prostata: diagnosis and treatment of localized and locally...
TRANSCRIPT

Prostata: Diagnosis and treatment of localized
and locally advanced prostate cancer
Oral Communications
Elisa Zanardi UOC Clinica di Oncologia Medica Ospedale Policlinico San Martino
Dipartimento di Medicina interna e Specialità mediche (DiMI) Genova
Milano, 02/03/2018

Oral abstracts
• Ten years final results of the TR.OG 03.04 (RADAR) randomised phase 3 trial evaluating duration of androgen suppression +/- zoledronic acid for locally advanced prostate cancer. David J. Joseph et al.
• Daily versus weekly prostate cancer image-guided radiotherapy: a phase 3 randomised trial. R. de Crevoisier et al.
• Transciptomic eterogeneity of androgen receptor activity in primary prostate cancer: identification and characterization of a low-AR active subclass. Daniel Spratt et al.

Oral abstracts
• Ten years final results of the TR.OG 03.04 (RADAR) randomised phase 3 trial evaluating duration of androgen suppression +/- zoledronic acid for locally advanced prostate cancer. David J. Joseph et al.
• Daily versus weekly prostate cancer image-guided radiotherapy: a phase 3 randomised trial. R. de Crevoisier et al.
• Transciptomic eterogeneity of androgen receptor activity in primary prostate cancer: identification and characterization of a low-AR active subclass. Daniel Spratt et al.

Background
• Long term adjuvant AS is more effective
than short term neo-adiuvant AS
• Prolonged AS is related to several complications: sexual dysfunction, gynaecomastia, hot flushes, weight gain, sarcopenia, loss of bone mineral density, fractures, anaemia, prolonged fatigue, prolonged hypogonadism, cognitive dysfunction, depression, the metabolic syndrome, myocardial infarctions
RTOG 92.02 (USA)
EORTC 22961 (Europe)

Objective
To develop a treatment that:
• Has side effects no worse than «short course» AS
• Is as effective as «long course» AS
An intermediate duration of AS (18 months) looked like a good option
In association with Zoledronic Acid:
• A drug that increase bone mineral density • Kills cancer cells in bone • Has a low side effect profile

Trial demographics Eligibility
• T2-T4, N0, M0; ECOG <2
(T2a provided PSA ≥10 and Gleason Score ≥7 )
Enrolment
• 1071 men
• Median age 68.7 years
• Median follow up 10.4 years
• Risk classification (MSK): high (66%); unfav. intermediate (31%); fav. Intermediate (2%)
End Points Main endpoint
• Prostate cancer-specific mortality
Secondary enpoints
• Oncologic endpoints (PSA progression, sites of tumor progression; castratin resistance; secondary therapeutic intervention; all cause mortality)
• Quality of life
• Adverse treatment effects

Results (1) PCSM: primary endpoint
A 29% reduction in distant progression was the main driver of the 30% reduction of PCSM

