proefschift bron
TRANSCRIPT
Uitnodiging
Novel Regenerative Strategies For The Treatment Of
Intervertebral Disc Herniation
Dinsdag 27 november 2012 om 15:45
in het auditorium van het hoofdgebouw van de
Vrije Universiteit De Boelelaan 1105 Amsterdam
Harry BronWijsmullerstraat 41-21058 JH Amsterdam
Paranimfen:Fleur Joor
Gert van den [email protected]
door:JL Bron
voor het bijwonen van de openbare verdediging van het proefschriftNovel Regenerative Strategies
For The Treatment Of Intervertebral Disc Herniation
JL Bron
Novel Regenerati
ve Strategies For The Treatment O
f Intervertebral Disc H
erniation
JL Bron
Novel Regenerative Strategies
For The Treatment Of
Intervertebral Disc Herniation
Johannes Leendert Bron
The studies described in this thesis are carried out at the department of orthopaedic surgery of the VU University Medical Center (VUMC), the department of oral cell biology of the Academic Centre for Dentistry (ACTA) and the FOM Institute for Atomic and Molecular Physics (AMOLF). The study was financially supported by Arthro Kinetics Ltd, Germany. The publication of this thesis was supported by: - Nederlandse Orthopaedische Vereniging - Stichting Anna Fonds - Skeletal Tissue Engineering Group Amsterdam - Dutch Spine Society - Bauerfeind - Implantcast - Inspine - DSM Biomedical Novel regenerative strategies for the treatment of intervertebral disc herniation Copyright © 2012 JL Bron, Amsterdam, The Netherlands Lay out: JL Bron Cover design: JL Bron & G van den Berg Print: Gildeprint Drukkerijen – Enschede ISBN:
VRIJE UNIVERSITEIT
Novel Regenerative Strategies
For The Treatment Of
Intervertebral Disc Herniation
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad Doctor aan
de Vrije Universiteit Amsterdam,
op gezag van de rector magnificus
prof.dr. L.M. Bouter,
in het openbaar te verdedigen
ten overstaan van de promotiecommissie
van de Faculteit der Geneeskunde
op dinsdag 27 november 2012 om 15.45 uur
in het auditorium van de universiteit,
De Boelelaan 1105
door
Johannes Leendert Bron
geboren te Leerdam
promotoren: prof.dr. B.J. van Royen
prof.dr.ir. Th.H. Smit
copromotor: prof.dr. G.H. Koenderink

Table of Contents
Chapter 1 General Introduction 7
Chapter 2 Rheological characterization of the nucleus pulposus 15
and dense collagen scaffolds intended for functional
replacement.
J Orthop Res. 2009; 27: 260-266
Chapter 3 Engineering alginate for intervertebral disc repair 31
J Mech Behav Biomed Mater. 2011; 4:1196-1205
Chapter 4 Migration of intervertebral disc cells into dense col- 57
lagen scaffolds intended for functional replacement
Mater Sci Mater Med. 2012; 23:813-821
Chapter 5 Repair, regenerative and supportive therapies of the 79
annulus fibrosus: achievements and challenges
Eur Spine J. 2009; 18:301-313
Chapter 6 Biomechanical and in vivo evaluation of experimental 109
closure devices of the annulus fibrosus designed for a
goat nucleus replacement model
Eur Spine J. 2010; 19:1347-1355
Addendum 1: Techniques and instruments 131
Addendum 2: Nucleus implant evaluation 137
Chapter 7 General discussion 149
Appendices 1. Summary 167
2. Nederlandse Samenvatting 171
3. Publications 177
4. Dankwoord 181
5. Curriculum Vitae 185

1 General Introduction

Chapter 1
8
Symptomatic lumbar disc herniation occurs in up to 2% of the general population
at some point in life [1]. Men are affected more often than woman, with a peak
incidence in the fourth and fifth decade of life [1,2]. Since the disease is mainly
distributed within the working and employed part of our society, the socio-
economic consequences are substantial [3]. In the vast majority of the patients
symptoms subside spontaneously within six weeks after presentation and these
patients are best off treated conservatively [2]. Another large part will experience
a decrease of symptoms in the following months and selection of patients suitable
for surgery is therefore still not without dispute [4]. Moreover, the results of
surgery are not always favourable in terms of outcome and recurrences [5].
Depending on the exact type and extent of the herniated disc rates of recurrence
(of pain), reherniation and reoperation can be as high as 38%, 27% and 21%
respectively [5]. It is therefore not surprising that advancements in knowledge,
imaging techniques and surgery are all continuously evaluated for their potential
in the development of better treatment strategies. In addition, during the past
decade a complete new area of research has evolved in medicine: Tissue
engineering. The latter yields a great promise for patients suffering from
symptomatic lumbar disc herniation and pioneering pre-clinical research is
presented in the current thesis.
Disc herniation
The spinal column combines its complex mechanical function with the protection
of the most delicate tissue our body harbours: the spinal cord. Failure to fulfil one
of its tasks will have dramatic consequences. The spinal column consists of the
bony vertebral bodies that articulate with each other by two facet joints
posteriorly and the intervertebral disc (IVD) anteriorly. The 33 vertebral bodies
are numbered according to their cranio-caudal position: cervical (7), thoracic (12),
Lumbar (5), sacral (5) and coccygeal (4). The spinal cord, or below the first lumbar
level the cauda equine, is located directly posterior of the IVD. Other borders are
the pedicles laterally and the laminae and flavum ligament posteriorly. Exiting
nerve roots leave the spinal canal via the intervertebral foramen, which is located
between two pedicles behind the posterolateral border of the IVD and anterior of
the facet joint.
General introduction
9
9
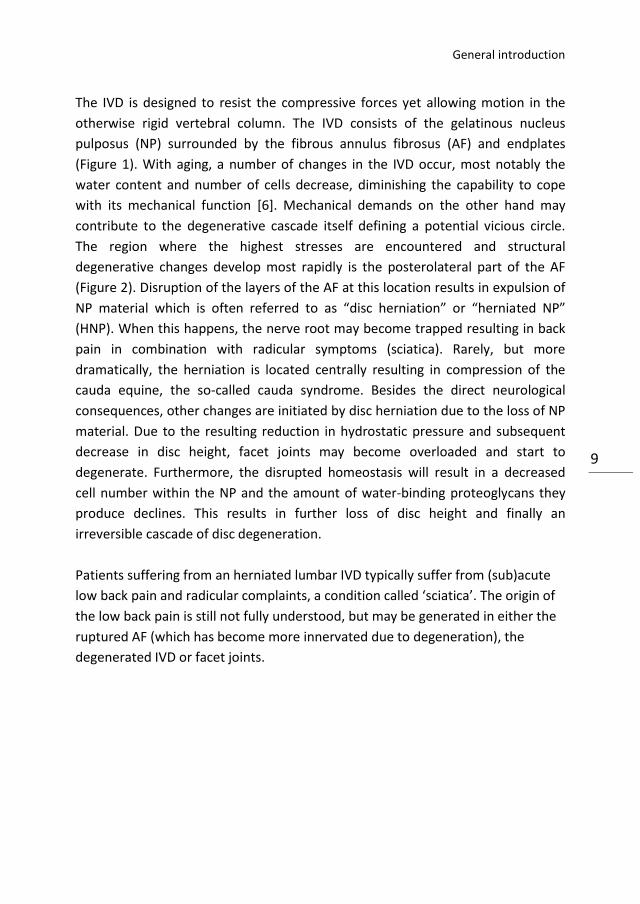
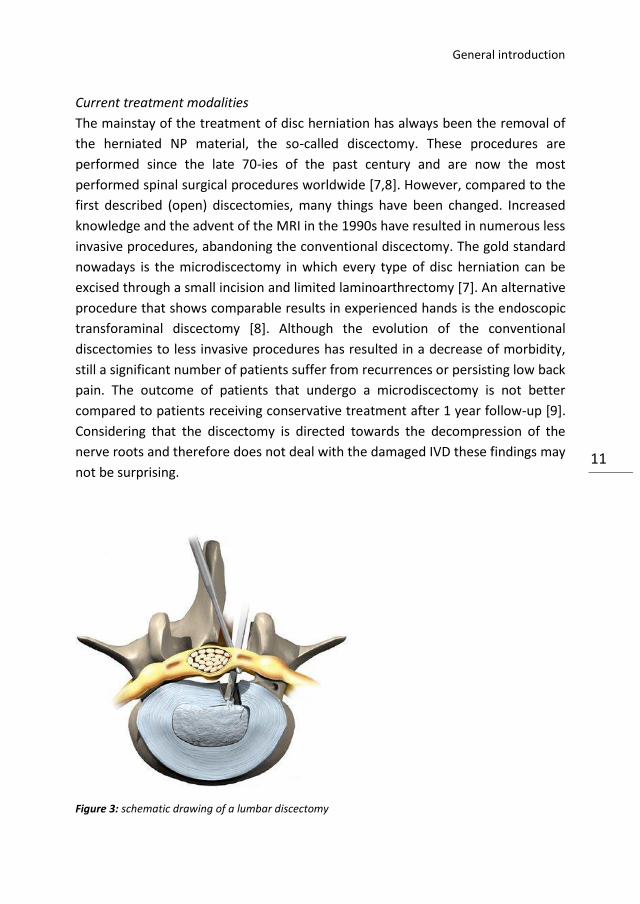
The IVD is designed to resist the compressive forces yet allowing motion in the
otherwise rigid vertebral column. The IVD consists of the gelatinous nucleus
pulposus (NP) surrounded by the fibrous annulus fibrosus (AF) and endplates
(Figure 1). With aging, a number of changes in the IVD occur, most notably the
water content and number of cells decrease, diminishing the capability to cope
with its mechanical function [6]. Mechanical demands on the other hand may
contribute to the degenerative cascade itself defining a potential vicious circle.
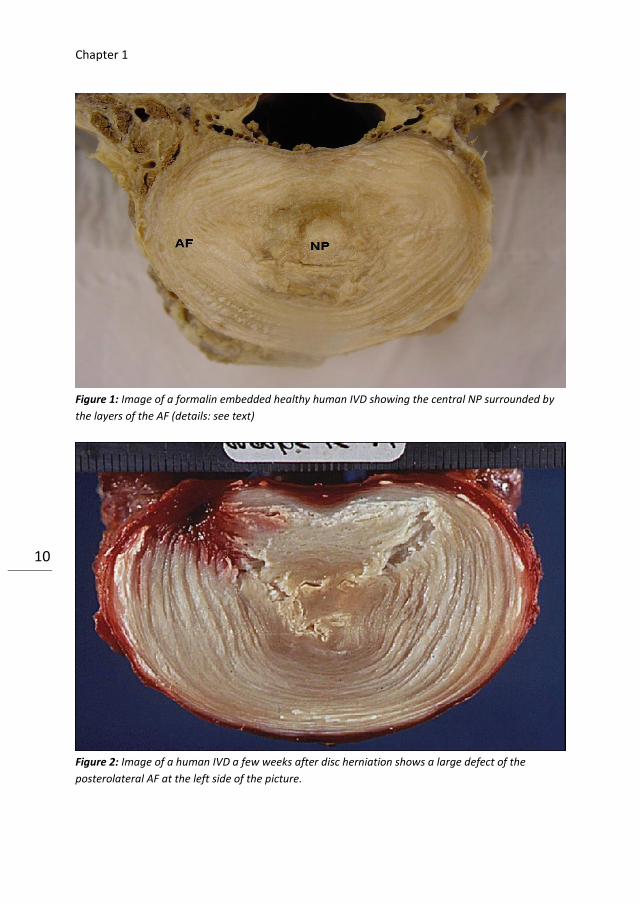
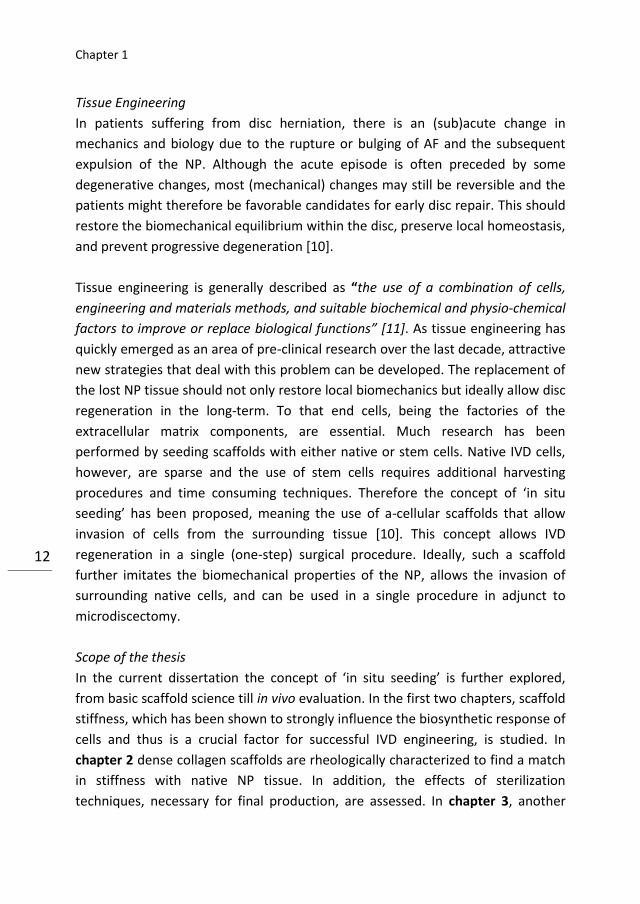
The region where the highest stresses are encountered and structural
degenerative changes develop most rapidly is the posterolateral part of the AF
(Figure 2). Disruption of the layers of the AF at this location results in expulsion of
NP material which is often referred to as “disc herniation” or “herniated NP”
(HNP). When this happens, the nerve root may become trapped resulting in back
pain in combination with radicular symptoms (sciatica). Rarely, but more
dramatically, the herniation is located centrally resulting in compression of the
cauda equine, the so-called cauda syndrome. Besides the direct neurological
consequences, other changes are initiated by disc herniation due to the loss of NP
material. Due to the resulting reduction in hydrostatic pressure and subsequent
decrease in disc height, facet joints may become overloaded and start to
degenerate. Furthermore, the disrupted homeostasis will result in a decreased
cell number within the NP and the amount of water-binding proteoglycans they
produce declines. This results in further loss of disc height and finally an
irreversible cascade of disc degeneration.
Patients suffering from an herniated lumbar IVD typically suffer from (sub)acute
low back pain and radicular complaints, a condition called ‘sciatica’. The origin of
the low back pain is still not fully understood, but may be generated in either the
ruptured AF (which has become more innervated due to degeneration), the
degenerated IVD or facet joints.
Chapter 1
10
Figure 1: Image of a formalin embedded healthy human IVD showing the central NP surrounded by
the layers of the AF (details: see text)
Figure 2: Image of a human IVD a few weeks after disc herniation shows a large defect of the
posterolateral AF at the left side of the picture.
General introduction
11
11
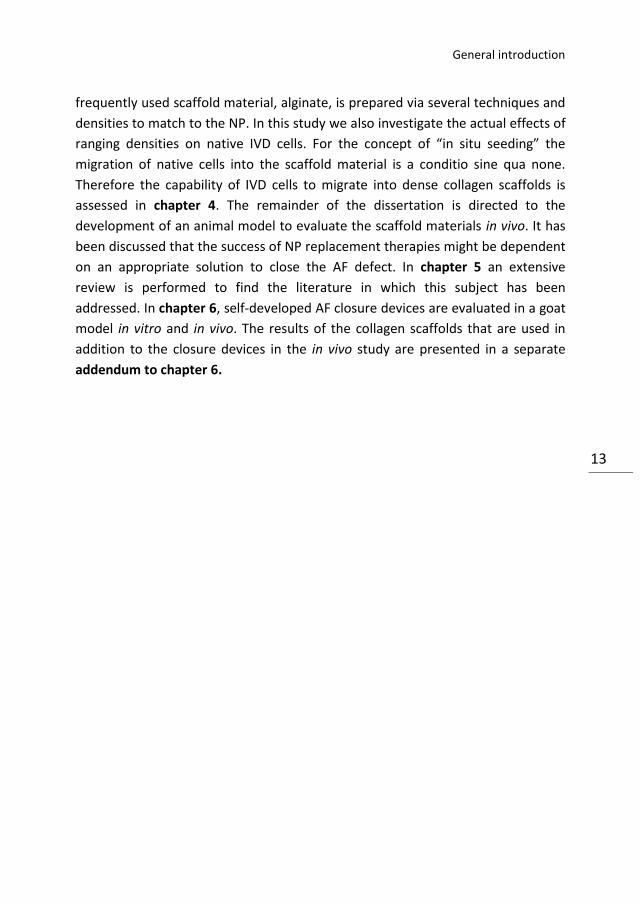
Current treatment modalities
The mainstay of the treatment of disc herniation has always been the removal of
the herniated NP material, the so-called discectomy. These procedures are
performed since the late 70-ies of the past century and are now the most
performed spinal surgical procedures worldwide [7,8]. However, compared to the
first described (open) discectomies, many things have been changed. Increased
knowledge and the advent of the MRI in the 1990s have resulted in numerous less
invasive procedures, abandoning the conventional discectomy. The gold standard
nowadays is the microdiscectomy in which every type of disc herniation can be
excised through a small incision and limited laminoarthrectomy [7]. An alternative
procedure that shows comparable results in experienced hands is the endoscopic
transforaminal discectomy [8]. Although the evolution of the conventional
discectomies to less invasive procedures has resulted in a decrease of morbidity,
still a significant number of patients suffer from recurrences or persisting low back
pain. The outcome of patients that undergo a microdiscectomy is not better
compared to patients receiving conservative treatment after 1 year follow-up [9].
Considering that the discectomy is directed towards the decompression of the
nerve roots and therefore does not deal with the damaged IVD these findings may
not be surprising.
Figure 3: schematic drawing of a lumbar discectomy
Chapter 1
12
Tissue Engineering
In patients suffering from disc herniation, there is an (sub)acute change in
mechanics and biology due to the rupture or bulging of AF and the subsequent
expulsion of the NP. Although the acute episode is often preceded by some
degenerative changes, most (mechanical) changes may still be reversible and the
patients might therefore be favorable candidates for early disc repair. This should
restore the biomechanical equilibrium within the disc, preserve local homeostasis,
and prevent progressive degeneration [10].
Tissue engineering is generally described as “the use of a combination of cells,
engineering and materials methods, and suitable biochemical and physio-chemical
factors to improve or replace biological functions” [11]. As tissue engineering has
quickly emerged as an area of pre-clinical research over the last decade, attractive
new strategies that deal with this problem can be developed. The replacement of
the lost NP tissue should not only restore local biomechanics but ideally allow disc
regeneration in the long-term. To that end cells, being the factories of the
extracellular matrix components, are essential. Much research has been
performed by seeding scaffolds with either native or stem cells. Native IVD cells,
however, are sparse and the use of stem cells requires additional harvesting
procedures and time consuming techniques. Therefore the concept of ‘in situ
seeding’ has been proposed, meaning the use of a-cellular scaffolds that allow
invasion of cells from the surrounding tissue [10]. This concept allows IVD
regeneration in a single (one-step) surgical procedure. Ideally, such a scaffold
further imitates the biomechanical properties of the NP, allows the invasion of
surrounding native cells, and can be used in a single procedure in adjunct to
microdiscectomy.
Scope of the thesis
In the current dissertation the concept of ‘in situ seeding’ is further explored,
from basic scaffold science till in vivo evaluation. In the first two chapters, scaffold
stiffness, which has been shown to strongly influence the biosynthetic response of
cells and thus is a crucial factor for successful IVD engineering, is studied. In
chapter 2 dense collagen scaffolds are rheologically characterized to find a match
in stiffness with native NP tissue. In addition, the effects of sterilization
techniques, necessary for final production, are assessed. In chapter 3, another
General introduction
13
13
frequently used scaffold material, alginate, is prepared via several techniques and
densities to match to the NP. In this study we also investigate the actual effects of
ranging densities on native IVD cells. For the concept of “in situ seeding” the
migration of native cells into the scaffold material is a conditio sine qua none.
Therefore the capability of IVD cells to migrate into dense collagen scaffolds is
assessed in chapter 4. The remainder of the dissertation is directed to the
development of an animal model to evaluate the scaffold materials in vivo. It has
been discussed that the success of NP replacement therapies might be dependent
on an appropriate solution to close the AF defect. In chapter 5 an extensive
review is performed to find the literature in which this subject has been
addressed. In chapter 6, self-developed AF closure devices are evaluated in a goat
model in vitro and in vivo. The results of the collagen scaffolds that are used in
addition to the closure devices in the in vivo study are presented in a separate
addendum to chapter 6.
Chapter 1
14
References
1. Rihn JA, Hilibrand AS, Radcliff K, Kurd M, Lurie J, Blood E, Albert TJ, Weinstein JN (2011)
Duration of symptoms resulting from lumbar disc herniation: Effect on treatment
outcomes. J Bone Joint Surg Am 93:1906-1914
2. Schneider C, Krayenbuhl N, Landolt H (2007) Conservative treatment of lumbar disc
disease: patient’s quality of life compared to an unexposed cohort. Acta Neuochir (Wien)
149: 785-791
3. Katz JN (2006) Lumbar disc disorders and low-back pain: socioeconomic factors and
consequences. J Bone Joint Surg Am 88 (suppl 2): 21-24
4. Jacobs WC, Van Tulder M, Arts M, Rubinstein SM, Van Middelkoop M, Ostelo R,
Verhagen A, Koes B, Peul WC (2011) Surgery versus conservative management of sciatica
due to a lumbar herniated disc: a systematic review. Eur Spine J 20: 513-522
5. Carragee EJ, Han MY, Suen PW, Kim D (2003) Clinical outcomes after lumbar discectomy
for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 85:
102-108
6. Chan WC, Sze KL, Samartzis D, Leung VY, Chan D (2011) Structure and biology of the
intervertebral disk in health and disease. Orthop Clin North Am 42(4):447-64, vii.
7. Postacchini F, Postacchini R (2011) Operative management of lumbar disc herniation:
the evolution of knowledge and surgical techniques in the last century. Acta Neurochir
Suppl 108: 17-21
8. Nellesteijn J, Ostelo R, Bartels R, Peul W, Van Royen BJ, Tulder M (2010) Transforaminal
endoscopic surgery for symptomatic lumbar disc herniations: a systematic review of the
literature. Eur Spine J 19: 181-204
9. Peul WC, Van Houwelingen HC, Van den Hout WB, Brand R. Eekhof JA, Tans JT, Thomeer
RT, Koes BW (2007) Surgery versus prolonged conservative treatment for sciatica. N Eng J
Med 356: 2245-2256
10. Hegewald AA, Ringe J, Sittinger M, Rhome C (2008) Regenerative treatment strategies
in spinal surgery. Front Biosci 13: 1507-1525
11. Wikipedia 2012: http://en.wikipedia.org/wiki/Tissue_engineering
2 Rheological characterization of the nucleus
pulposus and dense collagen scaffolds
intended for functional replacement
JL Bron
GH Koenderink
V Everts
TH Smit

Chapter 2
16 16
Abstract
Lumbar discectomy is an effective therapy for neurological decompression in
patients suffering from sciatica due to a herniated nucleus pulposus (NP).
However, high numbers of patients suffering from persisting postoperative low
back pain have resulted in many strategies targeting the regeneration of the NP.
For successful regeneration, the stiffness of scaffolds is increasingly recognized as
a potent mechanical cue for the differentiation and biosynthetic response of
(stem) cells. The aim of the current study is to characterize the viscoelastic
properties of the NP and to develop dense collagen scaffolds with similar
properties. The scaffolds consisted of highly dense (0.5% –12%) type I collagen
matrices, prepared by plastic compression. The complex modulus of the NP was
22 kPa (at 10 rad s-1), which should agree with a scaffold with a collagen
concentration of 23%. The loss tangent, indicative of energy dissipation, is higher
for the NP (0.28) than for the scaffolds (0.12) and was not dependent on the
collagen density. Gamma sterilization of the scaffolds increased the shear moduli
but also resulted in more brittle behavior and a reduced swelling capacity. In
conclusion, by tuning the collagen density, we can approach the stiffness of the
NP. Therefore, dense collagen is a promising candidate for tissue engineering of
the NP that deserves further study, such as the addition of other proteins.

Rheological characterization
17
Introduction
Lumbar discectomy is a well-established surgical procedure to decompress neural
structures in patients suffering from a symptomatic herniated lumbar
intervertebral disc. There are, however, serious adverse effects of disc herniation
and surgical evacuation on spinal biomechanics. Disc space narrowing may result
in discogenic pain or cause overloading in other structures including facet joints,
ligaments and muscles by altered motion [1]. The long-term sequelae after
discectomy significantly affects the quality of life of the relatively young and
employed patient population and therefore has serious socio-economic
consequences. This gave researchers the impetus to develop regenerative
strategies that deal with the damaged intervertebral disc, especially the nucleus
pulposus (NP) [2]. Scaffolds for NP replacement are enriched with stem cells,
growth factors, and/or additional molecules in order to promote and utilize the
regenerative potential of the human body [3]. Under physiological conditions,
cells within a scaffold are able to synthesize and secrete their own extracellular
matrix (ECM) [3]. Recently, it has been appreciated that their biosynthetic
response is strongly affected by the stiffness of the ECM [4,5]. The stiffness of the
ECM acts as a ‘‘passive’’ mechanical cue that can be more selective than soluble
factors [6]. By adjusting the stiffness of the scaffold to the targeted ECM, stem cell
differentiation and ECM synthesis can be directed [4,5].
The aim of this study is to mimic the elastic properties of the NP with dense
collagen scaffolds. Plastic compression of collagen solutions leads to significant
densification and viscoelastic properties that closely approach those of skeletal
tissue and has already been investigated for its potential in cartilage and bone
engineering [7 –10]. In the current study, we characterize the viscoelastic
properties of the NP by rheology [11,12] and screen dense collagen type I
scaffolds to determine which collagen density matches to these properties. Our
overall scope is to develop a collagen scaffold that could be used in in situ therapy
in patients with a herniated NP. Such a scaffold, combined with chemotactic
agents, should allow the in situ recruitment of progenitor and disc cells [13]. In
this concept, discomfort for patient and clinician is minimized, because the
harvesting and culturing of cells prior to the surgical procedure are not necessary.
Patients suffering from herniated discs could be treated in a one-step surgical
procedure, in which a discectomy is combined with a functional replacement [13]
Chapter 2
18 18
A-cellular collagen constructs require additional sterilization steps prior to this
stage. Because gamma sterilization has been described to have serious effects on
collagen matrices [14], its effect on rheology and swelling capacity of the current
dense collagen scaffolds is also assessed.
Materials and methods
NP Specimen Preparation
The lumbar spines of two mature female Dutch milk goats were harvested and
stored at -20 °C until the day of testing. After removal of the soft tissues and the
posterior and lateral elements, the intervertebral discs at the levels T12 –L1 until
L5 –L6 were separated from the upper and lower endplate by incision with a
surgical knife. The intervertebral discs were refrozen and the annulus fibrosis (AF)
was removed with a 9 mm circular trephine, sparing the NP. Rheological tests
were performed immediately after the NP samples were thawed. After the
rheological tests, the samples were weighed. The hydration status of the NP
samples was determined by weighing the samples before and after freeze drying.
Collagen Scaffold Preparation
The collagen scaffolds were prepared by using a rat-tail type 1 collagen gel with a
concentration of 6 mg/mL (0.6% w/w) collagen dissolved in 0.1% acetic acid
(Arthro Kinetics AG, Esslingen, Germany). The collagen gel (8/10 volume parts)
was mixed with (1/10 volume part) neutralization solution (Arthro Kinetics AG)
and (1/10 volume part) Dulbecco’s Modified Eagle Medium (Greiner Bio-one,
Kremsmunster, Austria). Variable amounts of the mixture were poured into a
cylinder (diameter 25 mm) with a polycarbonate cell culture insert (3 mm pores;
Nunc GmbH, Wiesbaden, Germany) at the bottom. The cylinder was then placed
in a CO2 incubator at 37.8 °C for 60 min to allow polymerization of the collagen.
When the collagen matrix was formed, a weight of 100 g was placed on top of the
matrix in the cylinder. The cylinder was placed back into the incubator overnight
for the filtration process to take place. The 3 mm pores allow fluid to pass
(filtrate), while retaining the collagen matrix itself (residue), thereby increasing
the collagen density. The final height of the collagen scaffolds was kept constant
at 3.6 mm, and the diameter was fixed by the cylinder diameter, 12.5 mm. The
Rheological characterization
19
final collagen density was varied by changing the amount of collagen solution in
the cylinders before compression. For example, 6% collagen samples were
obtained by adding 10 times the volume of collagen solution (17.5 mL) to the
cylinders compared to the final sample volume (1.75 mL). For each density, five
samples were made (4 rheological examination, 1 electron microscopy). Samples
were transferred directly from the cylinders to the rheometer for
characterization. After the rheological measurements, all samples were weighed
and the solid weight fraction was determined by freeze drying and weighing
again. From each collagen density one sample was transferred immediately from
the compression cylinders into 0.1 M Na-cacodylate buffer (pH 7.4) containing 4%
paraformaldehyde and 1% glutaaraldehyde. After 5 days in the fixative medium,
the samples were cut in two equal parts for transmission electron microscopy
(TEM). For electron microscopy the samples were dehydrated and embedded in
epoxy resin. Ultrathin sections were made with a diamond knife, contrasted with
uranyl and lead and examined in a Philips TEM.
Gamma-Irradiated Samples
Collagen samples, fabricated according to the protocol described above, with four
densities (0.5, 3, 6, and 10%) of collagen were packaged in containers made of
polyethylene filterplate and stored in sterile phosphate buffered saline at 48 °C.
The containers allow storage under wet conditions, yet prevent swelling of the
samples. For every concentration 10 samples were made. From these samples,
five were sent to Isotron (Ede, The Netherlands) immediately after fabrication to
undergo treatment with 15 kGg γ-irradiation according to the local medical
implant sterilization protocol. All samples underwent rheological characterization
3 days after preparation. After the rheological measurements, the samples were
weighed, put in 10 mL sterile water for 12 h at 48 °C, and weighed again to
determine the swelling capacity. The samples were finally freeze dried and
weighed again.
Rheological Measurements
The mechanical behavior of the collagen samples was assessed using a stress-
controlled rheometer (Paar Physica MCR501; Anton Paar, Graz, Austria) in parallel
plate configuration (40 mm diameter, 3.5 mm gap). For the NP samples, a parallel
Chapter 2
20 20
plate configuration was also used (20 mm diameter, 2 –3 mm gap). To prevent
sample slippage, sandpaper (CP918C P180; VSM Abrasives, O’Fallon, MO) was
attached to the plates. The discs were loaded between the plates, and the gap
was closed until the sample was in good contact with both plates (normal force <1
N). The tests were performed at a temperature of 37.8 °C in a humidified
chamber. Three types of measurements were performed in the following order:
time sweep, frequency sweep, and amplitude sweep. To exclude any time-
dependent relaxation during the tests, the samples were first equilibrated for 20
min. During this time, the normal force decreased to values below 0.1 N in all
samples. Subsequently, we probed the time-dependent shear moduli by
performing frequency sweep measurements over an angular frequency range of
0.2 –200 rad s-1 at a fixed strain amplitude of 1%, well within the linear regime.
Finally, the behavior of the samples at large deformations was tested by
amplitude sweep tests. Strain oscillations at a fixed frequency of 0.5 Hz and
gradually increasing strain amplitude were applied, until a maximum of 1000%
strain or until sample failure occurred. The shear modulus G*(ω) = σ (ω)/γ(ω)
follows from the ratio between stress (σ) and strain amplitude (γ). G*(ω) = G’+ iG”
is a complex quantity with an elastic storage modulus (G’) and viscous loss
modulus (G”). The absolute magnitude of the shear modulus,│G*│, was calculated
using │G*│= (G’2 + G”2)0,5. The ratio G”/G’ is called the damping factor and equals
the tangent of the phase angle difference between stress and strain (tan δ). Data
reported represent the mean from at least four replicates of each collagen sample
or 11 NP samples. Because the sample diameters were smaller than the plates,
the measured values had to be corrected before further evaluation. In a parallel
plate configuration, values are based on measurements at the outer edge of the
samples, where the strain is maximal. If the sample radius (Rsample) is smaller than
the plate radius (R), the moduli are underestimated by a factor (R/Rsample)4,
because the stress scales with R as 1/R3 while the strain is proportional to R. The
correction factor that was applied to the data was 6.55 for the collagen samples
and 24.4 for the NP samples.
Statistical Analysis
Differences between various sample groups were statistically analyzed using the
paired t-test.

