN estimates injections are responsible for (new cases):
5% of all HIV globally,
32% of HepB*
40% of HepC*
* in developing and transitional countries.
Existing infection control measures inadequate

EvaluateEvaluate
A B CD E
EvaluateEvaluate
A B CD E
EvaluateEvaluate
A B CD E
In medicine we often have the luxury of making a diagnosis through an incremental process:
Early suspicion
Clinical diagnosis
Laboratory confirmation
“ –is now pyrexial”
“wbc differential shows-”
“Chest Xray back as –”
“nurse found that the family had recently returned from –”
“PCR now suggests -”

EvaluateEvaluate
A B CD E
Implementing appropriate infection control should not bean incremental process.Just do it!!!
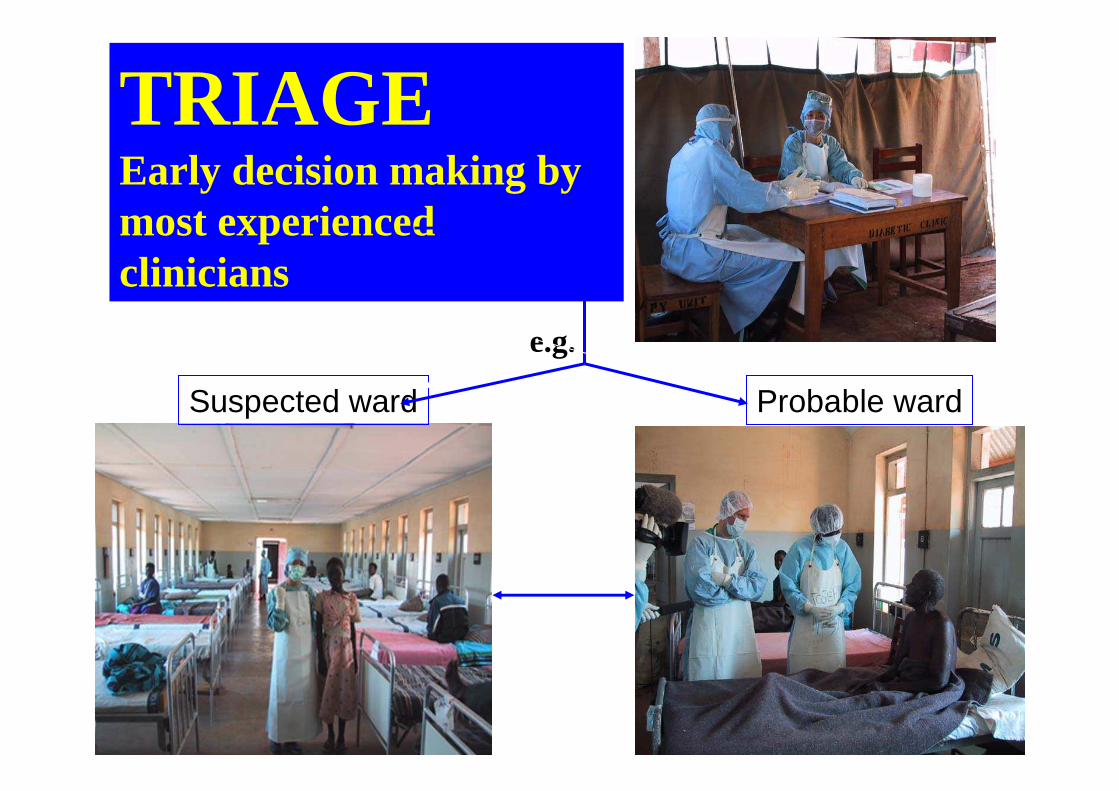
TRIAGE Early decision making by most experienced clinicians
Suspected ward Probable ward
e.g.

or
or
or
Case Definition in Triage usually too broad
1. Fever and History of Contact*
2. Feverand 3 or more symptoms:Headache, Vomiting, Loss of appetite,Diarrhea, Weakness, Abdominal pain,Body aches, dysphagia, dyspnea,Hiccoughs
3. Unexplained bleeding of any kind4. Any unexplained death
*Sleeping in the same household within one month*Direct physical contact with the case (dead or alive)
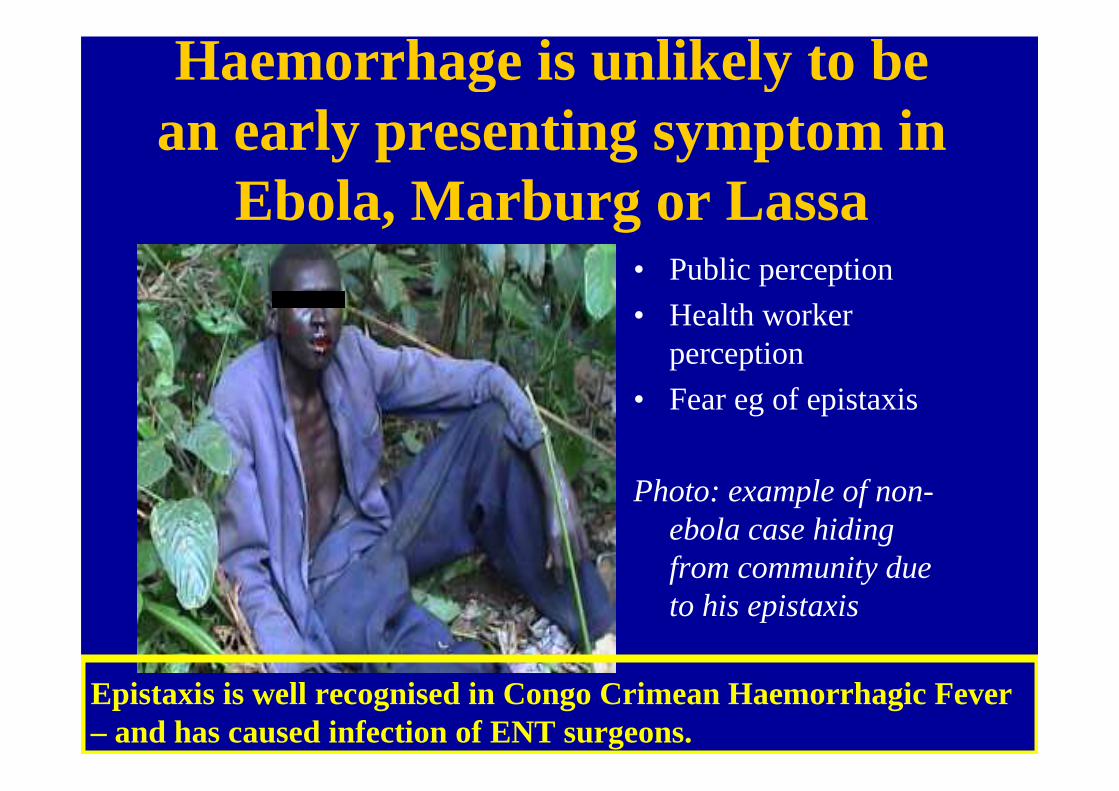
Haemorrhage is unlikely to be an early presenting symptom in
Ebola, Marburg or Lassa• Public perception
• Health worker perception
• Fear eg of epistaxis
Photo: example of non-ebola case hiding from community due to his epistaxis
Epistaxis is well recognised in Congo Crimean Haemorrhagic Fever – and has caused infection of ENT surgeons.