Results (2): Secondary endpoints

Cause of death by AS duration
Quality of life by AS duration

ZA vs no ZA: Oncological endpoints
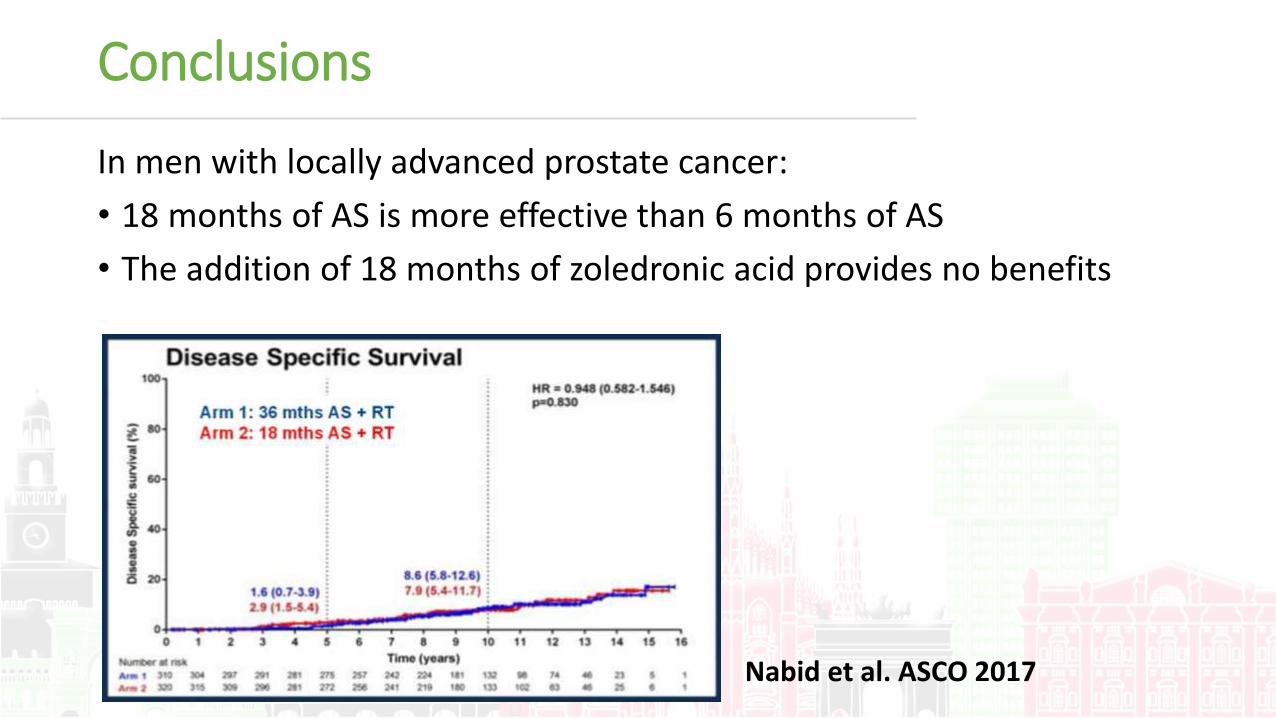
Conclusions
In men with locally advanced prostate cancer:
• 18 months of AS is more effective than 6 months of AS
• The addition of 18 months of zoledronic acid provides no benefits
Nabid et al. ASCO 2017
Oral abstracts
• Ten years final results of the TR.OG 03.04 (RADAR) randomised phase 3 trial evaluating duration of androgen suppression +/- zoledronic acid for locally advanced prostate cancer. David J. Joseph et al.
• Daily versus weekly prostate cancer image-guided radiotherapy: a phase 3 randomised trial. R. de Crevoisier et al.
• Transciptomic eterogeneity of androgen receptor activity in primary prostate cancer: identification and characterization of a low-AR active subclass. Daniel Spratt et al.
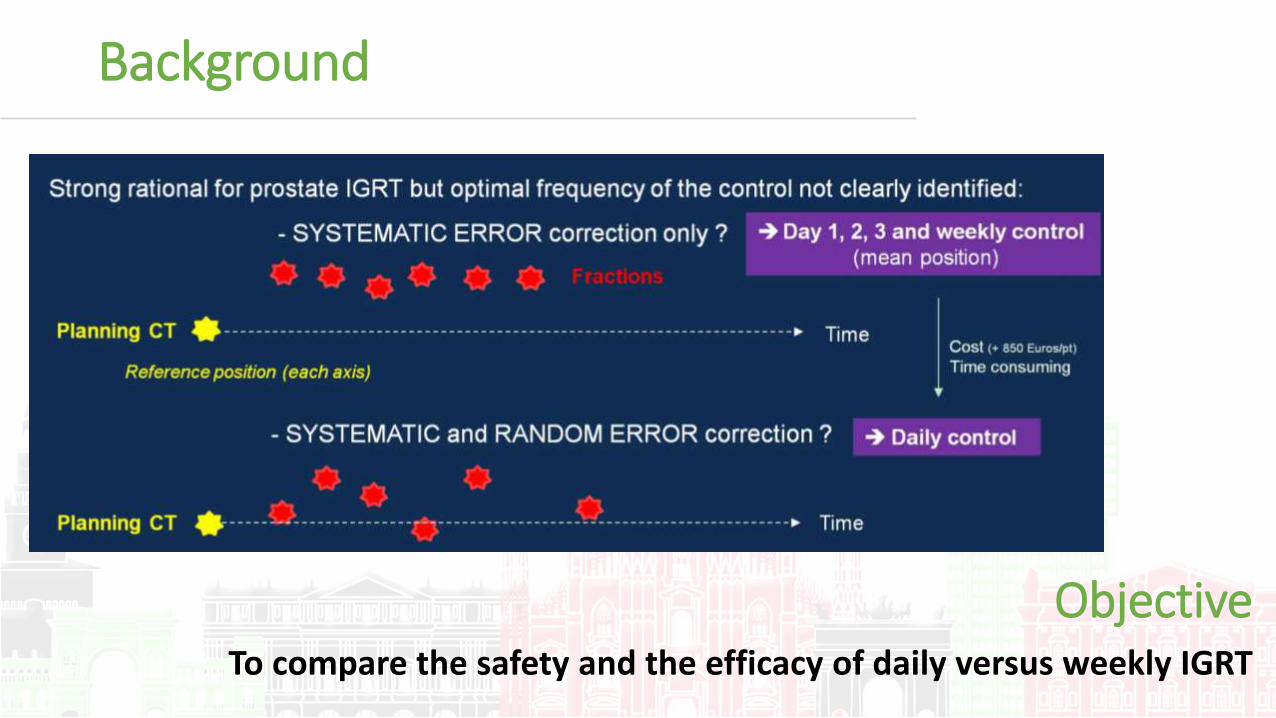
Background
Objective To compare the safety and the efficacy of daily versus weekly IGRT