Rheological characterization
21
Results
The mean weight of the NP samples was 210 (± 25.2) mg with a dry weight of 52.3
(± 10.9) mg, implying a water content of 75.2% (± 4.1). The mean weight of the
collagen samples was 1,390 (± 81) mg, and dry weights varied from 7 to 150 mg
(dependent on collagen concentration), implying a water content between 88%
and 99.5%. As a control of the collagen densities after compression, real densities
were calculated using test-weight and dry-weight. Real percentages of collagen
([dry-weight/test-weight] * 100%) of 3.2 (± 0.2), 6.0 (± 0.4), and 9.6 (± 0.4) were
found for the 3%, 6%, and 10% collagen samples respectively. Real densities of
collagen therefore did not significantly differ from intended densities. Plastic
compression resulted in collagen scaffolds with decreased water content and
increased density of collagen fibers. Individual fibers of collagen fibers were still
present, but the mean spacing between fibers greatly decreased upon
compression, as shown by the transmission electron micrographs in Figure 1.
A B
Figure 1: TEM images of sections of noncompressed (0.5%) (A) and a 20-fold compressed (10%) (B)
collagen scaffold. The collagen fibers display characteristic periodic D-banding. Otherwise there did not seem to be any structural changes in the length of the
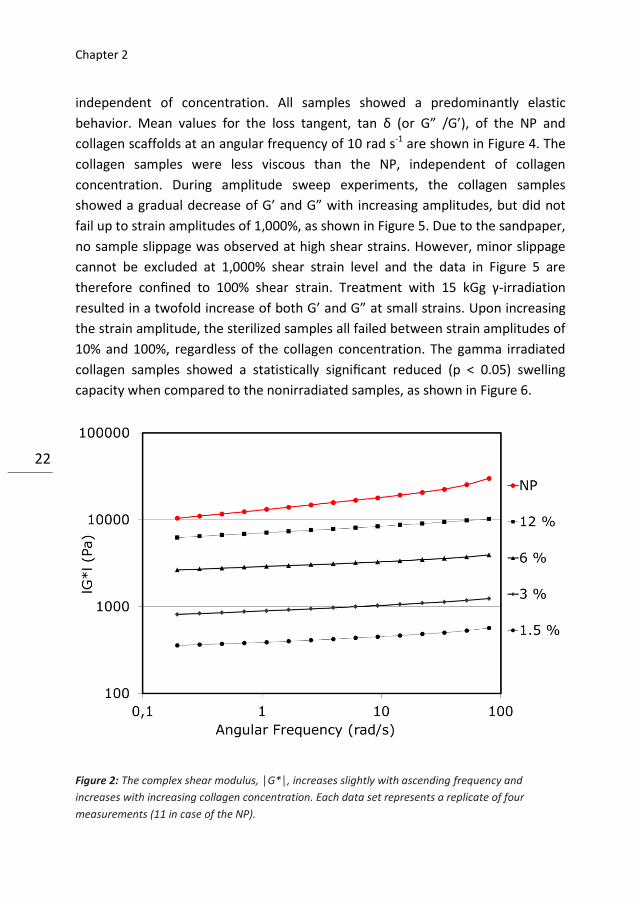
collagen fibers or alignment. The complex modulus,│G*│, was slightly frequency
dependent in both the NP and collagen samples, increasing at ascending
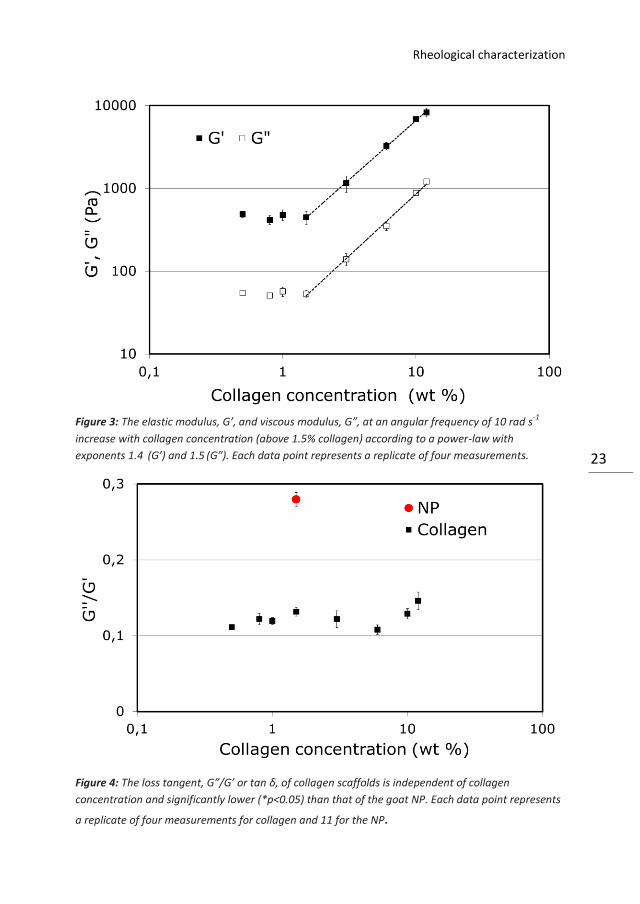
frequencies, as shown in Figure 2. At a frequency of 10 rad s-1, both the elastic
modulus, G’ , and viscous modulus, G” , increased with increasing collagen
concentration, as shown in Figure 3. This increase however, only occurred at
collagen densities above 1.5%. Below this concentration, the shear moduli were
Chapter 2
22 22
independent of concentration. All samples showed a predominantly elastic
behavior. Mean values for the loss tangent, tan δ (or G” /G’), of the NP and
collagen scaffolds at an angular frequency of 10 rad s-1 are shown in Figure 4. The
collagen samples were less viscous than the NP, independent of collagen
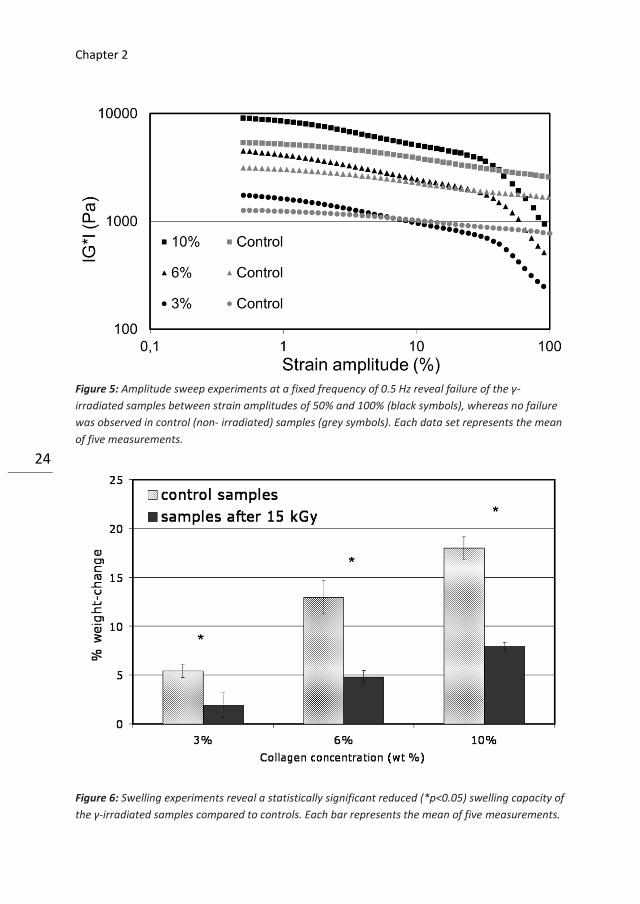
concentration. During amplitude sweep experiments, the collagen samples
showed a gradual decrease of G’ and G” with increasing amplitudes, but did not
fail up to strain amplitudes of 1,000%, as shown in Figure 5. Due to the sandpaper,
no sample slippage was observed at high shear strains. However, minor slippage
cannot be excluded at 1,000% shear strain level and the data in Figure 5 are
therefore confined to 100% shear strain. Treatment with 15 kGg γ-irradiation
resulted in a twofold increase of both G’ and G” at small strains. Upon increasing
the strain amplitude, the sterilized samples all failed between strain amplitudes of
10% and 100%, regardless of the collagen concentration. The gamma irradiated
collagen samples showed a statistically significant reduced (p < 0.05) swelling
capacity when compared to the nonirradiated samples, as shown in Figure 6.
Figure 2: The complex shear modulus, │G*│, increases slightly with ascending frequency and
increases with increasing collagen concentration. Each data set represents a replicate of four
measurements (11 in case of the NP).
Rheological characterization
23
Figure 3: The elastic modulus, G’, and viscous modulus, G”, at an angular frequency of 10 rad s
-1
increase with collagen concentration (above 1.5% collagen) according to a power-law with
exponents 1.4 (G’) and 1.5
(G”). Each data point represents a replicate of four measurements.
Figure 4: The loss tangent, G”/G’ or tan δ, of collagen scaffolds is independent of collagen
concentration and significantly lower (*p<0.05) than that of the goat NP. Each data point represents
a replicate of four measurements for collagen and 11 for the NP.
Chapter 2
24 24
Figure 5: Amplitude sweep experiments at a fixed frequency of 0.5 Hz reveal failure of the γ-
irradiated samples between strain amplitudes of 50% and 100% (black symbols), whereas no failure
was observed in control (non- irradiated) samples (grey symbols). Each data set represents the mean
of five measurements.
Figure 6: Swelling experiments reveal a statistically significant reduced (*p<0.05) swelling capacity of
the γ-irradiated samples compared to controls. Each bar represents the mean of five measurements.
Rheological characterization
25
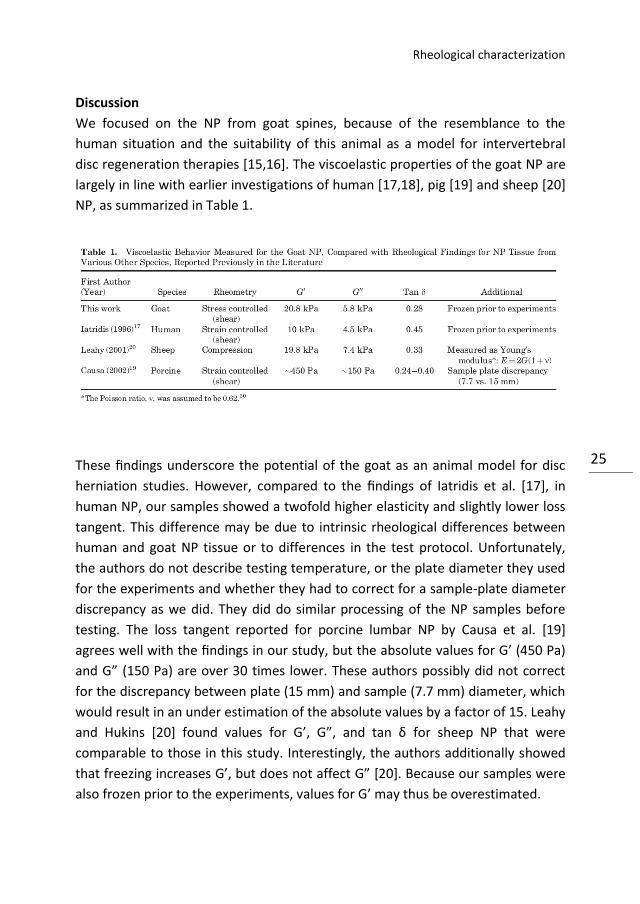
Discussion
We focused on the NP from goat spines, because of the resemblance to the
human situation and the suitability of this animal as a model for intervertebral
disc regeneration therapies [15,16]. The viscoelastic properties of the goat NP are
largely in line with earlier investigations of human [17,18], pig [19] and sheep [20]
NP, as summarized in Table 1.
These findings underscore the potential of the goat as an animal model for disc
herniation studies. However, compared to the findings of Iatridis et al. [17], in
human NP, our samples showed a twofold higher elasticity and slightly lower loss
tangent. This difference may be due to intrinsic rheological differences between
human and goat NP tissue or to differences in the test protocol. Unfortunately,
the authors do not describe testing temperature, or the plate diameter they used
for the experiments and whether they had to correct for a sample-plate diameter
discrepancy as we did. They did do similar processing of the NP samples before
testing. The loss tangent reported for porcine lumbar NP by Causa et al. [19]
agrees well with the findings in our study, but the absolute values for G’ (450 Pa)
and G” (150 Pa) are over 30 times lower. These authors possibly did not correct
for the discrepancy between plate (15 mm) and sample (7.7 mm) diameter, which
would result in an under estimation of the absolute values by a factor of 15. Leahy
and Hukins [20] found values for G’, G”, and tan δ for sheep NP that were
comparable to those in this study. Interestingly, the authors additionally showed
that freezing increases G’, but does not affect G” [20]. Because our samples were
also frozen prior to the experiments, values for G’ may thus be overestimated.
Chapter 2
26 26
In the context of regeneration of the damaged NP, we should note that our NP
samples were derived from healthy intervertebral discs. Earlier studies have
shown that G” increases in case of disc degeneration [18]. In this study, we used a
plastic compression technique to develop collagen I-based scaffolds with varying
concentrations and viscoelastic properties. This is a novel technique that was first
described by Brown et al. [21] as a form of cell-independent engineering. Central
in this concept is the reduction of the liquid content of the scaffold, which is a
result of the casting [21]. Plastic compression therefore yields scaffolds much
denser than conventional, uncompressed collagen type I matrices. The moduli of
these conventional scaffolds are typically below 1 kPa [22,23], and these scaffolds
should first grow stronger in culture [21]. Our technique of plastic compression
differs from earlier studies, because we use cell culture inserts with 3 mm pores
to reduce the liquid content instead of nylon and stainless steel meshes [7 –
10,21]. Furthermore, the dimensions of our scaffolds are much larger than
reported earlier and the compression times therefore longer. The latter reduces
the attractivity to enrich scaffolds with cells, which should not easily survive in
such large constructs [10].
To our knowledge, a detailed rheological characterization of dense collagen I
scaffolds, as in the current study, has not been reported previously in literature.
With our dense collagen scaffolds, we are able to approach the viscoelastic
properties of the NP, in particular its elasticity. The loss tangent, G”/G’, of the
collagen matrices is lower than that of the NP, and perhaps this could be
remedied by adding other components such as proteoglycans. We do not have an
explanation why the moduli only reveal a density-dependence at collagen
densities above 1.5%, as shown in Figure 3. Because the volume capacity of our
cylinders was confined, we could not obtain higher collagen densities than 12%.
The value for │G*│ of the 12% collagen scaffold is still below the value of the NP.
If we use the power law formula for the values of │G*│ above 1.5%, we can
extrapolate the collagen density that agrees with the │G*│ value of the NP. The
stiffness of the NP should than be matched by a scaffold containing 22.7%
collagen.
In the current study we also assessed the effects of a standard sterilization
treatment, which is a regulatory requirement for the acellular dense collagen
Rheological characterization
27
scaffolds to be sold as a medicinal product. Gamma irradiation is the method of
choice for sterilizing collagen biomaterials and is considered as the most reliable
method available [14]. In this study we showed that a standard sterilization
treatment with 15 kGy γ-irradiation results in an over twofold increase of G’ and
also a significant increase of G”. More importantly we showed that the resistance
to high amplitude strains decreases dramatically. Non-treated samples did not fail
below 1,000% whereas treated samples already failed at strain amplitudes of only
50%.
Plastic compression of collagen matrices results in compensatory swelling of the
samples when put free floating in water, which is density dependent. This might
be an advantage because it is comparable to the overnight rehydration of the NP
itself that occurs when external loads on the spine cease. The rheologic properties
are strongly related to the hydration state and variations due to the overnight
swelling should ideally be comparable. The swelling capacity of the samples was
significantly reduced by γ-sterilization. The effects of γ-irradiation can be
explained by the increase in the number of cross links and chain scission in the
collagen matrix due to the g-irradiation [14,24]. Chain scission of the collagen
peptide backbone results in a fraction of lower molecular weight material [24],
whereas the formation of additional cross links compensates to a certain extent
for this fragmentation [14]. The effects of γ-irradiation are dose-dependent and
lowering the dosage could lower the damage, but also result in subcomplete
sterilization [24]. Alternatives for γ-irradiation include ethylene oxide (Eto) and E-
beam sterilization [24]. However, these techniques have their own limitations and
drawbacks. Eto results in decreased helix stability and slower degradation rates
and potentially leaves toxic residues in the implants [25]. The effects of E-beam on
collagen are less well documented, but it has shown to result in a dramatic
increase of the inherent viscosity of other polymers [26]. It is therefore important
to check for structural and mechanical effects of sterilization procedures during
the development of implants and scaffolds. The importance of this subject is
currently not always recognized, but will gain attention when tissue engineering
makes the step from the developmental stage to clinical trials. Promising
developments in the field of collagen sterilization that are currently being
evaluated include pulsed electric field sterilization and the addition of free radical
scavengers to the treatment with γ-irradiation [27,28].
Chapter 2
28 28
Wilke et al. [29] already showed that collagen scaffolds are capable of restoring
disc height and stability after disc herniation. However, the authors also showed
that the risk of dislocation of the implant across the annulus defect forms a
serious problem. It seems important, therefore, to develop additional annulus
closure techniques or other methods to anchor the collagen scaffold within the
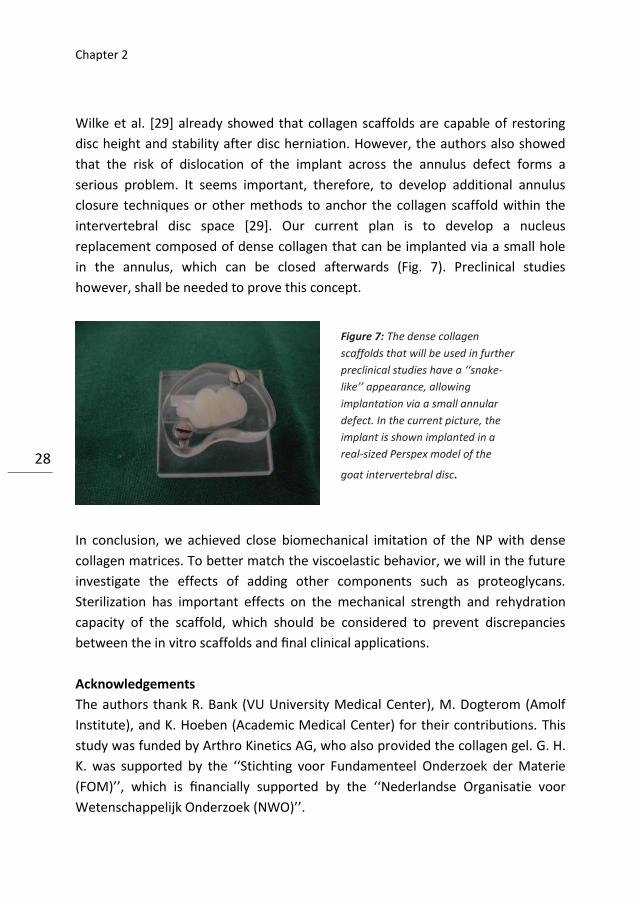
intervertebral disc space [29]. Our current plan is to develop a nucleus
replacement composed of dense collagen that can be implanted via a small hole
in the annulus, which can be closed afterwards (Fig. 7). Preclinical studies
however, shall be needed to prove this concept.
In conclusion, we achieved close biomechanical imitation of the NP with dense
collagen matrices. To better match the viscoelastic behavior, we will in the future
investigate the effects of adding other components such as proteoglycans.
Sterilization has important effects on the mechanical strength and rehydration
capacity of the scaffold, which should be considered to prevent discrepancies
between the in vitro scaffolds and final clinical applications.
Acknowledgements
The authors thank R. Bank (VU University Medical Center), M. Dogterom (Amolf
Institute), and K. Hoeben (Academic Medical Center) for their contributions. This
study was funded by Arthro Kinetics AG, who also provided the collagen gel. G. H.
K. was supported by the ‘‘Stichting voor Fundamenteel Onderzoek der Materie
(FOM)’’, which is financially supported by the ‘‘Nederlandse Organisatie voor
Wetenschappelijk Onderzoek (NWO)’’.
Figure 7: The dense collagen
scaffolds that will be used in further
preclinical studies have a ‘‘snake-
like’’ appearance, allowing
implantation via a small annular
defect. In the current picture, the
implant is shown implanted in a
real-sized Perspex model of the
goat intervertebral disc.
Rheological characterization
29
References
1. Boyd LM, Carter AJ (2006) Injectable biomaterials and vertebral endplate treatment for
repair and regeneration of the intervertebral disc. Eur Spine J 15(Suppl 3): S414-S421
2. Hegewald AA, Ringe J, Sittinger M, et al. (2008) Regenerative treatment strategies in
spinal surgery. Front Biosci 13: 1507-1525
3. Richardson SM, Mobasheri A, Freemont AJ, et al. (2007) Intervertebral disc biology,
degeneration and novel tissue engineering and regenerative medicine therapies. Histol
Histopathol 22: 1033-1041
4. Ghosh K, Pan Z, Guan E, et al. (2007) Cell adaptation to a physiologically relevant ECM
mimic with different viscoelastic properties. Biomaterials 28: 671-679
5. Zaman MH, Trapani LM, Sieminski AL, et al. (2006) Migration of tumor cells in 3D
matrices is governed by matrix stiffness along with cell-matrix adhesion and proteolysis.
Proc Natl Acad Sci USA 103: 10889-10894
6. Engler AJ, Sen S, Sweeney HL, et al. (2006) Matrix elasticity directs stem cell lineage
specification. Cell 126: 677-689
7. Bitar M, Brown RA, Salih V, et al. (2008) Effect of cell density on osteoblastic
differentiation and matrix degradation of biomimetic dense collagen scaffolds.
Biomacromolecules 9: 129-135
8. Mudera V, Morgan M, Cheema U, et al. (2007) Ultra-rapid engineered collagen
constructs tested in an in vivo nursery site. J Tissue Eng Regen Med 1: 192-198
9. Grad S, Gogolewski S, Alini M, et al. (2006) Effects of simple and complex motion
patterns on gene expression of chondrocytes seeded in 3D scaffolds. Tissue Eng 12: 3171-
3179
10. Nazhat SN, Neel EA, Kidane A, et al. (2007) Controlled microchannelling in dense
collagen scaffolds by soluble phosphate glass fibers. Biomacromolecules 8: 543-551
11. Kavanagh GM, Ross-Murphy SB. (1998) Rheological characterisation of polymer gels.
Prog Polym Sci 23: 533-562
12. Smith CM, Christian JJ, Warren WL, et al. (2007) Characterizing environmental factors
that impact the viability of tissue engineered constructs fabricated by a direct-write
bioassembly tool. Tissue Eng 13: 373-383
13. Abbushi A, Endres M, Cabraja M, et al. (2008) Regeneration of intervertebral disc
tissue by resorbable cell-free polyglycolic acid-based implants in a rabbit model of disc
degeneration. Spine 33: 1527-1532
14. Friess W. (1998) Collagen-biomaterial for drug delivery. Eur J Pharm Biopharm 45: 113-
136
15. Smit TH (2002) The use of a quadruped as an in vivo model for the study of the spine—
biomechanical considerations. Eur Spine J 11: 137-144
16. Ethier DB, Cain JE, Yaszemski MJ, et al. (1994) The influence of anulotomy selection on
disc competence. A. radiographic, biomechanical, and histologic analysis. Spine 19: 2071-
Chapter 2
30 30
2076
17. Iatridis JC, Weidenbaum M, Setton LA, et al. (1996) Is the nucleus pulposus a solid or a
fluid? Mechanical behaviors of the nucleus pulposus of the human intervertebral disc.
Spine 21: 1174-1184
18. Umehara S, Tadano S, Abumi K, et al. (1996) Effects of degeneration on the elastic
modulus distribution in the lumbar intervertebral disc. Spine 21: 811-819
19. Causa F, Manto L, Borzacchiello A, et al. (2002) Spatial and structural dependence of
mechanical properties of porcine intervertebral disc. J Mater Sci Mater Med 13: 1277-
1280
20. Leahy JC, Hukins DW (2001) Viscoelastic properties of the nucleus pulposus of the
intervertebral disk in compression. J. Mater Sci Mater Med 12: 689-692
21. Brown R, Wiseman M, Chuo C, et al. (2005) Ultrarapid engineering of biomemetic
materials and tissues: fabrication of nano- and microstructures by plastic compression.
Advanced Functional Materials 15: 1762-1770
22. Forgacs G, Newman SA, Hinner B, et al. (2003) Assembly of collagen matrices as a
phase transition revealed by structural and rheologic studies. Biophys J 84: 1272-1280
23. Wu CC, Ding SJ, Wang YH, et al. (2005) Mechanical properties of collagen gels derived
from rats of different ages. J. Biomater Sci Polym Ed 16: 1261-1275
24. Cheung DT, Perelman N, Tong D, et al. (1990) The effect of gamma-irradiation on
collagen molecules, isolated alpha-chains, and crosslinked native fibers. J Biomed Mater
Res 24: 581-589
25. Olde Damink LH, Dijkstra PJ, Van Luyn MJ, et al. (1995) Influence of ethylene oxide gas
treatment on the in vitro degradation behavior of dermal sheep collagen. J Biomed Mater
Res 29: 149-155
26. McManus AJ, Moser RC, Dabkowski RB, et al. (2007) Enhanced retention of polymer
physical characteristics and mechanical strength of 70:30 poly(L-lactide-co-D,L-lactide)
after ethylene oxide sterilization. J. Biomed Mater Res B Appl Biomater 82: 325-333
27. Seto A, Gatt CJ Jr, Dunn MG (2008) Radioprotection of tendon tissue via crosslinking
and free radical scavenging. Clin Orthop Relat Res 466: 1788-1795
28. Smith S, Griffiths S, Macgregor S, et al. (2009) Pulsed electric field as a potential new
method for microbial inactivation in scaffold materials for tissue engineering: The effect
on collagen as a scaffold. J. Biomed Mater Res A 90: 844-841
29. Wilke HJ, Heuer F, Neidlinger-Wilke C, et al. (2006) Is a collagen scaffold for a tissue
engineered nucleus replacement capable of restoring disc height and stability in an animal
model? Eur Spine J 15(Suppl 3): S433-S438
30. Cloyd JM, Malhotra NR, Weng L, et al. (2007) Material properties in unconfined
compression of human nucleus pulposus, injectable hyaluronic acid-based hydrogels and
tissue engineering scaffolds. Eur Spine J 16: 1892-1898

3 Engineering alginate for intervertebral disc
repair
JL Bron
LA Vonk
TH Smit
GH Koenderink
Chapter 3
32
Abstract
Alginate is frequently studied as a scaffold for intervertebral disc (IVD) repair,
since it closely mimics mechanical and cell-adhesive properties of the nucleus
pulposus (NP) of the IVD. The aim of this study was to assess the relation between
alginate concentration and scaffold stiffness and find preparation conditions
where the viscoelastic behaviour mimics that of the NP. In addition, we measured
the effect of variations in scaffold stiffness on the expression of extracellular
matrix molecules specific to the NP (proteoglycans and collagen) by native NP
cells. We prepared sample discs of different concentrations of alginate (1%–6%)
by two different methods, diffusion and in situ gelation. The stiffness increased
with increasing alginate concentration, while the loss tangent (dissipative
behaviour) remained constant. The diffusion samples were ten-fold stiffer than
samples prepared by in situ gelation. Sample discs prepared from 2% alginate by
diffusion closely matched the stiffness and loss tangent of the NP. The stiffness of
all samples declined upon prolonged incubation in medium, especially for samples
prepared by diffusion. The biosynthetic phenotype of native cells isolated from
NPs was preserved in alginate matrices up to 4 weeks of culturing. Gene
expression levels of extracellular matrix components were insensitive to alginate
concentration and corresponding matrix stiffness, likely due to the poor
adhesiveness of the cells to alginate. In conclusion, alginate can mimic the
viscoelastic properties of the NP and preserve the biosynthetic phenotype of NP
cells but certain limitations like long-term stability still have to be addressed.
Engineering alginate
33
Introduction
Transplantation systems based on scaffolds seeded with stem cells or native cells
offer a promising means to repair aged, damaged, or diseased tissues [18].
Accordingly, there has been much recent effort to design scaffolds that mimic the
bioadhesive and physical characteristics of natural extracellular matrices found in
tissues and can thus promote tissue-specific cell phenotype [20, 30]. A variety of
tissues can already be engineered by this approach, including artery, skin,
cartilage, bone, ligament, and tendon. Scaffold stiffness has been recognized as an
especially important cue to guide cell differentiation and extracellular matrix
(ECM) production [4,12,14] and this knowledge is now increasingly being
implemented in tissue engineering strategies [13]. The mechanical characteristics
of many tissues have been documented over the recent years, facilitating the
development of new generations of 3D scaffolds mimicking these features [4,21].
Our own research over the past years has focused on tissue engineering strategies
to repair damaged intervertebral discs (IVDs) [5-7]. The IVD is a cartilaginous
structure that lies between adjacent vertebrae, where it acts as a shock absorber
and allows motion of the otherwise rigid vertebral column [33]. The IVD consists
of a collagenous outer annulus fibrosus (AF) which surrounds the gelatinous inner
nucleus pulposus (NP). Ageing is accompanied by loss of water and proteoglycans
from the gelatinous NP, which becomes more fibrous, resulting in a more rigid
IVD. Although these changes are to some extent physiological, they may result in
symptomatic degenerative disc disease [33]. In some patients, early degeneration
of the AF may result in a posterior tear through which the NP can extrude (disc
herniation), compromising the neurological structures (spine and nerve roots)
that the vertebral column usually protects. The current clinical solution is to
evacuate the herniated NP material (discectomy), thereby relieving the
compressed nerves [17]. There are, however, serious adverse effects of disc
herniation and subsequent discectomy on spinal biomechanics resulting in
discogenic back pain that seriously affects the quality of life in many patients.
Much research is therefore directed towards the restoration of the herniated disc
either by replacement or regenerative approaches. Ideally, current discectomy
procedures should be combined with the replacement of the lost NP material by a
scaffold with (native or stem-) cells initiating disc regeneration instead of
degeneration [17].
Chapter 3
34
In chapter 2, we showed that the mechanical properties of the NP can be
mimicked using dense scaffolds of collagen I, which is a natural extracellular
matrix protein [6]. The scaffold stiffness approached that of the NP, but the
viscous modulus was lower. Aside from the difference in viscous behaviour, type I
collagen is not an optimal replacement of the NP, which is predominantly
composed of type II collagen and proteoglycans. Other 3D scaffold materials, such
as alginate, agarose and chitosan, have also been studied for NP regeneration,
and these might allow a closer match both from a mechanical and a biochemical
point of view [15,27,35]. Alginate is most often studied since it is inexpensive and
does not evoke adverse tissue reactions [27,28,32]. Alginate is a naturally
occurring, water soluble polysaccharide block copolymer composed of β-L-
mannuronic acid (M) and α-L-guluronic acid (G) that can be ionically crosslinked
by divalent ions, such as calcium [25]. The resulting matrix has a stiffness which is
determined by the alginate concentration and by the ratio between G and M
blocks [32]. Other conditions such as gelation temperature and type of crosslinker
also influence the final network structure and ensuing mechanical properties [3].
The aim of this study was to design alginate scaffolds with viscoelastic properties
that mimic those of the NP and to assess the biosynthetic response of native NP
cells. We therefore investigated the effects of variations in alginate concentration
on the viscoelastic (rheological) characteristics of scaffolds. In addition, we
compared two different methods of inducing alginate gelation, by diffusion and by
‘in situ’ gelation. In diffusion-induced gelation, calcium ions are allowed to diffuse
into the alginate gel via a porous membrane, leading to crosslinking [32]. “In situ”
gelation is performed by mixing insoluble calcium with the alginate solution and
then releasing calcium ions within the solution by enzymatically decreasing the pH
level [23]. Since it has been documented that alginate scaffolds rapidly loose their
stiffness in vivo [32], we monitored the time-dependent stiffness during
prolonged incubation in cell culture medium. Finally, to determine whether
variations in alginate concentration affect cell behaviour, we cultured native cells
isolated from goat NP and annulus fibrosus (AF) in alginate beads of different
alginate concentrations (2%, 4% and 6%). We monitored the gene expression
levels of the main natural components of the ECM of the NP (types I and II
collagen and aggrecan) up to 4 weeks. The gene expression levels were compared
Engineering alginate
35
to gene expression levels found in chondrocytes from articular cartilage (AC), for
which extensive studies have been performed of the preservation of phenotype in
alginate [10,16,29,31].
Materials and Methods
Preparation of alginate sample discs by calcium diffusion
Freeze dried alginate (LVCR sodium alginate, Monsanto, San Diego, CA) was
dissolved in water containing 0.9 wt% sodium chloride. Alginate solutions at four
different concentrations (1, 2, 4, and 6 wt%) were sterilized by autoclaving (121
°C, 15 min). Sample discs were prepared by pouring 2 ml of alginate solution into
tissue culture inserts (25 mm, pore size 0.4 μm; Nunc, Roskilde, Denmark). The
inserts were placed in Petri dishes containing an aqueous solution of 500 mM
calcium chloride, and a polycarbonate filter membrane (thickness 8 mm) was
placed on top, which was irrigated with 2 ml of the calcium solution. After two
hours at room temperature, alginate gelation was finished and the sample discs
were removed from the culture inserts. The samples intended for analysis after
prolonged storage in medium were transferred to 6-well plates containing 5 ml
Dulbecco’s Modified Eagles Medium (DMEM, Gibco, Paisley, UK) supplemented
with 1% streptomycin, penicillin and amphotericin B (all from Gibco). The medium
was refreshed every three days. Samples were assayed at three time points (0, 1
and 10 days), using five separate samples for each time point and each alginate
concentration.
Preparation of alginate sample discs by in situ gelation
Insoluble calcium carbonate powder was mixed at a concentration of 100 mM
with alginate solutions in 0.9% NaCl (2%, 4% or 6% alginate) and stirred. The
mixture was acidified by adding the enzyme Glucono Delta-Lactone (GDL, Sigma
Chemical Co. (St. Louis, MO)) to a final concentration of 80 mM. A volume of 2 ml
of the acidified mixture was injected into the wells of 12-well (well diameter 22
mm) plates using a syringe. After 2 h at room temperature, the gelled sample
discs were removed from the wells and transferred to the rheometer for analysis.
The samples intended for analysis after prolonged storage in medium were
transferred to 6-well plates containing 5 ml DMEM supplemented with 1%
Chapter 3
36
antibiotics. The medium was refreshed every three days. Samples were assayed at
two time points (0 and 10 days), using five separate samples for each time point
and each alginate concentration. The samples after 10 days of incubation showed
irregular edges and were therefore reduced to a size of 20.0 mm with a cork
borer.
Rheometry
The viscoelastic properties of the alginate discs were measured using a stress-
controlled rheometer (Paar Physica MCR501, Anton Paar, Graz, Austria) equipped
with a temperature-controlled steel bottom plate and 20 or 40 mm diameter steel
top plates. The alginate discs showed some variability in diameter after incubation
in culture medium, due to variable degrees of shrinkage. Since variations in
sample size complicate the interpretation of rheological data, we equalized the
sample diameters using cork borers. Samples prepared by diffusion were reduced
to a diameter of 20 mm at t = 0 and 15.4 mm for t = 1 and 10 days. In situ gelled
samples were perfectly circular directly after gelation, with a diameter of 22 mm;
they were measured using a 40mm top plate. After 10 days incubation, the
samples showed some edge irregularities. To exclude any edge effects, the
incubated samples were reduced to a diameter of 20 mm, matching the diameter
of the 20 mm top plate. For samples with a diameter smaller than the diameter of
the rheometer top plate, the absolute values of the shear moduli were corrected
as described earlier [6]. To prevent sample slippage, self-adhesive sandpaper
(CP918C P180, VSM Abrasives, O’Fallon, Missouri, USA) was attached to both
plates. The discs were loaded between the plates, and the top plate was lowered
until the sample was in good contact with both plates. The tests were performed
at a temperature of 37 °C in a humidified chamber. To exclude any time-
dependent relaxation during the tests, the samples were first equilibrated for 10
min. During this time, the normal force decreased to values below 0.25 N in all
samples. Subsequently, we probed the frequency-dependent shear moduli by
performing frequency sweep measurements over an angular frequency range of
0.2–200 rad s−1 at a strain amplitude of 1%, well within the linear regime. Finally,
to test the strength of the alginate discs, we subjected them to sinusoidally
oscillating shear at a fixed frequency of 0.5 Hz and gradually increasing strain
amplitude, until a maximum of 1000% strain or until sample failure occurred. The
shear modulus G∗(ω) follows from the ratio between stress (σ) and strain
Engineering alginate
37
amplitude (γ). G* is a complex quantity with an elastic (or storage) modulus (G′)
and viscous (or loss) modulus (G′′). The absolute magnitude of the shear modulus,
|G*|, was calculated using |G*| = ((G′)2 + (G′′)2)0.5. The ratio G′′/G′ is referred to
as the loss tangent, since it equals the tangent of the phase angle difference
between stress and strain (tan δ). Data reported represent the mean +/- S.E. from
5 samples per condition.
Isolation of native cells and cell culture in alginate
Cartilaginous tissues were obtained from skeletally mature female Dutch milk
goats (n = 8) that were sacrificed for other studies. All thoracic and lumbar
intervertebral discs (IVDs, T1-L2/L6-S1) and articular cartilage (AC) from the
glenohumeral joint were collected. The IVDs were dissected to separate the
nucleus pulposus (NP) from the annulus fibrosus (AF). To assure an adequate cell
number, tissues from two goats were mixed for every measurement.
Experiments were performed in quadruplicate. The tissues were dissected and
minced, and the cells were released by subjected the tissues to sequential
treatments first with DMEM supplemented with 1% foetal bovine serum (FBS,
HyClone, Logan, UT, USA), 100 U/ml penicillin, 100 μg/ml streptomycin, 2.5 μg/ml
amphotericin B and 2.5% (w/v) Pronase E (Sigma, St. Louis, MO) for 1 h, then with
DMEM supplemented with 25% FBS, 100 U/ml penicillin, 100 μg/ml streptomycin,
2.5 μg/ml amphotericin B and 0.125% (w/v) collagenase (CLS-2, Worthington,
Lakewood, NJ) for 16 h at 37 °C. After filtering the cell suspension through a 70
μm pore size cell strainer (BD Biosciences, San Diego, CA), isolated cells were
resuspended in an alginate solution (2, 4 and 6 (w/v) in 0.9% NaCl (0.2 μm sterile
filtered), creating a suspension of 4 × 106 cells/ml. The suspension was
homogenized by slow pipetting and transferred to a sterile syringe. Alginate beads
were formed by the diffusion method, dripping ~10 μL drops of the solution from
the syringe needle (26 gauge) into a calcium chloride solution (102 mM). The
beads were allowed to gel by inward diffusion of Ca2+ for 10 min at ambient
temperature. After washing twice in 0.9% NaCl and twice in DMEM, the alginate
beads were transferred to 24-well tissue culture dishes with 10 beads per well
(Greiner Bio-one, Kremsmuenster, Austria). The cells were cultured in 500 μl of
DMEM per well, supplemented with 10% FBS, 100 U/ml penicillin, 100 μg/ml
streptomycin, 2.5 μg/ml amphotericin B, and 50 μg/ml ascorbate-2-phosphate
(Sigma). We note that our purpose is to develop a clinical procedure where freshly
Chapter 3
38
harvested cells are immediately transplanted back into the patient in an alginate
scaffold. For this reason, we did not first do expansion in 2D culture, but
characterized gene expression for freshly isolated cells cultured in 3D.
Real-time PCR
Alginate beads were dissolved in alginate dissolving buffer (55 mM Na-citrate,
0.15 M NaCl, 30 mM Na2 EDTA, pH 6.8), total RNA was isolated from the cells with
the RNeasy mini kit (Qiagen, Gaithersburg, MD), and DNase I treatment was
performed as described by the manufacturer to remove any contaminating
genomic DNA. Total RNA (750 ng) was reverse transcribed using 250 U/ml
Transcriptor Reverse Transcriptase (Roche Diagnostics, Mannheim, Germany),
0.08 U random primers (Roche diagnostics), and 1 mM of each dNTP (Invitrogen,
Carlsbad, CA) in Transcriptor RT reaction buffer at 42 °C for 45 min followed by
inactivation of the enzyme at 80 °C for 5 min. Real-time PCR reactions were
performed using the SYBRGreen reaction kit according to the manufacturer’s
instructions (Roche Diagnostics) in a LightCycler 480 (Roche Diagnostics). The
Light-Cycler reactions were prepared in 20 μl total volume with 7 μl PCR-H2O, 0.5
μl forward primer (0.2 μM), 0.5 μl reverse primer (0.2 μM), 10 μl LightCycler
Mastermix (LightCycler 480 SYBR Green I Master; Roche Diagnostics), to which 2
μl of 5 times diluted cDNA was added as PCR template. Primers (Invitrogen) used
for real-time PCR are listed in Table 1. Specific primers were designed from
sequences available in data banks, based on homology in conserved domains
between human, mouse, rat, dog and cow. The amplified PCR fragment extended
over at least one exon-border (except for 18S). Tyrosine 3-
monooxygenase/tryptophan 5-monooxygenase activation protein, zeta
polypeptide (Ywhaz) and hypoxanthine 18S (ribosomal RNA) were used as
housekeeping genes and the gene expression levels were normalized using a
normalization factor calculated with the equation √ (Ywhaz x 18S). With the
LightCycler software (version 4), the crossing points were assessed and plotted
versus the serial dilution of known concentrations of the standards derived from
each gene using the Fit Points method. PCR efficiency was calculated by Light-
Cycler software and the data were used only if the calculated PCR efficiency was
between 1.85 and 2.0.
Engineering alginate
39
Target
gene Oligonucleotide sequence
Annealing
temperature (°C)
Product
size (bp)
Ywhaz Forward 5' GATGAAGCCATTGCTGAACTTG 3' 56 229
Reverse 5' CTATTTGTGGGACAGCATGGA 3'
18S Forward 5' GTAACCCGTTGAACCCCATT 3' 56 151
Reverse 5' CCATCCAATCGGTAGTAGCG 3'
Agc Forward 5' CAACTACCCGGCCATCC 3' 57 160
Reverse 5' GATGGCTCTGTAATGGAACAC 3'
Col1a1 Forward 5' TCCAACGAGATCGAGATCC 3' 57 191
Reverse 5' AAGCCGAATTCCTGGTCT 3'
Col2a1 Forward 5' AGGGCCAGGATGTCCGGCA 3' 56 195
Reverse 5' GGGTCCCAGGTTCTCCATCT 3'
Ywhaz, tyrosine 3-monooxygenase/tryptophan 5-monooxygenase activation protein, zeta
polypeptide; 18S, 18S ribosomal RNA; Agc, aggrecan; Col1a1, α1(I)procollagen; Col2a1,
α1(II)procollagen
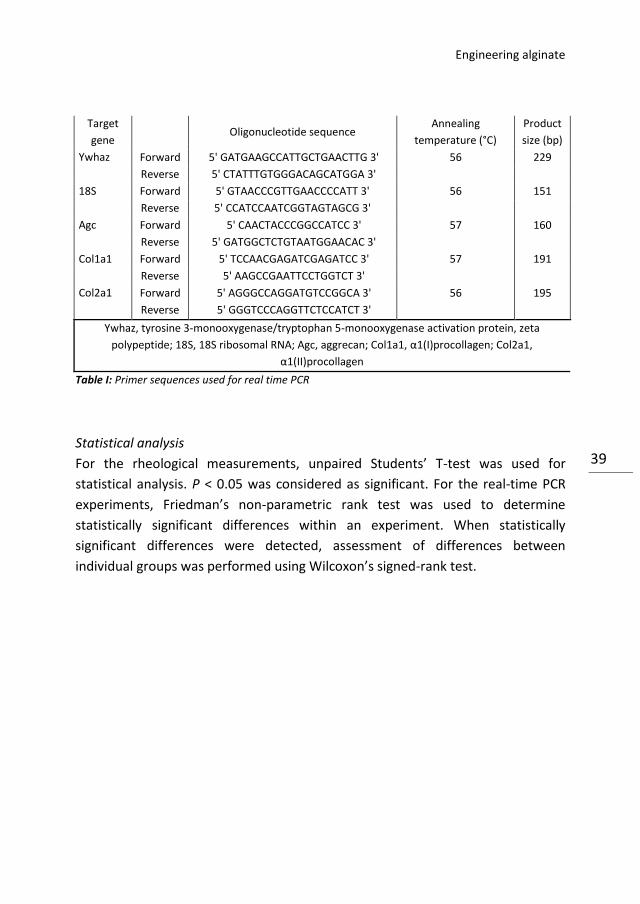
Table I: Primer sequences used for real time PCR
Statistical analysis
For the rheological measurements, unpaired Students’ T-test was used for
statistical analysis. P < 0.05 was considered as significant. For the real-time PCR
experiments, Friedman’s non-parametric rank test was used to determine
statistically significant differences within an experiment. When statistically
significant differences were detected, assessment of differences between
individual groups was performed using Wilcoxon’s signed-rank test.
Chapter 3
40
Results
Alginate sample discs prepared by different methods
We prepared alginate discs of concentrations between 1 and 6 wt% by two
different methods, namely by diffusion of Ca2+ ions from outside or by in situ
release of Ca2+ from calcium carbonate inside the alginate. To characterize the
viscoelastic properties, we performed small amplitude oscillatory shear tests on
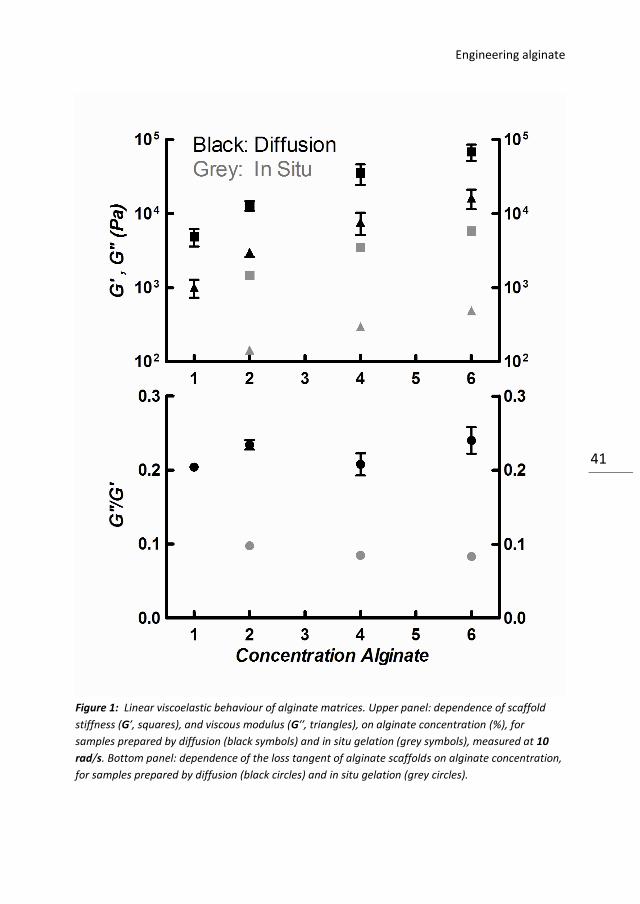
the alginate discs. Both series of samples became significantly stiffer with
increasing alginate concentration (square symbols, upper panel Fig. 1). However,
the samples prepared by diffusion (black squares) were at least ten-fold stiffer
than the in situ gelated samples (grey squares) at all alginate concentrations
(significant with P < 0.05). The sample-to-sample variability was higher for the
diffusion series than for the in situ series, as shown by the larger error bars. This
indicates that the diffusion samples were less homogeneous than the in situ
gelled samples, consistent with prior observations [32]. The viscous modulus of
the samples prepared by diffusion (black triangles) was also significantly larger
than that of the in situ polymerized samples (grey triangles). The loss tangent
(G′′/G′) was independent of alginate concentration for the diffusion gelated
samples (P > 0.05), as shown in the bottom panel of Fig. 1 (black circles). For the in
situ gelled samples (grey circles), the 4% and 6% alginate samples had a
significantly lower loss tangent than the 2% alginate samples (P < 0.05). The loss
tangent of the samples prepared by diffusion (black circles) was significantly
higher than that of samples that were gelled in situ (grey circles). These findings
implicate that the diffusion samples are stiffer but also have a higher viscosity. To
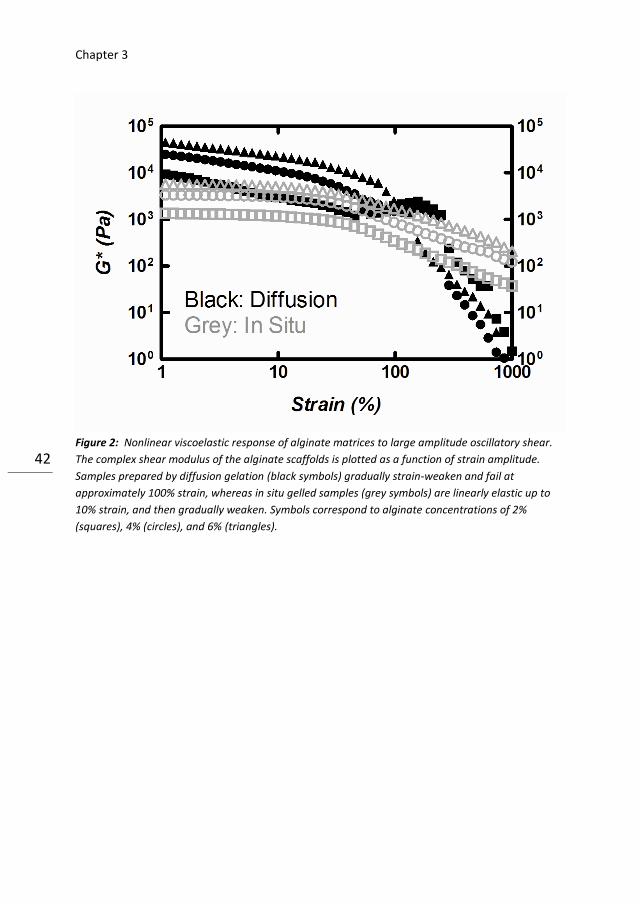
characterize the nonlinear viscoelastic behaviour, we subjected the alginate discs
to large amplitude oscillatory shear. The alginate samples prepared by diffusion
showed no appreciable linear elastic regime: their shear modulus immediately
started to decrease as the strain amplitude was raised, and they failed already at
strains of about 100% (black symbols in Fig. 2). In contrast, the samples prepared
by in situ gelation were linearly elastic up to strains of about 10%, and thereafter
gradually strain-weakened (grey symbols in Fig. 2).
Engineering alginate
41
Figure 1: Linear viscoelastic behaviour of alginate matrices. Upper panel: dependence of scaffold
stiffness (G′, squares), and viscous modulus (G′′, triangles), on alginate concentration (%), for
samples prepared by diffusion (black symbols) and in situ gelation (grey symbols), measured at 10
rad/s. Bottom panel: dependence of the loss tangent of alginate scaffolds on alginate concentration,
for samples prepared by diffusion (black circles) and in situ gelation (grey circles).
Chapter 3
42
Figure 2: Nonlinear viscoelastic response of alginate matrices to large amplitude oscillatory shear.
The complex shear modulus of the alginate scaffolds is plotted as a function of strain amplitude.
Samples prepared by diffusion gelation (black symbols) gradually strain-weaken and fail at
approximately 100% strain, whereas in situ gelled samples (grey symbols) are linearly elastic up to
10% strain, and then gradually weaken. Symbols correspond to alginate concentrations of 2%
(squares), 4% (circles), and 6% (triangles).
Engineering alginate
43
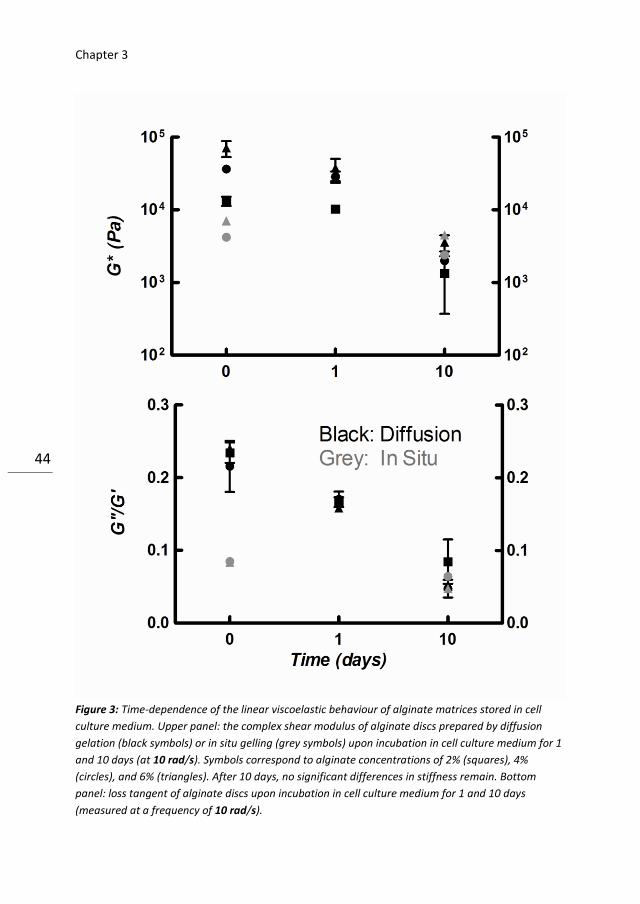
Stability of samples discs in cell culture medium
After prolonged incubation, all samples were visibly weaker than freshly prepared
samples. The samples of the lowest concentrations (1% for diffusion and 2% for in
situ gelation) had even become too fragile for testing by rheology. After 1 day of
incubation in cell culture medium, the diffusion samples already showed a 10%
reduction in elastic and viscous modulus (black symbols, upper panel Fig. 3). The
decreases of G′ and G′′ were statistically significant at alginate concentrations of
2% (black squares) and 6% samples (black triangles), but not at 4% (black circles;
G′ : P = 0.3, G′′ : P = 0.08). After 10 days, the moduli were ten-fold lower than the
original value at t = 0(P < 0.05). The samples gelled in situ also showed a
significant decline in stiffness, but less (~40% compared to the initial value), than
samples prepared by diffusion (~90% compared to the initial value), both at an
alginate concentration of 4% (grey circles) and 6% (grey triangles), as shown in the
upper panel of Fig. 3. After 10 days, there was no longer a significant difference in
stiffness between alginate samples of different concentrations or prepared by
different methods. As shown in the bottom panel of Fig. 3, the loss tangent of
samples prepared by diffusion (black symbols) and in situ gelling (grey symbols)
significantly decreased with increasing incubation time in medium, while being
independent of alginate concentration (compare 2%, squares, and 4%, circles).
The decrease of loss tangent of the 2% diffusion gelled samples only showed a
non-significant decline in the loss tangent after 10 days compared to day 0 and 1
(P = 0.07 and P = 0.16). After 10 days, the loss tangents of all samples were
statistically indistinguishable.
Chapter 3
44
Figure 3: Time-dependence of the linear viscoelastic behaviour of alginate matrices stored in cell
culture medium. Upper panel: the complex shear modulus of alginate discs prepared by diffusion
gelation (black symbols) or in situ gelling (grey symbols) upon incubation in cell culture medium for 1
and 10 days (at 10 rad/s). Symbols correspond to alginate concentrations of 2% (squares), 4%
(circles), and 6% (triangles). After 10 days, no significant differences in stiffness remain. Bottom
panel: loss tangent of alginate discs upon incubation in cell culture medium for 1 and 10 days
(measured at a frequency of 10 rad/s).
Engineering alginate
45
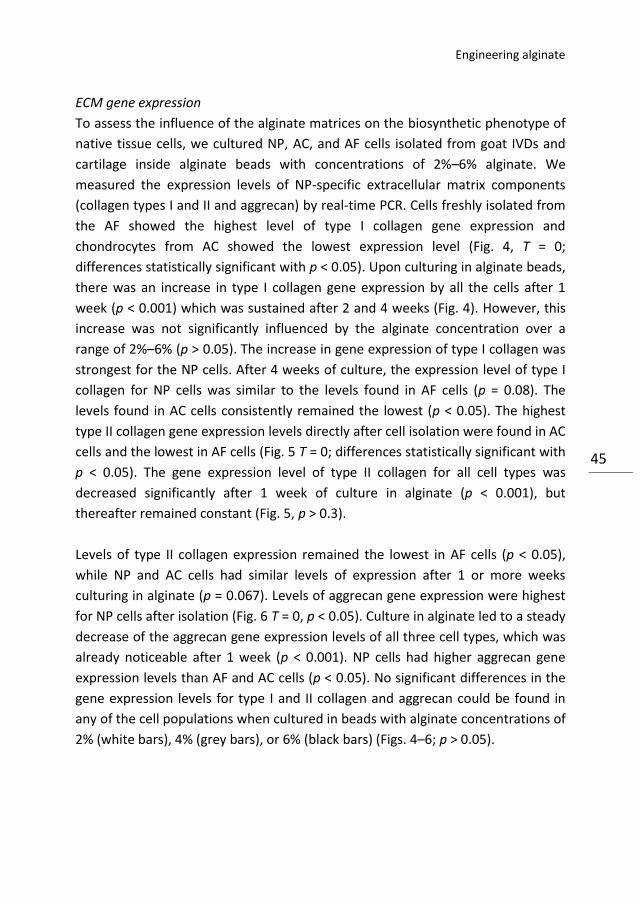
ECM gene expression
To assess the influence of the alginate matrices on the biosynthetic phenotype of
native tissue cells, we cultured NP, AC, and AF cells isolated from goat IVDs and
cartilage inside alginate beads with concentrations of 2%–6% alginate. We
measured the expression levels of NP-specific extracellular matrix components
(collagen types I and II and aggrecan) by real-time PCR. Cells freshly isolated from
the AF showed the highest level of type I collagen gene expression and
chondrocytes from AC showed the lowest expression level (Fig. 4, T = 0;
differences statistically significant with p < 0.05). Upon culturing in alginate beads,
there was an increase in type I collagen gene expression by all the cells after 1
week (p < 0.001) which was sustained after 2 and 4 weeks (Fig. 4). However, this
increase was not significantly influenced by the alginate concentration over a
range of 2%–6% (p > 0.05). The increase in gene expression of type I collagen was
strongest for the NP cells. After 4 weeks of culture, the expression level of type I
collagen for NP cells was similar to the levels found in AF cells (p = 0.08). The
levels found in AC cells consistently remained the lowest (p < 0.05). The highest
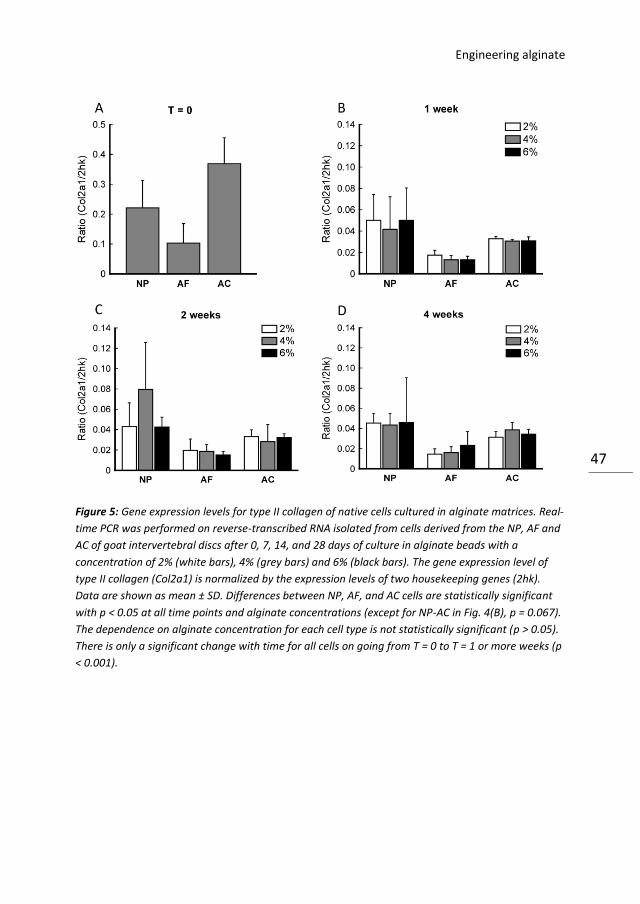
type II collagen gene expression levels directly after cell isolation were found in AC
cells and the lowest in AF cells (Fig. 5 T = 0; differences statistically significant with
p < 0.05). The gene expression level of type II collagen for all cell types was
decreased significantly after 1 week of culture in alginate (p < 0.001), but
thereafter remained constant (Fig. 5, p > 0.3).
Levels of type II collagen expression remained the lowest in AF cells (p < 0.05),
while NP and AC cells had similar levels of expression after 1 or more weeks
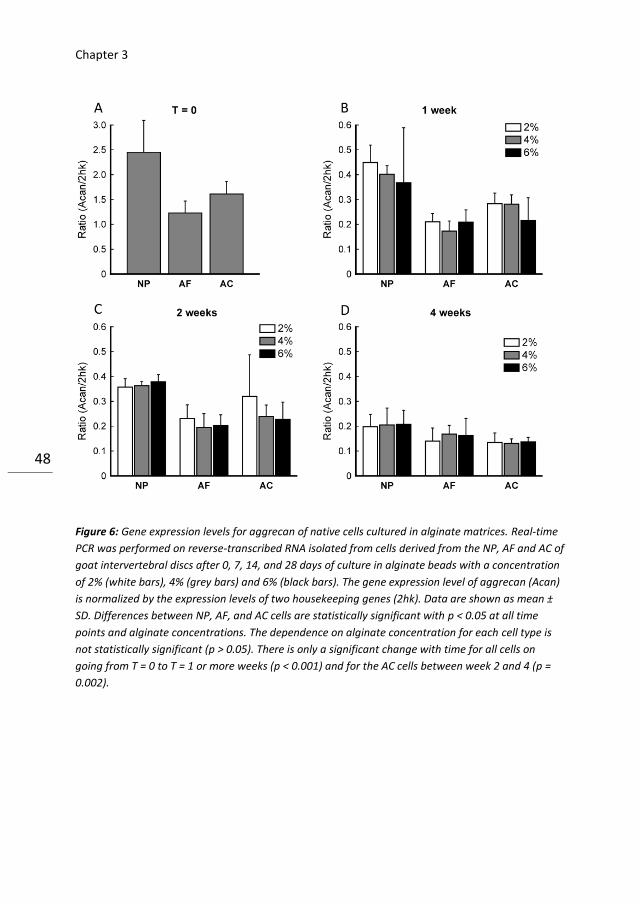
culturing in alginate (p = 0.067). Levels of aggrecan gene expression were highest
for NP cells after isolation (Fig. 6 T = 0, p < 0.05). Culture in alginate led to a steady
decrease of the aggrecan gene expression levels of all three cell types, which was
already noticeable after 1 week (p < 0.001). NP cells had higher aggrecan gene
expression levels than AF and AC cells (p < 0.05). No significant differences in the
gene expression levels for type I and II collagen and aggrecan could be found in
any of the cell populations when cultured in beads with alginate concentrations of
2% (white bars), 4% (grey bars), or 6% (black bars) (Figs. 4–6; p > 0.05).
Chapter 3
46
Figure 4: Gene expression levels for type I collagen of native cells cultured in alginate matrices. Real-
time PCR was performed on reverse-transcribed RNA isolated from cells derived from the NP, AF and
AC of goat intervertebral discs after 0, 7, 14, and 28 days of culture in alginate beads with a
concentration of 2% (white bars), 4% (grey bars) and 6% (black bars). The gene expression level of
type I collagen (Col1a1) is normalized by the expression levels of two housekeeping genes (2hk). Data
are shown as mean ± SD. Differences between NP, AF, and AC cells are statistically significant with p
< 0.05 at all time points and alginate concentrations (except for NP–AF in Fig. 4(D), p = 0.08). The
dependence on alginate concentration for each cell type is not statistically significant (p > 0.05).
Changes with time are significant for all cells on going from T = 0 to later time points (p < 0.001), and
for NP cells there is a significant increase between T = 1 week to 4 weeks (p = 0.03). Otherwise, there
are no statistically significant time changes.
Engineering alginate
47
Figure 5: Gene expression levels for type II collagen of native cells cultured in alginate matrices. Real-
time PCR was performed on reverse-transcribed RNA isolated from cells derived from the NP, AF and
AC of goat intervertebral discs after 0, 7, 14, and 28 days of culture in alginate beads with a
concentration of 2% (white bars), 4% (grey bars) and 6% (black bars). The gene expression level of
type II collagen (Col2a1) is normalized by the expression levels of two housekeeping genes (2hk).
Data are shown as mean ± SD. Differences between NP, AF, and AC cells are statistically significant
with p < 0.05 at all time points and alginate concentrations (except for NP-AC in Fig. 4(B), p = 0.067).
The dependence on alginate concentration for each cell type is not statistically significant (p > 0.05).
There is only a significant change with time for all cells on going from T = 0 to T = 1 or more weeks (p
< 0.001).
Chapter 3
48
Figure 6: Gene expression levels for aggrecan of native cells cultured in alginate matrices. Real-time
PCR was performed on reverse-transcribed RNA isolated from cells derived from the NP, AF and AC of
goat intervertebral discs after 0, 7, 14, and 28 days of culture in alginate beads with a concentration
of 2% (white bars), 4% (grey bars) and 6% (black bars). The gene expression level of aggrecan (Acan)
is normalized by the expression levels of two housekeeping genes (2hk). Data are shown as mean ±
SD. Differences between NP, AF, and AC cells are statistically significant with p < 0.05 at all time
points and alginate concentrations. The dependence on alginate concentration for each cell type is
not statistically significant (p > 0.05). There is only a significant change with time for all cells on
going from T = 0 to T = 1 or more weeks (p < 0.001) and for the AC cells between week 2 and 4 (p =
0.002).