Clinical challenges for Lassa
Recognition of Lassa in paediatric age group.
Infection control especially difficult in paediatric care.
Intensive care to maintain intra vascular volume, electrolytes especially potassium, airway, oxygenation and reduce intracranial pressure.

Sierra LeoneGeneral Paediatrics and Lassa
unit 2004• Sharing of IV vials, syringes, diluent
on paed. ward especially under 5s• Increase in paediatric cases accounted
for 46% of cases admitted to Lassa ward Jan-March 2004
• Paediatric ward volunteer nurse died 17th March
• Dr Conteh sustained needlesticktreating her and died on 4th April Lassa diagnosis confirmed
• Head nurse of Lassa ward diagnosed probable Lassa
Cha
in o
f tra
nsm
issi
on
Sta
ff tr
eatin
g co
lleag
ues
Demonstration slide of ICU
A patient with VHF e.g. with circulatory shock and respiratory distress would be admitted to acute wards (or ICU where these facilities exist e.g. UK).
Staff, other patients and relatives would be at great risk of nosocomial spread.

- or on a crowded medical ward.
Mission hospitals have often featured in nosocomialamplification.
Could this be due to more intense style of care e.g. nursing?

“NON – SPECIFIC”
• Fever >38 C (axillary) but inconsistent in Triage
• Headache• Muscle and joint pain but often unlike the
patients experience of malaria• Sore throat• Weakness but profound and unlike malariai.e. Detail is necessary if these are to be used in
screening

• Unable to sit up• Unable to drink• Unable to use vomit bowl or latrine• (Unable to talk)
• ? Exacerbated by K+K+K+K+
Incapacitated patients - further contributes to: dehydration (later shock) and infectivity
Severe Severe Severe Severe progressiveprogressiveprogressiveprogressive weaknesweaknesweaknesweaknesssss
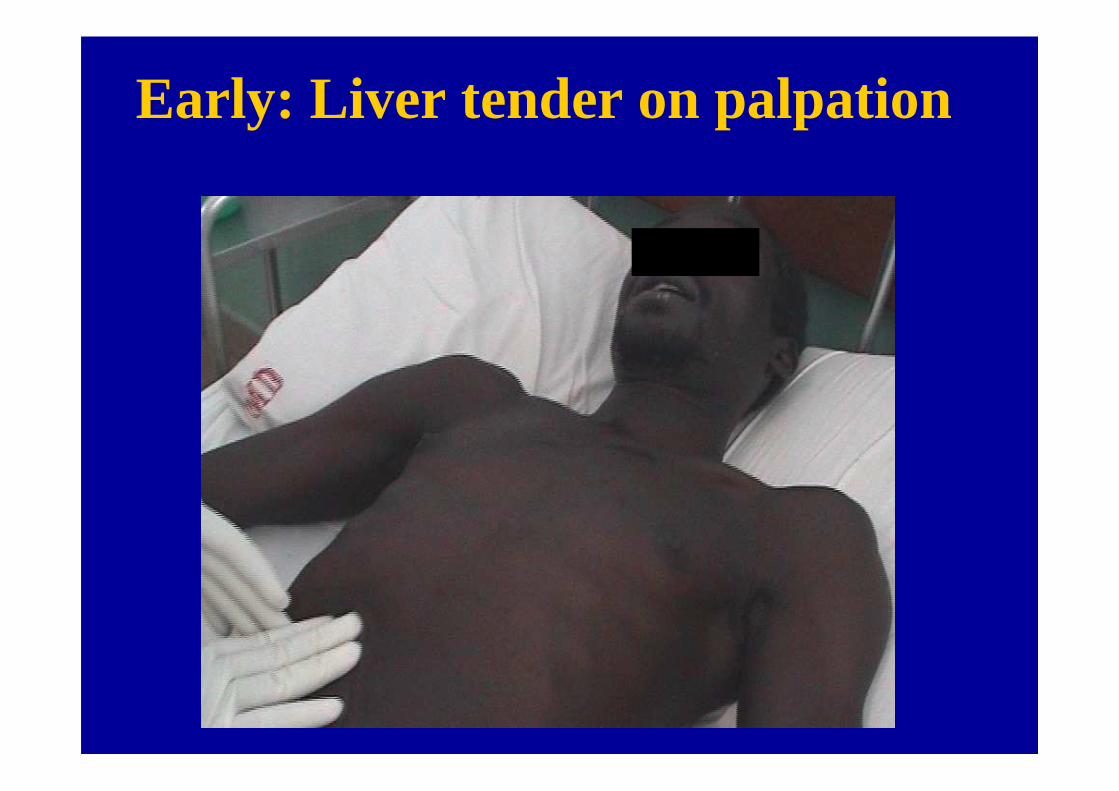
Early: Liver tender on palpation

Liver edge may become palpable

Increasingly tender each day

8-10 days: pain on percussion of Right lower ribs – in severe cases
EvaluateEvaluate
A B CD E

Picture from the movie Outbreak
Pictures of Pictures of barriers that barriers that spread fearspread fear