Characteristics of patients and treatment
Inclusion criteria • Intermediate and high risk localized prostate
cancer
• Total dose = 70-80 Gy (+ ADT for high risk)
• 3DCRT o IMRT (PTV margins 1cm / 5 mm post)
• Pelvic lymph node not irradiated
• IGRT modalities = by direct (CBCT) or indirect proste visualization (fiducials + 2DkV imaing)

Results
DFS: primary endpoint Biochemical recurrence: secondary endpoint

Toxicity: Secondary endpoints
Overall survival: Secondary endpoints

Conclusions Second cancer incidence: post hoc analysis
In men with locally advanced prostate cancer:
• Compared to weekly control, by improving targeting, daily control in prostate cancer IGRT significantly decrease the risks of recurrence and rectal toxicity but is associated with an increased risk of second cancer.
• Longer follow-up is however clearly needed to assess the rate of radiation-associated malignancies

Oral abstracts
• Ten years final results of the TR.OG 03.04 (RADAR) randomised phase 3 trial evaluating duration of androgen suppression +/- zoledronic acid for locally advanced prostate cancer. David J. Joseph et al.
• Daily versus weekly prostate cancer image-guided radiotherapy: a phase 3 randomised trial. R. de Crevoisier et al.
• Transciptomic eterogeneity of androgen receptor activity in primary prostate cancer: identification and characterization of a low-AR active subclass. Daniel Spratt et al.

Background
AR amplifications/mutations are the most common actionable alteration in mCRPC
AR and AR-Activity (AR-A) is heterogeneus in mCRPC: strong
correlation between AR and AR-A
In primary localized prostate the significance of AR-activity diversity is unknown
Objective
To understand the biological and clinical relevance of AR- activity heterogeneity in localized prostate cancer

Methods
Identification of a distinct subclass of low AR-A adenocarcinomas

Results (1)
AR-A associated with distinct cancer hallmarks
Low AR-A tumors have increased immuno-stimulatory properties

Low AR-A tumors have decreased DNA repair and increased predicted radiation sensitivity
Low AR-A tumors have increased NEPC expression and are more basal-like
Results (2)
Radiation sensitivity (PORTOS)

High AR and Low AR-A tumors have highest metastatic potential
Low AR-A tumors have increased rate
of distant metastasis
Results (3)

Clinically, tumors that develop CRPC have lower AR-A
Low AR-A tumors have unique drug sensitivities
Results (4)

Conclusions
1. AR-A is heterogeneuous in localized prostate cancer
10-15% of localized prosate adenocarcnoma have low AR-A
2. Low AR-A tumors have decreased DNA repair expression, a proimmune phenotype, and increased markers of NEPC
3. Clinically, low AR-A tumors are more likely to develop metastases
4. Low AR-A tumors appear more sensitive to XRT, PARPi, and platinum chemotherapy and less sensitive to taxanes and ADT
Biomarker enhanced trials in development

Oral abstracts
• Ten years final results of the TR.OG 03.04 (RADAR) randomised phase 3 trial evaluating duration of androgen suppression +/- zoledronic acid for locally advanced prostate cancer. David J. Joseph et al.
• Daily versus weekly prostate cancer image-guided radiotherapy: a phase 3 randomised trial. R. de Crevoisier et al.
• Transciptomic eterogeneity of androgen receptor activity in primary prostate cancer: identification and characterization of a low-AR active subclass. Daniel Spratt et al.