Engineering alginate
49
Discussion
The principal aim of the current study was to design alginate scaffolds with
viscoelastic properties that mimic those of the NP. We showed that the stiffness
of alginate scaffolds, crosslinked by diffusion of calcium into the alginate solution,
can be varied over two orders of magnitude (between 1 kPa and almost 100 kPa)
by varying the alginate concentration. The loss tangent was not affected by
variations in polymer concentration. The closest matching of the stiffness as well
as loss tangent of a healthy NP, which has a stiffness of 11 kPa and loss tangent of
about 0.24 [21], was found for 2% alginate scaffolds. Other cartilaginous tissues
are stiffer than even the most concentrated alginate discs (6%) (Table 2). It is
difficult to prepare more concentrated alginate discs because the high viscosity of
the pre-gelled solution renders it difficult to process and mould the gel and to mix
in cells [3]. However, this difficulty may be counteracted by stirring the alginate
solutions, which are shear-thinning [3]. Moreover, the stiffness of alginate
scaffolds may be tuned by other factors, such as the alginate source, G/M ratio,
cross linker type, and temperature [3,23,27,32]. However, these factors are not
always accessible for manipulation in the context of tissue engineering. The G/M
ratio depends on alginate source and processing and is therefore usually fixed
upon delivery [23,25]. Changes in Ca2+ concentration and temperature influence
gelation time and thereby matrix organization and stiffness [3], but these
variations are not always well tolerated by seeded cells. We also compared
samples derived by diffusion gelation to samples prepared by in situ release of
Ca2+ [32].
Chapter 3
50
The “in situ” method has several practical advantages over the diffusion method
for clinical applications in tissue engineering. The liquid solution can be injected
via a syringe and gelation occurs inside the tissue of interest. Moreover, in situ
gelation results in more homogeneous scaffolds with less spatial and sample to-
sample variation in biomechanical properties. Scaffolds prepared by diffusion are
notoriously inhomogeneous due to the diffusion kinetics of calcium ions. Although
we prepared the diffusion scaffolds under standardized circumstances, the
structural inhomogeneity appeared to affect the rheology and may have affected
cell phenotype. The stiffness of alginate samples prepared by in situ gelation was
much lower than that of the diffusion samples, consistent with prior findings [28].
To assess the applicability of alginate discs for IVD repair, it is also crucial to
characterize the biological response of native tissue cells to prolonged culture in
an alginate matrix. We therefore screened the effects of alginate scaffolds
(prepared by diffusion) on native cells by measuring gene expression of
extracellular matrix components that are naturally present in the NP. The relative
gene expression levels for types I and II collagen found in native IVD cells after
isolation is in line with the well-known collagenous composition of these tissues
[1]. The AF contains a mixture of type I and II collagen, the NP contains more type
II collagen than the AF, and the AC contains predominantly type II collagen [1,22].
Aside from collagens, proteoglycans (mainly aggrecan) are the main components
of cartilage. The NP contains the highest amount of proteoglycans and the AF the
lowest amount [1,22]. This is reflected by the high gene expression levels of
aggrecan seen in native NP cells and the low levels found in native AF cells. The
differences found between the cell populations after isolation were mostly
maintained during culture in alginate beads, suggesting that alginate preserves
the phenotypical characteristics of the cells. Although we observed a decrease in
the gene expression levels of type II collagen and aggrecan during culture in
alginate beads, it has been reported that AC and IVD cells do produce
considerable amounts of both proteins under these culture conditions
[8,16,31,37]. In contrast, cells cultured on polystyrene dishes lose the ability to
synthesize aggrecan and type II collagen and start to produce more type I collagen
[9]. We did not observe any effect of variations in the alginate concentration on
gene expression levels of type I and type II collagen or aggrecan by NP, AF or AC
cells cultured within alginate gels (Figs. 4–6). This observation is in contrast with

Engineering alginate
51
observations on other cell types cultured on top of flat elastic hydrogels, where a
pronounced influence of matrix stiffness on ECM synthesis has been documented
[4]. However, a requirement for a stiffness-responsive cell phenotype is that the
cell adheres to the scaffold material via integrin adhesions so that the cell can
exert traction forces to the matrix by actomyosin contractility [13]. Cells have no
integrin receptors for alginate and therefore adhere very weakly to alginate
matrices [3]. They can therefore not actively respond to matrix stiffness via focal
adhesion sites. Several methods to promote cell attachment to alginate matrices
are currently being studied; for instance, by coupling of extracellular matrix
proteins such as laminin, collagen, fibronectin, or RGD peptides [2,3,11,19]. We
note that another reason for the lack of sensitivity to matrix stiffness observed in
our study may be the rapid reduction of matrix stiffness upon prolonged exposure
to cell culture medium. Similarly, it has been documented that alginate scaffolds
rapidly soften after implantation in vivo [32]. This softening has been attributed to
the loss of divalent crosslinking cations at neutral pH [3].
In our study, we observed a 10% decline in stiffness after 1 day and a ten-fold
decline after 10 days in medium in samples prepared by diffusion (Fig. 3). The ‘in
situ’ gelled samples softened less in medium, but were much softer than samples
prepared by diffusion to begin with, so that their stiffness after 10 days was
similar to that of the diffusion samples. The consequence of the loss of stiffness is
that the 2% alginate scaffold no longer matched
the stiffness of the NP after 10 days. Moreover, even the stiffness of the 6%
alginate scaffolds was lower than that of the NP after 10 days. Several methods to
prevent the loss of stiffness during storage in medium have been reported.
Arguably the most straightforward method is to supplement Ca2+ to the medium.
However, this strategy is not attractive in the context of NP regeneration, where
chondrogenic differentiation is required, since calcium has osteogenic effects.
Moreover, the Ca2+ concentration of the environment is difficult to control after
in vivo implantation. An alternative strategy is the addition of cationic
polyethyleneimine to alginate to increase the resistance to de-crosslinking
[23,24]. Finally, the addition of cells is known to have stabilizing effects on the
alginate matrix [3]. We could not test this stabilizing effect with native IVD cells,
because there were not enough cells available for the large sample sizes required
for rheology. In fact, limited availability of cells is also a limiting factor for IVD
Chapter 3
52
engineering with native cells [5]. In patients, the availability of IVD tissue for
digestion is even less than in our study, in which we used pooled IVDs derived
from goat thoracic spines. An attractive alternative is the use of mesenchymal
stem cells [30], but differentiation towards NP or AF phenotypes is still not fully
directional [5]. Furthermore, specific phenotypic markers to distinguish both cell
types are currently being elucidated [26,34,36,37].
In conclusion, we showed that the stiffness of alginate scaffolds can be varied by
tuning the alginate polymer concentration and can be matched to the stiffness of
the NP. Moreover, the biosynthetic phenotype of native IVD cells is maintained
upon prolonged culture in alginate matrices. There are still some practical
limitations that need to be solved, specifically the long-term mechanical stability
in vivo, the bioadhesive properties, and the availability of tissue cells from the
patient. Current study underscores the potential of alginate as a scaffold material
for IVD engineering, but more importantly reveals some important limitations,
which in spite of many promising research over the past decade, still have to be
overcome.
Engineering alginate
53
References
1. Almarza AJ, Athanasiou KA (2004) Design characteristics for the tissue engineering of
cartilaginous tissues. Ann Biomed Eng 32: 2-17
2. Alsberg E, Anderson KW, Albeiruti A, Franceschi RT, Mooney DJ (2001) Cell-interactive
alginate hydrogels for bone tissue engineering. J Dent Res 80: 2025-2029
3. Augst AD, Kong HJ, Mooney DJ (2006) Alginate hydrogels as biomaterials. Macromol
Biosci 6: 623-633
4. Breuls RG, Jiya TU, Smit TH (2008) Scaffold stiffness influences cell behavior:
opportunities for skeletal tissue engineering. Open Orthop J 2: 103:109
5. Bron JL, Helder MN, Meisel HJ, Van Royen BJ, Smit TH (2009) Repair, regenerative and
supportive therapies of the annulus fibrosus: achievements and challenges. Eur Spine J 18:
301-313
6. Bron JL, Koenderink GH, Everts V, Smit TH (2009) Rheological characterization of the
nucleus pulposus and dense collagen scaffolds intended for functional replacement.
J Orthop Res 27: 620-626
7. Bron JL, Van der Veen AJ, Helder MN, Van Royen BJ, Smit TH (2010) Biomechanical and
in vivo evaluation of experimental closure devices of the annulus fibrosus designed for a
goat nucleus replacement model. Eur Spine J 19: 1347-1355
8. Chubinskaya S, Huch K, Schulze M, Otten L, Aydelotte MB, Cole AA (2001) Gene
expression by human articular chondrocytes cultured in alginate beads. J Histochem
Cytochem 49: 1211-1220
9. Darling EM, Athanasiou KA (2005) Rapid phenotypic changes in passaged articular
chondrocyte subpopulations. J Orthop Res 23: 425-432
10. De CF, Lesur C, Pastoureau P, Caliez A, Sabatini M (2004) Culture of chondrocytes in
alginate beads. Methods Mol Biol 100: 15-22
11. Degala S, Zipfel WR, Bonassar LJ (2011) Chondrocyte calcium signaling in response to
fluid flow is regulated by matrix adhesion in 3-D alginate scaffolds. Arch Biochem Biophys
505: 112-117
12. Discher DE, Janmey P, Wang YL (2005) Tissue cells feel and respond to the stiffness of
their substrate. Science 310: 1139-1143
13. Discher DE, Mooney DJ, Zandstra PW (2009) Growth factors, matrices, and forces
combine and control stem cells. Science 324: 1673-1677
14. Engler AJ, Sweeney HL, Discher DE, Schwarzbauer JE (2007) Extracellular matrix
elasticity directs stem cell differentiation. J Musculoskelet Neuronal Interact 7: 335
15. Gruber HE, Fisher Jr EC, Desai B, Stasky AA, Hoelscher G, Hanley Jr EN (1997) Human
intervertebral disc cells from the annulus: three-dimensional culture in agarose or alginate
and responsiveness to TGF-beta1. Exp Cell Res 235: 13-21
16. Hauselmann HJ, Fernandes RJ, Mok SS, Schmid TM, Block JA, Aydelotte MB, Kuettner
KE, Thonar EJ (1994) Phenotypic stability of bovine articular chondrocytes after

Chapter 3
54
long-term culture in alginate beads. J Cell Sci 107 (Pt. 1): 17-27
17. Hegewald AA, Ringe J, Sittinger M, Thome C (2008) Regenerative treatment strategies
in spinal surgery. Front Biosci 13: 1507-1525
18. Hubbell JA (2003) Materials as morphogenetic guides in tissue engineering. Curr Opin
Biotechnol 14: 551-558
19. Huebsch N, Arany PR, Mao AS, Shvartsman D, Ali OA, Bencherif SA, Rivera-Feliciano J,
Mooney DJ (2010) Harnessing traction-mediated manipulation of the cell/matrix interface
to control stem-cell fate. Nat Mater 9: 518-526
20. Huebsch N, Mooney DJ (2009) Inspiration and application in the evolution of
biomaterials. Nature 462: 426-432
21. Iatridis JC, Weidenbaum M, Setton LA, Mow VC (1996) Is the nucleus pulposus a solid
or a fluid? Mechanical behaviors of the nucleus pulposus of the human intervertebral disc.
Spine 21: 1174–1184 (Phila Pa 1976)
22. Kuettner KE, Cole AA (2005) Cartilage degeneration in different human joints.
Osteoarthr Cartilage 13: 93-103
23. Kuo CK, Ma PX (2001) Ionically crosslinked alginate hydrogels as scaffolds for tissue
engineering: part 1. Structure, gelation rate and mechanical properties. Biomaterials 22:
511-521
24. Kuo CK, Ma PX (2008) Maintaining dimensions and mechanical properties of ionically
crosslinked alginate hydrogel scaffolds in vitro. J Biomed Mater Res Part A 84: 899–907
25. Larsen B, Haug A (1971) Biosynthesis of alginate. 1. Composition and structure of
alginate produced by Azotobacter vinelandii (Lipman). Carbohydr Res 17: 287-296
26. Lee CR, Sakai D, Nakai T, Toyama K, Mochida J, Alini M, Grad S (2007) A phenotypic
comparison of intervertebral disc and articular cartilage cells in the rat. Eur Spine J 16:
2174-2185
27. Leone G, Torricelli P, Chiumiento A, Facchini A, Barbucci R (2008) Amidic alginate
hydrogel for nucleus pulposus replacement. J Biomed Mater Res Part A 84: 391-401
28. Li Z, Gunn J, Chen MH, Cooper A, Zhang M (2008) On-site alginate gelation for
enhanced cell proliferation and uniform distribution in porous scaffolds. J Biomed Mater
Res Part A 86: 552-559
29. Lin YJ, Yen CN, Hu YC, Wu YC, Liao CJ, Chu IM (2009) Chondrocytes culture in three-
dimensional porous alginate scaffolds enhanced cell proliferation, matrix synthesis and
gene expression. J Biomed Mater Res Part A 88: 23-33
30. Lutolf MP, Gilbert PM, Blau HM (2009) Designing materials to direct stem-cell fate.
Nature 462: 433-441
31. Masuda K, Sah RL, Hejna MJ, Thonar EJ (2003) A novel twostep method for the
formation of tissue-engineered cartilage by mature bovine chondrocytes: the alginate-
recoveredchondrocyte (ARC) method. J Orthop Res 21: 139-148
Engineering alginate
55
32. Nunamaker EA, Purcell EK, Kipke DR (2007) In vivo stability and biocompatibility of
implanted calcium alginate disks. J Biomed Mater Res Part A 83: 1128-1137
33. Roberts S, Evans H, Trivedi J, Menage J (2006) Histology and pathology of the human
intervertebral disc. J Bone Joint Surg Am 88 (Suppl. 2): 10-14
34. Rutges J, Creemers LB, Dhert W, Milz S, Sakai D, Mochida J, Alini M, Grad S (2010)
Variations in gene and protein expression in human nucleus pulposus in comparison with
annulus fibrosus and cartilage cells: potential associations with aging and degeneration.
Osteoarthr Cartilage 18: 416-423
35. Saad L, Spector M (2004) Effects of collagen type on the behavior of adult canine
annulus fibrosus cells in collagen–glycosaminoglycan scaffolds. J Biomed Mater Res Part A
71: 233-241
36. Sakai D, Nakai T, Mochida J, Alini M, Grad S (2009) Differential phenotype of
intervertebral disc cells: microarray and immunohistochemical analysis of canine nucleus
pulposus and anulus fibrosus. Spine 34: 1448-1456 (Phila Pa 1976)
37. Vonk LA, Kroeze RJ, Doulabi BZ, Hoogendoorn RJ, Huang C, Helder MN, Everts V, Bank
RA (2010) Caprine articular, meniscus and intervertebral disc cartilage: an integral analysis
of collagen network and chondrocytes. Matrix Biol 29: 209-218

Chapter 3
56
4 Migration of intervertebral disc cells into
dense collagen scaffolds intended for
functional replacement.
J L Bron
HW Mulder
LA Vonk
BZ Doulabi
MJ Oudhoff
TH Smit
Chapter 4
58
Abstract
Invasion of cells from surrounding tissues is a crucial step for regeneration when
using a-cellular scaffolds as a replacement of the nucleus pulposus (NP). Aim of
the current study was to assess whether NP and surrounding annulus fibrosus (AF)
cells are capable of migrating into dense collagen scaffolds. We seeded freshly
harvested caprine NP and AF cells onto scaffolds consisting of 1.5 and 3.0% type I
collagen matrices, prepared by plastic compression, to assess cell invasion. The
migration distance was dependent both on time and on collagen density and was
higher for NP (25% of scaffold thickness) compared to AF (10%) cells after 4
weeks. Migration distance was not enhanced by Hst-2, a peptide derived from
saliva known to enhance fibroblast migration, and this was confirmed in a scratch
assay. In conclusion, we revealed invasion of cells into dense collagen scaffolds
and therewith encouraging first steps towards the use of a-cellular scaffolds for
NP replacement.

Migration of intervertebral disc cells
59
Introduction
Lumbar discectomy is an effective therapy for neurological decompression in
patients suffering from a herniated nucleus pulposus (NP). Discectomies however,
do not deal with the damaged intervertebral disc (IVD) and may even further
aggravate existing damage [17]. In the majority of the patients, radiological signs
of disc degeneration are present after 2 years [18]. It is therefore not surprising,
that after a successful decompression, many patients suffer from persisting or
progressive low back pain. After 10 years follow-up, almost one third of the
patients are dissatisfied and a quarter underwent re-surgery in the meantime [5,
9, 16, 29]. During the last decade, increasing knowledge and technical
advancements in the field of tissue engineering have resulted in numerous
promising strategies to replace or regenerate the NP [17, 20]. Materials that have
been used include collagen, chitosan, alginate and fibrin [1–3, 6, 7, 19, 32]. All of
them have their own advantages, disadvantages, and clinical potential. In chapter
2, we showed that with very dense collagen scaffolds (23% or ~230 mg/mL),
prepared by plastic compression, the viscoelastic properties of native NP tissue
can be approached [6]. Scaffold stiffness is increasingly recognized as a potent
mechanical cue for the differentiation and biosynthetic response of (stem) cells [4,
6, 10–12, 14]. Our overall goal is to develop a-cellular collagen scaffolds that can
be used to replace the NP in one surgical procedure combined with a discectomy.
The scaffolds should prevent the degenerative cascade of the intervertebral disc
and surrounding structures, which is initiated directly after disc herniation.
Furthermore, restoration of the biomechanical properties should facilitate
regeneration of the herniated disc. The advantage of using an a-cellular scaffold is
the absence of time-consuming and expensive cell harvesting and culturing
techniques during surgery. Instead, cells from the surrounding tissue are
hypothesized to migrate into the scaffold thereby digesting the scaffold and
secreting their own native extra cellular matrix (ECM) [6, 17]. The invasion of cells,
also called ‘in situ seeding’, should occur from tissues that are in direct contact
with the scaffold and thus only include the remnants of the NP and the
surrounding annulus fibrosus (AF) [5].
The aim of the current study is to investigate if AF and NP cells are actually
capable of migrating into dense collagen scaffolds. We investigate the migration
of cells into scaffolds with densities of 1.5% (~15 mg/mL) and 3.0% (~30 mg/mL)
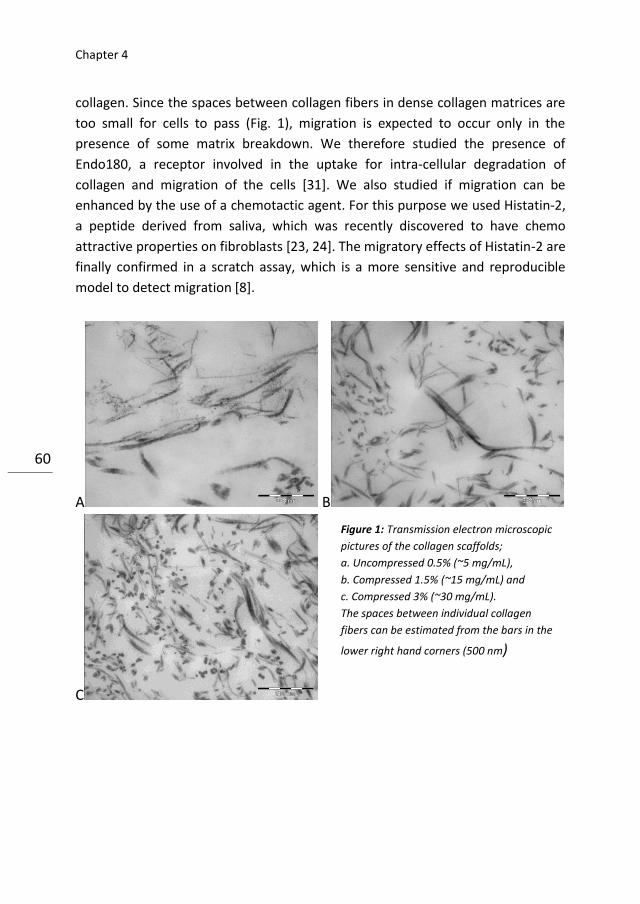
Chapter 4
60
collagen. Since the spaces between collagen fibers in dense collagen matrices are
too small for cells to pass (Fig. 1), migration is expected to occur only in the
presence of some matrix breakdown. We therefore studied the presence of
Endo180, a receptor involved in the uptake for intra-cellular degradation of
collagen and migration of the cells [31]. We also studied if migration can be
enhanced by the use of a chemotactic agent. For this purpose we used Histatin-2,
a peptide derived from saliva, which was recently discovered to have chemo
attractive properties on fibroblasts [23, 24]. The migratory effects of Histatin-2 are
finally confirmed in a scratch assay, which is a more sensitive and reproducible
model to detect migration [8].
A B
C
Figure 1: Transmission electron microscopic
pictures of the collagen scaffolds;
a. Uncompressed 0.5% (~5 mg/mL),
b. Compressed 1.5% (~15 mg/mL) and
c. Compressed 3% (~30 mg/mL).
The spaces between individual collagen
fibers can be estimated from the bars in the
lower right hand corners (500 nm)
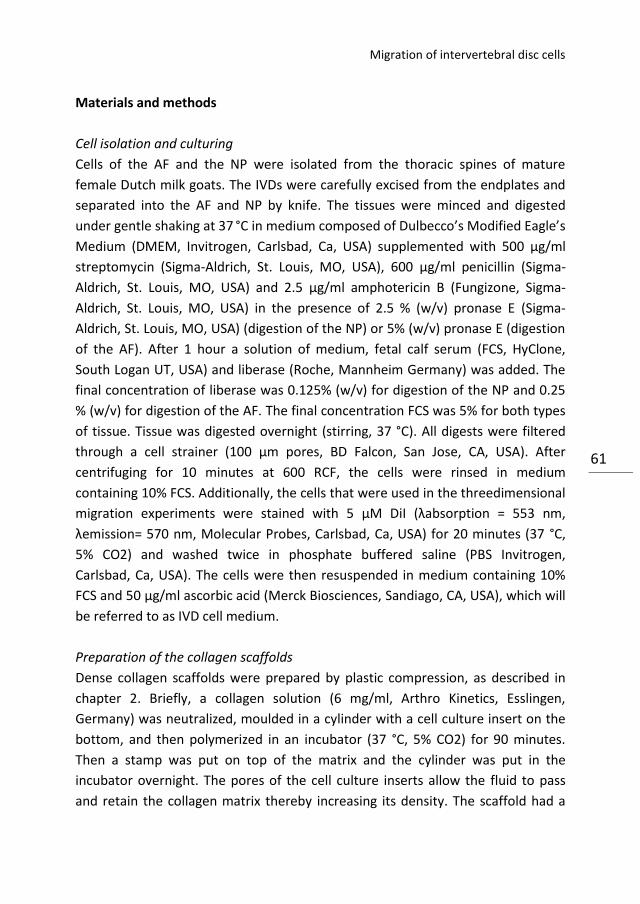
Migration of intervertebral disc cells
61
Materials and methods
Cell isolation and culturing
Cells of the AF and the NP were isolated from the thoracic spines of mature
female Dutch milk goats. The IVDs were carefully excised from the endplates and
separated into the AF and NP by knife. The tissues were minced and digested
under gentle shaking at 37 °C in medium composed of Dulbecco’s Modified Eagle’s
Medium (DMEM, Invitrogen, Carlsbad, Ca, USA) supplemented with 500 μg/ml
streptomycin (Sigma-Aldrich, St. Louis, MO, USA), 600 μg/ml penicillin (Sigma-
Aldrich, St. Louis, MO, USA) and 2.5 μg/ml amphotericin B (Fungizone, Sigma-
Aldrich, St. Louis, MO, USA) in the presence of 2.5 % (w/v) pronase E (Sigma-
Aldrich, St. Louis, MO, USA) (digestion of the NP) or 5% (w/v) pronase E (digestion
of the AF). After 1 hour a solution of medium, fetal calf serum (FCS, HyClone,
South Logan UT, USA) and liberase (Roche, Mannheim Germany) was added. The
final concentration of liberase was 0.125% (w/v) for digestion of the NP and 0.25
% (w/v) for digestion of the AF. The final concentration FCS was 5% for both types
of tissue. Tissue was digested overnight (stirring, 37 °C). All digests were filtered
through a cell strainer (100 μm pores, BD Falcon, San Jose, CA, USA). After
centrifuging for 10 minutes at 600 RCF, the cells were rinsed in medium
containing 10% FCS. Additionally, the cells that were used in the threedimensional
migration experiments were stained with 5 μM DiI (λabsorption = 553 nm,
λemission= 570 nm, Molecular Probes, Carlsbad, Ca, USA) for 20 minutes (37 °C,
5% CO2) and washed twice in phosphate buffered saline (PBS Invitrogen,
Carlsbad, Ca, USA). The cells were then resuspended in medium containing 10%
FCS and 50 μg/ml ascorbic acid (Merck Biosciences, Sandiago, CA, USA), which will
be referred to as IVD cell medium.
Preparation of the collagen scaffolds
Dense collagen scaffolds were prepared by plastic compression, as described in
chapter 2. Briefly, a collagen solution (6 mg/ml, Arthro Kinetics, Esslingen,
Germany) was neutralized, moulded in a cylinder with a cell culture insert on the
bottom, and then polymerized in an incubator (37 °C, 5% CO2) for 90 minutes.
Then a stamp was put on top of the matrix and the cylinder was put in the
incubator overnight. The pores of the cell culture inserts allow the fluid to pass
and retain the collagen matrix thereby increasing its density. The scaffold had a
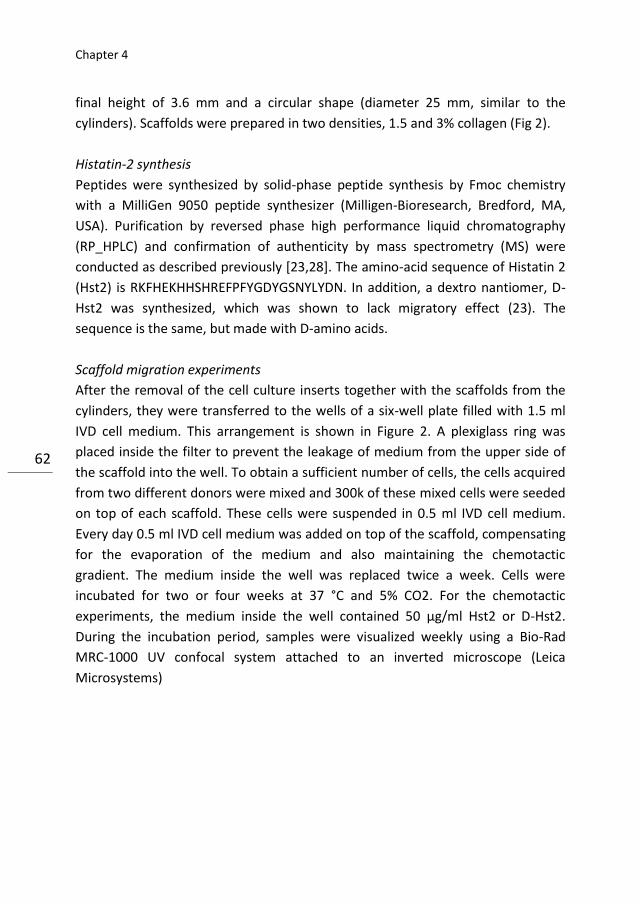
Chapter 4
62
final height of 3.6 mm and a circular shape (diameter 25 mm, similar to the
cylinders). Scaffolds were prepared in two densities, 1.5 and 3% collagen (Fig 2).
Histatin-2 synthesis
Peptides were synthesized by solid-phase peptide synthesis by Fmoc chemistry
with a MilliGen 9050 peptide synthesizer (Milligen-Bioresearch, Bredford, MA,
USA). Purification by reversed phase high performance liquid chromatography
(RP_HPLC) and confirmation of authenticity by mass spectrometry (MS) were
conducted as described previously [23,28]. The amino-acid sequence of Histatin 2
(Hst2) is RKFHEKHHSHREFPFYGDYGSNYLYDN. In addition, a dextro nantiomer, D-
Hst2 was synthesized, which was shown to lack migratory effect (23). The
sequence is the same, but made with D-amino acids.
Scaffold migration experiments
After the removal of the cell culture inserts together with the scaffolds from the
cylinders, they were transferred to the wells of a six-well plate filled with 1.5 ml
IVD cell medium. This arrangement is shown in Figure 2. A plexiglass ring was
placed inside the filter to prevent the leakage of medium from the upper side of
the scaffold into the well. To obtain a sufficient number of cells, the cells acquired
from two different donors were mixed and 300k of these mixed cells were seeded
on top of each scaffold. These cells were suspended in 0.5 ml IVD cell medium.
Every day 0.5 ml IVD cell medium was added on top of the scaffold, compensating
for the evaporation of the medium and also maintaining the chemotactic
gradient. The medium inside the well was replaced twice a week. Cells were
incubated for two or four weeks at 37 °C and 5% CO2. For the chemotactic
experiments, the medium inside the well contained 50 μg/ml Hst2 or D-Hst2.
During the incubation period, samples were visualized weekly using a Bio-Rad
MRC-1000 UV confocal system attached to an inverted microscope (Leica
Microsystems)
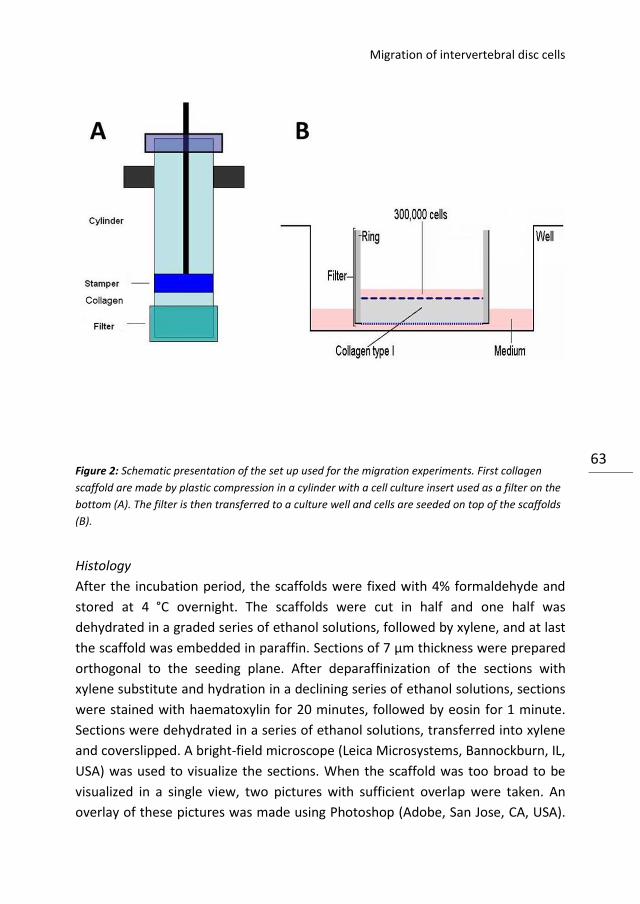
Migration of intervertebral disc cells
63 Figure 2: Schematic presentation of the set up used for the migration experiments. First collagen
scaffold are made by plastic compression in a cylinder with a cell culture insert used as a filter on the
bottom (A). The filter is then transferred to a culture well and cells are seeded on top of the scaffolds
(B).
Histology
After the incubation period, the scaffolds were fixed with 4% formaldehyde and
stored at 4 °C overnight. The scaffolds were cut in half and one half was
dehydrated in a graded series of ethanol solutions, followed by xylene, and at last
the scaffold was embedded in paraffin. Sections of 7 μm thickness were prepared
orthogonal to the seeding plane. After deparaffinization of the sections with
xylene substitute and hydration in a declining series of ethanol solutions, sections
were stained with haematoxylin for 20 minutes, followed by eosin for 1 minute.
Sections were dehydrated in a series of ethanol solutions, transferred into xylene
and coverslipped. A bright-field microscope (Leica Microsystems, Bannockburn, IL,
USA) was used to visualize the sections. When the scaffold was too broad to be
visualized in a single view, two pictures with sufficient overlap were taken. An
overlay of these pictures was made using Photoshop (Adobe, San Jose, CA, USA).
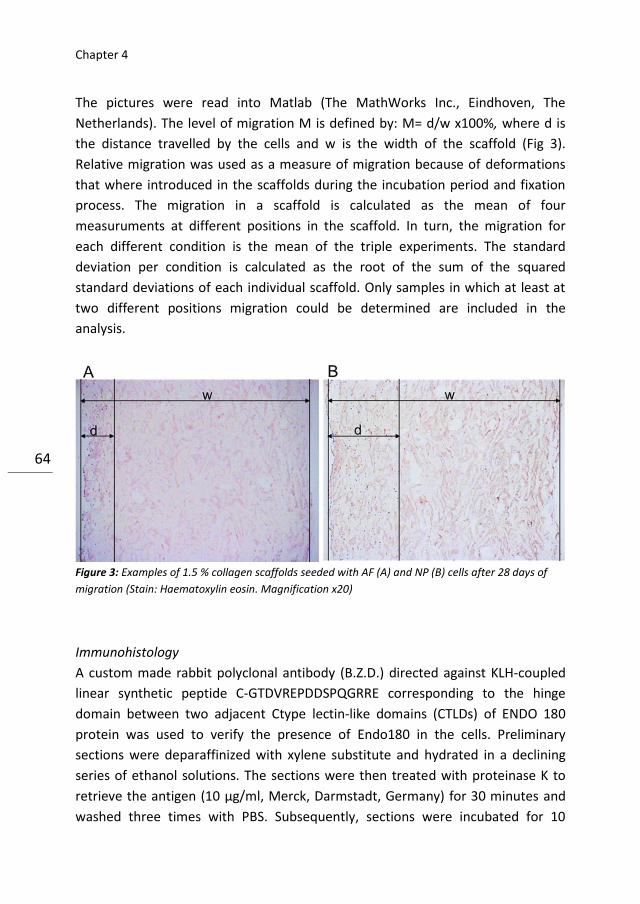
Chapter 4
64
The pictures were read into Matlab (The MathWorks Inc., Eindhoven, The
Netherlands). The level of migration M is defined by: M= d/w x100%, where d is
the distance travelled by the cells and w is the width of the scaffold (Fig 3).
Relative migration was used as a measure of migration because of deformations
that where introduced in the scaffolds during the incubation period and fixation
process. The migration in a scaffold is calculated as the mean of four
measuruments at different positions in the scaffold. In turn, the migration for
each different condition is the mean of the triple experiments. The standard
deviation per condition is calculated as the root of the sum of the squared
standard deviations of each individual scaffold. Only samples in which at least at
two different positions migration could be determined are included in the
analysis.
Figure 3: Examples of 1.5 % collagen scaffolds seeded with AF (A) and NP (B) cells after 28 days of
migration (Stain: Haematoxylin eosin. Magnification x20)
Immunohistology
A custom made rabbit polyclonal antibody (B.Z.D.) directed against KLH-coupled
linear synthetic peptide C-GTDVREPDDSPQGRRE corresponding to the hinge
domain between two adjacent Ctype lectin-like domains (CTLDs) of ENDO 180
protein was used to verify the presence of Endo180 in the cells. Preliminary
sections were deparaffinized with xylene substitute and hydrated in a declining
series of ethanol solutions. The sections were then treated with proteinase K to
retrieve the antigen (10 μg/ml, Merck, Darmstadt, Germany) for 30 minutes and
washed three times with PBS. Subsequently, sections were incubated for 10

Migration of intervertebral disc cells
65
minutes with 3% hydrogen peroxide in methanol to block endogenous peroxidase
activity and washed again with PBS. Sections were incubated with blocking
solution (Zymed Laboratories, San Francisco, CA, USA) for 30 minutes and
incubated with affinity purified primary antibody (1,3 μg/ml) for 30 minutes at
room temperature followed by incubation overnight at 4 oC. Universal negative
control (rabbit antibodies, Dako) was used as negative control. Next day sections
were washed with a solution of TBS, 0.25% BSA and 0.5% Triton X-100 and
incubated for 30 minutes with 1:500 diluted HRP-labelled sheep anti-rabbit
secondary antibody (Dako). After washing with PBS, sections were incubated for
15 minutes with 3,3’-diaminobenzidine (DAB) and hydrogen peroxide (peroxidase
substrate kit DAB, Vector Laboratories, Burlingame, CA, USA) and washed in
distilled water. Sections were counterstained with Mayer’s haematoxylin or 2
minutes.
Scratch assay
The effects of Hst2 on the migration of AF and NP cells were also examined in a
2D scratch assay. In 48-well plates, 25,000 cells were seeded and cultured until
confluence in IVD cell medium. After five hours of serum deprivation a scratch
was made using a sterile blue pipette tip. The following conditions were tested:
IVD cell medium without serum, IVD cell medium without serum containing 10, 50
or 100 μg/ml Hst2 or 50 μg/ml D-Hst2, and IVD cell medium. The scratch was
photographed at the day of creation (day 0) and after two days. For each sample
the surface area of the scratch was determined in the open source software
ImageJ. Per donor the mean of the experiments performed in triplicate was
calculated. From these mean values relative closure (RC) was calculated as
described by Oudhoff et al. [23] and given by: 20
20
SFSF
XXRC
. X0 is the mean
surface area of the scratch in a specified condition at day 0 and X2 is the mean
surface area at the second day. SF0 is the mean surface area of the scratch in
serum free medium at day 0 and SF2 is the mean surface area after two days of
exposure to serum free medium. Cells were fixed for 20 minutes in 4% para-
formaldehyde and stained with ALEXA-conjugated phalloidin (5 U/ml, Molecular
Probes) for 1 hour in a dark environment. In addition to the actin staining, the
nuclei of the cells were stained by the addition of vectashield with DAPI (Vector
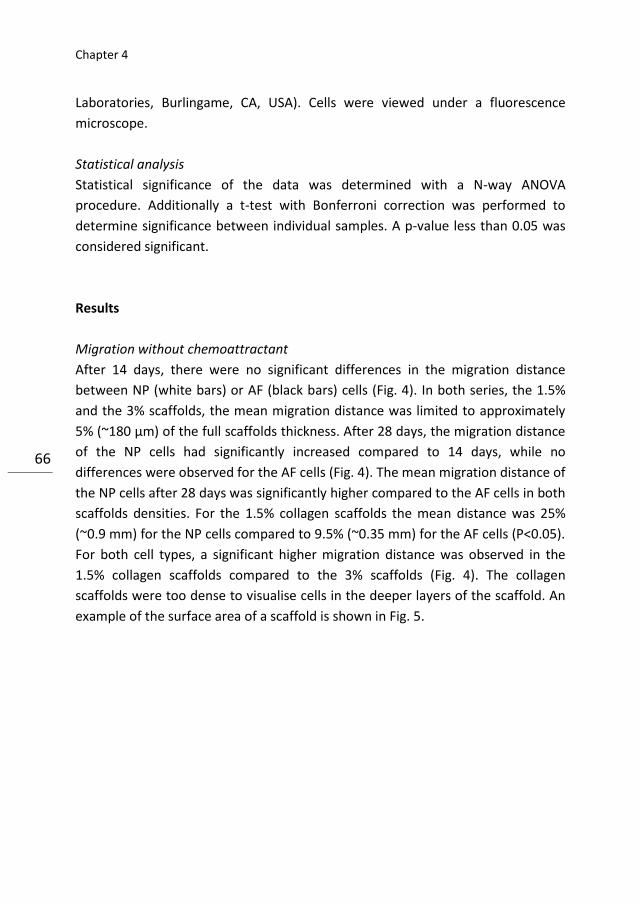
Chapter 4
66
Laboratories, Burlingame, CA, USA). Cells were viewed under a fluorescence
microscope.
Statistical analysis
Statistical significance of the data was determined with a N-way ANOVA
procedure. Additionally a t-test with Bonferroni correction was performed to
determine significance between individual samples. A p-value less than 0.05 was
considered significant.
Results
Migration without chemoattractant
After 14 days, there were no significant differences in the migration distance
between NP (white bars) or AF (black bars) cells (Fig. 4). In both series, the 1.5%
and the 3% scaffolds, the mean migration distance was limited to approximately
5% (~180 µm) of the full scaffolds thickness. After 28 days, the migration distance
of the NP cells had significantly increased compared to 14 days, while no
differences were observed for the AF cells (Fig. 4). The mean migration distance of
the NP cells after 28 days was significantly higher compared to the AF cells in both
scaffolds densities. For the 1.5% collagen scaffolds the mean distance was 25%
(~0.9 mm) for the NP cells compared to 9.5% (~0.35 mm) for the AF cells (P<0.05).
For both cell types, a significant higher migration distance was observed in the
1.5% collagen scaffolds compared to the 3% scaffolds (Fig. 4). The collagen
scaffolds were too dense to visualise cells in the deeper layers of the scaffold. An
example of the surface area of a scaffold is shown in Fig. 5.