Pictures that Pictures that spread calmspread calm
Ebola survivorEbola survivor
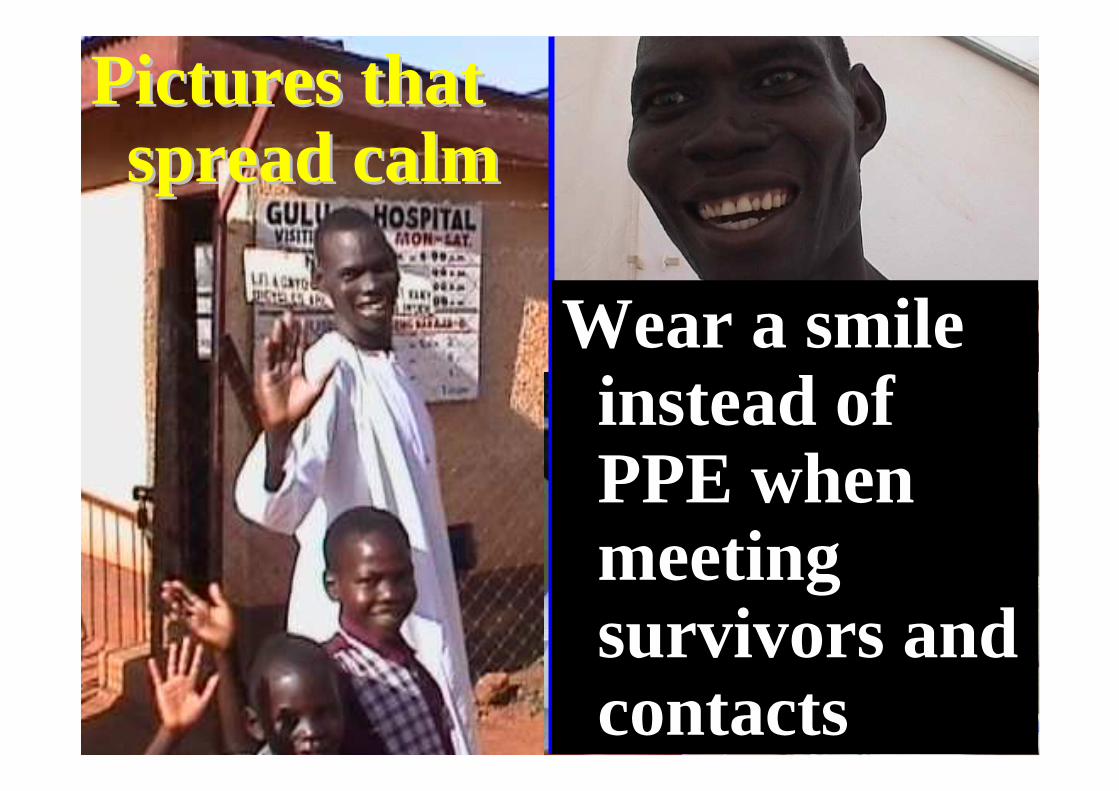
Pictures that Pictures that spread calmspread calm
Wear a smile Wear a smile instead of instead of PPE when PPE when meeting meeting survivors and survivors and contactscontacts