Migration of intervertebral disc cells
67
Figure 4: Graphic showing the results of the migration experiments of NP (white bars) and AF (black
bars) cells after 14 (at the left) and 28 days (at the right) in 1.5 and 3% collagen matrices. After 14
days, no significant differences are observed. After 28 days, NP cells show a significantly higher
migration compared to the AF cells. For both cell types the migration is higher in the 1.5 compared to
the 3% collagen scaffolds
Figure 5: Surface area of 1, 5% collagen type I scaffolds after 1 week of incubation. (a AF cells, b NP
cells. Membrane Stain DiI)
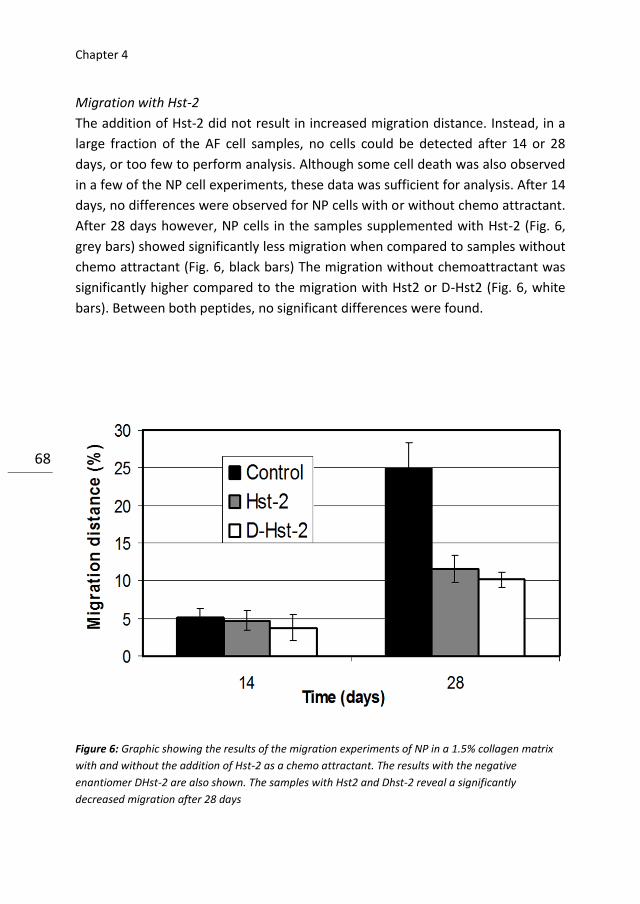
Chapter 4
68
Migration with Hst-2
The addition of Hst-2 did not result in increased migration distance. Instead, in a
large fraction of the AF cell samples, no cells could be detected after 14 or 28
days, or too few to perform analysis. Although some cell death was also observed
in a few of the NP cell experiments, these data was sufficient for analysis. After 14
days, no differences were observed for NP cells with or without chemo attractant.
After 28 days however, NP cells in the samples supplemented with Hst-2 (Fig. 6,
grey bars) showed significantly less migration when compared to samples without
chemo attractant (Fig. 6, black bars) The migration without chemoattractant was
significantly higher compared to the migration with Hst2 or D-Hst2 (Fig. 6, white
bars). Between both peptides, no significant differences were found.
Figure 6: Graphic showing the results of the migration experiments of NP in a 1.5% collagen matrix
with and without the addition of Hst-2 as a chemo attractant. The results with the negative
enantiomer DHst-2 are also shown. The samples with Hst2 and Dhst-2 reveal a significantly
decreased migration after 28 days

Migration of intervertebral disc cells
69
Expression of endo180
The expression of endo180 by both NP and AF was assessed using an antibody
directed to a hinge domain in the protein. Figure 7 shows that endo180 was
expressed on both cell types after 14 days of migration in 1.5% collagen scaffolds.
Similar results were obtained after 28 days of incubation and in 3% scaffolds.
Figure 7: Images showing the results of Endo180 staining (brown colour) (HE counterstain) of 1.5%
collagen scaffolds after 14 days of migration. a AF cells stained for Endo180 (brown colour), b AF
cells, negative control, c NP cells stained for Endo180 (brown colour), d NP cells negative control
Scratch assay
The scratches had a mean width of 666 µm (+/- 77). No statistically significant
differences between AF and NP cells were observed in any of the assays (Fig. 8).
The addition of Hst-2 to the medium had no significant effect on scratch closure
compared to the negative control (D-Hst-2) or serum free medium. The addition
of 10% serum to the medium resulted in complete closure of the scratch in both
Chapter 4
70
assays with NP and AF cells (7). Staining of the F-actin filaments, to visualize the
morphology of the cells, revealed different cell shapes for AF and NP cells (Fig. 9).
In addition, differences were found between cells inside and outside the scratch.
Non-migrated NP cells outside the scratch had a round, chondrocytic, morphology
(Fig. 9a), while NP cells that had migrated into the scratch were characterized by
long dendritic processes (Fig. 9b). Cells of the AF outside the scratch had a more
flattened, fibroblast like, appearance (Fig. 9c), whereas cells inside the scratch
were more elongated and aligned with each other (Fig. 9d). To confirm Hst-2
activity, a scratch assay was performed with human oral mucosa derived cells
(HO-1-N-1 cell line), known to be sensitive for Hst-2 stimulation [24]. This assay
showed a significant increased scratch closure after addition of Hst-2 (Fig. 10).
Figure 8: Graphic showing the results of the scratch assay. No significant differences are observed
between the samples supplemented with Hst-2 compared to the negative control (D-Hst2) or serum
free medium. The addition of 10% serum to the medium resulted in a significant increase in closure of
the scratches
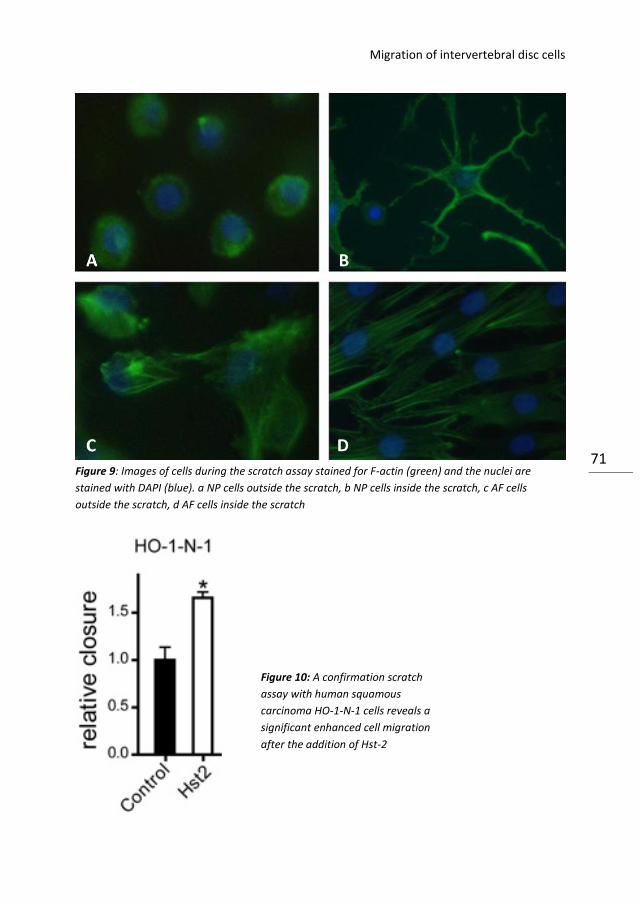
Migration of intervertebral disc cells
71 Figure 9: Images of cells during the scratch assay stained for F-actin (green) and the nuclei are
stained with DAPI (blue). a NP cells outside the scratch, b NP cells inside the scratch, c AF cells
outside the scratch, d AF cells inside the scratch
Figure 10: A confirmation scratch
assay with human squamous
carcinoma HO-1-N-1 cells reveals a
significant enhanced cell migration
after the addition of Hst-2

Chapter 4
72
Discussion
The aim of the current study was to assess the migration of native cells into
collagen scaffolds intended for functional replacement of the NP. Migration
distance proved to be both time and density dependent. After 14 days, the
observed migration was very limited for all cell types and collagen densities.
Although current conditions are not fully comparable to other studies, since
migration is usually studied from high towards low density matrices, a certain ‘lag
phase’ before migration occurs has been recognised [25]. A few explanations have
been suggested for this phenomenon [25]. Firstly, cells require some time to
overcome the differences in matrix stiffness [15, 25]. This could also explain the
relatively long lag period (14 days) in the current study compared to previously
reported periods (16 h), since in the current study cells had to migrate into a high
stiffness matrix from the outside [15, 25]. Secondly, cells need some time to
upregulate biosynthetic features such as actin–myosin activity necessary for
migration [22, 25]. This again seems to apply for the current condition, since we
used freshly harvested cells for the experiments. Prior to harvesting, these cells
are surrounded by their own pericellular matrix, interacting with neighbouring
cells and subjected to tensile forces (AF cells) or hydrostatic pressure (NP cell) [5,
13]. Migration was not enhanced by the addition of Hst-2, a peptide present in
human saliva, which was described to be an important wound closure-stimulating
factor [23]. The peptide was shown to enhance the activity of oral and non oral
fibroblasts in vitro [24]. The exact receptor, however, to which the protein binds,
remains unknown [23, 24], making it difficult hypothesize why IVD cells were
insensitive to the pro-migratory effects of Hst-2 and cell death was even
increased. A scratch assay, which is a more sensitive model to detect chemotaxis
[23], confirmed that NP and AF cells are insensitive to Hst-2. Migration of both AF
and NP cells was not enhanced by Hst2 or D-hst2 compared to the negative
control (serum free medium). All samples showed significantly less migration than
the positive control (medium with 10% serum), in which full closure of the
scratches was observed. The absence of any chemo attractive effects of Hst2 on
current IVD cell populations might be related to differences between human and
caprine cells. We used cells derived from goats, while human cells were used in
earlier studies [23, 24]. Interestingly, the scratch assay allowed visualising the
phenotypical differences between NP and AF cells, both before and during
migration (Fig. 9). These findings are of importance since specific phenotypical
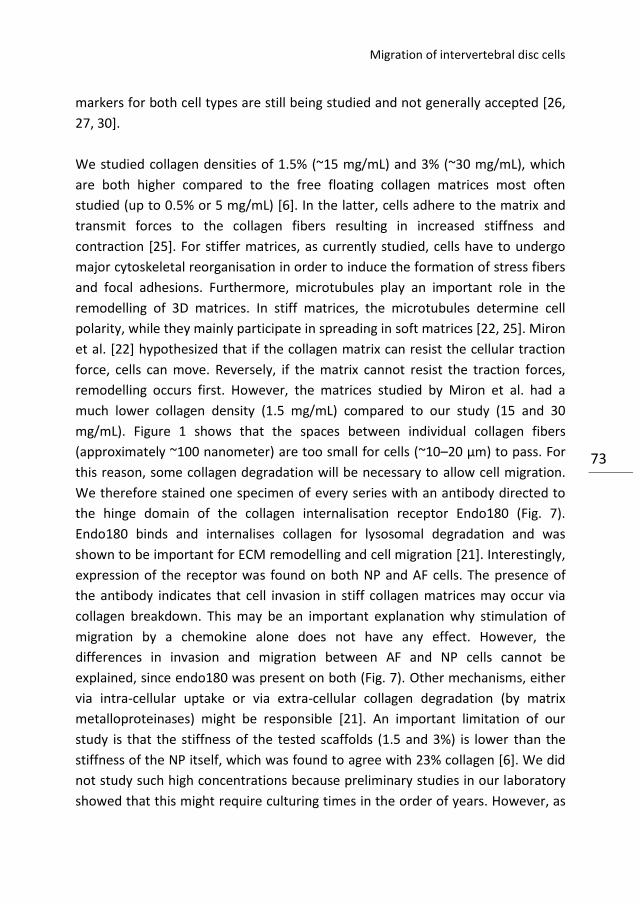
Migration of intervertebral disc cells
73
markers for both cell types are still being studied and not generally accepted [26,
27, 30].
We studied collagen densities of 1.5% (~15 mg/mL) and 3% (~30 mg/mL), which
are both higher compared to the free floating collagen matrices most often
studied (up to 0.5% or 5 mg/mL) [6]. In the latter, cells adhere to the matrix and
transmit forces to the collagen fibers resulting in increased stiffness and
contraction [25]. For stiffer matrices, as currently studied, cells have to undergo
major cytoskeletal reorganisation in order to induce the formation of stress fibers
and focal adhesions. Furthermore, microtubules play an important role in the
remodelling of 3D matrices. In stiff matrices, the microtubules determine cell
polarity, while they mainly participate in spreading in soft matrices [22, 25]. Miron
et al. [22] hypothesized that if the collagen matrix can resist the cellular traction
force, cells can move. Reversely, if the matrix cannot resist the traction forces,
remodelling occurs first. However, the matrices studied by Miron et al. had a
much lower collagen density (1.5 mg/mL) compared to our study (15 and 30
mg/mL). Figure 1 shows that the spaces between individual collagen fibers
(approximately ~100 nanometer) are too small for cells (~10–20 µm) to pass. For
this reason, some collagen degradation will be necessary to allow cell migration.
We therefore stained one specimen of every series with an antibody directed to
the hinge domain of the collagen internalisation receptor Endo180 (Fig. 7).
Endo180 binds and internalises collagen for lysosomal degradation and was
shown to be important for ECM remodelling and cell migration [21]. Interestingly,
expression of the receptor was found on both NP and AF cells. The presence of
the antibody indicates that cell invasion in stiff collagen matrices may occur via
collagen breakdown. This may be an important explanation why stimulation of
migration by a chemokine alone does not have any effect. However, the
differences in invasion and migration between AF and NP cells cannot be
explained, since endo180 was present on both (Fig. 7). Other mechanisms, either
via intra-cellular uptake or via extra-cellular collagen degradation (by matrix
metalloproteinases) might be responsible [21]. An important limitation of our
study is that the stiffness of the tested scaffolds (1.5 and 3%) is lower than the
stiffness of the NP itself, which was found to agree with 23% collagen [6]. We did
not study such high concentrations because preliminary studies in our laboratory
showed that this might require culturing times in the order of years. However, as
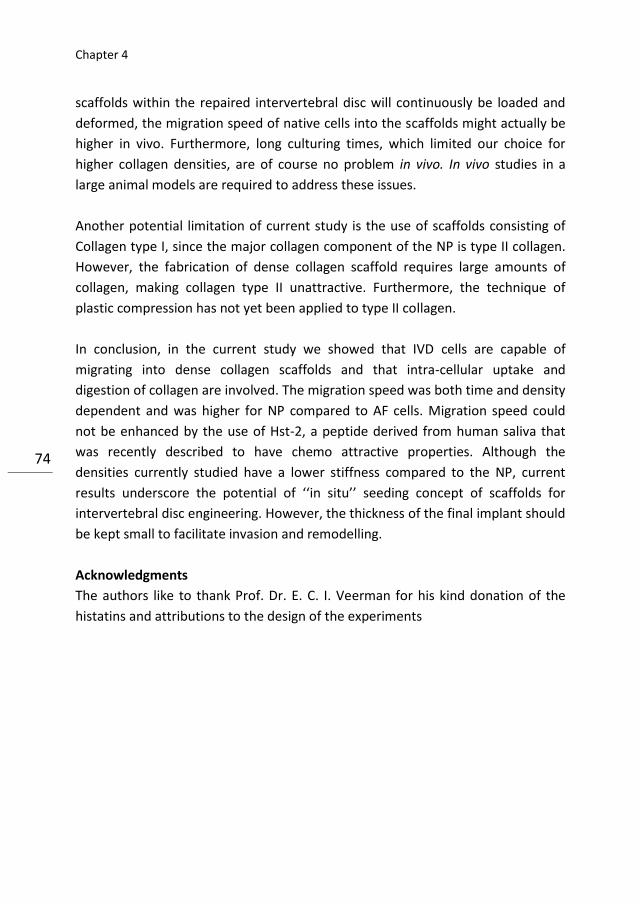
Chapter 4
74
scaffolds within the repaired intervertebral disc will continuously be loaded and
deformed, the migration speed of native cells into the scaffolds might actually be
higher in vivo. Furthermore, long culturing times, which limited our choice for
higher collagen densities, are of course no problem in vivo. In vivo studies in a
large animal models are required to address these issues.
Another potential limitation of current study is the use of scaffolds consisting of
Collagen type I, since the major collagen component of the NP is type II collagen.
However, the fabrication of dense collagen scaffold requires large amounts of
collagen, making collagen type II unattractive. Furthermore, the technique of
plastic compression has not yet been applied to type II collagen.
In conclusion, in the current study we showed that IVD cells are capable of
migrating into dense collagen scaffolds and that intra-cellular uptake and
digestion of collagen are involved. The migration speed was both time and density
dependent and was higher for NP compared to AF cells. Migration speed could
not be enhanced by the use of Hst-2, a peptide derived from human saliva that
was recently described to have chemo attractive properties. Although the
densities currently studied have a lower stiffness compared to the NP, current
results underscore the potential of ‘‘in situ’’ seeding concept of scaffolds for
intervertebral disc engineering. However, the thickness of the final implant should
be kept small to facilitate invasion and remodelling.
Acknowledgments
The authors like to thank Prof. Dr. E. C. I. Veerman for his kind donation of the
histatins and attributions to the design of the experiments
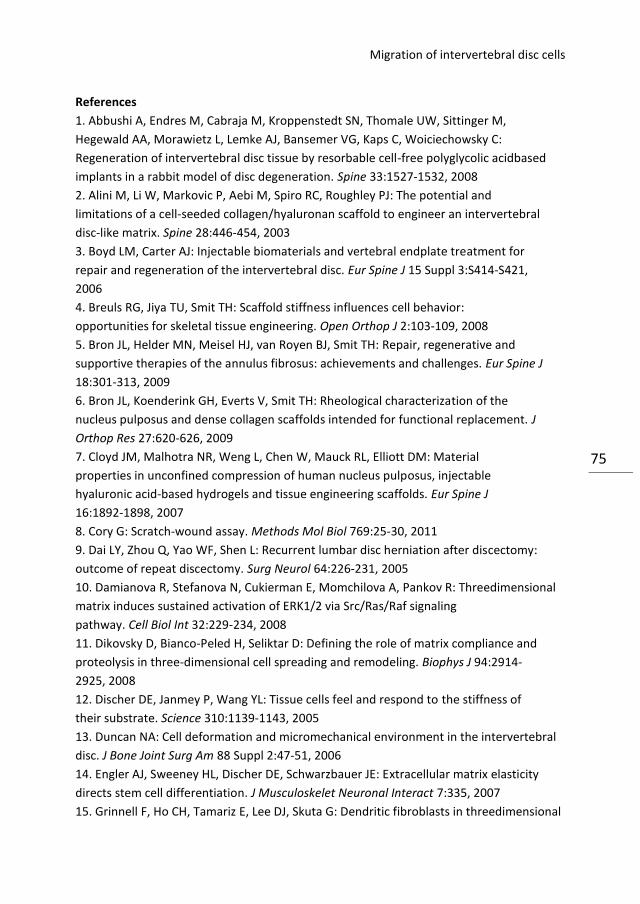
Migration of intervertebral disc cells
75
References
1. Abbushi A, Endres M, Cabraja M, Kroppenstedt SN, Thomale UW, Sittinger M,
Hegewald AA, Morawietz L, Lemke AJ, Bansemer VG, Kaps C, Woiciechowsky C:
Regeneration of intervertebral disc tissue by resorbable cell-free polyglycolic acidbased
implants in a rabbit model of disc degeneration. Spine 33:1527-1532, 2008
2. Alini M, Li W, Markovic P, Aebi M, Spiro RC, Roughley PJ: The potential and
limitations of a cell-seeded collagen/hyaluronan scaffold to engineer an intervertebral
disc-like matrix. Spine 28:446-454, 2003
3. Boyd LM, Carter AJ: Injectable biomaterials and vertebral endplate treatment for
repair and regeneration of the intervertebral disc. Eur Spine J 15 Suppl 3:S414-S421,
2006
4. Breuls RG, Jiya TU, Smit TH: Scaffold stiffness influences cell behavior:
opportunities for skeletal tissue engineering. Open Orthop J 2:103-109, 2008
5. Bron JL, Helder MN, Meisel HJ, van Royen BJ, Smit TH: Repair, regenerative and
supportive therapies of the annulus fibrosus: achievements and challenges. Eur Spine J
18:301-313, 2009
6. Bron JL, Koenderink GH, Everts V, Smit TH: Rheological characterization of the
nucleus pulposus and dense collagen scaffolds intended for functional replacement. J
Orthop Res 27:620-626, 2009
7. Cloyd JM, Malhotra NR, Weng L, Chen W, Mauck RL, Elliott DM: Material
properties in unconfined compression of human nucleus pulposus, injectable
hyaluronic acid-based hydrogels and tissue engineering scaffolds. Eur Spine J
16:1892-1898, 2007
8. Cory G: Scratch-wound assay. Methods Mol Biol 769:25-30, 2011
9. Dai LY, Zhou Q, Yao WF, Shen L: Recurrent lumbar disc herniation after discectomy:
outcome of repeat discectomy. Surg Neurol 64:226-231, 2005
10. Damianova R, Stefanova N, Cukierman E, Momchilova A, Pankov R: Threedimensional
matrix induces sustained activation of ERK1/2 via Src/Ras/Raf signaling
pathway. Cell Biol Int 32:229-234, 2008
11. Dikovsky D, Bianco-Peled H, Seliktar D: Defining the role of matrix compliance and
proteolysis in three-dimensional cell spreading and remodeling. Biophys J 94:2914-
2925, 2008
12. Discher DE, Janmey P, Wang YL: Tissue cells feel and respond to the stiffness of
their substrate. Science 310:1139-1143, 2005
13. Duncan NA: Cell deformation and micromechanical environment in the intervertebral
disc. J Bone Joint Surg Am 88 Suppl 2:47-51, 2006
14. Engler AJ, Sweeney HL, Discher DE, Schwarzbauer JE: Extracellular matrix elasticity
directs stem cell differentiation. J Musculoskelet Neuronal Interact 7:335, 2007
15. Grinnell F, Ho CH, Tamariz E, Lee DJ, Skuta G: Dendritic fibroblasts in threedimensional
Chapter 4
76
collagen matrices. Mol Biol Cell 14:384-395, 2003
16. Hakkinen A, Kiviranta I, Neva MH, Kautiainen H, Ylinen J: Reoperations after first
lumbar disc herniation surgery; a special interest on residives during a 5-year followup.
BMC Musculoskelet Disord 8:2, 2007
17. Hegewald AA, Ringe J, Sittinger M, Thome C: Regenerative treatment strategies in
spinal surgery. Front Biosci 13:1507-1525, 2008
18. Jonsson B, Stromqvist B: Repeat decompression of lumbar nerve roots. A prospective
two-year evaluation. J Bone Joint Surg Br 75:894-897, 1993
19. Leone G, Torricelli P, Chiumiento A, Facchini A, Barbucci R: Amidic alginate
hydrogel for nucleus pulposus replacement. J Biomed Mater Res A 84:391-401, 2008
20. Leung VY, Chan D, Cheung KM: Regeneration of intervertebral disc by mesenchymal
stem cells: potentials, limitations, and future direction. Eur Spine J 15 Suppl 3:S406-
S413, 2006
21. Messaritou G, East L, Roghi C, Isacke CM, Yarwood H: Membrane type-1 matrix
metalloproteinase activity is regulated by the endocytic collagen receptor Endo180. J
Cell Sci 122:4042-4048, 2009
22. Miron-Mendoza M, Seemann J, Grinnell F: Collagen fibril flow and tissue
translocation coupled to fibroblast migration in 3D collagen matrices. Mol Biol Cell
19:2051-2058, 2008
23. Oudhoff MJ, Bolscher JG, Nazmi K, Kalay H, van 't HW, Amerongen AV, Veerman
EC: Histatins are the major wound-closure stimulating factors in human saliva as
identified in a cell culture assay. FASEB J 22:3805-3812, 2008
24. Oudhoff MJ, van den Keijbus PA, Kroeze KL, Nazmi K, Gibbs S, Bolscher JG,
Veerman EC: Histatins enhance wound closure with oral and non-oral cells. J Dent
Res 88:846-850, 2009
25. Rhee S: Fibroblasts in Three Dimensional Matrices: Cell Migration and Matrix
Remodeling. Exp Mol Med 2009
26. Rutges J, Creemers LB, Dhert W, Milz S, Sakai D, Mochida J, Alini M, Grad S:
Variations in gene and protein expression in human nucleus pulposus in comparison
with annulus fibrosus and cartilage cells: potential associations with aging and
degeneration. Osteoarthritis Cartilage 18:416-423, 2010
27. Sakai D, Nakai T, Mochida J, Alini M, Grad S: Differential phenotype of
intervertebral disc cells: microarray and immunohistochemical analysis of canine
nucleus pulposus and anulus fibrosus. Spine (Phila Pa 1976 ) 34:1448-1456, 2009
28. Veerman EC, Valentijn-Benz M, Nazmi K, Ruissen AL, Walgreen-Weterings E, van
MJ, Doust AB, van't HW, Bolscher JG, Amerongen AV: Energy depletion protects
Candida albicans against antimicrobial peptides by rigidifying its cell membrane. J
Biol Chem 282:18831-18841, 2007
29. Videman T, Nurminen M: The occurrence of anular tears and their relation to lifetime
Migration of intervertebral disc cells
77
back pain history: a cadaveric study using barium sulfate discography. Spine 29:2668-
2676, 2004
30. Vonk LA, Kroeze RJ, Doulabi BZ, Hoogendoorn RJ, Huang C, Helder MN, Everts V,
Bank RA: Caprine articular, meniscus and intervertebral disc cartilage: an integral
analysis of collagen network and chondrocytes. Matrix Biol 29:209-218, 2010
31. Wienke D, MacFadyen JR, Isacke CM: Identification and characterization of the
endocytic transmembrane glycoprotein Endo180 as a novel collagen receptor. Mol
Biol Cell 14:3592-3604, 2003
32. Wilke HJ, Heuer F, Neidlinger-Wilke C, Claes L: Is a collagen scaffold for a tissue
engineered nucleus replacement capable of restoring disc height and stability in an
animal model? Eur Spine J 15 Suppl 3:S433-S438, 2006
Chapter 4
78
5 Repair, regenerative and supportive
therapies of the annulus fibrosus:
achievements and challenges.
JL Bron
MN Helder
HJ Meisel
BJ van Royen
TH Smit
Chapter 5
80
Abstract
Lumbar discectomy is a very effective therapy for neurological decompression in
patients suffering from sciatica due to a hernia nuclei pulposus. However, high
recurrence rates and persisting post-operative low back pain in these patients
require serious attention. In the past decade, tissue engineering strategies have
been developed mainly targeted to the regeneration of the nucleus pulposus (NP)
of the intervertebral disc. Accompanying techniques that deal with the damaged
annulus fibrous are now increasingly recognised as mandatory in order to prevent
re-herniation to increase the potential of NP repair and to confine NP
replacement therapies. In this chapter, the requirements, achievements and
challenges in this quickly emerging field of research are discussed.
Annulus fibrosus repair
81
Introduction
Lumbar discectomy is an effective therapy for neurological decompression in
patients suffering from an herniated nucleus pulposus (HNP), which can be safely
performed via minimal invasive procedures [44, 128]. Current discectomy
procedures, however, are not directed to treat the damaged intervertebral disc
(IVD) and may even further aggravate existing damage [16, 22, 45]. It is therefore
not surprising that successful neurological decompression is often followed by
periods of persisting low back pain, severely affecting the quality of life [7, 8, 45].
Another serious problem in these patients is the high recurrence rates after
discectomy, affecting up to 15% of the patients [7, 8, 16, 23, 42, 59, 63, 66, 98,
113, 115]. Since discectomy is still the most performed spinal surgical procedure
worldwide and mainly affects the employed population, the resulting socio-
economical consequences are dramatic [61].
This gives investigators the impetus to search for new strategies that also deal
with the damaged IVD in patients treated for HNP [68, 74, 105]. During the last 5
years, increasing knowledge and technical advancements in the field of tissue
engineering has resulted in numerous promising strategies to repair, replace or
regenerate the herniated nucleus pulposus (NP) [45, 105]. None of these
advancements, however, has yet resulted in a clinically proven effective therapy.
One of the major limitations is the lack of effective strategies that deal with the
damaged annulus fibrosus (AF) [125]. Since optimal regeneration of the NP should
lead to restoration of the physiological intradiscal pressure, the surrounding AF is
generally of too inferior quality to withstand these forces. Without sufficient
attention to the damaged AF, these treatments might be condemned to fail [5,
125]. Therefore, intervertebral disc engineering strategies are increasingly
focusing on the regeneration or repair of the AF in order to reduce the number of
re-herniations, increase the potential of NP engineering strategies and to
mechanically assist NP replacement therapies [6, 125]. In this chapter, we will
discuss the requirements, achievements and challenges in this rapidly emerging
field of research.
Chapter 5
82
Anatomy
Structure of the annulus fibrosus
The IVD is confined by the two cartilage endplates and is composed of two distinct
structures, the nucleus pulposus (NP), and the surrounding annulus fibrosus (AF)
[53, 130]. The two cartilage endplates offer anatomical limitation to the vertebral
bodies and morphology along the plate is distinguished by a central articular-like
cartilage under the NP and a peripheral fibrocartilage appropriately associated
with the AF. During embryogenesis, the AF develops from the mesenchyme,
whereas the NP is derived from the notochord [120]. The AF consists of water
(65– 90%), collagen (50–70% dry weight), proteoglycans (10– 20% dry weight) and
noncollagenous proteins (e.g. elastin) [14, 114]. The AF has a laminate structure
consisting of a minimum of 15 (posterior) to a maximum of 25 (lateral) concentric
layers [71]. The layers are composed of type 1 collagen fibres that alternate in
angles from 28º (peripheral AF) to 44º (central AF) with respect to the transverse
plane of the disc [17, 71, 84]. The spaces between the separate layers of the AF
are called interlamellar septae, and they contain proteoglycan aggregates and a
complex structure of linking elements creating interlamellar cohesion [14,
89,111]. At the periphery, some of the annulus fibres pass the endplates to
penetrate into the bone of the vertebral body as ‘‘Sharpey’s fibres’’ [57]. Central
fibres either insert into the cartilage of both endplates or bend with the NP (Fig.
1). The highly organised structure of the AF results in a complex anisotropic
behaviour, with the tensile, compressive, and shear properties differing in the
axial, circumferential, and radial directions [11, 106, 114].
Based on structural and cellular differences, the AF can be further distincted into
an inner and an outer part (Fig. 2) [14, 15, 71, 114]. The inner AF is a broad
transition zone between the highly organised collagenous structure of the outer
AF and the highly hydrated NP and consists of a mixture of extra cellular matrix
(ECM) components of both [20, 130]. The inner AF is less hydrated than the NP
and the layers are more widely spaced compared to the outer AF [52].
Mechanically, the inner AF is more subjected to the high hydrostatic pressures of
the NP than to the tensile forces in the outer AF [73, 112]. These differences have
major consequences on ECM synthesis and turnover [52]. The proportion type 1
collagen increases from the inner part towards the outer annulus, whereas type II
Annulus fibrosus repair
83
collagen follows a counterwise distribution [14, 20, 122, 130]. Other proteins that
have a specific distribution include decorin and biglycan (mainly outer AF) and
collagen type X [inner AF and (aged) NP] [55]. Elastin constitutes 2% of the dry
weight of the AF, but plays an important role in the recoil properties of the AF [97,
129]. In the outer AF, long elastic fibres are present within the lamellae, running
parallel to each other and into the same direction as the collagen bundles. In the
inner AF, the fibres are present between adjacent lamellae as well as more
regularly organised within the lamellae [129]. These fibre networks couple
adjacent lamellae together allowing them to work cooperatively during dynamic
loading and prevent separation of lamellae during torsional compressive loading
[76].
Annulus fibrosus cells
In mature subjects the cell density in the AF is about 9 x106 cells/cm3, which is
over two times higher as compared to the NP [98]. Although all cells in the AF are
derived from the mesenchyme, cells within the layers of the AF, the interlamellar
spaces and the inner AF have their own morphology and synthesize a distinct ECM
[14, 28, 52, 71, 90, 98, 130]. The cells experience not only differences in
mechanical environment as described above, but also a rise in pO2 and pH and a
decrease in hydration from the central NP to the outer layers of the AF [50, 52, 94,
98, 118]. In the layers of the outer annulus, fusiform shaped cells, aligning with
the collagen fibres and alternating with each lamella are found [71, 90, 106]. In
the periphery of the outer annulus, these cells are interconnected by very long
processes which results in a continuous communicating network [14, 77]. The
processes are gradually reduced in length and increased in thickness towards the
inner AF. In the most central part of the outer AF, the cells are completely isolated
without any apparent physical, intercellular connections [14]. These outer annulus
cells mainly produce type I collagen [130]. The cells in the interlamellar septae
have a more flattened, disc-shaped morphology that show many similarities to
the cells of the NP [14]. The predominant cell morphology in the inner annulus
consists of spherical shaped cells with one or two short processes, having the
highest frequency at the border with the NP [14]. These chondrocyte-like cells in
the inner annulus mainly produce type II collagen. A recent study showed that
cells derived from the human AF were able to differentiate into the chondrogenic
and adipogenic lineages [95]. This suggests that cells in the AF could be skeletal
Chapter 5
84
progenitor cells that could be recruited under pathologic conditions such as
herniation. Otherwise, progenitor cells from surrounding tissue might perhaps be
capable to migrate into the intervertebral disc in the circumstances.
Pathophysiology tissue retrieved from a herniated disc is more often vascularised
and is more highly innervated than healthy tissue [97]. Not surprisingly, this
variant morphology also demonstrates a proclivity to MMP and cytokine
expression, each of which would be expected to contribute to further re-
modelling [97]. Besides these clearly pathologic conditions, other structural
changes do occur during ageing that are to a certain extent physiological but
might have consequences for its strength (Fig. 1). In the ageing AF of rats, the
number of distinct layers was found to decrease gradually and this loss of volume
is compensated by increasing thickness of individual layers and thickening of the
inner annulus [90]. In addition, the fibre bundles within the layers become more
irregularly distributed with increased interbundle spaces [90]. The loss of distinct
layers carries with it the inability for a sustained response to loading and support
[1, 41].
Figure 1 (Page 85): Histological image (toluidine blue) of the canine intervertebral disc revealing the
relation between the nucleus pulposus (NP), annulus fibrosus (AF) and endplates (EP). Some of the
most central AF fibres bend with the NP (arrow)
Figure 2 (Page 85): Sagittal section specimen of the L3–L4 intervertebral disc of a middle aged
asymptomatic male subject. NP nucleus pulposus, IA inner annulus fibrosus, OA outer annulus
fibrosus. Defects in the outer annulus (asterisk) and tears (hat symbol) are visible in the outer
annulus, without a sign of herniation. The NP has a severely dehydrated appearance due to
conservation techniques>>
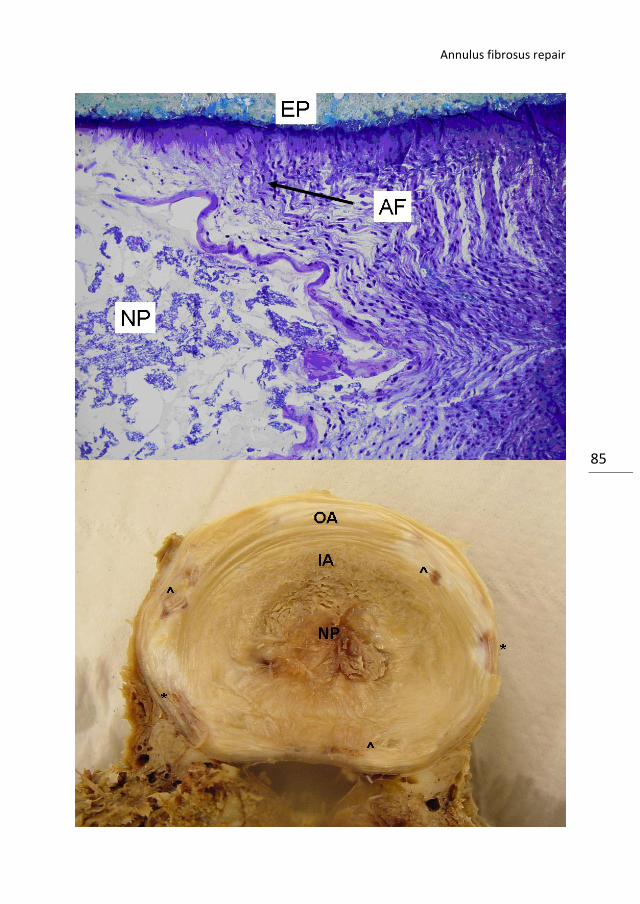
Annulus fibrosus repair
85
Chapter 5
86
Due to dehydration of the inner annulus, the compressive load is insufficiently
converted in the integral of progressive recruitment of tensile support. The lack of
annular tone in the degenerated disc results in a lag of mechanical conversion and
the annulus comes under the force of axial compression, further reducing the
anisotropic capacity for deformation in the normal, healthy disc [2, 49]. These
changes have most significant impact on the posterolateral location of the AF,
that has the highest frequency of layer interruption [71, 110]. This is also the
region where the highest stresses are observed during loading [26] and where
annular tears, fissures, protrusions, extrusion and/or sequestrations may develop
[86]. Annular tears are seen in more than half of the patients in early adulthood
and are invariably present in the elderly (Fig. 1) [119]. The degree of degeneration
varies between subjects, for which genetic and environmental (e.g. physical
loading, smoking) factors are held responsible [10, 13, 81, 88]. Patients with a
genetic predisposition are more prone to disc degeneration under repeated
mechanical loading [10].
The relation between loading and degeneration of the AF has been studied by
several authors, but our knowledge is still only fragmented. Elverfig et al. [27]
showed that shear stress increased the intracellular calcium concentration in AF
cells. The sensitivity for shear stress was increased in the presence of the
inflammatory cytokine II–1 [27]. Rannou et al. [92] showed that static
compression resulted in a significant increase of apoptotic cells in the inner AF in a
mouse model. The authors also found an increased caspase-9 activity and
decreased mitochondrial membrane potential following overload, suggesting that
degeneration might be mediated through the mitochondrial apoptotic pathway
[91]. Furthermore, vibratory loading has been associated with the activation of
signalling pathways that regulate ECM destruction in the IVD [127]. Yamazaki
showed that gene expression in AF cells for key ECM components such as
aggrecan and type II collagen was suppressed following vibratory loading [126].
Lastly, cyclic tensile stretch was found to regulate the ECM by decreasing
proteoglycan production through a post-translational regulation involving nitrite
oxide [92]. Gruber et al. hypothesized that the well-recognised reduction in cell
number in the AF during ageing is an important factor for degeneration. This
should result in a loss of cell–cell communication and hence a disruption of
coordinated cell function [40]. Finally, many adult IVD’s show signs of dehydration

Annulus fibrosus repair
87
and ‘‘brown degeneration’’, which is the result of post-translational collagen
modification resulting in the formation of chromophores [83, 104]. In these discs,
accumulated or enhanced oxidative stress of matrix proteins has resulted in
glycoxidation of proteins [83]. Advanced glycosylation end products are further
processed to carboxymethyl-lysine by free oxygen radicals, which can be detected
by antibodies and used as a biomarker for oxidative stress [82].
Intrinsic healing potential
The intrinsic capacity of the AF to cope with damage or degenerative changes has
been studied in several animal studies [3, 29, 34, 43, 62, 75, 79, 85, 99, 109]. Key
and Ford [62] studied the healing capacity of three different types of posterior AF
lesions in a dog model. The lesions included a square annular window, a
transverse incision and puncture with a 20-gauge needle. At follow up, they found
that the lesions were initially filled with extravasated blood, fibrin, bone and
cartilage debris that was gradually replaced by a thin layer of fibrous tissue at
later time points (up to 22 weeks). Some of the levels within the window and
incision lesion group developed slowly progressive disc protrusion, which was
most common in the transversely incised discs. The levels that underwent needle
puncture revealed nothing abnormal and the site of puncture could not be
identified after 22 weeks. A recent study, however, with rabbit discs in an organ
culture model showed that needle puncture has immediate and progressive
mechanical and biologic consequences that may lead to degenerative remodelling
[65]. The findings of Key and Ford have been underscored and complemented in
many studies afterwards [29, 43, 85, 97].
Smith et al. [109] further specified the healing process in three different phases.
During the first phase, the outer AF heals, caused by a proliferative reaction in the
fibrous tissue spreading from the lateral parts of the wound to the median parts.
In the second phase, starting after a few weeks and lasting up to one year post-
operative, changes occur in inner annular fibres. Similarly to the outer AF, the
lateral parts of the inner AF layers gradually heal by a slow appositional spread in
the median direction. During the last phase, there is an increase in the number of
collagenous fibres in the NP tissue that has remained in the AF wound tract, which
becomes increasingly dense [109]. Similar findings were more recently obtained in
sheep and dog studies [43, 85].
Chapter 5
88
From the studies performed thus far it can be concluded that he AF has only a
very limited regenerative capacity after annulotomy. Depending on the technique
that is used, healing results in a thin layer of biomechanical inferior fibrous tissue
[31]. One of the reasons for the limited healing capacity may be the fact that
exterior repairs are not matched, or insulated to the demands of progressive
recruitment of fibres to tensile force [41, 54]. The mechanical basis for shifting
axial loading to circumferential tension requires that the nucleus volume remain
elastic, deformable and contained. When the lateral aspects of the annulus are
violated or scarred, the ability of the fibres to adequately contain the nucleus
changes. In the case of static patient posture and prolonged loading, the disc will
experience creep that is proportional to the stage of disc degeneration. In
practice, disc degeneration results in a stiffer matrix that does not accommodate
the modelling of a disc with normal morphology. If it is not possible to reduce the
axial load, then the inevitability of sustaining increasing force in a stiffened matrix
will lead to accelerated herniation and more rapid propagation of anular fissures
[80].
Surgical strategies
The limited intrinsic healing capacity of the AF negatively affects the success rates
of discectomies and NP replacement therapies. It also decreases the potential of
intervertebral disc regenerative strategies. To dissolve this problem, attempts to
preserve, repair, reinforce or regenerate the AF in addition to these surgical
techniques are desired.
Annulus closure techniques
The most straightforward solution is per operative suturing of the annular defect
and this has been studied by Ahlgren et al. [3] in a sheep model. Although they
found that sutured discs showed a tendency towards stronger healing, this was
not significant [3]. Unfortunately, no further studies on this subject have been
reported. The Xclose and INclose implants are now commercially available for
annuloplasty and can be seen as modified sutures with anchors [12, 18]. Sutures,
however, are fully directed to containment of the NP (replacement) and do not
compensate the loss of annulus material nor reverse the biomechanical changes
that have occurred in the damaged AF. The Barricaid is a commercially available

Annulus fibrosus repair
89
implant used in adjunction to discectomies that fully bridges the defect in the AF
[36]. This implant even reinforces the complete posterior annulus and would
therefore even prevent contralateral herniation. Several other novel suture, seal
and barrier techniques are currently being developed, resulting in increasing
attention at scientific workshops and conferences [9, 12, 16, 18, 36, 60, 108, 117].
More detailed analyses are therefore expected in peer reviewed journals in the
near future. The momentum of acceptance, however, needs to be balanced in the
proof of principle. Risks imposed by criticism need to be weighed in both short-
and long-term successes. Clinical durability is the eventual arbiter of technology
value, and open trials with clear data will be required.
Regenerative strategies
Regeneration of the damaged AF is an attractive concept, since it allows
restoration of all functions of the AF, but is exceptionally complex to achieve.
Regenerative strategies can be divided into cell therapy, gene therapy and tissue
engineering with scaffolds [45]. In case of the AF, however, direct mechanical
strength and a certain volume to patch the defect seem required in order to
contain the NP [125]. Ideally, it should combine direct closure of the defect, as
discussed in the preceding section, with the potential for regeneration. Cell and
gene therapies are therefore not suitable as standalone therapies, but should be
combined with scaffolds. Below, these strategies are first discussed separately,
followed by an overview of the studies performed with the necessary scaffolds.
Annulus cells
Annulus fibrosus cells that are used for AF tissue engineering are derived from
humans or various other species (Table 1). The use of human disc cells as a cell
source for tissue engineering is difficult because normal healthy disc tissue is not
available for such a treatment strategy. In previous studies with tissue derived
from herniated discs, an increased degree of cell senescence was found that
accumulates over time [38, 96], thus hampering the applicability of this cell source
for regenerative strategies [38]. Furthermore, isolation of the cells retrieved from
human discectomy material does usually not allow division between inner and
outer AF cells. Therefore, cells used for studying annulus regeneration are often
harvested from IVD’s from healthy small animals. To increase cell number, the AF
cells are cultured in vitro first. These cells are isolated from native tissue and it is
Chapter 5
90
therefore important to realise that the environment differs greatly from that in
situ. Cells no longer have processes, a pericellular matrix and are isolated from
each other, and are cultured in gels that do not always allow cellular sliding [25].
Annulus cells have shown to lose their phenotype during two-dimensional (2D)
culturing. Chou et al. [20] showed that up to passage two, both inner and outer
annulus cells are not different from freshly isolated cells. At later passages,
however, both cell types became indistinguishable fibroblast-like with similar type
I collagen expression and protein elaboration. The negative effects of monolayer
culturing are currently further investigated with specialised 2D environments like
collagen coatings, well inserts, or micro-grooved polycaprolactone membranes
[21, 37, 58].
To prevent the loss of their phenotype, AF cells are usually cultured in three-
dimensional (3D) environments, such as alginate, agarose or collagen hydrogels
[4, 37, 39, 64, 100, 130]. Chou et al. [21] found NP and inner and outer AF cells to
adopt similar phenotypes after two weeks of culturing in alginate. NP cells and AF
cells displayed a rounded chondrocyte-like morphology, expressing high levels of
type II collagen versus type I collagen and accumulation of sulphated GAG’s.
Indeed, the adopted phenotypes are typically NP-like and it was not investigated
by these authors whether the changes are reversible [21]. Gruber et al. assessed
the ECM expression of AF cells in different 3D culture environments including
collagen sponge, collagen gel, agarose, alginate and fibrin [39]. Collagen sponges
supported the most abundant ECM formation, whereas the ECM production was
nearly absent in fibrin gel. The ECM production, however, included types I and II
collagen, aggrecan and chondroitin-6-sulfotransferase for all carriers and this is
not specific for AF cells. Moreover, although alginate might be appropriate for
inner AF cells, outer AF cells do not survive well in alginate and show a different
morphology and matrix expression than observed in vivo [52]. It can be concluded
that the appropriate culture environment for AF cells has yet to be elucidated.
AF cells are very sensitive to pressure effects during culturing and this might be
useful for tissue engineering strategies. Reza et al. [93] cultured inner and outer
AF cells in PGA scaffolds to evaluate the effect of dynamic hydrostatic pressures
(HP). Type II collagen production was enhanced in both cell types by the
application of HP. This effect, but also the effects on ECM elaboration and
Annulus fibrosus repair
91
organization, was more pronounced in the scaffold seeded with outer AF cells
[93]. The value of these results for AF engineering however, may be questioned,
since AF cells in vivo are more subject to tensile and shearing forces and mainly
produce type I collagen. An attractive alternative, that would prevent the
problems regarding senescence, limited supply and culturing of autologous AF
cells, would be the use of mesenchymal stem cells [30, 51]. There are currently,
however, no studies available demonstrating stem cells to differentiate into AF
cells. The lack of conclusive phenotypic markers for both, AF cells and stem cells,
makes it difficult to study this differentiation [30].
Gene and bio-active factors
Extra cellular matrix production of AF cells can be influenced by various gene and
bio-active factors [72, 93, 116, 126]. A few studies have addressed the effect of
osteogenic protein-1 (OP-1) on AF cells cultured in alginate beads [72, 116].
Masuda et al. showed that continuous stimulation of rabbit AF cells cultured in
alginate beads with recombinant OP-1 led to an increase in the total DNA,
collagen content and a pronounced effect on proteoglycan synthesis. However,
the authors also showed that this stimulation is more effective in NP cells,
compared to AF cells [72]. Takegami et al. [116] showed that AF cells that were
stimulated with OP-1 were able to repair the ECM that was depleted of sulphated
glycosaminoglycans by chondroitinase ABC exposure. Since these studies show
that OP-1 has greater effects on PG synthesis and on NP cells, it may be
questioned if OP-1 really offers advantages for AF engineering. Zhang et al.
studied the effects of several bone morphogenetic proteins (BMP’s) and Sox-9
transfection on AF cells. They found that collagen synthesis could be enhanced by
over-expression of BMP-13 and of the transcription factor Sox9 [131]. Although
these in vitro results are promising, the effects of these growth factors upon
application in animals or humans in vivo remain unknown.
Scaffolds
The ultimate goal of AF engineering is to achieve both direct mechanical stability
and to allow the formation of native tissue in the long term. In order to develop
suitable scaffolds for tissue engineering, general principles should be taken into
account including the immunogenicity, biocompatibility and biodegradability and
Chapter 5
92
method of graft delivery [67]. Specific requirements may be recognised for AF
scaffolds. They should:
– Fill and/or repair the AF gap to contain the NP (replacement)
– Allow fixation to the surrounding structures, i.e. endplates and/or surrounding
AF tissue
– Allow AF cells (or stem cells) to survive (differentiate), synthesize and secrete
the native ECM
– Have the characteristic anisotropic behaviour, to maintain/restore the
mechanical properties of a spinal motion segment
– Not irritate or adhere to the perineurium
Several scaffolds that could be used for AF tissue engineering have been proposed
and evaluated in in vitro or in small in vivo studies. In Table 1 these studies are
summarised, as well as to which extent they meet the aforementioned
requirements. Without exception, strategies for delivery and fixation in vivo are
lacking. Accurate mechanical characterizations are sparse. Only one study
reported of a scaffold material showing anisotropic behaviour, comparable to the
AF [84]. Anisotropy however, deserves further study, since a lack of tension was
found to influence collagenase and cytokine activity [24, 35]. The biphasic
appearance of the native AF has also been targeted by a single study. In this study,
the inner and outer AF were simulated by bone matrix gelatine (BMG) and poly-
caprolactone triol malate, respectively [122].
In general, these studies have been designed to investigate cell attachment,
morphology, proliferation and ECM production on the scaffolds. Native outer AF
cells have a typical elongated shape and this is observed in most scaffolds [47, 84,
107, 121]. Shao and Hunter, however, found spherical shaped cells in their
scaffolds that agree with an inner AF cell morphology. Interestingly, most studies
report of the production of type II collagen and aggrecan [19, 78, 84, 102, 107,
121, 122], instead of collagen type I [47, 48, 107, 124], while the latter is by far the
most common ECM component of the AF. Ideally the cells are seeded in a
homogenous fashion through the scaffolds. The disadvantage of the silk and BMG
scaffold is that the cells only can be seeded on top and invasion occurs only slowly
[19, 122]. Chang et al. tried to improve cell attachment onto the silk scaffold by
Annulus fibrosus repair
93
chemically coating the scaffold with the integrin binding motif RGD. RGD,
however, did not result in enhanced cell attachment, but did result in higher levels
of type II collagen and aggrecan [19]. Higher levels of type II collagen is an
insufficient bridge to repair. Given the fact that type II collagen does not bundle or
form fibrillated structures, expression obtained by using RGD peptides may be
questioned. Using decorin, or small proteoglycans, which have known function in
appropriately binding TGFb might be a separate consideration [70].
A critical structural entity of the annulus structure is the network of type I
collagen forming fibrils oriented in sheets around the nucleus. A number of
molecules present in the matrix regulate and direct the collagen fibril assembly by
interacting with the collagen molecule and also the formed fibril. Several of these
molecules bind by one domain to the collagen fibre and present another
functional domain to interact either with other fibres or with other collagen
matrix constituents such as type VI collagen. In this manner the collagen fibres are
cross-linked into a network that provides tensile strength and distributes load
over large parts of the AF. Assembly occurs both by end-to-end and side-to-side
associations. This process is catalyzed by both biglycan and decorin, where the
combined effect of direct binding of the core protein to the collagen-6 N-terminal
globular domain and the presence of the glycosaminoglycan side chain is
essential. Diminished function in these cross-bridging molecules will lead to loss of
mechanical properties of the collagen network and result in an impaired ability of
the AF to resist forces delivered by compression of the disc and particularly the
nucleus. Decorin has been shown in other systems to retard the TGFbeta affected
fibrotic pathway and as such might limit fibrous scarring and impose tissue
specific remodeling [32, 56].
Translation from in vitro results to the in vivo situation is difficult and the few
studies that have assessed the scaffolds in vivo do provide important additional
information. Mizuno et al. [78] implanted complete tissue engineered IVD
constructs consisting of calcium alginate discs surrounded by a polyglycolic acid
(PGA) ring seeded with AF cells in the dorsum of athymic mice. The tissue that was
formed after 12 weeks follow-up tissue did not resemble native AF tissue with
alignment of cells and tissue. Cell proliferation and viability was not quantified in
this study. Sato et al. performed laser vaporization in rabbits and the lacunas in

Chapter 5
94
the NP and hole in the annulus were filled with an AF cell seeded atelocollagen
honeycomb shaped scaffold with a membrane seal (ACHMS-scaffold) [101–103].
They found a marked accumulation of cartilage like matrix inside and around the
scaffold, which was histologically comparable to native AF tissue [102]. Although
this combined NP/AF concept seems promising, it might be questionable if this
technique is also feasible to be used to fill larger annulus defects. Novel strategies
for delivery and fixation may be required.
Alternative therapies
Wang et al. simulated a herniation in a swine model and delivered gelfoam,
platinum coil, bone cement and tissue glue into the discs. Analysis was performed
after two months by quantitative discomanometry. The gelfoam proved best in
maintaining disc integrity with resistance to significantly higher intradiscal
pressures compared to the other groups. The gelfoam group was the only group
that was not significantly weaker compared to the intact disc group. The authors
conclude that gelfoam may be a potentially clinically applicable method to
prevent re-herniation [123]. However, although the foam is safe to use according
to the authors, it may be questioned how effective this method is in preventing
re-herniation in larger annulus defect than the 18 gauge lateral needle hole in the
presented animal model.
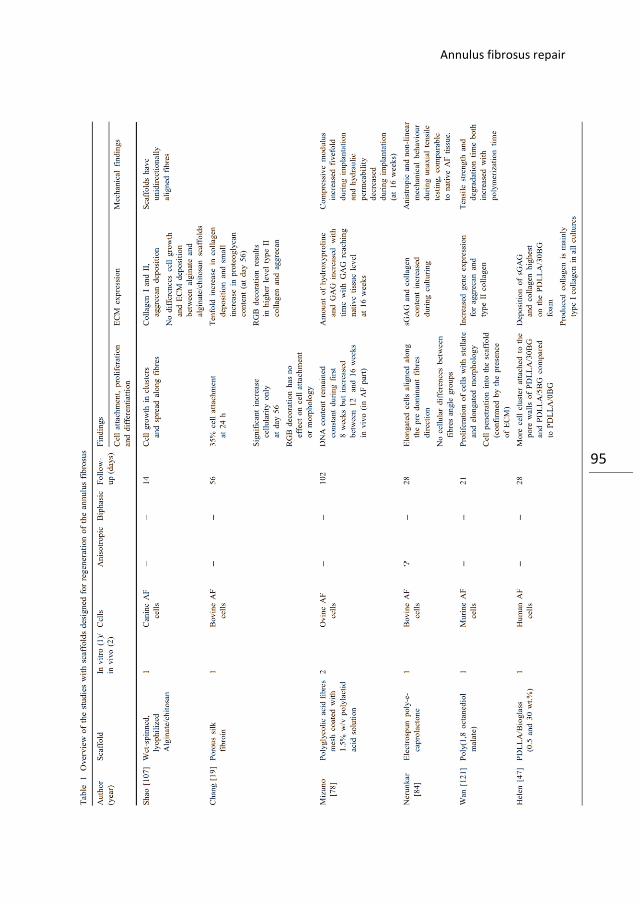
Annulus fibrosus repair
95
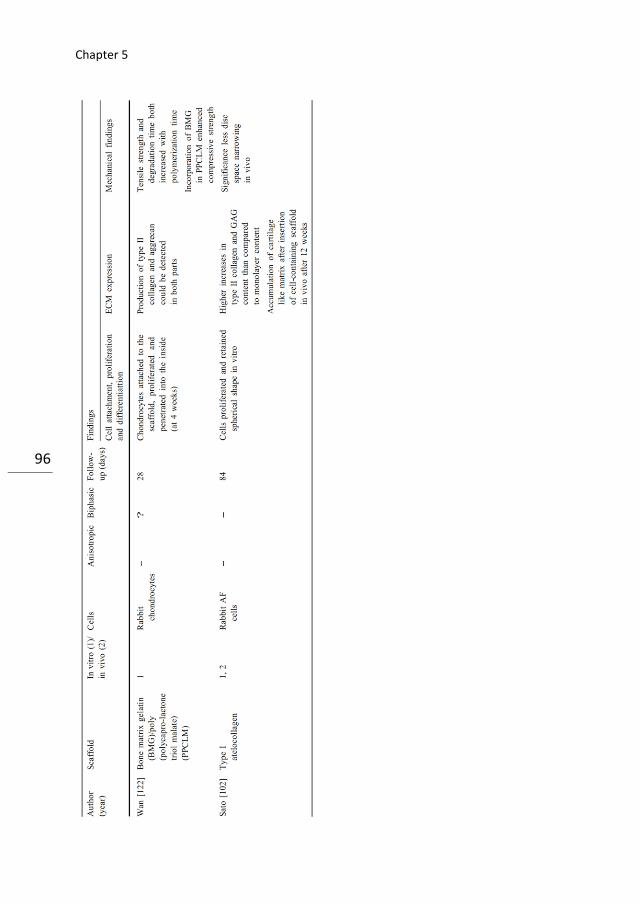
Chapter 5
96
Annulus fibrosus repair
97
Discussion
Research on the AF as a target for novel therapies has only just started to evolve.
There are several limitations and pitfalls in the research thus far that should be
noted. Experimental AF lesions are generally made at the (antero) lateral region of
healthy AF’s (Fig. 2) and extrapolation of these studies to humans is difficult [87].
Repair mechanisms in animal studies may differ compared to patients with HNP
due to the pathophysiological changes within the IVD that have occurred in the
period prior to HNP (Fig. 1) [16]. Furthermore, it is important to realise that
annulus fissures commonly develop bilaterally [2]. When successful patching of an
AF defect allows restoration of the physiological high intradiscal pressures, the
contralateral fissure may progress and become symptomatic. Complete annulus
and nucleus tissue engineered constructs as for example of Mizuno et al. [78]
would offer a solution for this, but are even more difficult in terms of
implantation. There are striking discrepancies between AF closure techniques and
regenerative strategies. Closure techniques are primarily focussing on restoration
of the mechanical integrity of the AF and do offer clear solutions for delivery and
fixation. These developments are mainly practised in vivo and scientific data is
only sparse. Regenerative therapies, on the other hand, target the engineering of
healthy and functional AF tissue, but lack strategies for implantation and fixation
and thus for clinical application. Of course, a combination of strategies that offer
direct mechanical stability and potential for remodelling AF tissue would be
preferred.
Future research
Now that the need for AF repair is increasingly recognised, many studies on this
subject are expected to be reported in the scientific literature in the upcoming
years. Both AF and NP engineering research are still in very early stages and
combined repair strategies should be attempted. Patients undergoing discectomy
should ideally benefit from a complete concept in which in one surgical procedure
the neurological structures are decompressed and the damaged NP and AF are
treated. The increasing knowledge on degradable (bio) polymers offers very
encouraging future perspectives [69]. Regenerative matrix scaffolds, biopath
materials, memory polymers, disc foams and synthetic gels to translate axial
loads, and bioactive hybrid polymers with differential sacrifice to generate cyclic

Chapter 5
98
loading during integration efforts might open new paths to successful treatment
of patients suffering from disc herniation. These therapies might be further
potentiated when combined with cell supplementation, bioactive factors and
cytokine modulation. The important role of mechanical loading in addition to IVD
engineering is yet underexposed. The use of an interspinous implant for example,
to favourably alter the motion, in addition to novel IVD engineering therapies in
patients undergoing lumbar discectomy deserves attention [33]. AF cells are a
phenotypically heterogeneous cell population. In many studies these differences
are disregarded and a mixture of AF cells is used. If we could reveal the exact
circumstances under which these cells elaborate, we might substitute these
different cell types by stem cells and stimulate them to differentiate into all native
cell types [46]. This should further prevent the inconveniences in the harvesting
and culturing procedures needed for AF cells.
Conclusion
Intervertebral disc regeneration offers promising perspectives for patients
suffering from low back pain due to disc herniation treated with lumbar
discectomy. Thus far, efforts for novel therapies have mainly been directed
towards replacement or regeneration of the NP. The real challenge, however, is
the development of strategies that deal with the damaged AF, preferably in a
combined approach with the NP. Regenerative therapies of the AF should always
be accompanied by a clear vision for future clinical application.
Acknowledgments
The authors are grateful to Timothy Ganey (Atlanta Medical Center, GA, USA) for
his contributions to the manuscript.
Annulus fibrosus repair
99
References
1. Acaroglu ER, Iatridis JC, Setton LA et al (1995) Degeneration and aging affect the tensile
behavior of human lumbar annulus fibrosus. Spine 20: 2690–2701.
2. Adams MA, Hutton WC (1985) Gradual disc prolapse. Spine 10 :524–531.
3. Ahlgren BD, Lui W, Herkowitz HN, Panjabi MM, Guiboux JP (2000) Effect of anular repair
on the healing strength of the intervertebral disc: a sheep model. Spine 25(17):2165–
2170.
4. Alini M, Li W, Markovic P et al (2003) The potential and limitations of a cell-seeded
collagen/hyaluronan scaffold to engineer an intervertebral disc-like matrix. Spine
28(5):446–454
5. Alini M, Roughley PJ, Antoniou J, Stoll T, Aebi M (2002) A biological approach to treating
disc degeneration: not for today, but maybe for tomorrow. Eur Spine J 11(Suppl 2):S215–
S220
6. Andersson GB, An HS, Oegema TR Jr, Setton LA (2006) Directions for future research. J
Bone Joint Surg Am 88(Suppl 2):110–114.
7. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE (2005) Long-term outcomes of surgical
and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year
results from the maine lumbar spine study. Spine 30(8):927–935.
8. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE (2005) Long-term outcomes of surgical
and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the
maine lumbar spine study. Spine 30(8):936–943.
9. Bajanes G, Perez A, Diaz M (2007) One year follow up of discectomy patients who
received a mesh to repair the annulus fibrosus, vol 7. Spine Arthroplasty Society, Berlin
10. Battie MC, Videman T (2006) Lumbar disc degeneration: epidemiology and genetics. J
Bone Joint Surg Am 88(Suppl 2):3–9.
11. Best BA, Guilak F, Setton LA et al (1994) Compressive mechanical properties of the
human anulus fibrosus and their relationship to biochemical composition. Spine
19(2):212–221
12. Bourgeault C, Beaubien B, Griffith S (2007) Biomechanical assessment of annulus
fibrosus repair with suture tethered anchors. Spine Arthroplasty Society, Berlin
13. Bron JL, van Royen BJ, Wuisman PI (2007) The clinical significance of lumbosacral
transitional anomalies. Acta Orthop Belg 73(6):687–695
14. Bruehlmann SB, Rattner JB, Matyas JR, Duncan NA (2002) Regional variations in the
cellular matrix of the annulus fibrosus of the intervertebral disc. J Anat 201(2):159–171.
15. Cao L, Guilak F, Setton LA (2007) Three-dimensional morphology of the pericellular
matrix of intervertebral disc cells in the rat. J Anat 211(4):444–452
16. Carragee EJ, Han MY, Suen PW, Kim D (2003) Clinical outcomes after lumbar
discectomy for sciatica: the effects of fragment type and anular competence. J Bone Joint
Surg Am 85-A(1):102–108
Chapter 5
100
17. Cassidy JJ, Hiltner A, Baer E (1989) Hierarchical structure of the intervertebral disc.
Connect Tissue Res 23(1):75–88.
18. Cauthen J (1999) Microsurgical reconstruction (annuloplasty) following lumbar
discectomy: preliminary report of a new technique. Proceedings of the AANS/CNS joint
section on spine and peripheral nerves, Orlando
19. Chang G, Kim HJ, Kaplan D, Vunjak-Novakovic G, Kandel RA (2007) Porous silk scaffolds
can be used for tissue engineering annulus fibrosus. Eur Spine J 16(11):1848–1857.
20. Chou AI, Bansal A, Miller GJ, Nicoll SB (2006) The effect of serial monolayer passaging
on the collagen expression profile of outer and inner anulus fibrosus cells. Spine
31(17):1875–1881.
21. Chou AI, Reza AT, Nicoll SB (2008) Distinct intervertebral disc cell populations adopt
similar phenotypes in three-dimensional culture. Tissue Eng Part A 14:2079–2087
22. Choy DS (2000) Familial incidence of intervertebral disc herniation: an hypothesis
suggesting that laminectomy and discectomy may be counterproductive. J Clin Laser Med
Surg 18(1):29–32
23. Dai LY, Zhou Q, Yao WF, Shen L (2005) Recurrent lumbar disc herniation after
discectomy: outcome of repeat discectomy. Surg Neurol 64(3):226–231.
24. Derderian CA, Bastidas N, Lerman OZ et al (2005) Mechanical strain alters gene
expression in an in vitro model of hypertrophic scarring. Ann Plast Surg 55(1):69–75.
25. Duncan NA (2006) Cell deformation and micromechanical environment in the
intervertebral disc. J Bone Joint Surg Am 88(Suppl 2):47–51.
26. Edwards WT, Ordway NR, Zheng Y et al (2001) Peak stresses observed in the posterior
lateral anulus. Spine 26(16):1753–1759.
27. Elfervig MK, Minchew JT, Francke E, Tsuzaki M, Banes AJ (2001) IL-1beta sensitizes
intervertebral disc annulus cells to fluid-induced shear stress. J Cell Biochem 82(2):290–
298.
28. Errington RJ, Puustjarvi K, White IR, Roberts S, Urban JP (1998) Characterisation of
cytoplasm-filled processes in cells of the intervertebral disc. J Anat 192(Pt 3):369–378.
29. Ethier DB, Cain JE, Yaszemski MJ et al (1994) The influence of anulotomy selection on
disc competence. A radiographic, biomechanical, and histologic analysis. Spine
19(18):2071–2076.
30. Evans C (2006) Potential biologic therapies for the intervertebral disc. J Bone Joint Surg
Am 88(Suppl 2):95–98.
31. Fazzalari NL, Costi JJ, Hearn TC et al (2001) Mechanical and pathologic consequences
of induced concentric anular tears in an ovine model. Spine 26(23):2575–2581.
32. Feng H, Danfelter M, Stromqvist B, Heinegard D (2006) Extracellular matrix in disc
degeneration. J Bone Joint Surg Am 88(Suppl 2):25–29.
Annulus fibrosus repair
101
33. Floman Y, Millgram MA, Smorgick Y, Rand N, Ashkenazi E (2007) Failure of the Wallis
interspinous implant to lower the incidence of recurrent lumbar disc herniations in
patients undergoing primary disc excision. J Spinal Disord Tech 20(5):337–341.
34. Ganey T, Libera J, Moos V et al (2003) Disc chondrocyte transplantation in a canine
model: a treatment for degenerated or damaged intervertebral disc. Spine 28(23):2609–
2620.
35. Garlet TP, Coelho U, Silva JS, Garlet GP (2007) Cytokine expression pattern in
compression and tension sides of the periodontal ligament during orthodontic tooth
movement in humans. Eur J Oral Sci 115(5):355–362.
36. Gorensek M, Vilandecic M, Woburn (2007) Clinical investigation of intrinsic
therapeutics Barricaid, a novel device for closing defects in the annulus. NASS 2006
37. Gruber HE, Fisher EC Jr, Desai B et al (1997) Human intervertebral disc cells from the
annulus: three-dimensional culture in agarose or alginate and responsiveness to TGF-
beta1. Exp Cell Res 235(1):13–21.
38. Gruber HE, Ingram JA, Norton HJ, Hanley EN Jr (2007) Senescence in cells of the aging
and degenerating intervertebral disc: immunolocalization of senescence-associated beta-
galactosidase in human and sand rat discs. Spine 32(3):321–327.
39. Gruber HE, Leslie K, Ingram J, Norton HJ, Hanley EN (2004) Cell-based tissue
engineering for the intervertebral disc: in vitro studies of human disc cell gene expression
and matrix production within selected cell carriers. Spine J 4(1):44–55.
40. Gruber HE, Ma D, Hanley EN Jr, Ingram J, Yamaguchi DT (2001) Morphologic and
molecular evidence for gap junctions and connexin 43 and 45 expression in annulus
fibrosus cells from the human intervertebral disc. J Orthop Res 19(5):985– 989.
41. Guerin HL, Elliott DM (2007) Quantifying the contributions of structure to annulus
fibrosus mechanical function using a nonlinear, anisotropic, hyperelastic model. J Orthop
Res 25(4):508–516.
42. Hakkinen A, Kiviranta I, Neva MH, Kautiainen H, Ylinen J (2007) Reoperations after first
lumbar disc herniation surgery; a special interest on residives during a 5-year follow-up.
BMC Musculoskelet Disord 8:2.
43. Hampton D, Laros G, McCarron R, Franks D (1989) Healing potential of the anulus
fibrosus. Spine 14(4):398–401.
44. Hansson E, Hansson T (2007) The cost-utility of lumbar disc herniation surgery. Eur
Spine J 16(3):329–337.
45. Hegewald AA, Ringe J, Sittinger M, Thome C (2008) Regenerative treatment strategies
in spinal surgery. Front Biosci 13:1507–1525.
46. Helder MN, Knippenberg M, Klein-Nulend J, Wuisman PI (2007) Stem cells from
adipose tissue allow challenging new concepts for regenerative medicine. Tissue Eng
13(8):1799–1808.

Chapter 5
102
47. Helen W, Gough JE (2007) Cell viability, proliferation and extracellular matrix
production of human annulus fibrosus cells cultured within PDLLA/Bioglass(R) composite
foam scaffolds in vitro. Acta Biomater 3:715–721
48. Helen W, Merry CL, Blaker JJ, Gough JE (2007) Threedimensional culture of annulus
fibrosus cells within PDLLA/Bioglass composite foam scaffolds: assessment of cell
attachment, proliferation and extracellular matrix production. Biomaterials 28(11):2010–
2020.
49. Heuer F, Schmidt H, Wilke HJ (2008) The relation between intervertebral disc bulging
and annular fiber associated strains for simple and complex loading. J Biomech 41:1086–
1094
50. Holm S, Maroudas A, Urban JP, Selstam G, Nachemson A (1981) Nutrition of the
intervertebral disc: solute transport and metabolism. Connect Tissue Res 8(2):101–119.
51. Hoogendoorn RJ, Lu ZF, Kroeze RJ et al (2008) Adipose stem cells for intervertebral disc
regeneration: current status and concepts for the future. J Cell Mol Med (in press)
52. Horner HA, Roberts S, Bielby RC et al (2002) Cells from different regions of the
intervertebral disc: effect of culture system on matrix expression and cell phenotype.
Spine 27(10):1018–1028.
53. Humzah MD, Soames RW (1988) Human intervertebral disc: structure and function.
Anat Rec 220(4):337–356.
54. Iatridis JC, ap Gwynn I (2004) Mechanisms for mechanical damage in the intervertebral
disc annulus fibrosus. J Biomech 37(8):1165–1175.
55. Inkinen RI, Lammi MJ, Lehmonen S et al (1998) Relative increase of biglycan and
decorin and altered chondroitin sulphate epitopes in the degenerating human
intervertebral disc. J Rheumatol 25(3):506–514
56. Jahanyar J, Joyce DL, Southard RE et al (2007) Decorin-mediated transforming growth
factor-beta inhibition ameliorates adverse cardiac remodeling. J Heart Lung Transplant
26(1):34–40.
57. Johnson EF, Chetty K, Moore IM, Stewart A, Jones W (1982) The distribution and
arrangement of elastic fibres in the intervertebral disc of the adult human. J Anat 135(Pt
2):301–309
58. Johnson WE, Wootton A, El HA et al (2006) Topographical guidance of intervertebral
disc cell growth in vitro: towards the development of tissue repair strategies for the
anulus fibrosus. Eur Spine J 15(Suppl 3):S389–S396.
59. Jonsson B, Stromqvist B (1993) Repeat decompression of lumbar nerve roots. A
prospective two-year evaluation. J Bone Joint Surg Br 75(6):894–897
60. Kamaric E, Gorensek S, Trummer M et al (2007) Surgical factors affecting after lumbar
discectomy: the need for an anular closure device. In Thera
61. Katz JN (2006) Lumbar disc disorders and low-back pain: socioeconomic factors and
consequences. J Bone Joint Surg Am 88(Suppl 2):21–24.
Annulus fibrosus repair
103
62. Key JA, Ford LT (1948) Experimental intervertebral-disc lesions. J Bone Joint Surg Am
30A(3):621–630
63. Kim JM, Lee SH, Ahn Y et al (2007) Recurrence after successful percutaneous
endoscopic lumbar discectomy. Minim Invasive Neurosurg 50(2):82–85.
64. Kluba T, Niemeyer T, Gaissmaier C, Grunder T (2005) Human anulus fibrosis and
nucleus pulposus cells of the intervertebral disc: effect of degeneration and culture system
on cell phenotype. Spine 30(24):2743–2748.
65. Korecki CL, Costi JJ, Iatridis JC (2008) Needle puncture injury affects intervertebral disc
mechanics and biology in an organ culture model. Spine 33(3):235–241.
66. Laus M, Bertoni F, Bacchini P, Alfonso C, Giunti A (1993) Recurrent lumbar disc
herniation: what recurs? (A morphological study of recurrent disc herniation). Chir Organi
Mov 78(3):147–154
67. Leung VY, Chan D, Cheung KM (2006) Regeneration of intervertebral disc by
mesenchymal stem cells: potentials, limitations, and future direction. Eur Spine J 15(Suppl
3):S406–S413.
68. Lotz JC, Kim AJ (2005) Disc regeneration: why, when, and how. Neurosurg Clin N Am
16(4):657–663, vii.
69. Lutolf MP, Hubbell JA (2005) Synthetic biomaterials as instructive extracellular
microenvironments for morphogenesis in tissue engineering. Nat Biotechnol 23(1):47–55.
70. Macri L, Silverstein D, Clark RA (2007) Growth factor binding to the pericellular matrix
and its importance in tissue engineering. Adv Drug Deliv Rev 59(13):1366–1381.
71. Marchand F, Ahmed AM (1990) Investigation of the laminate structure of lumbar disc
anulus fibrosus. Spine 15(5):402–410.
72. Masuda K, Takegami K, An H et al (2003) Recombinant osteogenic protein-1
upregulates extracellular matrix metabolism by rabbit annulus fibrosus and nucleus
pulposus cells cultured in alginate beads. J Orthop Res 21(5):922–930.
73. McNally DS, Adams MA (1992) Internal intervertebral disc mechanics as revealed by
stress profilometry. Spine 17(1):66–73.
74. Meisel HJ, Siodla V, Ganey T et al (2007) Clinical experience in cell-based therapeutics:
disc chondrocyte transplantation A treatment for degenerated or damaged intervertebral
disc. Biomol Eng 24(1):5–21.
75. Melrose J, Ghosh P, Taylor TK et al (1997) Elevated synthesis of biglycan and decorin in
an ovine annular lesion model of experimental disc degeneration. Eur Spine J 6(6):376–
384. 76. Melrose J, Smith SM, Appleyard RC, Little CB (2008) Aggrecan, versican and type
VI collagen are components of annular translamellar crossbridges in the intervertebral
disc. Eur Spine J 17(2):314–324.
77. Melrose J, Smith SM, Little CB et al (2008) Recent advances in annular pathobiology
provide insights into rim-lesion mediated intervertebral disc degeneration and potential
new approaches to annular repair strategies. Eur Spine J 17(9):1131–1148.
Chapter 5
104
78. Mizuno H, Roy AK, Vacanti CA et al (2004) Tissue-engineered composites of anulus
fibrosus and nucleus pulposus for intervertebral disc replacement. Spine 29(12):1290–
1297.
79. Moore RJ, Osti OL, Vernon-Roberts B, Fraser RD (1992) Changes in endplate vascularity
after an outer anulus tear in the sheep. Spine 17(8):874–878.
80. Natarajan RN, Williams JR, Andersson GB (2004) Recent advances in analytical
modeling of lumbar disc degeneration. Spine 29(23):2733–2741.
81. Nemoto Y, Matsuzaki H, Tokuhasi Y et al (2006) Histological changes in intervertebral
discs after smoking and cessation: experimental study using a rat passive smoking model. J
Orthop Sci 11(2):191–197.
82. Nerlich AG, Bachmeier BE, Schleicher E et al (2007) Immunomorphological analysis of
RAGE receptor expression and NFkappaB activation in tissue samples from normal and
degenerated intervertebral discs of various ages. Ann N Y Acad Sci 1096:239–248.
83. Nerlich AG, Schleicher ED, Boos N (1997) Volvo Award winner in basic science studies.
Immunohistologic markers for age-related changes of human lumbar intervertebral discs.
Spine 22(24):2781–2795.
84. Nerurkar NL, Elliott DM, Mauck RL (2007) Mechanics of oriented electrospun
nanofibrous scaffolds for annulus fibrosus tissue engineering. J Orthop Res 25(8):1018–
1028.
85. Osti OL, Vernon-Roberts B, Fraser RD (1990) 1990 Volvo Award in experimental
studies. Anulus tears and intervertebral disc degeneration. An experimental study using an
animal model. Spine 15(8):762–767.
86. Osti OL, Vernon-Roberts B, Moore R, Fraser RD (1992) Annular tears and disc
degeneration in the lumbar spine. A post-mortem study of 135 discs. J Bone Joint Surg Br
74(5):678–682
87. Paajanen H, Haapasalo H, Kotilainen E, Aunapuu M, Kettunen J (1999) Proliferation
potential of human lumbar disc after herniation. J Spinal Disord 12(1):57–60.
88. Perie D, Korda D, Iatridis JC (2005) Confined compression experiments on bovine
nucleus pulposus and annulus fibrosus: sensitivity of the experiment in the determination
of compressive modulus and hydraulic permeability. J Biomech 38(11):2164–2171.
89. Pezowicz CA, Robertson PA, Broom ND (2006) The structural basis of interlamellar
cohesion in the intervertebral disc wall. J Anat 208(3):317–330.
90. Postacchini F, Bellocci M, Massobrio M (1984) Morphologic changes in annulus
fibrosus during aging. An ultrastructural study in rats. Spine 9(6):596–603.
91. Rannou F, Lee TS, Zhou RH et al (2004) Intervertebral disc degeneration: the role of the
mitochondrial pathway in annulus fibrosus cell apoptosis induced by overload. Am J Pathol
164(3):915–924
Annulus fibrosus repair
105
92. Rannou F, Richette P, Benallaoua M et al (2003) Cyclic tensile stretch modulates
proteoglycan production by intervertebral disc annulus fibrosus cells through production
of nitrite oxide. J Cell Biochem 90(1):148–157.
93. Reza AT, Nicoll SB (2008) Hydrostatic pressure differentially regulates outer and inner
annulus fibrosus cell matrix production in 3D scaffolds. Ann Biomed Eng 36(2):204–213.
94. Richardson SM, Knowles R, Marples D, Hoyland JA, Mobasheri A (2008) Aquaporin
expression in the human intervertebral disc. J Mol Histol (in press)
95. Risbud MV, Guttapalli A, Tsai TT et al (2007) Evidence for skeletal progenitor cells in
the degenerate human intervertebral disc. Spine 32(23):2537–2544
96. Roberts S, Evans EH, Kletsas D, Jaffray DC, Eisenstein SM (2006) Senescence in human
intervertebral discs. Eur Spine J 15(Suppl 3):S312–S316.
97. Roberts S, Evans H, Trivedi J, Menage J (2006) Histology and pathology of the human
intervertebral disc. J Bone Joint Surg Am 88(Suppl 2):10–14.
98. Roughley PJ (2004) Biology of intervertebral disc aging and degeneration: involvement
of the extracellular matrix. Spine 29(23):2691–2699.
99. Rousseau MA, Ulrich JA, Bass EC et al (2007) Stab incision for inducing intervertebral
disc degeneration in the rat. Spine 32(1):17–24.
100. Saad L, Spector M (2004) Effects of collagen type on the behavior of adult canine
annulus fibrosus cells in collagen-glycosaminoglycan scaffolds. J Biomed Mater Res A
71(2):233– 241.
101. Sato M, Asazuma T, Ishihara M et al (2003) An experimental study of the
regeneration of the intervertebral disc with an allograft of cultured annulus fibrosus cells
using a tissue-engineering method. Spine 28(6):548–553.
102. Sato M, Asazuma T, Ishihara M et al (2003) An atelocollagen honeycomb-shaped
scaffold with a membrane seal (ACHMSscaffold) for the culture of annulus fibrosus cells
from an intervertebral disc. J Biomed Mater Res A 64(2):248–256.
103. Sato M, Kikuchi M, Ishihara M et al (2003) Tissue engineering of the intervertebral
disc with cultured annulus fibrosus cells using atelocollagen honeycomb-shaped scaffold
with a membrane seal (ACHMS scaffold). Med Biol Eng Comput 41(3):365–371.
104. Schroeder Y, Sivan S, Wilson W et al (2007) Are disc pressure, stress, and osmolarity
affected by intra- and extrafibrillar fluid exchange? J Orthop Res 25(10):1317–1324.
105. Sebastine IM, Williams DJ (2007) Current developments in tissue engineering of
nucleus pulposus for the treatment of intervertebral disc degeneration. Conf Proc IEEE Eng
Med Biol Soc 1:6400–6405.
106. Setton LA, Chen J (2006) Mechanobiology of the intervertebral disc and relevance to
disc degeneration. J Bone Joint Surg Am 88(Suppl 2):52–57.
107. Shao X, Hunter CJ (2007) Developing an alginate/chitosan hybrid fiber scaffold for
annulus fibrosus cells. J Biomed Mater Res A 82(3):701–710.
Chapter 5
106
108. Sherman J, Cauthen J, Griffith S (2007) Pre-clinical evaluation of a mesh device for
repairing the annulus fibrosus. Spine Arthroplasty Society, Berlin
109. Smith JW, Walmsley R (1951) Experimental incision of the intervertebral disc. J Bone
Joint Surg Br 33-B(4):612–625
110. Smith LJ, Byers S, Costi JJ, Fazzalari NL (2008) Elastic fibers enhance the mechanical
integrity of the human lumbar annulus fibrosus in the radial direction. Ann Biomed Eng
36(2):214–223.
111. Smith LJ, Fazzalari NL (2006) Regional variations in the density and arrangement of
elastic fibres in the anulus fibrosus of the human lumbar disc. J Anat 209(3):359–367.
112. Stokes IA (1987) Surface strain on human intervertebral discs. J Orthop Res 5(3):348–
355.
113. Suk KS, Lee HM, Moon SH, Kim NH (2001) Recurrent lumbar disc herniation: results of
operative management. Spine 26(6):672–676.
114. Sun DD, Leong KW (2004) A nonlinear hyperelastic mixture theory model for
anisotropy, transport, and swelling of annulus fibrosus. Ann Biomed Eng 32(1):92–102.
115. Swartz KR, Trost GR (2003) Recurrent lumbar disc herniation. Neurosurg Focus
15(3):E10.
116. Takegami K, An HS, Kumano F et al (2005) Osteogenic protein- 1 is most effective in
stimulating nucleus pulposus and annulus fibrosus cells to repair their matrix after
chondroitinase ABCinduced in vitro chemonucleolysis. Spine J 5(3):231–238.
117. Taylor W (2006) Biologic collagen PMMA injection (artifill) repairs mid-annular
concentric defects in the ovine model. Spine J 6(5S1):48S–49S
118. Urban JP, Holm S, Maroudas A, Nachemson A (1982) Nutrition of the intervertebral
disc: effect of fluid flow on solute transport. Clin Orthop Relat Res (170):296–302
119. Videman T, Nurminen M (2004) The occurrence of anular tears and their relation to
lifetime back pain history: a cadaveric study using barium sulfate discography. Spine
29(23):2668–2676.
120. Walmsley R (1953) The development and growth of the intervertebral disc. Edinburgh
Med J 60(8):341–364
121. Wan Y, Feng G, Shen FH et al (2007) Novel biodegradable poly(1, 8-octanediol
malate) for annulus fibrosus regeneration. Macromol Biosci 7(11):1217–1224.
122. Wan Y, Feng G, Shen FH, Laurencin CT, Li X (2008) Biphasic scaffold for annulus
fibrosus tissue regeneration. Biomaterials 29(6):643–652.
123. Wang YH, Kuo TF, Wang JL (2007) The implantation of noncell-based materials to
prevent the recurrent disc herniation: an in vivo porcine model using quantitative
discomanometry examination. Eur Spine J 16(7):1021–1027.
124. Wilda H, Gough JE (2006) In vitro studies of annulus fibrosus disc cell attachment,
differentiation and matrix production on PDLLA/45S5 Bioglass composite films.
Biomaterials 27(30):5220–5229.
Annulus fibrosus repair
107
125. Wilke HJ, Heuer F, Neidlinger-Wilke C, Claes L (2006) Is a collagen scaffold for a tissue
engineered nucleus replacement capable of restoring disc height and stability in an animal
model? Eur Spine J 15(Suppl 3):S433–S438.
126. Yamazaki S, Banes AJ, Weinhold PS et al (2002) Vibratory loading decreases
extracellular matrix and matrix metalloproteinase gene expression in rabbit annulus cells.
Spine J 2(6):415–420.
127. Yamazaki S, Weinhold PS, Graff RD et al (2003) Annulus cells release ATP in response
to vibratory loading in vitro. J Cell Biochem 90(4):812–818.
128. Yeung AT, Yeung CA (2007) Minimally invasive techniques for the management of
lumbar disc herniation. Orthop Clin North Am 38(3):363–372.
129. Yu J, Fairbank JC, Roberts S, Urban JP (2005) The elastic fiber network of the anulus
fibrosus of the normal and scoliotic human intervertebral disc. Spine 30(16):1815–1820.
130. Yu J, Tirlapur U, Fairbank J et al (2007) Microfibrils, elastin fibres and collagen fibres
in the human intervertebral disc and bovine tail disc. J Anat 210(4):460–471.
131. Zhang Y, Anderson DG, Phillips FM et al (2007) Comparative effects of bone
morphogenetic proteins and Sox9 overexpression on matrix accumulation by bovine
anulus fibrosus cells: implications for anular repair. Spine 32(23):2515–2520
108
6
Biomechanical and in vivo evaluation of experi-
mental closure devices of the annulus fibrosus
designed for a goat nucleus replacement model.
JL Bron
AJ van der Veen
MN Helder
BJ van Royen
TH Smit
Chapter 6
110
Abstract
Promising strategies are being developed to replace or regenerate the herniated
nucleus pulposus. However, clinical efficacy of these methods has still to be
addressed, and the lack of appropriate annulus closure techniques is increasingly
being recognised as a major limiting factor. In the current study, in vitro and in
vivo evaluation of novel annulus closure devices (ACDs) was performed. These
devices are intended to be used in adjunct to nucleus replacement therapies in an
experimental goat study. After a standardised discectomy had been performed,
different ACDs were implanted solely or in addition to a collagen nucleus
replacement implant. Biomechanical effects and axial failure load were assessed
in vitro and followed by in vivo evaluation in a goat model. On axial compression,
the average axial failure load for ACDs with four barb rings was significantly higher
compared to the implants with five barb rings. The increased range of flexion–
extension and latero-flexion observed after discectomy were restored to the
normal range after implantation of the implants. Positive findings with the four-
ring ACD were confirmed in goats after a follow-up of 2 weeks in vivo. However,
after 6 weeks most implants (n = 16) showed signs of destruction and
displacement. Although there seemed to be a tendency towards better results
when ACDs were placed in addition to the nucleus replacements, these
differences were not statistically significant. Moreover, two endplate reactions
extending into the subchondral bone were observed, most likely due to
continuous friction between the ACD and the vertebrae. Although current results
are encouraging first steps towards the development of an efficient ACD for
animal models, further optimisation is necessary. Current results also show that
one cannot rely on in vitro biomechanical studies with annulus closure
techniques, and these should always be confirmed in vivo in a large animal model.
Biomechanical and in vivo evaluation
111
Introduction
The lack of effective strategies to deal with the damaged annulus fibrosus (AF)
may currently be recognised as one of the major limiting factors for successful
intervertebral disc engineering after herniation [7, 8, 10, 11, 26]. During the last
decade, increasing knowledge and technical advancements in the field of tissue
engineering have resulted in numerous promising strategies to replace or
regenerate the nucleus pulposus (NP) [11, 19]. None of these advancements,
however, has yet resulted in a clinically proven effective therapy [12, 24]. Since
optimal regeneration of the NP should result in a restoration of the physiological
high intradiscal pressure, the surrounding AF is generally of too inferior quality to
withstand these forces [15]. In patients treated for disc herniation, there is often a
loss of annulus tissue, restricting the potential of sutures and glues [1, 12]. These
materials have limited strength, and the annulus usually has to be closed under
tension. Tissue engineering strategies of the AF that deal with the ‘gap’ due to loss
of AF tissue are currently being developed. However, the attempts are mainly
directed towards the engineering of native AF tissue, especially in the long term,
instead of providing instant mechanical strength after surgery [5]. These AF tissue
engineering attempts are therefore not ready to be used in adjunct nucleus
replacement strategies.
In this chapter, we investigate experimental ACDs, designed to be used in adjunct
to nucleus replacement therapies in a goat model. These devices are primarily
intended to enable the study of nucleus replacement therapies in animal models.
However, the findings may also reveal valuable information for the development
of human annulus closure devices. The purpose of the implants is to provide
immediate mechanical support without affecting the nucleus replacement
therapy or spinal biomechanics. Biomechanical and in vivo evaluation of the ACDs
were performed in a goat model, both solely and in addition to a collagen nucleus
replacement matrix that has been described earlier [12, 24].
Chapter 6
112
Materials and methods
Nucleus replacement model
A standardised discectomy procedure was developed, intended to allow the
evaluation of novel nucleus replacement therapies in vivo. The procedure was
designed for, and performed on mature Dutch female goat intervertebral discs.
Initially, the NP is evacuated with custom-made instruments (Fig. 1a). These
instruments consist of tubes with increasing diameter, which are used to make an
entry site laterally into the AF. Via the largest tube, with an outer diameter of 3
mm, instruments are inserted to evacuate the NP. The discectomy was always
performed as complete as possible without damaging the AF or the endplates,
and the result was judged by the surgeon before continuation. After evacuation,
the disc space is filled with a dense collagen implant (NuRes, Arthro Kinetics AG,
Esslingen, Germany) that has been described previously [6]. Shortly, collagen gel is
polymerised after which the density is increased by plastic compression. The
chosen density was 25% w/w of collagen, which has a stiffness comparable to the
native NP. For this study, the collagen matrix was prepared in a ‘snake’-like shape
(diameter 2.5 mm, length 30 mm, volume ~0.6 cm3), allowing implantation via the
tubes (Fig. 1b). After insertion of the collagen implant, the annulus defect was
closed with one of the four different versions of a polyethylene closure device
described below. (A more detailed description of the model is presented in:
addendum 1)
Annulus closure devices (ACDs)
We first performed extensive preliminary testing, using the same set up for axial
compression as described below (see ‘‘Biomechanical evaluation’’). These pilot
experiments (data not shown) were intended to determine the optimal shape and
dimensions of the annulus closure devices (Fig. 2a). All devices were intended to
close a standardised 3-mm circular defect in the AF of the goat intervertebral disc,
as described above. Four devices were further evaluated in the current study (Fig.
2b) since they were found to withstand axial compression forces over 1,000 N.
These four ACDs were composed of polyethylene and consisted of a core
(diameter 1.3 or 1.5 mm) with four or five barb rings that have a maximum
diameter of 3.5 mm (Fig. 2b). The ACDs were introduced into the AF till all barb