� Amplification of transmission
� Rapid international spread
� Cases reported by 26
�countries
�Challenge to international community
� $US30-140 billion economic cost
� Health systems exhausted
““ I felt naked without my maskI felt naked without my mask””
SARSSARS
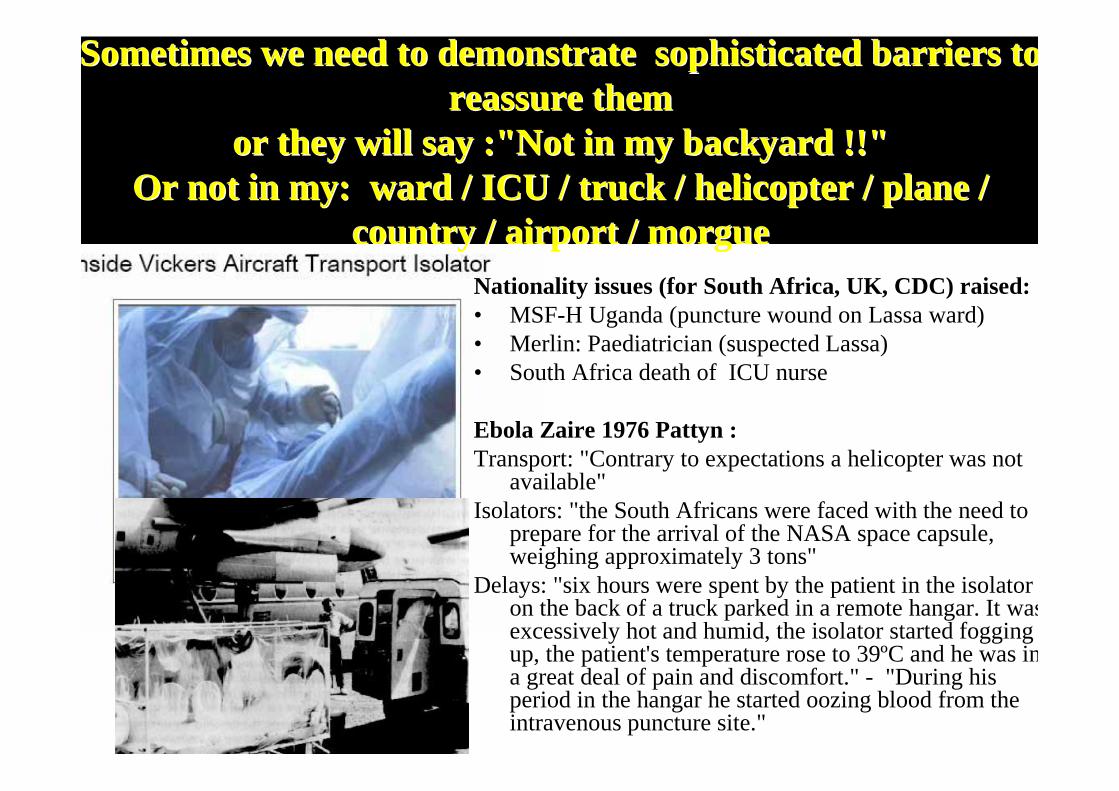
Sometimes we need to demonstrate sophisticated barriers to Sometimes we need to demonstrate sophisticated barriers to reassure them reassure them
or they will say :"Not in my backyardor they will say :"Not in my backyard !!"!!"Or not in my: Or not in my: ward / ICU / truck / helicopter / plane / ward / ICU / truck / helicopter / plane /
country / airport / morguecountry / airport / morgueNationality issues (for South Africa, UK, CDC) raised:• MSF-H Uganda (puncture wound on Lassa ward)• Merlin: Paediatrician (suspected Lassa)• South Africa death of ICU nurse
Ebola Zaire 1976 Pattyn :Transport: "Contrary to expectations a helicopter was not
available"Isolators: "the South Africans were faced with the need to
prepare for the arrival of the NASA space capsule, weighing approximately 3 tons"
Delays: "six hours were spent by the patient in the isolator on the back of a truck parked in a remote hangar. It was excessively hot and humid, the isolator started fogging up, the patient's temperature rose to 39ºC and he was in a great deal of pain and discomfort." - "During his period in the hangar he started oozing blood from the intravenous puncture site."
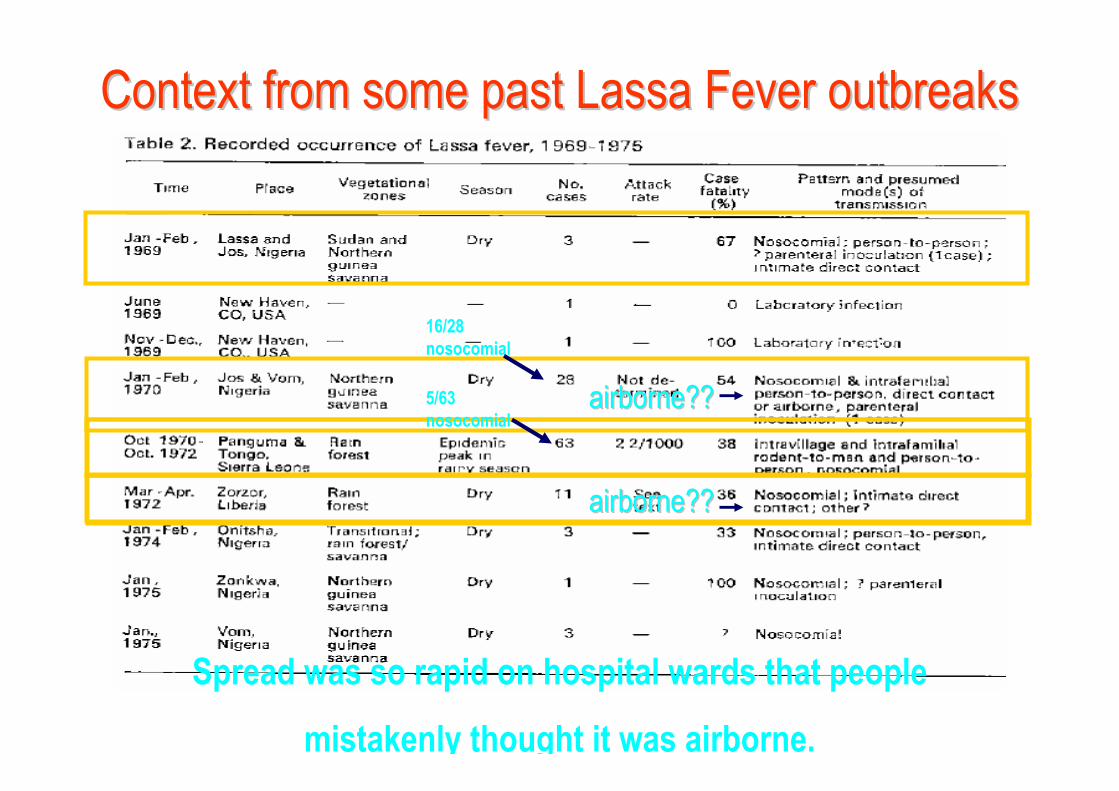
Spread was so rapid on hospital wards that people
mistakenly thought it was airborne.
Context from some past LassaContext from some past Lassa Fever Fever outbreaksoutbreaks
airborneairborne????
16/28
nosocomial
airborneairborne????
5/63
nosocomial

e.g. too weak to sit up
Vomiting, dehydrated, unable to use bowl

Diarrhoea incontinent

Research and development in respiratory protection
Further research
required for SARS:Surgical
masks
N95, N series filter
at least 95%
efficient,
99 or N100 or
*equivalent
Fit
testing
*Equivalent: or comparable national/regional standards applicable to the country of manufacture
•Remember user seal check if using a respirator•Avoid inappropriate use•Read/ discuss with manufacturer
N refers to not resistant to oil
EvaluateEvaluate