Biomechanical and in vivo evaluation
113
rings were inside the defect. The back end of ACDs was used to hold the implants
during implantation, and this was cut after implantation (Fig. 2c).
Intradiscal pressure calibration measurements
In order to determine the relation between the applied load and the pressure
inside the goat intervertebral disc, we first performed pressure measurements.
This information is essential to be sure whether the resulting pressures of the
applied loads in the current study are comparable to the intradiscal pressures
known from studies in vivo. For these calibration experiments, the lumbar spine
(L1–L6) of a goat, derived from a local abattoir, was meticulously cleaned of soft
tissues. The posterior elements were left intact. The spine was separated into
three separate motion segments by incision of the discs between L2–L3 and L4–
L5. The ends of the vertebrae were embedded in a low melting point bismuth
alloy, and the motion segments were placed in upright position in the
biomechanical testing apparatus (Instron, Norwood, MA, USA). First, a pressure
needle was inserted anteriorly into the core of each disc. Next, a load was applied
increasing with 50 N/s to a maximum of 1,000 N or a maximum of 3 MPa as
measured by the needle, whatever came first (higher pressures would result in
irreversible needle damage). Both the values for load and pressure were
documented. The measurements were repeated two times with the needle
inserted via both lateral sides of the discs.
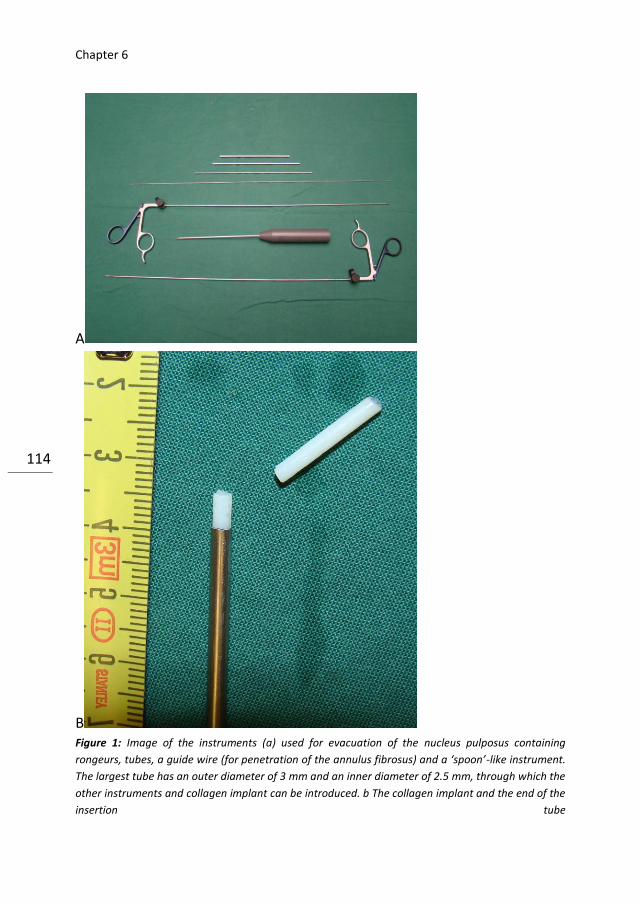
Chapter 6
114
A
B Figure 1: Image of the instruments (a) used for evacuation of the nucleus pulposus containing
rongeurs, tubes, a guide wire (for penetration of the annulus fibrosus) and a ‘spoon’-like instrument.
The largest tube has an outer diameter of 3 mm and an inner diameter of 2.5 mm, through which the
other instruments and collagen implant can be introduced. b The collagen implant and the end of the
insertion tube
Biomechanical and in vivo evaluation
115
Biomechanical evaluation
Biomechanical experiments were performed prior to the in vivo study on spinal
segments, derived from the local abattoir. Using the same set up as described
with the pressure experiments, the axial failure loads of different ACDs were
tested using the standardised nucleus replacement model. After the implants
were inserted, an axial compression load was applied to a maximum of 5,000 N.
The experiments were ended when failure, considered as the leakage of the
collagen implant or extrusion of closure devices, was observed. Each ACD was
tested on three different motion segments (L1–L2, L3–L4 and L5–L6). For every
experiment a freshly dissected spinal segment was used. In addition to the failure
experiments, the effects of the implants on the biomechanical behaviour of the
motion segments were investigated. These experiments were mainly performed
to exclude undesired effects on the range of latero-flexion or flexion–extension
due to the ACDs and to assess the possibility of the implants to restore the effects
after discectomy. After fixation in bismuth, 12 motions segments (four of each
different level) were multidirectionally tested using a four-point flexion–extension
set up and the instron 8872 testing machine (Instron Corp., Norwood, MA, USA).
The motion segments were submitted to four cycles of flexion–extension and
latero-flexion under a maximum moment of 2 Nm at a speed of 1º/s. Specimens
were tested before discectomy (native), after discectomy and with both implants
(nucleus implant and the four rings 1.5 mm ACD) inside. During all experiments,
the segments were kept moisturised by wrapping with surgical gauze drowned in
0.9% saline. Force–deformation data acquisition was performed for each direction
through materials testing software (Fast Track 2, Instron Corp., Norwood, MA,
USA). The range of motion-data of the third cycle of the tests was used for further
calculation. The mean changes in the range of motion after discectomy and
implantation of both implants were calculated as ratios compared to native values
(treatment over control).
In vivo evaluation
Surgical procedure and animal care were performed in compliance with the
regulations of the Dutch legislation for animal research, and the Animal Ethics
Committee of the VU University Medical Center approved the protocol. Ten goats
were sedated with 10 mg/kg ketamine and 1.5 mg atropine intramuscularly,
followed by 0.4 mg/kg etomidate intravenously. General anaesthesia was

Chapter 6
116
maintained with 4 µg/kg fentanyl per hour, 0.3 mg/kg midazolam per hour and
1.5–2.5% isoflurane. Before surgery, standardised lateral thoracolumbar
roentgenograms were obtained. A dorsal paravertebral incision was made. The
IVDs were identified using a left retroperitoneal approach and exposed after
mobilisation of the psoas muscle. Level determination was performed by
identification of the lowest rib. Two discectomies, as described above, were
randomly performed over the levels T13–L1, L2–L3 or L4–L5. At one of these
levels, the collagen nucleus implant was inserted after evacuation of the NP,
followed by closure of the annulus defect with the ACD (sterilised by γ-
irradiation). At the other level the plug was inserted solely. Two variants of the
ACDs were used in the 6-week follow-up group: four goats received implants with
a core diameter of 1.3 mm, the remainder with a core diameter of 1.5 mm. The
number (four) and diameter (3.5 mm) of the barb rings was the same for all
implants. Two of the goats were terminated by an overdose pentobarbital after 2
weeks and the remaining eight goats after 6 weeks. The latter group returned to
their habitual environment from 1 week postoperative until 1 week prior to the
autopsy. Evaluation was similar for all goats. After termination, the lumbar spines
of the goats were harvested, and magnetic resonance imaging (MRI) of the
explants was performed within 2 h. Hereafter, all soft tissue was removed, and
careful macroscopic inspection was performed. Finally, a band saw was used to
obtain transversal slices of the discs for macroscopic inspection. Both,
macroscopic examination and MR Imaging were used to determine the position of
the ACDs.
The position was classified as ‘‘in situ’’, partially displaced (maximum of two barb
rings outside the AF), or fully displaced (at least two barb rings outside the AF).
Statistics
To calculate differences between different implant groups, the Student T test was
used.

Biomechanical and in vivo evaluation
117
A B
C
Results
Pressure calibration measurements
The relation between the applied load and the pressure inside the three discs is
shown in Fig. 3. A load of 600 N corresponds with an intradiscal pressure of 3
MPa. No effect was observed by changing the place of needle insertion from
anterior to lateral, indicating that hydrostatic pressure was present within the
entire NP.
Figure 2: Overview image of
different closure systems used in
the pilot experiments (a) and in
current study (b). The implants vary
in the number of barb rings (4 or 5)
and in the diameter of the core (1.3
or 1.5 mm). The instrument that
was used to implant the devices is
shown in c
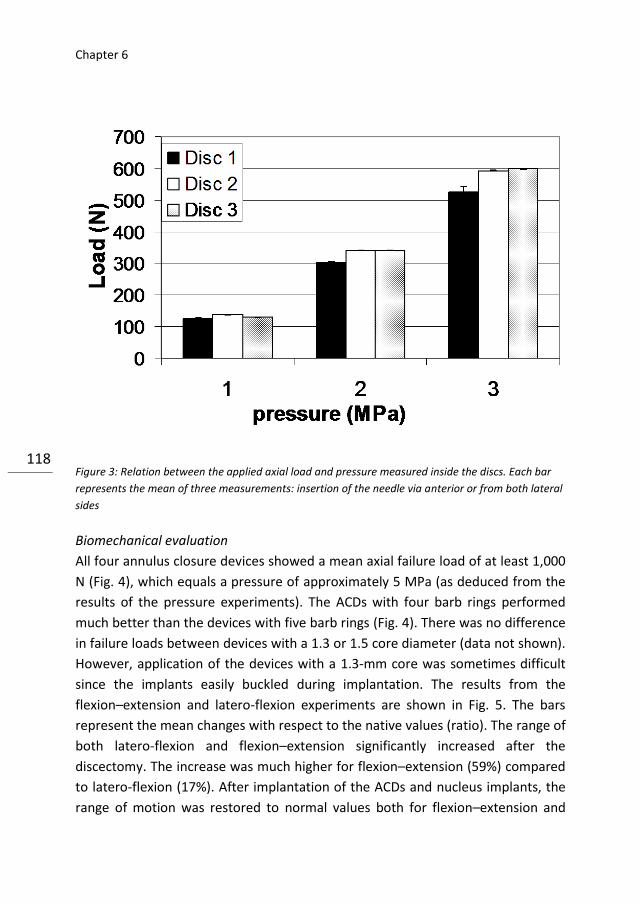
Chapter 6
118 Figure 3: Relation between the applied axial load and pressure measured inside the discs. Each bar
represents the mean of three measurements: insertion of the needle via anterior or from both lateral
sides
Biomechanical evaluation
All four annulus closure devices showed a mean axial failure load of at least 1,000
N (Fig. 4), which equals a pressure of approximately 5 MPa (as deduced from the
results of the pressure experiments). The ACDs with four barb rings performed
much better than the devices with five barb rings (Fig. 4). There was no difference
in failure loads between devices with a 1.3 or 1.5 core diameter (data not shown).
However, application of the devices with a 1.3-mm core was sometimes difficult
since the implants easily buckled during implantation. The results from the
flexion–extension and latero-flexion experiments are shown in Fig. 5. The bars
represent the mean changes with respect to the native values (ratio). The range of
both latero-flexion and flexion–extension significantly increased after the
discectomy. The increase was much higher for flexion–extension (59%) compared
to latero-flexion (17%). After implantation of the ACDs and nucleus implants, the
range of motion was restored to normal values both for flexion–extension and
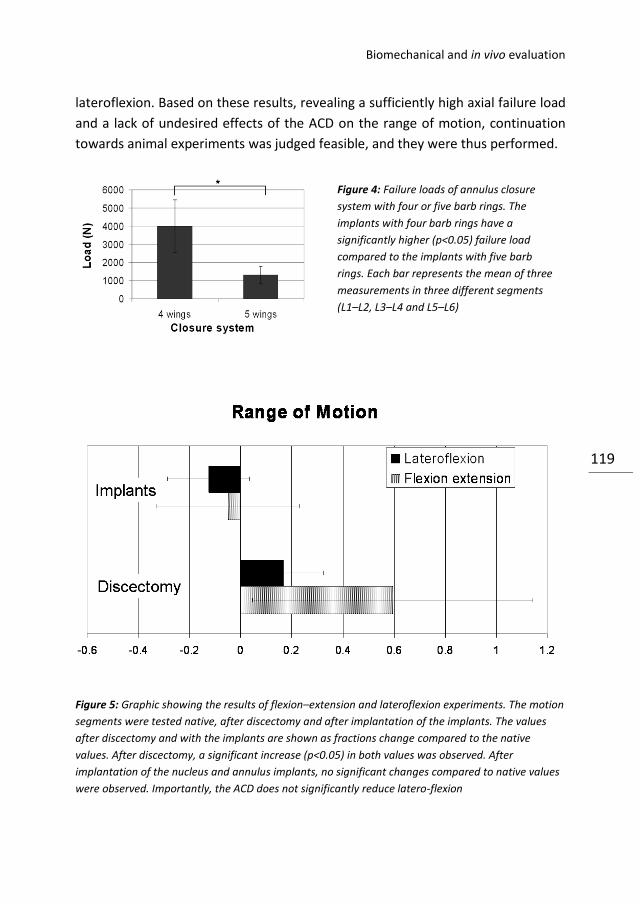
Biomechanical and in vivo evaluation
119
lateroflexion. Based on these results, revealing a sufficiently high axial failure load
and a lack of undesired effects of the ACD on the range of motion, continuation
towards animal experiments was judged feasible, and they were thus performed.
Figure 5: Graphic showing the results of flexion–extension and lateroflexion experiments. The motion
segments were tested native, after discectomy and after implantation of the implants. The values
after discectomy and with the implants are shown as fractions change compared to the native
values. After discectomy, a significant increase (p<0.05) in both values was observed. After
implantation of the nucleus and annulus implants, no significant changes compared to native values
were observed. Importantly, the ACD does not significantly reduce latero-flexion
Figure 4: Failure loads of annulus closure
system with four or five barb rings. The
implants with four barb rings have a
significantly higher (p<0.05) failure load
compared to the implants with five barb
rings. Each bar represents the mean of three
measurements in three different segments
(L1–L2, L3–L4 and L5–L6)
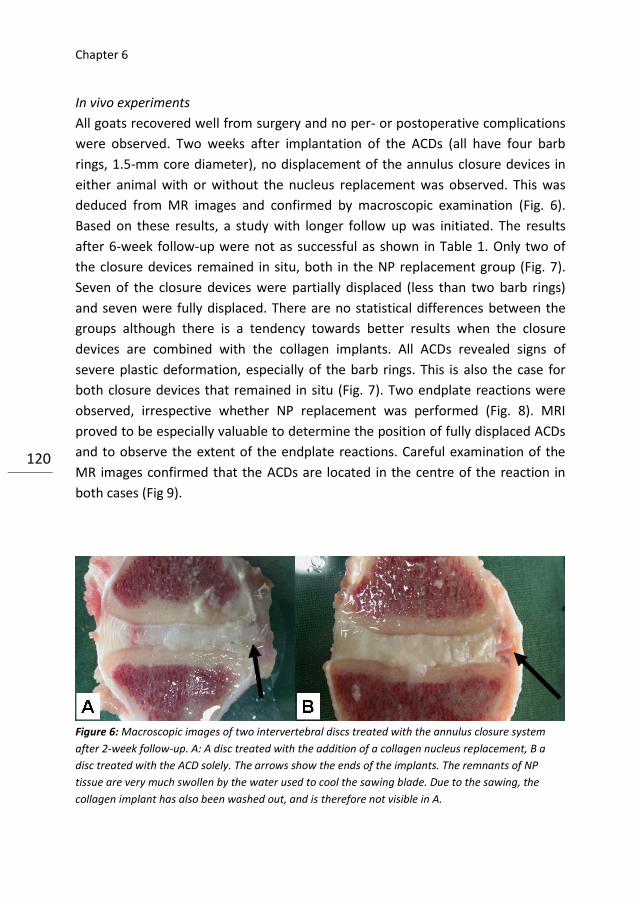
Chapter 6
120
In vivo experiments
All goats recovered well from surgery and no per- or postoperative complications
were observed. Two weeks after implantation of the ACDs (all have four barb
rings, 1.5-mm core diameter), no displacement of the annulus closure devices in
either animal with or without the nucleus replacement was observed. This was
deduced from MR images and confirmed by macroscopic examination (Fig. 6).
Based on these results, a study with longer follow up was initiated. The results
after 6-week follow-up were not as successful as shown in Table 1. Only two of
the closure devices remained in situ, both in the NP replacement group (Fig. 7).
Seven of the closure devices were partially displaced (less than two barb rings)
and seven were fully displaced. There are no statistical differences between the
groups although there is a tendency towards better results when the closure
devices are combined with the collagen implants. All ACDs revealed signs of
severe plastic deformation, especially of the barb rings. This is also the case for
both closure devices that remained in situ (Fig. 7). Two endplate reactions were
observed, irrespective whether NP replacement was performed (Fig. 8). MRI
proved to be especially valuable to determine the position of fully displaced ACDs
and to observe the extent of the endplate reactions. Careful examination of the
MR images confirmed that the ACDs are located in the centre of the reaction in
both cases (Fig 9).
Figure 6: Macroscopic images of two intervertebral discs treated with the annulus closure system
after 2-week follow-up. A: A disc treated with the addition of a collagen nucleus replacement, B a
disc treated with the ACD solely. The arrows show the ends of the implants. The remnants of NP
tissue are very much swollen by the water used to cool the sawing blade. Due to the sawing, the
collagen implant has also been washed out, and is therefore not visible in A.

Biomechanical and in vivo evaluation
121
Discussion
Figure 7: Image of one of the
implants that was still in situ after
6-week follow-up. There are clear
signs of destruction visible at the
barb rings of the implant (arrows).

Chapter 6
122
The need for annulus closure methods in addition to nucleus replacement
strategies is increasingly being recognised [3–5, 13, 20]. Wilke et al. [24] showed
that a collagen scaffold allows restoration of disc height and stability after
herniation in vitro. However, the absence of an appropriate annulus closure
technique limits the potential and applicability in vivo. These authors also showed
that glues, sutures or a combination of both are insufficient to provide sufficient
containment of a collagen scaffold [12]. This agrees with the findings in scientific
literature, in which an appropriate closure method has never been documented
thus far [1, 4]. In the current study, we found excellent results with experimental
ACDs in vitro and after 2-week follow-up in vivo. However, after 6 weeks, the
majority of the implants showed signs of migration and deformation. Since the
barb rings should gain adhesion into the layers of the annulus, it is not surprising
that their destruction results in implant extrusion. The ACDs in the goats after 2-
week follow-up showed only mild signs of damage. During these 2 weeks the
goats stayed in the shed of the university animal facilities and were recovering
from the surgeries. In this period, the animals might behave more quiescent than
they usually do. Between the second and sixth week after the surgeries, the goats
are fully recovered. The animals return to the farm and regain their usual
activities. This may result in increasing forces on the implants, and when the
damage to the barb rings accumulates to a certain level, the implants start to
displace. The former agrees with the finding that those implants that were fully
extruded were also the most damaged ones. The damage should have occurred
prior to the moment of extrusion since the implants are located in the soft tissue
directly adjacent to the disc, where no direct mechanical stresses are
encountered.
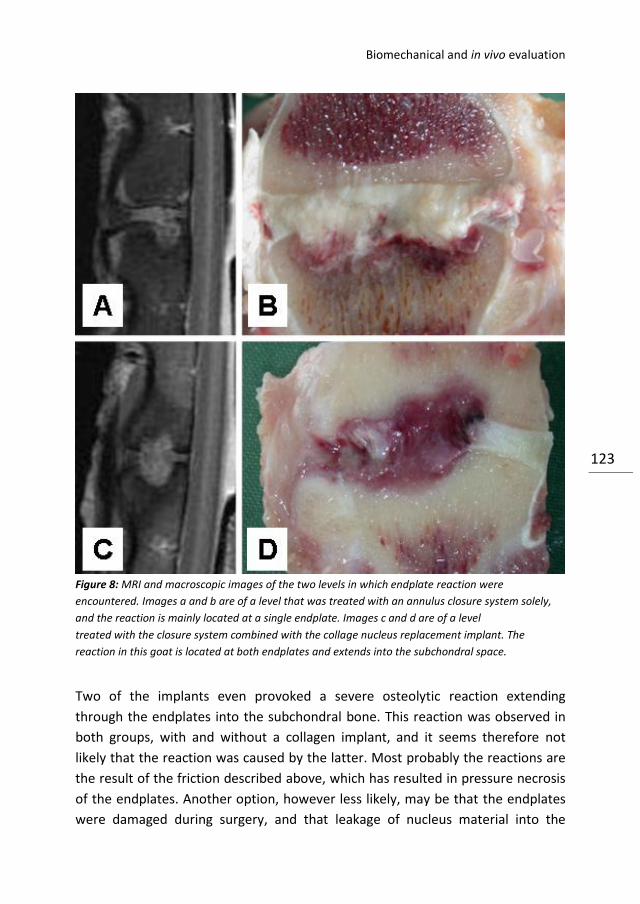
Biomechanical and in vivo evaluation
123
Figure 8: MRI and macroscopic images of the two levels in which endplate reaction were
encountered. Images a and b are of a level that was treated with an annulus closure system solely,
and the reaction is mainly located at a single endplate. Images c and d are of a level
treated with the closure system combined with the collage nucleus replacement implant. The
reaction in this goat is located at both endplates and extends into the subchondral space.
Two of the implants even provoked a severe osteolytic reaction extending
through the endplates into the subchondral bone. This reaction was observed in
both groups, with and without a collagen implant, and it seems therefore not
likely that the reaction was caused by the latter. Most probably the reactions are
the result of the friction described above, which has resulted in pressure necrosis
of the endplates. Another option, however less likely, may be that the endplates
were damaged during surgery, and that leakage of nucleus material into the
Chapter 6
124
subchondral bone provoked the reaction. The potential for nucleus material,
which normally does not encounter immune reactive cells due to the absent
vascularisation in the disc space, to initiate such a reaction has been hypothesised
earlier [2].
To prevent failure and endplate reactions, the design, dimensions and stiffness of
the closing devices can be altered. Current devices were fabricated from
polyethylene, which was used for its known biocompatibility. Polyethylene,
however, is a rather stiff material, and friction between the barb rings and
endplates might therefore have resulted in the observed reaction [18]. Taking a
less stiff material would have decreased the risk, but might probably result in
lower mechanical expulsion strength. The shape of the implants, especially of the
barb rings, deserves attention in further optimisation of the closure devices. We
performed several pilot experiments with different designed devices, but the
current shape showed the highest resistance to forces. We do not know, however,
why implants with four barb rings performed so much better than implants with
five barb rings.
The dimensions of the closure devices can also be adjusted. Intradiscal pressure
results in forces on the implants that are dependent of diameter and length. We
always made a standardised circular defect of 3 mm in the annulus, and the
diameter of the barb rings of the implants was 3.5 mm. The ring diameter was
chosen to promote adherence between the annulus layers. A larger diameter
would have increased this adherence, but would also have resulted in larger
expulsion forces from the pressurised NP and subsequent failure at lower axial
compression forces. The expulsion forces on the ACD depend on its cross-
sectional diameter, whereas the friction forces only depend on the circumference.
In addition, regarding the disc height of the goat (4–5 mm), a larger diameter
could also result in continuous contact between the implant and both endplates,
increasing the risk of adverse reactions and ring damage.
Although current biomechanical study results did not show a significant effect on
latero-flexion, a tendency towards some small restriction could already be
observed. Decreasing the diameter of both the defect and barb rings might
therefore have been preferred from a mechanical viewpoint and from the aim to
Biomechanical and in vivo evaluation
125
reduce contact with the endplate. Unfortunately, this was currently not possible
regarding the diameter of the nucleus implants. The length of the ACDs was
maximally 15 mm (between front of the first and the back of the last barb ring),
and this length was chosen since it always covers the whole lateral annulus. For
some goats, however, a smaller length would have been sufficient, but this can
only be judged afterwards at macroscopic evaluation. If current closure systems
would have passed the animal experiments, a decrease of the lengths to allow
more space for the nucleus replacements could have been evaluated.
The main goal of the biomechanical experiments was to predict failures of the
ACDs. We did not study torsion since the forces would be mainly distributed
through the facet joints with only a marginal increase of the intradiscal pressure
[21]. We found an axial load of 600 N to correspond to an intradiscal pressure of
approximately 3 MPa. The applied load will be partially distributed through the
annulus parts of the discs and/or posterior elements. We performed these
experiments to allow comparison of the forces known from pressure
measurements in vivo. A few studies have been performed measuring the
pressure inside the human intervertebral disc in vivo [16, 17]. Wilke et al. [25]
found a maximum intradiscal pressure of 2.3 MPa during the lifting of 20 kg
combined with flexion–extension forward. From our own in vivo measurements in
goats we know that the axial load can rise up to 900 N [9]. According to current
pressure measurements, this would correspond to a pressure over 4 MPa. Thus,
the peak pressure inside the goat intervertebral disc seems to be higher than the
peak pressure inside the human disc. This finding agrees with the fact that the
bone density of the vertebra of goats is higher compared to humans, indicating
higher stresses in vivo [23]. The differences might be explained by the fact that
the forces on the goat spine are generated by muscles and ligaments surrounding
the continuously bended spine. In the bipedal situation of humans, these
compressive forces are lower and more dependent on activity and posture [14].
Furthermore, we used motion segments derived from young goats (age 4 years),
and the osmotic pressure might therefore be higher compared to the adult
human disc [22]. The goat model was used, since prior studies have shown that
the absolute spinal forces in this animal are still comparable to that of humans
[12, 23]. The mean value of axial load of 4,000 N, which we found that the current
annulus closure system could withstand, provides a sufficient safety range. A
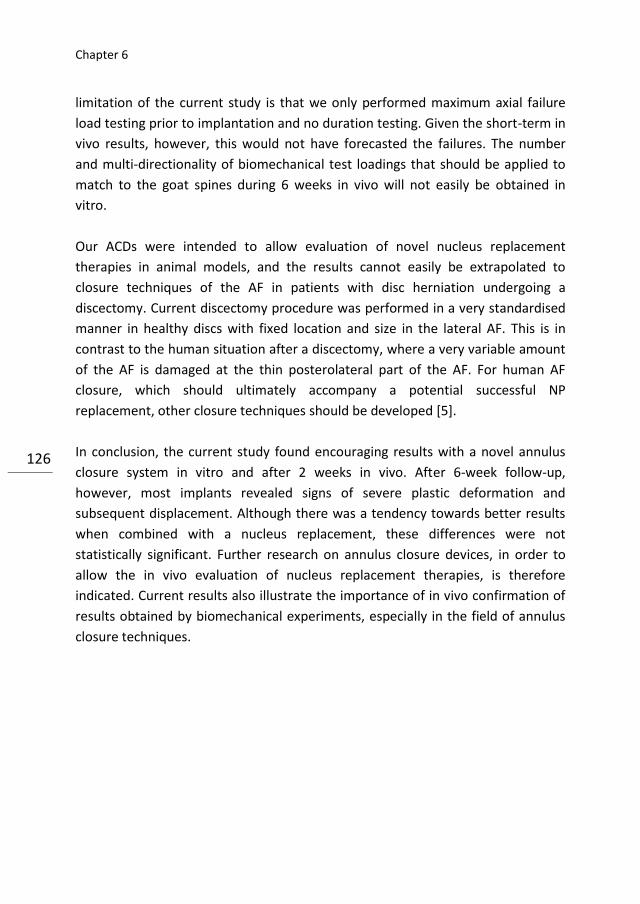
Chapter 6
126
limitation of the current study is that we only performed maximum axial failure
load testing prior to implantation and no duration testing. Given the short-term in
vivo results, however, this would not have forecasted the failures. The number
and multi-directionality of biomechanical test loadings that should be applied to
match to the goat spines during 6 weeks in vivo will not easily be obtained in
vitro.
Our ACDs were intended to allow evaluation of novel nucleus replacement
therapies in animal models, and the results cannot easily be extrapolated to
closure techniques of the AF in patients with disc herniation undergoing a
discectomy. Current discectomy procedure was performed in a very standardised
manner in healthy discs with fixed location and size in the lateral AF. This is in
contrast to the human situation after a discectomy, where a very variable amount
of the AF is damaged at the thin posterolateral part of the AF. For human AF
closure, which should ultimately accompany a potential successful NP
replacement, other closure techniques should be developed [5].
In conclusion, the current study found encouraging results with a novel annulus
closure system in vitro and after 2 weeks in vivo. After 6-week follow-up,
however, most implants revealed signs of severe plastic deformation and
subsequent displacement. Although there was a tendency towards better results
when combined with a nucleus replacement, these differences were not
statistically significant. Further research on annulus closure devices, in order to
allow the in vivo evaluation of nucleus replacement therapies, is therefore
indicated. Current results also illustrate the importance of in vivo confirmation of
results obtained by biomechanical experiments, especially in the field of annulus
closure techniques.
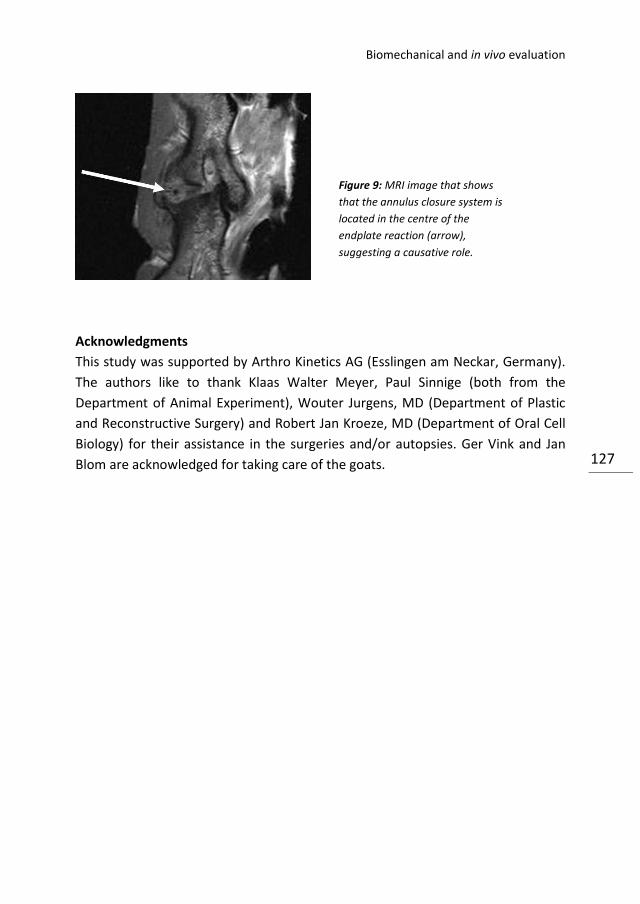
Biomechanical and in vivo evaluation
127
Acknowledgments
This study was supported by Arthro Kinetics AG (Esslingen am Neckar, Germany).
The authors like to thank Klaas Walter Meyer, Paul Sinnige (both from the
Department of Animal Experiment), Wouter Jurgens, MD (Department of Plastic
and Reconstructive Surgery) and Robert Jan Kroeze, MD (Department of Oral Cell
Biology) for their assistance in the surgeries and/or autopsies. Ger Vink and Jan
Blom are acknowledged for taking care of the goats.
Figure 9: MRI image that shows
that the annulus closure system is
located in the centre of the
endplate reaction (arrow),
suggesting a causative role.
Chapter 6
128
References
1. Ahlgren BD, Lui W, Herkowitz HN, Panjabi MM, Guiboux JP (2000) Effect of anular repair
on the healing strength of the intervertebral disc: a sheep model. Spine 25(17):2165–2170
2. Albert HB, Kjaer P, Jensen TS et al (2008) Modic changes, possible causes and relation to
low back pain. Med Hypotheses 70(2):361–368
3. Bajanes G, Perez A, Diaz M (2007) One year follow up of discectomy patients who
received a mesh to repair the annulus fibrosus, vol 7. Spine Arthroplasty Society, Berlin
4. Bourgeault C, Beaubien B, Griffith S (2007) Biomechanical assessment of annulus
fibrosus repair with suture tethered anchors, vol 7. Spine Arthroplasty Society, Berlin
5. Bron JL, Helder MN, Meisel HJ, van Royen BJ, Smit TH (2009) Repair, regenerative and
supportive therapies of the annulus fibrosus: achievements and challenges. Eur Spine J
18(3):301–313
6. Bron JL, Koenderink GH, Everts V, Smit TH (2009) Rheological characterization of the
nucleus pulposus and dense collagen scaffolds intended for functional replacement. J
Orthop Res 27(5):620–626
7. Carragee EJ, Han MY, Suen PW, Kim D (2003) Clinical outcomes after lumbar discectomy
for sciatica: the effects of fragment type and anular competence. J Bone Joint Surg Am 85-
A(1):102–108
8. Choy DS (2000) Familial incidence of intervertebral disc herniation: an hypothesis
suggesting that laminectomy and discectomy may be counterproductive. J Clin Laser Med
Surg 18(1):29–32
9. Dormans KW, Krijnen MR, Geertsen S, van Essen GJ, Wuisman PI, Smit TH (2004)
Telemetric strain measurements in an interbody fusion cage: a pilot goat study. In:
Proceedings of the 14th European Society of Biomechanics (ESB) conference. ’s-
Hertogenbosch, Netherlands, p 224
10. Hansson E, Hansson T (2007) The cost-utility of lumbar disc herniation surgery. Eur
Spine J 16(3):329–337
11. Hegewald AA, Ringe J, Sittinger M, Thome C (2008) Regenerative treatment strategies
in spinal surgery. Front Biosci 13:1507– 1525
12. Heuer F, Ulrich S, Claes L, Wilke HJ (2008) Biomechanical evaluation of conventional
anulus fibrosus closure methods required for nucleus replacement. Laboratory
investigation.
J Neurosurg Spine 9(3):307–313
13. Kamaric E, Gorensek M, Vilendecic M, Eustacchio S, Trummer M, Eskinja N, Ledic D,
Yeh O, Einhorn J, Lambrecht G (2006) Surgical factors affecting reherniation rate after
lumbar microdiscectomy: effect of defect size and amount of disc removed. Spine J 6(5
Suppl 1):38S
14. Ledet EH, Tymeson MP, DiRisio DJ, Cohen B, Uhl RL (2005) Direct real-time
measurement of in vivo forces in the lumbar spine. Spine J 5(1):85–94
Biomechanical and in vivo evaluation
129
15. Melrose J, Smith SM, Little CB et al (2008) Recent advances in annular pathobiology
provide insights into rim-lesion mediated intervertebral disc degeneration and potential
new approaches to annular repair strategies. Eur Spine J 17(9):1131–1148
16. Nachemson A (1965) The effect of forwards leaning on lumbar intradiscal pressure.
Acta Orthop Scand 35:314–328
17. Nachemson A, Morris JM (1964) In vivo measurements of intradiscal pressure.
Discometry, a method for the determination of pressure in the lower lumbar discs. J Bone
Joint Surg Am 46:1077–1092
18. Ries MD, Pruitt L (2005) Effect of cross-linking on the microstructure and mechanical
properties of ultra-high molecular weight polyethylene. Clin Orthop Relat Res 440:149–
156
19. Sebastine IM, Williams DJ (2007) Current developments in tissue engineering of
nucleus pulposus for the treatment of intervertebral disc degeneration. Conf Proc IEEE Eng
Med Biol Soc 1:6400–6405
20. Sherman J, Cauthen J, Griffith S (2007) Pre-clinical evaluation of a mesh device for
repairing the annulus fibrosus. Spine Arthroplasty society, Berlin
21. Shirazi-Adl A, Ahmed AM, Shrivastava SC (1986) Mechanical response of a lumbar
motion segment in axial torque alone and combined with compression. Spine 11(9):914–
927
22. Sivan S, Merkher Y, Wachtel E, Ehrlich S, Maroudas A (2006) Correlation of swelling
pressure and intrafibrillar water in young and aged human intervertebral discs. J Orthop
Res 24(6):1292–1298
23. Smit TH (2002) The use of a quadruped as an in vivo model for the study of the spine—
biomechanical considerations. Eur Spine J 11(2):137–144
24. Wilke HJ, Heuer F, Neidlinger-Wilke C, Claes L (2006) Is a collagen scaffold for a tissue
engineered nucleus replacement capable of restoring disc height and stability in an animal
model? Eur Spine J 15(Suppl 3):S433–S438
25. Wilke HJ, Neef P, Caimi M, Hoogland T, Claes LE (1999) New in vivo measurements of
pressures in the intervertebral disc in daily life. Spine 24(8):755–762
26. Yeung AT, Yeung CA (2007) Minimally invasive techniques for the management of
lumbar disc herniation. Orthop Clin North Am 38(3):363–372
Chapter 6
130

Addendum 1
Techniques and instruments

Addendum 1
132
Development of the model and instruments
All instruments were developed to be used via for minimal invasive surgery of the
goat lumbar spine. According to known anatomical dimensions of the goat IVD, a
real sized Perspex model of the goat IVD was made (Fig 1A). Since a lateral
surgical approach of the spine was intended, the IVD model has a hole at one side
laterally (Fig 2B). The model was used as a guide for further development of the
instruments. The first instrument is a guide wire designed to puncture the lateral
side of the IVD (Fig 2A, left). Position of the tip of the guide wire can be monitored
using the C-arm during surgery. Next, is a series of tubes with ascending diameter
that can be introduced over the guide wire to gradually increase the size of the AF
defect (Fig 2). The largest tube has an inner diameter of 2.6 mm en outer
diameter of 3 mm. After this last tube is introduced into the IVD, the guide wire
and other tubes are removed. All other instruments and implants are designed to
fit through this largest tube.
The next step is to evacuate to NP. The rongeurs and other instruments are shown
in figure 3. After the NP is evacuated, the NP replacement material can be
introduced through the tube. For the in vivo study, the NP space was filled with a
highly dense collagen scaffold, which was also shaped to fit through the tube
(length 50 mm, volume ~0.27 cm3) (Fig 4). The preparation and characteristics of
this collagen matrix (NuRes, Arthro Kinetics AG, Esslingen, Germany) has been
described in chapter 2 [5]. The chosen density was 25 % w/w of collagen, which
has a stiffness comparable to the native NP [5]. Finally, the size of the AF defect,
which was consistent with the outer size of the largest tube, was filled with a
custom made annulus closure device that has been described in chapter 6 (Fig 5)
[6]. Unfortunately, the ACD could not be introduced through the tube and was
inserted immediately after removal of the tube. All implants had been sterilized
before by γ-irradiation.