Collection of (multiple) specimensrisk of such procedures
Clear benefit to knowledge, sometimes might not alter management of individual case.
Public health requirement for specimens, Dr Carlo Urbani possibly infected while taking such samples.
High risk from advanced diagnostic procedures e.g. sampling for respiratory specimens
• Photo ICU in the UK
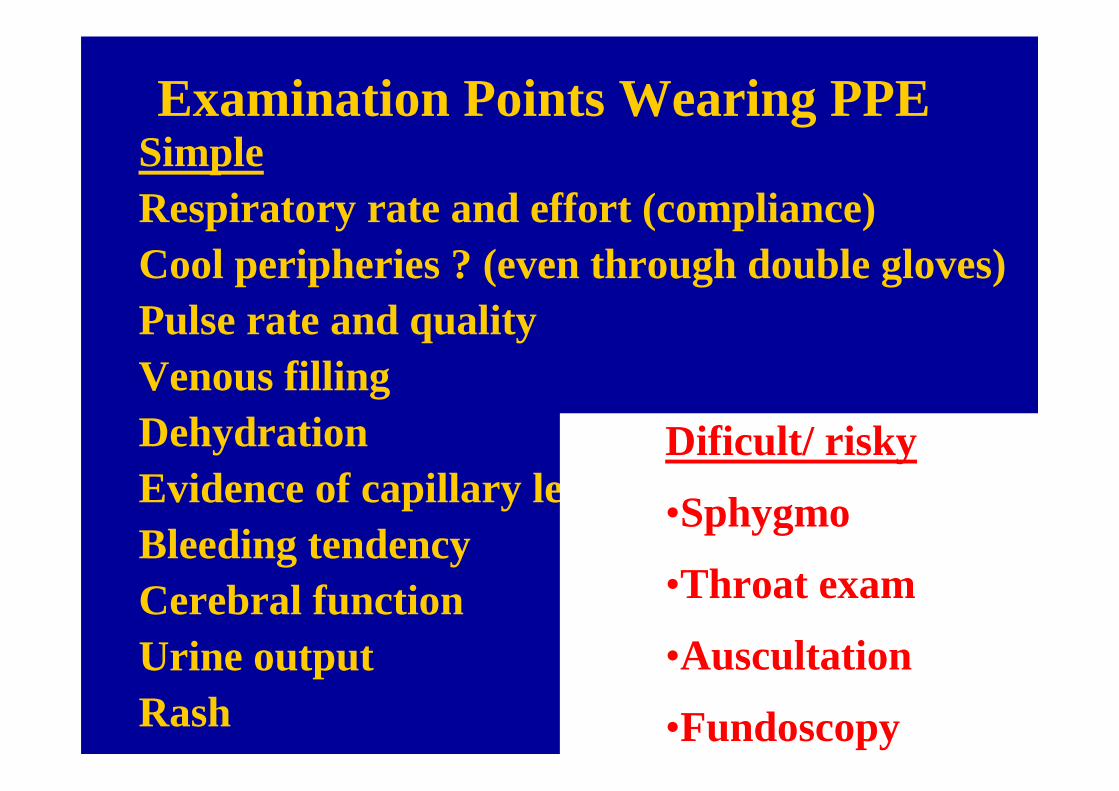
Examination Points Wearing PPESimpleRespiratory rate and effort (compliance)Cool peripheries ? (even through double gloves)Pulse rate and qualityVenous fillingDehydrationEvidence of capillary leakBleeding tendencyCerebral functionUrine outputRash
Dificult/ risky
•Sphygmo
•Throat exam
•Auscultation
•Fundoscopy

Eye protection: why is compliance so low?

E.g. Anti fog drops or goggles which do not fog are available

USE A BUDDY OR A MIRROR
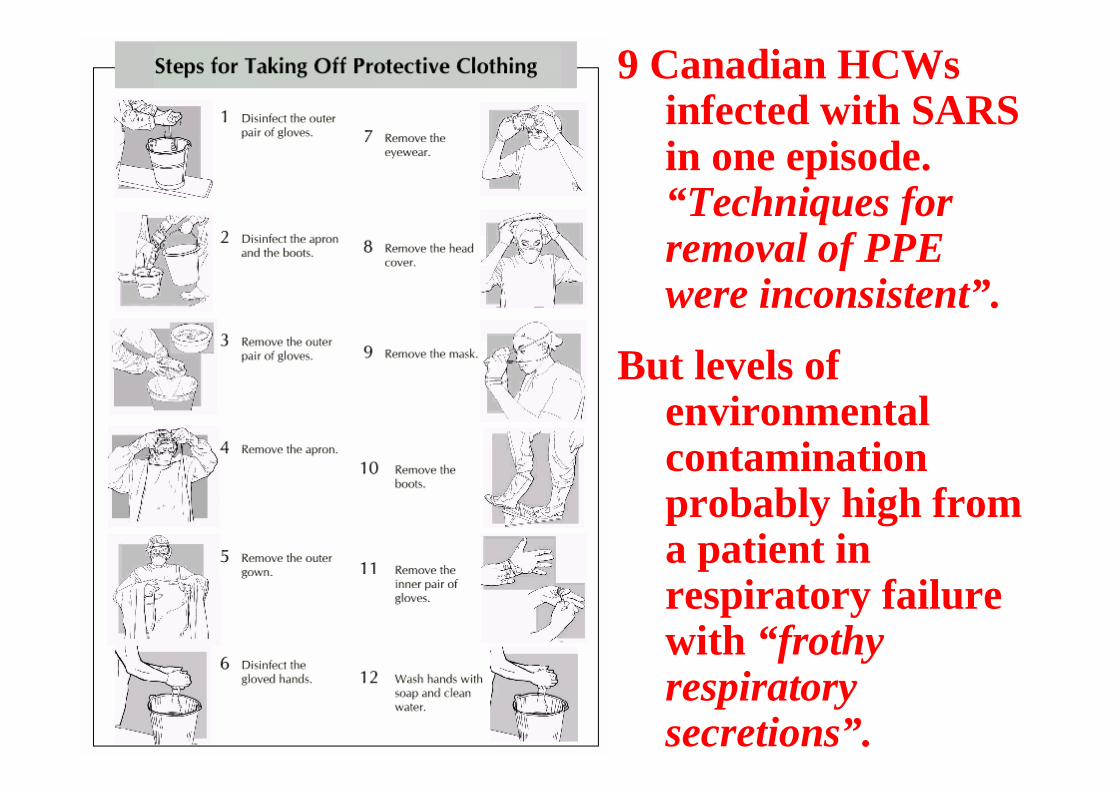
9 Canadian HCWsinfected with SARS in one episode. “Techniques for removal of PPE were inconsistent”.
But levels of environmental contamination probably high from a patient in respiratory failure with “frothy respiratory secretions” .
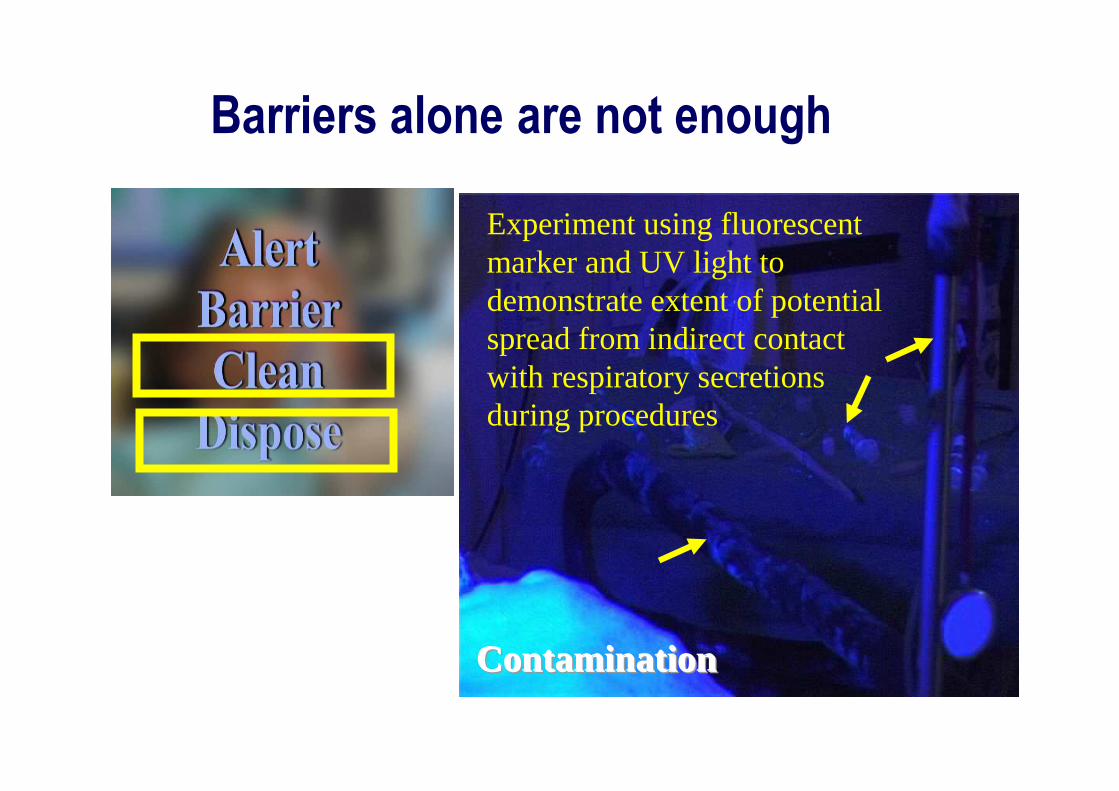
Barriers alone are not enough
Experiment using fluorescent marker and UV light to demonstrate extent of potential spread from indirect contact with respiratory secretions during procedures
ContaminationContaminationContamination

EvaluateEvaluate
A B CD E

Handwashing, handwashing & handwashing
Alcohol based hand hygiene products still require facilities to have access to water for cleaning.

Cleaning and disinfectionHands Environment Laundry
One ward 500litres/day of 1/100
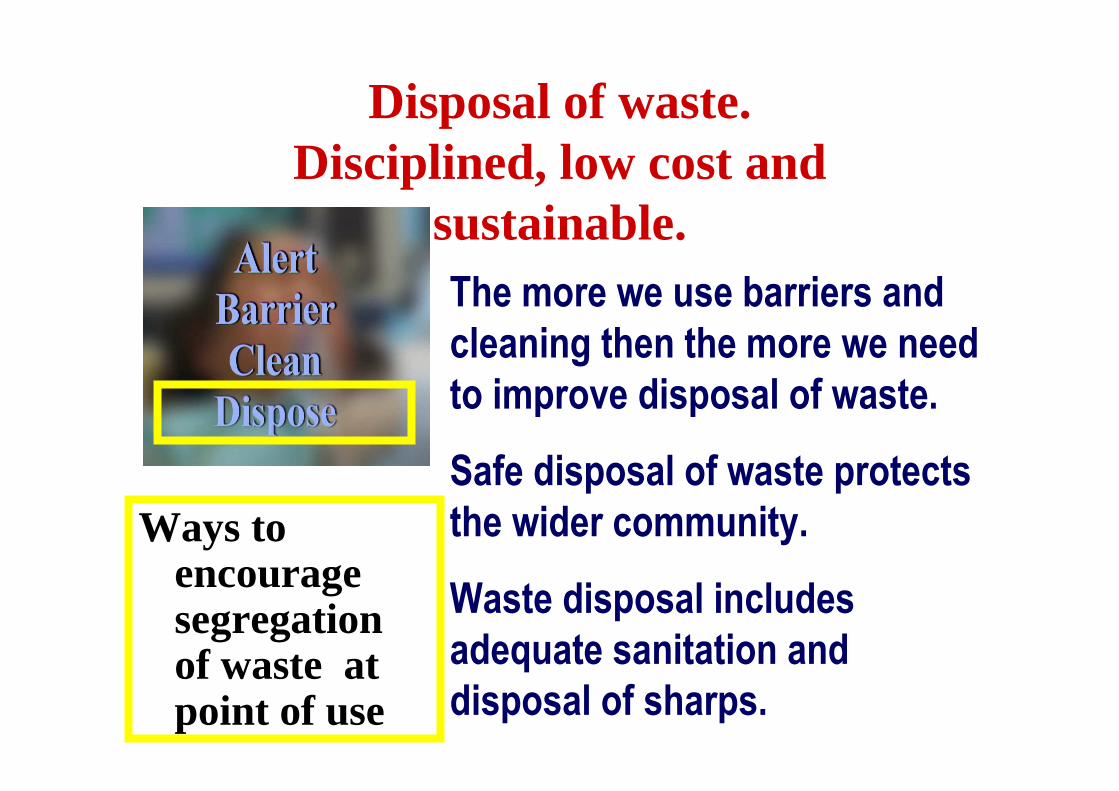
Disposal of waste. Disciplined, low cost and
sustainable.The more we use barriers and
cleaning then the more we need
to improve disposal of waste.
Safe disposal of waste protects
the wider community.
Waste disposal includes
adequate sanitation and
disposal of sharps.
Ways to encourage segregation of waste at point of use
EvaluateEvaluate
A B CD E