Techniques and instruments
133
A B Figure 1: Real size Perspex model of the goat IVD used for the development of the NP replacement
model. The Perspex model has a hole at one size laterally (B), which is consistent with place of the AF
defect using the posterolateral surgical approach.
A B Figure 2: shows the instruments intended to make a standardized defect in the AF. At the left (A) is a
guide wire used to make the initial defect in the AF. Then, the tubes are inserted over the wire (B) to
gradually increase the size of the defect. The largest tube has an outer diameter of 3 mm.
A B Figure 3: Instruments used for evacuation of native NP tissue (A). The instruments are designed to fit
through the largest tube (B).

Addendum 1
134
Figure 4: Images showing how the collagen implant is inserted into the Perspex model via the largest
tube. The collagen implant is delivered in a similar tube as the tube in the AF and is connected to the
back of the latter (A). A stamp is used to push the collagen from the tube into the disc space (B,C). In
image D shows the full implant (50 mm) inside the Perspex model.
Figure 5: The ACD’s that used to
close the defect in the AF after the
collagen implant is inserted.

Techniques and instruments
135
In current addendum we described the development of a NP replacement model
in order to evaluate scaffold materials via minimal invasive surgery in goats. The
model and instruments were tested in a pilot study in vivo using high density
collagen implants to replace the NP. Although the model was designed to be used
for minimal invasive surgery, an open approach was used for the pilot study. The
open approach allowed visualization of the AF defect, ascertained correct
insertion of the collagen implant and excluded the learning curve necessary for
minimal invasive spinal surgery. Furthermore, the ACD’s could not be inserted via
the same tube used for NP evacuation and the collagen implant, which is only one
among several limitations of the devices (see chapter 6). Overall, the standardized
NP replacement model turned out to be feasible in vivo. Clinically, the surgeries
were well tolerated by the animals and no complications were observed.
Addendum 1
136
Addendum 2
Nucleus implant evaluation
Addendum 2
138
Introduction
In chapter 6 an in vivo goat study was presented to evaluate annulus closure
devices (ACD’s). In this study a collagen nucleus implant was inserted in addition
to an ACD at one level in every of the ten goats. Since chapter 6 was mainly
directed to the development of a suitable ACD, no evaluation of the collagen
implants was performed. Although the number of animals and the short term
follow up in this study will not allow any firm conclusions on the collagen, it is the
first large animal nucleus replacement in vivo study reported till date in literature.
In this second addendum to chapter 6 we therefore perform an analysis of the
results of the collagen scaffolds that were implanted in addition to the ACD’s. The
addendum includes histologic and radiological (disc height index and MRI) analysis
of the levels treated with a collagen implant. As described in chapter 6, 2 of the
goats were terminated after 2 weeks and 8 goats after 6 weeks of follow-up.
Methods
Histology
Intervertebral discs were sectioned in 3 mm slices using a band saw (Exakt,
Norderstedt, Germany). Digital photographs of all paramidsagittal slices were
taken. Before further processing, slices were carefully inspected for the presence
of dense collagen, any tissue reaction, and for the position of the ACD. One
paramidsagittal slice was fixed in 10% neutral buffered formalin, decalcified,
paraffin-embedded, sectioned to 7 μm section and stained with haematoxylin and
eosin (H&E). Alcian Blue- Periodic Acid Schiff (AB-PAS) staining was performed on
adjacent sections. The pH of the AB used for the staining was 1.0. All sections
were screened for the presence of dense collagen and tissue reactions. Also, the
number of cells was counted and averaged in 5 randomly selected fields of view
(magnification x 20) of the NP of each disc.
IVD height measurements
Before and after each surgery and before autopsy, standardized lateral lumbar
radiographs were made. The X-rays were analysed digitally using image analysis
software (Centricity Radiology Web, GE Medical Systems, Milwaukee, WI, U.S.A.).
The Disc Height Index (DHI) was calculated by dividing the average IVD height by
the average adjacent caudal vertebral body height, as described previously [11,

Nucleus implant evaluation
139
13, 17]. DHI measurements were performed by two scorers (JB & Remco Sonnega)
on two separate occasions.
Magnetic Resonance Imaging
After harvesting the lumbar spines, MRI scans were made using a 1.5 Tesla clinical
imager (Symphony Quantum, Siemens AG Medical Solutions, Erlangen, Germany).
Sagittal sections were made using a T2-weighted spin echo sequence, a turbo
factor 5 and a spine array coil (time to repetition (TR): 3000msec., time to echo
(TE): 85 msec., field of view 200, matrix of 118x384, and a slice thickness of 3 mm
with a 10% gap).
Statistics
To calculate differences between different implant groups, Student’s unpaired T-
test was used.
Results
Macroscopic and histological evaluation
Macroscopy revealed that the dense collagen was still present in the IVD space,
but not yet integrated in the NP tissue after 6 weeks (Figure 1). This resulted in
the loss of the collagen material during sawing and processing for histology.
Microscopic screening of the coupes for the presence of the collagen scaffold did
not reveal any remnants. As in all experimental segments in this study the NP had
been removed, the macroscopic and microscopic grading scores that have been
developed for disc degeneration do not apply. All treated levels revealed
unilateral damage to the AF (Fig 2a) and damage to the NP due to the discectomy
(Fig 2b & d), compared to the control levels (Fig 2d). Two segments with adverse
reactions were observed (Fig 3 & 4). The first reaction was at level treated with an
ACD alone (Fig 3). The macroscopic picture of this IVD shows destruction of the
upper endplate and the formation of an osteophyte at the side of the ACD (Fig
3a). The ACD itself is destructed and dislocated. HE staining of the endplate
confirms the destruction and the invasion inflammatory cells reveals an extensive
immunological reaction (Fig 3b). The other adverse reaction is observed in a level
treated with a collagen implant and an ACD (Fig 4). Here the destruction involves
the NP, both endplates and the AF at the ACD side (Fig 4a). AB-PAS staining of the
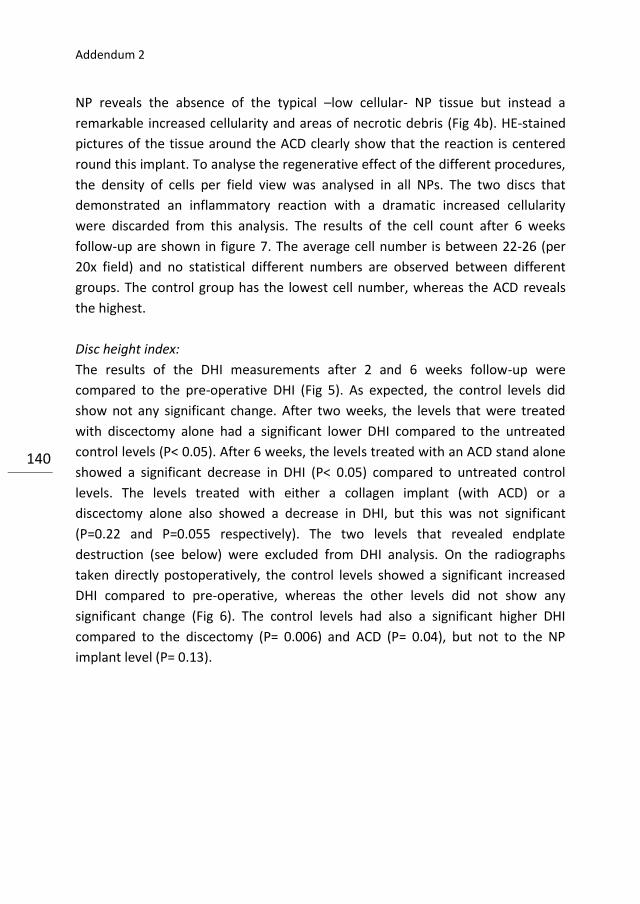
Addendum 2
140
NP reveals the absence of the typical –low cellular- NP tissue but instead a
remarkable increased cellularity and areas of necrotic debris (Fig 4b). HE-stained
pictures of the tissue around the ACD clearly show that the reaction is centered
round this implant. To analyse the regenerative effect of the different procedures,
the density of cells per field view was analysed in all NPs. The two discs that
demonstrated an inflammatory reaction with a dramatic increased cellularity
were discarded from this analysis. The results of the cell count after 6 weeks
follow-up are shown in figure 7. The average cell number is between 22-26 (per
20x field) and no statistical different numbers are observed between different
groups. The control group has the lowest cell number, whereas the ACD reveals
the highest.
Disc height index:
The results of the DHI measurements after 2 and 6 weeks follow-up were
compared to the pre-operative DHI (Fig 5). As expected, the control levels did
show not any significant change. After two weeks, the levels that were treated
with discectomy alone had a significant lower DHI compared to the untreated
control levels (P< 0.05). After 6 weeks, the levels treated with an ACD stand alone
showed a significant decrease in DHI (P< 0.05) compared to untreated control
levels. The levels treated with either a collagen implant (with ACD) or a
discectomy alone also showed a decrease in DHI, but this was not significant
(P=0.22 and P=0.055 respectively). The two levels that revealed endplate
destruction (see below) were excluded from DHI analysis. On the radiographs
taken directly postoperatively, the control levels showed a significant increased
DHI compared to pre-operative, whereas the other levels did not show any
significant change (Fig 6). The control levels had also a significant higher DHI
compared to the discectomy (P= 0.006) and ACD (P= 0.04), but not to the NP
implant level (P= 0.13).
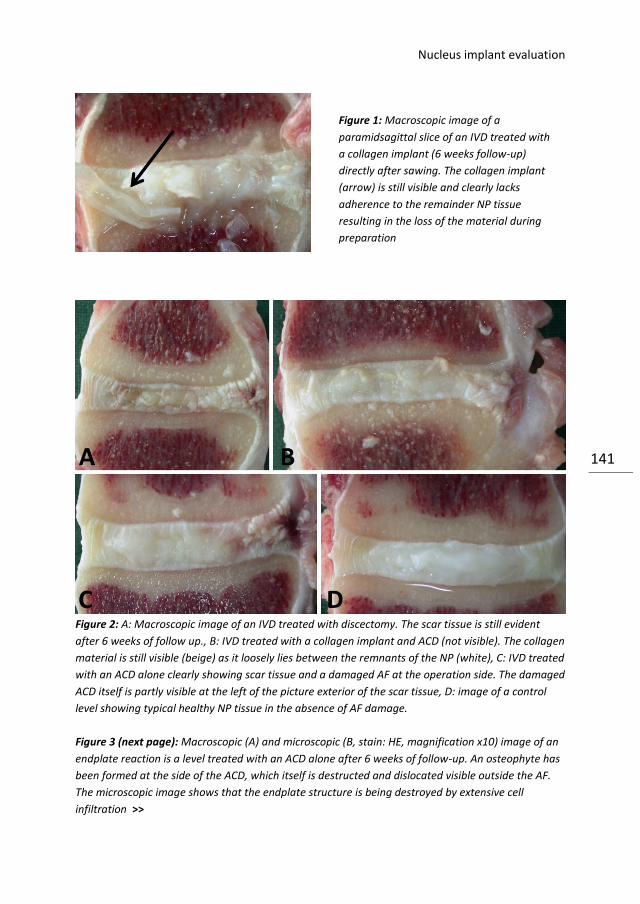
Nucleus implant evaluation
141
Figure 2: A: Macroscopic image of an IVD treated with discectomy. The scar tissue is still evident
after 6 weeks of follow up., B: IVD treated with a collagen implant and ACD (not visible). The collagen
material is still visible (beige) as it loosely lies between the remnants of the NP (white), C: IVD treated
with an ACD alone clearly showing scar tissue and a damaged AF at the operation side. The damaged
ACD itself is partly visible at the left of the picture exterior of the scar tissue, D: image of a control
level showing typical healthy NP tissue in the absence of AF damage.
Figure 3 (next page): Macroscopic (A) and microscopic (B, stain: HE, magnification x10) image of an
endplate reaction is a level treated with an ACD alone after 6 weeks of follow-up. An osteophyte has
been formed at the side of the ACD, which itself is destructed and dislocated visible outside the AF.
The microscopic image shows that the endplate structure is being destroyed by extensive cell
infiltration >>
Figure 1: Macroscopic image of a
paramidsagittal slice of an IVD treated with
a collagen implant (6 weeks follow-up)
directly after sawing. The collagen implant
(arrow) is still visible and clearly lacks
adherence to the remainder NP tissue
resulting in the loss of the material during
preparation
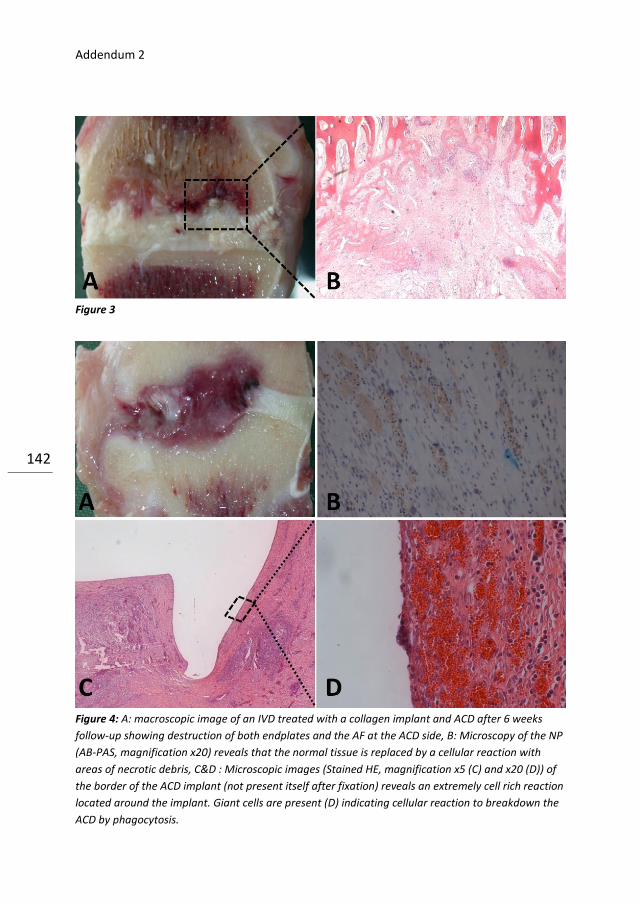
Addendum 2
142
Figure 3
Figure 4: A: macroscopic image of an IVD treated with a collagen implant and ACD after 6 weeks
follow-up showing destruction of both endplates and the AF at the ACD side, B: Microscopy of the NP
(AB-PAS, magnification x20) reveals that the normal tissue is replaced by a cellular reaction with
areas of necrotic debris, C&D : Microscopic images (Stained HE, magnification x5 (C) and x20 (D)) of
the border of the ACD implant (not present itself after fixation) reveals an extremely cell rich reaction
located around the implant. Giant cells are present (D) indicating cellular reaction to breakdown the
ACD by phagocytosis.
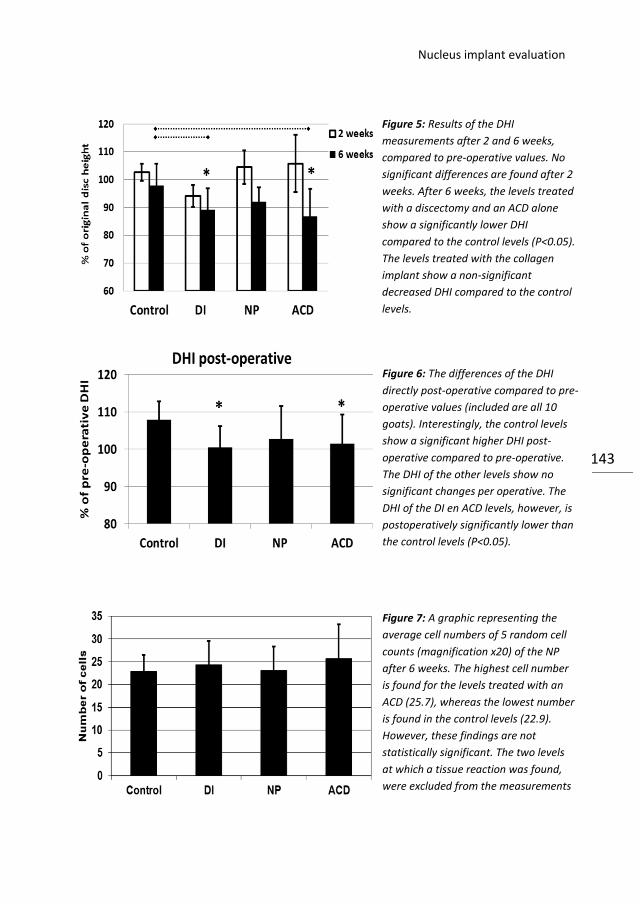
Nucleus implant evaluation
143
Figure 5: Results of the DHI
measurements after 2 and 6 weeks,
compared to pre-operative values. No
significant differences are found after 2
weeks. After 6 weeks, the levels treated
with a discectomy and an ACD alone
show a significantly lower DHI
compared to the control levels (P<0.05).
The levels treated with the collagen
implant show a non-significant
decreased DHI compared to the control
levels.
Figure 6: The differences of the DHI
directly post-operative compared to pre-
operative values (included are all 10
goats). Interestingly, the control levels
show a significant higher DHI post-
operative compared to pre-operative.
The DHI of the other levels show no
significant changes per operative. The
DHI of the DI en ACD levels, however, is
postoperatively significantly lower than
the control levels (P<0.05).
Figure 7: A graphic representing the
average cell numbers of 5 random cell
counts (magnification x20) of the NP
after 6 weeks. The highest cell number
is found for the levels treated with an
ACD (25.7), whereas the lowest number
is found in the control levels (22.9).
However, these findings are not
statistically significant. The two levels
at which a tissue reaction was found,
were excluded from the measurements

Addendum 2
144
MR Imaging:
MRI images of all levels in all goats after 6 weeks are shown in Figure 8. The
collagen implants are not visible on the MRI. Two segments showed an adverse
reaction: level one segment treated with an ACD alone the lower endplate is
involved and in a segment treated with an NP both endplates show extensive
destruction. Besides the two reactions described above, MR images do not reveal
any major differences between the treatments.
Figure 8: Sagittal MR images of all levels after 6 weeks follow-up. The first image of the ACD series
and the sixth image of the NP implant series reveal a tissue reaction. The first case only one endplate
is destructed, whereas both endplate are involved the latter.
Discussion
Macroscopic evaluation of the IVD’s revealed that the dense collagen was not yet
integrated in the matrix of the NP (Fig 1). Collagen breakdown in the IVD is
dependent on the remodeling and turnover capacity of the native cells. Since the
number of natives cells in NP tissue is low and cell turnover only slow [21], this
capacity is limited. [7]. The breakdown of collagen can be dramatically increased
under certain circumstances including inflammation and malignancy [7]. Currently
we did not observe an increase in the number of NP cells in the
Nucleus implant evaluation
145
IVD’s treated with collagen (Fig 4), thus excluding major inflammation. The high
density of the collagen (25% w/w), achieved by plastic compression, has a
stiffness comparable to native NP tissue [5] but also results in a further decreased
remodeling speed due to the restricted cell invasion and migration (chapter 4).
The DHI of the discected IVD’s could be preserved by implantation of a DCS
compared to untreated control levels after 6 weeks (Fig 5). The levels treated with
a discectomy or ACD alone showed a significant decrease in DHI. This suggests
that the collagen implant is capable of restoring local resistance to hydrostatic
and compressive forces. Of course, this greatly depends on containment capacity
of the ACD’s that is used. Current ACD’s were already described to be suboptimal
(only sufficient at in 2 out of 8 goats at 2 levels, partially sufficient[6] at 5 levels
and insufficient[6] at 1 level). The (untreated) control levels showed a significant
higher DHI directly post-operative compared to pre-operative. These differences
may be due to the decreased hydrostatic pressure in the IVD’s during surgery due
to the administration of muscle relaxants and lying position. In contrast to the
ACD and discectomy levels, the IVD’s treated with the collagen implants did not
show a significant difference in DHI directly post-operative compared to the
control levels. In the first pilot study we showed that the ACD’s do perform well in
containing the collagen implants during the first two weeks (see also: [6]). The
latter may be the reason that the levels with NP implant the pressure is (partly)
restored directly post-operatively. Unsterilized dense collagen has the capacity to
absorb water from the surrounding tissues resulting in swelling of the scaffolds.
Current scaffolds, however, were sterilized by γ-irradiation and this results in an
increase in the number of cross links and chain scission in the collagen matrix,
both blocking the swelling potential [5]. From a practical point of view the latter is
unfortunate, since the swelling capacity could have attributed to the hydrostatic
pressure.
Several radiological and histological grading systems for grading disc degeneration
have been proposed [11, 13, 18, 24]. These grading systems however, have very
limited value for a NP replacement model. For example, MRI grading systems rely
on the signal intensity of the NP on T2-weighted images, reflecting water content.
The healthy NP is a proteoglycan-rich matrix with a high capacity to retain water.
Degeneration results in a reduction inproteoglycan content within the NP, with a
Addendum 2
146
subsequent reduction in water content. These changes facilitate a MRI based
classification system [18]. In the current study however, the NP tissue was
replaced by a dense collagen scaffold, which has a much lower water content
compared to the proteoglycan-rich NP matrix. Perhaps MRI based grading could
become useful for longer follow-up periods, when the collagen becomes replaced
by native NP tissue. Currently, the DHI measured on plain lateral radiographs
turned out to be more useful, but MRI did show its suitability in revealing the two
tissue reactions. Also histological grading systems proved not useful in this study.
These score systems use the NP, AF and endplates to grade degeneration [24]. In
the current study the NP and AF were both damaged by the discectomy, always
resulting in low scores. The endplates did not reveal abnormalities, except the two
levels with adverse reactions on the ACD. Again these grading systems could gain
some relevance during longer follow-up when treated levels will regenerate or
otherwise progress to extensive degeneration with subsequent changes.
We did measure the cell number in the NP tissue, which was not statistically
different between the various groups. Degeneration is accompanied by decreased
cellularity, whereas inflammatory responses on the implanted material would be
associated with increased cellularity. Both however, were not observed. The cell
numbers that were found (20-25 cells/field, Fig 7) are comparable to earlier
observations (average 17.1) at our department (Hoogendoorn et al, data
submitted).
In conclusion, although the dense collagen scaffolds showed to preserve disc
height till six weeks after discectomy, the results were negatively influenced by
insufficient annulus closure and the lack of appropriate scoring systems. Before
the model can be used for studies with longer follow up periods or other
scaffolds, optimization of the ACD and the development of grading systems
designed for NP replacement are crucial.
Acknowledgment
The authors like to than Remko Sonnega, MD for his attributions to the disch
height measurements.

Nucleus implant evaluation
147
References to the addenda
1. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE (2005) Long-term outcomes of surgical
and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the
maine lumbar spine study. Spine 30(8):936-943.
2. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE (2005) Long-term outcomes of surgical
and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year
results from the maine lumbar spine study. Spine 30(8):927- 935.
3. Battie MC, Videman T (2006) Lumbar disc degeneration: epidemiology and genetics. J
Bone Joint Surg Am 88 Suppl 2:3-9.
4. Bron JL, Helder MN, Meisel HJ, van Royen BJ, Smit TH (2009) Repair, regenerative and
supportive therapies of the annulus fibrosus: achievements and challenges. Eur Spine J
18(3):301-313.
5. Bron JL, Koenderink GH, Everts V, Smit TH (2008) Rheological characterization of the
nucleus pulposus and dense collagen scaffolds intended for functional replacement. J
Orthop Res.
6. Bron JL, van der Veen AJ, Helder MN, van Royen BJ, Smit TH (2010) Biomechanical and
in vivo evaluation of experimental closure devices of the annulus fibrosus designed for a
goat nucleus replacement model. Eur Spine J 19(8):1347-1355.
7. Everts V, van der ZE, Creemers L, Beertsen W (1996) Phagocytosis and intracellular
digestion of collagen, its role in turnover and remodelling. Histochem J 28(4):229-245.
8. Ganey T, Libera J, Moos V et al. (2003) Disc chondrocyte transplantation in a canine
model: a treatment for degenerated or damaged intervertebral disc. Spine 28(23):2609-
2620.
9. Haugen AJ, Grovle L, Brox JI et al. (2011) Estimates of success in patients with sciatica
due to lumbar disc herniation depend upon outcome measure. Eur Spine J.
10. Hegewald AA, Ringe J, Sittinger M, Thome C (2008) Regenerative treatment strategies
in spinal surgery. Front Biosci 13:1507-1525.
11. Hoogendoorn RJ, Helder MN, Kroeze RJ et al. (2008) Reproducible long-term disc
degeneration in a large animal model. Spine (Phila Pa 1976 ) 33(9):949-954.
12. Hoogendoorn RJ, Lu ZF, Kroeze RJ et al. (2008) Adipose stem cells for intervertebral
disc regeneration: current status and concepts for the future. J Cell Mol Med 12(6A):2205-
2216.
13. Hoogendoorn RJ, Wuisman PI, Smit TH, Everts VE, Helder MN (2007) Experimental
intervertebral disc degeneration induced by chondroitinase ABC in the goat. Spine (Phila
Pa 1976 ) 32(17):1816-1825.
14. Humzah MD, Soames RW (1988) Human intervertebral disc: structure and function.
Anat Rec 220(4):337-356.
15. Katz JN (2006) Lumbar disc disorders and low-back pain: socioeconomic factors and
consequences. J Bone Joint Surg Am 88 Suppl 2:21-24.

Addendum 2
148
16. Kim JM, Lee SH, Ahn Y et al. (2007) Recurrence after successful percutaneous
endoscopic lumbar discectomy. Minim Invasive Neurosurg 50(2):82-85.
17. Lu DS, Shono Y, Oda I, Abumi K, Kaneda K (1997) Effects of chondroitinase ABC and
chymopapain on spinal motion segment biomechanics. An in vivo biomechanical,
radiologic, and histologic canine study. Spine (Phila Pa 1976 ) 22(16):1828-1834.
18. Masuda K, Aota Y, Muehleman C et al. (2005) A novel rabbit model of mild,
reproducible disc degeneration by an anulus needle puncture: correlation between the
degree of disc injury and radiological and histological appearances of disc degeneration.
Spine (Phila Pa 1976 ) 30(1):5-14.
19. Nellensteijn J, Ostelo R, Bartels R et al. (2010) Transforaminal endoscopic surgery for
symptomatic lumbar disc herniations: a systematic review of the literature. Eur Spine J
19(2):181-204.
20. Postacchini F, Postacchini R (2011) Operative management of lumbar disc herniation :
the evolution of knowledge and surgical techniques in the last century. Acta Neurochir
Suppl 108:17-21.
21. Risbud MV, Schipani E, Shapiro IM (2010) Hypoxic regulation of nucleus pulposus cell
survival: from niche to notch. Am J Pathol 176(4):1577-1583.
22. Suk KS, Lee HM, Moon SH, Kim NH (2001) Recurrent lumbar disc herniation: results of
operative management. Spine 26(6):672-676.
23. Swartz KR, Trost GR (2003) Recurrent lumbar disc herniation. Neurosurg Focus
15(3):E10.
24. Thompson JP, Pearce RH, Schechter MT et al. (1990) Preliminary evaluation of a
scheme for grading the gross morphology of the human intervertebral disc. Spine (Phila Pa
1976 ) 15(5):411-415.
25. Yeung AT, Yeung CA (2007) Minimally invasive techniques for the management
of lumbar disc herniation. Orthop Clin North Am 38(3):363-372.
7 General Discussion

Chapter 7
150
Disc herniation
Low back pain (LBP) is a leading cause of disability in our population, affecting
most people at some point in life. Chronic LBP decreases quality of life and has
significant socio-economic consequences due to absenteeism from work and
increased medical consumption [37]. LBP is a multifactorial condition in which
muscular, psychological and socioeconomic factors act in concert. Intervertebral
disc (IVD) degeneration is also a strong etiological factor, but the exact
contribution is still unclear since imaging modalities often do not correlate with
symptomatology [6]. IVD degeneration is a complex disease, in which changes to
certain extent develop physiologically due to aging, but can become pathologic in
severe degeneration with no clear border inbetween. Due to degeneration,
several structural changes occur in the IVD, most notably the dehydration of the
nucleus pulposus (NP) in association with tears in the annulus fibrosus (AF) and
endplates (Schmorl’s nodes) [6]. Damage to the AF may diminish its capability to
cope with the local stresses and as a result the NP may herniate through the
disrupted AF [6]. Initially, the herniated NP material results in direct mechanical
compression of the nerve roots that are located posterior of the IVD.
Furthermore, in the absence of vascularity the NP is normally an immune
privileged tissue. Herniation of this material provokes an inflammatory response
further adding to the irritation of the nerve roots [35]. Disc herniation occurs in up
to 2% of the general population and these patients can often recall an episode of
(sub)acute LBP in combination with radicular complaints. Whereas the radicular
symptoms will resolve spontaneously in over two-thirds of the patients within 6
weeks, the LBP often persists or even progresses. In contrast to other forms of
disc degeneration that develop in a slow progressive manner, in IVD herniation
there is an acute change in local biomechanics and a disruption of homeostasis.
The loss of intradiscal pressure results in decreased disc height and a diminished
capability of the NP cells to maintain their ECM. The ECM, rich in waterbinding
proteoglycans, is essential for the water maintaining capacity of the IVD. That IVD
cells need a certain hydrostatic pressure to function properly was recently
demonstrated in a clinical study among astronauts. The absence of gravity during
the space flight and subsequent reduced IVD pressure resulted in an increased
incidence of IVD herniation in the period after the flight [18]. If the biomechanical
changes due to herniation are not reversed, progression to advanced stages of
IVD degeneration will usually be inevitable, explaining the persisting LBP in
General discussion
151
patients after an episode of IVD herniation. Moreover, if the local effects of the
IVD herniation are reversed quickly, homeostasis might be restored, however if
treatment is delayed degenerative changes become irreversible. Recently it was
shown that if treatment for IVD herniation is delayed over 6 months, outcomes
are worse following both operative and non-operative treatment [33]. The aim of
this thesis was to develop a tissue engineered strategy to reverse the state after
IVD herniation and to restore local homeostasis. To minimize patient discomfort,
the therapy should ideally be combined with the neurological decompression
surgery. In this thesis, we have translated this strategy into practice, starting with
material design and ending up with the in vivo evaluation in a large animal model.
Tissue engineering
Tissue engineering is generally described as “the use of a combination of cells,
engineering and materials methods, and suitable biochemical and physio-chemical
factors to improve or replace biological functions” [1]. It is also referred to as
“regenerative medicine”, underscoring its relation to and among other medical
disciplines. Tissue engineering has evolved very quickly as an area of research
since the 90s of the past century. Where initial opportunistic research
hypothesized that the injection of stem cells would be sufficient for the
regeneration of virtually every organ or tissue, scientists now slowly learn all
circumstances that are involved [23, 30]. For the herniated intervertebral disc,
numerous regenerative strategies have been studied, however broad clinical
success is still lacking. In the end, this will rely on clinical treatment outcomes and
costs and these will require clinical trials to establish superiority over conventional
treatment standards [24]. Figure 1 shows the development pathway for novel
regenerative therapies. Even when all the steps in the figure have been passed
successfully, commercial success is not guaranteed. Education of the clinicians
with the intention to use tissue engineered products for their patients will be
crucial. This will require scientific experts, parties involved in the
fabrication/development and clinicians to work in concert.
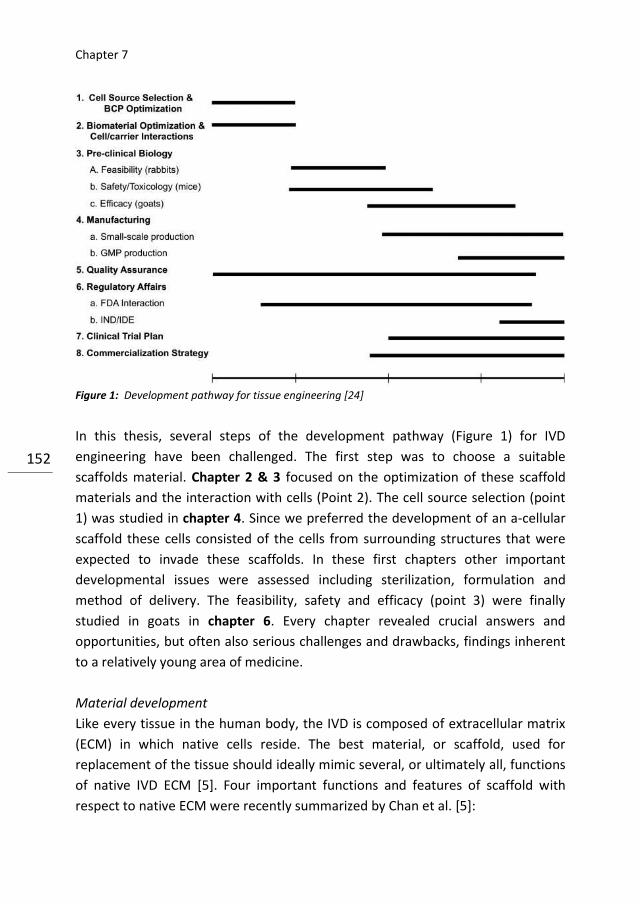
Chapter 7
152
Figure 1: Development pathway for tissue engineering [24]
In this thesis, several steps of the development pathway (Figure 1) for IVD
engineering have been challenged. The first step was to choose a suitable
scaffolds material. Chapter 2 & 3 focused on the optimization of these scaffold
materials and the interaction with cells (Point 2). The cell source selection (point
1) was studied in chapter 4. Since we preferred the development of an a-cellular
scaffold these cells consisted of the cells from surrounding structures that were
expected to invade these scaffolds. In these first chapters other important
developmental issues were assessed including sterilization, formulation and
method of delivery. The feasibility, safety and efficacy (point 3) were finally
studied in goats in chapter 6. Every chapter revealed crucial answers and
opportunities, but often also serious challenges and drawbacks, findings inherent
to a relatively young area of medicine.
Material development
Like every tissue in the human body, the IVD is composed of extracellular matrix
(ECM) in which native cells reside. The best material, or scaffold, used for
replacement of the tissue should ideally mimic several, or ultimately all, functions
of native IVD ECM [5]. Four important functions and features of scaffold with
respect to native ECM were recently summarized by Chan et al. [5]:

General discussion
153
1. Architecture: Scaffolds should provide void volume for vascularization and
remodeling and the rate of degradation should match to the new ECM formation.
2. Cyto-compatibility: The scaffolds should allow (native) cells to attach, grow,
proliferate and differentiate
3. Bioactivity: scaffold may include biological cues to influence cell morphology,
alignment, migration speed and differentiation.
4. Mechanical properties: scaffolds should provide mechanical and shape stability
of a tissue defect. Interestingly the mechanical properties of a scaffold are also
known to influence the biosynthetic cell response and thus act as a passive cue.
At this moment, these material demands are principally qualitative and
quantification is highly desirable with respect to material development. Numerous
(bio)polymers and materials have been suggested as a suitable candidate for IVD
engineering including collagen, alginate, gelatin, chitosan, poly-L-lactic acid and
hyaluronan [5]. All of the materials have their advantages and disadvantages and
the optimal material, fulfilling al the desired functions, will probably yet have to
be invented. Beside the desired functions described above other concerns are
involved in choosing the optimal scaffold, these involve availability, costs and
handling [4]. The NP itself exists of Type II collagen, proteoglycans and small
fractions of several other (glyco)proteins including elastin, fibronectin, laminins
and tenasins [6]. It is not possible to remake the tissue in vitro, and attempts to
overcome this problem have proposed. Mercuri et al. for example, harvested
porcine NP’s which were completely decellularized using a combination of
chemical detergents, before the scaffolds were repopulated with human adipose-
derived stem cells [25]. Although their results seem promising the technique is
very laborious and time consuming and not necessary since the aim of tissue
engineering is to shape the optimal environment in which cells are able to
synthesize and maintain the desired ECM [11]. In this thesis, we choose two very
promising biomaterials to imitate the visco-elastic properties of the NP: collagen
(chapter 2) and alginate (chapter 3). For this purpose, we first determined the
visco-elastic properties of the goat NP and showed that this is comparable to the
human NP known from literature.
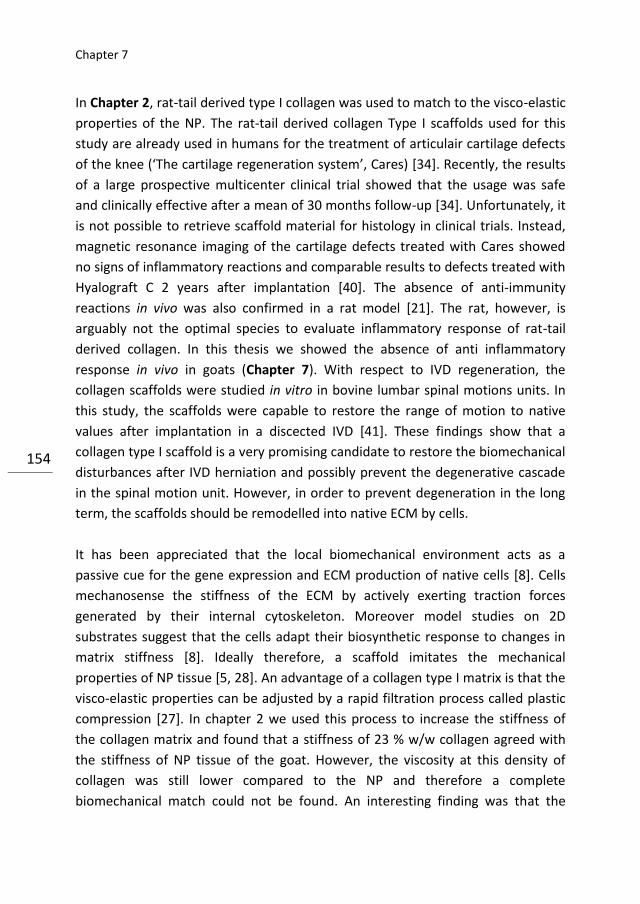
Chapter 7
154
In Chapter 2, rat-tail derived type I collagen was used to match to the visco-elastic
properties of the NP. The rat-tail derived collagen Type I scaffolds used for this
study are already used in humans for the treatment of articulair cartilage defects
of the knee (‘The cartilage regeneration system’, Cares) [34]. Recently, the results
of a large prospective multicenter clinical trial showed that the usage was safe
and clinically effective after a mean of 30 months follow-up [34]. Unfortunately, it
is not possible to retrieve scaffold material for histology in clinical trials. Instead,
magnetic resonance imaging of the cartilage defects treated with Cares showed
no signs of inflammatory reactions and comparable results to defects treated with
Hyalograft C 2 years after implantation [40]. The absence of anti-immunity
reactions in vivo was also confirmed in a rat model [21]. The rat, however, is
arguably not the optimal species to evaluate inflammatory response of rat-tail
derived collagen. In this thesis we showed the absence of anti inflammatory
response in vivo in goats (Chapter 7). With respect to IVD regeneration, the
collagen scaffolds were studied in vitro in bovine lumbar spinal motions units. In
this study, the scaffolds were capable to restore the range of motion to native
values after implantation in a discected IVD [41]. These findings show that a
collagen type I scaffold is a very promising candidate to restore the biomechanical
disturbances after IVD herniation and possibly prevent the degenerative cascade
in the spinal motion unit. However, in order to prevent degeneration in the long
term, the scaffolds should be remodelled into native ECM by cells.
It has been appreciated that the local biomechanical environment acts as a
passive cue for the gene expression and ECM production of native cells [8]. Cells
mechanosense the stiffness of the ECM by actively exerting traction forces
generated by their internal cytoskeleton. Moreover model studies on 2D
substrates suggest that the cells adapt their biosynthetic response to changes in
matrix stiffness [8]. Ideally therefore, a scaffold imitates the mechanical
properties of NP tissue [5, 28]. An advantage of a collagen type I matrix is that the
visco-elastic properties can be adjusted by a rapid filtration process called plastic
compression [27]. In chapter 2 we used this process to increase the stiffness of
the collagen matrix and found that a stiffness of 23 % w/w collagen agreed with
the stiffness of NP tissue of the goat. However, the viscosity at this density of
collagen was still lower compared to the NP and therefore a complete
biomechanical match could not be found. An interesting finding was that the