1. PROTECT staff
2. PROTECT caregiver
3. PROTECT other suspect patients
4. Treat with ORAL REHYDRATION
5. Treat with IV REHYDRATION and other parenteral therapy
6. INTENSIVE CARE
Large Isolation UnitLarge Isolation UnitPRIORITY SETTINGPRIORITY SETTINGTO PREVENT TO PREVENT NOSOCOMIAL NOSOCOMIAL AMPLIFICATIONAMPLIFICATION
PROTECT other caregivers
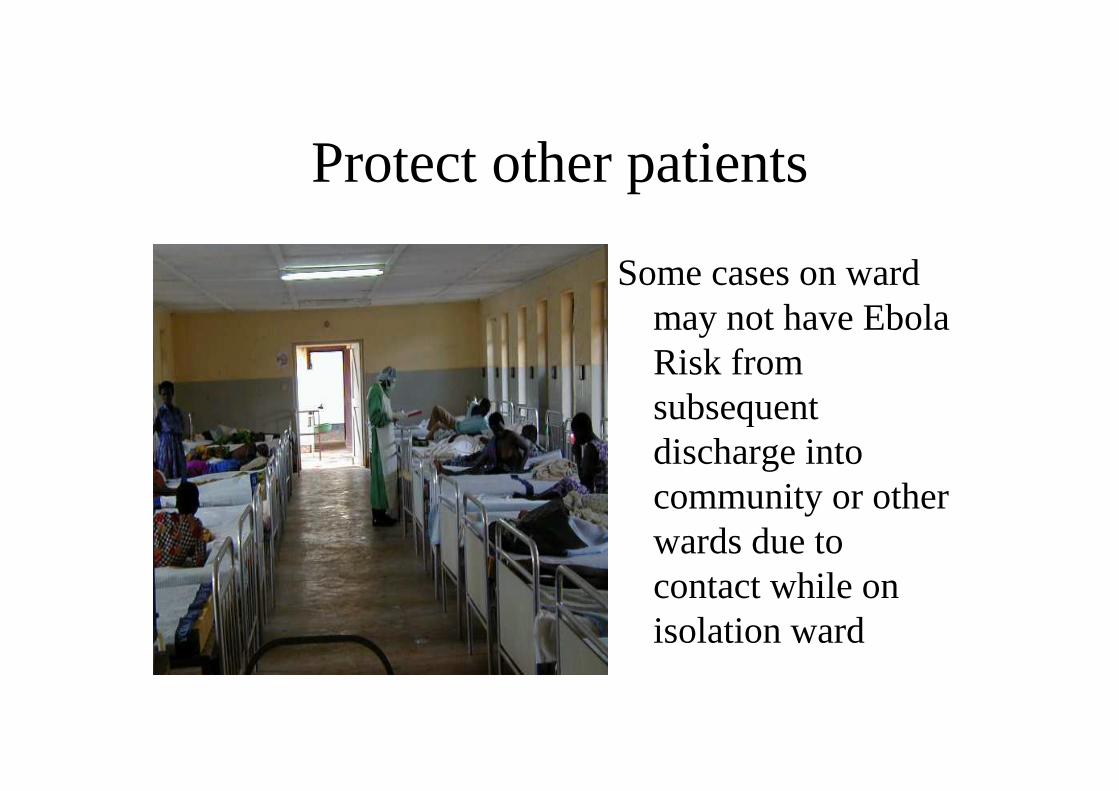
Protect other patients
Some cases on ward may not have Ebola Risk from subsequent discharge into community or other wards due to contact while on isolation ward
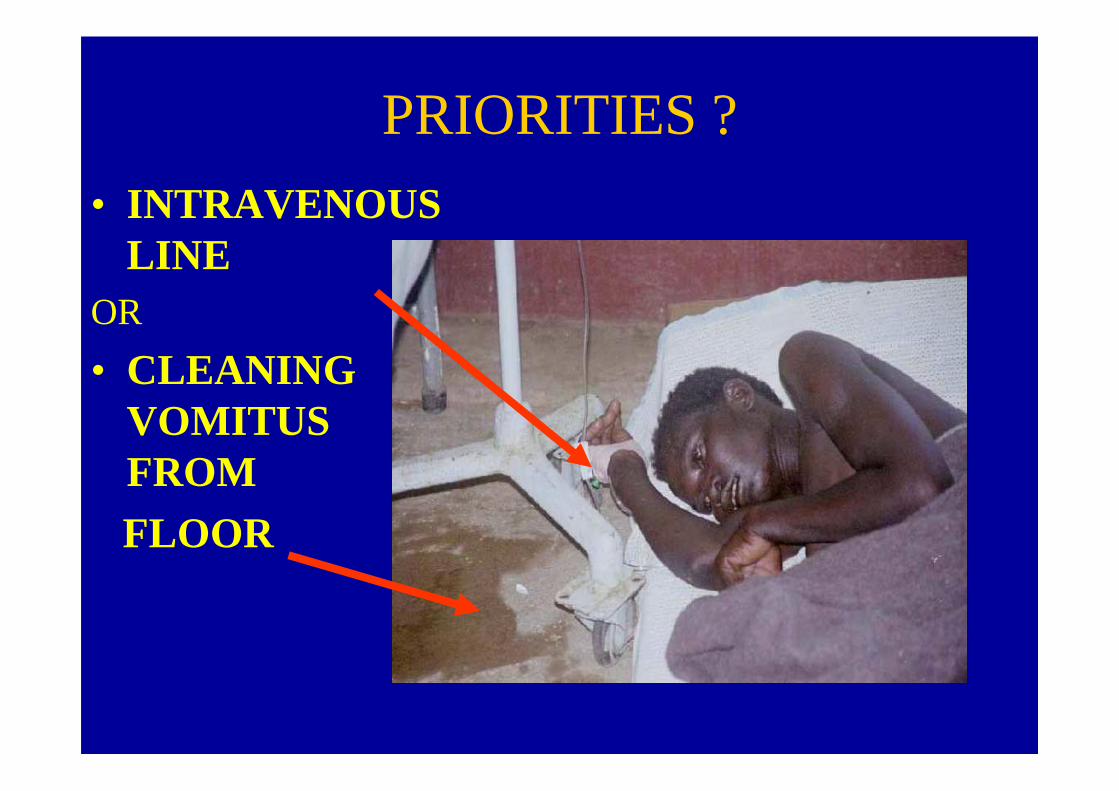
PRIORITIES ?
• INTRAVENOUS LINE
OR
• CLEANING VOMITUS FROM FLOOR

5 days: weakness usually severe
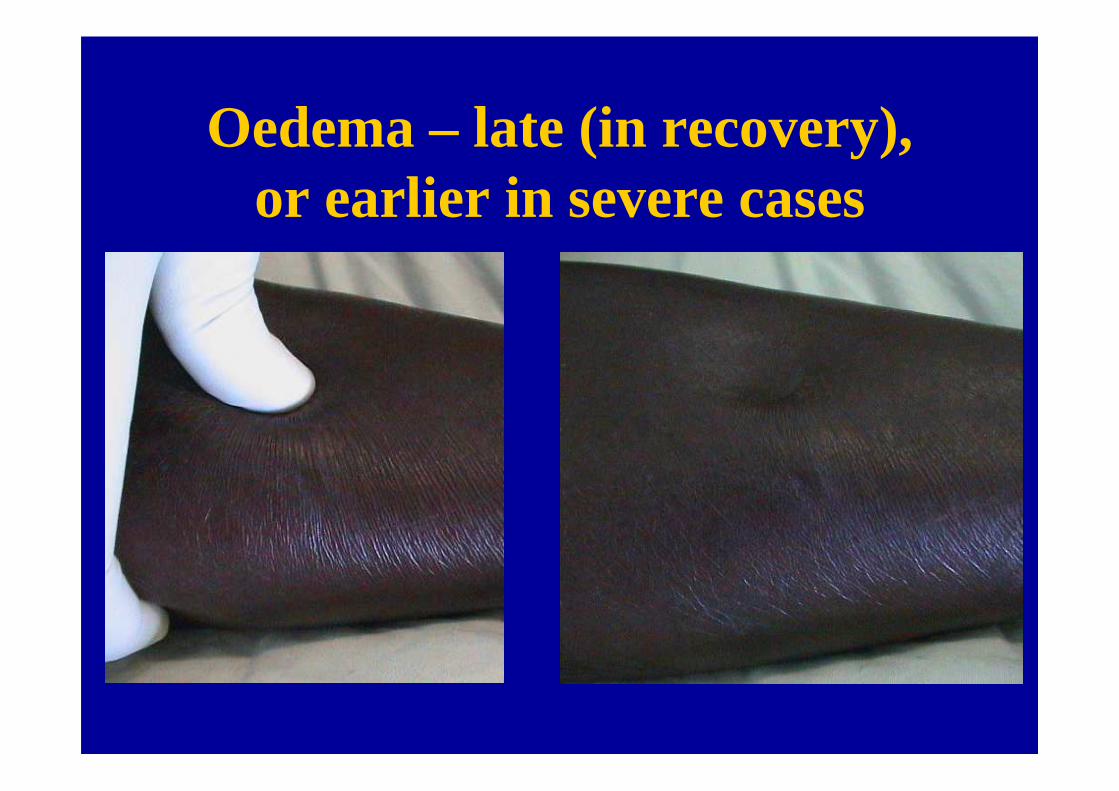
Oedema – late (in recovery), or earlier in severe cases
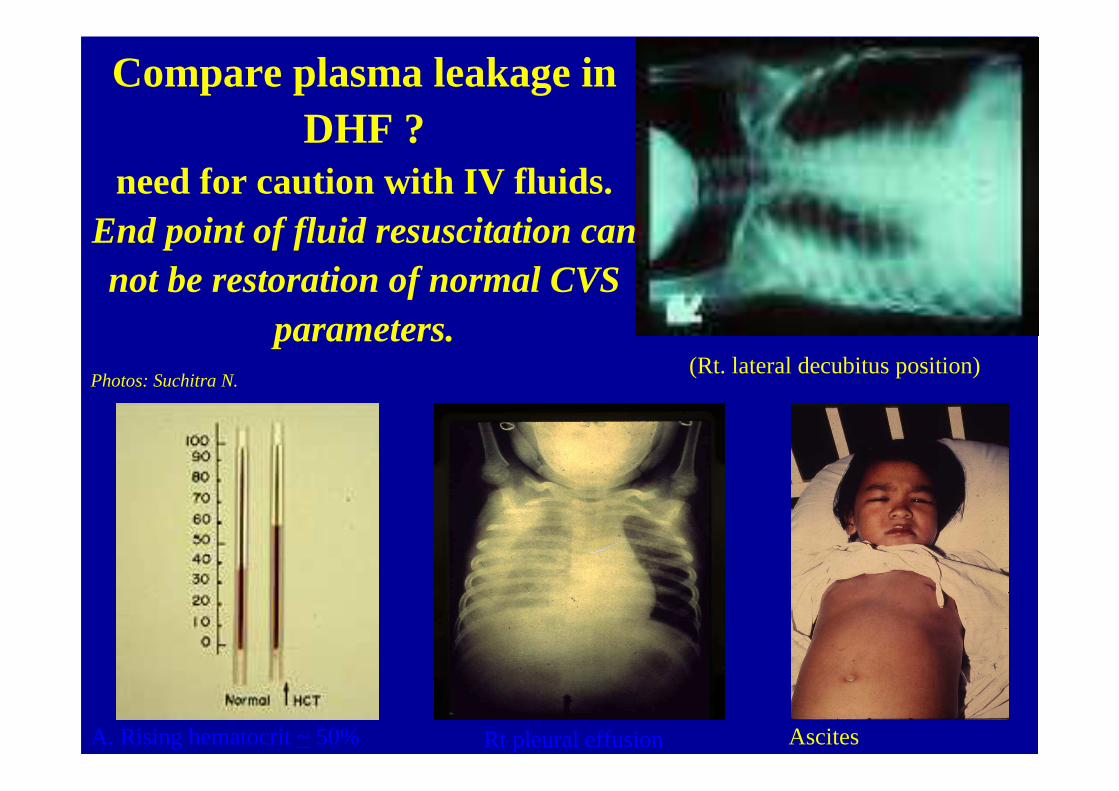
A. Rising hematocrit ~50%
Compare plasma leakage in DHF ?
need for caution with IV fluids.End point of fluid resuscitation can not be restoration of normal CVS
parameters.(Rt. lateral decubitus position)
Rt pleural effusion Ascites
Photos: Suchitra N.

Thank Thank you.you.
Treatment Summary slide
KiplingBarrack room ballad.Where would I be when the bullets fly?
Where will I be when I come to die?
Why, somewhere anigh my chum.
If he he’s liquor he’ll give me some.
If I’m dying he’ll hold my head,
And he’ll write ‘em home when I’m dead.
Gawd send us a trusty chum!
MardelIsolation room balladWhere would I be with a DNP?
Why somewhere anigh my mum.If I need fluid she’ll give me someWith a cup, spoon and potassium.
But if theres signs of capillary leak,Its not IV fluids I want that week
‘Cos they’ll just make my lungs all wetWhen I need all the O2 I can get.
So we don’t always need some drip stands,But Gawd help my mum keep clean hands.