General discussion
155
swelling capacity of dense collagen scaffolds increases with increasing density.
This is a favorable finding with respect to the replacement of NP tissue that has
also an impressive capacity to swell. In contrast, free floating collagen scaffolds,
often studied as scaffolds as well, are known to shrink by the contraction of the
seeded cells. In Chapter 2, we also showed that γ-sterilization has important
effects on the visco-elastic properties of scaffolds. Sterilization techniques, such
as γ-sterilization, are necessary steps before materials can be used in vivo and the
effects are not always foreseen by scientist involved in the pre-clinical research. In
the absence of an exact biomechanical match, type I collagen should still be
considered as an attractive scaffold material for IVD engineering. The wide
availability (e.g. rat-tail, bovine, transgenic) and known biocompatibility are
noteworthy. The handling, however, is perhaps the most interesting feature of
type I collagen. Plastic compression allows to produce scaffolds rapidly in virtually
every collagen density [27]. Cells survive when added prior to compression
resulting in completely seeded scaffolds [27], or the scaffolds can be used as a-
cellular scaffolds as in the current studies. Besides the visco-elastic properties of
the scaffold, the local hydrostatic pressure also influences cell response [32]. In
the IVD space this is dependent on the forces on the motion segment and the
capacity of the annulus closure technique to seal the defect.
In chapter 3, we evaluated alginate as a scaffold material for NP replacement.
Alginate is a natural polysaccharide used for numerous medical applications due
to its non-toxic nature, wide availability, low costs and simple handling and gelling
behaviour [10]. In addition, the biosynthetic activity of chondrocytes, like NP cells,
cultured in alginate matrices is comparable to the activity in native NP ECM [22,
39]. Alginate beads are therefore widely used as a 3D culture environment for
these cell types [38]. Moreover, initial in vitro and in vivo studies on alginate as a
scaffold material for NP replacement showed encouraging results [22, 26].
However, inferior biomechanical properties, especially after some time in
physiological solutions, have been recognized as important limitations for the
usage of alginate as a scaffold material [10]. In our study, alginate was prepared
via two different techniques [29] and in different densities to imitate the visco
elastic behavior of the NP. The 2% alginate scaffolds prepared by diffusion
gelation closely matched the visco-elastic properties of the NP, even more closely
than the collagen scaffolds described in the preceding chapter. The moduli
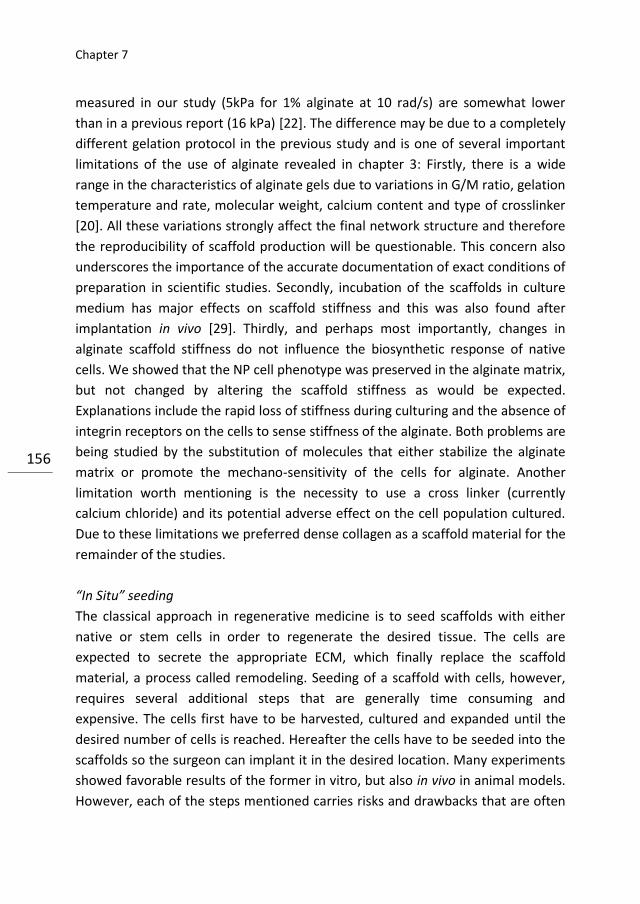
Chapter 7
156
measured in our study (5kPa for 1% alginate at 10 rad/s) are somewhat lower
than in a previous report (16 kPa) [22]. The difference may be due to a completely
different gelation protocol in the previous study and is one of several important
limitations of the use of alginate revealed in chapter 3: Firstly, there is a wide
range in the characteristics of alginate gels due to variations in G/M ratio, gelation
temperature and rate, molecular weight, calcium content and type of crosslinker
[20]. All these variations strongly affect the final network structure and therefore
the reproducibility of scaffold production will be questionable. This concern also
underscores the importance of the accurate documentation of exact conditions of
preparation in scientific studies. Secondly, incubation of the scaffolds in culture
medium has major effects on scaffold stiffness and this was also found after
implantation in vivo [29]. Thirdly, and perhaps most importantly, changes in
alginate scaffold stiffness do not influence the biosynthetic response of native
cells. We showed that the NP cell phenotype was preserved in the alginate matrix,
but not changed by altering the scaffold stiffness as would be expected.
Explanations include the rapid loss of stiffness during culturing and the absence of
integrin receptors on the cells to sense stiffness of the alginate. Both problems are
being studied by the substitution of molecules that either stabilize the alginate
matrix or promote the mechano-sensitivity of the cells for alginate. Another
limitation worth mentioning is the necessity to use a cross linker (currently
calcium chloride) and its potential adverse effect on the cell population cultured.
Due to these limitations we preferred dense collagen as a scaffold material for the
remainder of the studies.
“In Situ” seeding
The classical approach in regenerative medicine is to seed scaffolds with either
native or stem cells in order to regenerate the desired tissue. The cells are
expected to secrete the appropriate ECM, which finally replace the scaffold
material, a process called remodeling. Seeding of a scaffold with cells, however,
requires several additional steps that are generally time consuming and
expensive. The cells first have to be harvested, cultured and expanded until the
desired number of cells is reached. Hereafter the cells have to be seeded into the
scaffolds so the surgeon can implant it in the desired location. Many experiments
showed favorable results of the former in vitro, but also in vivo in animal models.
However, each of the steps mentioned carries risks and drawbacks that are often
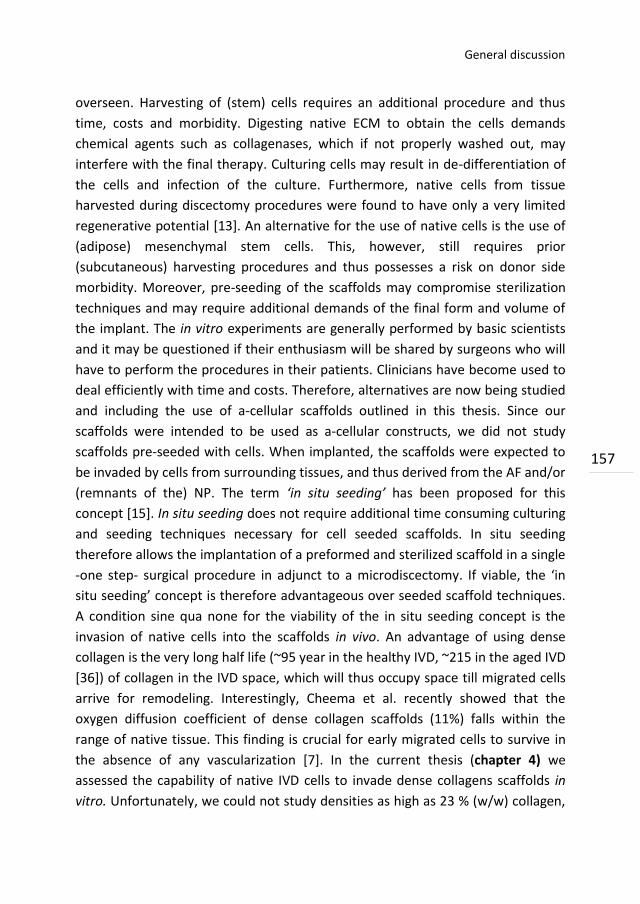
General discussion
157
overseen. Harvesting of (stem) cells requires an additional procedure and thus
time, costs and morbidity. Digesting native ECM to obtain the cells demands
chemical agents such as collagenases, which if not properly washed out, may
interfere with the final therapy. Culturing cells may result in de-differentiation of
the cells and infection of the culture. Furthermore, native cells from tissue
harvested during discectomy procedures were found to have only a very limited
regenerative potential [13]. An alternative for the use of native cells is the use of
(adipose) mesenchymal stem cells. This, however, still requires prior
(subcutaneous) harvesting procedures and thus possesses a risk on donor side
morbidity. Moreover, pre-seeding of the scaffolds may compromise sterilization
techniques and may require additional demands of the final form and volume of
the implant. The in vitro experiments are generally performed by basic scientists
and it may be questioned if their enthusiasm will be shared by surgeons who will
have to perform the procedures in their patients. Clinicians have become used to
deal efficiently with time and costs. Therefore, alternatives are now being studied
and including the use of a-cellular scaffolds outlined in this thesis. Since our
scaffolds were intended to be used as a-cellular constructs, we did not study
scaffolds pre-seeded with cells. When implanted, the scaffolds were expected to
be invaded by cells from surrounding tissues, and thus derived from the AF and/or
(remnants of the) NP. The term ‘in situ seeding’ has been proposed for this
concept [15]. In situ seeding does not require additional time consuming culturing
and seeding techniques necessary for cell seeded scaffolds. In situ seeding
therefore allows the implantation of a preformed and sterilized scaffold in a single
-one step- surgical procedure in adjunct to a microdiscectomy. If viable, the ‘in
situ seeding’ concept is therefore advantageous over seeded scaffold techniques.
A condition sine qua none for the viability of the in situ seeding concept is the
invasion of native cells into the scaffolds in vivo. An advantage of using dense
collagen is the very long half life (~95 year in the healthy IVD, ~215 in the aged IVD
[36]) of collagen in the IVD space, which will thus occupy space till migrated cells
arrive for remodeling. Interestingly, Cheema et al. recently showed that the
oxygen diffusion coefficient of dense collagen scaffolds (11%) falls within the
range of native tissue. This finding is crucial for early migrated cells to survive in
the absence of any vascularization [7]. In the current thesis (chapter 4) we
assessed the capability of native IVD cells to invade dense collagens scaffolds in
vitro. Unfortunately, we could not study densities as high as 23 % (w/w) collagen,
Chapter 7
158
since the time frames (> years) this would require are not compatible with in vitro
culturing [27]. We studied densities up to 3% collagen that are still much higher
compared to the densities generally studied (0,05% collagen). We showed that
both NP and AF cells are capable of invading the scaffolds. As was expected, the
migration decreased with increasing collagen densities. Interestingly we found a
significantly greater migration capacity of NP cells compared to AF cells. Intuitively
we had expected the fibroblast-like AF cells to have a greater migration capacity
in dense collagen than the chondrocyte-like NP cells. Unfortunately, no
comparable studies that either confirm or reject these findings are published. The
chemokine Hst-2, derived from saliva was not found to have any pro-migratory
effects on goat IVD cells. Hegewald et al. showed that the chemokine CXCL10 did
actively recruit human AF cells [14]. The migration of human NP cells on the other
hand was found to be enhanced by human serum [12]. The latter was actually
confirmed by our own findings in the scratch assay in chapter 4.
The animals
Having shown that the visco-elastic properties of the NP can be approached with
an a-cellular scaffold that also allows the invasion of native cells, our next step
was to develop a model to evaluate the scaffold in vivo. Although substantial
research is performed on the development and characterization of scaffolds for
NP engineering, the number of studies that actually performed in vivo evaluation
is very limited. There is only one comparable study which was performed in a
small animal model. Huanng and colleagues recently reported the in vivo
evaluation of collagenα/hyaluronan/chondroitin-6-sulfate scaffolds seeded with
NP cells in a rabbit model [16]. Curiously, no annulus closure technique was
described and might perhaps have been not necessary in the small animal model.
The authors found maintenance of the disc height and a restoration of the T2
weighted MRI signal after 24 weeks follow-up. Other in vivo studies used scaffolds
only as injectable carriers for (stem) cells in disc degeneration. These studies in
rabbits [16] or pigs [31] do not deal with the annulus defect typically for disc
herniation and are therefore not comparable. One last in vivo study worth
mentioning reported the implantation of complete tissue engineered IVD’s
consisting of polyglycolic acid and calcium alginate matrices seeded with native
cells in mice [26]. Although the ECM production was in line with native tissue up
to 12 weeks, the method of delivery of these constructs is perhaps too
General discussion
159
complicated to be feasible in humans. The number of in vivo studies for NP
scaffolds is remarkably small compared to the massive in vitro work that has been
published. Possibly, more in vivo studies have been performed, but not been
accepted for publication since the results were negative [24]. A potential
explanation for this, and one of the main concerns of NP replacement models in
general, is the necessity of a closure technique for the AF [41]. During the
planning of the animal studies we soon experienced the problem ourselves and
decided to start to summarize all available data from literature on this subject
first. This resulted in an extensive review (Chapter 5) from which it can be
concluded that, despite numerous attempts, an appropriate AF closing technique
is not yet invented. Since our intention was to evaluate dense collagen implants in
goats, we needed some AF closure technique and started to test several custom
made AF closure devices. These devices were designed to the goat dimensions
and should be compatible with our NP replacement model. After thorough in vitro
and in vivo (2 weeks) evaluation (Chapter 6) of potential devices we found devices
which closed the AF sufficiently. These devices were then used for a next pilot in
vivo study (6 weeks) to evaluate the collagen scaffolds. However, after six weeks
follow-up the ACD’s showed important signs of dislodgement and destruction. We
therefore could still not perform the full in vivo evaluation of the collagen
implants that we aimed. However, we did show that the disc height could be
preserved in the levels treated with the collagen scaffolds, results that are in line
with the findings of Huanng et al. [16]. They also found restored hydration (based
on MRI) of the IVD after 24 weeks follow up. We could not make a quantitative
analysis of the MR images, since the surgical disturbances were still predominant
after 6 weeks follow up. Moreover, the AF closure devices have their own effects
on MRI signal, essentially disturbing appropriate quantification. Haunng et al
however, used a small animal model, which has a very limited value for
translation to humans [24]. Small animal have significantly different spinal
biomechanics and the small volume of the disc affects transport [3, 24].
Remaining disc height and an acceptable MRI T2 signal is therefore not very
informative. The use of these animals should be preserved for safety studies, but
feasibility studies require a large animal model as was used in the current thesis
[24]. Although the replacement model was feasible, the surgeries reproducible
and the harm to the animals acceptable the results are strongly negatively
influenced due to the lack of an appropriate AF closure technique. Therefore no

Chapter 7
160
firm conclusions can be drawn. The experiments deserve further study,
accompanied by a proper AF closure technique.
Future perspectives
Substantial research in the field of tissue engineering has been based on trial and
error rather than on firm scientific knowledge. Not surprisingly, since many
factors and circumstances affecting the success of the regenerative medicine still
have to be revealed. For example, we studied the visco-elastic properties of a
scaffold because this has been recognized as a cue for differentiation and ECM
production. However, first studies on this subject have been published only five
years ago and involved cells seeded on a flat surfaces [9]. Meanwhile, similar
findings were observed in 3D environments, but the exact value, and the relation
to other local circumstances such as the hydrostatic pressure, the biochemical
environment and scaffold degradation rates remains unclear [32]. During the past
decade, in vitro research using scaffolds, native cells or stem cells, have detected
several individual factors involved in the regeneration of tissues. Probably we still
know only a small portion of all the factors and basic research will remain to have
a crucial position, before fully scientifically based regenerative strategies can be
designed. Even when we are aware of all the factors involved, we still have to
study their interactions, counteractions and synergies. This can only be properly
studied in vivo and studies in relevant animal models are therefore required.
Small animal models are useful for screening purposes, but large animal models
are required to mimic nutritional and surgical constraints to human application
[24]. Early tissue engineering attempts should be accompanied by a vision how
the final clinical application will look like and address demands like formulation,
delivery and sterilization [4, 19]. To evaluate therapies that are intended to
regenerate the herniated IVD, there is a need for standardized magnetic
resonance imaging grading and/ or scoring systems [2]. The scoring systems
should be developed in animal models with histologic confirmation and then
translated to the human situation in which histology is not an option [24]. An
alternative to the use of animal models, is the use of a bioculture system in which
entire IVD’s can be studied under physiological circumstances and with longer
time frames [17]. These systems have the advantage to reduce the number of
animals needed for research and are currently being developed and their exact
value will become clear in the near future. We showed that the lack of AF closure
General discussion
161
techniques impedes the in vivo evaluation. Moreover, in our goat model only a
standardized defect in the lateral region of the AF had to be closed. In the patients
suffering from disc herniation the defects are irregular, located posteriorly close
to the neurological structures and sometimes even bilaterally. Appropriate
closure of the AF defect in these patients will be even more challenging and might
further delay tissue engineering development that may have passed the pre
clinical stage successfully. Several suggestions and requires for annulus closure
techniques were extensively described in Chapter 5. An important possibility to
prevent the unnecessary repeating of (animal) studies with not publishable
negative outcomes is the dissemination of these results between internationally
established spinal research sites [24].
In the end, the most important question will be if the patients actually will benefit
from the new therapy. Improper patient selecting may place a potential beneficial
procedure in disrepute [19]. Clinicians should be instructed how to implement the
new types of therapy in their surgical practice. This will demand close cooperation
between scientists, industry and medical personnel [24]. Tissue engineering sites
should be close to the operating theaters within the same complex. It requires
massive efforts to achieve all this but the improvement of health care may be
likewise if the promise of tissue engineering is finally fulfilled.

Chapter 7
162
References
1. Wikipedia. 2011.
2. Andersson GB, An HS, Oegema TR, Jr., Setton LA (2006) Directions for future
research. J Bone Joint Surg Am 88 Suppl 2:110-114.
3. Beckstein JC, Sen S, Schaer TP, Vresilovic EJ, Elliott DM (2008) Comparison of
animal discs used in disc research to human lumbar disc: axial compression
mechanics and glycosaminoglycan content. Spine (Phila Pa 1976 ) 33(6):E166-
E173.
4. Bron JL, Helder MN, Meisel HJ, van Royen BJ, Smit TH (2009) Repair, regenerative
and supportive therapies of the annulus fibrosus: achievements and challenges.
Eur Spine J 18(3):301-313.
5. Chan BP, Leong KW (2008) Scaffolding in tissue engineering: general approaches
and tissue-specific considerations. Eur Spine J 17 Suppl 4:467-479.
6. Chan WC, Sze KL, Samartzis D, Leung VY, Chan D (2011) Structure and biology of
the intervertebral disk in health and disease. Orthop Clin North Am 42(4):447-64,
vii.
7. Cheema U, Rong Z, Kirresh O et al. (2011) Oxygen diffusion through collagen
scaffolds at defined densities: implications for cell survival in tissue models. J
Tissue Eng Regen Med.
8. De Santis G, Lennon AB, Boschetti F et al. (2011) How can cells sense the elasticity
of a substrate? An analysis using a cell tensegrity model. Eur Cell Mater 22:202-
213.
9. Engler AJ, Sen S, Sweeney HL, Discher DE (2006) Matrix elasticity directs stem cell
lineage specification. Cell 126(4):677-689.
10. Ghahramanpoor MK, Hassani Najafabadi SA, Abdouss M, Bagheri F, Baghaban EM
(2011) A hydrophobically-modified alginate gel system: utility in the repair of
articular cartilage defects. J Mater Sci Mater Med 22(10):2365-2375.
11. Gilchrist CL, Darling EM, Chen J, Setton LA (2011) Extracellular matrix ligand and
stiffness modulate immature nucleus pulposus cell-cell interactions. PLoS One
6(11):e27170.
12. Haberstroh K, Enz A, Zenclussen ML et al. (2009) Human intervertebral disc-
derived cells are recruited by human serum and form nucleus pulposus-like tissue
upon stimulation with TGF-beta3 or hyaluronan in vitro. Tissue Cell 41(6):414-
420.
13. Hegewald AA, Endres M, Abbushi A et al. (2011) Adequacy of herniated disc
tissue as a cell source for nucleus pulposus regeneration. J Neurosurg Spine
14(2):273-280.
14. Hegewald AA, Neumann K, Kalwitz G et al. (2011) The Chemokines CXCL10 and
XCL1 Recruit Human Annulus Fibrosus Cells. Spine (Phila Pa 1976 ).
General discussion
163
15. Hegewald AA, Ringe J, Sittinger M, Thome C (2008) Regenerative treatment
strategies in spinal surgery. Front Biosci 13:1507-1525.
16. Huang B, Zhuang Y, Li CQ, Liu LT, Zhou Y (2011) Regeneration of the
Intervertebral Disc with Nucleus Pulposus Cell-seeded
Collagenalpha/Hyaluronan/Chondroitin-6-sulfate tri-copolymer Constructs in a
Rabbit Disc Degeneration Model. Spine (Phila Pa 1976 ).
17. Jim B, Steffen T, Moir J, Roughley P, Haglund L (2011) Development of an intact
intervertebral disc organ culture system in which degeneration can be induced as
a prelude to studying repair potential. Eur Spine J 20(8):1244-1254.
18. Johnston SL, Campbell MR, Scheuring R, Feiveson AH (2010) Risk of herniated
nucleus pulposus among U.S. astronauts. Aviat Space Environ Med 81(6):566-574.
19. Kandel R, Roberts S, Urban JP (2008) Tissue engineering and the intervertebral
disc: the challenges. Eur Spine J 17 Suppl 4:480-491.
20. Kuo CK, Ma PX (2001) Ionically crosslinked alginate hydrogels as scaffolds for
tissue engineering: part 1. Structure, gelation rate and mechanical properties.
Biomaterials 22(6):511-521.
21. Kuroda T, Matsumoto T, Mifune Y et al. (2011) Therapeutic strategy of third-
generation autologous chondrocyte implantation for osteoarthritis. Ups J Med Sci
116(2):107-114.
22. Leone G, Torricelli P, Chiumiento A, Facchini A, Barbucci R (2008) Amidic alginate
hydrogel for nucleus pulposus replacement. J Biomed Mater Res A 84(2):391-401.
23. Lim JM, Lee M, Lee EJ, Gong SP, Lee ST (2011) Stem cell engineering: limitation,
alternatives, and insight. Ann N Y Acad Sci 1229:89-98.
24. Masuda K, Lotz JC (2010) New challenges for intervertebral disc treatment using
regenerative medicine. Tissue Eng Part B Rev 16(1):147-158.
25. Mercuri JJ, Gill SS, Simionescu DT (2011) Novel tissue-derived biomimetic scaffold
for regenerating the human nucleus pulposus. J Biomed Mater Res A 96(2):422-
435.
26. Mizuno H, Roy AK, Vacanti CA et al. (2004) Tissue-engineered composites of
anulus fibrosus and nucleus pulposus for intervertebral disc replacement. Spine
29(12):1290-1297.
27. Mudera V, Morgan M, Cheema U, Nazhat S, Brown R (2007) Ultra-rapid
engineered collagen constructs tested in an in vivo nursery site. J Tissue Eng
Regen Med 1(3):192-198.
28. Nerurkar NL, Elliott DM, Mauck RL (2010) Mechanical design criteria for
intervertebral disc tissue engineering. J Biomech 43(6):1017-1030.
29. Nunamaker EA, Purcell EK, Kipke DR (2007) In vivo stability and biocompatibility
of implanted calcium alginate disks. J Biomed Mater Res A 83(4):1128-1137.
Chapter 7
164
30. Ott HC, Mathisen DJ (2011) Bioartificial tissues and organs: are we ready to
translate? Lancet.
31. Revell PA, Damien E, Di Silvio L et al. (2007) Tissue engineered intervertebral disc
repair in the pig using injectable polymers. J Mater Sci Mater Med 18(2):303-308.
32. Reza AT, Nicoll SB (2008) Hydrostatic pressure differentially regulates outer and
inner annulus fibrosus cell matrix production in 3D scaffolds. Ann Biomed Eng
36(2):204-213.
33. Rihn JA, Hilibrand AS, Radcliff K et al. (2011) Duration of symptoms resulting from
lumbar disc herniation: effect on treatment outcomes: analysis of the Spine
Patient Outcomes Research Trial (SPORT). J Bone Joint Surg Am 93(20):1906-
1914.
34. Schneider U, Rackwitz L, Andereya S et al. (2011) A Prospective Multicenter Study
on the Outcome of Type I Collagen Hydrogel-Based Autologous Chondrocyte
Implantation (CaReS) for the Repair of Articular Cartilage Defects in the Knee. Am
J Sports Med.
35. Shamji MF, Setton LA, Jarvis W et al. (2010) Proinflammatory cytokine expression
profile in degenerated and herniated human intervertebral disc tissues. Arthritis
Rheum 62(7):1974-1982.
36. Sivan SS, Wachtel E, Tsitron E et al. (2008) Collagen turnover in normal and
degenerate human intervertebral discs as determined by the racemization of
aspartic acid. J Biol Chem 283(14):8796-8801.
37. Steenstra IA, Anema JR, van Tulder MW et al. (2006) Economic evaluation of a
multi-stage return to work program for workers on sick-leave due to low back
pain. J Occup Rehabil 16(4):557-578.
38. Vonk LA, Doulabi BZ, Huang C et al. (2010) Preservation of the chondrocyte's
pericellular matrix improves cell-induced cartilage formation. J Cell Biochem
110(1):260-271.
39. Wang CC, Yang KC, Lin KH et al. (2012) Cartilage regeneration in SCID mice using a
highly organized three-dimensional alginate scaffold. Biomaterials 33(1):120-127.
40. Welsch GH, Mamisch TC, Zak L et al. (2010) Evaluation of cartilage repair tissue
after matrix-associated autologous chondrocyte transplantation using a
hyaluronic-based or a collagen-based scaffold with morphological MOCART
scoring and biochemical T2 mapping: preliminary results. Am J Sports Med
38(5):934-942.
41. Wilke HJ, Heuer F, Neidlinger-Wilke C, Claes L (2006) Is a collagen scaffold for a
tissue engineered nucleus replacement capable of restoring disc height and
stability in an animal model? Eur Spine J 15 Suppl 3:S433-S438.

Appendices

166
167
Appendix 1
Summary

Summary
168
Lumbar discectomy is an effective therapy for neurological decompression in
patients suffering from sciatica due to a herniated nucleus pulposus (NP).
Discectomies however, do not deal with the damaged intervertebral disc (IVD)
and high numbers of patients suffer from persisting postoperative low back pain.
This has resulted in many strategies targeting the regeneration of the NP. In this
thesis we developed a novel tissue engineering strategy to treat patients suffering
from an herniated intervertebral disc (IVD). In chapter 2-4 the materials and cells
were described and optimized. In chapter 5-6 a model was developed to evaluate
the materials in goats in vivo.
In chapter 2 we used rheology to assess the visco elastic properties of the nucleus
pulposus (NP) of goats. We used plastic compression to increase the density of
collagen type I scaffolds and aimed to imitate the visco elastic properties of the
NP. We also assessed the effect of a standard treatment with γ-sterilization on the
scaffolds. We found a complex modulus of 22 kPa for the NP which agreed with a
collagen density of approximately 23 %. However, the loss tangent, indicative of
energy dissipation, was independent of the collagen density and could not be
matched to the value of the NP. Treatment by γ-sterilization resulted in an
increase of the shear moduli, but also in a more brittle behaviour and a reduced
swelling capacity.
In chapter 3 we used alginate as a scaffold material and aimed to mimic the visco-
elastic properties of the NP. We also assessed the effects of different alginate
stifnessess on native cells. Alginate scaffolds were prepared by two different
techniques (diffusion and in situ gelation) and in concentrations ranging from 1 to
6 %. The 2% alginate scaffolds prepared by diffusion gelation showed the best
match to the visco-elastic properties of the NP. However, the visco elastic
properties rapidly declined upon incubation in medium. The biosynthetic
phenotype of the cells was preserved in alginate, but no differences were found
between the various scaffold densities most likely due to the poor adhesiveness of
the cells to alginate.
In chapter 4 we assessed the capability of native cells to invade dense collagen
scaffolds in vitro. The invasion of cells from the surrounding tissues, the
(remnants of the) NP and the annulus fibrosus (AF), is crucial for the use of a-

Summary
169 169
cellular scaffolds. In this chapter we also assessed if migration could be enhanced
by the addition of Histatin-2, a chemokine derived from human saliva that was
shown to enhance the migration of fibroblast. We found that migration distance
was density dependent and was higher for NP compared to AF cells after 4 weeks
of culturing. We also observed a lag phase, before migration occurred. Histatin-2
did not enhance cell migration and this was confirmed in a separate scratch-assay.
Although the densities used in this study were lower (1,5 and 3%) compared to
the density shown to mimic the NP (23%), we proved that native cells are capable
of invading dense collagen scaffolds and the in situ seeding concept might be
viable.
Numerous regenerative treatment strategies have being developed targeting the
NP. However, accompanying techniques that deal with the damaged AF are
increasingly being recognised as mandatory in order to prevent re-herniations and
to increase the potential of the NP replacing strategies. In chapter 5 we
summarized and discussed all available literature on AF closure techniques of the
AF including the attempts performed by commercial parties. We showed that
several attempts to repair, support or regenerate the AF have been studied, but a
successful clinical application is still far away. In general, tissue engineering
strategies lack a vision on the final clinical application and repair therapies lack
scientific evidence.
In chapter 6 we designed and tested annulus closure devices intended to be used
in our goat nucleus replacement model. First a standardised defect (3 mm) in the
lateral region of the AF was created through which a nucleotomy was performed.
The AF defect was filled with one of the annulus closure devices (ACD’s) with and
without the addition of a collagen nucleus replacement. First studies were
performed on goat cadaveric lumbar spines. We showed that ACD’s with four
barb rings could withstand the highest axial load. We further showed that the
increased range of flexion-extension and lateroflexion due to the discectomy
could be restored by implanting an ACD and collagen implant. The positive results
were confirmed in a goat pilot study (n=2) after two weeks follow up. However, in
a second pilot study (n=8) most ACD’s revealed signs of destruction and/or
displacement after 6 weeks follow-up. In addition we found two endplate
reactions extending into the subchondral bone, most likely due to continuous
Summary
170
friction of the ACD’s between the vertebrae. The ACD’s showed a tendency to
perform better when they were implanted together with a collagen implant.
In the first addendum to chapter 6 we described the development the
replacement model in detail. First, a Perspex model of the goat IVD was used to
design the instruments and implants with appropriate dimensions. The
instruments consisted of metal tubes with ascending diameter to punctuate the
AF. Via the largest tube, with an outer diameter of 3 mm, all instruments and
implants, except for the ACD can be inserted. In the second addendum to chapter
6, we present the results of the collagen scaffold that was used in adjunct to
ACD’s in the goat study. After 6 weeks the disc height index in goats treated with
the collagen implants was not significantly decreased compared to untreated
control levels. Levels that received a discectomy or ACD alone did show a
significant decrease in disc height. Macroscopy revealed that the dense collagen
was not yet integrated with the NP tissue and therefore lost during sawing and
preparation for histology. Histologic and magnetic resonance imaging score were
not useful to evaluate the results after 6 weeks follow up. There was no difference
in cell number between the different treatments after 6 weeks.
In conclusion, we showed that the visco elastic properties of the IVD can be
imitated with scaffold materials that also allow the invasion of native cells.
However, the promising results can not yet be translated to in vivo studies due to
the lack of appropriate AF closure techniques.
171
Appendix 2
Nederlandse Samenvatting
Samenvatting
172
Een rughernia (voluit: hernia nuclei pulposi) is een veelvoorkomende en
invaliderende ziekte. De huidige operatieve behandeling bestaat uit het
verwijderen van het gehernieerde tussenwervelschijf weefsel (discectomie),
waardoor de zenuwbeknelling wordt opgeheven. Hierbij wordt de beschadigde
tussenwervelschijf zelf echter niet behandeld en veel patiënten houden hierna
dan ook rugklachten. Voor het herstel van de tussenwervelschijf bestaat op dit
moment nog geen goede therapie. In dit proefschrift worden potentiele nieuwe
behandelingsopties ontwikkeld die regeneratie van de tussenwervelschijf tot doel
hebben. In het eerste deel (hoofdstukken 2-4) worden materialen en cellen voor
tussenwervelschijf regeneratie onderzocht en geoptimaliseerd. In het tweede deel
(hoofdstukken 5-6) wordt een model ontwikkeld om de materialen te kunnen
testen in vivo in geiten.
In hoofdstuk 2 wordt eerst door middel van reologie de visco-elasticiteit van de
geiten nucleus pulposus (NP) bepaald. Vervolgens wordt geprobeerd om deze
visco-elasticiteit na te bootsen met type I collageen scaffolds. Hiervoor wordt met
behulp van plastische compressie de dichtheid van deze scaffolds verhoogd. Ook
wordt onderzocht wat de effecten van een standaard sterilisatie proces middels γ-
irradiatie zijn op de visco-elastische eigenschappen van de scaffolds. De NP blijkt
qua visco-elasticiteit ongeveer overeen te komen met collageen scaffolds die een
dichtheid van 23% hebben. De verhouding tussen de viscositeit en elasticiteit
blijkt echter wel lager in de scaffolds vergeleken met de NP. Door behandeling
met γ-irradiatie stijgt de elasticiteit, maar wordt het materiaal ook breekbaarder
en neemt de zwelcapaciteit sterk af.
In hoofdstuk 3 wordt alginaat als een potentieel scaffold materiaal voor de NP
onderzocht. De alginaat scaffolds worden op 2 verschillende manieren gemaakt
(via ‘diffusie’ en ‘in situ’ gelling) in concentraties tussen de 1 en 6% om zo te
kijken welke de visco-elastische eigenschappen van de NP het dichtst benadert.
Ook wordt onderzocht wat het effect van de verschillende stijfheden alginaat op
het gedrag van natieve tussenwervelschijf cellen is. De 2% alginaat scaffolds,
bereid via de diffusie methode, blijken de visco-elasticiteit van de NP het sterkst
te benaderen. Echter, wanneer de scaffolds in kweekmedium worden gelegd
treedt er een zeer snelle sterke afname van de stijfheid op. Ook blijkt dat het
fenotype van de cellen weliswaar blijft behouden in alginaat, maar er blijkt geen
Samenvatting
173 173
relatie met de stijfheid ervan. Dit laatste kan waarschijnlijk worden verklaard door
de slechte binding van tussenwervelschijf cellen aan het alginaat.
In hoofdstuk 4 wordt onderzocht of natieve tussenwervelschijf cellen in staat zijn
om collageen scaffolds in te groeien in vitro. De ingroei van cellen uit de
omgevende structuren, de (overblijfselen van de) NP of annulus fibrosus (AF), is
een cruciale voorwaarde voor het gebruik van a-cellulaire scaffolds voor NP
regeneratie. In dit hoofdstuk kijken we ook of de celmigratie kan worden
bespoedigd met behulp van histatine-2, een chemokine uit menselijk speeksel
waarvan is aangetoond dat het de migratie van fibroblasten versnelt. De
celmigratie blijkt afhankelijk van de collageen concentratie en hoger voor NP
vergeleken met AF cellen na 4 weken. De migratie blijkt pas op gang te komen na
een bepaalde periode. Histatine-2 is geen migratie bevorderende factor bij onze
celpopulatie en dit wordt ook bevestigd in een (2D) scratch assay. Ondanks dat de
collageen dichtheden die in dit hoofdstuk worden onderzocht nog lager liggen dan
de beoogde collageendichtheid (uit hoofdstuk 2), zijn de natieve cellen in staat
zijn om de collageen scaffolds te in te groeien. Dit bevestigt dat a-cellulaire
collageen scaffolds mogelijk kunnen worden gebruikt voor NP regeneratie.
Er is in de afgelopen decade veel onderzoek gedaan naar de regeneratie van de
NP. Hieruit blijkt steeds meer de noodzaak om een therapie te ontwikkelen die
het defect in de omringende AF aanpakt, om zo het aantal re-herniaties te
verlagen en het succes van potentiele NP regeneratie therapieën te verhogen. In
hoofdstuk 5 geven we een overzicht van alle beschikbare literatuur over het
sluiten van de AF. Er blijken diverse pogingen gedaan te zijn om de AF te
repareren of regenereren, maar een succesvolle klinische therapie lijkt nog ver
weg. Bij de beschreven regeneratieve pogingen ontbreekt vaak een duidelijke
visie betreffende de uiteindelijke toepassing, terwijl bij de directe
repareerpogingen juist een wetenschappelijke onderbouwing ontbreekt.
In Hoofdstuk 6 testen we enkele zelfontworpen implantaten om het AF defect ons
geiten model te sluiten. Eerst wordt een gestandaardiseerd 3 mm groot defect
gemaakt lateraal op de AF, waardoor de NP wordt uitgeruimd (discectomie). Het
defect in de AF wordt vervolgens gesloten de afsluit implantaten. We testen
tussenwervelschijven waar alleen een AF implantaat wordt ingebracht als ook die
Samenvatting
174
waar ook een collageen NP implantaat wordt ingebracht. In het eerste deel van de
eerste experimenten worden de implantaten in tussenwervelschijven ex vivo
getest. Hierbij blijkt een 3.5 mm groot AF afsluit implantaat met vier zijringen de
hoogste axiale belasting aan te kunnen. Ook blijkt dat de toegenomen flexie-
extensie en lateroflexie die optreedt na een discectomie weer kan worden
hersteld met behulp van een AF en collageen NP implantaat samen. De positieve
resultaten worden bevestigd in 2 geiten in vivo na 2 weken follow up. Na 6 weken
follow up (n=8) blijken echter de meeste AF afsluit implantaten gedestrueerd en
verplaatst. Ook blijkt op 2 niveaus sprake van een forse eindplaatreaktie,
waarschijnlijk door continu frictie van de AF implantaten. Er lijkt een trend dat de
AF afsluit implantaten het iets beter doen wanneer ze gebruikt worden samen
met een collageen implantaat dan wanneer standalone.
In het eerste addendum bij hoofdstuk 6 wordt de ontwikkeling van het diermodel
gedetailleerder beschreven. Er wordt begonnen om met behulp van een perspex
model van de geiten tussenwervelschijf de benodigde instrumenten en
implantaten te ontwikkelen met juiste dimensies. De instrumenten bestaan uit
metalen holle buisjes, welke over een voordraad en over elkaar kunnen worden
opgevoerd door de laterale AF. Door de grootste buis (buitenste diameter 3 mm)
kunnen vervolgens alle andere instrumenten en implantaten, behoudens de AF
afsluit implantaten, worden geïntroduceerd. In het tweede addendum bij
hoofdstuk 6 worden de collageen scaffolds, die in combinatie met de ACD’s waren
gebruikt in hoofdstuk 6, geanalyseerd. Deze analyse omvat de
tussenwervelschijfhoogte, macro- en microscopie en MRI. Na 6 weken blijkt de
hoogte van de tussenwervelschijf in de geiten die werden behandeld met een
collageen implant niet significant afgenomen ten opzichte van onbehandelde
controle niveaus. De tussenwervelschijven die worden behandeld met alleen een
discectomie of een AF implantaat zonder collageen implantaat tonen wel een
significante afname. Macroscopisch blijkt het collageen na 6 weken nog niet te
zijn vastgegroeid met de omgeving waardoor het grotendeels verloren gaat
tijdens het zagen en voorbereiden voor histologie. Voorts blijken bestaande
histologische en MRI scores niet bruikbaar om de resultaten na 6 weken te
evalueren. Er is geen significant verschil in aantallen cellen tussen de verschillende
behandelingen.

Samenvatting
175 175
In dit proefschrift toonden we aan dat de visco elastische eigenschappen van de
tussenwervelschijf kan worden nagebootst met scaffold materialen. Deze
materialen laten ook de invasie van natieve cellen toe. De bemoedigende
resultaten kunnen echter niet in vivo worden bevestigd door het gebrek aan een
adequate annulus sluiting.

Samenvatting
176
177
Appendix 3
Publications
Publications
178
Publications contributing to this thesis
- Bron JL, Koenderink GH, Everts V, Smit TH. Rheological characterization of the
Nucleus pulposus and dense collagen scaffolds intended for functional
replacement. J Orthop Res. 2009; 27:260-266
- Bron JL, Vonk LA, Smit TH, Koenderink GH. Engineering alginate for
intervertebral disc repair. J Mech Behav Biomed Mater 2011;4:1196-205
- Bron JL, Mulder HW, Vonk LA, Boulabi BZ, Oudhoff MJ, Smit TH. Migration of
intervertebral disc cells into collagen scaffolds intended for functional
replacement. J Mater Sci Mater Med. 2012; 23:813-821
- Bron JL, Helder MN, Meisel HJ, Van Royen BJ, Smit TH. Repair, regenerative
and supportive treatment strategies of the Annulus Fibrosus; Achievements
and challenges. Eur Spine J. 2009; 801:301-313
- Bron JL, Van der Veen AJ, Helder MN, Smit TH. Biomechanical and in vivo
evaluation of experimental closure devices of the annulus fibrosus designed for
a goat nucleus replacement model. Eur Spine J. 2010;19:1347-1355
- Bron JL, Van royen BJ, Helder MN, Sonnega RJ, Smit TH. Development of a
minimal-invasive lumbar disc repair model and evaluation in a goat pilot study
in vivo. Eur Spine J. 2012; submitted
Other publications (international)
- Bron JL, Brinkman JM, Visser M, Wuisman PI. A slow growing mass on the
back in a 63-year old man. Clin Orthop Rel Res. 2006; 452: 274-283
- Van Royen BJ, Noske DP, Bron JL, Vandertop WP. Basilar impression in
osteogenesis imperfecta: Can it be treated with halo traction followed by
posterior fusion? Acta Neurochirurgica. 2006; 148: 1301-1305
- Bron JL, Saouti R, De Gast A. Treatment of posterior knee dislocation in a
patient with multiple sclerosis after knee replacement. Acta Orthop Belg.
2007; 73: 118-121
- Brinkman JM, Bron JL, Wuisman PI, Van Diest PJ, Comans EF, Molthoff CF. The
correlation between clinical, nuclear and histologic findings in a patient with
Von Recklinghausen’s disease. World J Surg Oncol. 2007; 5: 130
- Bron JL, Van Kemenade FJ, Verhoof OJ, Wuisman PI. Long-term follow-up in a
patient with disseminated spinal hydatidosis. Acta Orthop Belg. 2007; 73: 678-
682
Publications
179 179 179
- Bron JL, Van Royen BJ, Wuisman PI. The clinical Significance of lumbosacral
transitional vertebrae. Acta Orthop Belg. 2007; 73: 687-695
- Verhoof OJ, Bron JL, Wapstra FH, Van Royen BJ. High failure rate of the
interspinous distraction device (X-Stop) for the treatment of lumbar spinal
stenosis caused by degenerative spondylolisthesis. Eur Spine J. 2008; 17: 188-
192
- Langeveld AR, Bron JL, De Bruijn AJ. Lower back pain and bladder dysfunction.
sBMJ. 2008; 16: 120
- Bron JL, Mooi WJ, Saouti R, Wuisman PI. A 31-year-old female patient with a
slow growing pre-patellar mass. Clin Orthop Rel Res. 2008; 466:1511-15
- Bron JL, De Vries MK, Snieders MN, Van der Horst-Bruinsma IE, Van Royen BJ.
The Andersson lesion of the spine in Ankylosing Spondylitis revisited. Clin
Rheumatol. 2009; 28: 883-892
Other publications (national):
- Nijveldt RJ, Teerlink T, Hoven B van der, Siroen MP, Bron JL, Rauwerda JA,
Girbes AR, Van Leeuwen PA. Hoge plasma concentratie van ADMA als
onafhankelijke sterftevoorspeller op bij intensivecarepatiënten. Ned Tijdschr
Geneeskd. 2004; 148; 782-7.
- Bron JL, Jaspars EH, Molenkamp BG, Meijer S, Mooi WJ, Van Leeuwen PA. Drie
patienten met op Spitz naevus gelijkende afwijkingen die later een melanoom
bleken te zijn. Ned Tijdschr Geneeskd. 2005; 149:1852-8.
- Bron JL, Van Solinge GB, Langeveld AR, Jiya TU, Wuisman PI. Drie tevoren
gezonde personen met een vermoeidheidsbreuk. Ned Tijdschr Geneeskd.
2007; 151: 621-628
- Bron JL, Wuisman PI. Diagnose in beeld: Een patiënte met een gezwollen knie.
Ned Tijdschr Geneeskd. 2007; 151: 2564-2565
- Bron JL, Van Royen BJ, Wuisman PI. Het interspinale implantaat –
behandelingsoptie bij het syndroom van Verbiest? Ned Tijdschr Orthopaedie.
2007; 14: 5-11

Publications
180
181
Appendix 4
Dankwoord
Dankwoord
182
Wanneer je als arts aan een promotie onderzoek begint ben je aangewezen op de
hulp en ondersteuning van velen. Mijn dank is groot voor alle betrokkenen bij o.a.
de orthopedie, Arthro Kinetics, orale celbiologie, orale biochemie, UPC en AMOLF.
Dit geldt ook voor alle mede auteurs, collegae, studenten, de paranimfen en
uiteraard de leescommissie. Hier geen opsomming van namen, wel wil ik enkelen
persoonlijk bedanken.
Prof. Dr. Paul Wuisman;
Prof Wuisman stond aan de wieg van mijn onderzoek en daarom hier als eerste
genoemd. Visie, enthousiasme en een onuitputtelijke bron van goede ideeën. Gaf
mij het vertrouwen om aan een promotie onderzoek te beginnen en regelde dat ik
tot die tijd als ANIOS in de kliniek aan de slag kon. Zijn onverwachte overlijden in
2007 was dan ook een grote tegenslag. Tot het eind is prof. Wuisman de
inspiratiebron gebleven voor mijn onderzoek en als mens zal ik hem blijven
missen.
Prof. Dr. Ir. Theo Smit;
Beste Theo, zonder jouw steun was dit boekje er niet gekomen. Na het verlies van
prof Wuisman en het, tijdens de kredietcrisis, wegvallen van de financiële steun
voor mijn onderzoek nam jij het voortouw. Het waren soms angstige momenten,
maar door jouw inzet en steun is het uiteindelijk goed gekomen. Als niet-clinicus
temidden van met name klinische wetenschappers was jouw tegenwicht
verhelderend en onmisbaar. Als wetenschapper scherp en kritisch, als mens
eerlijk, bescheiden en betrokken. Het maakt jou de ideale begeleider en
promotor.
Prof. Dr. Barend van Royen;
Beste Barend, geheel onverwacht moest jij alle onderzoeksprojecten op je nemen.
Mijn onderzoek viel daar ook onder. Ik ben je erg dankbaar dat jij deze taak zo
goed hebt opgepakt en me aan het einde de rust en steun hebt gegeven die ik
nodig had. Naast promotor ben je inmiddels als opleider ook verantwoordelijk
voor de volgende grote stap in mijn carrière.
Dankwoord
183 183
Prof. Dr. Gijsje Koenderink;
Beste Gijsje, tijdens jouw eerste rondleiding door het AMOLF (FOM-instituut voor
Atoom- en molecuulfysica) zag ik een wereld die ver af stond van het voor mij
vertrouwde ziekenhuis. Maar jouw enthousiasme om een brug te slaan tussen
deze 2 werelden werkte direct aanstekelijk. Terwijl ik in de weken hierna in een
verlaten kelder van het AMOLF begon met mijn onderzoek aan de gloednieuwe
reometers, zette jij in korte tijd een hele nieuwe onderzoeksgroep op. Toen ik
dacht dat mijn boekje wel naar de drukker kon, kwam er alsnog een
roodgekleurde correctie versie terug van alle spelfouten die je alsnog had
ontdekt. Veel dank voor je gedreven, enthousiaste en altijd kritische houding!
184

185 185
Appendix 5
Curriculum Vitae

Curriculum vitae
186
Johannes Leendert (Harry) Bron was born on Januari 18th, 1980 in Leerdam, The
Netherlands. After graduating from high school (Heerenlanden College, Leerdam)
in 1999, he began studying Medicine at the Vrije Universiteit Amsterdam. During
his medical internships he participated in orthopaedic research with Prof. Dr.
P.I.J.M. Wuisman at the department of Orthopaedic Surgery of the VU University
Medical Center Amsterdam. After receiving his medical degree (cum laude) in
2005, he started to work as an orthopaedic resident at the same department. In
2006 he started his PhD-project focusing on novel regenerative strategies of the
intervertebral disc as described in this thesis (promotores: prof. dr. B.J. van Royen
and prof. dr. ir. T.H. Smit). Directly after this he started his surgical residency (part
of his orthopaedic training) in the Spaarne Ziekenhuis in Hoofddorp (Head: dr.
G.J.M. Akkersdijk). Currently he works as an orthopaedic resident at the VU
University Medical Center (Head: prof. dr. B.J. van Royen).